Ponseti Technique for the Management of Congenital Talipes Equinovarus in a Rural Set-Up in India: Experience of 356 Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Ethical Considerations
2.3. Inclusion and Exclusion Criteria
2.4. Evaluation of Final Outcome
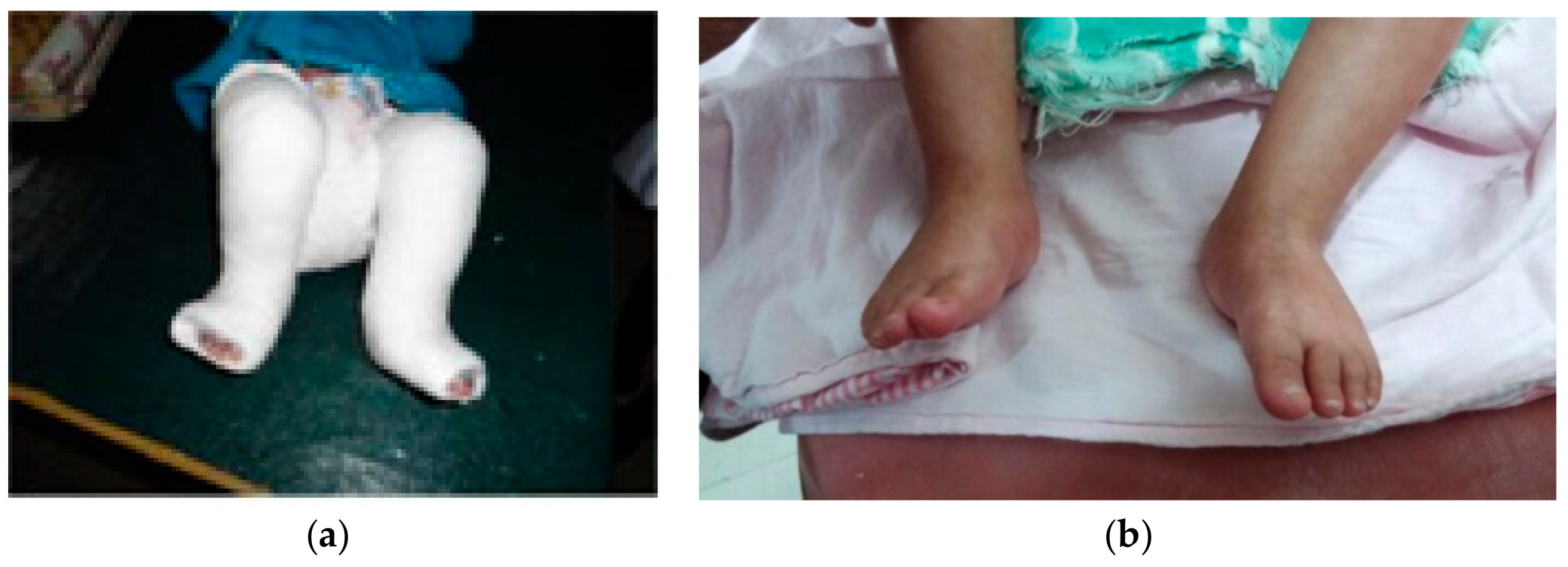
- (a)
- correction of the deformity by weekly serial casting;
- (b)
- maintenance of that correction by bracing.
2.5. Statistical Analysis
3. Results
3.1. Age
3.2. Laterality
3.3. Consaguinity and Family History
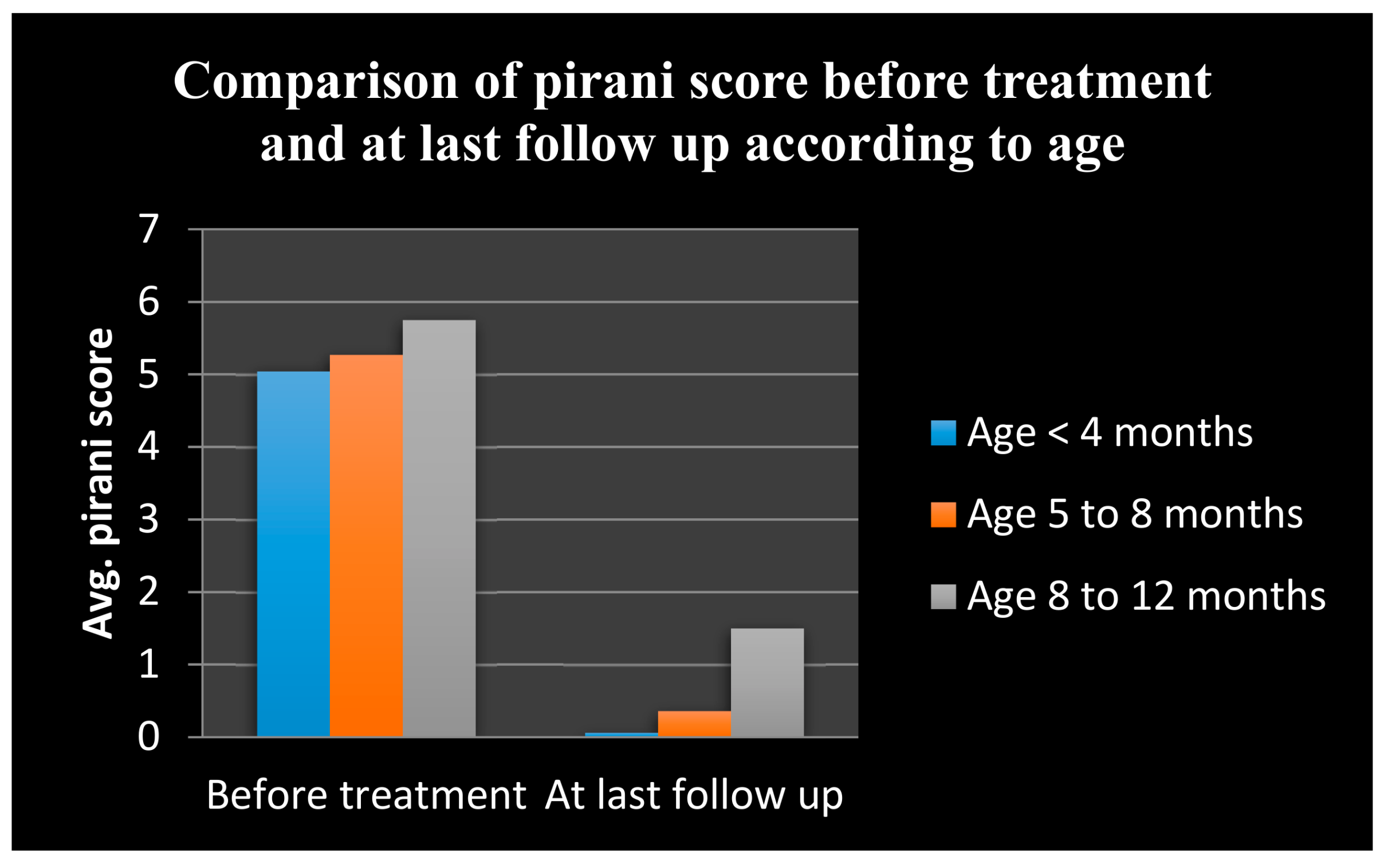
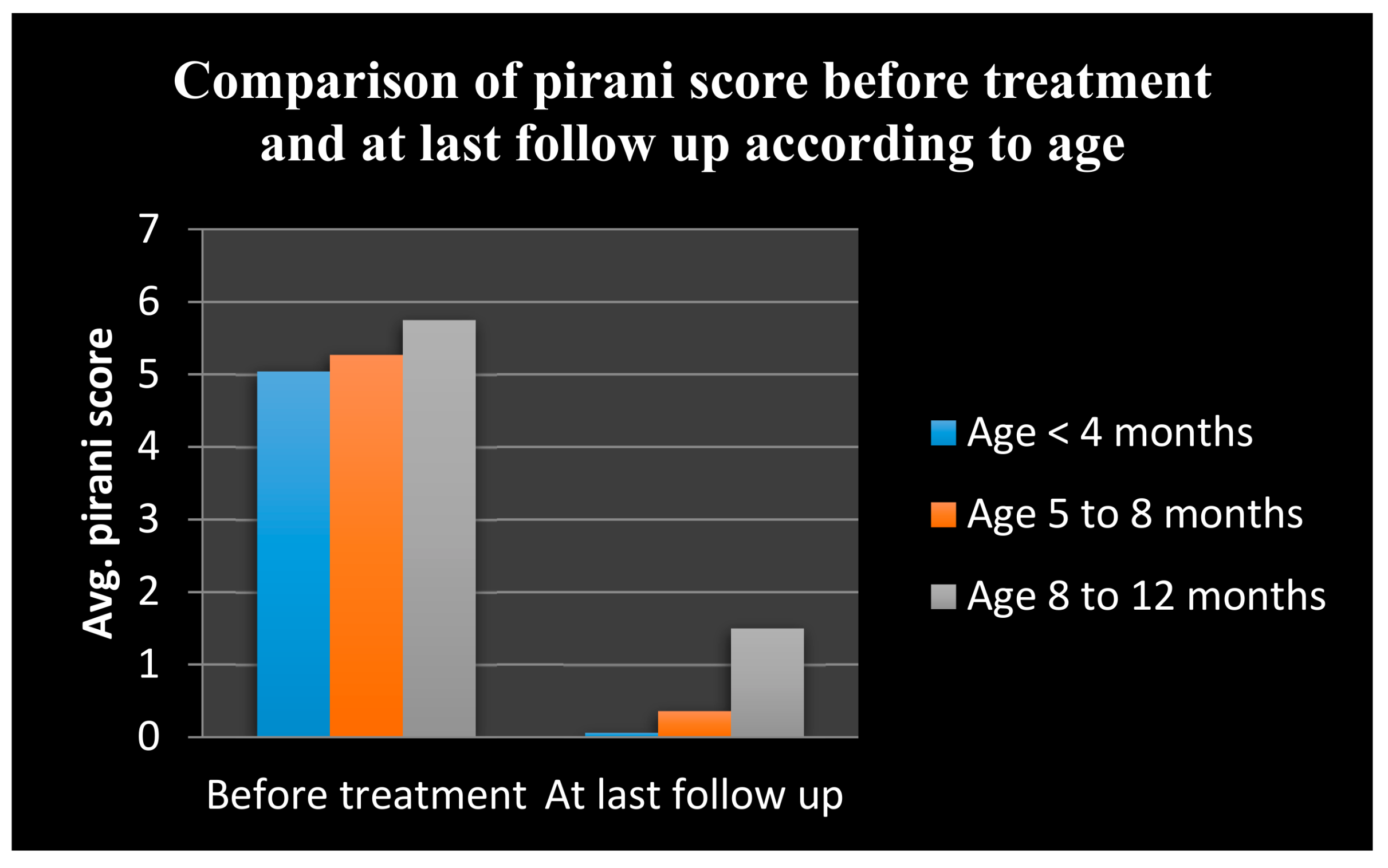
3.4. Pirani Score
- The mean + standard deviation (SD) at initial and final Pirani score in the age group of ≤4 months were 5.04 + 0. 85 and 0.06 + 0.21, respectively.
- The mean + SD at initial and final Pirani score in the age group of >4–8 months were 5.27 + 0.65 and 0.36 + 0.39, respectively.
- The mean + SD at initial and final Pirani score in the age group of >8–12 months were 5.75 + 0.61 and 1.50 + 1.41 respectively.
3.5. Number of Casts
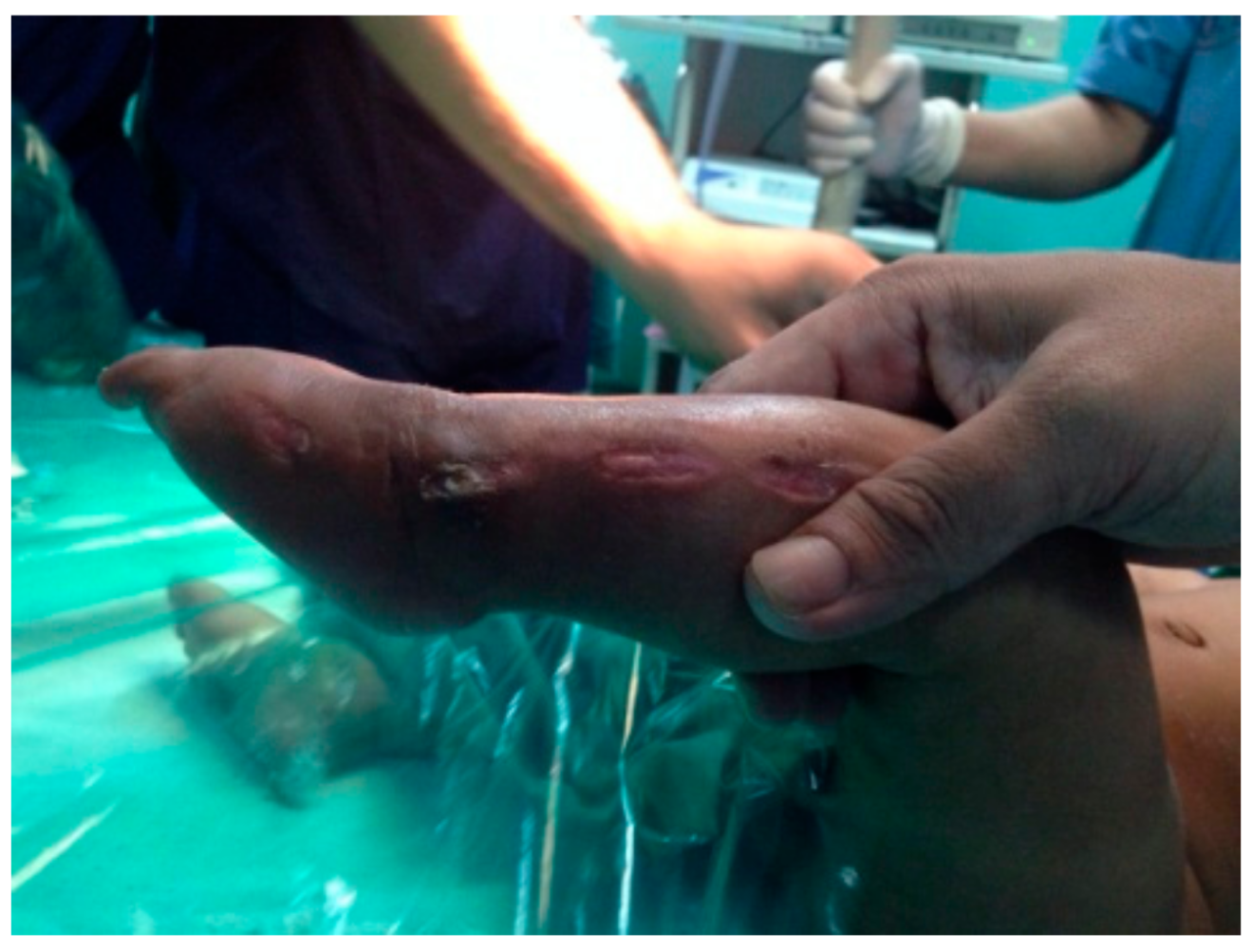
3.6. Complications
3.7. Final Outcome
3.8. Comparison of Cost of Treatment
4. Discussion
4.1. Demographic and Etiological Variables
4.2. Pirani Score
4.3. Tenotomy and Number of Casts
4.4. Complications
4.5. Final Functional Outcome
4.6. Cost-Effectiveness
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- De Hoedt, A.M. Clubfoot Image Classification, University of Iowa, Iowa Research Online. 2013. Available online: http://ir.uiowa.edu/etd/4836 (accessed on 5 December 2017).
- Staheli, L. Clubfoot: Ponseti Management; Global HELP Publications: Seattle, WA, USA, 2003; pp. 4–5. [Google Scholar]
- Globalclubfoot. India | Global Clubfoot Initiative. 2018. Available online: http://globalclubfoot.com/countries/india/ (accessed on 31 March 2018).
- Africa Clubfoot Training Project. Chapter 2 Africa Clubfoot Training Basic & Advanced Clubfoot Treatment Provider Courses—Participant Manual; Africa Clubfoot Training Project; University of Oxford: Oxford, UK, 2017. [Google Scholar]
- Kelly, D.M. Congenital anomalies of the lower extremity. In Campbell’s Operative Orthopaedics, 12th ed.; Canale, S., Beaty, J., Eds.; Mosby Elsevier: Philadelphia, PA, USA, 2013; pp. 994–1012. [Google Scholar]
- Morcuende, J.; Dolan, L.; Dietz, F.; Ponseti, I. Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics 2004, 113, 376. [Google Scholar] [CrossRef] [PubMed]
- Ponseti, I.V.; Smoley, E.N. Congenital clubfoot: The results of treatment. J. Bone Joint Surg. 1963, 45, 261–344. [Google Scholar] [CrossRef]
- Morcuende, J. Keynote Address. In Proceedings of the 5th Australasian Ponseti Conference, Melbourne, Australia, 28–29 March 2014. [Google Scholar]
- Khan, M.A.; Chinoy, M.A.; Moosa, R.; Ahmed, S.K. Significance of Pirani score at bracing-implications for recognizing a corrected clubfoot. Iowa Orthop. J. 2017, 37, 151–156. [Google Scholar] [PubMed]
- Dobbs, M.B.; Nunley, R.; Schoenecker, P.L. Long term follow up of patients with clubfoot treated with extensive soft tissue releases. J. Bone Joint Surg. Am. 2006, 88, 986–996. [Google Scholar] [CrossRef] [PubMed]
- Cosma, D.; Vasilescu, D.; Vasilescu, D.; Valeanu, M. Comparative results of the conservative treatment in clubfoot by two different protocols. J. Pediatr. Orthop. B 2007, 16, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Faizan, M.; Jilani, L.Z.; Abbas, M.; Zahid, M.; Asif, N. Management of idiopathic clubfoot by Ponseti technique in children presenting after one year of age. J. Foot Ankle Surg. 2015, 54, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Staheli, L. Clubfoot: Ponseti Management, 3rd ed.; Global HELP Publications: Seattle, WA, USA, 2009. [Google Scholar]
- Pirani, S.; Outerbridge, H.K.; Sawatzky, B.; Stothers, K. A reliable method of clinically evaluating a virgin clubfoot evaluation. In Proceedings of the 21st World Congress of SICOT, Sydney, Australia, 11 October 1999. [Google Scholar]
- Ikeda, K. Conservative treatment of idiopathic clubfoot. J. Pediatr. Orthop. 1992, 12, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Bensahel, H.; Guillaume, A.; Czukonyi, Z.; Desgrippes, Y. Results of physical therapy for idiopathic clubfoot: A long-term follow-up study. J. Pediatr. Orthop. 1990, 10, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Nather, A.; Bose, K. Conservative and surgical treatment of clubfoot. J. Pediatr. Orthop. 1987, 7, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Blakeslee, T.J. Congenital idiopathic talipes equinovarus (clubfoot). Current concepts. Clin. Podiatr. Med. Surg. 1997, 14, 9. [Google Scholar] [PubMed]
- Aronson, J.; Puskarich, C.L. Deformity and disability from treated clubfoot. J. Pediatr. Orthop. 1990, 10, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Karski, T.; Wosko, I. Experience in the conservative treatment of congenital clubfoot in newborns and infants. J. Pediatr. Orthop. 1989, 9, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, M.B.; Rudzki, J.; Purcell, D.B.; Walton, T.; Porter, K.R.; Gurnett, C.A. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J. Bone Joint Surg. Am. 2004, 86, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Bryman, A.; Cramer, D. Quantitative Data Analysis with IBM SPSS 17, 18 and 19: A Guide for Social Scientists; Routledge: New York, NY, USA, 2011. [Google Scholar]
- Gadhok, K.; Belthur, M.V.; Aroojis, A.J.; Cook, T.; Oprescu, F.; Ranade, A.S.; Morcuende, J.A. Qualitative assessment of the challenges to the treatment of idiopathic clubfoot by the Ponseti method in urban India. Iowa Orthop. J. 2012, 32, 135–140. [Google Scholar] [PubMed]
- Changulani, M.; Garg, N.K.; Rajagopal, T.S.; Bass, A.; Nayagam, S.N.; Sampath, J.; Bruce, C.E. Treatment of idiopathic club foot using the Ponseti method. Initial experience. J. Bone Joint Surg. Br. 2006, 88, 1385–1387. [Google Scholar] [CrossRef] [PubMed]
- Lehman, W.; Mohaideen, A.; Madan, S.; Scher, D.; Van Bosse, H.; Iannacone, M.; Bazzi, J.S.; Feldman, D.S. A method for the early evaluation of the Ponseti (Iowa) technique for the treatment of idiopathic clubfoot. J. Pediatr. Orthop. B 2003, 12, 133–140. [Google Scholar] [PubMed]
- Sætersdal, C.; Fevang, J.; Fosse, L.; Engesæter, L. Good results with the Ponseti method: A multicenter study of 162 clubfeet followed for 2–5 years. Acta Orthop. 2012, 83, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Pavone, V.; Testa, G.; Costarella, L.; Pavone, P.; Sessa, G. Congenital idiopathic talipes equinovarus: An evaluation in infants treated by the Ponseti method. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 2675–2679. [Google Scholar] [PubMed]
- Sreenivas, T.; Nataraj, A. Parental consanguinity and associated factors in congenital talipes equinovarus. Foot 2012, 22, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.M.; Dietz, F.R. Treatment of idiopathic clubfoot. A thirty-year follow-up note. J. Bone Joint Surg. Am. 1995, 77, 1477–1489. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Singh, S.; Patel, P.; Patel, J.; Varshney, M.K. Evaluation of the utility of the Ponseti method of correction of clubfoot deformity in a developing nation. Int. Orthop. 2008, 32, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Sakale, H.; Agrawal, A.; Singh, A.; Sahoo, B.; Jain, A. Treatment of idiopathic clubfoot by Ponseti method. J. Orthop. Traumatol. Rehab. 2017, 9, 25. [Google Scholar] [CrossRef]
- Ferreira, L.F.A.; Nogueira, M.P.; Pereira, J.C.R.; Duarte, P.S. Comparison of hospital costs and duration of treatment with two different clubfoot protocols. Iowa Orthop. J. 2011, 31, 49–51. [Google Scholar] [PubMed]
- Hussain, H.; Burfat, A.M.; Samad, L.; Jawed, F.; Chinoy, M.A.; Khan, M.A. Cost-effectiveness of the Ponseti method for treatment of clubfoot in Pakistan. World J. Surg. 2014, 38, 2217–2222. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.E.; Holmer, H.; Maraka, J.; Ayana, B.; Hansen, L.; Lavy, C.B.D. Cost-effectiveness of club-foot treatment in low-income and middle-income countries by the Ponseti method. BMJ Glob. Health 2016, 1, e000023. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Urban Population of Total Retrieved On. 2016. Available online: https://www.coursehero.com/file/p5tinva/World-Bank-2016-Urban-Population-of-total-Retrieved-on-March-23-2016/ (accessed on 3 April 2018).












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age of Patients (Months) | Number of Patients | Percentage (%) |
|---|---|---|
| ≤4 | 225 | 63.33 |
| >4–8 | 83 | 23.33 |
| >8–12 | 48 | 13.33 |
| Total | 356 | 100 |
| Age (Months) | Pirani Score (Pre Treatment) | Pirani Score (Last Follow Up) | Wilcoxon Z Value | p Value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| ≤4 | 5.04 | 0.85 | 0.06 | 0.21 | 5.61 | <0.0001 |
| >4–8 | 5.27 | 0.65 | 0.36 | 0.39 | 2.99 | <0.005 |
| >8–12 | 5.75 | 0.61 | 1.50 | 1.41 | 2.21 | <0.05 |
| Age (Months) | Total Number of Casts | |
|---|---|---|
| Mean | SD | |
| ≤4 | 6.56 | 0.75 |
| >4–8 | 7 | 1 |
| >8–12 | 8.33 | 1.86 |
| Age (Months) | Functional Outcome | ||
|---|---|---|---|
| Excellent | Good | Poor | |
| ≤4 | 220 (97.77%) | 03 (1.3%) | 02 (0.8%) |
| >4–8 | 53 (63.9%) | 20 (24%) | 10 (12%) |
| >8–12 | 02 (4%) | 18 (3.7%) | 28 (58.33%) |
| Total | 275 (77.2%) | 41 (11.5%) | 40 (11.2%) |
| Ponseti Method (Variables) | USD | Turcos Method (Variables) | USD |
|---|---|---|---|
| Cast and other consummables | 25 | Pre-operative antibiotics | 06 |
| Tenotomy charges | 11 | Pre-operative investigations | 12 |
| Dennis Brown (DB) Splint | 19 | Removal of stitches and k wires | 14 |
| Other hospital charges | 16 | Post-operative antibiotics | 12 |
| Hospital stay (3 days) | 26 | ||
| DB splint and ankle foot orthosis | 26 | ||
| Total | 71 | 96 |
| Studies | Unilateral (%) | Bilateral (%) |
|---|---|---|
| Ponseti et al. [7] | 40 (60%) | 27 (40%) |
| Lehman et al. [25] | 15 (50%) | 15 (50%) |
| Changulani et al. [24] | 32 (48%) | 34 (52%) |
| Christian et al. [26] | 70 (60%) | 46 (40%) |
| Pavone et al. [27] | 50 (61%) | 32 (39%) |
| Our study | 190 (53.33%) | 166 (46.67%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malhotra, R.; Mohapatra, A.; Arora, G.; Choudhury, P.; Joshi, H.; Patel, P. Ponseti Technique for the Management of Congenital Talipes Equinovarus in a Rural Set-Up in India: Experience of 356 Patients. Children 2018, 5, 49. https://doi.org/10.3390/children5040049
Malhotra R, Mohapatra A, Arora G, Choudhury P, Joshi H, Patel P. Ponseti Technique for the Management of Congenital Talipes Equinovarus in a Rural Set-Up in India: Experience of 356 Patients. Children. 2018; 5(4):49. https://doi.org/10.3390/children5040049
Chicago/Turabian StyleMalhotra, Rohit, Ashutosh Mohapatra, Geetika Arora, Priyam Choudhury, Hitesh Joshi, and Pranav Patel. 2018. "Ponseti Technique for the Management of Congenital Talipes Equinovarus in a Rural Set-Up in India: Experience of 356 Patients" Children 5, no. 4: 49. https://doi.org/10.3390/children5040049