
Modeling the Construct of an Expert Evidence-Adaptive Knowledge Base for a Pressure Injury Clinical Decision Support System

Abstract
:1. Introduction
2. Methods
2.1. Knowledge Acquisition
2.1.1. Understanding the Decision-Making
2.1.2. Determining the Decision Flow for the PI-CDSS Construct
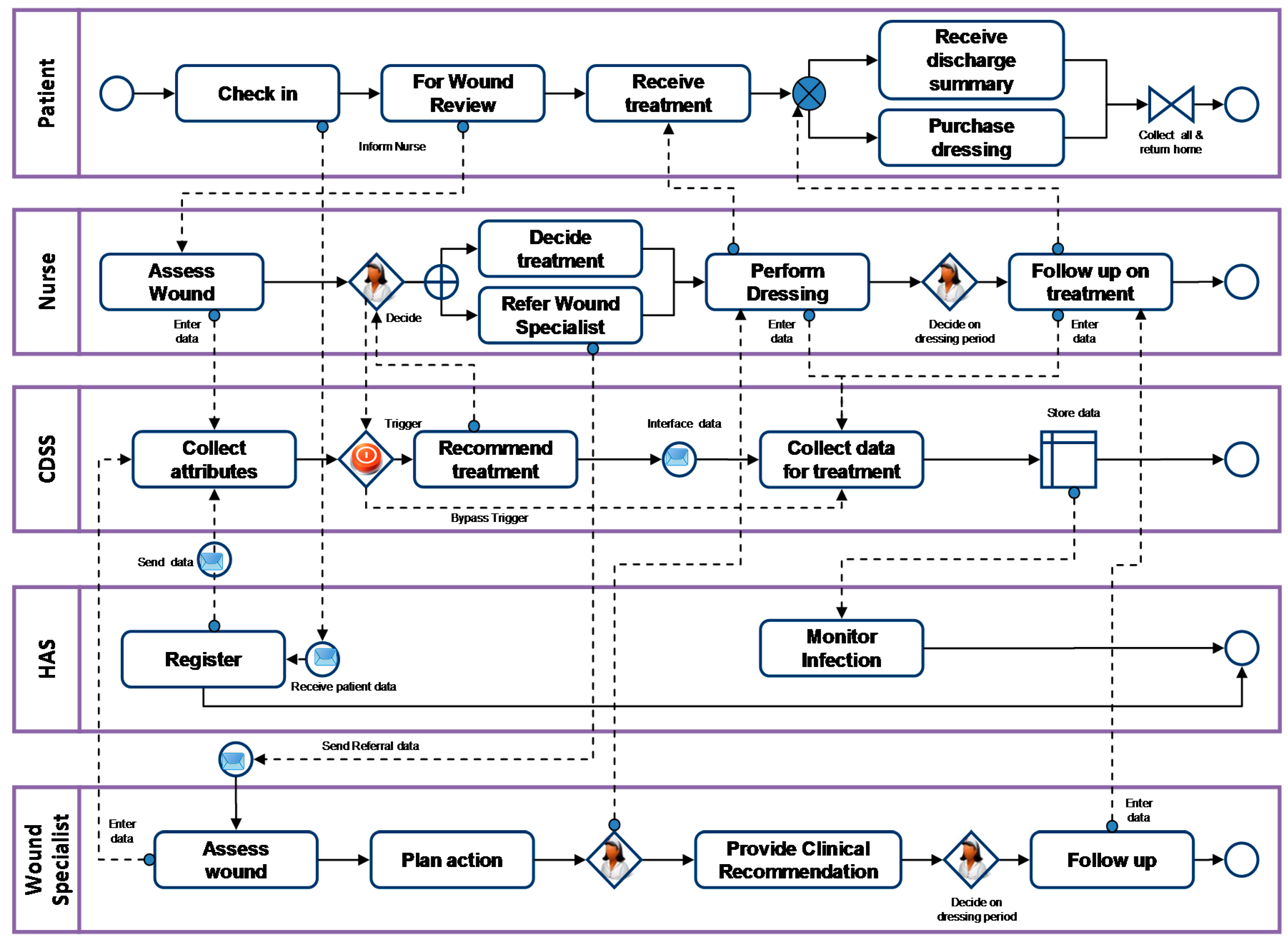
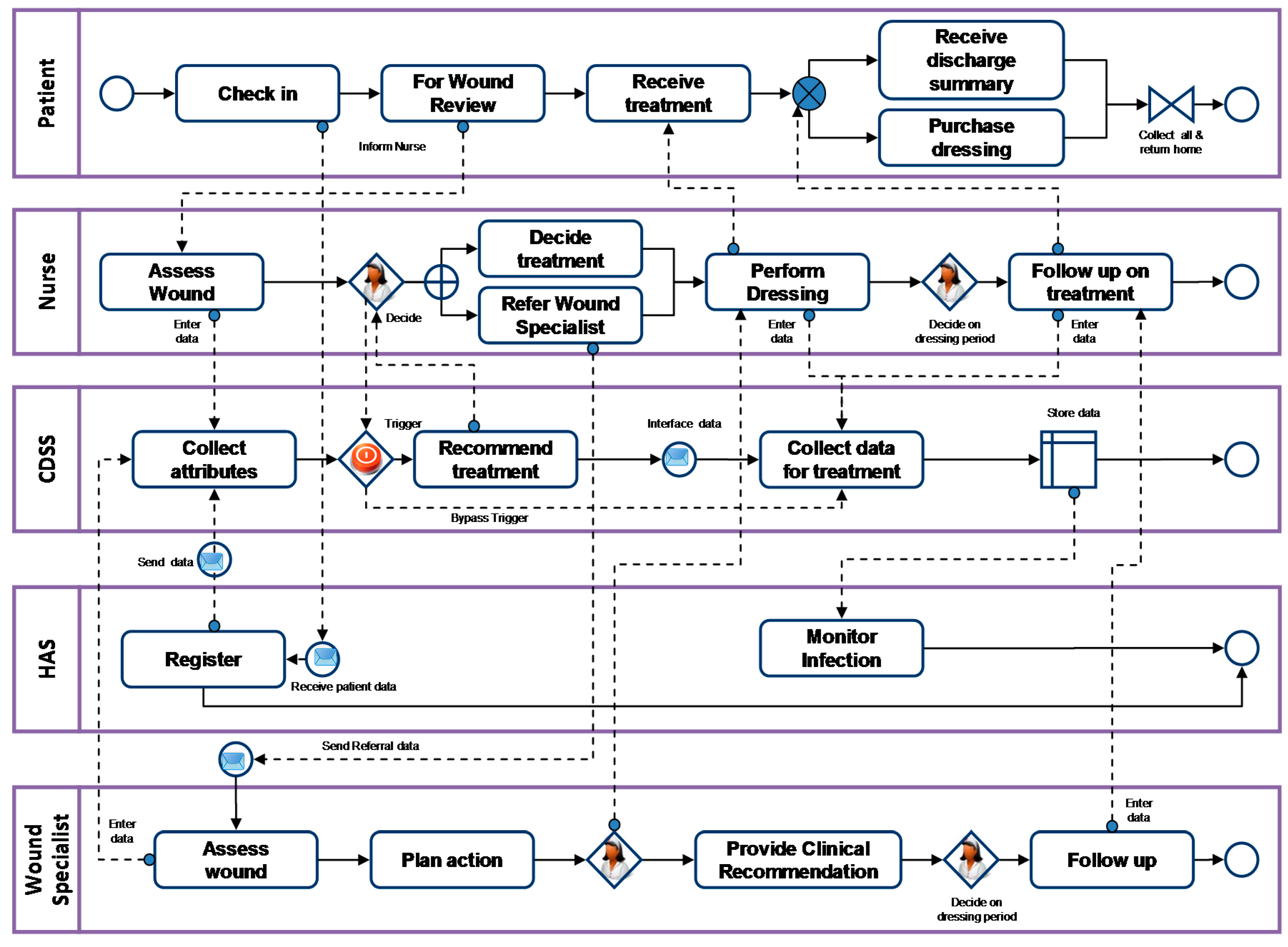
2.1.3. Modeling the Workflow
2.2. Knowledge Representation
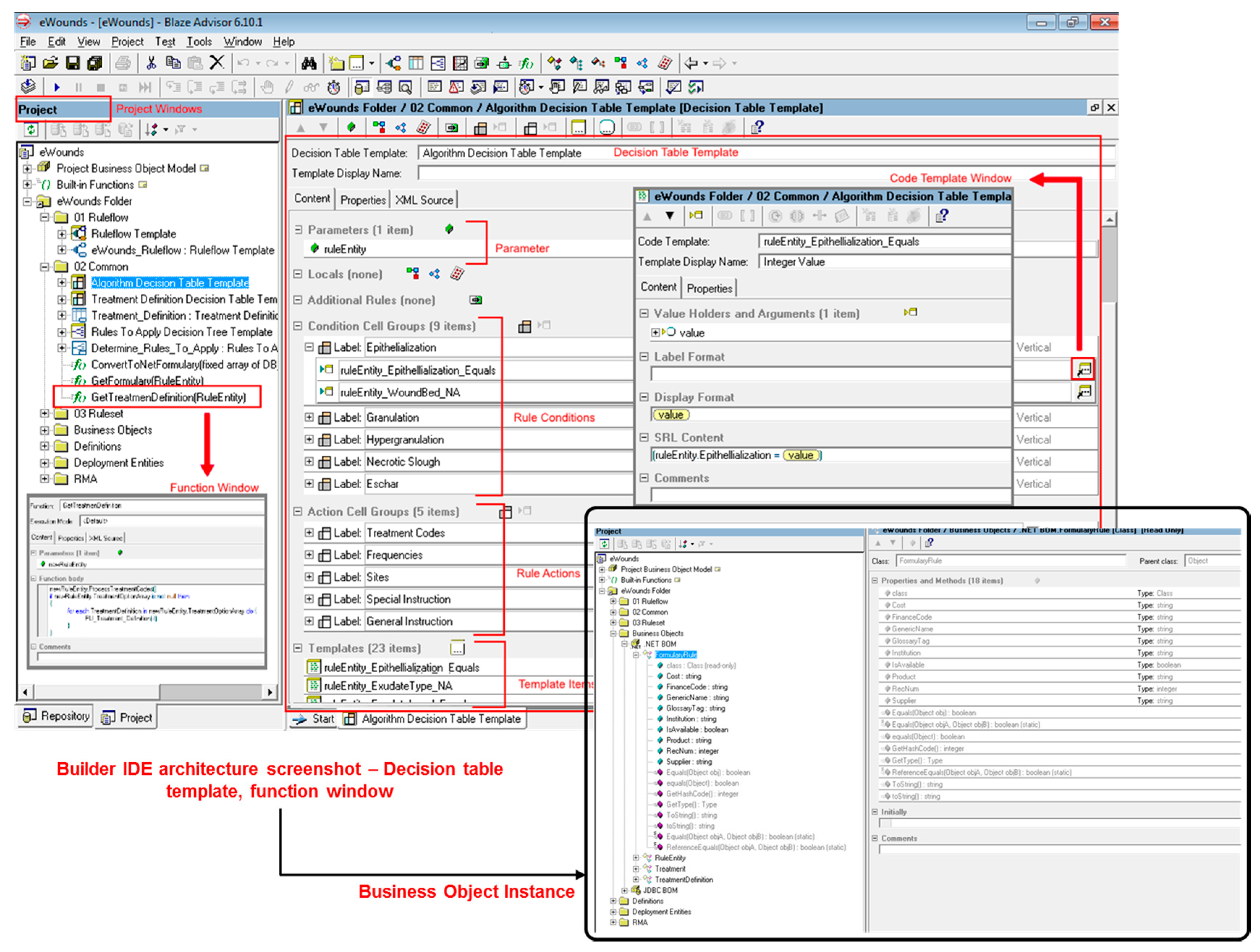
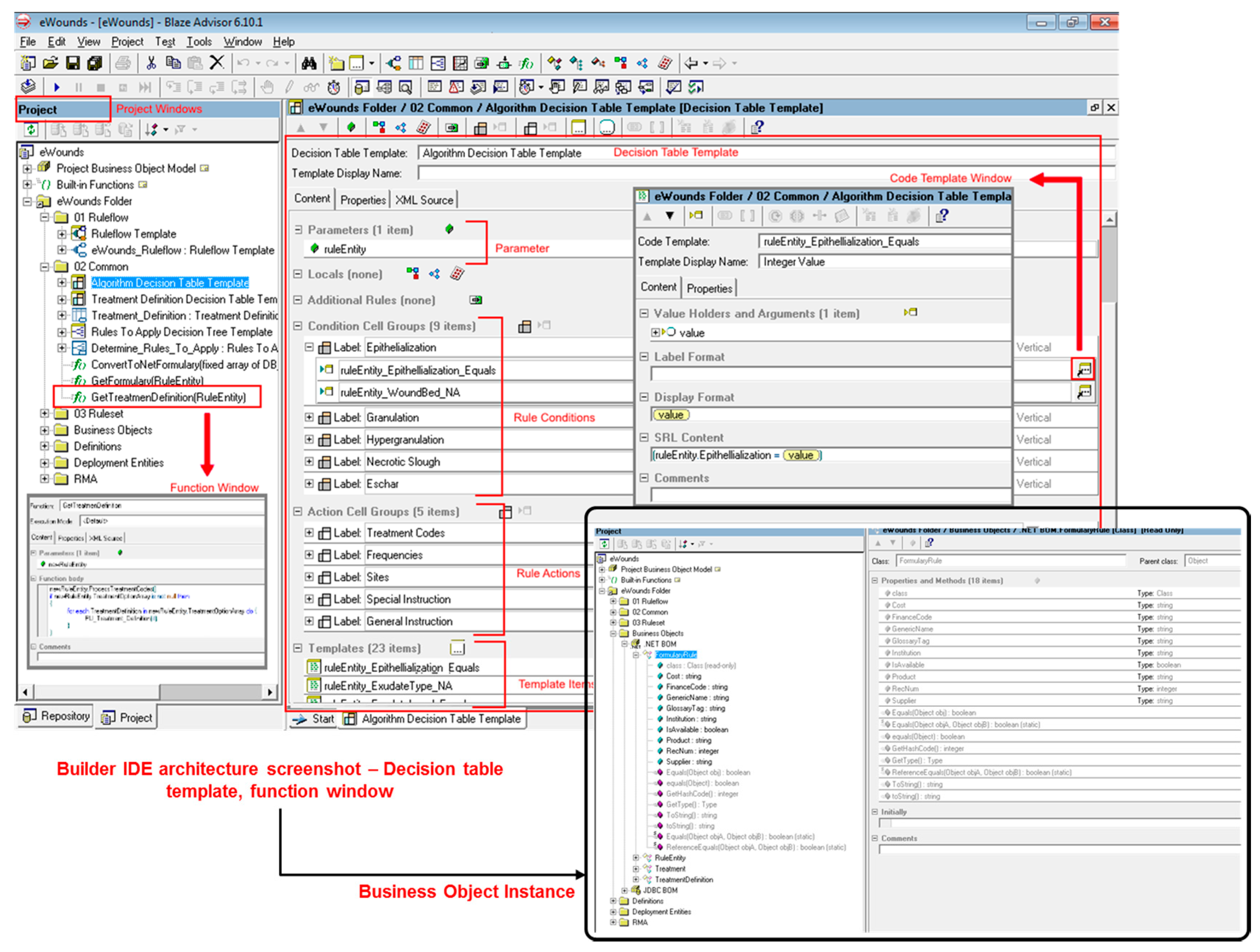
2.2.1. Engineering the Builder Integrated Development Environment
2.2.2. Defining Rule Entity
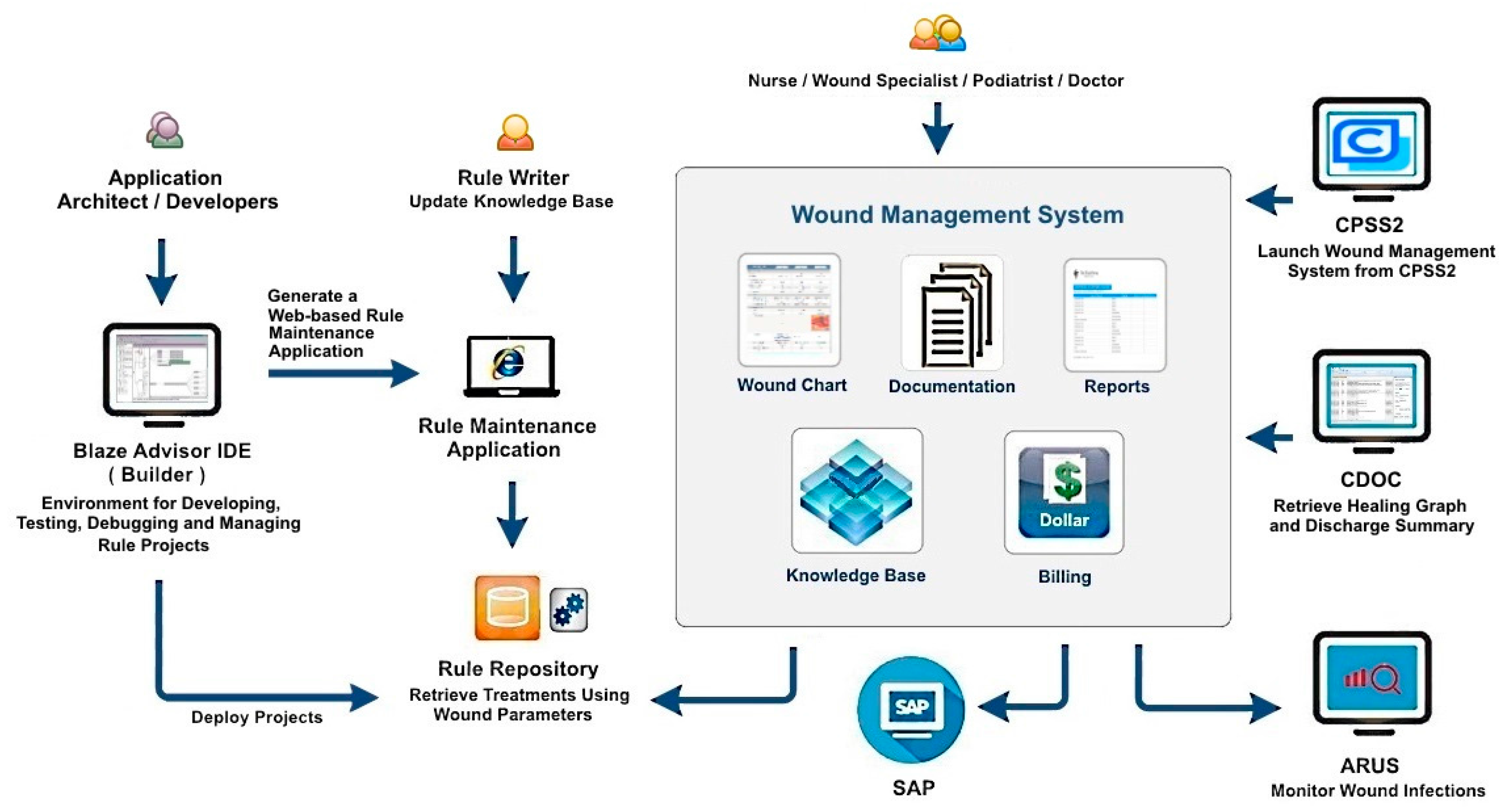
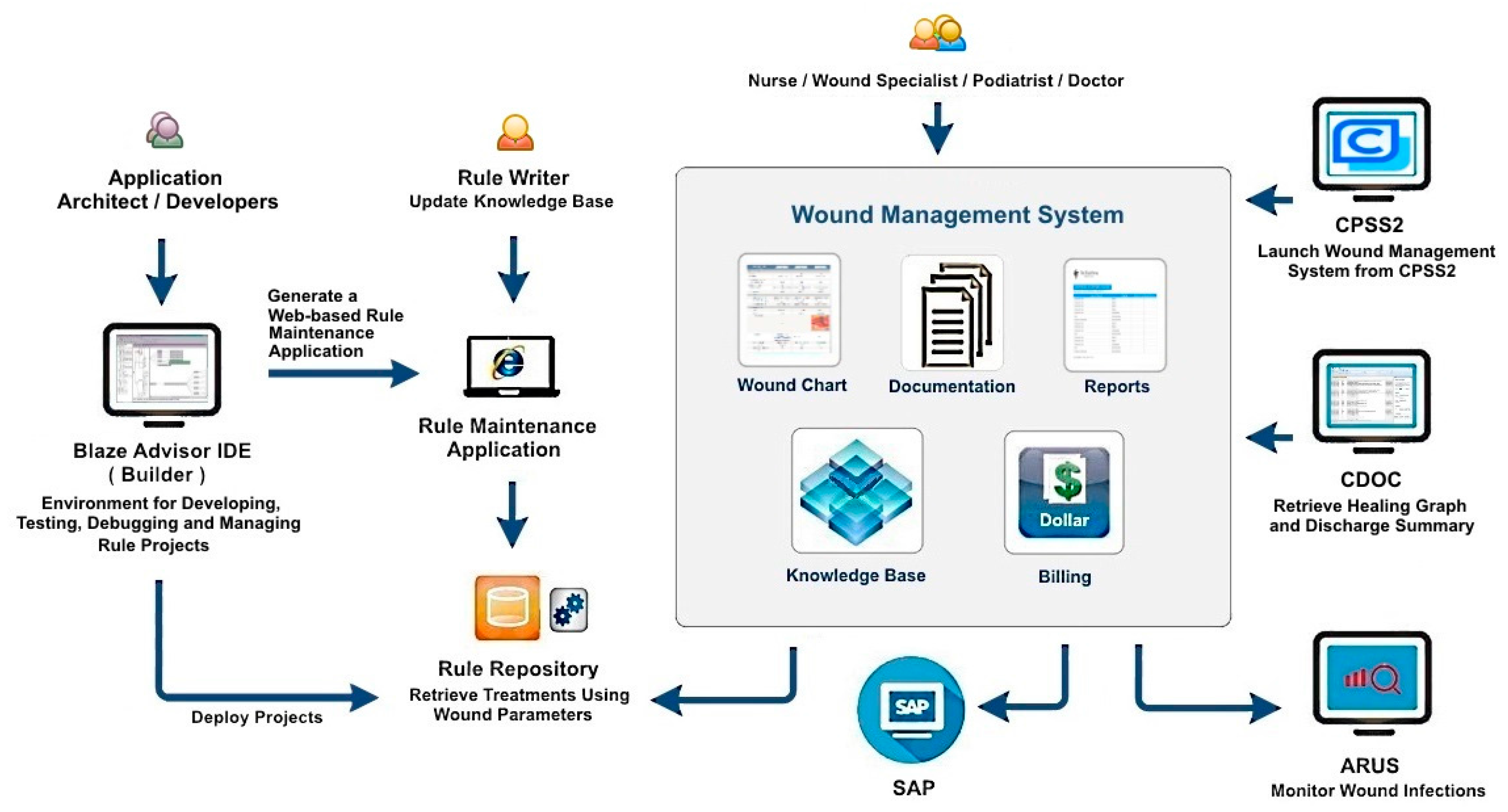
2.2.3. Designing the Architecture of the PI-CDSS Construct
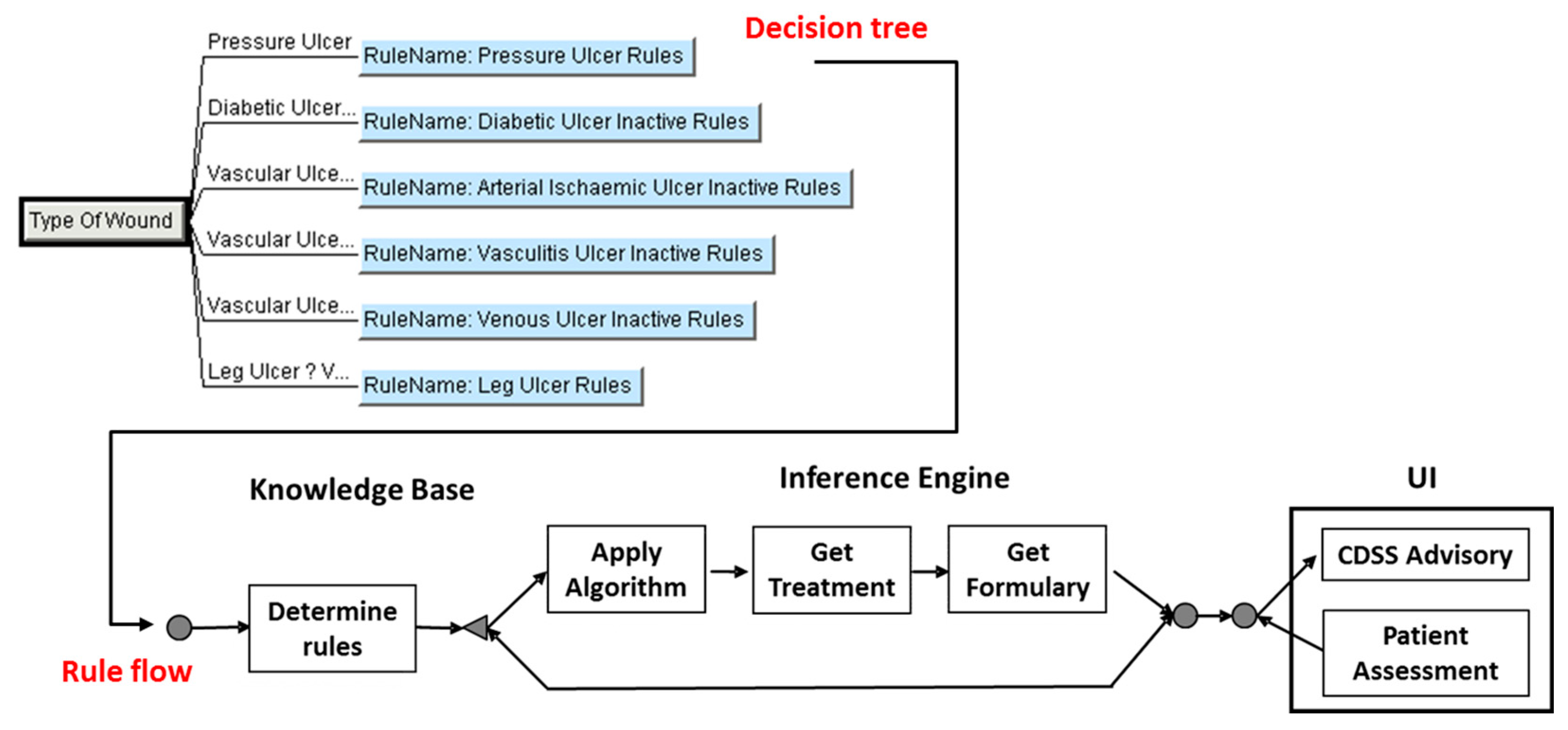
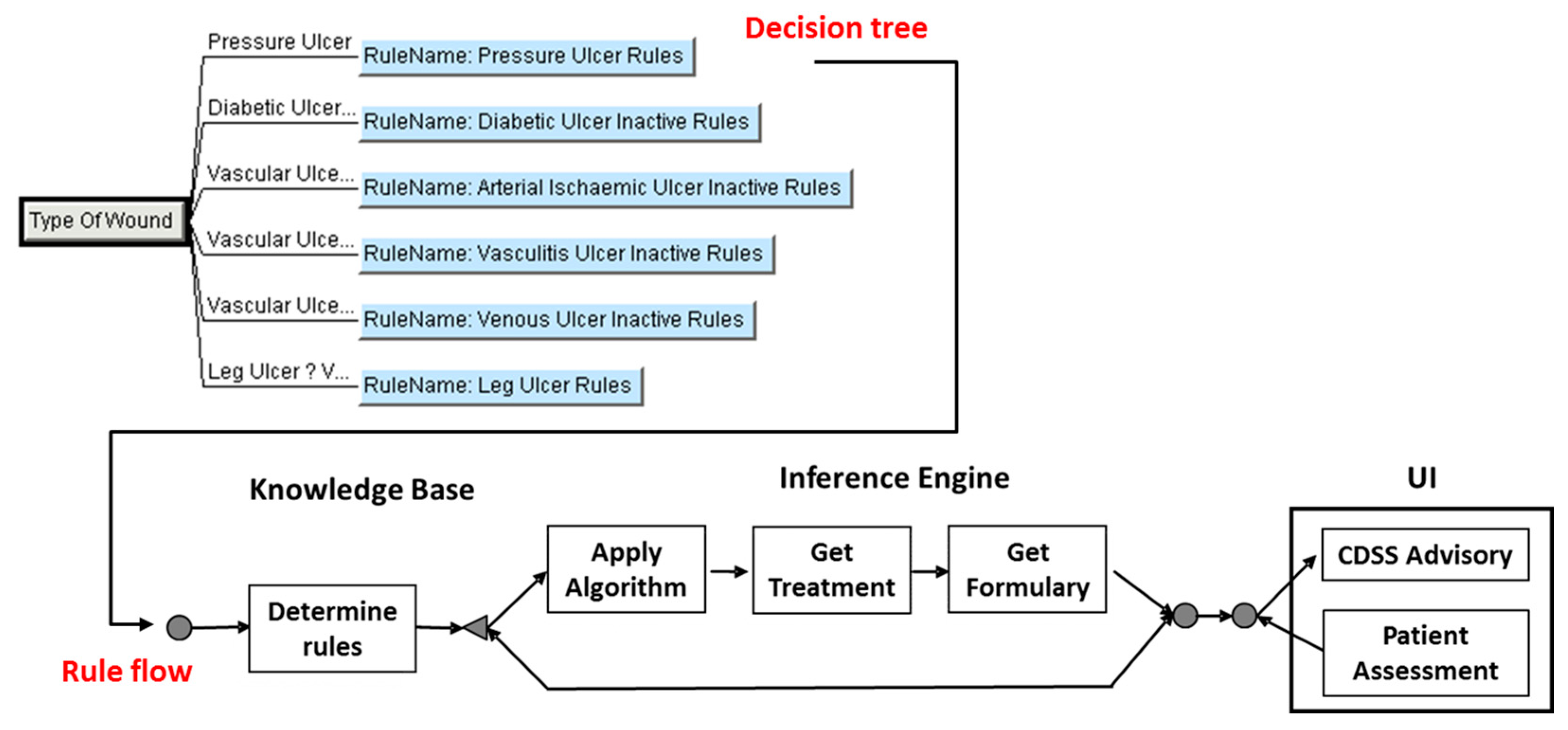
2.2.4. Representing the Decision Tree and Rule Flows
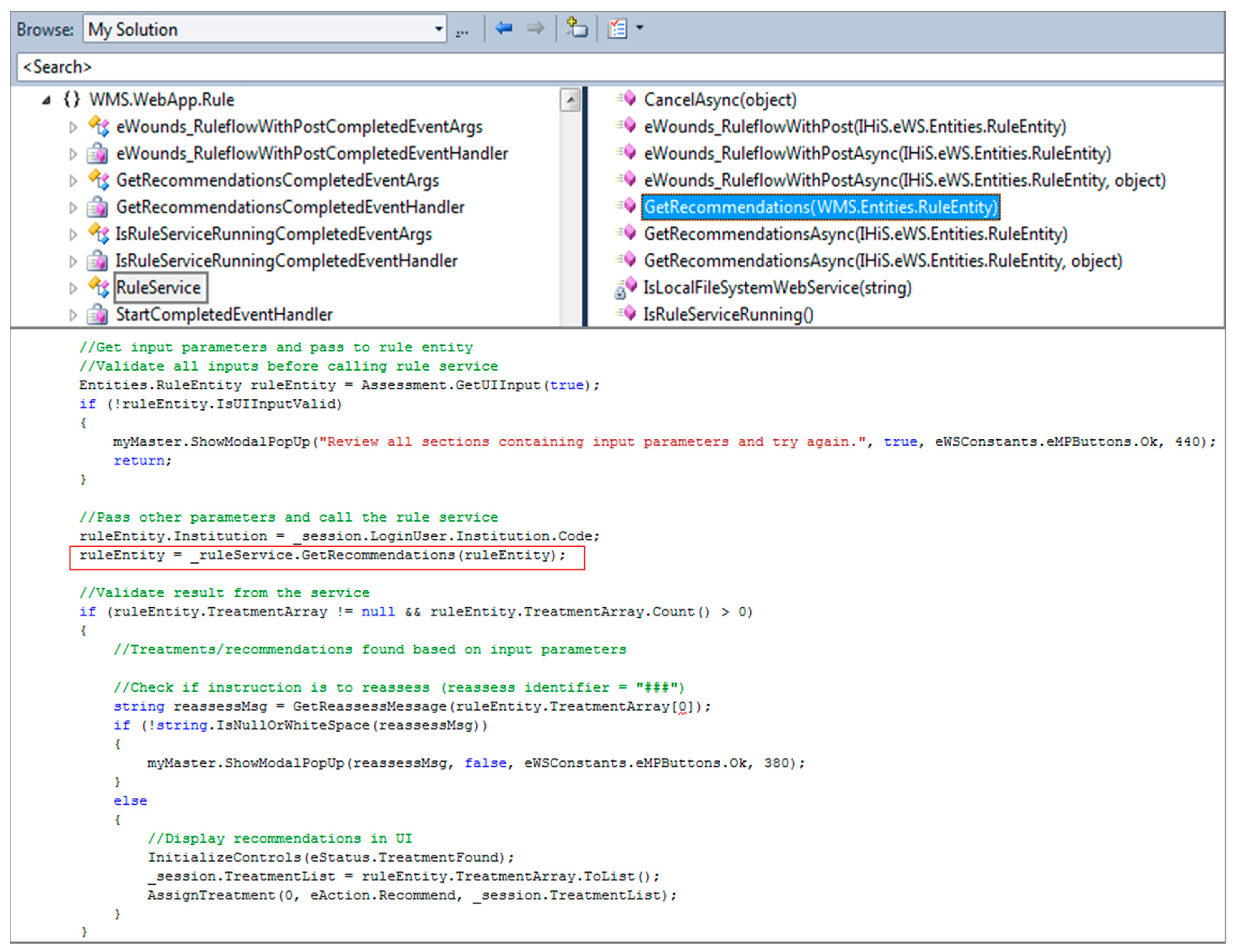
2.2.5. Deploying the Rule Project as Web Service
2.3. Knowledge Application
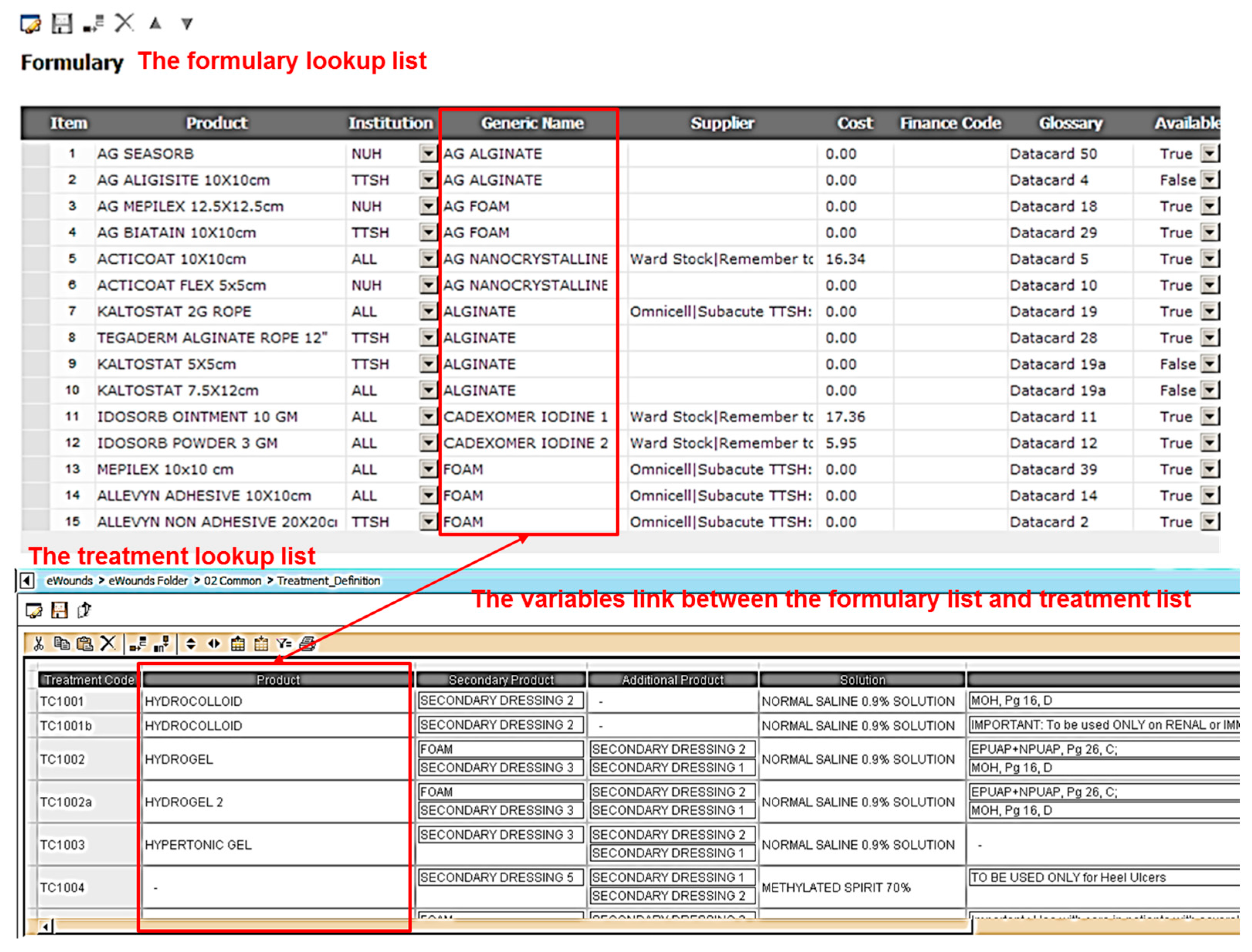
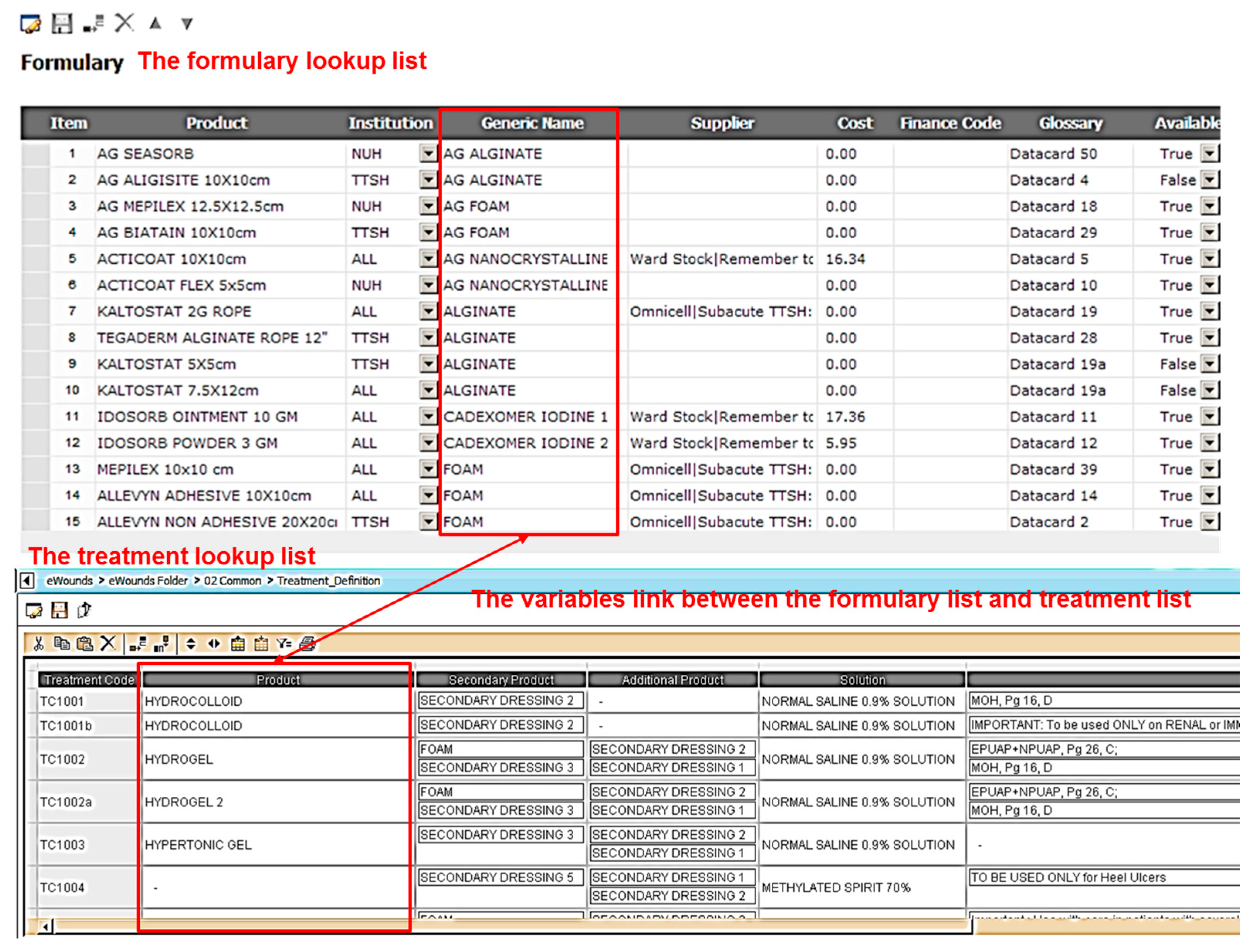
2.3.1. Specifying the Lookup Domains
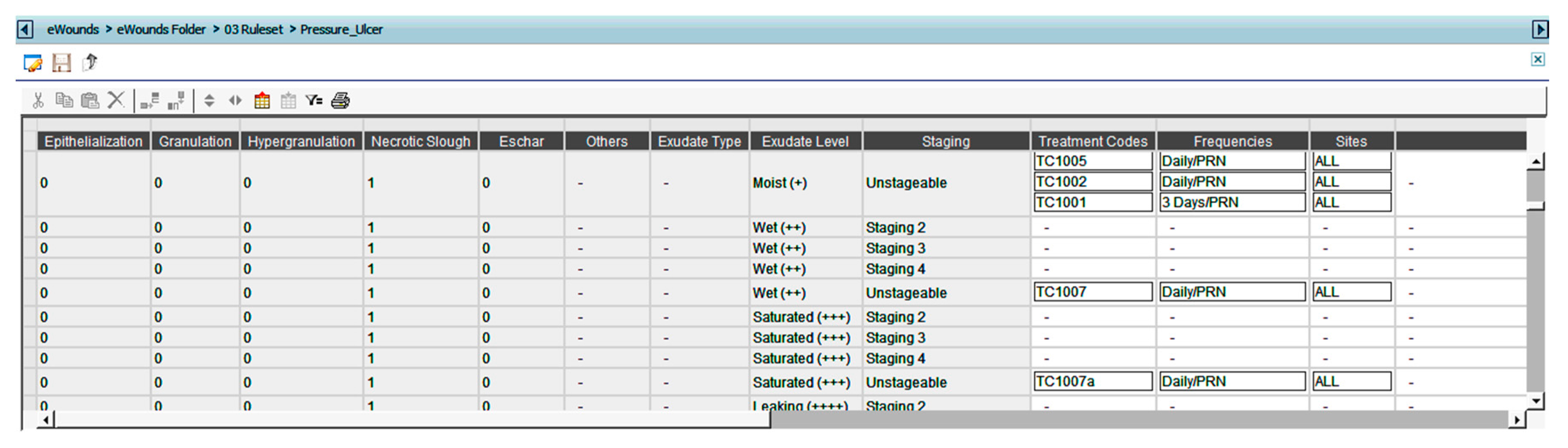
2.3.2. Authoring the Rule Sets
2.4. Knowledge Evaluation
- IF the wound type is PRESSURE ULCER,
- AND the wound bed is SLOUGHY,
- AND wound stage is UNSTAGEABLE,
- AND the exudate level is MOIST,
- THEN the treatment modalities should be
- Treatment Modality 1: Primary product = Cadexomer Iodine, AND Secondary product = FOAM AND Additional product = Transparent dressing AND Solution = Normal Saline 0.9% AND Frequency for dressing change = Daily/PRN, AND Instructions = Use with care in patients with severely impaired renal functions or a history of thyroid disorder, pregnant women, and children.
- Treatment Modality 2: Primary product = Hydrogel, AND Secondary product = FOAM, AND Additional product = Transparent dressing AND Solution = Normal Saline 0.9% AND Frequency for dressing change = Daily/PRN.
- Treatment Modality 3: Primary product = Hydrocolloid, AND Secondary product = Transparent dressing AND Solution = Normal Saline 0.9% AND Frequency for dressing change = 3 days/PRN.
3. Discussion
Limitations
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Funding
References
- Dowding, D.; Mitchell, N.; Randell, R.; Foster, R.; Lattimer, V.; Thompson, C. Nurses’ use of computerised clinical decision support systems: A case site analysis. J. Clin. Nurs. 2009, 18, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, E.S.; Dluhy, N.M.; Chin, E. Modelling novice clinical reasoning for a computerized decision support system. J. Adv. Nurs. 2005, 49, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Sittig, D.F.; Wright, A.; Osheroff, J.A.; Middleton, B.; Teich, J.M.; Ash, J.S.; Campbell, E.; Bates, D.W. Grand challenges in clinical decision support. J. Biomed. Inform. 2008, 41, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.; Glasspool, D.; Patkar, V.; Austin, M.; Black, L.; South, M.; Robertson, D.; Vincent, C. Delivering clinical decision support services: There is nothing as practical as a good theory. J. Biomed. Inform. 2010, 43, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.F.; Tian, Y.; Zhou, T.S.; Araki, K.; Li, J.S. Integrating hl7 rim and ontology for unifiedknowledge and data representation in clinicaldecision support systems. Comput. Methods Programs Biomed. 2016, 123, 94–108. [Google Scholar] [CrossRef] [PubMed]
- Sintchenko, V.; Coiera, E.; Gilbert, G.L. Decision support systems for antibiotic prescribing. Curr. Opin. Infect. Dis. 2008, 21, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Banning, M. A review of clinical decision making: Models and current research. J. Clin. Nurs. 2008, 17, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Enoch, S.; Harding, K. Wound bed preparation: The science behind the removal of barriers to healing (part 1). Wounds 2003, 15, 1–22. [Google Scholar]
- Haesler, E. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide; Cambridge Media: Osborne Park, Australia, 2014; pp. 1–72. [Google Scholar]
- Velickovski, F.; Ceccaroni, L.; Roca, J.; Burgos, F.; Galdiz, J.B.; Marina, N.; Lluch-Ariet, M. Clinical decision support systems (CDSS) for preventive management of copd patients. J. Transl. Med. 2014, 12, S9. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, M. Clinical decision support: Strategies for success. Procedia Comput. Sci. 2014, 37, 422–427. [Google Scholar] [CrossRef]
- Weiner, B.J.; Lewis, M.A.; Linnan, L.A. Using organization theory to understand the determinants of effective implementation of worksite health promotion programs. Health Educ. Res. 2009, 24, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Fico Blaze Advisor Decision Rules Management System. Available online: http://www.fico.com/cn/latest-thinking/product-sheet/fico-blaze-advisor-business-rules-management-product-sheet (accessed on 1 April 2017).
- Svatek, V.; Dudas, M.; Zamazal, O. Adapting ontologies to best-practice artifacts using transformation patterns: Method, implementation and use cases. J. Web. Semant. 2016, 40, 52–64. [Google Scholar] [CrossRef]
- Staggers, N.; Thompson, C.B. The evolution of definitions for nursing informatics: A critical analysis and revised definition. J. Am. Med. Inform. Assoc. 2002, 9, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Leslie, S.J.; Hartswood, M.; Meurig, C.; McKee, S.P.; Slack, R.; Procter, R.; Denvir, M.A. Clinical decision support software for management of chronic heart failure: Development and evaluation. Comput. Biol. Med. 2006, 36, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Wagholikar, K.B.; MacLaughlin, K.L.; Kastner, T.M.; Casey, P.M.; Henry, M.; Greenes, R.A.; Liu, H.F.; Chaudhry, R. Formative evaluation of the accuracy of a clinical decision support system for cervical cancer screening. J. Am. Med. Inform. Assoc. 2013, 20, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, S.T.R.; Thursky, K.A. Using formative evaluation to improve uptake of a web-based tool to support antimicrobial stewardship. J. Clin. Pharm. Ther. 2013, 38, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Khong, P.C.; Hoi, S.Y.; Holroyd, E.; Wang, W. Nurses’ clinical decision making on adopting a wound clinical decision support system. Comput. Inform. Nurs. 2015, 33, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Dohi, T.; Fujiwara, T. Towards quantitative software reliability assessment in incremental development processes. In Proceedings of the 33rd International Conference on Software Engineering; ACM: New York, NY, USA, 2011; pp. 41–50. [Google Scholar]
- Varonen, H.; Kortteisto, T.; Kaila, M. What may help or hinder the implementation of computerized decision support systems (CDSSs): A focus group study with physicians. Fam. Pract. 2008, 25, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, C.; Nalley, K.; Mannion, C.; Bhattacharyya, P.; Blake, P.; Pecora, A.; Goy, A.; Suh, K.S. Clinical decision support systems for improving diagnostic accuracy and achieving precision medicine. J. Clin. Bioinform. 2015, 5, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Sim, L.L.; Ban, K.H.; Tan, T.W.; Sethi, S.K.; Loh, T.P. Development of a clinical decision support system for diabetes care: A pilot study. PLoS ONE 2017, 12, e0173021. [Google Scholar] [CrossRef] [PubMed]
- El-Masri, S.; El-Sappagh, S.H. An adaptive evidence based medicine system based on a clinical decision support system. Sci. Ser. Data Rep. 2012, 4, 160–172. [Google Scholar]
- Sim, I.; Gorman, P.; Greenes, R.A.; Haynes, B.; Kaplan, B.; Lehmann, H.; Tang, P.C. Clinical decision support systems for the practice of evidence-based medicine. J. Am. Med. Inform. Assoc. 2001, 8, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Skorkowska-Telichowska, K.; Czemplik, M.; Kulma, A.; Szopa, J. The local treatment and available dressings designed for chronic wounds. J. Am. Acad. Dermatol. 2013, 68, e117–e126. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | If | AND | AND | Then | AND | AND | AND | AND |
|---|---|---|---|---|---|---|---|---|
| INPUT (Antecedent) | OUTPUT (Consequent) | |||||||
| Class | Wound Staging | Wound-Bed Appearance | Exudate Level | Primary Treatment | Secondary Treatment | Frequency | Solutions | Instruction |
| Variables | Stage 1 Stage 2 Stage 3 Stage 4 Unstageable Deep Tissue Injury | Epithelization Granulation Hyper-granulation Slough Eschar | Dry Moist Wet Saturated Leaking | FOAM with/without Ag Alginate with/without Ag Hydrocolloid Hydrogels Nanocrystalline dressing with/without Ag Cadexomer Iodine Wound contact layer Methylated Spirit 70% Hypertonic gel Hypertonic saline impregnated gauze | FOAM Gamgee Gauze Transparent dressings | 3 days 5 days EOD Daily BD TDS PRN Others | Normal saline 0.9% Water for irrigation Methylated Spirit 70% Potassium permanganate solution Povidone iodine wash | e.g., Use with care in patients with severely impaired renal functions or a history of thyroid disorder, pregnant women and children |
| Assessor | Treatment Modalities | Instructions | Alerts | No Instructions | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Total Number of Rules | Mismatched Number/Percentage | Total String Numbers | Mismatched Number/Percentage | Total String Numbers | Mismatched Number/Percentage | Total String Numbers | Mismatched Number/Percentage | ||||
| R1 | 344 | 10 | (2.9%) | 58 | 2 | (3.4%) | 173 | 19 | (11.0%) | 53 | 5 | (9.4%) |
| R2 | 344 | 53 | (15.4%) | 58 | 22 | (37.9%) | 173 | 22 | (12.7%) | 53 | 31 | (58.5%) |
| R3 | 69 | 4 | (5.8%) | 30 | 0 | (0.0%) | 21 | 1 | (4.8%) | 18 | 1 | (5.6%) |
| R4 | 64 | 4 | (6.3%) | 24 | 2 | (8.3%) | 24 | 4 | (16.7%) | 16 | 1 | (6.3%) |
| Total | 821 | 71 | (8.6%) | 170 | 26 | (15.3%) | 391 | 46 | (11.8%) | 140 | 38 | (27.1%) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khong, P.C.B.; Lee, L.N.; Dawang, A.I. Modeling the Construct of an Expert Evidence-Adaptive Knowledge Base for a Pressure Injury Clinical Decision Support System. Informatics 2017, 4, 20. https://doi.org/10.3390/informatics4030020
Khong PCB, Lee LN, Dawang AI. Modeling the Construct of an Expert Evidence-Adaptive Knowledge Base for a Pressure Injury Clinical Decision Support System. Informatics. 2017; 4(3):20. https://doi.org/10.3390/informatics4030020
Chicago/Turabian StyleKhong, Peck Chui Betty, Leng Noey Lee, and Apolino Ilagan Dawang. 2017. "Modeling the Construct of an Expert Evidence-Adaptive Knowledge Base for a Pressure Injury Clinical Decision Support System" Informatics 4, no. 3: 20. https://doi.org/10.3390/informatics4030020
APA StyleKhong, P. C. B., Lee, L. N., & Dawang, A. I. (2017). Modeling the Construct of an Expert Evidence-Adaptive Knowledge Base for a Pressure Injury Clinical Decision Support System. Informatics, 4(3), 20. https://doi.org/10.3390/informatics4030020