

Assessment of Climate Risks, Vulnerability of Urban Health Systems, and Individual Adaptation Strategies in the City of N’Djaména (Chad)

 ,
,
Abstract
:1. Introduction
- Show the urban climatic risks and their impacts on the health systems of the city of N’Djaména;
- List the vulnerability factors relating to city dwellers and health systems (health infrastructure, health personnel, living environment, and human health) in the city of N’Djaména;
- List adaptation and resilience strategies used at the individual level to facilitate recommendations for a kind of urban planning that takes into account the resilience of health systems.
2. Literature Review
2.1. Vulnerability of Health Systems and Impacts of Climate Risks
2.2. Adaptation and Resilience of Healthcare Systems and Individuals
3. Materials and Methods
3.1. Study Area
3.2. Sampling and Data Used
- −
- Socio-economic characteristics (gender);
- −
- Onset of recurrent diseases and season of onset;
- −
- Vulnerability factors as perceived by city dwellers;
- −
- Coping strategies used by populations in the face of climate-related diseases.
3.3. Data Processing and Analysis
3.3.1. Pettitt Homogeneity Test
3.3.2. Mann–Kendall Trend Test
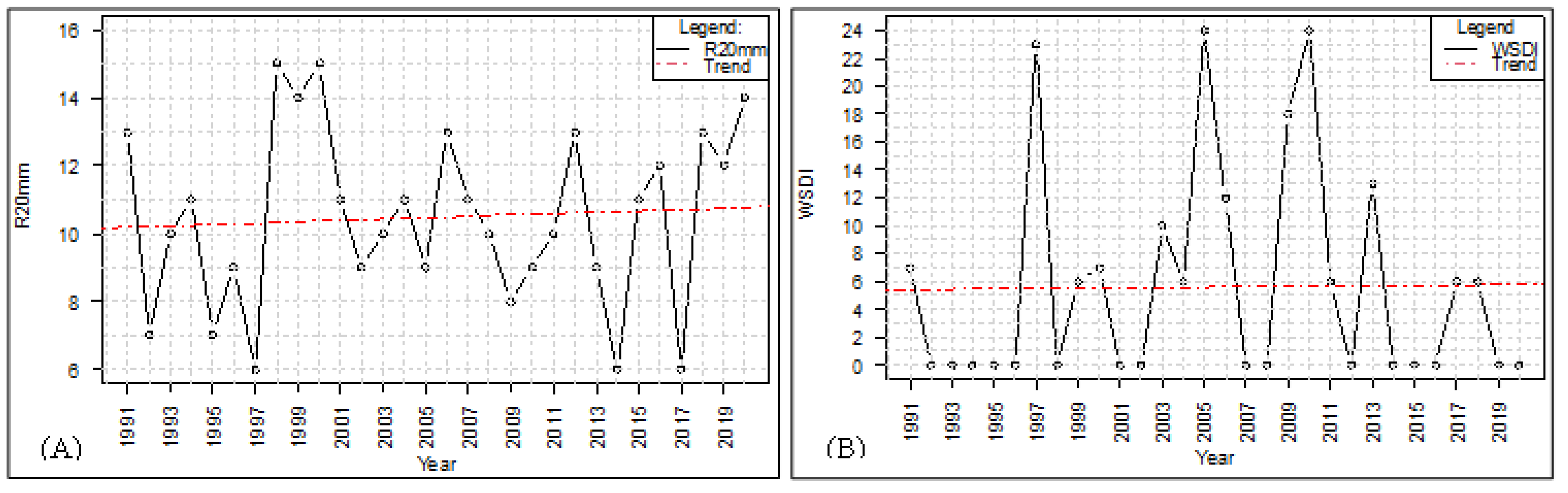
- WSDI represents the annual totals of days with at least six consecutive days of maximum temperatures above the 90th percentile. This index is an indicator of heat waves.
- R20 designates the total number of days with precipitation greater than or equal to 20 mm. This index is used to identify intense precipitation events.
- SPI, the standardized precipitation index, is used to assess the interannual variability of time series as well as periods of rainfall deficits and surpluses.
4. Results
4.1. Precipitation Risk Analysis
4.2. Analysis of Climatic Extremes
4.3. Wind Speed Dynamics
4.4. Impacts of Climate Change on Health Components
4.4.1. Impacts of Flooding on Health Facilities, Living Environment, and Food Supply
4.4.2. Impacts of Rising Temperatures on Living Conditions and Diet
4.4.3. Impacts of High Winds on Food and Institutional Health Governance
4.5. Perception of the Seasons in Which the Most Recurrent Diseases Appear
4.6. Vulnerability Factors
4.7. Coping Strategies Used by Local Populations
5. Discussion
5.1. Climate Risks, Vulnerability, and Impacts on the Healthcare Sector
5.2. Impacts of Climate Risks on Healthcare Systems
5.3. Vulnerability and Sources of Fragility in Healthcare Systems
5.4. Individual and Institutional Coping Strategies
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ebi, K.L.; Barrio, M.O.D. Lessons Learned on Health Adaptation to Climate Variability and Change: Experiences across Low- and Middle-Income Countries. Environ. Health Perspect. 2017, 125, 065001. [Google Scholar] [CrossRef]
- Nhamo, G.; Agyepong, A.O. Climate change adaptation and local government: Institutional complexities surrounding Cape Town’s Day Zero. J. Disaster Risk Stud. 2019, 11, 717. [Google Scholar] [CrossRef]
- IPCC, WGII, Sixth Assessment, Chapter 6. 2022. Available online: https://www.ipcc.ch/report/ar6/wg2/ (accessed on 30 October 2023).
- ClimaHealth. Opinion: Protection from Climate Change Requires Strong Health Systems, Maddie West & Joy Shumake-Guillemot, WMO-WHO Joint Office for Climate and Health. 2023. Available online: https://climahealth.info/opinion-protection-from-climate-change-requires-strong-health-systems/ (accessed on 24 October 2023).
- Verisk Maplecroft 2016. Climate Change Vulnerability 2017. Available online: https://reliefweb.int/report/world/climate-change-vulnerability-index-2017 (accessed on 2 November 2023).
- Abdoulay, M.; Julius, T.N.; Paul, N. Variabilité climatique au Tchad: Perception et stratégie d’adaptation paysanne à Kélo (Tchad). Rev. Electron. Sci. L’environnement VertigO 2022, 22, 1–17. [Google Scholar]
- Baohoutou, L. Les Précipitations en Soudanienne Tchadienne Durant les Quatre Dernières (1960–1999): Variabilités et Impacts. Ph.D. Thesis, Université de Nice, Nice, France, 2007; 245p. [Google Scholar]
- Bedoum, A.; Clobite, B.; Mbanghoguinan, A.; Issak, B.L. Impact de la variabilité pluviométrique et de la sécheresse au sud du Tchad: Effets du changement climatique. Rev. Ivoir. Sci. Technol. 2014, 23, 13–30. [Google Scholar]
- Kitoto, O.A.P. Réchauffement climatique et migration vers les rives du lac Tchad. Migr. Soc. 2016, 163, 149–166. [Google Scholar]
- République du Tchad. Contribution Déterminée au Niveau National Actualisée (CDN Actualisée Tchad); Ministère de l’Environnement, de la Pêche et du Développement Durable: N’Djaména, Chad, 2021; 50p. [Google Scholar]
- WHO. Checklists to Assess Vulnerabilities in Health Care Facilities in the Context of Climate Change; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Dumenu, W.K.; Obeng, E.A. Climate Change and Rural Communities in Ghana: Social Vulnerability, Impacts, Adaptations and Policy Implications. Environ. Sci. Policy 2016, 55, 208–217. [Google Scholar] [CrossRef]
- Peirce, A.M.; Espira, L.M.; Larson, P.S. Climate Change-Related Catastrophic Rainfall Events and Non-Communicable Respiratory Disease: A Systematic Review of the Literature. Climate 2022, 10, 101. [Google Scholar] [CrossRef]
- Lala, B.; Hagishima, A. Impact of Escalating Heat Waves on Students’ Well-Being and Overall Health: A Survey of Primary School Teachers. Climate 2023, 11, 126. [Google Scholar] [CrossRef]
- Ashrafuzzaman, M.; Gomes, C.; Guerra, J. The Changing Climate Is Changing Safe Drinking Water, Impacting Health: A Case in the Southwestern Coastal Region of Bangladesh (SWCRB). Climate 2023, 11, 146. [Google Scholar] [CrossRef]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Hetcheli, F.; Dandonougbo, I.; Biakouye, A.K. Du village à l’espace périurbain: Mutations socio-économiques du canton d’Adétikopé, un territoire sous influence de Lomé (Togo). In Revue NOTES SCIENTIFIQUES Homme et Société; Numéro Spécial; Université de Lomé: Lomé, Togo, 2017; pp. 311–334. [Google Scholar]
- Chersich, M.F.; Wright, C.Y. Climate change adaptation in South Africa: A case study on the role of the health sector. Glob. Health 2019, 15, 22. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.E.; Brown, C.L.; Conlon, K.; Herring, S.; Kunkel, K.E.; Lawrimore, J.; Luber, G.; Schreck, C.; Smith, A.; Uejio, C. Changes in extreme events and the potential impacts on human health. J. Air Waste Manag. Assoc. 2018, 68, 265–287. [Google Scholar] [CrossRef] [PubMed]
- Herslund, L.B.; Jalayer, F.; Jean-Baptiste, N.; Jorgensen, G.; Kabisch, S.; Kombe, W.; Lindley, S.; Nyed, P.K.; Pauleit, S.; Printz, A.; et al. A multi-dimensional assessment of urban vulnerability to climate change in Sub-Saharan Africa. Nat. Hazards 2015, 82, 149–172. [Google Scholar] [CrossRef]
- Allarané, N.; Azagoun, V.V.A.; Atchadé, A.J.; Hetcheli, F.; Atela, J. Urban Vulnerability and Adaptation Strategies against Recurrent Climate Risks in Central Africa: Evidence from N’Djaména City (Chad). Urban Sci. 2023, 7, 97. [Google Scholar] [CrossRef]
- Jamali, A.; Robati, M.; Nikoomaram, H.; Farsad, F.; Aghamohammadi, H. Urban Resilience and Climate Change: Developing a Multidimensional Index to Adapt against Climate Change in the Iranian Capital City of Tehran. Urban Sci. 2023, 7, 7. [Google Scholar] [CrossRef]
- Ezzati, F.; Mosadeghrad, A.M.; Jaafaripooyan, E. Resiliency of the Iranian healthcare facilities against the COVID-19 pandemic: Challenges and solutions. BMC Health Serv. Res. 2023, 23, 207. [Google Scholar] [CrossRef] [PubMed]
- Xie, E.; Howard, C.; Buchman, S.; Miller, F.A. Acting on climate change for a healthier future: Critical role for primary care in Canada. Can. Fam. Physician 2021, 67, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.M.; Isfahani, P.; Eslambolchi, L.; Zahmatkesh, M.; Afshari, M. Strategies to strengthen a climate-resilient health system: A scoping review. Glob. Health 2023, 19, 62. [Google Scholar]
- Green, M.S.; Pri-Or, N.G.; Capeluto, G.; Epstein, Y.; Paz, S. Climate change and health in Israel: Adaptation policies for extreme weather events. Isr. J. Health Policy Res. 2013, 2, 23. [Google Scholar] [CrossRef]
- WHO. WHO Guidance for Climate-Resilient and Environmentally Sustainable Health Care Facilities; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kjellstrom, T.; Briggs, D.; Freyberg, C.; Lemke, B.; Otto, M.; Hyatt, O. Heat, Human Performance, and Occupational Health: A Key Issue for the Assessment of Global Climate Change Impacts. Annu. Rev. Public Health 2016, 37, 97–112. [Google Scholar] [CrossRef]
- WHO. Operational Framework for Building Climate Resilient Health Systems; World Health Organisation: Geneva, Switzerland, 2015; 56p, Available online: https://apps.who.int/iris/bitstream/handle/10665/189951/9789241565073_eng.pdf (accessed on 4 November 2023).
- Noubayamal, D.E. Vers une Ville-Verte: Proposition du Projet de Développement Urbain de la Commune du 9e Arrondissement de N’Djaména (Tchad). Master’s Thesis, EAMAU, Lomé, Togo, 2018; 195p. [Google Scholar]
- INSEED. Deuxième Recensement Général de la Population et de l’Habitat; Résultats Globaux: N’Djaména, Tchad, 2009; 87p. [Google Scholar]
- Hassane, M.H.; Mahamat, H.A.; Danvidé, T.B. Analyse du processus d’extension de la ville de N’Djamena au Tchad (1900–2018). Geo-Eco-Trop 2021, 45, 507–516. [Google Scholar]
- Pettitt, A. A Non-Parametric Approach to the Change-Point Problem. J. R. Stat. Soc. 1979, 28, 126–135. [Google Scholar] [CrossRef]
- Buishand, T.A. Tests for detecting a shift in the mean of hydrological time series. J. Hydrol. 1984, 73, 51–69. [Google Scholar] [CrossRef]
- Das, S.; Banerjee, S. Investigations of changes in seasonal streamflow and sediment load in the Subarnarekha-Burhabalang basins using Mann-Kendall and Pettitt tests. Arab. J. Geosci. 2021, 14, 946. [Google Scholar] [CrossRef]
- Sneyers, R. Sur l’analyse statistique des séries d’observations. In Note Technique; n°143, OMM-N°415; OMM: Genève, Switzerland, 1975; 192p. [Google Scholar]
- Zhang, X.; Yang, F. RClimDex (1.0) User Manual; Climate Research Branch Environment Canada: Toronto, ON, Canada, 2004; 23p.
- Mckee, T.B.; Doesken, N.J.; Kleist, J. The relationship of drought frequency and duration to time scales. In Proceedings of the Eighth Conference on Applied Climatology, Anaheim, CA, USA, 17–22 January 1993. [Google Scholar]
- OMM. Guide d’Utilisation de l’Indice de Précipitation Normalisé; OMM-N°1090; OMM: Geneva, Switzerland, 2012; 25p. [Google Scholar]
- Hlahla, S.; Hill, T.R. Responses to Climate Variability in Urban Poor Communities in Pietermaritzburg, Kwazulu-Natal, South Africa. Sage Open 2018, 8, 2158244018800914. [Google Scholar] [CrossRef]
- MEPDD. Troisième Communication Nationale (TCN) du Tchad sur les Changements Climatiques; Ministère de l’Environnement, de la Pêche et du Développement Durable: N’Djaména, Chad, 2020; 103p. [Google Scholar]
- Atchadé, A.J.; Kanda, M.; Folega, F.; Atela, J.; Dourma, M.; Wala, K.; Akpagana, K. Urban Ecosystem Services and Determinants of Stakeholders’ Perception for Sustainable Cities Planning in Cotonou (Benin). Sustainability 2023, 15, 9424. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N’Djaména | Number of Respondents | Percentage (%) |
|---|---|---|
| 1er arrondissement | 26 | 8 |
| 2e arrondissement | 26 | 8 |
| 3e arrondissement | 16 | 4 |
| 4e arrondissement | 29 | 9 |
| 5e arrondissement | 35 | 11 |
| 6e arrondissement | 20 | 6 |
| 7e arrondissement | 70 | 21 |
| 8e arrondissement | 57 | 17 |
| 9e arrondissement | 27 | 8 |
| 10e arrondissement | 27 | 8 |
| Total | 333 | 100 |
| SPI Class | Dryness/Humidity Ratio |
|---|---|
| 2.0 and more | Extremely damp |
| 1.5 to 1.99 | Very damp |
| 1.0 to 1.49 | Moderately damp |
| −0.99 to 0.99 | Near normal |
| −1.0 to −1.49 | Moderately dry |
| −1.5 to −1.99 | Very dry |
| −2 and less | Extremely dry |
| Climate Risks | Health Components | |||
|---|---|---|---|---|
| Health Facilities | Living Environment | Food | Institutional Health Governance | |
| Flooding |
|
|
|
|
| Heat waves |
|
|
|
|
| Strong winds |
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allarané, N.; Atchadé, A.J.; Azagoun, V.V.A.; Houngnigbe, A.I.; Gouataine Seingue, R.; N’Dilbé, T.-R.; Hetcheli, F. Assessment of Climate Risks, Vulnerability of Urban Health Systems, and Individual Adaptation Strategies in the City of N’Djaména (Chad). Climate 2024, 12, 5. https://doi.org/10.3390/cli12010005
Allarané N, Atchadé AJ, Azagoun VVA, Houngnigbe AI, Gouataine Seingue R, N’Dilbé T-R, Hetcheli F. Assessment of Climate Risks, Vulnerability of Urban Health Systems, and Individual Adaptation Strategies in the City of N’Djaména (Chad). Climate. 2024; 12(1):5. https://doi.org/10.3390/cli12010005
Chicago/Turabian StyleAllarané, Ndonaye, Assouhan Jonas Atchadé, Vidjinnagni Vinasse Ametooyona Azagoun, Adanvo Isaac Houngnigbe, Romain Gouataine Seingue, Tob-Ro N’Dilbé, and Follygan Hetcheli. 2024. "Assessment of Climate Risks, Vulnerability of Urban Health Systems, and Individual Adaptation Strategies in the City of N’Djaména (Chad)" Climate 12, no. 1: 5. https://doi.org/10.3390/cli12010005