
Repositioning of HMG-CoA Reductase Inhibitors as Adjuvants in the Modulation of Efflux Pump-Mediated Bacterial and Tumor Resistance

Abstract
:1. Introduction
2. Antibacterial Effects of Statins
2.1. The Role of HMG-CoA Reductase in Bacteria
2.2. Isoprenoid Intermediates in Bacteria
2.3. The Role of Bacterial Efflux Mechanisms in Antibiotic Resistance and the Effects of Statins on Antibiotic Resistance
2.4. Quorum Sensing: A Possible Target for the Reversal of Efflux-Mediated Resistance
2.5. Statins in Managing Specific Bacterial Infections
3. Anticancer Effects of Statins
3.1. Potential Anticancer Mechanisms of Action of Statins
3.2. Statins in Epidemiologic Studies
3.3. In Vitro Anticancer Effects of Statins
3.4. In Vivo Anticancer Effects of Statins

{kind=link}
{kind=link}
{kind=link}
| Statins | Cancer Type | Study Type | Combination Agent | Findings | Ref. |
|---|---|---|---|---|---|
| Atorvastatin | Breast | In vitro | - | The antiproliferative effects of atorvastatin on breast cancer cells (MCF-7) are mediated by the induction of apoptosis and autophagy. | [212] |
| Simvastatin | In vitro | - | Simvastatin-induced breast cancer cell apoptosis, inhibited proliferation, and the deactivation of PI3K/Akt and MAPK/ERK pathways. | [213] | |
| Simvastatin | In vitro | Doxorubicin | Simvastatin synergistically acts with the anticancer agent doxorubicin against breast cancer MCF-7 cells, probably through a down-regulation of the cell cycle or induction of apoptosis. | [214] | |
| Lovastatin | In vitro | - | Lovastatin-mediated MCF-7 breast cancer cell death involves the activation of LKB1-AMPK-p38MAPK-p53-survivin cascade. | [215] | |
| Mevastatin | In vitro and vivo | Histone deacetylase inhibitors (HDACi) | Combination treatment inhibited autophagic flux by preventing Vps34/Beclin 1 complex formation and downregulating prenylated Rab7, an active form of the small GTPase necessary for autophagosome–lysosome fusion in triple-negative breast cancer cells. | [216] | |
| Lovastatin, mevastatin, pitavastatin calcium, and simvastatin | In vitro | - | Statins possess different anticancer activity in human breast cancer MDA-MB-231 and MCF-7 cell lines. Pitavastatin and simvastatin showed the highest activity in colony formation assay and migration and reduced the growth of MCF-7 spheroids. | [217] | |
| Atorvastatin | In vitro/ex vivo and vivo | - | Statins can block the outgrowth of breast cancer metastases. | [218] | |
| Atorvastatin | Prostate | In vitro | - | Atorvastatin induces autophagy in prostate cancer pC3 cells through the activation of LC3 transcription. | [219] |
| Simvastatin and fluvastatin | In vitro | - | Statins decrease cell proliferation and induce cell apoptosis, possibly mediated through the downregulation of AKT/FOXO1 phosphorylation in prostate cancer cells. | [220] | |
| Atorvastatin, mevastatin, simvastatin and rosuvastatin | In vitro | - | Lipophilic statins reduce the migration and colony formation of PC-3 cells in human bone marrow stroma via inhibiting GGPP production, decreasing the formation, and the spread of metastatic prostate colonies. | [193] | |
| Lovastatin | Ovarian | In vitro and vivo | - | Lovastatin influenced the expression of genes associated with DNA replication, glycolysis, Rho/PLC signaling, and cholesterol biosynthesis pathways. | [221] |
| Simvastatin, atorvastatin, rosuvastatin, lovastatin, fluvastatin, and pravastatin | In vitro | Carboplatin or paclitaxel | All the tested statins except pravastatin demonstrated single-agent activity against monolayers. Statins exhibited conflicting effects on the autophagy pathway. | [222] | |
| Atorvastatin | In vitro | - | The antiproliferative activity of atorvastatin was connected with the induction of apoptosis, autophagy, cellular stress, and cell cycle G1 arrest through the inhibition of AKT/mTOR and the activation of the MAPK pathways. In addition, atorvastatin inhibited cell adhesion, invasion, and decreased the expression of VEGF and MMP 9. c-Myc was downregulated in ovarian cancer, | [223] | |
| Atorvastatin, fluvastatin, and simvastatin | Cervical | In vitro | - | Statins exert antitumor effects on cervical cancer via the inhibition of cell proliferation and the induction of cell death and oxidative stress. | [224] |
| Simvastatin | Gastric | In vitro | - | Simvastatin inhibited the proliferation and migration of intestinal (NCI-N87) and diffuse (Hs746T) metastatic gastric tumor cell lines by reducing mevalonolactone, FPP, and GPP. | [225] |
| Simvastatin | Colorectal | In vitro | - | Simvastatin prompts the apoptosis of human colon cancer cells and inhibits IGF-1-induced ERK and Akt expression via the downregulation of IGF-1R expression and pro-apoptotic ERK activity. | [226] |
| Atorvastatin | In vitro and vivo | Nobiletin | Co-treatments of nobiletin and atorvastatin synergistically induced growth inhibitory effects, extensive cell cycle arrest, and apoptosis on the colon cancer cells. In addition, the combination synergistically enhanced chemopreventive activities against colon carcinogenesis in rats. | [227] | |
| Atorvastatin | Liver | In vitro | - | Atorvastatin induces microRNA-145 expression in hepatic cancer cells HEPG2 through regulation of the PI3K/AKT signaling pathway. | [228] |
| Pravastatin and fluvastatin | In vitro | PBR ligands | Statins induced G1/S cell cycle arrest and apoptosis in hepatocellular carcinoma cells, and the efficacy of treatment with statins was synergistically enhanced by ligands of the peripheral benzodiazepine receptor (PBR). | [229] | |
| Pitavastatin | In vitro and vivo | - | Pitavastatin inhibited growth and colony formation and induced arrest at the G1 phase of liver cancer Huh-7 and SMMC7721 cells. It also promoted caspase-9 and caspase-3 cleavage. Pitavastatin reduced tumor growth and improved the survival of tumor-bearing mice. | [230] | |
| Simvastatin | Lung | In vitro and vivo | - | Simvastatin inhibits proliferation and osteolytic bone metastases of lung adenocarcinoma cells in vitro and in vivo. Its mechanism might be linked with regulating the CD44, P53, and MMP family and inactivating the MAPK/ERK signaling pathway. | [203] |
| Pitavastatin and fluvastatin | In vitro | Erlotinib | Statins/erlotinib combination’s induced cytotoxicity is synergistic, can overcome erlotinib resistance in K-ras-mutated NSCLC, and depends on apoptosis. | [231] | |
| Simvastatin and Lovastatin | Melanoma and neuroblast-oma | In vitro | TRAIL sodium arsenite | Treatment of melanoma cells with statin enhanced TRAIL-induced apoptosis due to suppression of the NF-κB and STAT3-transcriptional targets (including COX-2) and downregulation of cFLIP-L (a caspase-8 inhibitor) protein levels. Moreover, co-treatment with sodium arsenite and TRAIL or simvastatin and TRAIL efficiently induced apoptotic commitment in human neuroblastoma cells. | [232] |
| Lovastatin, atorvastatin, simvastatin, pravastatin, and fluvastatin | Melanoma | In vitro | - | Pravastatin was the least effective cytotoxic of the five tested statins on melanoma cells. Lovastatin produces apoptosis in multiple melanoma cell lines through a geranylation-specific mechanism via caspase-dependent signaling. | [115] |
| Simvastatin | Head and neck | In vitro | Celecoxib | Simvastatin and celecoxib alone and in a combined treatment significantly reduced head and neck SCC viability, proliferation, and the secretion of IL-6 and IL-8. | [233] |
| Simvastatin | In vitro | Monocarboxylate transporter 1 (MCT1) | Simvastatin induces metabolic reprogramming in head and neck squamous cell carcinoma mice, reducing lactate production and promoting cancer sensitivity to MCT1 inhibitors. | [234] | |
| Pitavastatin | In vitro | - | Pitavastatin activates the FOXO3a/PUMA apoptotic axis via regulation of nuclear translocation of FOXO3a through Akt/FOXO3a or AMPK/FOXO3a signaling. | [235] | |
| Atorvastatin | In vitro and vivo | - | Atorvastatin significantly reduced the active form of RhoC in vitro and diminished cell motility, invasion, proliferation, and colony formation. A significant decrease in p-ERK1/2 and p-STAT3 in atorvastatin-treated cell lines was observed. In vivo, experiments have shown the inhibition of angiogenesis and lung metastases. | [236] |
3.5. Clinical Trials of Statins
| Statins | Cancer Type | Phase | No. of Patients | Combination Agent | Findings | Ref. |
|---|---|---|---|---|---|---|
| Fluvastatin | Breast | II | 40 | 3–6 months statin perioperative | After statins use, Ki67 was reduced and caspase 3 increased. | [239] |
| Simvastatin | III | 60 | FAC | Simvastatin combined with FAC shows improvements in objective response rate and pathological response in patients with LABC. | [245] | |
| Atorvastatin | II | 42 | - | Atorvastatin decreased breast cancer proliferation via cell cycle regulatory effects through cyclin D1 and p27. | [246] | |
| Pravastatin | Liver | II | 83 | Transcatheter arterial embolization (TAE) followed by 5-FU | Median survival was 18 months in the pravastatin group compared to 9 months in controls (p = 0.006). | [247] |
| Pravastatin | II | 312 | Sorafenib | A combination of sorafenib and pravastatin did not improve overall survival compared to sorafenib alone. | [248] | |
| Simvastatin | Gastric | III | Capecitabine–cisplatin | Adding simvastatin to capecitabine–cisplatin does not increase PFS. | [249] | |
| Pravastatin | II | 30 | ECC | The addition of pravastatin to ECC in patients with advanced gastric cancer did not improve the outcome. | [250] | |
| Simvastatin | Colorectal | III | 269 | FOLFIRI/XELIRI | Adding simvastatin to the XELIRI/FOLFIRI regimens did not improve PFS in patients with previously treated metastatic colorectal cancer. | [251] |
3.6. Drug Efflux Pumps in Cancer and Modulating Efflux Pumps in Cancer with Statins
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic Effects of Statins on the Cardiovascular System. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef]
- Laufs, U.; Liao, J.K. Isoprenoid Metabolism and the Pleiotropic Effects of Statins. Curr. Atheroscler. Rep. 2003, 5, 372–378. [Google Scholar] [CrossRef]
- Blais, J.E.; Wei, Y.; Yap, K.K.; Alwafi, H.; Ma, T.T.; Brauer, R.; Lau, W.C.; Man, K.K.; Siu, C.W.; Tan, K.C.; et al. Trends in Lipid-Modifying Agent Use in 83 Countries. Atherosclerosis 2021, 328, 44–51. [Google Scholar] [CrossRef]
- Zeichner, S.; Mihos, C.G.; Santana, O. The Pleiotropic Effects and Therapeutic Potential of the Hydroxy-Methyl-Glutaryl-CoA Reductase Inhibitors in Malignancies: A Comprehensive Review. J. Cancer Res. Ther. 2012, 8, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Jiang, X.; Yan, W.; Huang, Q.; Sun, H.; Zhang, X.; Zhang, Z.; Ye, W.; Wu, Y.; Govers, F.; et al. The Mevalonate Pathway Is Important for Growth, Spore Production, and the Virulence of Phytophthora Sojae. Front. Microbiol. 2021, 12, 772994. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.K. Isoprenoids as Mediators of the Biological Effects of Statins. J. Clin. Investig. 2002, 110, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Gbelcová, H.; Rimpelová, S.; Knejzlík, Z.; Šáchová, J.; Kolář, M.; Strnad, H.; Repiská, V.; D’Acunto, W.C.; Ruml, T.; Vítek, L. Isoprenoids Responsible for Protein Prenylation Modulate the Biological Effects of Statins on Pancreatic Cancer Cells. Lipids Health Dis. 2017, 16, 250. [Google Scholar] [CrossRef]
- Lombard, J.; Moreira, D. Origins and Early Evolution of the Mevalonate Pathway of Isoprenoid Biosynthesis in the Three Domains of Life. Mol. Biol. Evol. 2011, 28, 87–99. [Google Scholar] [CrossRef]
- Brown, E.D.; Wright, G.D. Antibacterial Drug Discovery in the Resistance Era. Nature 2016, 529, 336–343. [Google Scholar] [CrossRef]
- Seukep, A.J.; Kuete, V.; Nahar, L.; Sarker, S.D.; Guo, M. Plant-Derived Secondary Metabolites as the Main Source of Efflux Pump Inhibitors and Methods for Identification. J. Pharm. Anal. 2020, 10, 277–290. [Google Scholar] [CrossRef]
- Rácz, B.; Spengler, G. Repurposing Antidepressants and Phenothiazine Antipsychotics as Efflux Pump Inhibitors in Cancer and Infectious Diseases. Antibiotics 2023, 12, 137. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Tong, Z.; Shi, J.; Jia, Y.; Deng, T.; Wang, Z. Reversion of Antibiotic Resistance in Multidrug-Resistant Pathogens Using Non-Antibiotic Pharmaceutical Benzydamine. Commun. Biol. 2021, 4, 1328. [Google Scholar] [CrossRef]
- Varga, B.; Csonka, Á.; Csonka, A.; Molnár, J.; Amaral, L.; Spengler, G. Possible Biological and Clinical Applications of Phenothiazines. Anticancer Res. 2017, 37, 5983–5993. [Google Scholar] [CrossRef] [PubMed]
- Thangamani, S.; Mohammad, H.; Abushahba, M.F.N.; Hamed, M.I.; Sobreira, T.J.P.; Hedrick, V.E.; Paul, L.N.; Seleem, M.N. Exploring Simvastatin, an Antihyperlipidemic Drug, as a Potential Topical Antibacterial Agent. Sci. Rep. 2015, 5, 16407. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Livney, Y.D.; Assaraf, Y.G. Rationally Designed Nanovehicles to Overcome Cancer Chemoresistance. Adv. Drug Deliv. Rev. 2013, 65, 1716–1730. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer Treatment and Survivorship Statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef]
- Ashburn, T.T.; Thor, K.B. Drug Repositioning: Identifying and Developing New Uses for Existing Drugs. Nat. Rev. Drug Discov. 2004, 3, 673–683. [Google Scholar] [CrossRef]
- Pushpakom, S.; Iorio, F.; Eyers, P.A.; Escott, K.J.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug Repurposing: Progress, Challenges and Recommendations. Nat. Rev. Drug Discov. 2019, 18, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Li, J.; Xie, H.; Wang, Y. Review of Drug Repositioning Approaches and Resources. Int. J. Biol. Sci. 2018, 14, 1232–1244. [Google Scholar] [CrossRef] [PubMed]
- Jourdan, J.P.; Bureau, R.; Rochais, C.; Dallemagne, P. Drug Repositioning: A Brief Overview. J. Pharm. Pharmacol. 2020, 72, 1145–1151. [Google Scholar] [CrossRef]
- Antoszczak, M.; Markowska, A.; Markowska, J.; Huczyński, A. Old Wine in New Bottles: Drug Repurposing in Oncology. Eur. J. Pharmacol. 2020, 866, 172784. [Google Scholar] [CrossRef] [PubMed]
- Corbett, A.; Williams, G.; Ballard, C. Drug Repositioning in Alzheimer’s Disease. Front. Biosci. 2015, 7, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Huo, Y.; Zhang, H.Y. Genetic Mechanisms of Asthma and the Implications for Drug Repositioning. Genes 2018, 9, 237. [Google Scholar] [CrossRef]
- Kanzaki, A.; Toi, M.; Nakayama, K.; Bando, H.; Mutoh, M.; Uchida, T.; Fukumoto, M.; Takebayashi, Y. Expression of Multidrug Resistance-Related Transporters in Human Breast Carcinoma. Jpn. J. Cancer Res. 2001, 92, 452–458. [Google Scholar] [CrossRef]
- Baguley, B.C. Multiple Drug Resistance Mechanisms in Cancer. Mol. Biotechnol. 2010, 46, 308–316. [Google Scholar] [CrossRef]
- Divyashree, M.; Mani, M.K.; Reddy, D.; Kumavath, R.; Ghosh, P.; Azevedo, V.; Barh, D. Clinical Applications of Antimicrobial Peptides (AMPs): Where Do We Stand Now? Protein Pept. Lett. 2020, 27, 120–134. [Google Scholar] [CrossRef]
- Fic, M.; Gomulkiewicz, A.; Grzegrzolka, J.; Podhorska-Okolow, M.; Zabel, M.; Dziegiel, P.; Jablonska, K. The Impact of Melatonin on Colon Cancer Cells’ Resistance to Doxorubicin in an In Vitro Study. Int. J. Mol. Sci. 2017, 18, 1396. [Google Scholar] [CrossRef]
- Hennessy, E.; Adams, C.; Reen, F.J.; O’Gara, F. Is There Potential for Repurposing Statins as Novel Antimicrobials? Antimicrob. Agents Chemother. 2016, 60, 5111–5121. [Google Scholar] [CrossRef] [PubMed]
- Masadeh, M.; Mhaidat, N.; Alzoubi, K.; Al-Azzam, S.; Alnasser, Z. Antibacterial activity of statins: A comparative study of atorvastatin, simvastatin, and rosuvastatin. Ann. Clin. Microbiol. Antimicrob. 2012, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Jerwood, S.; Cohen, J. Unexpected Antimicrobial Effect of Statins. J. Antimicrob. Chemother. 2008, 61, 362–364. [Google Scholar] [CrossRef] [PubMed]
- Ko, H.H.T.; Lareu, R.R.; Dix, B.R.; Hughes, J.D. In Vitro Antibacterial Effects of Statins against Bacterial Pathogens Causing Skin Infections. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.; Linde, C.; Pütsep, K.; Pohanka, A.; Normark, S.; Henriques-Normark, B.; Andersson, J.; Björkhem-Bergman, L. Studies on the Antibacterial Effects of Statins—In Vitro and In Vivo. PLoS ONE 2011, 6, e24394. [Google Scholar] [CrossRef] [PubMed]
- Statt, S.; Ruan, J.W.; Hung, L.Y.; Chang, C.Y.; Huang, C.T.; Lim, J.H.; Li, J.D.; Wu, R.; Kao, C.Y. Statin-Conferred Enhanced Cellular Resistance against Bacterial Pore-Forming Toxins in Airway Epithelial Cells. Am. J. Respir. Cell Mol. Biol. 2015, 53, 689–702. [Google Scholar] [CrossRef]
- Kistowska, M.; Rossy, E.; Sansano, S.; Gober, H.J.; Landmann, R.; Mori, L.; De Libero, G. Dysregulation of the Host Mevalonate Pathway during Early Bacterial Infection Activates Human TCR Γδ Cells. Eur. J. Immunol. 2008, 38, 2200–2209. [Google Scholar] [CrossRef]
- de Paula, T.P.; Santos, P.C.; do Nascimento Arifa, R.D.; Vieira, A.T.; de Matos Baltazar, L.; Ávila, T.V.; Fagundes, C.T.; Garcia, Z.M.; Lima, R.L.; Teixeira, M.M.; et al. Treatment with Atorvastatin Provides Additional Benefits to Imipenem in a Model of Gram-Negative Pneumonia Induced by Klebsiella pneumoniae in Mice. Antimicrob. Agents Chemother. 2018, 62, e00764-17. [Google Scholar] [CrossRef]
- Mehl, A.; Harthug, S.; Lydersen, S.; Paulsen, J.; Åsvold, B.O.; Solligård, E.; Damås, J.K.; Edna, T.H. Prior Statin Use and 90-Day Mortality in Gram-Negative and Gram-Positive Bloodstream Infection: A Prospective Observational Study. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 609–617. [Google Scholar] [CrossRef]
- Ghayda, R.A.; Han, C.H.; Lee, K.H.; Kim, J.S.; Kim, S.E.; Hong, S.H.; Kim, M.; Kronbichler, A.; Tizaoui, K.; Li, H.; et al. The Effect of Statins on Mortality among Patients with Infection: Umbrella Review of Meta-Analyses. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2685–2695. [Google Scholar] [CrossRef]
- Duan, H.; Liu, T.; Zhang, X.; Yu, A.; Cao, Y. Statin Use and Risk of Tuberculosis: A Systemic Review of Observational Studies. Int. J. Infect. Dis. 2020, 93, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Grudzinska, F.S.; Davinder, D.P.S.; Parekh, D.; Rachel, D.C.A.; Jaimin, P.; Nightingale, P.; Walton, G.M.; Sapey, E.; Thickett, D.R. Statin Therapy in Patients with Community-Acquired Pneumonia. Clin. Med. 2017, 17, 403–407. [Google Scholar] [CrossRef]
- Xu, Q.; Zheng, B.; Shen, P.; Xiao, Y. Protective Efficacy of Statins in Patients with Klebsiella pneumoniae Bloodstream Infection. Front. Cell. Infect. Microbiol. 2023, 12, 1087701. [Google Scholar] [CrossRef]
- Parihar, S.P.; Guler, R.; Khutlang, R.; Lang, D.M.; Hurdayal, R.; Mhlanga, M.M.; Suzuki, H.; Marais, A.D.; Brombacher, F. Statin Therapy Reduces the Mycobacterium tuberculosis Burden in Human Macrophages and in Mice by Enhancing Autophagy and Phagosome Maturation. J. Infect. Dis. 2014, 209, 754–763. [Google Scholar] [CrossRef]
- Mishra, R.; Krishan, S.; Siddiqui, A.N.; Kapur, P.; Khayyam, K.U.; Sharma, M. Potential Role of Adjuvant Drugs on Efficacy of First Line Oral Antitubercular Therapy: Drug Repurposing. Tuberculosis 2020, 120, 101902. [Google Scholar] [CrossRef]
- Foster, T.J. Can β-Lactam Antibiotics Be Resurrected to Combat MRSA? Trends Microbiol. 2019, 27, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Janda, S.; Young, A.; FitzGerald, J.M.; Etminan, M.; Swiston, J. The Effect of Statins on Mortality from Severe Infections and Sepsis: A Systematic Review and Meta-Analysis. J. Crit. Care 2010, 25, 656.e7–656.e22. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Wen, X.; Peng, J.; Lu, Y.; Guo, Z.; Lu, J. Systematic Review and Meta-Analysis on the Association between Outpatient Statins Use and Infectious Disease-Related Mortality. PLoS ONE 2012, 7, e51548. [Google Scholar] [CrossRef]
- Wilding, E.I.; Brown, J.R.; Bryant, A.P.; Chalker, A.F.; Holmes, D.J.; Ingraham, K.A.; Iordanescu, S.; So, C.Y.; Rosenberg, M.; Gwynn, M.N. Identification, Evolution, and Essentiality of the Mevalonate Pathway for Isopentenyl Diphosphate Biosynthesis in Gram-Positive Cocci. J. Bacteriol. 2000, 182, 4319–4327. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Yasukawa, J.; Ishii, M.; Hayashi, Y.; Miyazaki, S.; Sekimizu, K. A Critical Role of Mevalonate for Peptidoglycan Synthesis in Staphylococcus aureus. Sci. Rep. 2016, 6, 22894. [Google Scholar] [CrossRef]
- Kuzuyama, T.; Hemmi, H.; Takahashi, S. Mevalonate Pathway in Bacteria and Archaea. In Comprehensive Natural Products II; Elsevier: Amsterdam, The Netherlands, 2010; Volume 1, pp. 493–516. [Google Scholar]
- Lee, E.D.; Navas, K.I.; Portnoy, D.A. The Nonmevalonate Pathway of Isoprenoid Biosynthesis Supports Anaerobic Growth of Listeria monocytogenes. Infect. Immun. 2020, 88, e00788-19. [Google Scholar] [CrossRef] [PubMed]
- Heuston, S.; Begley, M.; Davey, M.S.; Eberl, M.; Casey, P.G.; Hill, C.; Gahan, C.G.M. HmgR, a Key Enzyme in the Mevalonate Pathway for Isoprenoid Biosynthesis, Is Essential for Growth of Listeria monocytogenes EGDe. Microbiology 2012, 158, 1684–1693. [Google Scholar] [CrossRef] [PubMed]
- Begley, M.; Gahan, C.G.M.; Kollas, A.K.; Hintz, M.; Hill, C.; Jomaa, H.; Eberl, M. The Interplay Between Classical and Alternative Isoprenoid Biosynthesis Controls Γδ T Cell Bioactivity of Listeria monocytogenes. FEBS Lett. 2004, 561, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Begley, M.; Bron, P.A.; Heuston, S.; Casey, P.G.; Englert, N.; Wiesner, J.; Jomaa, H.; Gahan, C.G.M.; Hill, C. Analysis of the Isoprenoid Biosynthesis Pathways in Listeria monocytogenes Reveals a Role for the Alternative 2-C-Methyl-D-Erythritol 4-Phosphate Pathway in Murine Infection. Infect. Immun. 2008, 76, 5392–5401. [Google Scholar] [CrossRef] [PubMed]
- Du, D.; Wang-Kan, X.; Neuberger, A.; van Veen, H.W.; Pos, K.M.; Piddock, L.J.V.; Luisi, B.F. Multidrug Efflux Pumps: Structure, Function and Regulation. Nat. Rev. Microbiol. 2018, 16, 523–539. [Google Scholar] [CrossRef]
- Kawai, Y.; Mickiewicz, K.; Errington, J. Lysozyme Counteracts β-Lactam Antibiotics by Promoting the Emergence of L-Form Bacteria. Cell 2018, 172, 1038–1049.e10. [Google Scholar] [CrossRef]
- Vandevelde, N.M.; Tulkens, P.M.; Van Bambeke, F. Modulating Antibiotic Activity towards Respiratory Bacterial Pathogens by Co-Medications: A Multi-Target Approach. Drug Discov. Today 2016, 21, 1114–1129. [Google Scholar] [CrossRef]
- Al-Quadan, T.; Price, C.T.; London, N.; Schueler-Furman, O.; AbuKwaik, Y. Anchoring of Bacterial Effectors to Host Membranes through Host-Mediated Lipidation by Prenylation: A Common Paradigm. Trends Microbiol. 2011, 19, 573–579. [Google Scholar] [CrossRef]
- Marakasova, E.S.; Akhmatova, N.K.; Amaya, M.; Eisenhaber, B.; Eisenhaber, F.; van Hoek, M.L.; Baranova, A.V. Prenylation: From Bacteria to Eukaryotes. Mol. Biol. 2013, 47, 622–633. [Google Scholar] [CrossRef]
- Wassmann, C.S.; Rolsted, A.P.; Lyngsie, M.C.; Torres-Puig, S.; Kronborg, T.; Vestergaard, M.; Ingmer, H.; Pontoppidan, S.P.; Klitgaard, J.K. The Menaquinone Pathway Is Important for Susceptibility of Staphylococcus aureus to the Antibiotic Adjuvant, Cannabidiol. Microbiol. Res. 2022, 257, 126974. [Google Scholar] [CrossRef]
- Bouhss, A.; Trunkfield, A.E.; Bugg, T.D.H.; Mengin-Lecreulx, D. The Biosynthesis of Peptidoglycan Lipid-Linked Intermediates. FEMS Microbiol. Rev. 2008, 32, 208–233. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.D.; McDowell, S.A. Pleiotropic Effects of Statins: New Therapeutic Approaches to Chronic, Recurrent Infection by Staphylococcus aureus. Pharmaceutics 2021, 13, 2047. [Google Scholar] [CrossRef] [PubMed]
- Manalo, R.V.M.; Josol, V.J.D.; Gloriani, N.G. The Differential Effects of Atorvastatin Co-Administered with Ampicillin on the Bacterial Growth and Biofilm Formation of Staphylococcus aureus. Curr. Med. Res. Pract. 2017, 7, 178–183. [Google Scholar] [CrossRef]
- Ko, H.H.T.; Lareu, R.R.; Dix, B.R.; Hughes, J.D. Statins: Antimicrobial Resistance Breakers or Makers? PeerJ 2017, 5, e3952. [Google Scholar] [CrossRef]
- Nassaji, M.; Ghorbani, R.; Afshar, R.K. The Effect of Statins Use on the Risk and Outcome of Acute Bacterial Infections in Adult Patients. J. Clin. Diagn. Res. 2015, 9, OC09–OC12. [Google Scholar] [CrossRef]
- Bose, S.; Steussy, C.N.; López-Pérez, D.; Schmidt, T.; Kulathunga, S.C.; Seleem, M.N.; Lipton, M.; Mesecar, A.D.; Rodwell, V.W.; Stauffacher, C.V. Targeting Enterococcus Faecalis HMG-CoA Reductase with a Non-Statin Inhibitor. Commun. Biol. 2023, 6, 360. [Google Scholar] [CrossRef]
- Sherman, M.M.; Petersen, L.A.; Dale Poulter, C. Isolation and Characterization of Isoprene Mutants of Escherichia coli. J. Bacteriol. 1989, 171, 3619–3628. [Google Scholar] [CrossRef]
- Liu, C.I.; Liu, G.Y.; Song, Y.; Yin, F.; Hensler, M.E.; Jeng, W.Y.; Nizet, V.; Wang, A.H.J.; Oldfield, E. A Cholesterol Biosynthesis Inhibitor Blocks Staphylococcus aureus Virulence. Science 2008, 319, 1391–1394. [Google Scholar] [CrossRef]
- Rudolf, J.D.; Alsup, T.A.; Xu, B.; Li, Z. Bacterial Terpenome. Nat. Prod. Rep. 2021, 38, 905–980. [Google Scholar] [CrossRef]
- Dias, K.J.S.D.O.; Miranda, G.M.; Bessa, J.R.; Araújo, A.C.J.D.; Freitas, P.R.; Almeida, R.S.D.; Paulo, C.L.R.; Neto, J.B.D.A.; Coutinho, H.D.M.; Ribeiro-Filho, J. Terpenes as Bacterial Efflux Pump Inhibitors: A Systematic Review. Front. Pharmacol. 2022, 13, 953982. [Google Scholar] [CrossRef]
- Nickels, J.D.; Poudel, S.; Chatterjee, S.; Farmer, A.; Cordner, D.; Campagna, S.R.; Giannone, R.J.; Hettich, R.L.; Myles, D.A.A.; Standaert, R.F.; et al. Impact of Fatty-Acid Labeling of Bacillus subtilis Membranes on the Cellular Lipidome and Proteome. Front. Microbiol. 2020, 11, 914. [Google Scholar] [CrossRef] [PubMed]
- García-Fernández, E.; Koch, G.; Wagner, R.M.; Fekete, A.; Stengel, S.T.; Schneider, J.; Mielich-Süss, B.; Geibel, S.; Markert, S.M.; Stigloher, C.; et al. Membrane Microdomain Disassembly Inhibits MRSA Antibiotic Resistance. Cell 2017, 171, 1354–1367.e20. [Google Scholar] [CrossRef]
- Nowicka, B.; Kruk, J. Occurrence, Biosynthesis and Function of Isoprenoid Quinones. Biochim. et Biophys. Acta (BBA)-Bioenerg. 2010, 1797, 1587–1605. [Google Scholar] [CrossRef] [PubMed]
- Abby, S.S.; Kazemzadeh, K.; Vragniau, C.; Pelosi, L.; Pierrel, F. Advances in Bacterial Pathways for the Biosynthesis of Ubiquinone. Biochim. et Biophys. Acta (BBA)-Bioenerg. 2020, 1861, 148259. [Google Scholar] [CrossRef] [PubMed]
- Pierrel, F.; Burgardt, A.; Lee, J.H.; Pelosi, L.; Wendisch, V.F. Recent Advances in the Metabolic Pathways and Microbial Production of Coenzyme Q. World J. Microbiol. Biotechnol. 2022, 38, 58. [Google Scholar] [CrossRef] [PubMed]
- Mitchison-Field, L.M.; Belin, B.J. Bacterial Lipid Biophysics and Membrane Organization. Curr. Opin. Microbiol. 2023, 74, 102315. [Google Scholar] [CrossRef]
- López, D.; Kolter, R. Functional Microdomains in Bacterial Membranes. Genes Dev. 2010, 24, 1893–1902. [Google Scholar] [CrossRef]
- De Gaetano, G.V.; Lentini, G.; Famà, A.; Coppolino, F.; Beninati, C. Antimicrobial Resistance: Two-Component Regulatory Systems and Multidrug Efflux Pumps. Antibiotics 2023, 12, 965. [Google Scholar] [CrossRef]
- Varela, M.F.; Stephen, J.; Lekshmi, M.; Ojha, M.; Wenzel, N.; Sanford, L.M.; Hernandez, A.J.; Parvathi, A.; Kumar, S.H. Bacterial Resistance to Antimicrobial Agents. Antibiotics 2021, 10, 593. [Google Scholar] [CrossRef]
- Teelucksingh, T.; Thompson, L.K.; Cox, G. The Evolutionary Conservation of Escherichia coli Drug Efflux Pumps Supports Physiological Functions. J. Bacteriol. 2020, 202, e00367-20. [Google Scholar] [CrossRef]
- Sharma, A.; Gupta, V.K.; Pathania, R. Efflux Pump Inhibitors for Bacterial Pathogens: From Bench to Bedside. Indian J. Med. Res. 2019, 149, 129–145. [Google Scholar] [CrossRef]
- Baran, A.; Kwiatkowska, A.; Potocki, L. Antibiotics and Bacterial Resistance—A Short Story of an Endless Arms Race. Int. J. Mol. Sci. 2023, 24, 5777. [Google Scholar] [CrossRef]
- Figueiredo, E.P.; Ribeiro, J.M.; Nishio, E.K.; Scandorieiro, S.; Costa, A.F.; Cardozo, V.F.; Oliveira, A.G.; Durán, N.; Panagio, L.A.; Kobayashi, R.K.T.; et al. New Approach for Simvastatin as an Antibacterial: Synergistic Effect with Bio-Synthesized Silver Nanoparticles against Multidrug-Resistant Bacteria. Int. J. Nanomed. 2019, 14, 7975–7985. [Google Scholar] [CrossRef]
- Cook, G.M.; Greening, C.; Hards, K.; Berney, M. Energetics of Pathogenic Bacteria and Opportunities for Drug Development. In Advances in Microbial Physiology; Academic Press: Cambridge, MA, USA, 2014; Volume 65, pp. 1–62. [Google Scholar] [CrossRef]
- Koyama, N.; Inokoshi, J.; Tomoda, H. Anti-Infectious Agents against MRSA. Molecules 2013, 18, 204–224. [Google Scholar] [CrossRef]
- Reusch, V.M. Lipopolymers, Isoprenoids, and the Assembly of the Gram-Positive Cell Wall. Crit. Rev. Microbiol. 1984, 11, 129–155. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M. The Mycobacterial Cell Envelope-Lipids. Cold Spring Harb. Perspect. Med. 2014, 4, a021105. [Google Scholar] [CrossRef] [PubMed]
- Saalim, M.; Villegas-Moreno, J.; Clark, B.R. Bacterial Alkyl-4-Quinolones: Discovery, Structural Diversity and Biological Properties. Molecules 2020, 25, 5689. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Bassler, B.L. Bacterial Quorum Sensing in Complex and Dynamically Changing Environments. Nat. Rev. Microbiol. 2019, 17, 371–382. [Google Scholar] [CrossRef]
- Whiteley, M.; Diggle, S.P.; Greenberg, E.P. Progress in and Promise of Bacterial Quorum Sensing Research. Nature 2017, 551, 313–320. [Google Scholar] [CrossRef] [PubMed]
- López, D.; Vlamakis, H.; Kolter, R. Biofilms. Cold Spring Harb. Perspect. Biol. 2010, 2, a000398. [Google Scholar] [CrossRef]
- Yang, S.; Lopez, C.R.; Lynn Zechiedrich, E. Quorum Sensing and Multidrug Transporters in Escherichia coli. Proc. Natl. Acad. Sci. USA 2006, 103, 2386–2391. [Google Scholar] [CrossRef] [PubMed]
- Cabuhat, K.S.P.; Moron-Espiritu, L.S. Quorum Sensing Orchestrates Antibiotic Drug Resistance, Biofilm Formation, and Motility in Escherichia coli and Quorum Quenching Activities of Plant-Derived Natural Products: A Review. J. Pure Appl. Microbiol. 2022, 16, 1538–1549. [Google Scholar] [CrossRef]
- Hennessy, E.; Mooij, M.J.; Legendre, C.; Jerry Reen, F.; O’Callaghan, J.; Adams, C.; O’Gara, F. Statins Inhibit In Vitro Virulence Phenotypes of Pseudomonas aeruginosa. J. Antibiot. 2013, 66, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Stoltz, D.A.; Ozer, E.A.; Ng, C.J.; Yu, J.M.; Reddy, S.T.; Lusis, A.J.; Bourquard, N.; Parsek, M.R.; Zabner, J.; Shih, D.M. Paraoxonase-2 Deficiency Enhances Pseudomonas aeruginosa Quorum Sensing in Murine Tracheal Epithelia. Am. J. Physiol. Lung. Cell. Mol. Physiol. 2007, 292, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Ozer, E.A.; Pezzulo, A.; Shih, D.M.; Chun, C.; Furlong, C.; Lusis, A.J.; Greenberg, E.P.; Zabner, J. Human and Murine Paraoxonase 1 Are Host Modulators of Pseudomonas aeruginosa Quorum-Sensing. FEMS Microbiol. Lett. 2005, 253, 29–37. [Google Scholar] [CrossRef]
- Gajdács, M.; Spengler, G. The Role of Drug Repurposing in the Development of Novel Antimicrobial Drugs: Non-Antibiotic Pharmacological Agents as Quorum Sensing-Inhibitors. Antibiotics 2019, 8, 270. [Google Scholar] [CrossRef]
- Verma, N.; Srivastava, S.; Malik, R.; Goyal, P.; Pandey, J. Inhibition and Disintegration of Bacillus subtilis Biofilm with Small Molecule Inhibitors Identified through Virtual Screening for Targeting TasA(28–261), the Major Protein Component of ECM. J. Biomol. Struct. Dyn. 2023, 41, 2431–2447. [Google Scholar] [CrossRef]
- Santajit, S.; Sookrung, N.; Indrawattana, N. Quorum Sensing in ESKAPE Bugs: A Target for Combating Antimicrobial Resistance and Bacterial Virulence. Biology 2022, 11, 1466. [Google Scholar] [CrossRef]
- Alav, I.; Sutton, J.M.; Rahman, K.M. Role of Bacterial Efflux Pumps in Biofilm Formation. J. Antimicrob. Chemother. 2018, 73, 2003–2020. [Google Scholar] [CrossRef]
- Sionov, R.V.; Steinberg, D. Targeting the Holy Triangle of Quorum Sensing, Biofilm Formation, and Antibiotic Resistance in Pathogenic Bacteria. Microorganisms 2022, 10, 1239. [Google Scholar] [CrossRef]
- Abdelaziz, A.A.; El-Barrawy, M.A.; El-Nagar, R.A.M. Potent Synergistic Combination of Rosuvastatin and Levofloxacin against Staphylococcus aureus: In Vitro and in Vivo Study. J. Appl. Microbiol. 2021, 131, 182–196. [Google Scholar] [CrossRef]
- Graziano, T.S.; Cuzzullin, M.C.; Franco, G.C.; Schwartz-Filho, H.O.; De Andrade, E.D.; Groppo, F.C.; Cogo-Müller, K. Statins and Antimicrobial Effects: Simvastatin as a Potential Drug against Staphylococcus aureus Biofilm. PLoS ONE 2015, 10, e0128098. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.G.; Barry, C.E.; Flynn, J.L. Tuberculosis: What We Don’t Know Can, and Does, Hurt Us. Science 2010, 328, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Del Carmen Guerra-De-Blas, P.; Torres-González, P.; Bobadilla-Del-Valle, M.; Sada-Ovalle, I.; Ponce-De-León-Garduño, A.; Sifuentes-Osornio, J. Potential Effect of Statins on Mycobacterium tuberculosis Infection. J. Immunol. Res. 2018, 2018, 7617023. [Google Scholar] [CrossRef]
- Parikh, A.; Childress, C.; Deitrick, K.; Lin, Q.; Rukstalis, D.; Yang, W. Statin-Induced Autophagy by Inhibition of Geranylgeranyl Biosynthesis in Prostate Cancer PC3 Cells. Prostate 2010, 70, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Dutta, N.K.; Bruiners, N.; Pinn, M.L.; Zimmerman, M.D.; Prideaux, B.; Dartois, V.; Gennaro, M.L.; Karakousis, P.C. Statin Adjunctive Therapy Shortens the Duration of TB Treatment in Mice. J. Antimicrob. Chemother. 2016, 71, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Lin, K.D.; Hsu, W.H.; Chang, H.L.; Yang, Y.H.; Hsiao, P.J.; Shin, S.J. Statin, Calcium Channel Blocker and Beta Blocker Therapy May Decrease the Incidence of Tuberculosis Infection in Elderly Taiwanese Patients with Type 2 Diabetes. Int. J. Mol. Sci. 2015, 16, 11369–11384. [Google Scholar] [CrossRef]
- Meregildo-Rodriguez, E.D.; Chunga-Chévez, E.V.; Gianmarco, R.A.L.; Vásquez-Tirado, G.A. Further Insights into to the Role of Statins against Active Tuberculosis: Systematic Review and Meta-Analysis. Infez. Med. 2022, 30, 194–203. [Google Scholar] [CrossRef]
- Caffrey, A.R.; Timbrook, T.T.; Noh, E.; Sakoulas, G.; Opal, S.M.; Nizet, V.; Laplante, K.L. Evidence to Support Continuation of Statin Therapy in Patients with Staphylococcus aureus Bacteremia. Antimicrob. Agents Chemother. 2017, 61, e02228-16. [Google Scholar] [CrossRef]
- Liappis, A.P.; Kan, V.L.; Rochester, C.G.; Simon, G.L. The Effect of Statins on Mortality in Patients with Bacteremia. Clin. Infect. Dis. 2001, 33, 1352–1357. [Google Scholar] [CrossRef]
- López-Cortés, L.E.; Gálvez-Acebal, J.; Del Toro, M.D.; Velasco, C.; De Cueto, M.; Caballero, F.J.; Muniain, M.A.; Pascual, Á.; Rodríguez-Baño, J. Effect of Statin Therapy in the Outcome of Bloodstream Infections Due to Staphylococcus aureus: A Prospective Cohort Study. PLoS ONE 2013, 8, e82958. [Google Scholar] [CrossRef] [PubMed]
- Jakobisiak, M.; Golab, J. Potential Antitumor Effects of Statins (Review). Int. J. Oncol. 2003, 23, 1055–1069. [Google Scholar] [CrossRef] [PubMed]
- Shellman, Y.G.; Ribble, D.; Miller, L.; Gendall, J.; VanBuskirk, K.; Kelly, D.; Norris, D.A.; Dellavalle, R.P. Lovastatin-Induced Apoptosis in Human Melanoma Cell Lines. Melanoma Res. 2005, 15, 83–89. [Google Scholar] [CrossRef]
- Gbelcová, H.; Leníček, M.; Zelenka, J.; Knejzlík, Z.; Dvořáková, G.; Zadinová, M.; Poučková, P.; Kudla, M.; Balaž, P.; Ruml, T.; et al. Differences in Antitumor Effects of Various Statins on Human Pancreatic Cancer. Int. J. Cancer 2008, 122, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Gizzo, S.; Quaranta, M.; Battista Nardelli, G.; Noventa, M. Lipophilic Statins as Anticancer Agents: Molecular Targeted Actions and Proposal in Advanced Gynaecological Malignancies. Curr. Drug Targets 2015, 16, 1142–1159. [Google Scholar] [CrossRef] [PubMed]
- Sheikholeslami, K.; Sher, A.A.; Lockman, S.; Kroft, D.; Ganjibakhsh, M.; Nejati-Koshki, K.; Shojaei, S.; Ghavami, S.; Rastegar, M. Simvastatin Induces Apoptosis in Medulloblastoma Brain Tumor Cells via Mevalonate Cascade Prenylation Substrates. Cancers 2019, 11, 994. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Karamouzis, M.V.; Papavassiliou, A.G. Post-Translational Modifications and Regulation of the RAS Superfamily of GTPases as Anticancer Targets. Nat. Rev. Drug Discov. 2007, 6, 541–555. [Google Scholar] [CrossRef]
- Riganti, C.; Aldieri, E.; Doublier, S.; Bosia, A.; Ghigo, D. Statins-Mediated Inhibition of Rho GTPases as a Potential Tool in Anti-Tumor Therapy. Mini Rev. Med. Chem. 2008, 8, 609–618. [Google Scholar] [CrossRef]
- Kazanietz, M.G.; Caloca, M.J. The Rac GTPase In Cancer: From Old Concepts to New Paradigms. Cancer Res. 2017, 77, 5445–5451. [Google Scholar] [CrossRef]
- Matusewicz, L.; Meissner, J.; Toporkiewicz, M. The Effect of Statins on Cancer Cells—Review. Tumor Biol. 2015, 36, 4889–4904. [Google Scholar] [CrossRef]
- Ahmadi, M.; Amiri, S.; Pecic, S.; Machaj, F.; Rosik, J.; Łos, M.J.; Alizadeh, J.; Mahdian, R.; Simone, C.; Rosa, S.; et al. Molecular Basis of Disease Pleiotropic Effects of Statins: A Focus on Cancer. Biochim. Biophys. Acta–Mol. Basis Dis. 2020, 1866, 165968. [Google Scholar] [CrossRef] [PubMed]
- Li, M.I.N.; Min, W.E.I.; Wang, J.; Wang, L.U.; Li, Y.A.N.; Zhou, N.; Yang, Z.; Qian, Q. Effects of Mevalonate Kinase Interference on Cell Differentiation, Apoptosis, Prenylation and Geranylgeranylation of Human Keratinocytes Are Attenuated by Farnesyl Pyrophosphate or Geranylgeranyl Pyrophosphate. Exp. Ther. Med. 2020, 19, 2861–2870. [Google Scholar] [CrossRef] [PubMed]
- Reuter, C.W.M.; Morgan, M.A.; Bergmann, L. Review Article Targeting the Ras Signaling Pathway: A Rational, Mechanism-Based Treatment for Hematologic Malignancies? The RAS Gene Family. Blood 2000, 96, 1655–1669. [Google Scholar] [CrossRef] [PubMed]
- Denoyelle, C.; Vasse, M.; Ko, M.; Vannier, J.; Mishal, Z.; Ganne, F.; Soria, J.; Soria, C. Cerivastatin, an Inhibitor of HMG-CoA Reductase, Inhibits the Signaling Pathways Involved in the Invasiveness and Metastatic Properties of Highly Invasive Breast Cancer Cell Lines: An In Vitro Study. Carcinogenesis 2001, 22, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Waller, D.D.; Park, J.; Tsantrizos, Y.S. Inhibition of Farnesyl Pyrophosphate (FPP) and/or Geranylgeranyl Pyrophosphate (GGPP) Biosynthesis and Its Implication in the Treatment of Cancers. Crit. Rev. Biochem. Mol. Biol. 2019, 54, 41–60. [Google Scholar] [CrossRef] [PubMed]
- Ricco, N.; Flor, A.; Wolfgeher, D.; Efimova, E.V.; Ramamurthy, A.; Appelbe, O.K.; Brinkman, J.; Truman, A.W.; Spiotto, M.T.; Kron, S.J. Mevalonate Pathway Activity as a Determinant of Radiation Sensitivity in Head and Neck Cancer. Mol. Oncol. 2019, 13, 1927–1943. [Google Scholar] [CrossRef] [PubMed]
- Zeki, A.A.; Bratt, J.M.; Chang, K.Y.; Franzi, L.M.; Ott, S.; Silveria, M.; Fiehn, O.; Last, J.A.; Kenyon, N.J. Intratracheal Instillation of Pravastatin for the Treatment of Murine Allergic Asthma: A Lung-Targeted Approach to Deliver Statins. Physiol. Rep. 2015, 3, e12352. [Google Scholar] [CrossRef]
- Hu, M.; Tomlinson, B. Evaluation of the Pharmacokinetics and Drug Interactions of the Two Recently Developed Statins, Rosuvastatin and Pitavastatin. Expert Opin. Drug Metab. Toxicol. 2014, 10, 51–65. [Google Scholar] [CrossRef]
- Kato, S.; Smalley, S.; Sadarangani, A.; Chen-Lin, K.; Oliva, B.; Brañes, J.; Carvajal, J.; Gejman, R.; Owen, G.I.; Cuello, M. Lipophilic but Not Hydrophilic Statins Selectively Induce Cell Death in Gynecological Cancers Expressing High Levels of HMG-CoA Reductase. J. Cell. Mol. Med. 2010, 14, 1180–1193. [Google Scholar] [CrossRef]
- Amerongen, G.P.V.N.; Koolwijk, P.; Versteilen, A.; Hinsbergh, V.W.M. Endothelial Cell Migration and Angiogenesis In Vitro. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 211–217. [Google Scholar] [CrossRef]
- Jo, A.; Dembinska-Kiec, A.; Guevara, I.; Zdzienicka, A.; Zmudzinska-Grochot, D.; Florek, I.; Wo, A.; Szuba, A.; Cooke, J.P. Nitric Oxide Induces the Synthesis of Vascular Endothelial Growth Factor by Rat Vascular Smooth Muscle Cells. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 659–666. [Google Scholar] [CrossRef]
- Weis, M.; Heeschen, C.; Glassford, A.J.; Cooke, J.P. Statins Have Biphasic Effects on Angiogenesis. Circulation 2002, 105, 739–745. [Google Scholar] [CrossRef]
- Dworacka, M.; Iskakova, S.; Weso, A.; Zharmakhanova, G. Simvastatin Attenuates the Aberrant Expression of Angiogenic Factors Induced by Glucose Variability. Diabetes Res. Clin. Pract. 2018, 143, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Asakage, M.; Tsuno, N.H.; Kitayama, J.; Kawai, K. 3-Hydroxy-3-Methylglutaryl-Coenzyme A Reductase Inhibitor (Pravastatin) Inhibits Endothelial Cell Proliferation Dependent on G 1 Cell Cycle Arrest. Anticancer Drugs 2004, 15, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Kusama, T.; Mukai, M.; Akedo, H.; Inoue, M.; Nakamura, H.; Iwasaki, T.; Tatsuta, M. 3-Hydroxy-3-Methylglutaryl-Coenzyme a Reductase Inhibitors Reduce Human Pancreatic Cancer Cell Invasion and Metastasis. Gastroenterology 2002, 122, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Stine, J.E.; Han, X.; Schointuch, M.; Zhou, C.; Gilliam, T.; Gehrig, P.A.; Bae-Jump, V.L. The HMG-CoA Reductase Inhibitor Simvastatin Exhibits Antitumorigenic and Antimetastatic Effects in Ovarian Cancer. Gynecol. Oncol. 2014, 133, 111–112. [Google Scholar] [CrossRef]
- Nübel, T.; Dippold, W.; Kleinert, H.; Kaina, B.; Fritz, G. Lovastatin Inhibits Rho-Regulated Expression of E-Selectin by TNFalpha and Attenuates Tumor Cell Adhesion. FASEB J. 2004, 18, 140–142. [Google Scholar] [CrossRef]
- Silva, J.; Beckedorf, A.; Bieberich, E. Osteoblast-Derived Oxysterol Is a Migration-Inducing Factor for Human Breast Cancer Cells. J. Biol. Chem. 2003, 278, 25376–25385. [Google Scholar] [CrossRef]
- Fang, Z.; Tang, Y.; Fang, J.; Zhou, Z.; Xing, Z.; Guo, Z.; Guo, X.; Wang, W.; Jiao, W.; Xu, Z.; et al. Simvastatin Inhibits Renal Cancer Cell Growth and Metastasis via AKT/MTOR, ERK and JAK2/STAT3 Pathway. PLoS ONE 2013, 8, e62823. [Google Scholar] [CrossRef]
- Fan, Z.; Jiang, H.; Wang, Z.; Qu, J. Atorvastatin Partially Inhibits the Epithelial-Mesenchymal Transition in A549 Cells Induced by TGF-Β1 by Attenuating the Upregulation of SphK1. Oncol. Rep. 2016, 36, 1016–1022. [Google Scholar] [CrossRef]
- Siddiqui, R.A.; Harvey, K.A.; Xu, Z.; Natarajan, S.K.; Davisson, V.J. Characterization of Lovastatin-Docosahexaenoate Anticancer Properties against Breast Cancer Cells. Bioorg. Med. Chem. 2014, 22, 1899–1908. [Google Scholar] [CrossRef] [PubMed]
- Ghalali, A.; Wiklund, F.; Zheng, H.; Stenius, U.; Högberg, J. Atorvastatin Prevents ATP-Driven Invasiveness via P2X7 and EHBP1 Signaling in PTEN-Expressing Prostate Cancer Cells. Carcinogenesis 2014, 35, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Bi, E.; Lu, Y.; Su, P.; Huang, C.; Liu, L.; Wang, Q.; Yang, M.; Kalady, M.F.; Qian, J.; et al. Cholesterol Induces CD8+ T Cell Exhaustion in the Tumor Microenvironment. Cell. Metab. 2019, 30, 143–156.e5. [Google Scholar] [CrossRef]
- Gruenbacher, G.; Gander, H.; Nussbaumer, O.; Nussbaumer, W.; Rahm, A.; Thurnher, M. IL-2 Costimulation Enables Statin-Mediated Activation of Human NK Cells, Preferentially through a Mechanism Involving CD56+ Dendritic Cells. Cancer Res. 2010, 70, 9611–9620. [Google Scholar] [CrossRef] [PubMed]
- Poggi, A.; Boero, S.; Musso, A.; Zocchi, M.R. Selective Role of Mevalonate Pathway in Regulating Perforin but Not FasL and TNFalpha Release in Human Natural Killer Cells. PLoS ONE 2013, 8, e62932. [Google Scholar] [CrossRef]
- Kladniew, B.R.; Polo, M.; Montero Villegas, S.; Galle, M.; Crespo, R.; García De Bravo, M. Synergistic Antiproliferative and Anticholesterogenic Effects of Linalool, 1,8-Cineole, and Simvastatin on Human Cell Lines. Chem. Biol. Interact. 2014, 214, 57–68. [Google Scholar] [CrossRef]
- Zhong, S.; Zhang, X.; Chen, L.; Ma, T.; Tang, J.; Zhao, J. Statin Use and Mortality in Cancer Patients: Systematic Review and Meta-Analysis of Observational Studies. Cancer Treat. Rev. 2015, 41, 554–567. [Google Scholar] [CrossRef] [PubMed]
- Kuoppala, J.; Lamminpää, A.; Pukkala, E. Statins and Cancer: A Systematic Review and Meta-Analysis. Eur. J. Cancer 2008, 44, 2122–2132. [Google Scholar] [CrossRef]
- Liu, B.; Yi, Z.; Guan, X.; Zeng, Y.X.; Ma, F. The Relationship between Statins and Breast Cancer Prognosis Varies by Statin Type and Exposure Time: A Meta-Analysis. Breast Cancer Res. Treat. 2017, 164, 1–11. [Google Scholar] [CrossRef]
- Bonovas, S.; Filioussi, K.; Tsavaris, N.; Sitaras, N.M. Use of Statins and Breast Cancer: A Meta-Analysis of Seven Randomized Clinical Trials and Nine Observational Studies. J. Clin. Oncol. 2005, 23, 8606–8612. [Google Scholar] [CrossRef]
- Tan, N.; Klein, E.A.; Li, J.; Moussa, A.S.; Jones, J.S. Statin Use and Risk of Prostate Cancer in a Population of Men Who Underwent Biopsy. J. Urol. 2011, 186, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Geybels, M.S.; Wright, J.L.; Holt, S.K.; Kolb, S.; Feng, Z.; Stanford, J.L. Statin Use in Relation to Prostate Cancer Outcomes in a Population-Based Patient Cohort Study. Prostate 2013, 73, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Agalliu, I.; Salinas, C.A.; Hansten, P.D.; Ostrander, E.A.; Stanford, J.L. Statin Use and Risk of Prostate Cancer: Results from a Population-Based Epidemiologic Study. Am. J. Epidemiol. 2008, 168, 250–260. [Google Scholar] [CrossRef]
- Tamburrino, D.; Crippa, S.; Partelli, S.; Archibugi, L.; Arcidiacono, P.G.; Falconi, M.; Capurso, G. Statin Use Improves Survival in Patients with Pancreatic Ductal Adenocarcinoma: A Meta-Analysis. Dig. Liver Dis. 2020, 52, 392–399. [Google Scholar] [CrossRef]
- Iarrobino, N.A.; Gill, B.; Bernard, M.E.; Mishra, M.V.; Champ, C.E. Targeting Tumor Metabolism with Statins during Treatment for Advanced-Stage Pancreatic Cancer. Am. J. Clin. Oncol. 2018, 41, 1125–1131. [Google Scholar] [CrossRef]
- Voorneveld, P.W.; Reimers, M.S.; Bastiaannet, E.; Jacobs, R.J.; van Eijk, R.; Zanders, M.M.J.; Herings, R.M.C.; van Herk-Sukel, M.P.P.; Kodach, L.L.; van Wezel, T.; et al. Statin Use after Diagnosis of Colon Cancer and Patient Survival. Gastroenterology 2017, 153, 470–479.e4. [Google Scholar] [CrossRef]
- Li, L.; Cui, N.; Hao, T.; Zou, J.; Jiao, W.; Yi, K.; Yu, W. Statins Use and the Prognosis of Colorectal Cancer: A Meta-Analysis. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101588. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.H.; Yoo, T.G.; Jeong, S.M.; Shin, D.W. Association of Aspirin, Metformin, and Statin Use with Gastric Cancer Incidence and Mortality: A Nationwide Cohort Study. Cancer Prev. Res. 2021, 14, 95–104. [Google Scholar] [CrossRef]
- Islam, M.M.; Poly, T.N.; Walther, B.A.; Yang, H.C.; Li, Y.C. Statin Use and the Risk of Hepatocellular Carcinoma: A Meta-Analysis of Observational Studies. Cancers 2020, 12, 671. [Google Scholar] [CrossRef]
- Majidi, A.; Na, R.; Jordan, S.J.; De Fazio, A.; Webb, P.M. Statin Use and Survival Following a Diagnosis of Ovarian Cancer: A Prospective Observational Study. Int. J. Cancer 2021, 148, 1608–1615. [Google Scholar] [CrossRef]
- Kim, D.S.; Ahn, H.S.; Kim, H.J. Statin Use and Incidence and Mortality of Breast and Gynecology Cancer: A Cohort Study Using the National Health Insurance Claims Database. Int. J. Cancer 2022, 150, 1156–1165. [Google Scholar] [CrossRef] [PubMed]
- Song, M.K.; Shin, B.S.; Ha, C.S.; Park, W.Y. Would Lipophilic Statin Therapy as a Prognostic Factor Improve Survival in Patients with Uterine Cervical Cancer? Int. J. Gynecol. Cancer 2017, 27, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Cardwell, C.R.; Hicks, B.M.; Hughes, C.; Murray, L.J. Statin Use after Diagnosis of Breast Cancer and Survival a Population-Based Cohort Study. Epidemiology 2015, 26, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.L.; Habel, L.A.; Flick, E.D.; Quesenberry, C.P.; Caan, B. Post-Diagnosis Statin Use and Breast Cancer Recurrence in a Prospective Cohort Study of Early Stage Breast Cancer Survivors. Breast Cancer Res. Treat. 2008, 109, 573–579. [Google Scholar] [CrossRef]
- Manthravadi, S.; Shrestha, A.; Madhusudhana, S. Impact of Statin Use on Cancer Recurrence and Mortality in Breast Cancer: A Systematic Review and Meta-Analysis. Int. J. Cancer 2016, 139, 1281–1288. [Google Scholar] [CrossRef]
- Allott, E.H.; Ebot, E.M.; Stopsack, K.H.; Gonzalez-Feliciano, A.G.; Markt, S.C.; Wilson, K.M.; Ahearn, T.U.; Gerke, T.A.; Downer, M.K.; Rider, J.R.; et al. Statin Use Is Associated with Lower Risk of PTEN-Null and Lethal Prostate Cancer. Clin. Cancer Res. 2020, 26, 1086–1093. [Google Scholar] [CrossRef]
- Coogan, P.F.; Kelly, J.P.; Strom, B.L.; Rosenberg, L. Statin and NSAID Use and Prostate Cancer Risk. Pharmacoepidemiol. Drug Saf. 2010, 19, 752–755. [Google Scholar] [CrossRef]
- Lytras, T.; Nikolopoulos, G.; Bonovas, S. Statins and the Risk of Colorectal Cancer: An Updated Systematic Review and Meta-Analysis of 40 Studies. World J. Gastroenterol. 2014, 20, 1858–1870. [Google Scholar] [CrossRef]
- Verdoodt, F.; Kjær Hansen, M.; Kjaer, S.K.; Pottegård, A.; Friis, S.; Dehlendorff, C. Statin Use and Mortality among Ovarian Cancer Patients: A Population-Based Cohort Study. Int. J. Cancer 2017, 141, 279–286. [Google Scholar] [CrossRef]
- Mohammadian-Hafshejani, A.; Sherwin, C.M.T.; Heidari-Soureshjani, S. Do Statins Play Any Role in Reducing the Incidence and Mortality of Ovarian Cancer? A Systematic Review and Meta-Analysis. J. Prev. Med. Hyg. 2020, 61, E331–E339. [Google Scholar] [CrossRef]
- Chen, Y.; Han, L.; Zheng, A. Association between Statin Use and the Risk, Prognosis of Gynecologic Cancer: A Meta-Analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 268, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Lebo, N.L.; Griffiths, R.; Hall, S.; Dimitroulakos, J.; Johnson-Obaseki, S. Effect of Statin Use on Oncologic Outcomes in Head and Neck Squamous Cell Carcinoma. Head Neck 2018, 40, 1697–1706. [Google Scholar] [CrossRef]
- Seliger, C.; Meier, C.R.; Becker, C.; Jick, S.S.; Bogdahn, U.; Hau, P.; Leitzmann, M.F. Statin Use and Risk of Glioma: Population-Based Case–Control Analysis. Eur. J. Epidemiol. 2016, 31, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Seliger, C.; Schaertl, J.; Gerken, M.; Luber, C.; Proescholdt, M.; Riemenschneider, M.J.; Leitzmann, M.F.; Hau, P.; Klinkhammer-Schalke, M. Use of Statins or NSAIDs and Survival of Patients with High-Grade Glioma. PLoS ONE 2018, 13, e0207858. [Google Scholar] [CrossRef] [PubMed]
- Ung, M.H.; MacKenzie, T.A.; Onega, T.L.; Amos, C.I.; Cheng, C. Statins Associate with Improved Mortality among Patients with Certain Histological Subtypes of Lung Cancer. Lung Cancer 2018, 126, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Casey, P.J.; Kumar, A.P.; Pervaiz, S. Deciphering the Signaling Networks Underlying Simvastatin-Induced Apoptosis in Human Cancer Cells: Evidence for Non-Canonical Activation of RhoA and Rac1 GTPases. Cell Death Dis. 2013, 4, e568. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, J.; Zeki, A.A.; Mirzaei, N.; Tewary, S.; Rezaei Moghadam, A.; Glogowska, A.; Nagakannan, P.; Eftekharpour, E.; Wiechec, E.; Gordon, J.W.; et al. Mevalonate Cascade Inhibition by Simvastatin Induces the Intrinsic Apoptosis Pathway via Depletion of Isoprenoids in Tumor Cells. Sci. Rep. 2017, 7, 44841. [Google Scholar] [CrossRef]
- Koyuturk, M.; Ersoz, M.; Altiok, N. Simvastatin Induces Apoptosis in Human Breast Cancer Cells: P53 and Estrogen Receptor Independent Pathway Requiring Signalling through JNK. Cancer Lett. 2007, 250, 220–228. [Google Scholar] [CrossRef]
- Göbel, A.; Zinna, V.M.; Dell’Endice, S.; Jaschke, N.; Kuhlmann, J.D.; Wimberger, P.; Rachner, T.D. Anti-Tumor Effects of Mevalonate Pathway Inhibition in Ovarian Cancer. BMC Cancer 2020, 20, 703. [Google Scholar] [CrossRef]
- Zhong, W.B.; Wang, C.Y.; Chang, T.C.; Lee, W. Sen Lovastatin Induces Apoptosis of Anaplastic Thyroid Cancer Cells via Inhibition of Protein Geranylgeranylation and de Novo Protein Synthesis. Endocrinology 2003, 144, 3852–3859. [Google Scholar] [CrossRef]
- Miller, T.; Yang, F.; Wise, C.E.; Meng, F.; Priester, S.; Munshi, M.K.; Guerrier, M.; Dostal, D.E.; Glaser, S.S. Simvastatin Stimulates Apoptosis in Cholangiocarcinoma by Inhibition of Rac1 Activity. Dig. Liver Dis. 2011, 43, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, D.; Tsubaki, M.; Takeda, T.; Tomonari, Y.; Koumoto, Y.I.; Sakaguchi, K.; Nishida, S. Statins Induce Apoptosis through Inhibition of Ras Signaling Pathways and Enhancement of Bim and P27 Expression in Human Hematopoietic Tumor Cells. Tumor Biol. 2017, 39, 1010428317734947. [Google Scholar] [CrossRef]
- Sarrabayrouse, G.; Synaeve, C.; Leveque, K.; Favre, G.; Tilkin-Mariamé, A.F. Statins Stimulate In Vitro Membrane FasL Expression and Lymphocyte Apoptosis through RhoA/ROCK Pathway in Murine Melanoma Cells. Neoplasia 2007, 9, 1078–1090. [Google Scholar] [CrossRef] [PubMed]
- Hoque, A.; Chen, H.; Xu, X.C. Statin Induces Apoptosis and Cell Growth Arrest in Prostate Cancer Cells. Cancer Epidemiol. Biomarkers Prev. 2008, 17, 88–94. [Google Scholar] [CrossRef]
- Sivaprasad, U.; Abbas, T.; Dutta, A. Differential Efficacy of 3-Hydroxy-3-Methylglutaryl CoA Reductase Inhibitors on the Cell Cycle of Prostate Cancer Cells. Mol. Cancer Ther. 2006, 5, 2310–2316. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.S.; Kang, X.L.; Zhou, J.G.; Lv, X.F.; Tang, Y.B.; Guan, Y.Y. Involvement of Chk1-Cdc25A-Cyclin A/CDk2 Pathway in Simvastatin Induced S-Phase Cell Cycle Arrest and Apoptosis in Multiple Myeloma Cells. Eur. J. Pharmacol. 2011, 670, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, A.; Asano, T.; Kuroda, K.; Sato, A.; Asakuma, J.; Ito, K.; Hayakawa, M.; Sumitomo, M.; Asano, T. STAT3 Inhibitor WP1066 as a Novel Therapeutic Agent for Renal Cell Carcinoma. Br. J. Cancer 2010, 102, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Georgakopoulos-Soares, I.; Chartoumpekis, D.V.; Kyriazopoulou, V.; Zaravinos, A. EMT Factors and Metabolic Pathways in Cancer. Front. Oncol. 2020, 10, 449. [Google Scholar] [CrossRef]
- Koohestanimobarhan, S.; Salami, S.; Imeni, V.; Mohammadi, Z.; Bayat, O. Lipophilic Statins Antagonistically Alter the Major Epithelial-to-Mesenchymal Transition Signaling Pathways in Breast Cancer Stem–like Cells via Inhibition of the Mevalonate Pathway. J. Cell. Biochem. 2019, 120, 2515–2531. [Google Scholar] [CrossRef]
- Collisson, E.A.; Kleer, C.; Wu, M.; De, A.; Gambhir, S.S.; Merajver, S.D.; Kolodne, M.S. Atorvastatin Prevents RhoC Isoprenylation, Invasion, and Metastasis in Human Melanoma Cells. Mol. Cancer Ther. 2003, 2, 941–948. [Google Scholar]
- Brown, M.; Hart, C.; Tawadros, T.; Ramani, V.; Sangar, V.; Lau, M.; Clarke, N. The Differential Effects of Statins on the Metastatic Behaviour of Prostate Cancer. Br. J. Cancer 2012, 106, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, A.; Sumitomo, M.; Asakuma, J.; Asano, T.; Asano, T.; Hayakawa, M. 3-Hydroxy-3-Methylglutaryl-Coenzyme A Reductase Inhibitor, Fluvastatin, as a Novel Agent for Prophylaxis of Renal Cancer Metastasis. Clin. Cancer Res. 2004, 10, 8648–8655. [Google Scholar] [CrossRef] [PubMed]
- Nübel, T.; Dippold, W.; Kaina, B.; Fritz, G. Ionizing Radiation-Induced E-Selectin Gene Expression and Tumor Cell Adhesion Is Inhibited by Lovastatin and All-Trans Retinoic Acid. Carcinogenesis 2004, 25, 1335–1344. [Google Scholar] [CrossRef]
- Sethunath, V.; Hu, H.; De Angelis, C.; Veeraraghavan, J.; Qin, L.; Wang, N.; Simon, L.M.; Wang, T.; Fu, X.; Nardone, A.; et al. Targeting the Mevalonate Pathway to Overcome Acquired Anti-HER2 Treatment Resistance in Breast Cancer. Mol. Cancer Res. 2019, 17, 2318–2330. [Google Scholar] [CrossRef] [PubMed]
- Roudier, E.; Mistafa, O.; Stenius, U. Statins Induce Mammalian Target of Rapamycin (MTOR)-Mediated Inhibition of Akt Signaling and Sensitize P53-Deficient Cells to Cytostatic Drugs. Mol. Cancer Ther. 2006, 5, 2706–2715. [Google Scholar] [CrossRef] [PubMed]
- Khanzada, U.K.; Pardo, O.E.; Meier, C.; Downward, J.; Seckl, M.J.; Arcaro, A. Potent Inhibition of Small-Cell Lung Cancer Cell Growth by Simvastatin Reveals Selective Functions of Ras Isoforms in Growth Factor Signalling. Oncogene 2006, 25, 877–887. [Google Scholar] [CrossRef]
- Martirosyan, A.; Clendening, J.W.; Goard, C.A.; Penn, L.Z. Lovastatin Induces Apoptosis of Ovarian Cancer Cells and Synergizes with Doxorubicin: Potential Therapeutic Relevance. BMC Cancer 2010, 10, 103. [Google Scholar] [CrossRef]
- Calabro, A.; Tai, J.; Allen, S.L.; Budman, D.R. In-Vitro Synergism of m-TOR Inhibitors, Statins, and Classical Chemotherapy: Potential Implications in Acute Leukemia. Anticancer Drugs 2008, 19, 705–712. [Google Scholar] [CrossRef]
- Shojaei, S.; Koleini, N.; Samiei, E.; Aghaei, M.; Cole, L.K.; Alizadeh, J.; Islam, M.I.; Vosoughi, A.R.; Albokashy, M.; Butterfield, Y.; et al. Simvastatin Increases Temozolomide-Induced Cell Death by Targeting the Fusion of Autophagosomes and Lysosomes. FEBS J. 2020, 287, 1005–1034. [Google Scholar] [CrossRef]
- Cemeus, C.; Zhao, T.T.; Barrett, G.M.; Lorimer, I.A.; Dimitroulakos, J. Lovastatin Enhances Gefitinib Activity in Glioblastoma Cells Irrespective of EGFRvIII and PTEN Status. J. Neurooncol. 2008, 90, 9–17. [Google Scholar] [CrossRef]
- Sanli, T.; Liu, C.; Rashid, A.; Hopmans, S.N.; Tsiani, E.; Schultz, C.; Farrell, T.; Singh, G.; Wright, J.; Tsakiridis, T. Lovastatin Sensitizes Lung Cancer Cells to Ionizing Radiation: Modulation of Molecular Pathways of Radioresistance and Tumor Suppression. J. Thorac. Oncol. 2011, 6, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Ghosh-Choudhury, N.; Mandal, C.C.; Ghosh-Choudhury, N.; Ghosh Choudhury, G. Simvastatin Induces Derepression of PTEN Expression via NFκB to Inhibit Breast Cancer Cell Growth. Cell. Signal. 2010, 22, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Kochuparambil, S.T.; Al-Husein, B.; Goc, A.; Soliman, S.; Somanath, P.R. Anticancer Efficacy of Simvastatin on Prostate Cancer Cells and Tumor Xenografts Is Associated with Inhibition of Akt and Reduced Prostate-Specific Antigen Expression. J. Pharmacol. Exp. Ther. 2011, 336, 496–505. [Google Scholar] [CrossRef]
- Jiang, P.; Mukthavaram, R.; Chao, Y.; Nomura, N.; Bharati, I.S.; Fogal, V.; Pastorino, S.; Teng, D.; Cong, X.; Pingle, S.C.; et al. In Vitro and in Vivo Anticancer Effects of Mevalonate Pathway Modulation on Human Cancer Cells. Br. J. Cancer 2014, 111, 1562–1571. [Google Scholar] [CrossRef]
- Liu, H.; Wang, Z.; Li, Y.; Li, W.; Chen, Y. Simvastatin Prevents Proliferation and Bone Metastases of Lung Adenocarcinoma In Vitro and In Vivo. Neoplasma 2013, 60, 240–245. [Google Scholar] [CrossRef]
- Peng, P.; Wei, W.; Long, C.; Li, J. Atorvastatin Augments Temozolomide’s Efficacy in Glioblastoma via Prenylation-Dependent Inhibition of Ras Signaling. Biochem. Biophys. Res. Commun. 2017, 489, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Cui, X.X.; Gao, Z.; Zhao, Y.; Lin, Y.; Shih, W.J.; Huang, M.T.; Liu, Y.; Rabson, A.; Reddy, B.; et al. Atorvastatin and Celecoxib in Combination Inhibits the Progression of Androgen-Dependent LNCaP Xenograft Prostate Tumors to Androgen Independence. Cancer Prev. Res. 2010, 3, 114–124. [Google Scholar] [CrossRef]
- Bocci, G.; Fioravanti, A.; Orlandi, P.; Bernardini, N.; Collecchi, P.; Del Tacca, M.; Danesi, R. Fluvastatin Synergistically Enhances the Antiproliferative Effect of Gemcitabine in Human Pancreatic Cancer MIAPaCa-2 Cells. Br. J. Cancer 2005, 93, 319–330. [Google Scholar] [CrossRef]
- Lee, J.; Lee, I.; Han, B.; Park, J.O.; Jang, J.; Park, C.; Kang, W.K. Effect of Simvastatin on Cetuximab Resistance in Human Colorectal Cancer with KRAS Mutations. J. Natl. Cancer Inst. 2011, 103, 674–688. [Google Scholar] [CrossRef]
- Alarcon Martinez, T.; Zeybek, N.D.; Müftüoğlu, S. Evaluation of the Cytotoxic and Autophagic Effects of Atorvastatin on Mcf-7 Breast Cancer Cells. Balk. Med. J. 2018, 35, 256–262. [Google Scholar] [CrossRef]
- Wang, T.; Seah, S.; Loh, X.; Chan, C.W.; Hartman, M.; Goh, B.C.; Lee, S.C. Simvastatin-Induced Breast Cancer Cell Death and Deactivation of PI3K/Akt and MAPK/ERK Signalling Are Reversed by Metabolic Products of the Mevalonate Pathway. Oncotarget 2016, 7, 2532–2544. [Google Scholar] [CrossRef] [PubMed]
- Buranrat, B.; Suwannaloet, W.; Naowaboot, J. Simvastatin Potentiates Doxorubicin Activity against MCF-7 Breast Cancer Cells. Oncol. Lett. 2017, 14, 6243–6250. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Chyuan, I.T.; Shiue, C.; Yu, M.C.; Hsu, Y.F.; Hsu, M.J. Lovastatin-Mediated MCF-7 Cancer Cell Death Involves LKB1-AMPK-P38MAPK-P53-Survivin Signalling Cascade. J. Cell. Mol. Med. 2020, 24, 1822–1836. [Google Scholar] [CrossRef]
- Lin, Z.; Zhang, Z.; Jiang, X.; Kou, X.; Bao, Y.; Liu, H.; Sun, F.; Ling, S.; Qin, N.; Jiang, L.; et al. Mevastatin Blockade of Autolysosome Maturation Stimulates LBH589-Induced Cell Death in Triple-Negative Breast Cancer Cells. Oncotarget 2017, 8, 17833–17848. [Google Scholar] [CrossRef] [PubMed]
- Bytautaite, M.; Petrikaite, V. Comparative Study of Lipophilic Statin Activity in 2d and 3d In Vitro Models of Human Breast Cancer Cell Lines Mda-Mb-231 and Mcf-7. OncoTargets Ther. 2020, 13, 13201–13209. [Google Scholar] [CrossRef]
- Beckwitt, C.H.; Clark, A.M.; Ma, B.; Whaley, D.; Oltvai, Z.N.; Wells, A. Statins Attenuate Outgrowth of Breast Cancer Metastases. Br. J. Cancer 2018, 119, 1094–1105. [Google Scholar] [CrossRef]
- Toepfer, N.; Childress, C.; Parikh, A.; Rukstalis, D.; Yang, W. Atorvastatin Induces Autophagy in Prostate Cancer PC3 Cells through Activation of LC3 Transcription. Cancer Biol. Ther. 2011, 12, 691–699. [Google Scholar] [CrossRef]
- Deng, J.L.; Zhang, R.; Zeng, Y.; Zhu, Y.S.; Wang, G. Statins Induce Cell Apoptosis through a Modulation of AKT/FOXO1 Pathway in Prostate Cancer Cells. Cancer Manag. Res. 2019, 11, 7231–7242. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Kashima, H.; Wu, R.C.; Jung, J.G.; Kuan, J.C.; Gu, J.; Xuan, J.; Sokoll, L.; Visvanathan, K.; Shih, I.M.; et al. Mevalonate Pathway Antagonist Suppresses Formation of Serous Tubal Intraepithelial Carcinoma and Ovarian Carcinoma in Mouse Models. Clin. Cancer Res. 2015, 21, 4652–4662. [Google Scholar] [CrossRef]
- Robinson, E.; Nandi, M.; Wilkinson, L.L.; Arrowsmith, D.M.; Curtis, A.D.M.; Richardson, A. Preclinical Evaluation of Statins as a Treatment for Ovarian Cancer. Gynecol. Oncol. 2013, 129, 417–424. [Google Scholar] [CrossRef]
- Jones, H.M.; Fang, Z.; Sun, W.; Clark, L.H.; Stine, J.E.; Tran, A.Q.; Sullivan, S.A.; Gilliam, T.P.; Zhou, C.; Bae-Jump, V.L. Atorvastatin Exhibits Anti-Tumorigenic and Anti-Metastatic Effects in Ovarian Cancer In Vitro. Am. J. Cancer Res. 2017, 7, 2478–2490. [Google Scholar]
- Crescencio, M.E.; Rodríguez, E.; Páez, A.; Masso, F.A.; Montaño, L.F.; López-Marure, R. Statins Inhibit the Proliferation and Induce Cell Death of Human Papilloma Virus Positive and Negative Cervical Cancer Cells. Int. J. Biomed. Sci. 2009, 5, 411–420. [Google Scholar]
- Ortiz, N.; Díaz, C. Mevalonate Pathway as a Novel Target for the Treatment of Metastatic Gastric Cancer. Oncol. Lett. 2020, 20, 320. [Google Scholar] [CrossRef]
- Jang, H.J.; Hong, E.M.; Park, S.W.; Byun, H.W.; Koh, D.H.; Choi, M.H.; Kae, S.H.; Lee, J. Statin Induces Apoptosis of Human Colon Cancer Cells and Downregulation of Insulin-like Growth Factor 1 Receptor via Proapoptotic ERK Activation. Oncol. Lett. 2016, 12, 250–256. [Google Scholar] [CrossRef]
- Wu, X.; Song, M.; Qiu, P.; Rakariyatham, K.; Li, F.; Gao, Z.; Cai, X.; Wang, M.; Xu, F.; Zheng, J.; et al. Synergistic Chemopreventive Effects of Nobiletin and Atorvastatin on Colon Carcinogenesis. Carcinogenesis 2017, 38, 455–464. [Google Scholar] [CrossRef]
- Docrat, T.F.; Nagiah, S.; Krishnan, A.; Naidoo, D.B.; Chuturgoon, A.A. Atorvastatin Induces MicroRNA-145 Expression in HEPG2 Cells via Regulation of the PI3K/AKT Signalling Pathway. Chem. Biol. Interact. 2018, 287, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Sutter, A.P.; Maaser, K.; Höpfner, M.; Huether, A.; Schuppan, D.; Scherübl, H. Cell Cycle Arrest and Apoptosis Induction in Hepatocellular Carcinoma Cells by HMG-CoA Reductase Inhibitors. Synergistic Antiproliferative Action with Ligands of the Peripheral Benzodiazepine Receptor. J. Hepatol. 2005, 43, 808–816. [Google Scholar] [CrossRef] [PubMed]
- You, H.Y.; Zhang, W.J.; Xie, X.M.; Zheng, Z.H.; Zhu, H.L.; Jiang, F.Z. Pitavastatin Suppressed Liver Cancer Cells In Vitro and In Vivo. OncoTargets Ther. 2016, 9, 5383–5388. [Google Scholar] [CrossRef]
- Otahal, A.; Aydemir, D.; Tomasich, E.; Minichsdorfer, C. Delineation of Cell Death Mechanisms Induced by Synergistic Effects of Statins and Erlotinib in Non-Small Cell Lung Cancer Cell (NSCLC) Lines. Sci. Rep. 2020, 10, 959. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, V.N.; Hei, T.K. Regulation of Apoptosis in Human Melanoma and Neuroblastoma Cells by Statins, Sodium Arsenite and TRAIL: A Role of Combined Treatment versus Monotherapy. Apoptosis 2011, 16, 1268–1284. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, T.; Scherzad, A.; Hackenberg, S.; Ickrath, P.; Schendzielorz, P.; Hagen, R.; Kleinsasser, N. Additive Antitumor Effects of Celecoxib and Simvastatin on Head and Neck Squamous Cell Carcinoma In Vitro. Int. J. Oncol. 2017, 51, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Mehibel, M.; Ortiz-Martinez, F.; Voelxen, N.; Boyers, A.; Chadwick, A.; Telfer, B.A.; Mueller-Klieser, W.; West, C.M.; Critchlow, S.E.; Williams, K.J.; et al. Statin-Induced Metabolic Reprogramming in Head and Neck Cancer: A Biomarker for Targeting Monocarboxylate Transporters. Mol. Biotechnol. 2018, 8, 16804. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Tilija Pun, N.; Jang, W.J.; Bae, J.W.; Jeong, C.H. Pitavastatin Induces Apoptosis in Oral Squamous Cell Carcinoma through Activation of FOXO3a. J. Cell. Mol. Med. 2020, 24, 7055–7066. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.; Sharma, S.; Kumar, B.; Teknos, T.N. Atorvastatin Inhibits RhoC Function and Limits Head and Neck Cancer Metastasis. Oral Oncol. 2013, 49, 778–786. [Google Scholar] [CrossRef]
- Higgins, M.J.; Prowell, T.M.; Blackford, A.L.; Byrne, C.; Khouri, N.F.; Slater, S.A.; Jeter, S.C.; Armstrong, D.K.; Davidson, N.E.; Emens, L.A.; et al. A Short-Term Biomarker Modulation Study of Simvastatin in Women at Increased Risk of a New Breast Cancer. Breast Cancer Res. Treat. 2012, 131, 915–924. [Google Scholar] [CrossRef]
- Vinayak, S.; Schwartz, E.J.; Jensen, K.; Lipson, J.; Alli, E.; McPherson, L.; Fernandez, A.M.; Sharma, V.B.; Staton, A.; Mills, M.A.; et al. A Clinical Trial of Lovastatin for Modification of Biomarkers Associated with Breast Cancer Risk. Breast Cancer Res. Treat. 2013, 142, 389–398. [Google Scholar] [CrossRef]
- Garwood, E.R.; Kumar, A.S.; Baehner, F.L.; Moore, D.H.; Au, A.; Hylton, N.; Flowers, C.I.; Garber, J.; Lesnikoski, B.A.; Hwang, E.S.; et al. Fluvastatin Reduces Proliferation and Increases Apoptosis in Women with High Grade Breast Cancer. Breast Cancer Res. Treat. 2010, 119, 137–144. [Google Scholar] [CrossRef]
- Longo, J.; Hamilton, R.J.; Masoomian, M.; Khurram, N.; Branchard, E.; Mullen, P.J.; Elbaz, M.; Hersey, K.; Chadwick, D.; Ghai, S.; et al. A Pilot Window-of-Opportunity Study of Preoperative Fluvastatin in Localized Prostate Cancer. Prostate Cancer Prostatic Dis. 2020, 23, 630–637. [Google Scholar] [CrossRef]
- Han, J.Y.; Lee, S.H.; Yoo, N.J.; Lee, S.H.; Moon, Y.J.; Yun, T.; Kim, H.T.; Lee, J.S. A Randomized Phase II Study of Gefitinib plus Simvastatin versus Gefitinib Alone in Previously Treated Patients with Advanced Non-Small Cell Lung Cancer. Clin. Cancer Res. 2011, 17, 1553–1560. [Google Scholar] [CrossRef]
- Hus, M.; Grzasko, N.; Szostek, M.; Pluta, A.; Helbig, G.; Woszczyk, D.; Adamczyk-Cioch, M.; Jawniak, D.; Legiec, W.; Morawska, M.; et al. Thalidomide, Dexamethasone and Lovastatin with Autologous Stem Cell Transplantation as a Salvage Immunomodulatory Therapy in Patients with Relapsed and Refractory Multiple Myeloma. Ann. Hematol. 2011, 90, 1161–1166. [Google Scholar] [CrossRef]
- Goss, G.D.; Jonker, D.J.; Laurie, S.A.; Weberpals, J.I.; Oza, A.M.; Spaans, J.N.; la Porte, C.; Dimitroulakos, J. A Phase I Study of High-Dose Rosuvastatin with Standard Dose Erlotinib in Patients with Advanced Solid Malignancies. J. Transl. Med. 2016, 14, 83. [Google Scholar] [CrossRef]
- Baas, J.M.; Krens, L.L.; Ten Tije, A.J.; Erdkamp, F.; Van Wezel, T.; Morreau, H.; Gelderblom, H.; Guchelaar, H.J. Safety and Efficacy of the Addition of Simvastatin to Cetuximab in Previously Treated KRAS Mutant Metastatic Colorectal Cancer Patients. Investig. New Drugs 2015, 33, 1242–1247. [Google Scholar] [CrossRef] [PubMed]
- Yulian, E.D.; Siregar, N.C. Bajuadji Combination of Simvastatin and FAC Improves Response to Neoadjuvant Chemotherapy in Locally Advanced Breast Cancer. Cancer Res. Treat. 2021, 53, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Feldt, M.; Bjarnadottir, O.; Kimbung, S.; Jirström, K.; Bendahl, P.O.; Veerla, S.; Grabau, D.; Hedenfalk, I.; Borgquist, S. Statin-Induced Anti-Proliferative Effects via Cyclin D1 and P27 in a Window-of-Opportunity Breast Cancer Trial. J. Transl. Med. 2015, 13, 133. [Google Scholar] [CrossRef]
- Kawata, S.; Yamasaki, E.; Nagase, T.; Inui, Y.; Ito, N.; Matsuda, Y.; Inada, M.; Tamura, S.; Noda, S.; Imai, Y.; et al. Effect of Pravastatin on Survival in Patients with Advanced Hepatocellular Carcinoma. A Randomized Controlled Trial. Br. J. Cancer 2001, 84, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Jouve, J.L.; Lecomte, T.; Bouché, O.; Barbier, E.; Khemissa Akouz, F.; Riachi, G.; Nguyen Khac, E.; Ollivier-Hourmand, I.; Debette-Gratien, M.; Faroux, R.; et al. Pravastatin Combination with Sorafenib Does Not Improve Survival in Advanced Hepatocellular Carcinoma. J. Hepatol. 2019, 71, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Kang, J.H.; Lee, J.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Hwang, I.G.; Lee, S.C.; Park, K.W.; et al. Simvastatin plus Capecitabine-Cisplatin versus Placebo plus Capecitabine-Cisplatin in Patients with Previously Untreated Advanced Gastric Cancer: A Double-Blind Randomised Phase 3 Study. Eur. J. Cancer 2014, 50, 2822–2830. [Google Scholar] [CrossRef] [PubMed]
- Konings, I.R.H.M.; Van Der Gaast, A.; Van Der Wijk, L.J.; De Jongh, F.E.; Eskens, F.A.L.M.; Sleijfer, S. The Addition of Pravastatin to Chemotherapy in Advanced Gastric Carcinoma: A Randomised Phase II Trial. Eur. J. Cancer 2010, 46, 3200–3204. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Kim, T.W.; Hong, Y.S.; Han, S.W.; Lee, K.H.; Kang, H.J.; Hwang, I.G.; Lee, J.Y.; Kim, H.S.; Kim, S.T.; et al. A Randomised, Double-Blind, Placebo-Controlled Multi-Centre Phase III Trial of XELIRI/FOLFIRI plus Simvastatin for Patients with Metastatic Colorectal Cancer. Br. J. Cancer 2015, 113, 1421–1426. [Google Scholar] [CrossRef]
- Kartal-Yandim, M.; Adan-Gokbulut, A.; Baran, Y. Molecular Mechanisms of Drug Resistance and Its Reversal in Cancer. Crit. Rev. Biotechnol. 2016, 36, 716–726. [Google Scholar] [CrossRef]
- Zheng, H.C. The Molecular Mechanisms of Chemoresistance in Cancers. Oncotarget 2017, 8, 59950–59964. [Google Scholar] [CrossRef]
- Catalano, A.; Iacopetta, D.; Ceramella, J.; Scumaci, D.; Giuzio, F.; Saturnino, C.; Aquaro, S.; Rosano, C.; Sinicropi, M.S. Multidrug Resistance (MDR): A Widespread Phenomenon in Pharmacological Therapies. Molecules 2022, 27, 616. [Google Scholar] [CrossRef]
- Kathawala, R.J.; Gupta, P.; Ashby, C.R.; Chen, Z.S. The Modulation of ABC Transporter-Mediated Multidrug Resistance in Cancer: A Review of the Past Decade. Drug Resist. Updat. 2015, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-P.; Calcagno, A.; Ambudkar, S. Reversal of ABC Drug Transporter-Mediated Multidrug Resistance in Cancer Cells: Evaluation of Current Strategies. Curr. Mol. Pharmacol. 2012, 1, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Ozben, T. Mechanisms and Strategies to Overcome Multiple Drug Resistance in Cancer. FEBS Lett. 2006, 580, 2903–2909. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.I.; Haber, M.; Henderson, M.J.; Norris, M.D. ABC Transporters in Cancer: More than Just Drug Efflux Pumps. Nat. Rev. Cancer 2010, 10, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Vasiliou, V.; Vasiliou, K.; Nebert, D.W. Human ATP-Binding Cassette (ABC) Transporter Family. Hum. Genom. 2009, 3, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Gillet, J.P.; Efferth, T.; Remacle, J. Chemotherapy-Induced Resistance by ATP-Binding Cassette Transporter Genes. Biochim. Biophys. Acta 2007, 1775, 237–262. [Google Scholar] [CrossRef]
- Dong, J.; Qin, Z.; Zhang, W.D.; Cheng, G.; Yehuda, A.G.; Ashby, C.R.; Chen, Z.S.; Cheng, X.D.; Qin, J.J. Medicinal Chemistry Strategies to Discover P-Glycoprotein Inhibitors: An Update. Drug Resist. Updat. 2020, 49, 100681. [Google Scholar] [CrossRef]
- Gottesman, M.M.; Fojo, T.; Bates, S.E. Multidrug Resistance in Cancer: Role of ATP-Dependent Transporters. Nat. Rev. Cancer 2002, 2, 48–58. [Google Scholar] [CrossRef]
- Carocci, A.; Catalano, A.; Turi, F.; Lovece, A.; Cavalluzzi, M.M.; Bruno, C.; Colabufo, N.A.; Contino, M.; Perrone, M.G.; Franchini, C.; et al. Stereoselective Modulation of P-Glycoprotein by Chiral Small Molecules. ChemMedChem 2016, 11, 93–101. [Google Scholar] [CrossRef]
- Penson, R.T.; Oliva, E.; Skates, S.J.; Glyptis, T.; Fuller, A.F.; Goodman, A.; Seiden, M.V. Expression of Multidrug Resistance-1 Protein Inversely Correlates with Paclitaxel Response and Survival in Ovarian Cancer Patients: A Study in Serial Samples. Gynecol. Oncol. 2004, 93, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Aires, V.; Colin, D.J.; Doreau, A.; Pietro, A.D.; Heydel, J.M.; Artur, Y.; Latruffe, N.; Delmas, D. P-Glycoprotein 1 Affects Chemoactivities of Resveratrol against Human Colorectal Cancer Cells. Nutrients 2019, 11, 2098. [Google Scholar] [CrossRef] [PubMed]
- Hsia, T.C.; Lin, C.C.; Wang, J.J.; Ho, S.T.; Kao, A. Relationship between Chemotherapy Response of Small Cell Lung Cancer and P-Glycoprotein or Multidrug Resistance-Related Protein Expression. Lung 2002, 180, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Chen, Z.S.; Ambudkar, S.V. Tyrosine Kinase Inhibitors as Modulators of ABC Transporter-Mediated Drug Resistance. Drug Resist. Updat. 2012, 15, 70–80. [Google Scholar] [CrossRef]
- Deeley, R.G.; Westlake, C.; Cole, S.P.C. Transmembrane Transport of Endo- and Xenobiotics by Mammalian ATP-Binding Cassette Multidrug Resistance Proteins. Physiol. Rev. 2006, 86, 849–899. [Google Scholar] [CrossRef]
- Kachalaki, S.; Ebrahimi, M.; Mohamed Khosroshahi, L.; Mohammadinejad, S.; Baradaran, B. Cancer Chemoresistance; Biochemical and Molecular Aspects: A Brief Overview. Eur. J. Pharm. Sci. 2016, 89, 20–30. [Google Scholar] [CrossRef]
- Abbott, B.L. ABCG2 (BCRP) Expression in Normal and Malignant Hematopoietic Cells. Hematol. Oncol. 2003, 21, 115–130. [Google Scholar] [CrossRef]
- Jackson, S.M.; Manolaridis, I.; Kowal, J.; Zechner, M.; Taylor, N.M.I.; Bause, M.; Bauer, S.; Bartholomaeus, R.; Bernhardt, G.; Koenig, B.; et al. Structural Basis of Small-Molecule Inhibition of Human Multidrug Transporter ABCG2. Nat. Struct. Mol. Biol. 2018, 25, 333–340. [Google Scholar] [CrossRef]
- Telbisz, Á.; Müller, M.; Özvegy-Laczka, C.; Homolya, L.; Szente, L.; Váradi, A.; Sarkadi, B. Membrane Cholesterol Selectively Modulates the Activity of the Human ABCG2 Multidrug Transporter. Biochim. Biophys. Acta 2007, 1768, 2698–2713. [Google Scholar] [CrossRef]
- Eckford, P.D.W.; Sharom, F.J. Interaction of the P-Glycoprotein Multidrug Efflux Pump with Cholesterol: Effects on ATPase Activity, Drug Binding and Transport. Biochemistry 2008, 47, 13686–13698. [Google Scholar] [CrossRef] [PubMed]
- Glodkowska-Mrowka, E.; Mrowka, P.; Basak, G.W.; Niesiobedzka-Krezel, J.; Seferynska, I.; Wlodarski, P.K.; Jakobisiak, M.; Stoklosa, T. Statins Inhibit ABCB1 and ABCG2 Drug Transporter Activity in Chronic Myeloid Leukemia Cells and Potentiate Antileukemic Effects of Imatinib. Exp. Hematol. 2014, 42, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Carolyn, A.G.; Mather, R.G.; Vinepal, B.; Clendening, J.W.; Martirosyan, A.; Boutros, P.C.; Sharom, F.J.; Penn, L.Z. Differential Interactions between Statins and P-glycoprotein Implications for Exploiting Statins as Anticancer Agents. Int. J. Cancer 2010, 127, 2936–2948. [Google Scholar] [CrossRef]
- Duncan, R.E.; El-Sohemy, A.; Archer, M.C. Regulation of HMG-CoA Reductase in MCF-7 Cells by Genistein, EPA, and DHA, Alone and in Combination with Mevastatin. Cancer Lett. 2005, 224, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Staedler, D.; Chapuis-Bernasconi, C.; Dehmlow, H.; Fischer, H.; Juillerat-Jeanneret, L.; Aebi, J.D. Cytotoxic Effects of Combination of Oxidosqualene Cyclase Inhibitors with Atorvastatin in Human Cancer Cells. J. Med. Chem. 2012, 55, 4990–5002. [Google Scholar] [CrossRef]
- Mallappa, S.; Neeli, P.K.; Karnewar, S.; Kotamraju, S. Doxorubicin Induces Prostate Cancer Drug Resistance by Upregulation of ABCG4 through GSH Depletion and CREB Activation: Relevance of Statins in Chemosensitization. Mol. Carcinog. 2019, 58, 1118–1133. [Google Scholar] [CrossRef]
- Riganti, C.; Orecchia, S.; Pescarmona, G.; Betta, P.G.; Ghigo, D.; Bosia, A. Statins Revert Doxorubicin Resistance via Nitric Oxide in Malignant Mesothelioma. Int. J. Cancer 2006, 119, 17–27. [Google Scholar] [CrossRef]
- Palko-Łabuz, A.; Środa-Pomianek, K.; Wesołowska, O.; Kostrzewa-Susłow, E.; Uryga, A.; Michalak, K. MDR Reversal and Pro-Apoptotic Effects of Statins and Statins Combined with Flavonoids in Colon Cancer Cells. Biomed. Pharmacother. 2019, 109, 1511–1522. [Google Scholar] [CrossRef]
- Środa-Pomianek, K.; Michalak, K.; Palko-Łabuz, A.; Uryga, A.; Świątek, P.; Majkowski, M.; Wesołowska, O. The Combined Use of Phenothiazines and Statins Strongly Affects Doxorubicin-Resistance, Apoptosis, and Cox-2 Activity in Colon Cancer Cells. Int. J. Mol. Sci. 2019, 20, 955. [Google Scholar] [CrossRef]
- Rigoni, M.; Riganti, C.; Vitale, C.; Griggio, V.; Campia, I.; Robino, M.; Foglietta, M.; Castella, B.; Sciancalepore, P.; Buondonno, I.; et al. Simvastatin and Downstream Inhibitors Circumvent Constitutive and Stromal Cell-Induced Resistance to Doxorubicin in IGHV Unmutated CLL Cells. Oncotarget 2015, 6, 29833–29846. [Google Scholar] [CrossRef]
- Sieczkowski, E.; Lehner, C.; Ambros, P.F.; Hohenegger, M. Double Impact on P-glycoprotein by Statins Enhances Doxorubicin Cytotoxicity in Human Neuroblastoma Cells. Int. J. Cancer 2010, 126, 2025–2035. [Google Scholar] [CrossRef] [PubMed]
- Toppo, A.L.; Yadav, M.; Dhagat, S.; Ayothiraman, S.; Satya Eswari, J. Molecular Docking and ADMET Analysis of Synthetic Statins for HMG-CoA Reductase Inhibition Activity. Indian J. Biochem. Biophys. 2021, 58, 127–134. [Google Scholar]
- Suganya, S.; Nandagopal, B.; Anbarasu, A. Natural Inhibitors of HMG-CoA Reductase—An In Silico Approach Through Molecular Docking and Simulation Studies. J. Cell. Biochem. 2017, 118, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Marahatha, R.; Basnet, S.; Bhattarai, B.R.; Budhathoki, P.; Aryal, B.; Adhikari, B.; Lamichhane, G.; Poudel, D.K.; Parajuli, N. Potential Natural Inhibitors of Xanthine Oxidase and HMG-CoA Reductase in Cholesterol Regulation: In Silico Analysis. BMC Complement. Med. Ther. 2021, 21, 1. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Sharma, R.; Kumar, A. Comparative Potential of Simvastatin, Rosuvastatin and Fluvastatin against Bacterial Infection: An In Silico and In Vitro Study. Orient. Pharm. Exp. Med. 2019, 19, 259–275. [Google Scholar] [CrossRef]
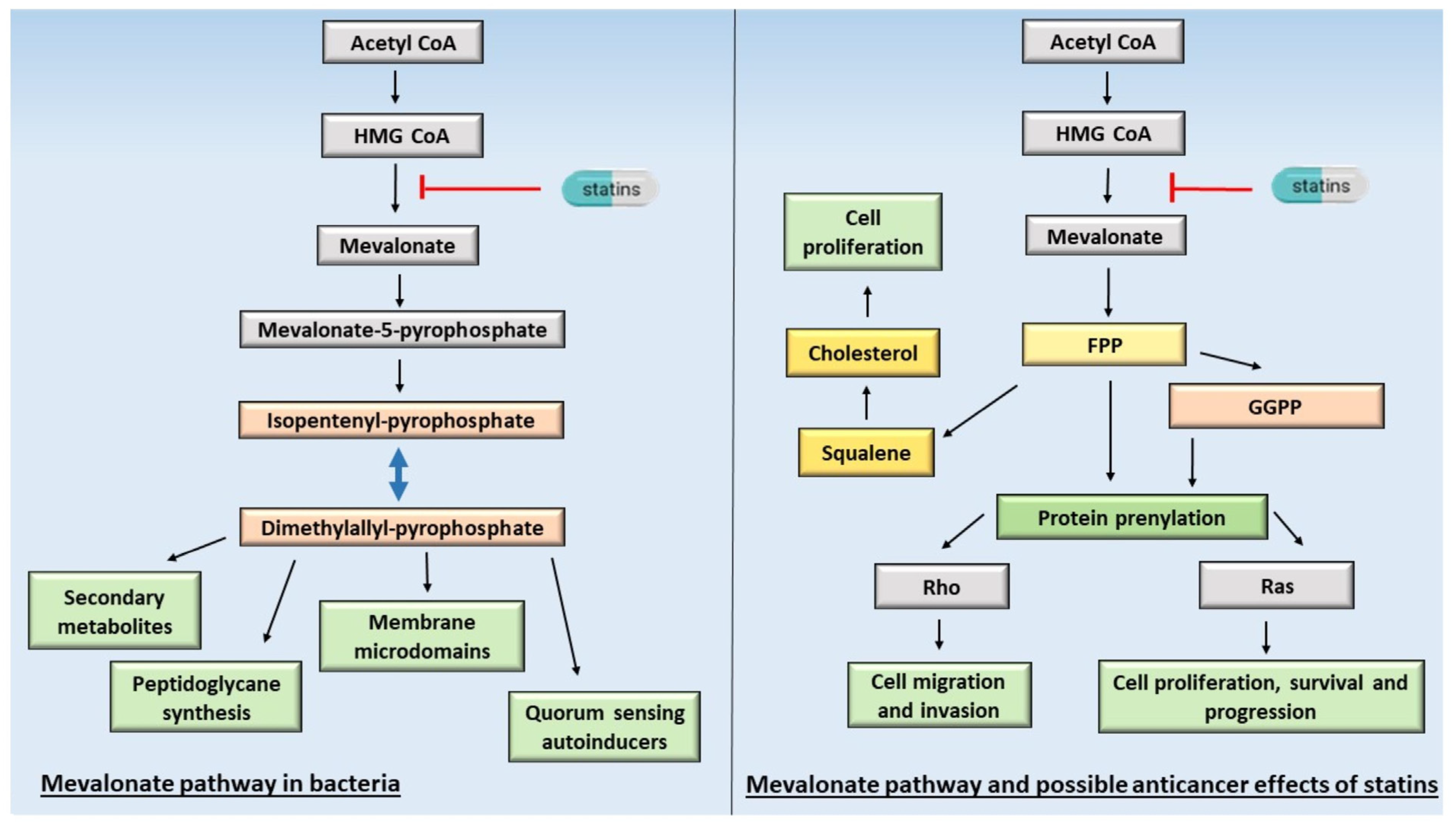
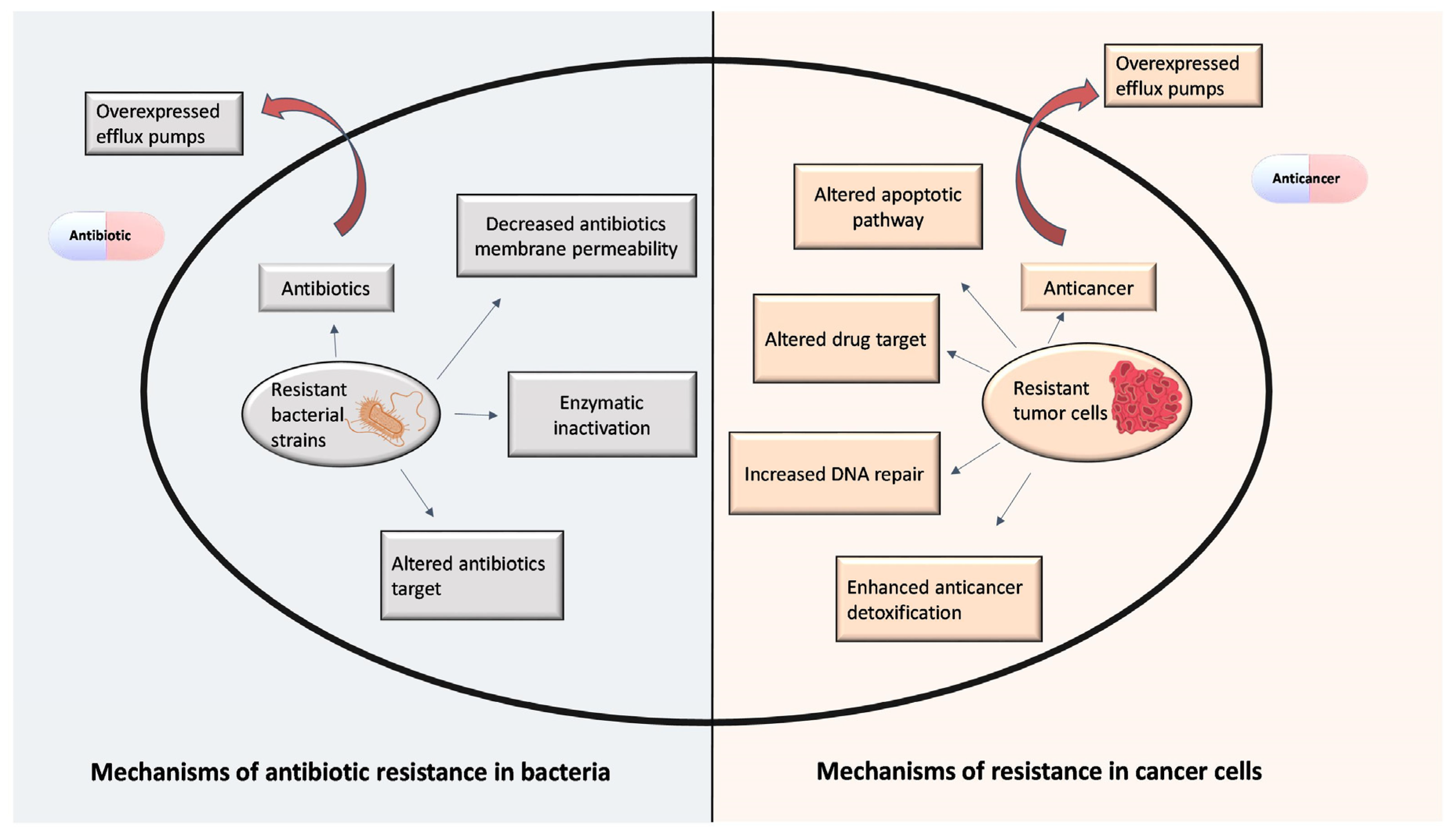

| Statins | Cancer Type | Study Type | No. of Patients | Combination Agent | Findings | Ref. |
|---|---|---|---|---|---|---|
| NR | Breast | Cohort study | 17,880 | - | The use of statins after diagnosis of breast cancer reduced breast cancer mortality and all-cause mortality. | [165] |
| Lipophilic statins | Cohort study | 1811 | - | The use of lipophilic statins after breast cancer diagnosis was related to a reduced risk of breast cancer recurrence. | [166] | |
| Atorvastatin, rosuvastatin, simvastatin, lovastatin, pitavastatin, pravastatin, and fluvastatin | Meta-analysis | 75,684 | - | Lipophilic statin use was associated with improved DFS for patients with breast cancer. In addition, there was an improvement in cancer-specific survival and overall survival. | [167] | |
| Atorvastatin, simvastatin, lovastatin, pravastatin and rosuvastatin | Prostate | Cohort study | 44,126 | - | Statins are associated with a lower risk of PTEN-null and lethal prostate cancer. | [168] |
| NR | Case–control study | 1367 | NSAIDs | The use of statins alone or in combination with NSAIDs had no protective effects on the risk of advanced prostate cancer. | [169] | |
| NR | Colorectal | Meta-analysis | ~8.2 million | - | The study confirmed a modest significant protective effect of statin use at therapeutic doses on CRC. | [170] |
| NR | Ovarian | Cohort study | 4419 | - | Ovarian cancer patients’ statin use after diagnosis was not associated with the reduction in mortality. | [171] |
| NR | Meta-analysis | 1,254,501 | Statin use was not significantly associated with risks but reduced mortality in ovarian cancer patients. | [172] | ||
| Atorvastatin, lovastatin, simvastatin, pravastatin, rosuvastatin and fluvastatin | Cohort study | 958 | - | In ovarian cancer, lipophilic statins slightly improve patients’ survival with no effect with hydrophilic statins. | [162] | |
| Atorvastatin, rosuvastatin, simvastatin, lovastatin, pitavastatin, pravastatin, and fluvastatin | Endometrial cancer | Meta-analysis | ~1,700,000 | - | Statin use decreases mortality of endometrial cancer risks. | [173] |
| NR | Head and neck | Cohort study | 1194 | - | Statin use at the time of the diagnosis improved overall and disease-free survival of HPV-negative SCC of the larynx, hypopharynx, and nasopharynx. | [174] |
| Atorvastatin, rosuvastatin, simvastatin, pravastatin, and fluvastatin | Glioblastoma | Case–control study | 27,159 | - | Statin use was not associated with the risk of GBM. | [175] |
| Simvastatin, atorvastatin, cerivastatin, fluvastatin, lovastatin, and pravastatin | Cohort study | 1093 | - | The use of statins was not associated with improved OS or PFS in GBM patients. | [176] | |
| Atorvastatin, simvastatin, lovastatin, pravastatin, and rosuvastatin | Lung | Cohort study | 19,974 | - | Statin use in patients with SCC and adenocarcinoma lung cancer was associated with a decreased mortality risk. | [177] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schelz, Z.; Muddather, H.F.; Zupkó, I. Repositioning of HMG-CoA Reductase Inhibitors as Adjuvants in the Modulation of Efflux Pump-Mediated Bacterial and Tumor Resistance. Antibiotics 2023, 12, 1468. https://doi.org/10.3390/antibiotics12091468
Schelz Z, Muddather HF, Zupkó I. Repositioning of HMG-CoA Reductase Inhibitors as Adjuvants in the Modulation of Efflux Pump-Mediated Bacterial and Tumor Resistance. Antibiotics. 2023; 12(9):1468. https://doi.org/10.3390/antibiotics12091468
Chicago/Turabian StyleSchelz, Zsuzsanna, Hiba F. Muddather, and István Zupkó. 2023. "Repositioning of HMG-CoA Reductase Inhibitors as Adjuvants in the Modulation of Efflux Pump-Mediated Bacterial and Tumor Resistance" Antibiotics 12, no. 9: 1468. https://doi.org/10.3390/antibiotics12091468