
AED Inequity among Social Groups in Guangzhou
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
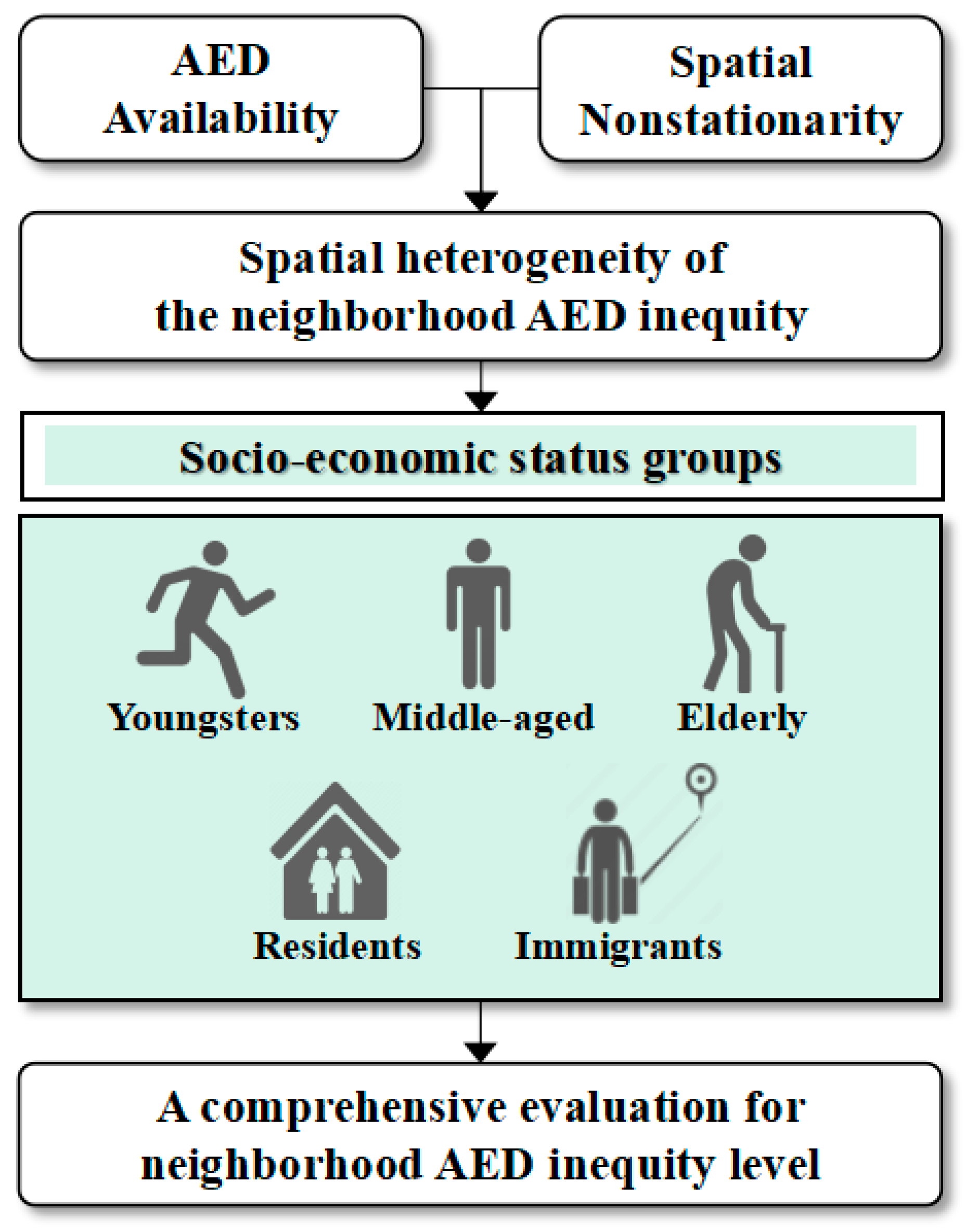
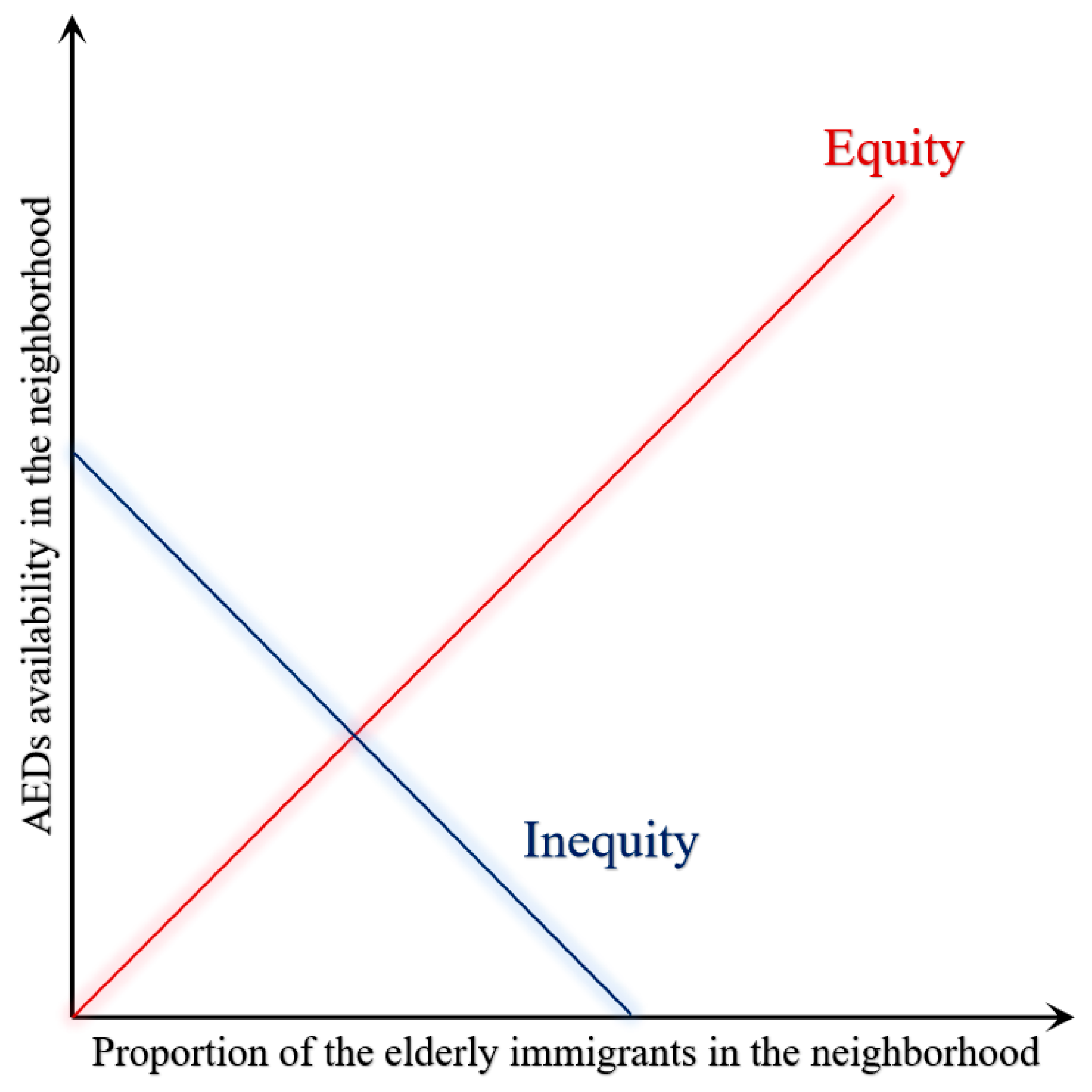
2.1. Theoretical Framework
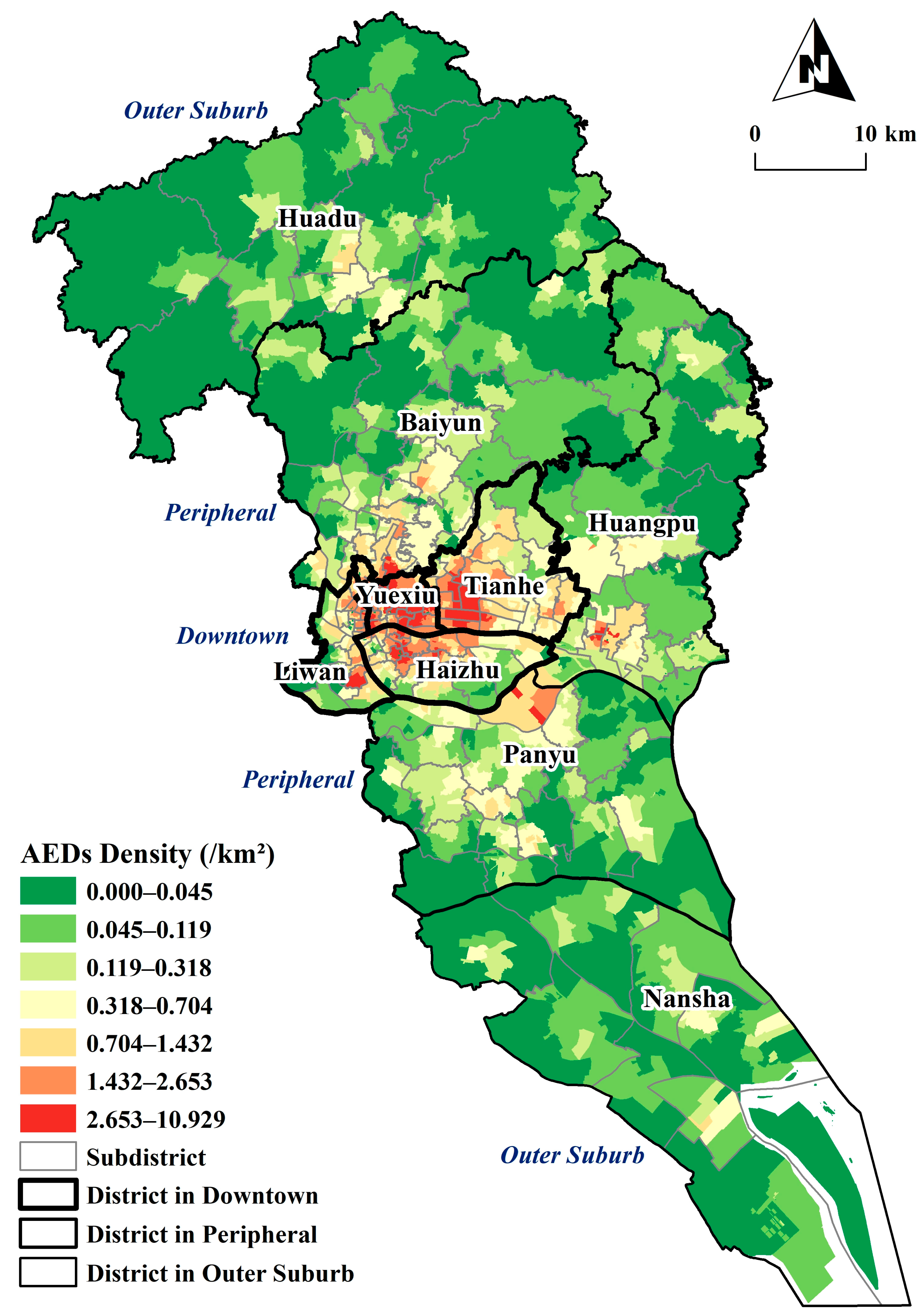
2.2. Study Area
2.3. AED Data
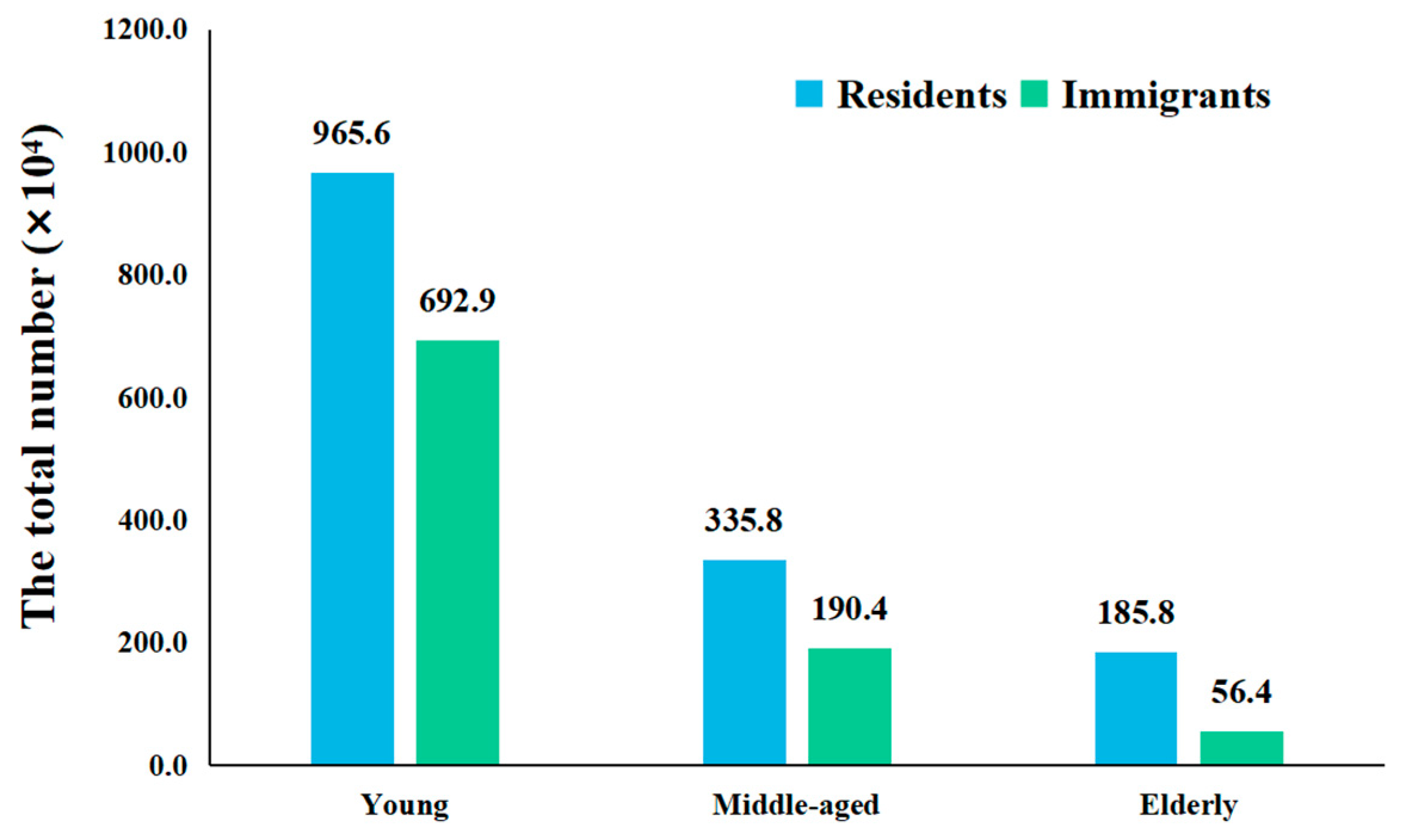
2.4. Demographic Data
2.5. Geographically Weighted Regression
3. Results
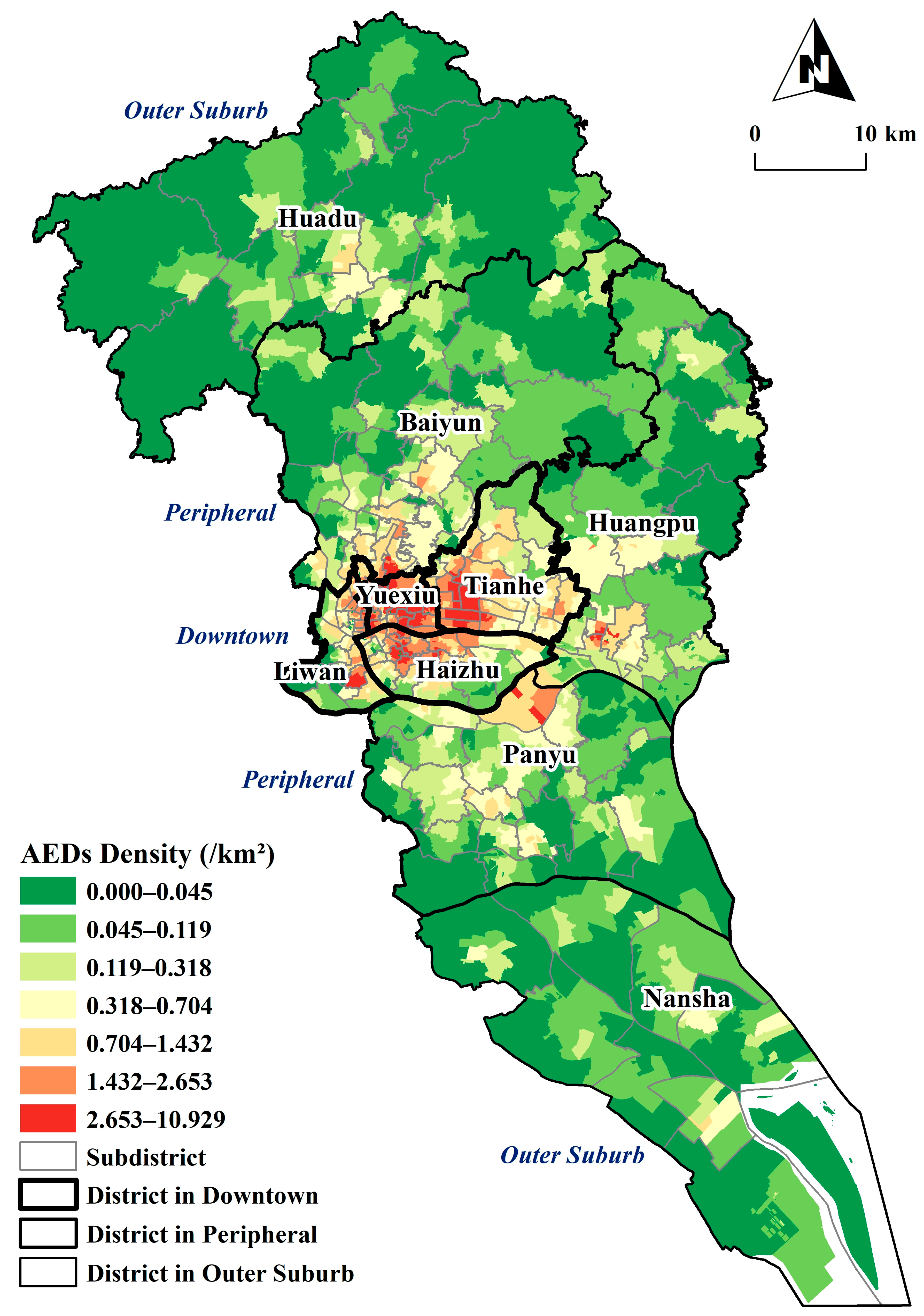
3.1. Spatial Distribution of AED Availability
3.2. Global AED Inequity
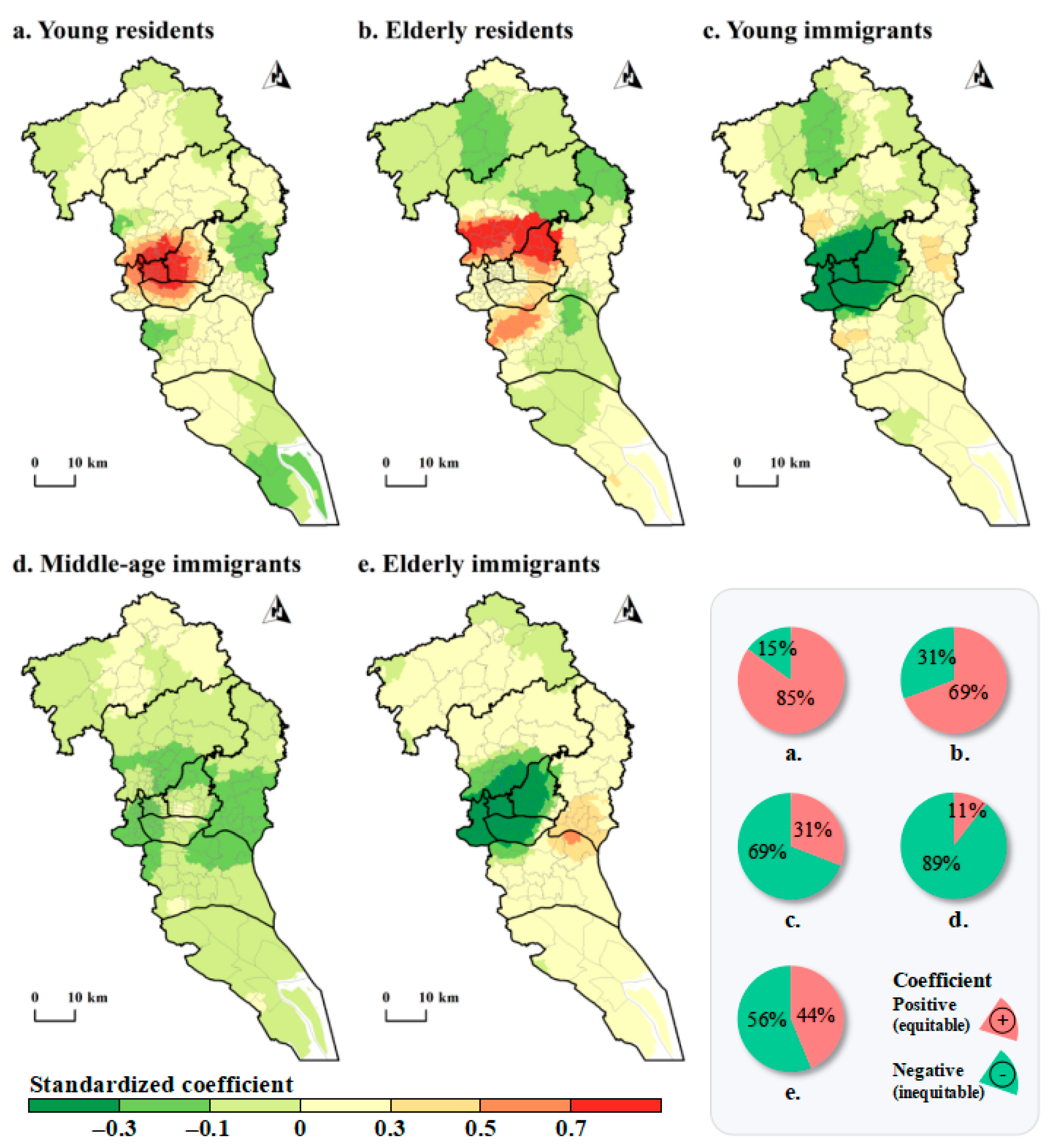
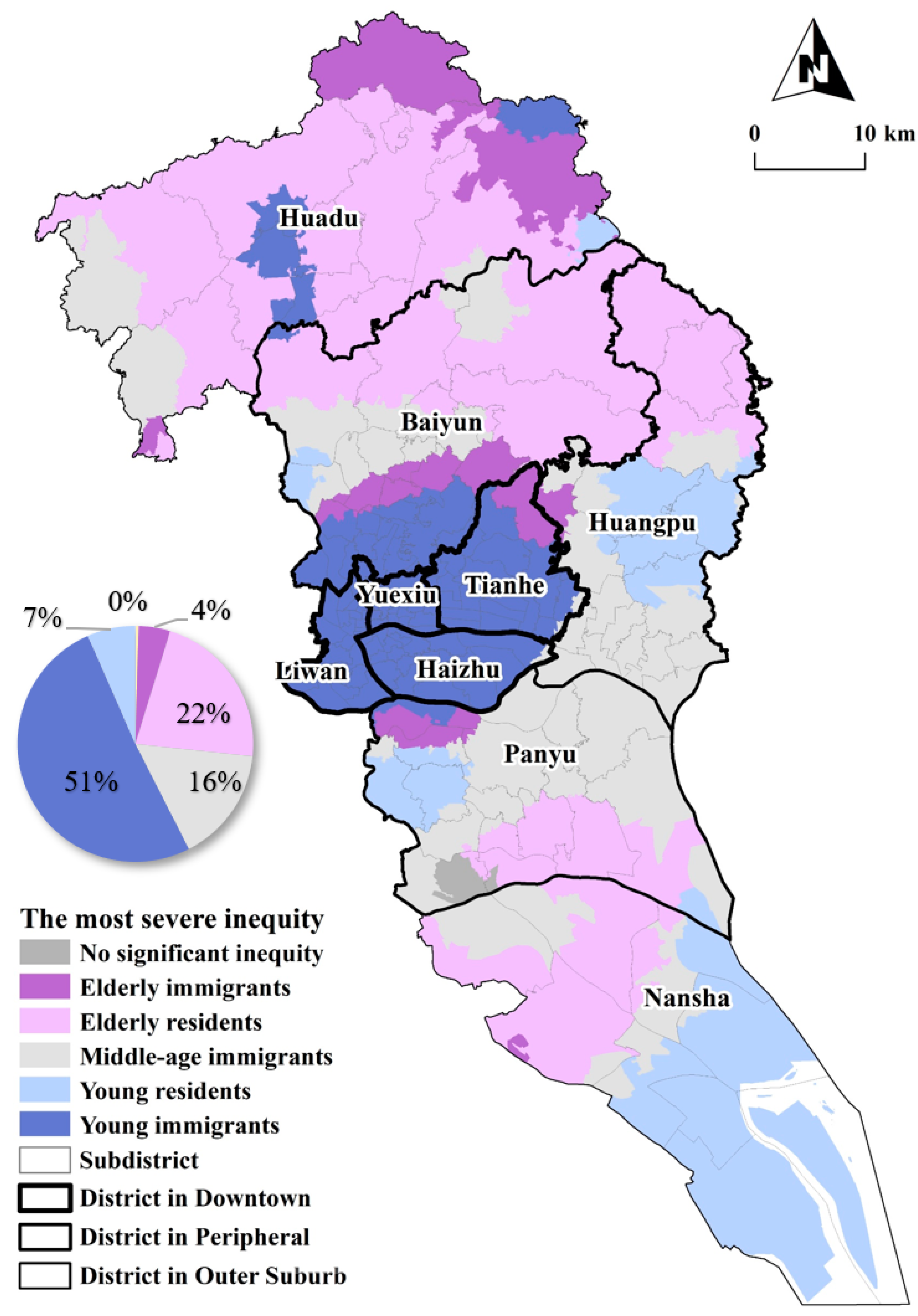
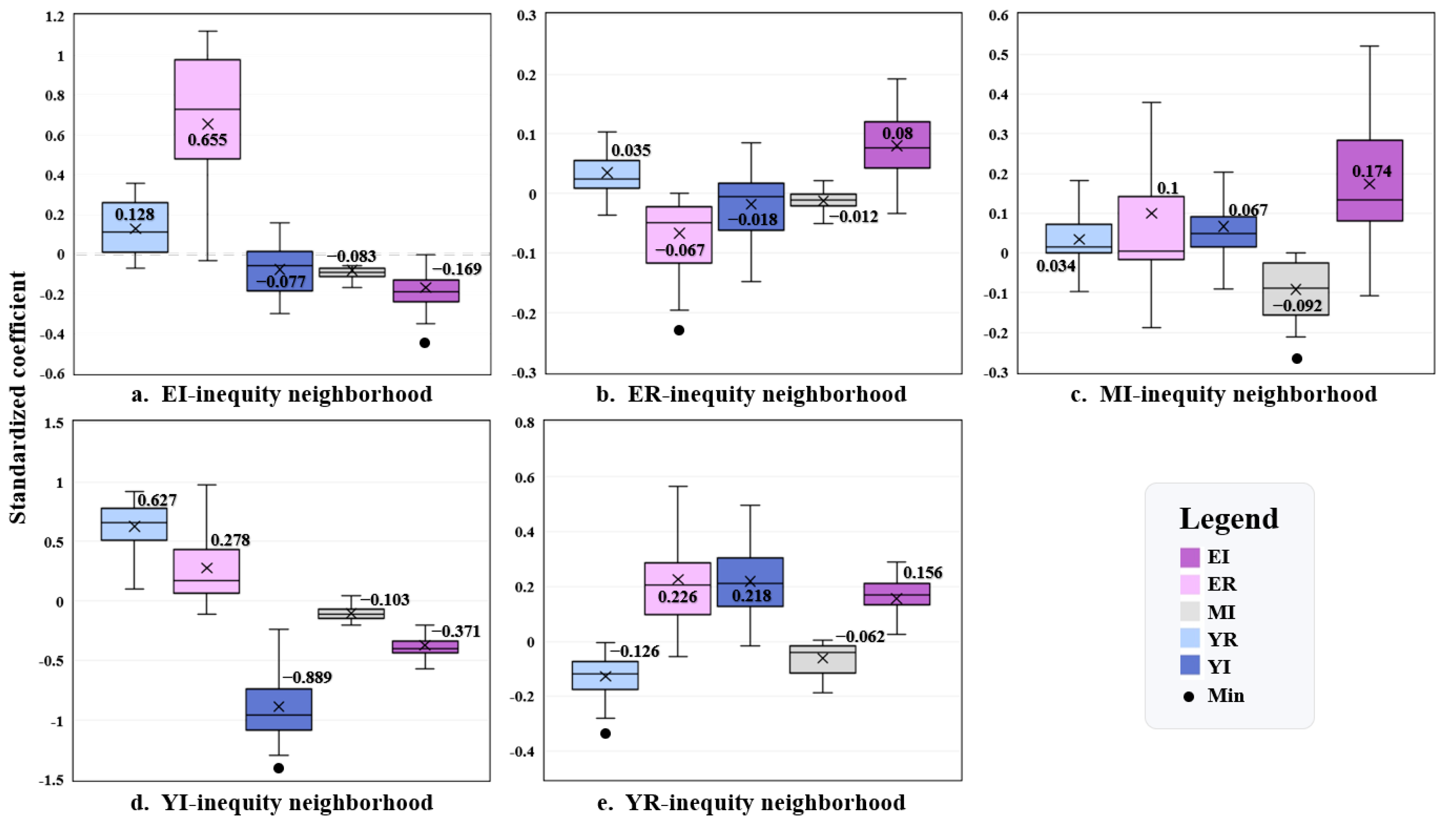
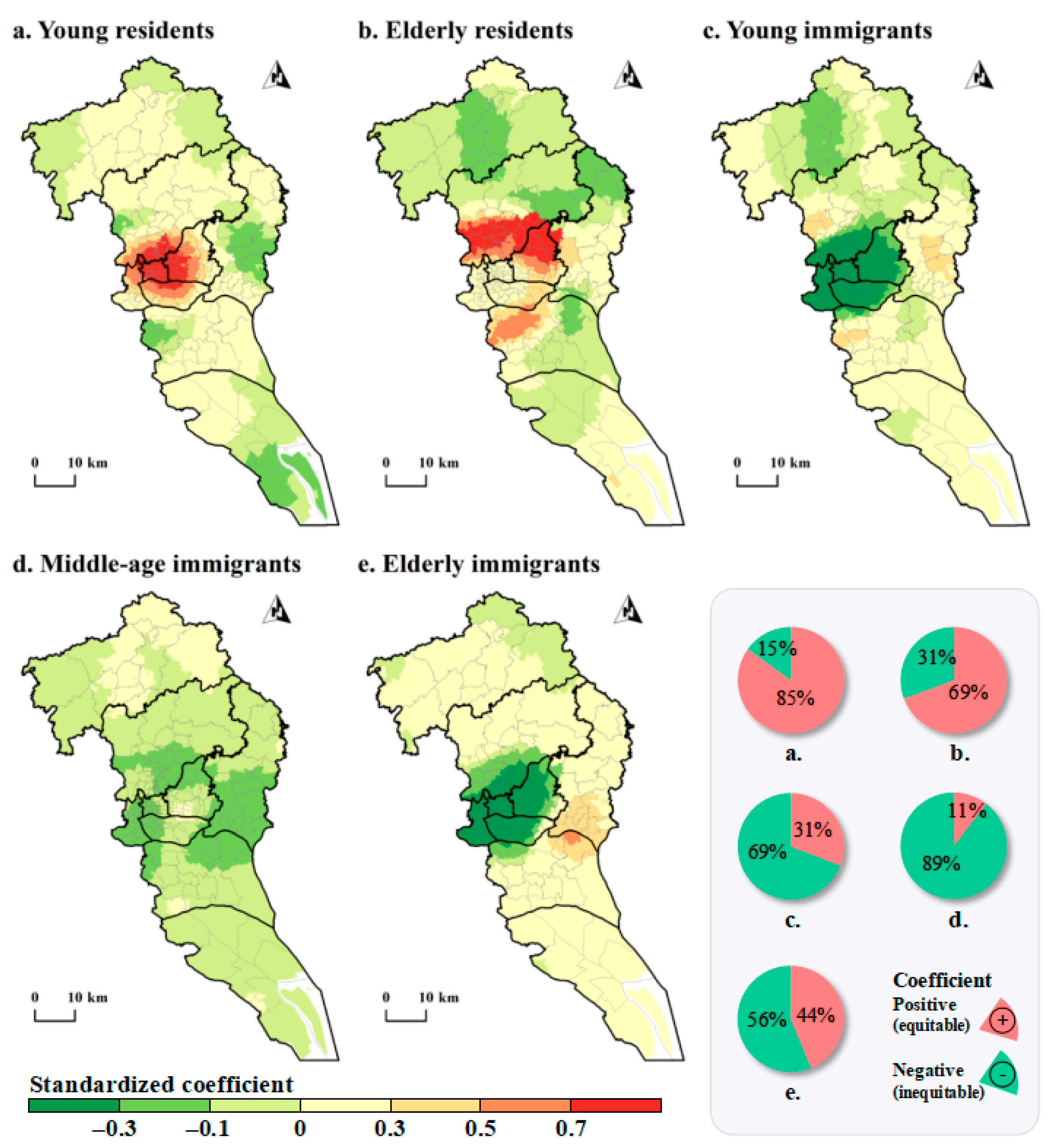
3.3. Local AED Inequity
3.3.1. Young Residents
3.3.2. Elderly Residents
3.3.3. Young Immigrants
3.3.4. Middle-Aged Immigrants
3.3.5. Elderly Immigrants
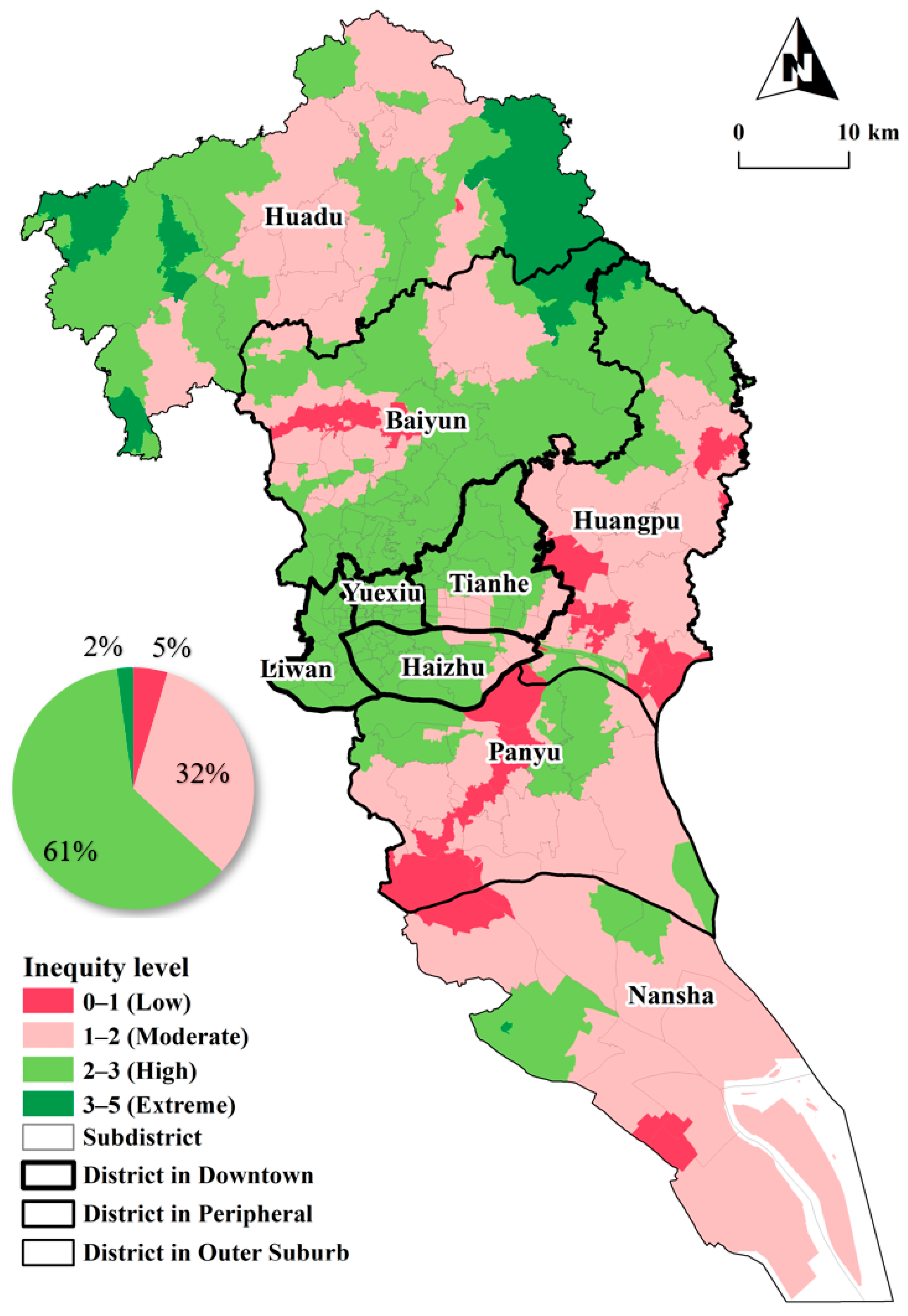
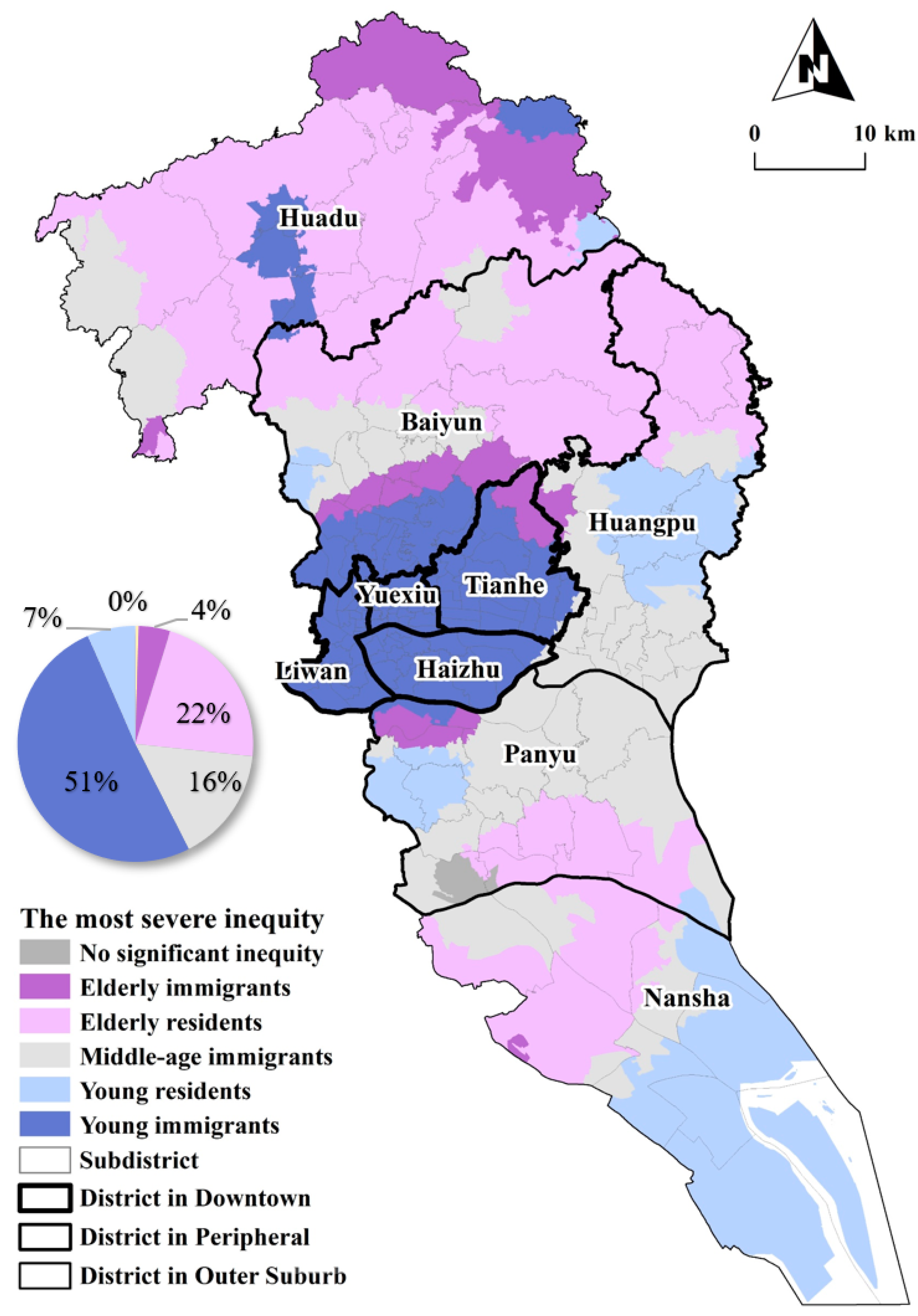
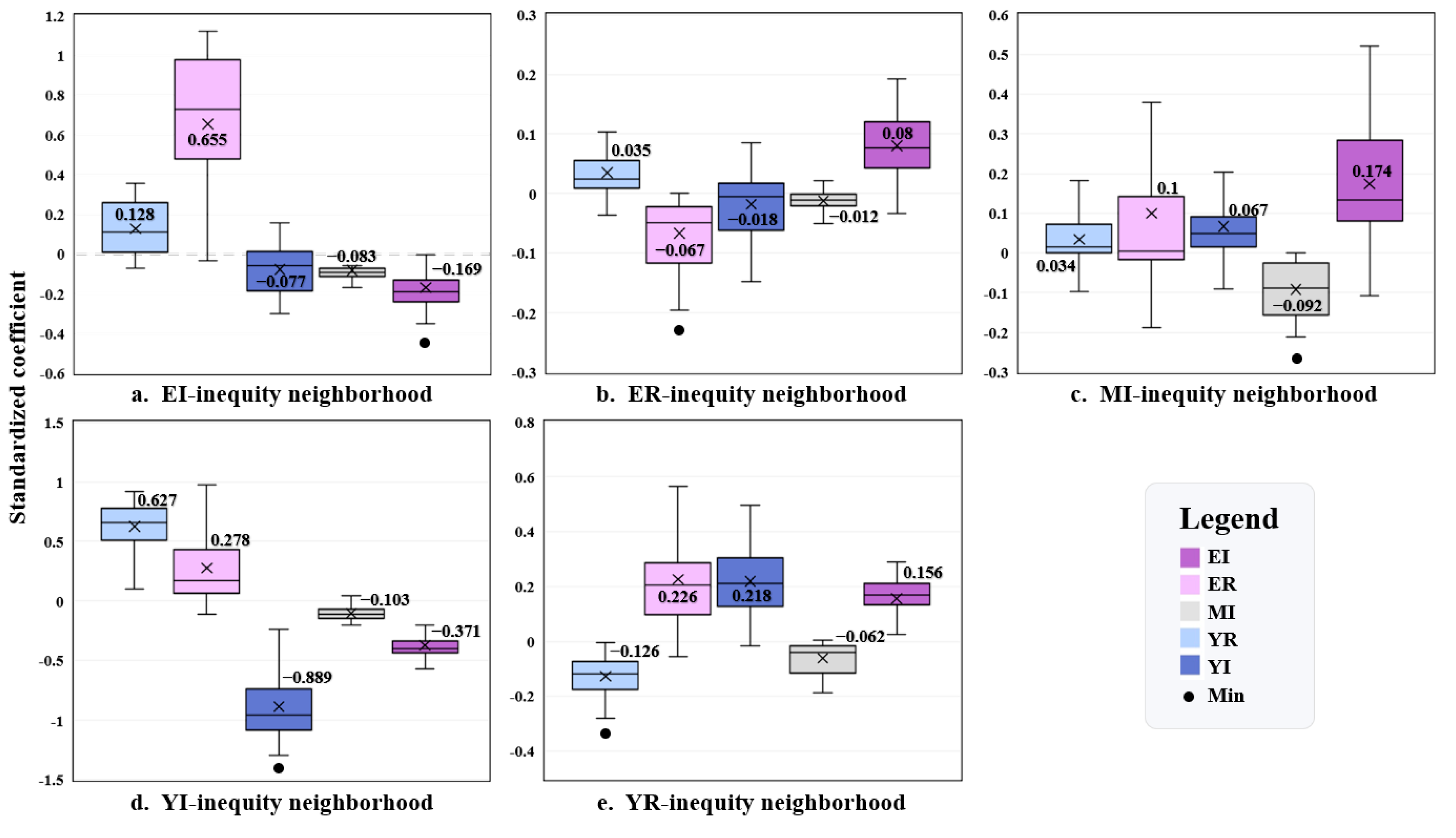
3.4. Spatial Patterns of AED Inequity Level
4. Discussion
4.1. Inequitable Access to AED in Guangzhou
4.2. Implications for AED Facility Management and Optimization
4.3. Theoretical Implications
4.4. Limitations
- Although this study examines inequity in AED facilities from the perspective of spatial heterogeneity, it could not cover the analysis of the whole social group due to the availability of data, such as for groups with different housing sizes.
- The neighborhood administrative boundary is taken as the spatial unit in this study, and the analysis modeling results may be affected by the modifiable areal unit problem [64].
- Due to data availability, our analysis does not cover the historical OHCA cases. Future studies should obtain more comprehensive variables, AED facility data of more cities, and modeling to consider scale effects.
- This study measured the AED availability based on the maximum rescue time. Further investigation should incorporate both minimum and maximum rescue time ranges for comprehensive understanding.
- Since the collinearity problem needs to be solved before the linear regression model is adopted, one kind of social group was omitted from the model result. In the next step, we will consider other models to avoid this limitation, because inequity is equally important for each social group.
- Although this study identified spatial heterogeneity in the inequality of access to AEDs across social groups, the next step should be to explore the relationship between the equity of various social groups in each neighborhood.
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kitamura, T.; Iwami, T.; Kawamura, T.; Nagao, K.; Tanaka, H.; Hiraide, A. Nationwide Public-Access Defibrillation in Japan. N. Engl. J. Med. 2010, 362, 994–1004. [Google Scholar] [CrossRef]
- Zhang, S. Sudden Cardiac Death in China: Current Status and Future Perspectives. Europace 2015, 17, ii14–ii18. [Google Scholar] [CrossRef]
- The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on Cardiovascular Health and Diseases in China 2022: An Updated Summary. Biomed. Environ. Sci. 2023, 35, 669–701. [Google Scholar] [CrossRef]
- Brooks, S.C.; Hsu, J.H.; Tang, S.K.; Jeyakumar, R.; Chan, T.C.Y. Determining Risk for Out-of-Hospital Cardiac Arrest by Location Type in a Canadian Urban Setting to Guide Future Public Access Defibrillator Placement. Ann. Emerg. Med. 2013, 61, 530–538.e2. [Google Scholar] [CrossRef] [PubMed]
- Deakin, C.D.; Shewry, E.; Gray, H.H. Public Access Defibrillation Remains out of Reach for Most Victims of Out-of-Hospital Sudden Cardiac Arrest. Heart 2014, 100, 619–623. [Google Scholar] [CrossRef]
- Pulver, A.; Wei, R. Optimizing the Spatial Location of Medical Drones. Appl. Geogr. 2018, 90, 9–16. [Google Scholar] [CrossRef]
- Blom, M.T.; Beesems, S.G.; Homma, P.C.M.; Zijlstra, J.A.; Hulleman, M.; van Hoeijen, D.A.; Bardai, A.; Tijssen, J.G.P.; Tan, H.L.; Koster, R.W. Improved Survival After Out-of-Hospital Cardiac Arrest and Use of Automated External Defibrillators. Circulation 2014, 130, 1868–1875. [Google Scholar] [CrossRef] [PubMed]
- Folke, F.; Lippert, F.K.; Nielsen, S.L.; Gislason, G.H.; Hansen, M.L.; Schramm, T.K.; Sørensen, R.; Fosbøl, E.L.; Andersen, S.S.; Rasmussen, S.; et al. Location of Cardiac Arrest in a City Center: Strategic Placement of Automated External Defibrillators in Public Locations. Circulation 2009, 120, 510–517. [Google Scholar] [CrossRef]
- Lwanga, A.; Garcia-Sayan, E.; Lwanga, S.; Karreman, E.; Mohamed, A. Automated External Defibrillators and Survival After Nonresidential Out of Hospital Cardiac Arrest in a Small North American City. Am. J. Cardiol. 2017, 119, 1979–1982. [Google Scholar] [CrossRef]
- Ringh, M.; Hollenberg, J.; Palsgaard-Moeller, T.; Svensson, L.; Rosenqvist, M.; Lippert, F.K.; Wissenberg, M.; Malta Hansen, C.; Claesson, A.; Viereck, S.; et al. The Challenges and Possibilities of Public Access Defibrillation. J. Intern. Med. 2018, 283, 238–256. [Google Scholar] [CrossRef]
- Fredman, D.; Haas, J.; Ban, Y.; Jonsson, M.; Svensson, L.; Djarv, T.; Hollenberg, J.; Nordberg, P.; Ringh, M.; Claesson, A. Use of a Geographic Information System to Identify Differences in Automated External Defibrillator Installation in Urban Areas with Similar Incidence of Public Out-of-Hospital Cardiac Arrest: A Retrospective Registry-Based Study. BMJ Open 2017, 7, e014801. [Google Scholar] [CrossRef] [PubMed]
- Pollack, R.A.; Brown, S.P.; Rea, T.; Aufderheide, T.; Barbic, D.; Buick, J.E.; Christenson, J.; Idris, A.H.; Jasti, J.; Kampp, M.; et al. Impact of Bystander Automated External Defibrillator Use on Survival and Functional Outcomes in Shockable Observed Public Cardiac Arrests. Circulation 2018, 137, 2104–2113. [Google Scholar] [CrossRef]
- Tsai, Y.-S.; Ko, P.C.-I.; Huang, C.-Y.; Wen, T.-H. Optimizing Locations for the Installation of Automated External Defibrillators (AEDs) in Urban Public Streets through the Use of Spatial and Temporal Weighting Schemes. Appl. Geogr. 2012, 35, 394–404. [Google Scholar] [CrossRef]
- Bonnet, B.; Gama Dessavre, D.; Kraus, K.; Ramirez-Marquez, J.E. Optimal Placement of Public-Access AEDs in Urban Environments. Comput. Ind. Eng. 2015, 90, 269–280. [Google Scholar] [CrossRef]
- Chen, G.; Widener, M.J.; Zhu, M.; Wang, C.C. Identification of Priority Areas for Public-Access Automated External Defibrillators (AEDs) in Metropolitan Areas: A Case Study in Hangzhou, China. Appl. Geogr. 2023, 154, 102922. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Wen, T.-H. Optimal Installation Locations for Automated External Defibrillators in Taipei 7-Eleven Stores: Using GIS and a Genetic Algorithm with a New Stirring Operator. Comput. Math. Methods Med. 2014, 2014, 241435. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.-C.; Chen, C.-W.; Chen, C.-C.; Kuo, C.-L.; Fan, I.; Ho, C.-K.; Liu, I.-C.; Chan, T.-C. Spatial Decision on Allocating Automated External Defibrillators (AED) in Communities by Multi-Criterion Two-Step Floating Catchment Area (MC2SFCA). Int. J. Health Geogr. 2016, 15, 17. [Google Scholar] [CrossRef] [PubMed]
- Aeby, D.; Staeger, P.; Dami, F. How to Improve Automated External Defibrillator Placement for Out-of-Hospital Cardiac Arrests: A Case Study. PLoS ONE 2021, 16, e0250591. [Google Scholar] [CrossRef] [PubMed]
- Rea, T.D.; Olsufka, M.; Bemis, B.; White, L.; Yin, L.; Becker, L.; Copass, M.; Eisenberg, M.; Cobb, L. A Population-Based Investigation of Public Access Defibrillation: Role of Emergency Medical Services Care. Resuscitation 2010, 81, 163–167. [Google Scholar] [CrossRef]
- Yang, L.; Xiong, L.; Yang, W. An Accessibility Spatial Search Algorithm to Optimize Defibrillator Deployment in Indoor Space. Int. J. Geogr. Inf. Sci. 2021, 35, 1251–1272. [Google Scholar] [CrossRef]
- Yasunaga, H.; Miyata, H.; Horiguchi, H.; Tanabe, S.; Akahane, M.; Ogawa, T.; Koike, S.; Imamura, T. Population Density, Call-Response Interval, and Survival of out-of-Hospital Cardiac Arrest. Int. J. Health Geogr. 2011, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Tsukigase, K.; Tanaka, H.; Takyu, H. Mismatch between Sites of Incidence of Out-of-Hospital Cardiac Arrest and Locations of Installed Automated External Defibrillator in the Tokyo Metropolitan Area. WJCD 2017, 7, 185–194. [Google Scholar] [CrossRef]
- Jin, T.; Cheng, L.; Wang, K.; Cao, J.; Huang, H.; Witlox, F. Examining Equity in Accessibility to Multi-Tier Healthcare Services across Different Income Households Using Estimated Travel Time. Transp. Policy 2022, 121, 1–13. [Google Scholar] [CrossRef]
- Mayaud, J.R.; Tran, M.; Nuttall, R. An Urban Data Framework for Assessing Equity in Cities: Comparing Accessibility to Healthcare Facilities in Cascadia. Comput. Environ. Urban Syst. 2019, 78, 101401. [Google Scholar] [CrossRef]
- Mishra, S.; Sahu, P.K.; Sarkar, A.K.; Mehran, B.; Sharma, S. Geo-Spatial Site Suitability Analysis for Development of Health Care Units in Rural India: Effects on Habitation Accessibility, Facility Utilization and Zonal Equity in Facility Distribution. J. Transp. Geogr. 2019, 78, 135–149. [Google Scholar] [CrossRef]
- Gu, Z.; Luo, X.; Tang, M.; Liu, X. Does the Edge Effect Impact the Healthcare Equity? An Examination of the Equity in Hospitals Accessibility in the Edge City in Multi-Scale. J. Transp. Geogr. 2023, 106, 103513. [Google Scholar] [CrossRef]
- Hare, T.S.; Barcus, H.R. Geographical Accessibility and Kentucky’s Heart-Related Hospital Services. Appl. Geogr. 2007, 27, 181–205. [Google Scholar] [CrossRef]
- Rong, P.; Zheng, Z.; Kwan, M.-P.; Qin, Y. Evaluation of the Spatial Equity of Medical Facilities Based on Improved Potential Model and Map Service API: A Case Study in Zhengzhou, China. Appl. Geogr. 2020, 119, 102192. [Google Scholar] [CrossRef]
- Yan, X.; Shan, L.; He, S.; Zhang, J. Cross-City Patient Mobility and Healthcare Equity and Efficiency: Evidence from Hefei, China. Travel Behav. Soc. 2022, 28, 1–12. [Google Scholar] [CrossRef]
- Zhao, P.; Li, S.; Liu, D. Unequable Spatial Accessibility to Hospitals in Developing Megacities: New Evidence from Beijing. Health Place 2020, 65, 102406. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, B.; Shen, Y.; Li, L. Assessing Accessibility to Service Facilities for Older People in Age-Restricted Communities from the Perspective of Equity. J. Transp. Health 2022, 27, 101515. [Google Scholar] [CrossRef]
- Cheng, T.; Liu, C.; Yang, H.; Wang, N.; Liu, Y. From Service Capacity to Spatial Equity: Exploring a Multi-Stage Decision-Making Approach for Optimizing Elderly-Care Facility Distribution in the City Centre of Tianjin, China. Sustain. Cities Soc. 2022, 85, 104076. [Google Scholar] [CrossRef]
- Darcy, S. The Politics of Disability and Access: The Sydney 2000 Games Experience. Disabil. Soc. 2003, 18, 737–757. [Google Scholar] [CrossRef]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M.E. Geographically Weighted Regression: A Method for Exploring Spatial Nonstationarity. Geogr. Anal. 2010, 28, 281–298. [Google Scholar] [CrossRef]
- Yang, W.; Yang, R.; Zhou, S. The Spatial Heterogeneity of Urban Green Space Inequity from a Perspective of the Vulnerable: A Case Study of Guangzhou, China. Cities 2022, 130, 103855. [Google Scholar] [CrossRef]
- Lin, J.; Wang, Q.; Li, X. Socioeconomic and Spatial Inequalities of Street Tree Abundance, Species Diversity, and Size Structure in New York City. Landsc. Urban Plan. 2021, 206, 103992. [Google Scholar] [CrossRef]
- Shi, H.; Huang, H.; Ma, D.; Chen, L.; Zhao, M. Capturing Urban Recreational Hotspots from GPS Data: A New Framework in the Lens of Spatial Heterogeneity. Comput. Environ. Urban Syst. 2023, 103, 101972. [Google Scholar] [CrossRef]
- Gao, F.; Liao, S.; Wang, Z.; Cai, G.; Feng, L.; Yang, Z.; Chen, W.; Chen, X.; Li, G. Revealing Disparities in Different Types of Park Visits Based on Cellphone Signaling Data in Guangzhou, China. J. Environ. Manag. 2024, 351, 119969. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Wu, J.; Xiao, J.; Li, X.; Liao, S.; Chen, W. Spatially Explicit Carbon Emissions by Remote Sensing and Social Sensing. Environ. Res. 2023, 221, 115257. [Google Scholar] [CrossRef]
- Shi, H.; Yu, L.; Xu, Y.; Liu, Y.; Zhao, M. The Impact of the Streetscape Built Environment on Recreation Satisfaction: A Case Study of Guangzhou. J. Transp. Geogr. 2023, 112, 103702. [Google Scholar] [CrossRef]
- Guangzhou Municipal Government. Work Plan for the Allocation of AED in Public Places of Guangzhou (Draft for Comment); Guangzhou Municipal Government: Guangzhou, China, 2021.
- Liao, S.; Gao, F.; Feng, L.; Wu, J.; Wang, Z.; Chen, W. Observed Equity and Driving Factors of Automated External Defibrillators: A Case Study Using WeChat Applet Data. ISPRS Int. J. Geo-Inf. 2023, 12, 444. [Google Scholar] [CrossRef]
- Valenzuela, T.D.; Roe, D.J.; Nichol, G.; Clark, L.L.; Spaite, D.W.; Hardman, R.G. Outcomes of Rapid Defibrillation by Security Officers after Cardiac Arrest in Casinos. N. Engl. J. Med. 2000, 343, 1206–1209. [Google Scholar] [CrossRef] [PubMed]
- Gundry, J.W.; Comess, K.A.; DeRook, F.A.; Jorgenson, D.; Bardy, G.H. Comparison of Naive Sixth-Grade Children with Trained Professionals in the Use of an Automated External Defibrillator. Circulation 1999, 100, 1703–1707. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C.Y.; Demirtas, D.; Kwon, R.H. Optimizing the Deployment of Public Access Defibrillators. Manag. Sci. 2016, 62, 3617–3635. [Google Scholar] [CrossRef]
- Jin, X.; Bolt, G.; Hooimeijer, P. Africans in Guangzhou: Is the Ethnic Enclave Model Applicable in the Chinese Context? Cities 2021, 117, 103320. [Google Scholar] [CrossRef]
- Liu, Y.; Li, Z.; Breitung, W. The Social Networks of New-Generation Migrants in China’s Urbanized Villages: A Case Study of Guangzhou. Habitat Int. 2012, 36, 192–200. [Google Scholar] [CrossRef]
- Zhou, S.; Xie, M.; Kwan, M.-P. Ageing in Place and Ageing with Migration in the Transitional Context of Urban China: A Case Study of Ageing Communities in Guangzhou. Habitat Int. 2015, 49, 177–186. [Google Scholar] [CrossRef]
- Deng, X.; Liu, Y.; Gao, F.; Liao, S.; Zhou, F.; Cai, G. Spatial Distribution and Mechanism of Urban Occupation Mixture in Guangzhou: An Optimized GeoDetector-Based Index to Compare Individual and Interactive Effects. IJGI 2021, 10, 659. [Google Scholar] [CrossRef]
- Deasy, C.; Bray, J.E.; Smith, K.; Harriss, L.R.; Bernard, S.A.; Cameron, P. Out-of-Hospital Cardiac Arrests in the Older Age Groups in Melbourne, Australia. Resuscitation 2011, 82, 398–403. [Google Scholar] [CrossRef]
- Su, Y.-J.; Lai, Y.-C.; Chen, C.-C.; Chang, W.-H. Out-of-hospital cardiac arrest in the elderly. Int. J. Gerontol. 2008, 2, 67–71. [Google Scholar] [CrossRef]
- Li, S.; Lyu, D.; Huang, G.; Zhang, X.; Gao, F.; Chen, Y.; Liu, X. Spatially Varying Impacts of Built Environment Factors on Rail Transit Ridership at Station Level: A Case Study in Guangzhou, China. J. Transp. Geogr. 2020, 82, 102631. [Google Scholar] [CrossRef]
- Gao, F.; Li, S.; Tan, Z.; Zhang, X.; Lai, Z.; Tan, Z. How Is Urban Greenness Spatially Associated with Dockless Bike Sharing Usage on Weekdays, Weekends, and Holidays? IJGI 2021, 10, 238. [Google Scholar] [CrossRef]
- Fotheringham, A.; Brunsdon, C.F.; Charlton, M. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Deng, X.; Gao, F.; Liao, S.; Li, S. Unraveling the Association between the Built Environment and Air Pollution from a Geospatial Perspective. J. Clean. Prod. 2023, 386, 135768. [Google Scholar] [CrossRef]
- Chen, G.; Wang, C.C.; Jin, P.; Xia, B.; Xiao, L.; Chen, S.; Luo, J. Evaluation of Healthcare Inequity for Older Adults: A Spatio-Temporal Perspective. J. Transp. Health 2020, 19, 100911. [Google Scholar] [CrossRef]
- Steels, S. Key Characteristics of Age-Friendly Cities and Communities: A Review. Cities 2015, 47, 45–52. [Google Scholar] [CrossRef]
- Liu, L.; Feng, J.; Ren, F.; Xiao, L. Examining the Relationship between Neighborhood Environment and Residential Locations of Juvenile and Adult Migrant Burglars in China. Cities 2018, 82, 10–18. [Google Scholar] [CrossRef]
- Ouyang, W.; Wang, B.; Tian, L.; Niu, X. Spatial Deprivation of Urban Public Services in Migrant Enclaves under the Context of a Rapidly Urbanizing China: An Evaluation Based on Suburban Shanghai. Cities 2017, 60, 436–445. [Google Scholar] [CrossRef]
- Huang, G.; Xue, D.; Guo, Y.; Wang, C. Constrained Voluntary Informalisation: Analysing Motivations of Self-Employed Migrant Workers in an Urban Village, Guangzhou. Cities 2020, 105, 102760. [Google Scholar] [CrossRef]
- Tian, L.; Yao, Z.; Fan, C.; Zhou, L. A Systems Approach to Enabling Affordable Housing for Migrants through Upgrading Chengzhongcun: A Case of Xiamen. Cities 2020, 105, 102186. [Google Scholar] [CrossRef]
- Feero, S.; Hedges, J.R.; Stevens, P. Demographics of Cardiac Arrest: Association with Residence in a Low-Income Area. Acad. Emerg. Med. 1995, 2, 11–16. [Google Scholar] [CrossRef]
- Jonsson, M.; Härkönen, J.; Ljungman, P.; Nordberg, P.; Ringh, M.; Hirlekar, G.; Rawshani, A.; Herlitz, J.; Ljung, R.; Hollenberg, J. Inequalities in Income and Education Are Associated with Survival Differences After Out-of-Hospital Cardiac Arrest: Nationwide Observational Study. Circulation 2021, 144, 1915–1925. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Li, S.; Tan, Z.; Wu, Z.; Zhang, X.; Huang, G.; Huang, Z. Understanding the Modifiable Areal Unit Problem in Dockless Bike Sharing Usage and Exploring the Interactive Effects of Built Environment Factors. Int. J. Geogr. Inf. Sci. 2021, 35, 1905–1925. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Variables | Explanation | Mean | SD |
|---|---|---|---|---|
| Social groups | Young residents (YR) | Proportion of residents aged 19–45 (%) | 31.57 | 0.05 |
| Middle-aged residents (MR) | Proportion of residents aged 46–60 (%) | 14.37 | 0.04 | |
| Elderly residents (ER) | Proportion of residents aged above 60 (%) | 10.25 | 0.06 | |
| Young immigrants (YI) | Proportion of immigrants aged 19–45 (%) | 18.46 | 0.09 | |
| Middle-aged immigrants (MI) | Proportion of immigrants aged 46–60 (%) | 6.31 | 0.03 | |
| Elderly immigrants (EI) | Proportion of immigrants aged above 60 (%) | 2.34 | 0.02 | |
| Control variables | Population density (POP) | Population density (person/km2) | 27,512.36 | 29,854.67 |
| Road density (RD) | Road density (km/ km2) | 6.72 | 7.03 |
| Categories | Variables | Coefficient | Robust SE | Robust t | Robust P | VIF |
|---|---|---|---|---|---|---|
| Intercept | 0.979 | 0.030 | 32.441 | 0.000 | - | |
| Social groups | YR | −0.122 | 0.028 | −4.369 | 0.000 | 1.807 |
| ER | 0.689 | 0.054 | 12.832 | 0.000 | 2.304 | |
| YI | 0.519 | 0.054 | 9.572 | 0.000 | 2.175 | |
| MI | −0.303 | 0.033 | −9.177 | 0.000 | 1.494 | |
| EI | 0.205 | 0.083 | 2.481 | 0.013 | 1.311 | |
| Control variables | POP | 0.674 | 0.002 | 10.689 | 0.000 | 1.407 |
| RD | 0.536 | 0.003 | 9.974 | 0.000 | 1.032 | |
| Model diagnostics | R2: 0.336, adjusted R2: 0.324, AICc: −3752.491, Koenker (BP): 178.213 **, Jarque–Bera: 402.121 ** | |||||
| Categories | Variables | Min | Max | Mean | SD |
|---|---|---|---|---|---|
| Intercept | −0.011 | 2.511 | 1.253 | 0.031 | |
| Social groups | YR | −0.279 | 0.919 | 0.329 | 0.067 |
| ER | −0.196 | 1.147 | 0.186 | 0.290 | |
| YI | −1.294 | 0.497 | −0.434 | 0.108 | |
| MI | −0.211 | 0.046 | −0.077 | 0.060 | |
| EI | −0.568 | 0.520 | −0.140 | 0.054 | |
| Control variables | POP | 0.105 | 0.684 | 0.489 | 0.347 |
| RD | 0.078 | 0.541 | 0.414 | 0.607 | |
| Model diagnostics | R2: 0.724, adjusted R2: 0.702, AICc: −3856.174, bandwidth: 24,247.853 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, F.; Lu, S.; Liao, S.; Chen, W.; Chen, X.; Wu, J.; Wu, Y.; Li, G.; Han, X. AED Inequity among Social Groups in Guangzhou. ISPRS Int. J. Geo-Inf. 2024, 13, 140. https://doi.org/10.3390/ijgi13040140
Gao F, Lu S, Liao S, Chen W, Chen X, Wu J, Wu Y, Li G, Han X. AED Inequity among Social Groups in Guangzhou. ISPRS International Journal of Geo-Information. 2024; 13(4):140. https://doi.org/10.3390/ijgi13040140
Chicago/Turabian StyleGao, Feng, Siyi Lu, Shunyi Liao, Wangyang Chen, Xin Chen, Jiemin Wu, Yunjing Wu, Guanyao Li, and Xu Han. 2024. "AED Inequity among Social Groups in Guangzhou" ISPRS International Journal of Geo-Information 13, no. 4: 140. https://doi.org/10.3390/ijgi13040140
APA StyleGao, F., Lu, S., Liao, S., Chen, W., Chen, X., Wu, J., Wu, Y., Li, G., & Han, X. (2024). AED Inequity among Social Groups in Guangzhou. ISPRS International Journal of Geo-Information, 13(4), 140. https://doi.org/10.3390/ijgi13040140