

The Application of Digital Technologies and Artificial Intelligence in Healthcare: An Overview on Nutrition Assessment


 , ,
, ,  , and
, and 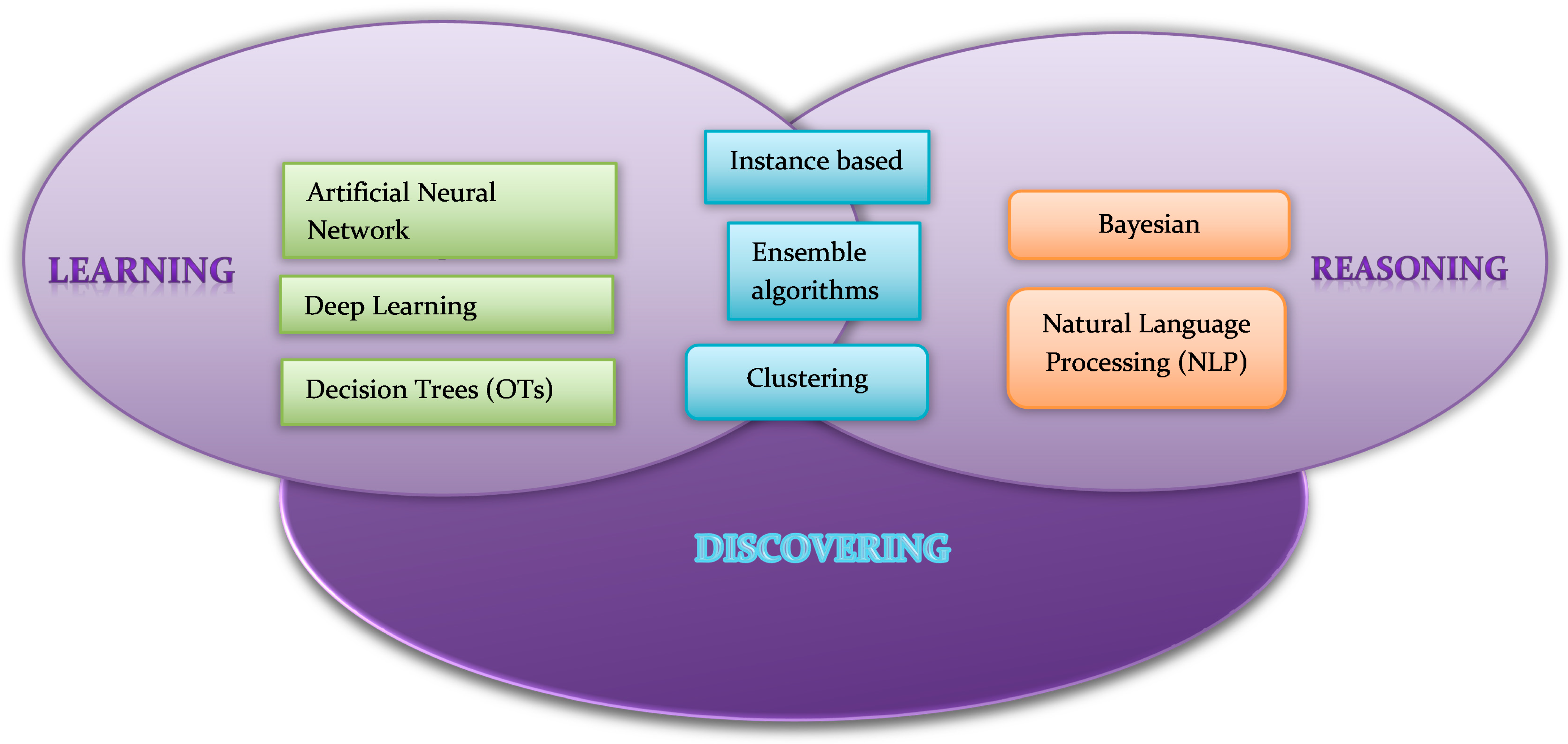{kind=link}
Abstract
:1. Introduction
2. Digital Technologies and Devices in Nutrition
3. Principles of Artificial Intelligence
4. Artificial Intelligence in the Management of Nutrition-Related Diseases
4.1. Artificial Intelligence in Diabetes
4.2. Artificial Intelligence in Obesity
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Artificial Intelligence. Definition of Artificial Intelligence in English by Oxford Dictionaries; Oxford Dictionaries: Oxford, UK, 2023. [Google Scholar]
- Scerri, M.; Grech, V. Artificial Intelligence in Medicine. Early Hum. Dev. 2020, 145, 105017. [Google Scholar] [CrossRef] [PubMed]
- Manne1, R.; Kantheti, S.C. Application of Artificial Intelligence in Healthcare: Chances and Challenges. Curr. Appl. Sci. Technol. 2021, 40, 78–89. [Google Scholar] [CrossRef]
- Dugan, T.M.; Mukhopadhyay, S.; Carroll, A.; Downs, S. Machine Learning Techniques for Prediction of Early Childhood Obesity. Appl. Clin. Inform. 2015, 6, 506–520. [Google Scholar] [PubMed] [Green Version]
- Ghelani, D.P.; Moran, L.J.; Johnson, C.; Mousa, A.; Naderpoor, N. Mobile Apps for Weight Management: A Review of the Latest Evidence to Inform Practice. Front. Endocrinol. 2020, 11, 412. [Google Scholar] [CrossRef]
- Mehta, N.; Devarakonda, M.V. Machine Learning, Natural Language Programming, and Electronic Health Records: The Next Step in the Artificial Intelligence Journey? J. Allergy Clin. Immunol. 2018, 141, 2019–2021.e1. [Google Scholar] [CrossRef] [Green Version]
- Pellegrini, C.A.; Pfammatter, A.F.; Conroy, D.E.; Spring, B. Smartphone Applications to Support Weight Loss: Current Perspectives. Adv. Health Care Technol. 2015, 1, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Wiens, J.; Shenoy, E.S. Machine Learning for Healthcare: On the Verge of a Major Shift in Healthcare Epidemiology. Clin. Infect. Dis. 2018, 66, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://sensortower.com/blog/mobile-wellness-market-trends-2021 (accessed on 12 January 2023).
- Limketkai, B.N.; Mauldin, K.; Manitius, N.; Jalilian, L.; Salonen, B.R. The Age of Artificial Intelligence: Use of Digital Technology in Clinical Nutrition. Curr. Surg. Rep. 2021, 9, 20. [Google Scholar] [CrossRef]
- Flores Mateo, G.; Granado-Font, E.; Ferré-Grau, C.; Montaña-Carreras, X. Mobile Phone Apps to Promote Weight Loss and Increase Physical Activity: A Systematic Review and Meta-Analysis. J. Med. Internet. Res. 2015, 17, e253. [Google Scholar] [CrossRef] [Green Version]
- Amft, O.; Kusserow, M.; Tröster, G. Bite Weight Prediction from Acoustic Recognition of Chewing. IEEE Trans. Biomed. Eng. 2009, 56, 1663–1672. [Google Scholar] [CrossRef] [Green Version]
- Bruno, V.; Resende, S.; Juan, C. A Survey on Automated Food Monitoring and Dietary Management Systems. J. Health Med. Inform. 2017, 8, 272. [Google Scholar]
- Zhang, W.; Yu, Q.; Siddiquie, B.; Divakaran, A.; Sawhney, H. “Snap-n-Eat”: Food Recognition and Nutrition Estimation on a Smartphone. J. Diabetes Sci. Technol. 2015, 9, 525–533. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Plourde, H.; Bouzo, V.; Kilgour, R.D.; Cohen, T.R. Validity and Usability of a Smartphone Image-Based Dietary Assessment App Compared to 3-Day Food Diaries in Assessing Dietary Intake Among Canadian Adults: Randomized Controlled Trial. JMIR Mhealth Uhealth. 2020, 8, e16953. [Google Scholar] [CrossRef]
- High Level Group in Artificial Intelligence. A Definition of AI: Main Capabilities and Disciplines; European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Alloghani, M.; Aljaaf, A.; Hussain, A.; Baker, T.; Mustafina, J.; Al-Jumeily, D.; Khalaf, M. Implementation of Machine Learning Algorithms to Create Diabetic Patient Re-Admission Profiles. BMC Med. Inform. Decis. Mak. 2019, 19, 253. [Google Scholar] [CrossRef] [Green Version]
- An, Q.; Rahman, S.; Zhou, J.; Kang, J.J. A Comprehensive Review on Machine Learning in Healthcare Industry: Classification, Restrictions, Opportunities and Challenges. Sensors 2023, 23, 4178. [Google Scholar] [CrossRef]
- Kirk, D.; Kok, E.; Tufano, M.; Tekinerdogan, B.; Feskens, E.J.M.; Camps, G. Machine Learning in Nutrition Research. Adv. Nutr. 2022, 13, 2573–2589. [Google Scholar] [CrossRef]
- Zhang, C.; Ma, Y. Ensemble Machine Learning. Methods and Applications; Springer Science: New York, NY, USA, 2012. [Google Scholar]
- Howley, T.; Madden, M.G. The Genetic Kernel Support Vector Machine: Description and Evaluation. Artif. Intell. Rev. 2005, 24, 379–395. [Google Scholar] [CrossRef]
- Sarker, I.H. Machine Learning: Algorithms, Real-World Applications and Research Directions. SN Comput. Sci. 2021, 2, 160. [Google Scholar] [CrossRef]
- Talukder, A.; Ahammed, B. Machine Learning Algorithms for Predicting Malnutrition among Under-Five Children in Bangladesh. Nutrition 2020, 78, 110861. [Google Scholar] [CrossRef]
- Fu, Y.; Gou, W.; Hu, W.; Mao, Y.; Tian, Y.; Liang, X.; Guan, Y.; Huang, T.; Li, K.; Guo, X.; et al. Integration of an Interpretable Machine Learning Algorithm to Identify Early Life Risk Factors of Childhood Obesity among Preterm Infants: A Prospective Birth Cohort. BMC Med. 2020, 18, 184. [Google Scholar] [CrossRef]
- Panaretos, D.; Koloverou, E.; Dimopoulos, A.; Kouli, G.; Vamvakari, M.; Tzavelas, G.; Pitsavos, C.; Panagiotakos, D. A Comparison of Statistical and Machine-Learning Techniques in Evaluating the Association between Dietary Patterns and 10-year Cardiometabolic Risk (2002–2012): The ATTICA Study. Brit. J. Nutr. 2018, 120, 326–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigdon, J.; Basu, S. Machine Learning with Sparse Nutrition Data to Improve Cardiovascular Mortality Risk Prediction in the USA Using Nationally Randomly Sampled Data. BMJ Open. 2019, 9, e032703. [Google Scholar] [CrossRef] [PubMed]
- Dongare, A.D.; Kharde, R.R.; Kachare, A.D. Introduction to Artificial Neural Network. Int. J. Eng. Innov. Technol. 2012, 2, 189–194. [Google Scholar]
- Deng, L.; Yu, D. Deep Learning: Methods and Applications. Found. Trends Signal Process 2014, 7, 197–387. [Google Scholar] [CrossRef] [Green Version]
- Liddy, E.D. Natural Language Processing. In Encyclopedia of Library and Information Science, 2nd ed.; Marcel Decker, Inc.: New York, NY, USA, 2001. [Google Scholar]
- Forouhi, N.G.; Wareham, N.J. Epidemiology of diabetes. Medicine 2022, 50, 638–643. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Messer, L.H.; Forlenza, G.P.; Sherr, J.L.; Wadwa, R.P.; Buckingham, B.A.; Weinzimer, S.A.; Maahs, D.M.; Slover, R.H. Optimizing Hybrid Closed-Loop Therapy in Adolescents and Emerging Adults Using the MiniMed 670G System. Diabetes Care 2018, 41, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, J.L.; Sherr, J.L.; Cengiz, E.; Carria, L.; Roy, A.; Voskanyan, G.; Tamborlane, W.V.; Weinzimer, S.A. Effect of Insulin Feedback on Closed-Loop Glucose Control: A Crossover Study. J. Diabetes Sci. Technol. 2012, 6, 1123–1130. [Google Scholar] [CrossRef] [Green Version]
- Ly, T.T.; Weinzimer, S.A.; Maahs, D.M.; Sherr, J.L.; Roy, A.; Grosman, B.; Cantwell, M.; Kurtz, N.; Carria, L.; Messer, L.; et al. Automated Hybrid Closed-Loop Control with a Proportional-Integral-Derivative Based System in Adolescents and Adults with Type 1 Diabetes: Individualizing Settings for Optimal Performance. Pediatr. Diabetes. 2017, 18, 348–355. [Google Scholar] [CrossRef]
- Garg, S.K.; Weinzimer, S.A.; Tamborlane, W.V.; Buckingham, B.A.; Bode, B.W.; Bailey, T.S.; Brazg, R.L.; Ilany, J.; Slover, R.H.; Anderson, S.M.; et al. Glucose Outcomes with the In-Home Use of a Hybrid Closed-Loop Insulin Delivery System in Adolescents and Adults with Type 1 Diabetes. Diabetes Technol. Thera. 2017, 19, 155–163. [Google Scholar] [CrossRef]
- Hovorka, R.; Canonico, V.; Chassin, L.J.; Haueter, U.; Massi-Benedetti, M.; Orsini Federici, M.; Pieber, T.R.; Schaller, H.C.; Schaupp, L.; Vering, T.; et al. Nonlinear Model Predictive Control of Glucose Concentration in Subjects with Type 1 Diabetes. Physiol. Meas. 2004, 25, 905–920. [Google Scholar] [CrossRef] [Green Version]
- Wilinska, M.E.; Chassin, L.J.; Acerini, C.L.; Allen, J.M.; Dunger, D.B.; Hovorka, R. Simulation Environment to Evaluate Closed-Loop Insulin Delivery Systems in Type 1 Diabetes. J. Diabetes Sci. Technol. 2010, 4, 132–144. [Google Scholar] [CrossRef] [Green Version]
- Man, C.D.; Micheletto, F.; Lv, D.; Breton, M.; Kovatchev, B.; Cobelli, C. The UVA/PADOVA Type 1 Diabetes Simulator: New Features. J. Diabetes Sci. Technol. 2014, 8, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Sun, Q.; Jankovic, M.V.; Mougiakakou, S.G. Reinforcement Learning-Based Adaptive Insulin Advisor for Individuals with Type 1 Diabetes Patients under Multiple Daily Injections Therapy. IEEE Eng. Med. Biol. Soc. 2019, 2019, 3609–3612. [Google Scholar]
- Xie, J.; Wang, Q. Benchmarking Machine Learning Algorithms on Blood Glucose Prediction for Type I Diabetes in Comparison with Classical Time-Series Models. IEEE Trans. Biomed. Eng. 2020, 67, 3101–3124. [Google Scholar] [CrossRef]
- Cleveringa, F.G.; Welsing, P.M.; van den Donk, M.; Gorter, K.J.; Niessen, L.W.; Rutten, G.E.; Redekop, W.K. Cost-Effectiveness of the Diabetes Care Protocol, a Multifaceted Computerized Decision Support Diabetes Management Intervention that Reduces Cardiovascular Risk. Diabetes Care 2010, 33, 258–263. [Google Scholar] [CrossRef] [Green Version]
- Alotaibi, M.M.; Istepanian, R.; Philip, N. A Mobile Diabetes Management and Educational System for Type-2 Diabetics in Saudi Arabia (SAED). Mhealth 2016, 2, 33. [Google Scholar] [CrossRef] [Green Version]
- Contreras, I.; Kiefer, S.; Vehi, J. Adaptive Workflows for Diabetes Management: Self-Management Assistant and Remote Treatment for Diabetes. Stud. Health Technol. Inform. 2017, 237, 151–156. [Google Scholar]
- Greaves, F.; Ramirez-Cano, D.; Millett, C.; Darzi, A.; Donaldson, L. Use of Sentiment Analysis for Capturing Patient Experience from Free-Text Comments Posted Online. J. Med. Internet Res. 2013, 15, e239. [Google Scholar] [CrossRef]
- Valdez, R.S.; Guterbock, T.M.; Fitzgibbon, K.; Williams, I.C.; Wellbeloved-Stone, C.A.; Bears, J.E.; Menefee, H.K. From Loquacious to Reticent: Understanding Patient Health Information Communication to Guide Consumer Health IT Design. J. Am. Med. Inform. Assoc. 2017, 24, 680–696. [Google Scholar] [CrossRef]
- Chen, A.T. Exploring Online Support Spaces: Using Cluster Analysis to Examine Breast Cancer, Diabetes and Fibromyalgia Support Groups. Patient Educ. Couns. 2012, 87, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Hamon, T.; Gagnayre, R. Improving Knowledge of Patient Skills thanks to Automatic Analysis of Online Discussions. Patient Educ. Couns. 2013, 92, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Eghbali-Zarch, M.; Tavakkoli-Moghaddam, R.; Esfahanian, F.; Sepehri, M.M.; Azaron, A. Pharmacological Therapy Selection of Type 2 Diabetes based on the SWARA and Modified MULTIMOORA Methods under a Fuzzy Environment. Artif. Intell. Med. 2018, 87, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Kurasawa, H.; Hayashi, K.; Fujino, A.; Takasugi, K.; Haga, T.; Waki, K.; Noguchi, T.; Ohe, K. Machine-Learning-Based Prediction of a Missed Scheduled Clinical Appointment by Patients with Diabetes. J. Diabetes Sci. Technol. 2016, 10, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Stewart, Z.A.; Wilinska, M.E.; Hartnell, S.; Temple, R.C.; Rayman, G.; Stanley, K.P.; Simmons, D.; Law, G.R.; Scott, E.M.; Hovorka, R.; et al. Closed-Loop Insulin Delivery during Pregnancy in Women with Type 1 Diabetes. N. Engl. J. Med. 2016, 375, 644–654. [Google Scholar] [CrossRef]
- Hazlehurst, B.L.; Lawrence, J.M.; Donahoo, W.T.; Sherwood, N.E.; Kurtz, S.E.; Xu, S.; Steiner, J.F. Automating Assessment of Lifestyle Counseling in Electronic Health Records. Am. J. Prev. Med. 2014, 46, 457–464. [Google Scholar] [CrossRef] [Green Version]
- Rigla, M.; Martínez-Sarriegui, I.; García-Sáez, G.; Pons, B.; Hernando, M.E. Gestational Diabetes Management Using Smart Mobile Telemedicine. J. Diabetes Sci. Technol. 2018, 12, 260–264. [Google Scholar] [CrossRef] [Green Version]
- Caballero-Ruiz, E.; García-Sáez, G.; Rigla, M.; Villaplana, M.; Pons, B.; Hernando, M.E. A Web-Based Clinical Decision Support System for Gestational Diabetes: Automatic Diet Prescription and Detection of Insulin Needs. Int. J. Med. Inform. 2017, 102, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Everett, E.; Kane, B.; Yoo, A.; Dobs, A.; Mathioudakis, N. A Novel Approach for Fully Automated, Personalized Health Coaching for Adults with Prediabetes: Pilot Clinical Trial. J. Med. Internet Res. 2018, 20, e72. [Google Scholar] [CrossRef] [Green Version]
- Yom-Tov, E.; Feraru, G.; Kozdoba, M.; Mannor, S.; Tennenholtz, M.; Hochberg, I. Encouraging Physical Activity in Patients with Diabetes: Intervention Using a Reinforcement Learning System. J. Med. Internet Res. 2017, 19, e338. [Google Scholar] [CrossRef]
- Lin, X.; Li, H. Obesity: Epidemiology, Pathophysiology, and Therapeutics. Front Endocrinol. 2021, 12, 706978. [Google Scholar] [CrossRef]
- Controlling the Global Obesity Epidemic. Available online: https://www.who.int/activities/controlling-the-global-obesity-epidemic (accessed on 3 February 2023).
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Lean, M.E.; Han, T.S.; Morrison, C.E. Waist Circumference as a Measure for Indicating Need for Weight Management. BMJ 1995, 311, 158–161. [Google Scholar] [CrossRef] [Green Version]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 3 February 2023).
- Colmenarejo, G. Machine Learning Models to Predict Childhood and Adolescent Obesity: A Review. Nutrients. 2020, 12, 2466. [Google Scholar] [CrossRef]
- Pei, Z.; Flexeder, C.; Fuertes, E.; Thiering, E.; Koletzko, B.; Cramer, C.; Berdel, D.; Lehmann, I.; Bauer, C.P.; Heinrich, J.; et al. Early Life Risk Factors of Being Overweight at 10 Years of Age: Results of the German Birth Cohorts GINIplus and LISAplus. Eur. J. Clin. Nutr. 2013, 67, 855–862. [Google Scholar] [CrossRef] [Green Version]
- Hammond, R.; Athanasiadou, R.; Curado, S.; Aphinyanaphongs, Y.; Abrams, C.; Messito, M.J.; Gross, R.; Katzow, M.; Jay, M.; Razavian, N.; et al. Predicting Childhood Obesity using Electronic Health Records and Publicly Available Data. PLoS ONE 2019, 14, e0215571. [Google Scholar] [CrossRef] [Green Version]
- Spring, B.; Duncan, J.M.; Janke, E.A.; Kozak, A.T.; McFadden, H.G.; DeMott, A.; Pictor, A.; Epstein, L.H.; Siddique, J.; Pellegrini, C.A.; et al. Integrating Technology into Standard Weight Loss Treatment: A Randomized Controlled Trial. JAMA Intern. Med. 2013, 173, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Hatoum, I.J.; Blackstone, R.; Hunter, T.D.; Francis, D.M.; Steinbuch, M.; Harris, J.L.; Kaplan, L.M. Clinical Factors Associated with Remission of Obesity-Related Comorbidities After Bariatric Surgery. JAMA Surg. 2016, 151, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A.H.; Adler, S.; Stevens, H.B.; Darcy, A.M.; Morton, J.M.; Safer, D.L. What Variables are Associated with Successful Weight Loss Outcomes for Bariatric Surgery after 1 Year? Surg. Obes. Relat. Dis. 2014, 10, 697–704. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G. Neural Networks for Classification: A Survey. IEEE Trans. Syst. Man. Cybern. 2000, 30, 451–462. [Google Scholar] [CrossRef] [Green Version]
- Courcoulas, A.P.; Christian, N.J.; O’Rourke, R.W.; Dakin, G.; Patchen Dellinger, E.; Flum, D.R.; Melissa Kalarchian, P.D.; Mitchell, J.E.; Patterson, E.; Pomp, A.; et al. Preoperative Factors and 3-Year Weight Change in the Longitudinal Assessment of Bariatric Surgery (LABS) Consortium. Surg. Obes. Relat. Dis. 2015, 11, 1109–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Gemming, L.; Hanning, R.; Allman-Farinelli, M. Smartphone Apps and the Nutrition Care Process: Current Perspectives and Future Considerations. Patient Educ. Couns. 2018, 101, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Michel, M.; Burbidge, A. Nutrition in the Digital Age—How Digital Tools Can Help to Solve the Personalized Nutrition Conundrum. Trends Food Sci. Technol. 2019, 90, 194–200. [Google Scholar] [CrossRef]
- Verma, M.; Hontecillas, R.; Tubau-Juni, N.; Abedi, V.; Bassaganya-Riera, J. Challenges in Personalized Nutrition and Health. Front. Nutr. 2018, 5, 117. [Google Scholar] [CrossRef] [Green Version]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salinari, A.; Machì, M.; Armas Diaz, Y.; Cianciosi, D.; Qi, Z.; Yang, B.; Ferreiro Cotorruelo, M.S.; Villar, S.G.; Dzul Lopez, L.A.; Battino, M.; et al. The Application of Digital Technologies and Artificial Intelligence in Healthcare: An Overview on Nutrition Assessment. Diseases 2023, 11, 97. https://doi.org/10.3390/diseases11030097
Salinari A, Machì M, Armas Diaz Y, Cianciosi D, Qi Z, Yang B, Ferreiro Cotorruelo MS, Villar SG, Dzul Lopez LA, Battino M, et al. The Application of Digital Technologies and Artificial Intelligence in Healthcare: An Overview on Nutrition Assessment. Diseases. 2023; 11(3):97. https://doi.org/10.3390/diseases11030097
Chicago/Turabian StyleSalinari, Alessia, Michele Machì, Yasmany Armas Diaz, Danila Cianciosi, Zexiu Qi, Bei Yang, Maria Soledad Ferreiro Cotorruelo, Santos Gracia Villar, Luis Alonso Dzul Lopez, Maurizio Battino, and et al. 2023. "The Application of Digital Technologies and Artificial Intelligence in Healthcare: An Overview on Nutrition Assessment" Diseases 11, no. 3: 97. https://doi.org/10.3390/diseases11030097