
New Regenerative and Anti-Aging Medicine Approach Based on Single-Stranded Alpha-1 Collagen for Neo-Collagenesis Induction: Clinical and Instrumental Experience of a New Injective Polycomponent Formulation for Dermal Regeneration
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Patient Selection and Study Design
2.4. Evaluation
2.5. Injection Technique
2.6. Statistical Analysis
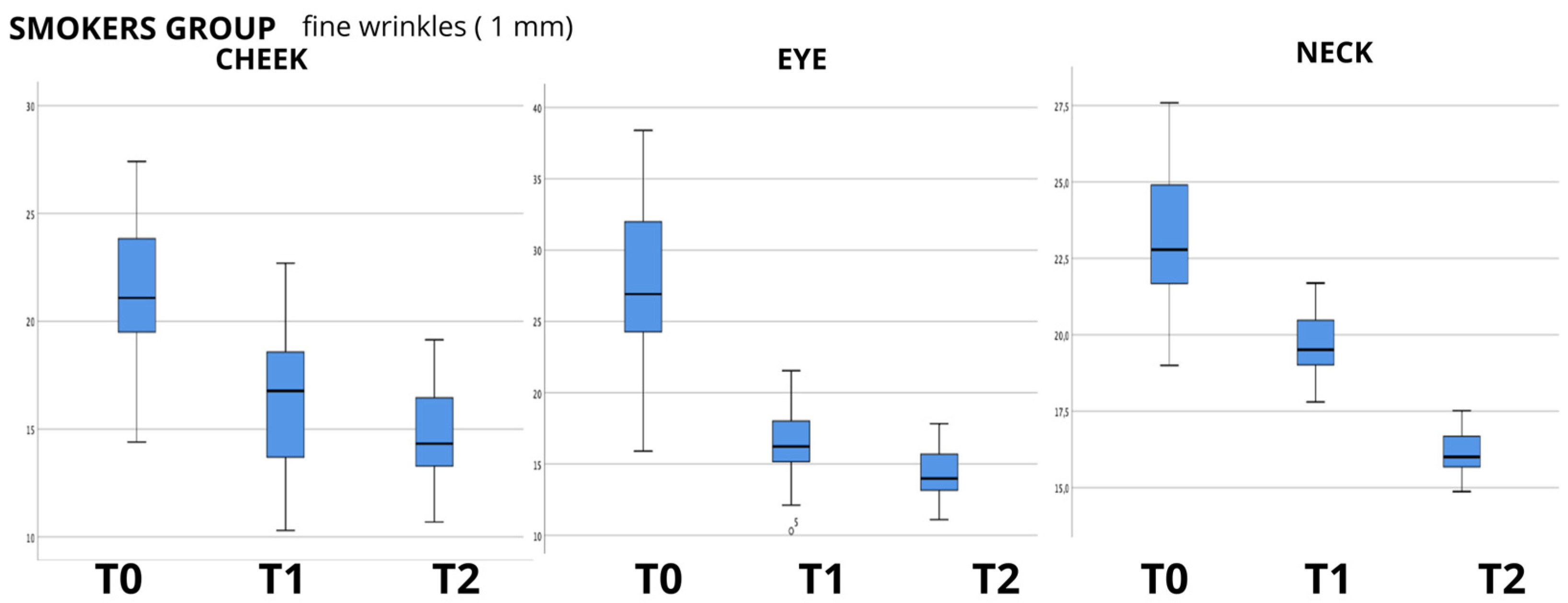
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shin, J.-W.; Kwon, S.-H.; Choi, J.-Y.; Na, J.-I.; Huh, C.-H.; Choi, H.-R.; Park, K.-C. Molecular Mechanisms of Dermal Aging and Antiaging Approaches. Int. J. Mol. Sci. 2019, 20, 2126. [Google Scholar] [CrossRef] [PubMed]
- Knapp, T.R.; Kaplan, E.N.; Daniels, J.R. Injectable collagen for soft tissue augmentation. Plast. Reconstr. Surg. 1977, 60, 398–405. [Google Scholar] [PubMed]
- Cooperman, L.S.; Mackinnon, V.; Bechler, G.; Pharriss, B.B. Injectable collagen: A six-year clinical investigation. Aesthetic Plast. Surg. 1985, 9, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.N.; Falces, E.; Tolleth, H. Clinical utilization of injectable collagen. Ann. Plast. Surg. 1983, 10, 437–451. [Google Scholar] [CrossRef] [PubMed]
- Watson, W.; Kaye, R.L.; Klein, A.; Stegman, S. Injectable collagen: A clinical overview. Cutis 1983, 31, 543–546. [Google Scholar] [PubMed]
- Augello, F.R.; Lombardi, F.; Artone, S.; Ciafarone, A.; Altamura, S.; Di Marzio, L.; Cifone, M.G.; Palumbo, P.; Giuliani, M.; Cinque, B. Evaluation of the Effectiveness of an Innovative Polycomponent Formulation on Adult and Aged Human Dermal Fibroblasts. Biomedicines 2023, 11, 2410. [Google Scholar] [CrossRef] [PubMed]
- Semkova, M.E.; Hsuan, J.J. TGFβ-1 Induced Cross-Linking of the Extracellular Matrix of Primary Human Dermal Fibroblasts. Int. J. Mol. Sci. 2021, 22, 984. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, F.V. Correction of age- and disease-related contour deficiencies of the face. Aesthetic Plast. Surg. 1985, 9, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Stegman, S.J.; Tromovitch, T.A. Implantation of collagen for depressed scars. J. Dermatol. Surg. Oncol. 1980, 6, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Burke, K.E.; Naughton, G.; Cassai, N. A histological, immunological, and electron microscopic study of bovine collagen implants in the human. Ann. Plast. Surg. 1985, 14, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Rapaport, M.J.; Salit, R.; Rivkin, L. Collagen injections for aging skin lines (wrinkles). J. Am. Acad. Dermatol. 1984, 11, 250–252. [Google Scholar] [CrossRef] [PubMed]
- Matti, B.A.; Nicolle, F.V. Clinical use of Zyplast in correction of age- and disease-related contour deficiencies of the face. Aesthetic Plast. Surg. 1990, 14, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Stegman, S.J.; Chu, S.; Armstrong, R.C. Adverse Reactions to Bovine Collagen Implant: Clinical and Histologic Features. J. Dermatol. Surg. Oncol. 1988, 14, 39–48. [Google Scholar] [CrossRef]
- Klein, A.W.; Elson, M.L. The history of substances for soft tissue augmentation. Dermatol. Surg. 2000, 26, 1096–1105. [Google Scholar] [CrossRef] [PubMed]
- Friedman, P.M.; Mafong, E.A.; Kauvar, A.N.B.; Geronemus, R.G. Safety data of injectable nonanimal stabilized hyaluronic acid gel for soft tissue augmentation. Dermatol. Surg. 2002, 28, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Messaraa, C.; Metois, A.; Walsh, M.; Hurley, S.; Doyle, L.; Mansfield, A.; O’Connor, C.; Mavon, A. Wrinkle and roughness measurement by the Antera 3D and its application for evaluation of cosmetic products. Skin Res. Technol. 2018, 24, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Linming, F.; Wei, H.; Anqi, L.; Yuanyu, C.; Heng, X.; Sushmita, P.; Yiming, L.; Li, L. Comparison of two skin imaging analysis instruments: The VISIA® from Canfield vs the ANTERA 3D® CS from Miravex. Skin Res. Technol. 2018, 24, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Pusic, A.L.; Klassen, A.F.; Scott, A.M.; Cano, S.J. Development and psychometric evaluation of the FACE-Q satisfaction with appearance scale: A new patient-reported outcome instrument for facial aesthetics patients. Clin. Plast. Surg. 2013, 40, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Klassen, A.F.; Cano, S.J.; Scott, A.M.; Pusic, A.L. Measuring outcomes that matter to face-lift patients: Development and validation of FACE-Q appearance appraisal scales and adverse effects checklist for the lower face and neck. Plast. Reconstr. Surg. 2014, 133, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Panchapakesan, V.; Klassen, A.F.; Cano, S.J.; Scott, A.M.; Pusic, A.L. Development and psychometric evaluation of the FACE-Q Aging Appraisal Scale and Patient-Perceived Age Visual Analog Scale. Aesthetic Surg. J. 2013, 33, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Klassen, A.F.; Cano, S.J.; Scott, A.; Snell, L.; Pusic, A.L. Measuring patient-reported outcomes in facial aesthetic patients: Development of the FACE-Q. Facial Plast. Surg. 2010, 26, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Narins, R.S.; Brandt, F.; Leyden, J.; Lorenc, Z.P.; Rubin, M.; Smith, S. A randomized, double-blind, multicenter comparison of the efficacy and tolerability of Restylane versus Zyplast for the correction of nasolabial folds. Dermatol. Surg. 2003, 29, 588–595. [Google Scholar] [CrossRef]
- Carruthers, A.; Carruthers, J. Scale Summit. Dermatol. Surg. 2008, 34 (Suppl. S2), S149. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, A.; Carruthers, J.; Hardas, B.; Kaur, M.; Goertelmeyer, R.; Jones, D.; Rzany, B.; Cohen, J.; Kerscher, M.; Flynn, T.C.; et al. A validated brow positioning grading scale. Dermatol. Surg. 2008, 34 (Suppl. S2), S150–S154. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, A.; Carruthers, J.; Hardas, B.; Kaur, M.; Goertelmeyer, R.; Jones, D.; Rzany, B.; Cohen, J.; Kerscher, M.; Flynn, T.C.; et al. A validated grading scale for forehead lines. Dermatol. Surg. 2008, 34 (Suppl. S2), S155–S160. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, A.; Carruthers, J.; Hardas, B.; Kaur, M.; Goertelmeyer, R.; Jones, D.; Rzany, B.; Cohen, J.; Kerscher, M.; Flynn, T.C.; et al. A validated grading scale for crow’s feet. Dermatol. Surg. 2008, 34 (Suppl. S2), S173–S178. [Google Scholar] [CrossRef]
- Carruthers, A.; Carruthers, J. A validated facial grading scale: The future of facial ageing measurement tools? J. Cosmet. Laser Ther. 2010, 12, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Messaraa, C.; Metois, A.; Walsh, M.; Flynn, J.; Doyle, L.; Robertson, N.; Mansfield, A.; O’Connor, C.; Mavon, A. Antera 3D capabilities for pore measurements. Skin Res. Technol. 2018, 24, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Shi, K.; Hong, L.; Zhao, J.; Yu, J. Antera 3D camera: A novel method for evaluating the therapeutic efficacy of fractional CO2 laser for surgical incision scars. J. Cosmet. Dermatol. 2018, 17, 1041–1045. [Google Scholar] [CrossRef] [PubMed]
- Hurley, S.; Messaraa, C.; O’Connor, C.; Metois, A.; Walsh, M.; Mc Namee, D.; Mansfield, A.; Robertson, N.; Doyle, L.; Mavon, A. DermaTOP Blue and Antera 3D as methods to assess cosmetic solutions targeting eyelid sagging. Skin Res. Technol. 2020, 26, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Ikuta, K.; Fukuoka, K.; Suyama, Y.; Morita, M.; Kimura, Y.; Umeda, R.; Kanayama, H.; Ohga, M.; Nakagaki, M.; Yagi, S. Comparison of Antera 3D® and TcPO2 for Evaluation of Blood Flow in Skin. Yonago Acta Med. 2023, 66, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Anqi, S.; Xiukun, S.; Ai’e, X. Quantitative evaluation of sensitive skin by ANTERA 3D® combined with GPSkin Barrier®. Skin Res. Technol. 2022, 28, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Matias, A.R.; Ferreira, M.; Costa, P.; Neto, P. Skin colour, skin redness and melanin biometric measurements: Comparison study between Antera® 3D, Mexameter® and Colorimeter®. Skin Res. Technol. 2015, 21, 346–362. [Google Scholar] [CrossRef] [PubMed]
- Knapp, T.R.; Luck, E.; Daniels, J.R. Behavior of solubilized collagen as a bioimplant. J. Surg. Res. 1977, 23, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Zeide, D.A. Adverse reactions to collagen implants. Clin. Dermatol. 1986, 4, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.P.; William Hanke, C.; Swanson, N.A. Dermal implants: Safety of products injected for soft tissue augmentation. J. Am. Acad. Dermatol. 1989, 21, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Choi, Y.S.; Kim, S.M.; Kim, Y.J.; Rhie, J.W.; Jun, Y.J. Efficacy and safety of porcine collagen filler for nasolabial fold correction in Asians: A prospective multicenter, 12 months follow-up study. J. Korean Med. Sci. 2014, 29 (Suppl. S3), S217–S221. [Google Scholar] [CrossRef] [PubMed]
- Charriere, G.; Bejot, M.; Schnitzler, L.; Ville, G.; Hartmann, D.J. Reactions to a bovine collagen implant. Clinical and immunologic study in 705 patients. J. Am. Acad. Dermatol. 1989, 21, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.-H.; Lee, Y.-J.; Rhie, J.-W.; Suh, D.-S.; Oh, D.-Y.; Lee, J.-H.; Kim, Y.-J.; Kim, S.-M.; Jun, Y.-J. Comparative study of the effectiveness and safety of porcine and bovine atelocollagen in Asian nasolabial fold correction. J. Plast. Surg. Hand Surg. 2015, 49, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Olenius, M. The first clinical study using a new biodegradable implant for the treatment of lips, wrinkles, and folds. Aesthetic Plast. Surg. 1998, 22, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Dover, J.; Monheit, G.; Narins, R.; Sadick, N.; Werschler, W.P.; Karnik, J.; Smith, S.R. Five-Year Safety and Satisfaction Study of PMMA-Collagen in the Correction of Nasolabial Folds. Dermatol. Surg. 2015, 41 (Suppl. S1), S302–S313. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Kim, Y.J. Foreign body granulomas after the use of dermal fillers: Pathophysiology, clinical appearance, histologic features, and treatment. Arch. Plast. Surg. 2015, 42, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Lemperle, G.; Gauthier-Hazan, N.; Wolters, M.; Eisemann-Klein, M.; Zimmermann, U.; Duffy, D.M. Foreign body granulomas after all injectable dermal fillers: Part 1. Possible causes. Plast. Reconstr. Surg. 2009, 123, 1842–1863. [Google Scholar] [CrossRef]
- Inglefield, C.; Samuelson, U.E.; Landau, M.; DeVore, D. Bio-Dermal Restoration with Rapidly Polymerizing Collagen: A Multicenter Clinical Study. Aesthetic Surg. J. 2018, 38, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, L.; Natali, M.L.; Brunetti, C.; Sannino, A.; Gallo, N. An Update on the Clinical Efficacy and Safety of Collagen Injectables for Aesthetic and Regenerative Medicine Applications. Polymers 2023, 15, 1020. [Google Scholar] [CrossRef] [PubMed]
- Duranti, F.; Salti, G.; Bovani, B.; Calandra, M.; Rosati, M.L. Injectable hyaluronic acid gel for soft tissue augmentation. A clinical and histological study. Dermatol. Surg. 1998, 24, 1317–1325. [Google Scholar] [CrossRef]
- Wang, Y.; Viennet, C.; Robin, S.; Berthon, J.-Y.; He, L.; Humbert, P. Precise role of dermal fibroblasts on melanocyte pigmentation. J. Dermatol. Sci. 2017, 88, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Gostyński, A.; Pasmooij, A.M.G.; Del Rio, M.; Diercks, G.F.; Pas, H.H.; Jonkman, M.F. Pigmentation and melanocyte supply to the epidermis depend on type XVII collagen. Exp. Dermatol. 2014, 23, 130–132. [Google Scholar] [CrossRef]
- Moon, H.-R.; Jung, J.M.; Kim, S.Y.; Song, Y.; Chang, S.E. TGF-β3 suppresses melanogenesis in human melanocytes cocultured with UV-irradiated neighboring cells and human skin. J. Dermatol. Sci. 2020, 99, 100–108. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Statistics | |||||||
|---|---|---|---|---|---|---|---|
| Number of Patients | Female | Male | Age Minimum | Age Maximum | Mean | Std. Deviation | |
| Normal group | 50 | 42 | 8 | 30 | 70 | 49.76 | 10.916 |
| Smoker group | 20 | 18 | 2 | 31 | 70 | 52.5 | 13.233 |
| Acne group | 30 | 27 | 3 | 27 | 48 | 40.17 | 4.92 |
| SGAIS SCALE | ||
|---|---|---|
| Rating | Description | |
| 5 | very much improved | optimal cosmetic result |
| 4 | much improved | marked improvement in appearance from the initial condition, but not optimal for the patient. A touch up would slightly improve the result |
| 3 | improved | obvious improvement in appearance from the initial condition, but a touch up or retreatment is indicated |
| 2 | no change | the appearance is essentially the same as the original condition |
| 1 | worse | the appearance is worse than the original condition |
| Friedman Test Wrinkle Depth | ||||||
|---|---|---|---|---|---|---|
| Normal Group | Smoker Group | Acne Group | ||||
| χ Square | Sig. (2-Tailed) | χ Square | Sig. (2-Tailed) | χ Square | Sig. (2-Tailed) | |
| CHEEK wrinkle depth (1 mm filter) | 20.28 | 0.000 | 30.9 | 0.000 | 43.46 | 0.000 |
| CHEEK wrinkle depth (2 mm filter) | 36.48 | 0.000 | 40 | 0.000 | 56.26 | 0.000 |
| CHEEK wrinkle depth (4 mm filter) | 38.92 | 0.000 | 36.1 | 0.000 | 39.26 | 0.000 |
| EYE wrinkle depth (1 mm filter) | 43.72 | 0.000 | 31.6 | 0.000 | ||
| EYE wrinkle depth (2 mm filter) | 20.52 | 0.000 | 30.1 | 0.000 | ||
| EYE wrinkle depth (4 mm filter) | 17.76 | 0.000 | 12.7 | 0.002 | ||
| NECK wrinkle depth (1 mm filter) | 6.76 | 0.034 | 40 | 0.000 | ||
| NECK wrinkle depth (2 mm filter) | 0.52 | 0.771 | 18.1 | 0.000 | ||
| NECK wrinkle depth (4 mm filter) | 9.64 | 0.000 | 40 | 0.000 | ||
| Friedman Test Hemoglobin Values (Antera 3D Scanner) | ||||||
|---|---|---|---|---|---|---|
| Normal Group | Smoker Group | Acne Group | ||||
| χ Square | Sig. (2-Tailed) | χ Square | Sig. (2-Tailed) | χ Square | Sig. (2-Tailed) | |
| CHEEK wrinkle depth (1 mm filter) | 0.579 | 0.749 | 34.9 | 0.000 | 46.33 | 0.000 |
| EYE wrinkle depth (1 mm filter) | 4.318 | 0.115 | 25.139 | 0.000 | ||
| NECK wrinkle depth (1 mm filter) | 4.404 | 0.111 | 21 | 0.000 | ||
| Friedman Test Hemoglobin Values (Antera 3D Scanner) | ||||||
| Normal Group | Smoker Group | Acne Group | ||||
| χ Square | Sig. (2-tailed) | χ Square | Sig. (2-tailed) | χ Square | Sig. (2-tailed) | |
| CHEEK wrinkle depth (1 mm filter) | 24.121 | 0.000 | 37.696 | 0.000 | 10.41 | 0.005 |
| EYE wrinkle depth (1 mm filter) | 29.249 | 0.000 | 34.9 | 0.000 | ||
| NECK wrinkle depth (1 mm filter) | 3.146 | 0.207 | 8.532 | 0.014 | ||
| Correlations between WRINKLE DEPTH Versus AGE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NORMAL GROUP | SMOKER GROUP | ACNE GROUP | ||||||||
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | ||
| CHEEK wrinkle depth (1 mm filter) versus patient’s age | Sig. (2-tailed) | 0.43 | 0.343 | 0.763 | 0.142 | 0.453 | 0.282 | 0.223 | 0.223 | 0.259 |
| CHEEK wrinkle depth (2 mm filter) versus patient’s age | Sig. (2-tailed) | 0.314 | 0.744 | 0.352 | 0.535 | 0.378 | 0.282 | 0.267 | 0.223 | 0.816 |
| CHEEK wrinkle depth (4 mm filter) versus patient’s age | Sig. (2-tailed) | 0.156 | 0.551 | 0.821 | 0.672 | 0.819 | 0.282 | 0.223 | 0.223 | 0.259 |
| EYE wrinkle depth (1 mm filter) versus patient’s age | Sig. (2-tailed) | 0.731 | 0.591 | 0.92 | 0.073 | 0.453 | 0.282 | |||
| EYE wrinkle depth (2 mm filter) versus patient’s age | Sig. (2-tailed) | 0.86 | 0.172 | 0.352 | 0.181 | 0.063 | 0.282 | |||
| EYE wrinkle depth (4 mm filter) versus patient’s age | Sig. (2-tailed) | 0.953 | 0.388 | 0.821 | 0.064 | 0.378 | 0.282 | |||
| NECK wrinkle depth (1 mm filter) versus patient’s age | Sig. (2-tailed) | 0.687 | 0.663 | 0.586 | 0.063 | 0.063 | 0.282 | |||
| NECK wrinkle depth (2 mm filter) versus patient’s age | Sig. (2-tailed) | 0.123 | 0.7 | 0.953 | 0.579 | 0.819 | 0.282 | |||
| NECK wrinkle depth (4 mm filter) versus patient’s age | Sig. (2-tailed) | 0.214 | 0.063 | 0.563 | 0.214 | 0.033 | 0.563 | |||
| Correlations between MELANIN QUATITY Versus AGE | ||||||||||
| NORMAL GROUP | SMOKER GROUP | ACNE GROUP | ||||||||
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | ||
| CHEEK melanin quantity versus patient’s age | Sig. (2-tailed) | 0.192 | 0.207 | 0.33 | 0.26 | 0.057 | 0.409 | 0.23 | 0.355 | 0.986 |
| EYE melanin quantity versus patient’s age | Sig. (2-tailed) | 0.906 | 0.078 | 0.833 | 0.647 | 0.646 | 0.298 | |||
| NECK melanin quantity versus patient’s age | Sig. (2-tailed) | 0.226 | 0.699 | 0.524 | 0.647 | 0.109 | 0.295 | |||
| Correlations between HEMOGLOBIN QUANTITY Versus AGE | ||||||||||
| NORMAL GROUP | SMOKER GROUP | ACNE GROUP | ||||||||
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | ||
| CHEEK melanin quantity versus patient’s age | Sig. (2-tailed) | 0.597 | 0.109 | 0.627 | 0.101 | 0.252 | 0.28 | 0.654 | 0.37 | 0.691 |
| EYE melanin quantity versus patient’s age | Sig. (2-tailed) | 0.43 | 0.374 | 0.614 | 0.06 | 0.591 | 0.326 | |||
| NECK melanin quantity versus patient’s age | Sig. (2-tailed) | 0.358 | 0.393 | 0.31 | 0.073 | 0.102 | 0.31 | |||
| Face Q Questionnaire Results | |||
|---|---|---|---|
| Normal Group | |||
| Number of Patients | Chi-Square | Asymp. Sig | |
| Aging appraisal questions | 50 | 40.968 | 0.000 |
| Facial appearance questions | 50 | 70.235 | 0.000 |
| Appraisal lines overall questions | 50 | 47.582 | 0.000 |
| Appraisal neck questions | 50 | 48.042 | 0.000 |
| Skin quality questions | 50 | 49.834 | 0.000 |
| Smokers Group | |||
| Aging appraisal questions | 20 | 13.13 | 0.001 |
| Facial appearance questions | 20 | 27.103 | 0.000 |
| Appraisal lines overall questions | 20 | 28.43 | 0.000 |
| Appraisal neck questions | 20 | 15.233 | 0.000 |
| Skin quality questions | 20 | 13.899 | 0.001 |
| Acne Group | |||
| Aging appraisal questions | 30 | 24.122 | 0.000 |
| Facial appearance questions | 30 | 36.735 | 0.000 |
| Appraisal lines overall questions | 30 | 27.291 | 0.000 |
| Appraisal neck questions | 30 | 36.439 | 0.000 |
| Skin quality questions | 30 | 32.739 | 0.000 |
| Wilcoxon Signed-Rank Test SGAIS QUESTIONNAIRE | ||||||
|---|---|---|---|---|---|---|
| NORMAL GROUP | SMOKER GROUP | ACNE GROUP | ||||
| Wilcoxon Signed-Rank Test | Z | Asymp. Sig. (2-Tailed) | Z | Asymp. Sig. (2-Tailed) | Z | Asymp. Sig. (2-Tailed) |
| −3.186 | 0.001 | −2.111 b | 0.035 | −4.244 b | 0.000 | |
| NORMAL GROUP | SMOKER GROUP | ACNE GROUP | ||||
| T1 | T2 | T1 | T2 | T1 | T2 | |
| Very Much Improved | 16% | 18% | 15% | 25% | 0% | 10% |
| Much Improved | 12% | 25% | 10% | 20% | 0% | 60% |
| Improved | 70% | 32% | 70% | 55% | 76.6% | 30% |
| No Change | 2% | 0% | 5% | 0% | 23.3% | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Rosa, L.; De Pasquale, A.; Baldassano, S.; Marguglio, N.; Drid, P.; Proia, P.; Vasto, S. New Regenerative and Anti-Aging Medicine Approach Based on Single-Stranded Alpha-1 Collagen for Neo-Collagenesis Induction: Clinical and Instrumental Experience of a New Injective Polycomponent Formulation for Dermal Regeneration. Biomedicines 2024, 12, 916. https://doi.org/10.3390/biomedicines12040916
Di Rosa L, De Pasquale A, Baldassano S, Marguglio N, Drid P, Proia P, Vasto S. New Regenerative and Anti-Aging Medicine Approach Based on Single-Stranded Alpha-1 Collagen for Neo-Collagenesis Induction: Clinical and Instrumental Experience of a New Injective Polycomponent Formulation for Dermal Regeneration. Biomedicines. 2024; 12(4):916. https://doi.org/10.3390/biomedicines12040916
Chicago/Turabian StyleDi Rosa, Luigi, Antonino De Pasquale, Sara Baldassano, Noemi Marguglio, Patrik Drid, Patrizia Proia, and Sonya Vasto. 2024. "New Regenerative and Anti-Aging Medicine Approach Based on Single-Stranded Alpha-1 Collagen for Neo-Collagenesis Induction: Clinical and Instrumental Experience of a New Injective Polycomponent Formulation for Dermal Regeneration" Biomedicines 12, no. 4: 916. https://doi.org/10.3390/biomedicines12040916