
Associations among COVID-19 Family Stress, Family Functioning, and Child Health-Related Quality of Life through Lifestyle Behaviors in Children

Abstract
:1. Introduction
1.1. COVID-19 Family Stress, Family Functioning, and Health-Related Quality of Life
1.2. Research Hypothesis
- (1)
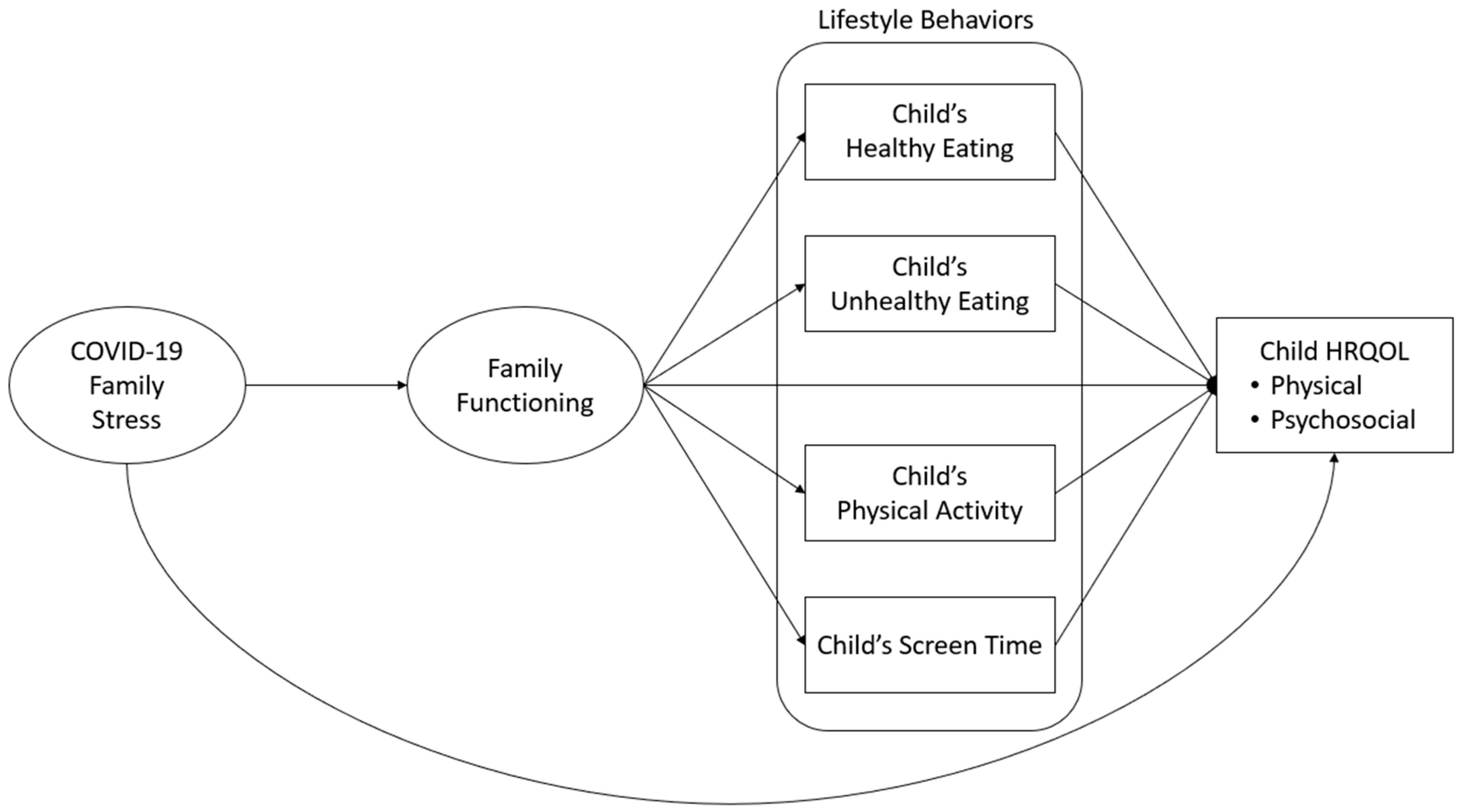
- COVID-19 family stress is negatively related to family functioning and child physical and psychosocial HRQOL;
- (2)
- Family functioning is positively associated with child healthy eating and PA and negatively associated with child unhealthy eating and screen time;
- (3)
- Family functioning is positively related to child physical and psychosocial HRQOL;
- (4)
- Child healthy food intake and PA are positively related to both child physical and psychosocial HRQOL;
- (5)
- Child unhealthy diet and screen time are negatively related to child physical and psychosocial HRQOL;
- (6)
- Children’s lifestyle behaviors convey indirect effects of family functioning on HRQOL.
2. Materials and Methods
2.1. Sample Recruitment and Data Collection Procedures
2.2. Study Measures
2.2.1. COVID-19 Family Stress
2.2.2. Family Functioning
2.2.3. Child’s Dietary Intake
2.2.4. Child Physical Activity
2.2.5. Child’s Screen Time
2.2.6. Child HRQOL
2.2.7. Race/Ethnicity
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Path Analysis for the Total Sample
3.3. Multi-Group Path Analysis Results for Boys and Girls
3.4. Indirect Pathways
4. Discussion
4.1. COVID-19 Family Stress and Family Functioning
4.2. COVID-19 Family Stress and Child Physical HRQOL
4.3. Family Functioning and Child Food Intake
4.4. Unhealthy Diets in Children and Their Psychosocial HRQOL
4.5. Child Gender Differences
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus United States Overview. Available online: https://coronavirus.jhu.edu/region/united-states (accessed on 10 February 2023).
- National Academies of Sciences, Engineering, and Medicine. Addressing the Long-Term Effects of the COVID-19 Pandemic on Children and Families; Coker, T.R., Gootman, J.A., Backes, E.P., Eds.; National Academies Press: Washington, DC, USA, 2023; ISBN 978-0-309-69695-1. [Google Scholar]
- Ruiz-Roso, M.B.; de Carvalho Padilha, P.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Aires, M.T.; de Oliveira Cardoso, L.; et al. COVID-19 Confinement and Changes of Adolescent’s Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 Virus Outbreak on Movement and Play Behaviours of Canadian Children and Youth: A National Survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Nobari, H.; Fashi, M.; Eskandari, A.; Villafaina, S.; Murillo-Garcia, Á.; Pérez-Gómez, J. Effect of Covid-19 on Health-Related Quality of Life in Adolescents and Children: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 14563. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, K.; Nigg, C.; Niessner, C.; Schmidt, S.C.E.; Oriwol, D.; Hanssen-Doose, A.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Worth, A.; et al. The Impact of COVID-19 on the Interrelation of Physical Activity, Screen Time and Health-Related Quality of Life in Children and Adolescents in Germany: Results of the Motorik-Modul Study. Children 2021, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- WHO. Constitution of the World Health Organization; World Health Organization: Geneva, Switzerland, 1948. [Google Scholar]
- De Civita, M.; Regier, D.; Alamgir, A.H.; Anis, A.H.; FitzGerald, M.J.; Marra, C.A. Evaluating Health-Related Quality-of-Life Studies in Paediatric Populations. Pharmacoeconomics 2005, 23, 659–685. [Google Scholar] [CrossRef] [PubMed]
- Seid, M.; Varni, J.W.; Jacobs, J.R. Pediatric Health-Related Quality-of-Life Measurement Technology: Intersections between Science, Managed Care, and Clinical Care. J. Clin. Psychol. Med. Settings 2000, 7, 17–27. [Google Scholar] [CrossRef]
- Wallander, J.L.; Koot, H.M. Quality of Life in Children: A Critical Examination of Concepts, Approaches, Issues, and Future Directions. Clin. Psychol. Rev. 2016, 45, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Burwinkle, T.M.; Seid, M. The PedsQLTM 4.0 as a School Population Health Measure: Feasibility, Reliability, and Validity. Qual. Life Res. 2006, 15, 203–215. [Google Scholar] [CrossRef] [PubMed]
- USA Facts US Coronavirus Vaccine Tracker. Available online: https://usafacts.org/visualizations/covid-vaccine-tracker-states/ (accessed on 20 February 2024).
- Manuti, A.; Van der Heijden, B.; Kruyen, P.; De Vos, A.; Zaharie, M.; Lo Presti, A. Editorial: How Normal Is the New Normal? Individual and Organizational Implications of the COVID-19 Pandemic. Front. Psychol. 2022, 13, 931236. [Google Scholar] [CrossRef]
- Gayatri, M.; Puspitasari, M.D. The Impact of COVID-19 Pandemic on Family Well-Being: A Literature Review. Fam. J. 2023, 31, 606–613. [Google Scholar] [CrossRef]
- Feinberg, M.E.; Mogle, A.J.; Lee, J.; Tornello, S.L.; Hostetler, M.L.; Cifelli, J.A.; Bai, S.; Hotez, E. Impact of the COVID-19 Pandemic on Parent, Child, and Family Functioning. Fam. Process 2022, 61, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, M.; Lionetti, F.; Pastore, M.; Fasolo, M. Parents’ Stress and Children’s Psychological Problems in Families Facing the COVID-19 Outbreak in Italy. Front. Psychol. 2020, 11, 1713. [Google Scholar] [CrossRef] [PubMed]
- Gilic, B.; Ostojic, L.; Corluka, M.; Volaric, T.; Sekulic, D. Contextualizing Parental/Familial Influence on Physical Activity in Adolescents before and during COVID-19 Pandemic: A Prospective Analysis. Children 2020, 7, 125. [Google Scholar] [CrossRef] [PubMed]
- Masarik, A.S.; Conger, R.D. Stress and Child Development: A Review of the Family Stress Model. Curr. Opin. Psychol. 2017, 13, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Peltz, J.S.; Crasta, D.; Daks, J.S.; Rogge, R.D. Shocks to the System: The Influence of COVID-19–Related Stressors on Coparental and Family Functioning. Dev. Psychol. 2021, 57, 1693–1707. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.B.; Baldwin, L.M.; Bishop, D.S. The McMaster Family Assessment Device. J. Marital. Fam. Ther. 1983, 9, 171–180. [Google Scholar] [CrossRef]
- Lewandowski, A.S.; Palermo, T.M.; Stinson, J.; Handley, S.; Chambers, C.T. Systematic Review of Family Functioning in Families of Children and Adolescents with Chronic Pain. J. Pain. 2010, 11, 1027–1038. [Google Scholar] [CrossRef] [PubMed]
- Haverman, L.; Limperg, P.F.; Young, N.L.; Grootenhuis, M.A.; Klaassen, R.J. Paediatric Health-Related Quality of Life: What Is It and Why Should We Measure It? Arch. Dis. Child. 2017, 102, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Rezaei-Dehaghani, A.; Keshvari, M.; Paki, S. The Relationship between Family Functioning and Academic Achievement in Female High School Students of Isfahan, Iran, in 2013–2014. Iran J. Nurs. Midwifery Res. 2018, 23, 183. [Google Scholar] [CrossRef]
- Kroneman, L.M.; Loeber, R.; Hipwell, A.E.; Koot, H.M. Girls’ Disruptive Behavior and Its Relationship to Family Functioning: A Review. J. Child. Fam. Stud. 2009, 18, 259–273. [Google Scholar] [CrossRef]
- Robson, S.M.; McCullough, M.B.; Rex, S.; Munafò, M.R.; Taylor, G. Family Meal Frequency, Diet, and Family Functioning: A Systematic Review with Meta-Analyses. J. Nutr. Educ. Behav. 2020, 52, 553–564. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; McLaughlin, J.; Fitzgerald, A. The Relationship between Adverse Childhood Experiences, Family Functioning, and Mental Health Problems among Children and Adolescents: A Systematic Review. J. Fam. Ther. 2020, 42, 291–316. [Google Scholar] [CrossRef]
- Sanders, M.R.; Turner, K.M.T. The Importance of Parenting in Influencing the Lives of Children. In Handbook of Parenting and Child Development Across the Lifespan; Springer International Publishing: Cham, Switzerland, 2018; pp. 3–26. [Google Scholar]
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The Influence of Physical Activity, Sedentary Behavior on Health-Related Quality of Life among the General Population of Children and Adolescents: A Systematic Review. PLoS ONE 2017, 12, e0187668. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, B.; Hardy, L.L.; Baur, L.A.; Burlutsky, G.; Mitchell, P. Physical Activity and Sedentary Behaviors and Health-Related Quality of Life in Adolescents. Pediatrics 2012, 130, e167–e174. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Wang, N.; Ware, R.S.; Sha, Y.; Xu, F. Lifestyle-Related Behaviors and Health-Related Quality of Life among Children and Adolescents in China. Health Qual. Life Outcomes 2021, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Floody, P.; Caamaño-Navarrete, F.; Guzmán-Guzmán, I.P.; Jerez-Mayorga, D.; Martínez-Salazar, C.; Álvarez, C. Food Habits and Screen Time Play a Major Role in the Low Health Related to Quality of Life of Ethnic Ascendant Schoolchildren. Nutrients 2020, 12, 3489. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, B.; Louie, J.C.T.; Flood, V.M.; Burlutsky, G.; Hardy, L.L.; Baur, L.A.; Mitchell, P. Influence of Obesogenic Behaviors on Health-Related Quality of Life in Adolescents. Asia Pac. J. Clin. Nutr. 2014, 23, 121–127. [Google Scholar]
- Chen, G.; Ratcliffe, J.; Olds, T.; Magarey, A.; Jones, M.; Leslie, E. BMI, Health Behaviors, and Quality of Life in Children and Adolescents: A School-Based Study. Pediatrics 2014, 133, e868–e874. [Google Scholar] [CrossRef] [PubMed]
- Boraita, R.J.; Ibort, E.G.; Torres, J.M.D.; Alsina, D.A. Gender Differences Relating to Lifestyle Habits and Health-Related Quality of Life of Adolescents. Child. Indic. Res. 2020, 13, 1937–1951. [Google Scholar] [CrossRef]
- Hourani, E.M.; Hammad, S.M.; Shaheen, A.; Amre, H.M. Health-Related Quality of Life Among Jordanian Adolescents. Clin. Nurs. Res. 2017, 26, 337–353. [Google Scholar] [CrossRef]
- Meyer, M.; Oberhoffer, R.; Hock, J.; Giegerich, T.; Müller, J. Health-related Quality of Life in Children and Adolescents: Current Normative Data, Determinants and Reliability on Proxy-report. J. Paediatr. Child. Health 2016, 52, 628–631. [Google Scholar] [CrossRef] [PubMed]
- Celik, H.; Lagro-Janssen, T.A.L.M.; Widdershoven, G.G.A.M.; Abma, T.A. Bringing Gender Sensitivity into Healthcare Practice: A Systematic Review. Patient Educ. Couns. 2011, 84, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Hijkoop, A.; ten Kate, C.A.; Madderom, M.J.; Ijsselstijn, H.; Reuser, J.A.; Koopman, H.; van Rosmalen, J.; Rietman, A.B. Sex Differences in Children’s Health Status as Measured by the Pediatric Quality of Life Inventory (PedsQL)TM: Cross-Sectional Findings from a Large School-Based Sample in the Netherlands. BMC Pediatr. 2021, 21, 580. [Google Scholar] [CrossRef] [PubMed]
- Oertelt-Prigione, S. Putting Gender into Sex- and Gender-Sensitive Medicine. EClinicalMedicine 2020, 20, 100305. [Google Scholar] [CrossRef] [PubMed]
- Prolific Academic Ltd. Available online: https://www.prolific.com/ (accessed on 31 December 2021).
- Turner, A.M.; Engelsma, T.; Taylor, J.O.; Sharma, R.K.; Demiris, G. Recruiting Older Adult Participants through Crowdsourcing Platforms: Mechanical Turk versus Prolific Academic. AMIA Annu. Symp. Proc. 2020, 2020, 1230–1238. [Google Scholar] [PubMed]
- Kim, K.W.; Wallander, J.L. Influences of Parental COVID-19 Stress and Family Functioning on Children’s Weight-Related Behaviors, Weight Status, and Quality of Life. Available online: https://osf.io/xezqr (accessed on 31 October 2023).
- Kim, K.W. Associations among COVID-19 Stress, Family Functioning and Child Health-Related Quality of Life through Lifestyle Behaviors of Children. Available online: https://osf.io/bm42k/ (accessed on 13 December 2023).
- Prime, H.; Wade, M.; Browne, D.T. Risk and Resilience in Family Well-Being during the COVID-19 Pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Prime, H.; Wade, M.; May, S.S.; Jenkins, J.M.; Browne, D.T. The COVID-19 Family Stressor Scale: Validation and Measurement Invariance in Female and Male Caregivers. Front. Psychiatry 2021, 12, 669106. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. The Dietary Screener in the 2009 California Health Interview Survey. 2019. Available online: https://epi.grants.cancer.gov/diet/screeners/ (accessed on 17 October 2022).
- Cartwright, M.; Wardle, J.; Steggles, N.; Simon, A.E.; Croker, H.; Jarvis, M.J. Stress and Dietary Practices in Adolescents. Health Psychol. 2003, 22, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, A.D.; Chung, P.J. Racial and Ethnic Disparities in Dietary Intake among California Children. J. Acad. Nutr. Diet. 2016, 116, 439–448. [Google Scholar] [CrossRef]
- Allison, P.D. Missing Data Techniques for Structural Equation Modeling. J. Abnorm. Psychol. 2003, 112, 545–557. [Google Scholar] [CrossRef]
- Bryne, B.M. Structural Equation Modeling with Mplus: Basic Concepts, Applications, and Programming, 2nd ed.; Routledge/Taylor & Francis Group: Abingdon, UK, 2012. [Google Scholar]
- Hu, L.; Bentler, P.M. Fit Indices in Covariance Structure Modeling: Sensitivity to Under parameterized Model Misspecification. Psychol. Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Yuan, K.-H.; Chan, W.; Marcoulides, G.A.; Bentler, P.M. Assessing Structural Equation Models by Equivalence Testing with Adjusted Fit Indexes. Struct. Equ. Model. 2016, 23, 319–330. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample Size in Factor Analysis. Psychol. Methods 1999, 4, 84–99. [Google Scholar] [CrossRef]
- Boomsa, A. Nonconvergence, Improper Solutions, and Starting Values in LISREL Maximum Likelihood Estimation. Psychometrika 1985, 50, 229–242. [Google Scholar] [CrossRef]
- Boomsa, A. Robustness of LISREL against Small Sample Sizes in Factor Analysis Models. In Systems Under Indirection Observation: Causality, Structure, Prediction (Part I); North Holland: Amsterdam, The Netherlands, 1982; pp. 149–173. [Google Scholar]
- Bentler, P.M.; Chou, C.H. Practical Issues in Structural Modeling. Sociol. Methods Res. 1987, 16, 78–117. [Google Scholar] [CrossRef]
- Bollen, K.A. Structural Equations with Latent Variables; Wiley: Hoboken, NJ, USA, 1989. [Google Scholar]
- Nunnally, J.C. Psychometric Theory; McGraw-Hill: New York City, NY, USA, 1967. [Google Scholar]
- Ahrens, W.H.; Cox, D.J.; Budhwar, G. Use of the Arcsine and Square Root Transformations for Subjectively Determined Percentage Data. Weed Sci. 2017, 38, 452–458. [Google Scholar] [CrossRef]
- Eales, L.; Ferguson, G.M.; Gillespie, S.; Smoyer, S.; Carlson, S.M. Family Resilience and Psychological Distress in the COVID-19 Pandemic: A Mixed Methods Study. Dev. Psychol. 2021, 57, 1563–1581. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, H.; Zeng, H.; Zhang, S.; Du, Q.; Jiang, T.; Du, B. The Differential Psychological Distress of Populations Affected by the COVID-19 Pandemic. Brain Behav. Immun. 2020, 87, 49–50. [Google Scholar] [CrossRef]
- Conger, R.D.; Ge, X.; Elder, G.H.; Lorenz, F.O.; Simons, R.L. Economic Stress, Coercive Family Process, and Developmental Problems of Adolescents. Child. Dev. 1994, 65, 541–561. [Google Scholar] [CrossRef]
- Rossi, L.; Behme, N.; Breuer, C. Physical Activity of Children and Adolescents during the COVID-19 Pandemic—A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 11440. [Google Scholar] [CrossRef]
- Walsh, F. Normal Family Processes: Growing Diversity and Complexity, 3rd ed.; The Guilford Press: New York, NY, USA, 2003. [Google Scholar]
- Snoek, H.M.; Engels, R.C.M.E.; Janssens, J.M.A.M.; van Strien, T. Parental Behaviour and Adolescents’ Emotional Eating. Appetite 2007, 49, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Coccia, C.; Darling, C.A.; Rehm, M.; Cui, M.; Sathe, S.K. Adolescent Health, Stress and Life Satisfaction: The Paradox of Indulgent Parenting. Stress Health 2012, 28, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Zubrick, S.R.; Williams, A.A.; Silburn, G.; Vimpani, G. Indicators of Social and Family Functioning; Department of Family and Community Services: Canberra, ACT, Australia, 2000.
- Melguizo-Ibáñez, E.; Viciana-Garófano, V.; Zurita-Ortega, F.; Ubago-Jiménez, J.L.; González-Valero, G. Physical Activity Level, Mediterranean Diet Adherence, and Emotional Intelligence as a Function of Family Functioning in Elementary School Students. Children 2020, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean Diet and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses of Observational Studies and Randomised Trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Khalid, S.; Williams, C.M.; Reynolds, S.A. Is There an Association between Diet and Depression in Children and Adolescents? A Systematic Review. Br. J. Nutr. 2016, 116, 2097–2108. [Google Scholar] [CrossRef] [PubMed]
- Spencer, S.J.; Korosi, A.; Layé, S.; Shukitt-Hale, B.; Barrientos, R.M. Food for Thought: How Nutrition Impacts Cognition and Emotion. NPJ Sci. Food 2017, 1, 7. [Google Scholar] [CrossRef] [PubMed]
- Mörkl, S.; Wagner-Skacel, J.; Lahousen, T.; Lackner, S.; Holasek, S.J.; Bengesser, S.A.; Painold, A.; Holl, A.K.; Reininghaus, E. The Role of Nutrition and the Gut-Brain Axis in Psychiatry: A Review of the Literature. Neuropsychobiology 2020, 79, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.; Tombeau Cost, K.; Fuller, A.; Birken, C.S.; Anderson, L.N. Sex and Gender Differences in Childhood Obesity: Contributing to the Research Agenda. BMJ Nutr. Prev. Health 2020, 3, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Abedi, V.; Olulana, O.; Avula, V.; Chaudhary, D.; Khan, A.; Shahjouei, S.; Li, J.; Zand, R. Racial, Economic, and Health Inequality and COVID-19 Infection in the United States. J. Racial Ethn. Health Disparities 2021, 8, 732–742. [Google Scholar] [CrossRef]
- Tai, D.B.G.; Shah, A.; Doubeni, C.A.; Sia, I.G.; Wieland, M.L. The Disproportionate Impact of COVID-19 on Racial and Ethnic Minorities in the United States. Clin. Infect. Dis. 2021, 72, 703–706. [Google Scholar] [CrossRef]
- Hussong, A.M.; Midgette, A.J.; Richards, A.N.; Petrie, R.C.; Coffman, J.L.; Thomas, T.E. COVID-19 Life Events Spill-Over on Family Functioning and Adolescent Adjustment. J. Early Adolesc. 2022, 42, 359–388. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Parent’s gender | % |
| Father (N = 113) | 50.9 |
| Mother (N = 109) | 49.1 |
| Parent’s age | M years |
| Father | 38.6 (SD = 7.1) |
| Mother | 39.7 (SD = 8.0) |
| Respondent’s relationship to the child | % |
| Biological mother | 43.4 |
| Biological father | 48.7 |
| Adoptive mother | 1.8 |
| Adoptive father | 0.4 |
| Foster father | 0.9 |
| Stepfather | 0.9 |
| Grandparent | 3.1 |
| Parent’s partner, boyfriend, or girlfriend | 0.4 |
| Other relative (brother, sister, uncle, aunt, etc.) | 0.4 |
| Father’s educational level | % |
| Some high school but did not graduate | 0.8 |
| High school graduate and GED | 6.7 |
| Some college, or 2-year degree (AA or AS) | 19.3 |
| 4-year college graduate (BA, BB, or BS) | 52.9 |
| More than a 4-year college degree (Ph.D., MD, etc.) | 20.2 |
| Mother’s educational level | % |
| 8th grade or less | 1.8 |
| Some high school but did not graduate | 1.8 |
| High school graduate and GED | 12.6 |
| Some college, or 2-year degree (AA or AS) | 22.5 |
| 4-year college graduate (BA, BB, or BS) | 41.4 |
| More than a 4-year college degree (Ph.D., MD, etc.) | 19.8 |
| Child’s gender | % |
| Boy (N = 119) | 53.6 |
| Girl (N = 102) | 45.9 |
| Child’s age | M years |
| Boy | 8.4 (SD = 2.5) |
| Girl | 7.8 (SD = 2.2) |
| Child’s race | % |
| Asian | 1.3 |
| Black | 5.7 |
| Latinx | 2.2 |
| White | 75.3 |
| Other | 15.4 |
| Variables | Scale | Total | Boys | Girls |
|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | ||
| COVID-19 Family Stress | ||||
| Experienced increased altercations with family members. | 1–3 | 1.26 (0.50) | 1.20 (0.49) | 1.27 (0.51) |
| Experienced increased emotional withdrawal from family members. | 1.39 (0.62) | 1.35 (0.61) | 1.43 (0.64) | |
| Children have become harder to manage. | 1.44 (0.64) | 1.45 (0.61) | 1.43 (0.67) | |
| More relationship conflicts with my partner. | 1.27 (0.52) | 1.24 (0.47) | 1.31 (0.58) | |
| Family Functioning | ||||
| In times of crisis, we can turn to each other for support. | 1–4 | 3.48 (0.60) | 3.54 (0.56) | 3.41 (0.64) |
| We can express feelings to each other. | 3.35 (0.60) | 3.37 (0.60) | 3.33 (0.59) | |
| We are able to make decisions about how to solve problems. | 3.36 (0.66) | 3.43 (0.63) | 3.29 (0.67) | |
| We confide in each other. | 3.60 (0.62) | 3.68 (0.56) | 3.51 (0.66) | |
| Child Healthy Food Intake | 1–10 | 3.68 (2.02) | 3.55 (2.03) | 3.91 (2.03) |
| Child Unhealthy Food Intake | 1–20 | 4.03 (3.11) | 2.99 (2.37) | 3.87 (3.47) |
| Child Physical Activity | 0–14 | 6.81 (4.10) | 7.18 (4.22) | 6.57 (4.07) |
| Child Screentime | 0–28 | 9.36 (5.32) | 9.91 (4.91) | 8.60 (5.55) |
| Child Physical HRQOL | 0–100 | 88.81 (11.71) | 89.23 (12.01) | 88.34 (11.40) |
| Child Psychosocial HRQOL | 82.15 (15.78) | 82.64 (15.65) | 81.59 (15.98) |
| Items | Factor Loadings | CFI | TLI | RMSEA |
|---|---|---|---|---|
| COVID-19 Family Stress | ||||
| Experienced increased altercations with family members. | 0.83 | 0.99 | 0.97 | 0.08 90% CI: 0.00, 0.17 |
| Experienced increased emotional withdrawal from family members. | 0.70 | |||
| Children have become harder to manage. | 0.61 | |||
| More relationship conflicts with my partner (if I am in a relationship). | 0.72 | |||
| Family Functioning | ||||
| In times of crisis, we can turn to each other for support. | 0.77 | 1.00 | 1.00 | 0.00 90% CI: 0.00, 0.13 |
| We are able to make decisions about how to solve problems | 0.86 | |||
| We can express feelings to each other. | 0.72 | |||
| We confide in each other. | 0.82 |
| Indirect Effect | Estimate (β) | SE | Bootstrap 95% CI |
|---|---|---|---|
| Total Group | |||
| Family functioning → | 0.05 | 0.01 | 0.02, 0.10 |
| Child unhealthy food intake → | |||
| Child physical HRQOL | |||
| Family functioning → | 0.06 | 0.02 | 0.02, 0.10 |
| Child unhealthy food intake → | |||
| Child psychosocial HRQOL | |||
| Girls | |||
| Family functioning → | 0.10 | 0.05 | 0.02, 0.20 |
| Child unhealthy food intake → | |||
| Child psychosocial HRQOL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.W.; Wallander, J.L.; Wiebe, D. Associations among COVID-19 Family Stress, Family Functioning, and Child Health-Related Quality of Life through Lifestyle Behaviors in Children. Children 2024, 11, 483. https://doi.org/10.3390/children11040483
Kim KW, Wallander JL, Wiebe D. Associations among COVID-19 Family Stress, Family Functioning, and Child Health-Related Quality of Life through Lifestyle Behaviors in Children. Children. 2024; 11(4):483. https://doi.org/10.3390/children11040483
Chicago/Turabian StyleKim, Kay W., Jan L. Wallander, and Deborah Wiebe. 2024. "Associations among COVID-19 Family Stress, Family Functioning, and Child Health-Related Quality of Life through Lifestyle Behaviors in Children" Children 11, no. 4: 483. https://doi.org/10.3390/children11040483