Seasonality of Discrepancies between Admission and Discharge Diagnosis for Medicare Patients



Abstract
1. Introduction
2. Terminologies
3. Materials and Methods
3.1. Data and Attributes
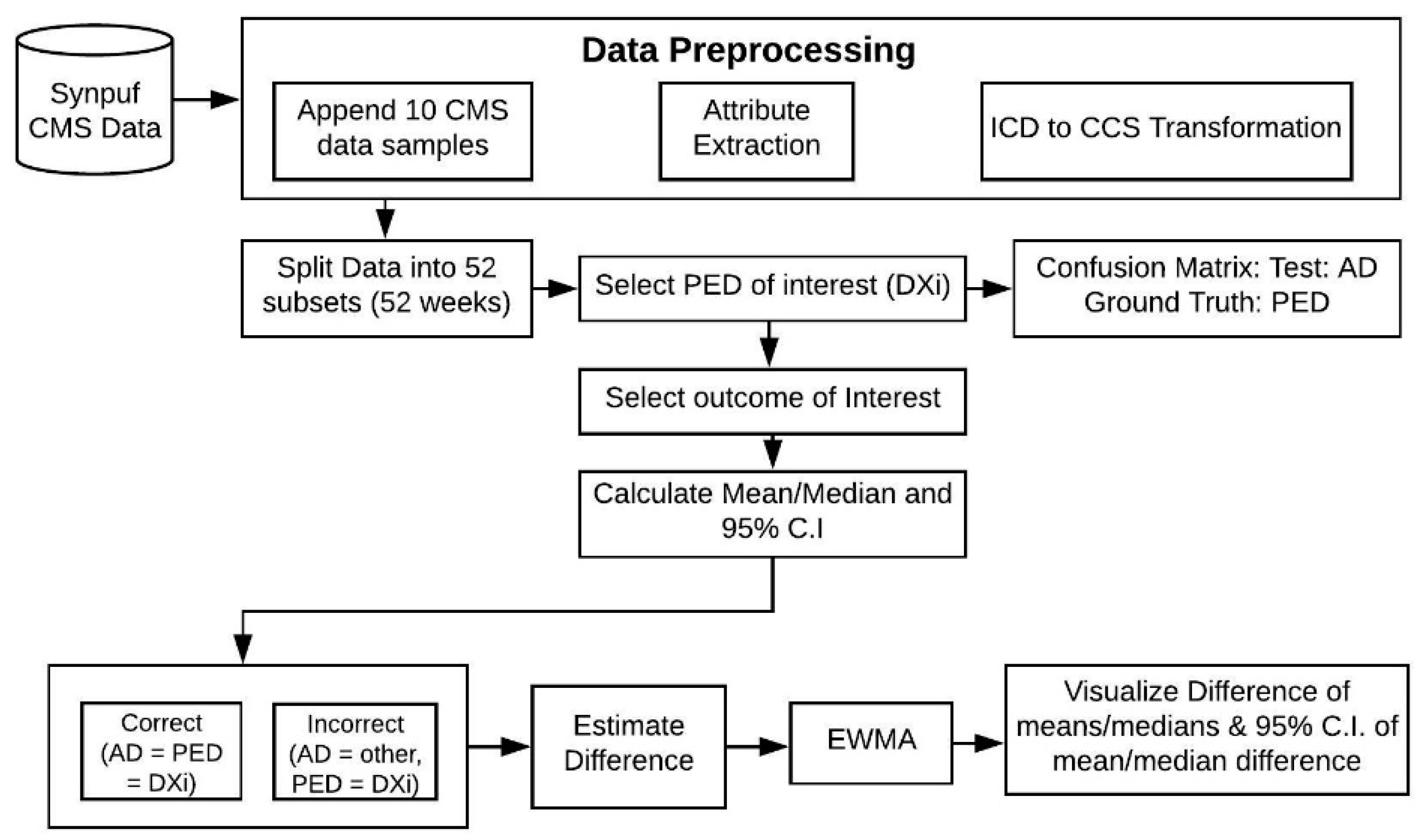
3.2. Methodological Framework
4. Results
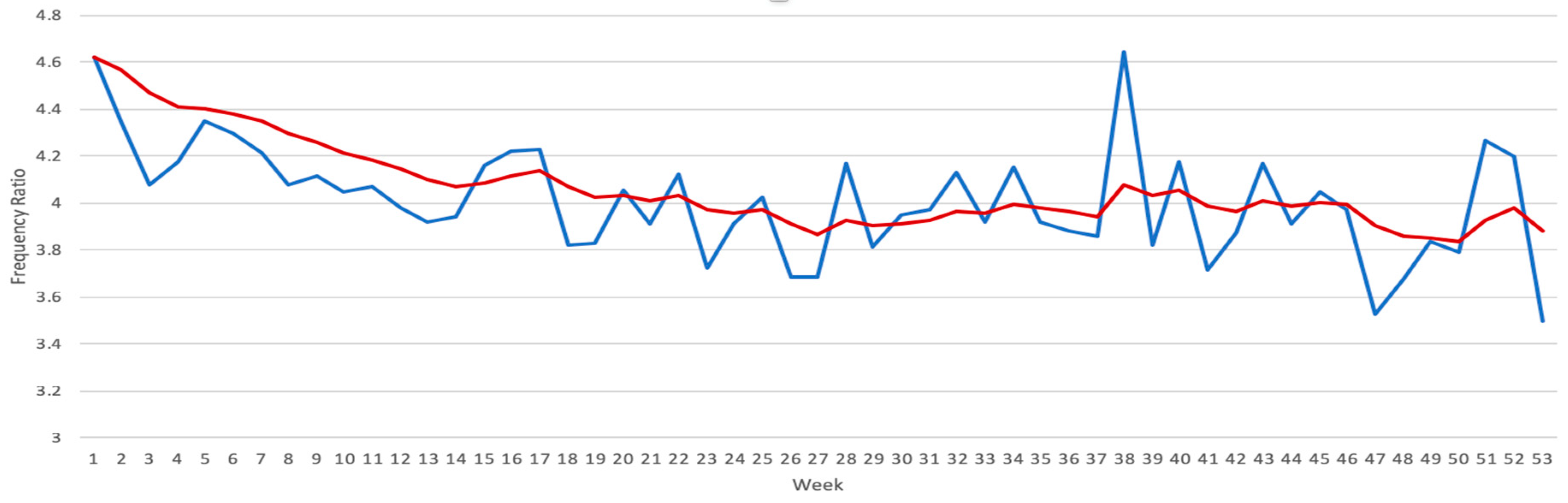
4.1. Seasonal Variations of Disease Frequency
4.2. Mismatch between Admission and Principal Exit Diagnosis
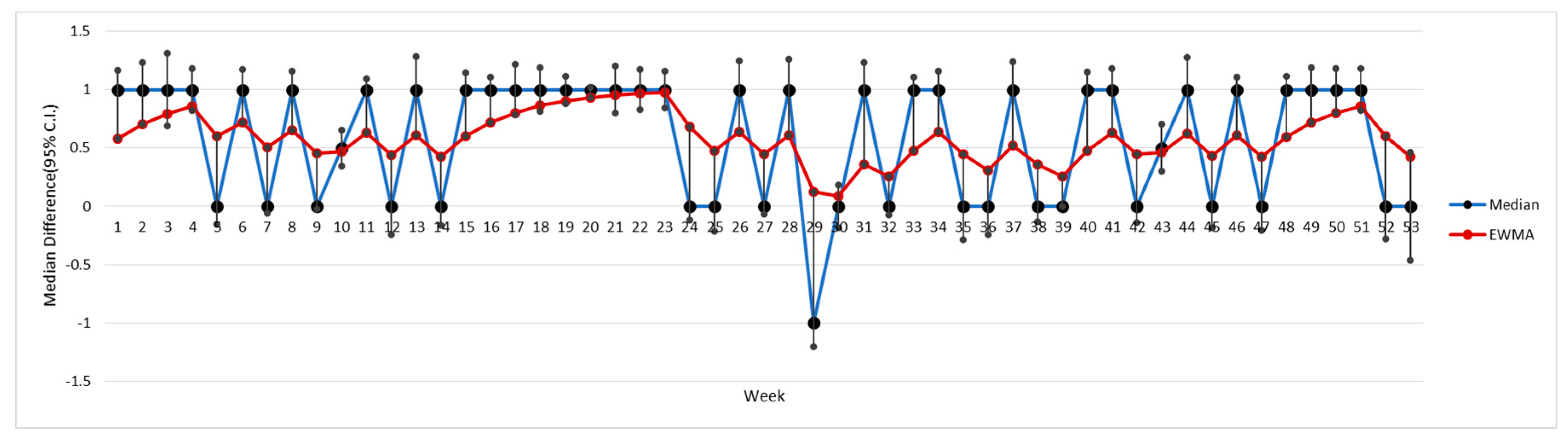
4.3. Seasonal Comparison of LOS between Correct–Incorrect Diagnoses
4.3.1. Example 1: Pneumonia
4.3.2. Example 2: Aneurysm
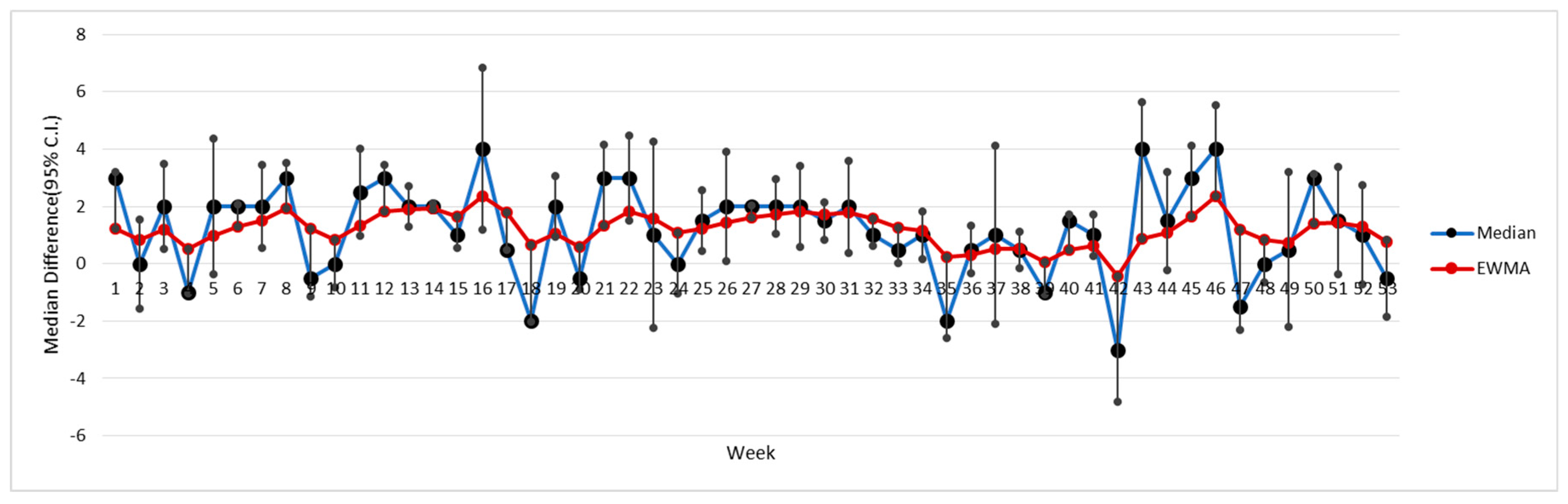
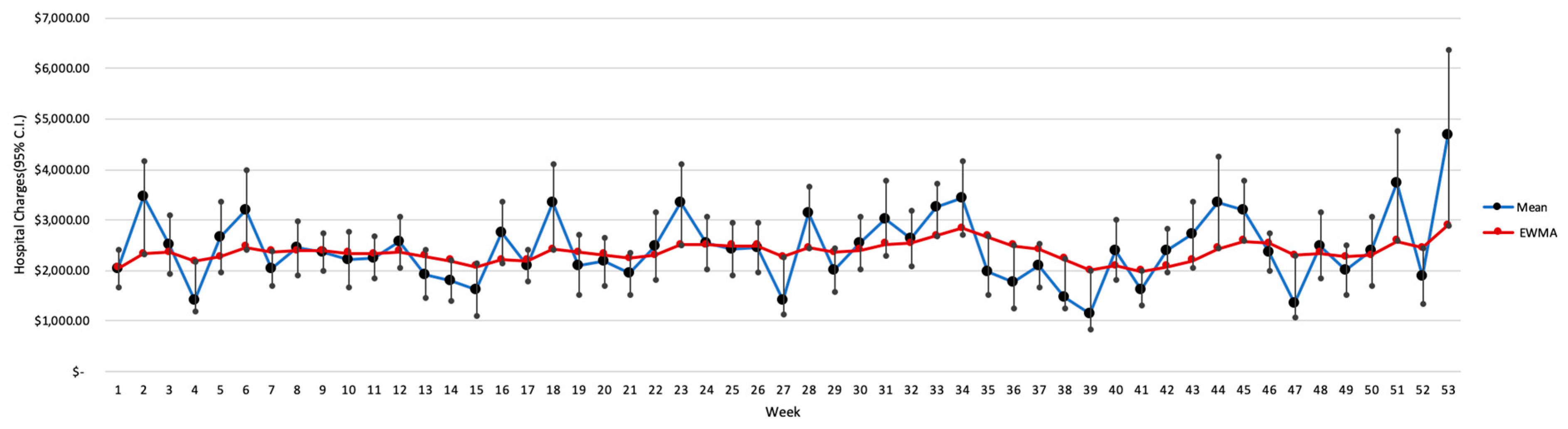
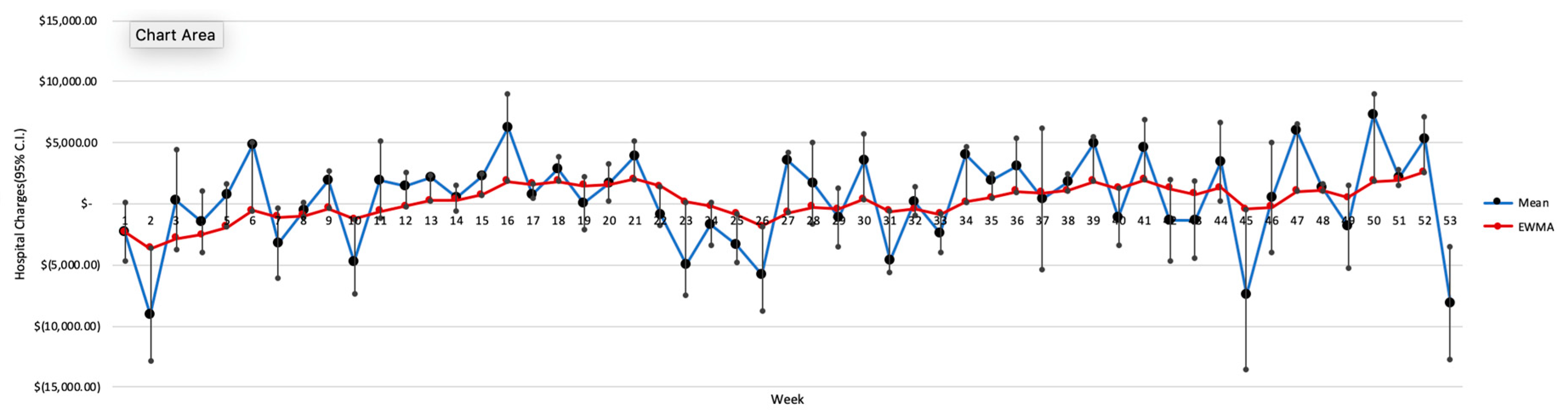
4.4. Seasonal Comparison of Charges between Correct–Incorrect Dxs
4.4.1. Example 1: Pneumonia
4.4.2. Example 2: Aneurysm
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Simpao, A.F.; Ahumada, L.M.; Rehman, M.A. Big data and visual analytics in anaesthesia and health care. Br. J. Anaesth. 2015, 115, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Raghupathi, W.; Raghupathi, V. Big data analytics in healthcare: Promise and potential. Health Inf. Sci. Syst. 2014, 2, 3. [Google Scholar] [CrossRef] [PubMed]
- Kucharska-Newton, A.M.; Heiss, G.; Ni, H.; Stearns, S.C.; Puccinelli-Ortega, N.; Wruck, L.M.; Chambless, L. Identification of Heart Failure Events in Medicare Claims: The Atherosclerosis Risk in Communities (ARIC) Study. J. Card. Fail. 2016, 22, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Estep, J.D.; Starling, R.C.; Horstmanshof, D.A.; Milano, C.A.; Selzman, C.H.; Shah, K.B.; Loebe, M.; Moazami, N.; Long, J.W.; Stehlik, J.; et al. ROADMAP Study Investigators Risk Assessment and Comparative Effectiveness of Left Ventricular Assist Device and Medical Management in Ambulatory Heart Failure Patients: Results from the ROADMAP Study. J. Am. Coll. Cardiol. 2015, 66, 1747–1761. [Google Scholar] [CrossRef] [PubMed]
- Rostomyan, L.; Daly, A.F.; Petrossians, P.; Nachev, E.; Lila, A.R.; Lecoq, A.-L.; Lecumberri, B.; Trivellin, G.; Salvatori, R.; Moraitis, A.G.; et al. Clinical and genetic characterization of pituitary gigantism: An international collaborative study in 208 patients. Endocr. Relat. Cancer 2015, 22, 745–757. [Google Scholar] [CrossRef] [PubMed]
- Fry, D.E.; Pine, M.; Nedza, S.M.; Locke, D.G.; Reband, A.M.; Pine, G. Risk-adjusted outcomes in Medicare inpatient nephrectomy patients. Medicine (Baltimore) 2016, 95, e4784. [Google Scholar] [CrossRef] [PubMed]
- Diagnosis Discrepancies and LOS|Journal of Hospital Medicine. Available online: https://www.journalofhospitalmedicine.com/jhospmed/article/127663/diagnosis-discrepancies-and-los (accessed on 2 November 2018).
- Leske, M.C.; Sorensen, A.A.; Zimmer, J.G. Discrepancies between admission and discharge diagnoses in a university hospital. Med. Care 1978, 16, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Daly, P.A.; Tu, J.V. A multicenter study of the coding accuracy of hospital discharge administrative data for patients admitted to cardiac care units in Ontario. Am. Heart J. 2002, 144, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Maude, J. Differential diagnosis: The key to reducing diagnosis error, measuring diagnosis and a mechanism to reduce healthcare costs. Diagnosis 2014, 1, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.J.; Hoffer, E.P.; Barnett, G.O.; Kim, R.J.; Famiglietti, K.T.; Chueh, H.C. Impact of a computer-based diagnostic decision support tool on the differential diagnoses of medicine residents. J. Grad. Med. Educ. 2012, 4, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Fegaras, L.; Zikos, D. Temporal Modification of Apriori to Find Seasonal Variations Between Symptoms and Diagnoses. In Proceedings of the 11th PErvasive Technologies Related to Assistive Environments Conference, PETRA’18, Corfu, Greece, 26–29 June 2018; ACM: New York, NY, USA, 2018; pp. 490–494. [Google Scholar]
- Healthcare Cost and Utilization Project. Clinical Classifications Software (CCS) for ICD-9-CM. Available online: https://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp (accessed on 1 November 2018).
- Johnson, T.; McNutt, R.; Odwanzy, R.; Patel, D.; Baker, S. Discrepancy between admission and discharge diagnoses as a predictor of hospital length of stay. J. Hosp. Med. 2009, 4, 234–239. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Organization International Classification of Diseases: 9th Revision, Basic Tabulation List with Alphabetic Index; World Health Organization: Geneva, Switzerland, 1978. [Google Scholar]
- UMLS Metathesaurus—CCS (Clinical Classifications Software)—Synopsis. Available online: https://www.nlm.nih.gov/research/umls/sourcereleasedocs/current/CCS/ (accessed on 2 November 2018).
- Centers for Medicare and Medicaid Services (CMS) Linkable 2008–2010 Medicare Data Entrepreneurs’ Synthetic Public Use File (DE-SynPUF). Available online: https://www.cms.gov/Research-Statistics-Data-and-Systems/Downloadable-Public-Use-Files/SynPUFs/DE_Syn_PUF.html (accessed on 1 November 2018).
- Aggarwal, R.; Ringold, S.; Khanna, D.; Neogi, T.; Johnson, S.R.; Miller, A.; Brunner, H.I.; Ogawa, R.; Felson, D.; Ogdie, A.; et al. Distinctions Between Diagnostic and Classification Criteria? Arthritis Care Res. (Hoboken) 2015, 67, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Sorknaes, A.D.; Madsen, H.; Hallas, J.; Jest, P.; Hansen-Nord, M. Nurse tele-consultations with discharged COPD patients reduce early readmissions—An interventional study. Clin. Respir. J. 2011, 5, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.I.; Alstadhaug, K.B.; Bekkelund, S.I. Acceptability, Feasibility, and Cost of Telemedicine for Nonacute Headaches: A Randomized Study Comparing Video and Traditional Consultations. J. Med. Internet Res. 2016, 18, e140. [Google Scholar] [CrossRef] [PubMed]
- Sakhnini, A.; Saliba, W.; Schwartz, N.; Bisharat, N. The derivation and validation of a simple model for predicting in-hospital mortality of acutely admitted patients to internal medicine wards. Medicine (Baltimore) 2017, 96, e7284. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SynPUF Attribute | Description | Comments |
|---|---|---|
| Admitting ICD-9 Diagnosis Code | Initial Dx code on the institutional claim indicating the beneficiary’s initial diagnosis at the time of admission, before any further patient investigation took place | Referred to as AD (Admission Diagnosis) |
| ICD-9 Diagnosis Code 1 | The beneficiary’s principal exit diagnosis. It typically represents the health problem that caused the need for hospitalization. This attribute is our ground truth | Referred to as PED (Principal Exit Diagnosis) |
| Claims Admission Date | The date the beneficiary was admitted to the hospital or skilled nursing facility | To calculate the length of stay (LOS, based on the discharge-admission dates) |
| Beneficiary Discharge Date | The date when the patient was discharged from the hospital | |
| Claim Payment Amount | The amount of payment made from the Medicare trust fund for the services covered by the claim record | The amount (USD) associated with the diagnostic-related groups |
| Discharge Dx | N | P (AD = PED) | Discharge Dx | N | P (AD = PED) |
|---|---|---|---|---|---|
| Congestive heart failure | 32,367 | 47.13 | Acute Cardiovasc. | 14,419 | 48.36 |
| Pneumonia | 29,619 | 52.20 | Fluid/electrolytes Dx | 12,784 | 45.43 |
| Osteoarthrosis | 23,870 | 72.26 | Respiratory failure | 12,458 | 43.30 |
| Dysrhythmia | 23,007 | 56.52 | Hip fracture | 12,316 | 44.85 |
| Chronic Obstr. Pulm. Disease | 20,680 | 45.18 | Acute renal failure | 12,051 | 36.32 |
| Coronary atheromatosis | 19,064 | 27.04 | Back problem | 11,207 | 74.82 |
| Rehabilitation | 17,324 | 82.87 | Chest pain | 11,170 | 81.34 |
| Medical Device Compl. | 16,526 | 25.09 | Skin infection | 10,220 | 68.80 |
| Urinary Tract Infection | 16,386 | 45.45 | Gastroint. hemorr. | 9750 | 71.74 |
| Acute Myocard. Infraction | 16,214 | 23.84 | Mood disorders | 9613 | 40.27 |
| Spring | Principal Exit DX | Fall | Principal Exit DX | ||||
| Pneumonia | Other | Pneumonia | Other | ||||
| Admission DX | Pneumonia | 4317 | 2912 | Admission DX | Pneumonia | 3399 | 2356 |
| Other Dx | 3989 | 17,3046 | Other Dx | 3161 | 140,855 | ||
| Summer | Principal Exit DX | Winter | Principal Exit Dx | ||||
| Pneumonia | Other | Pneumonia | Other | ||||
| Admission DX | Pneumonia | 3930 | 2715 | Admission DX | Pneumonia | 3816 | 2587 |
| Other Dx | 3771 | 163,843 | Other Dx | 3547 | 147,968 | ||
| Spring | Summer | Fall | Winter | |
|---|---|---|---|---|
| Recall [TP/(TP + FN)] | 0.5197 | 0.5103 | 0.5181 | 0.5183 |
| Precision [TP/(TP + FP)] | 0.5972 | 0.5914 | 0.5906 | 0.5960 |
| F-Score [2TP/(2TP + FP + FN)] | 0.5558 | 0.5479 | 0.5520 | 0.5544 |
| Spring | Principal Exit DX | Fall | Principal Exit DX | ||||
| Aneurysm | Other | Aneurysm | Other | ||||
| Admission DX | Aneurysm | 325 | 396 | Admission DX | Aneurysm | 229 | 275 |
| Other Dx | 447 | 183,096 | Other Dx | 347 | 148,920 | ||
| Summer | Principal Exit DX | Winter | Principal Exit Dx | ||||
| Aneurysm | Other | Aneurysm | Other | ||||
| Admission DX | Aneurysm | 274 | 340 | Admission DX | Aneurysm | 266 | 304 |
| Other Dx | 415 | 173,230 | Other Dx | 356 | 156,992 | ||
| Spring | Summer | Fall | Winter | |
|---|---|---|---|---|
| Recall [TP/(TP + FN)] | 0.4210 | 0.3977 | 0.3976 | 0.4277 |
| Precision [TP/(TP + FP)] | 0.4508 | 0.4463 | 0.4544 | 0.4667 |
| F-Score [2TP/(2TP + FP + FN)] | 0.4354 | 0.4206 | 0.4241 | 0.4463 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrestha, A.; Zikos, D.; Fegaras, L. Seasonality of Discrepancies between Admission and Discharge Diagnosis for Medicare Patients. Technologies 2018, 6, 111. https://doi.org/10.3390/technologies6040111
Shrestha A, Zikos D, Fegaras L. Seasonality of Discrepancies between Admission and Discharge Diagnosis for Medicare Patients. Technologies. 2018; 6(4):111. https://doi.org/10.3390/technologies6040111
Chicago/Turabian StyleShrestha, Aashara, Dimitrios Zikos, and Leonidas Fegaras. 2018. "Seasonality of Discrepancies between Admission and Discharge Diagnosis for Medicare Patients" Technologies 6, no. 4: 111. https://doi.org/10.3390/technologies6040111
APA StyleShrestha, A., Zikos, D., & Fegaras, L. (2018). Seasonality of Discrepancies between Admission and Discharge Diagnosis for Medicare Patients. Technologies, 6(4), 111. https://doi.org/10.3390/technologies6040111