
Ambient Assisted Living and Health-Related Outcomes—A Systematic Literature Review


Abstract
:1. Introduction
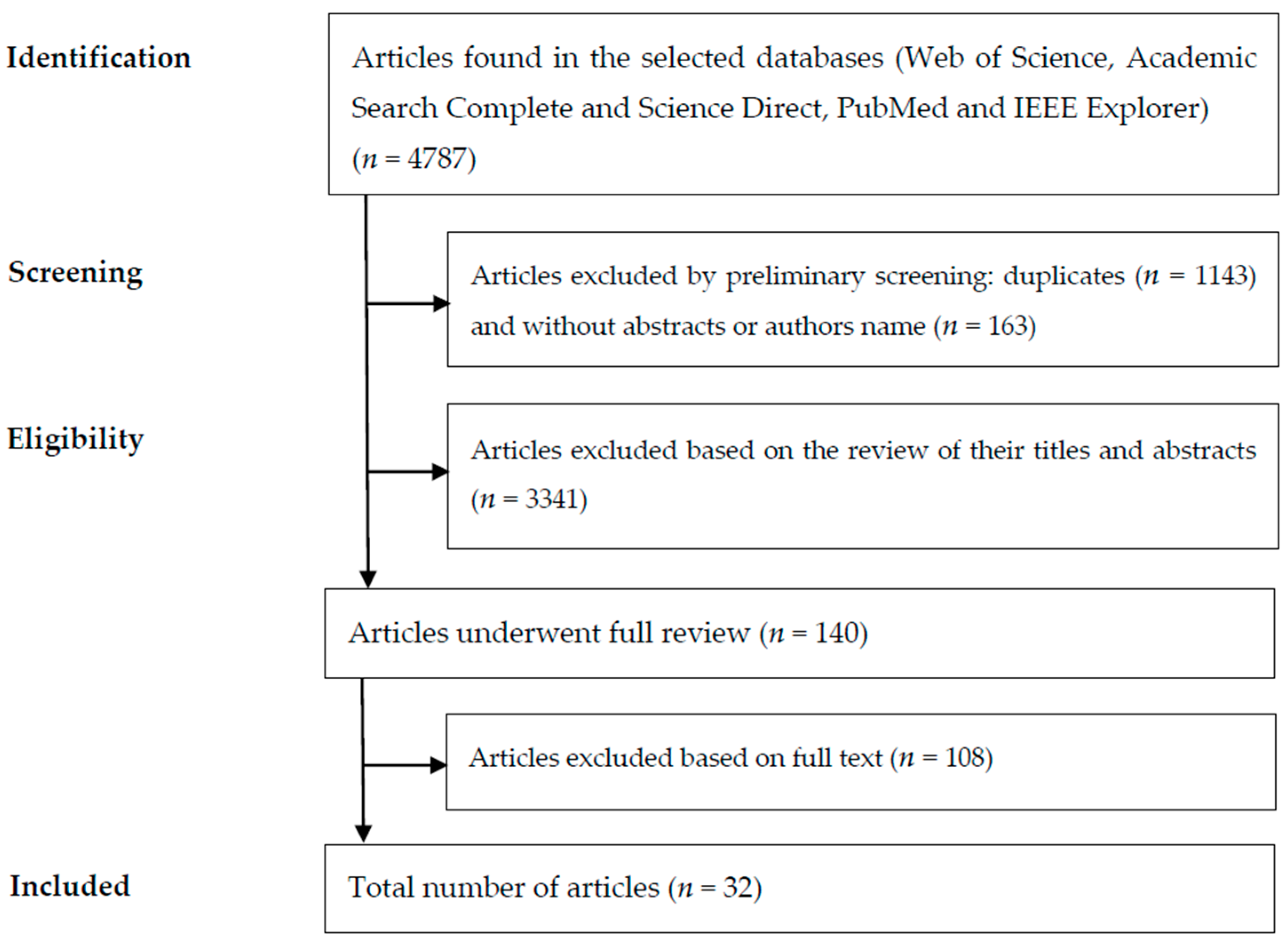
2. Materials and Methods
- What AAL solutions reported in the literature to improve health conditions were evaluated in terms of health-related outcomes?
- Does the literature present evidence on the impact of AAL solutions in terms of health-related outcomes?
- What methods are being used to measure the impact of AAL solutions in terms of health-related outcomes?
- Technologies: studies that describe the structure and rules needed to make judgments about AAL systems and how to implement them; the hardware components required for the implementation of AAL systems; the technologies and methods used to model the situation of a person, a place or object considered relevant to the interaction between a user and a system; technologies and methods that enhance the effectiveness and usability of a system and its interfaces; or studies related to privacy and security challenges imposed by AAL implementations.
- Systems: practical AAL systems applied in a specified context and with a well-defined aim.
- Conceptual articles: innovative concepts related to AAL or that may contribute to its development.
3. Results
- Activities of Daily Living (ADL) instruments: instruments that measure the skills of a person in performing basic activities, such as activities related to independent living (i.e., self-care, dressing, eating or mobility) [41].
- Instrumental Activities of Daily Living (IADL) instruments: instruments that measure the skills required for a person to live in a community, such as shopping, managing finances, housekeeping, and meal preparation [41].
- World Health Organization Quality of Life for Older Persons (WHOQOL-OLD): an instrument designed to measure the quality of life of older adults [42].
- Patient Health Questionnaire-9 (PHQ-9): a self-administered diagnostic instrument to assess depression [43].
- 10-min walking test: a test to assess disability by measuring a person’s performance [44].
- Time Up and Go: a test to measure the time it takes a person to stand up from an armchair, walk a distance of three meters, turn, walk back to the chair, and sit down [45].
- Inverted L exercise: a physical exercise where the body stays in the position of an L.
- Mini-Mental State Examination (MMSE): a screening instrument for the detection of dementia [46].
- World Health Organization Quality of Life—Brief (WHOQOL-BREF): abbreviated version of the World Health Organization Quality of Life—100 (WHOQOL-100), to assess quality of life [47].
- EuroQol five dimensions questionnaire (EQ-5D): a generic five-part questionnaire with a visual analogue self-rating scale [48] to measure health status.
- Health-threatening events in the past: a questionnaire related to house conditions, the frequency of falls, chronic diseases, previous health-threatening events, level of social support and medicine intake [33].
- Support for limitations: a questionnaire related to physical limitations during ADL or the need of support for ADL activities or for memory tasks [33].
- Center for Epidemiologic Studies Depression Scale (CES-D): a self-report instrument designed to measure depressive symptomatology [49].
- Hospital Anxiety and Depression Scale (HADS): a self-report instrument designed to detect states of depression and anxiety in a hospital or medical outpatient clinic setting [50].
- Montreal Cognitive Assessment (MOCA): an instrument designed to assess cognitive impairment [51].
- 36-Item Short Form Survey (SF-36): a 36-item self-report instrument designed to assess overall health conditions, including health-related quality of life [52].
- De Jong scale: an instrument designed to assess emotional and social loneliness [53].
- Pittsburgh Sleep Quality Index (PSQI): a self-rated questionnaire to assess sleep quality and disturbances [54].
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kinsella, K.G.; Phillips, D.R. Global Aging: The Challenge of Success; Population Reference Bureau: Washington, DC, USA, 2005; Volume 60. [Google Scholar]
- World Health Organization (WHO). Global Strategy and Action Plan on Ageing and Health; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Queirós, A.; Silva, A.G.; Alvarelhão, J.; Teixeira, A.; Da Rocha, N.P. Ambient Assisted Living Technologies, Systems and Services: A Systematic Literature Review. In Proceedings of the 2nd International Living Usability Lab Workshop on AAL Latest Solutions, Trends and Applications, Vilamoura, Algarve, Portugal, 1–4 February 2012; pp. 14–26. [Google Scholar]
- Glass, T.A.; McAtee, M.J. Behavioral science at the crossroads in public health: Extending horizons, envisioning the future. Soc. Sci. Med. 2006, 62, 1650–1671. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.M.; Machin, D. Quality of Life: The Assessment, Analysis and Interpretation of Patient-Reported Outcomes; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Porter, M.E.; Larsson, S.; Lee, T.H. Standardizing patient outcomes measurement. N. Engl. J. Med. 2016, 374, 504–506. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- European Economic and Social Comitte. Opinion of the European Economic and Social Committee on the Proposal for a Decision of the European Parliament and of the Council on the Participation by the Community in a Research and Development Programme Aimed at Enhancing the Quality of Life of Older People through the Use of new Information and Communication Technologies (ICT), Undertaken by Several Member States. Official J. Eur. Union 2008, 51, C224/02. [Google Scholar]
- Lindgren, H.; Baskar, J.; Guerrero, E.; Nieves, J.C.; Nilsson, I.; Yan, C. Computer-Supported Assessment for Tailoring Assistive Technology. In Proceedings of the 6th International Conference on Digital Health Conference, Montréal, QC, Canada, 11–13 April 2016; pp. 1–10. [Google Scholar]
- Moreno, P.A.; Hernando, M.E.; Gómez, E.J.; Del Egido, R.P.; Matilla, Ó.B.; de Poorter, A.; Ortiz, A.H.; Vidal, F.G. Teleconsulting: A Medical Application Based on IP Multimedia Subsystem Technology for Ambient Assisted Living. In Proceedings of the 2nd International Symposium on Applied Sciences in Biomedical and Communication Technologies, Bratislava, Slovakia, 24–27 November 2009; pp. 1–6. [Google Scholar]
- Leone, A.; Diraco, G.; Siciliano, P. Detecting falls with 3D range camera in ambient assisted living applications: A preliminary study. Med. Eng. Phys. 2011, 33, 770–781. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Caballero, A.; Martínez-Rodrigo, A.; Pastor, J.M.; Castillo, J.C.; Lozano-Monasor, E.; López, M.T.; Zangróniz, R.; Latorre, J.M.; Fernández-Sotos, A. Smart environment architecture for emotion detection and regulation. J. Biomed. Inf. 2016, 64, 55–73. [Google Scholar] [CrossRef] [PubMed]
- Haritou, M.; Glickman, Y.; Androulidakis, A.; Xefteris, S.; Anastasiou, A.; Baboshin, A.; Cuno, S.; Koutsouris, D. A technology platform for a novel home care delivery service to patients with dementia. J. Med. Imaging Health Inf. 2012, 2, 49–55. [Google Scholar] [CrossRef]
- Doyle, J.; Kealy, A.; Loane, J.; Walsh, L.; O’mullane, B.; Flynn, C.; Macfarlane, A.; Bortz, B.; Knapp, R.B.; Bond, R. An integrated home-based self-management system to support the wellbeing of older adults. J. Ambient Intell. Smart Environ. 2014, 6, 359–383. [Google Scholar]
- Corchado, J.M.; Bajo, J.; Abraham, A. GerAmi: Improving healthcare delivery in geriatric residences. IEEE Intell. Syst. 2008, 23. [Google Scholar] [CrossRef]
- Bono-Nuez, A.; Martín-del-Brío, B.; Blasco-Marín, R.; Casas-Nebra, R.; Roy-Yarza, A. Quality of life evaluation of elderly and disabled people by using self-organizing maps. Distrib. Comput. Artif. Intell. Bioinf. Soft Comput. Ambient Assist. Living 2009, 906–913. [Google Scholar] [CrossRef]
- Hamdan, S.; Al Osman, H.; Eid, M.; El Saddik, A. A Biofeedback System for Sleep Management. In Proceedings of the 2012 IEEE International Symposium on Robotic and Sensors Environments (ROSE), Magdeburg, Germany, 16–18 November 2012; pp. 133–137. [Google Scholar]
- Tsardoulias, E.G.; Kintsakis, A.M.; Panayiotou, K.; Thallas, A.G.; Reppou, S.E.; Karagiannis, G.G.; Iturburu, M.; Arampatzis, S.; Zielinski, C.; Prunet, V. Towards an integrated robotics architecture for social inclusion—The RAPP paradigm. Cogn. Syst. Res. 2017, 43, 157–173. [Google Scholar] [CrossRef]
- Dadlani, P.; Markopoulos, P.; Sinitsyn, A.; Aarts, E. Supporting peace of mind and independent living with the Aurama awareness system. J. Ambient Intell. Smart Environ. 2011, 3, 37–50. [Google Scholar]
- Doukas, C.; Metsis, V.; Becker, E.; Le, Z.; Makedon, F.; Maglogiannis, I. Digital cities of the future: Extending@ home assistive technologies for the elderly and the disabled. Telemat. Inf. 2011, 28, 176–190. [Google Scholar] [CrossRef]
- Fratu, O.; Pena, C.; Craciunescu, R.; Halunga, S. Fog Computing System for Monitoring Mild Dementia and COPD Patients-Romanian Case Study. In Proceedings of the 2015 12th International Conference on Telecommunication in Modern Satellite, Cable and Broadcasting Services (TELSIKS), Nis, Serbia, 14–17 October 2015; pp. 123–128. [Google Scholar]
- Leone, A.; Diraco, G.; Siciliano, P. Context-aware AAL services through a 3D sensor-based platform. J. Sens. 2013, 2013, 792978. [Google Scholar] [CrossRef]
- Zejda, D. Deep Design for Ambient Intelligence: Toward Acceptable Appliances for Higher quAlity of Life of the Elderly. In Proceedings of the 2010 Sixth International Conference on Intelligent Environments (IE), Kuala Lumpur, Malaysia, 19–21 July 2010; pp. 277–282. [Google Scholar]
- Villalba, E.; Salvi, D.; Peinado, I.; Ottaviano, M.; Arredondo, M.T. Validation Results of the User Interaction in a Heart Failure Management System. In Proceedings of the 2009 eTELEMED’09 International Conference on eHealth, Telemedicine, and Social Medicine, Cancun, Mexico, 1–7 February 2009; pp. 81–86. [Google Scholar]
- Augusto, J.; Mulvenna, M.; Zheng, H.; Wang, H.; Martin, S.; McCullagh, P.; Wallace, J. Night optimised care technology for users needing assisted lifestyles. Behav. Inf. Technol. 2014, 33, 1261–1277. [Google Scholar] [CrossRef]
- Armentia, A.; Gangoiti, U.; Priego, R.; Estevez, E.; Marcos, M. A Multi-Agent Based Approach to Support Adaptability in Home Care Applications. IFAC-PapersOnLine 2015, 48, 1–6. [Google Scholar] [CrossRef]
- Obukata, R.; Oda, T.; Barolli, L. Design of an Ambient Intelligence Testbed for Improving Quality of Life. In Proceedings of the 2016 30th International Conference on Advanced Information Networking and Applications Workshops (WAINA), Crans-Montana, Switzerland, 23–25 March 2016; pp. 714–719. [Google Scholar]
- Bono-Nuez, A.; Blasco, R.; Casas, R.; Martín-del-Brío, B. Ambient intelligence for quality of life assessment. J. Ambient Intell. Smart Environ. 2014, 6, 57–70. [Google Scholar]
- Lee, C.S.; Wang, M.H.; Acampora, G.; Hsu, C.Y.; Hagras, H. Diet assessment based on type-2 fuzzy ontology and fuzzy markup language. Int. J. Intell. Syst. 2010, 25, 1187–1216. [Google Scholar] [CrossRef]
- Mowafey, S.; Gardner, S. Towards Ambient Intelligence in Assisted Living: The Creation of an Intelligent Home Care. In Proceedings of the Science and Information Conference (SAI), London, UK, 7–9 October 2013; pp. 51–60. [Google Scholar]
- Rocha, A.; Martins, A.; Freire, J.C.; Boulos, M.N.K.; Vicente, M.E.; Feld, R.; van de Ven, P.; Nelson, J.; Bourke, A.; ÓLaighin, G. Innovations in health care services: The CAALYX system. Int. J. Med. Inf. 2013, 82, e307–e320. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, S.; De Paz, J.F.; Villarrubia, G.; Zato, C.; Bajo, J.; Corchado, J.M. Multi-agent information fusion system to manage data from a WSN in a residential home. Inf. Fusion 2015, 23, 43–57. [Google Scholar] [CrossRef]
- Siegel, C.; Prazak-Aram, B.; Kropf, J.; Kundi, M.; Dorner, T. Evaluation of a modular scalable system for silver-ager located in assisted living homes in Austria—Study protocol of the ModuLAAr ambient assisted living project. BMC Public Health 2014, 14, 736. [Google Scholar] [CrossRef] [PubMed]
- Walsh, L.; Kealy, A.; Loane, J.; Doyle, J.; Bond, R. Inferring Health Metrics from Ambient Smart Home Data. In Proceedings of the 2014 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Belfast, UK, 2–5 November 2014; pp. 27–32. [Google Scholar]
- Sixsmith, A.; Meuller, S.; Lull, F.; Klein, M.; Bierhoff, I.; Delaney, S.; Savage, R. SOPRANO—An Ambient Assisted Living System for Supporting Older People at Home. In Proceedings of the International Conference on Smart Homes and Health Telematics, Tours, France, 1–3 July 2009; pp. 233–236. [Google Scholar]
- Kaklauskas, A.; Zavadskas, E.K.; Naimavicienė, J.; Krutinis, M.; Plakys, V.; Venskus, D. Model for a complex analysis of intelligent built environment. Autom. Constr. 2010, 19, 326–340. [Google Scholar] [CrossRef]
- Aquilano, M.; Cavallo, F.; Bonaccorsi, M.; Esposito, R.; Rovini, E.; Filippi, M.; Esposito, D.; Dario, P.; Carrozza, M.C. Ambient Assisted Living and Ageing: Preliminary Results of RITA Project. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), San Diego, CA, USA, 28 August–1 September 2012; pp. 5823–5826. [Google Scholar]
- Cavallo, F.; Limosani, R.; Manzi, A.; Bonaccorsi, M.; Esposito, R.; Di Rocco, M.; Pecora, F.; Teti, G.; Saffiotti, A.; Dario, P. Development of a socially believable multi-robot solution from town to home. Cogn. Comput. 2014, 6, 954–967. [Google Scholar] [CrossRef]
- Wessig, K. Self Evolutory Systems and the Kinetics of Aging. In Proceedings of the 2015 8th International Conference on Human System Interactions (HSI), Warsaw, Poland, 25–27 June 2015; pp. 11–14. [Google Scholar]
- Pereira, F.; Carvalho, V.; Soares, F.; Machado, J.; Bezerra, K.; Silva, R.; Matos, D. Development of a Medical Care Terminal for Efficient Monitoring of Bedridden Subjects. J. Eng. 2016, 2016, 3591059. [Google Scholar] [CrossRef]
- Spector, W.D.; Fleishman, J.A. Combining activities of daily living with instrumental activities of daily living to measure functional disability. J. Gerontol. Ser. B 1998, 53, S46–S57. [Google Scholar] [CrossRef]
- Power, M.; Quinn, K.; Schmidt, S. Development of the WHOQOL-old module. Qual. Life Res. 2005, 14, 2197–2214. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Phq-9. J. Gen. Int. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Singh, S.J.; Morgan, M.; Scott, S.; Walters, D.; Hardman, A.E. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax 1992, 47, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Gerizatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Lourenço, R.A.; Veras, R.P. Mini-Mental State Examination: Psychometric characteristics in elderly outpatients. Revista de Saúde Pública 2006, 40, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Group, W. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar]
- Group, T.E. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- De Jong-Gierveld, J.; Kamphuls, F. The development of a Rasch-type loneliness scale. Appl. Psychol. Meas. 1985, 9, 289–299. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatr. Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Martins, A.I.; Queirós, A.; Silva, A.G.; Rocha, N.P. Usability Evaluation of Ambient Assisted Living Systems Using a Multi-Method Approach. In Proceedings of the 7th International Conference on Software Development and Technologies for Enhancing Accessibility and Fighting Info-exclusion, Vila Real, Portugal, 1–3 December 2016; pp. 261–268. [Google Scholar]
- Siegel, C.; Dorner, T.E. Information technologies for active and assisted living—Influences to the quality of life of an ageing society. Int. J. Med. Inf. 2017, 100, 32–45. [Google Scholar] [CrossRef] [PubMed]
- European Comission. eHealth Action Plan 2012–2020-Innovative Healthcare for the 21st Century; European Comission: Brussels, Belgium, 2012. [Google Scholar]
- Korhonen, I.; Barddram, J. Guest editorial introduction to the special section on pervasive healthcare. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, P.; Mihailidis, A. A Survey on Ambient-Assisted Living Tools for Older Adults. IEEE J. Biomed. Health Inf. 2013, 17, 579–590. [Google Scholar] [CrossRef]


{kind=link}
| Ref. | Year | Objective |
|---|---|---|
| [9] | 2016 | Development of automated methods to infer behaviors such as anxiety, poor sleep, depression and loneliness in order to tailor assistive technology for the purpose of providing just-in-time adaptive interventions targeting multiple domains. |
| [10] | 2009 | Development of a medical teleconsulting application based on the IP Multimedia Subsystem (IMS). |
| [11] | 2011 | Development and test of a real-time system based on a self-calibrated 3D time-of-flight camera to detect the falls of older adults. |
| [12] | 2016 | Detection of a patient’s emotional state by analyzing their physiological signals, facial expressions and behaviors. |
| [13] | 2012 | Application of the AAL paradigm to increase the quality of life of patients by developing novel devices and applications to enhance contact with their daily environments. |
| [14] | 2014 | Designing, deploying and testing an integrated home-based AAL system for older adults, consisting of ambient monitoring, behavior recognition and feedback to support self-management of wellness. |
| [15] | 2008 | Development of Geriatric Ambient Intelligence: an intelligent environment that integrates multi-agent systems, mobile devices, RFID, and Wi-Fi technologies to facilitate the management and control of geriatric residences, allowing case-based planning, the scheduling of functionalities and the facilitation of patient data. |
| [16] | 2009 | Development of a tool to evaluate the quality of life of older adults based on kitchen activity extracted from data provided by appliances. |
| [17] | 2012 | Use of biofeedback systems to measure, quantify and improve the quality of sleep. |
| [18] | 2016 | Development of a cloud-based integrated approach that enables robotic devices to seamlessly deploy robotic applications, relieving the robots themselves from computational burdens. |
| [19] | 2011 | Design and evaluation of Aurama: a system to support the awareness of older adults living alone. |
| [20] | 2010 | Overview of technical and other issues in extending at-home (@home) assistive technologies for older adults and disabled people. |
| [21] | 2015 | Presentation of a monitoring system, eWALL, that conforms Romanian healthcare regulations and the requirements of procedures for Chronic Obstructive Pulmonary Disease and Mild Dementia patients. |
| [22] | 2013 | Monitoring platform based on 3D sensors for AAL services delivered in smart environments. |
| [23] | 2010 | Design approach, considering not only tasks but also the immediate emotions or habits and behaviors of users. |
| [24] | 2009 | Products developed in the European MyHeart Project that intends to perform heart monitoring using wearable garments and portable devices. |
| [25] | 2014 | Nighttime support of people in the early stages of dementia. |
| [26] | 2015 | Development of a generic infrastructure that manages distributed applications for home care. |
| [27] | 2016 | AmI testbed, investigating the performance of OLSR and WEP in indoor environments, considering a Line-of-Sight scenario. |
| [28] | 2014 | Application of context awareness and artificial intelligence to provide digested and objective information about the evolution of a person’s quality of life. |
| [29] | 2010 | Combination of type-2 fuzzy sets and ontology models for diet assessment. |
| [30] | 2013 | The living environment as a pseudo robot, providing a non-invasive, self-learning, intelligent control system that constantly adapts to the requirements of individuals. |
| [31] | 2013 | Development of the Complete Ambient Assisted Living eXperiment (CAALYX) system. |
| [32] | 2015 | A Multi-Agent System (MAS) specifically designed to manage data from Wireless Sensor Networks deployed in a residential home for older adults. |
| [33] | 2014 | Analysis of the technology acceptance and the effects of AAL on the quality of life of people at an advanced age living in assisted-living homes. |
| [34] | 2014 | Association between permanently deployed ambient sensors as part of smart aware apartments and clinically validated health-condition questionnaires. |
| [35] | 2009 | The Service-oriented programmable smart environments for older Europeans (SOPRANO) and its technical components as part of a socio-technical system that models both the human and machine domains within a single conceptual framework. |
| [36] | 2010 | Analysis of an intelligent built environment by undertaking a complex analysis of micro, meso and macro environment factors affecting an intelligent built environment in order to present recommendations on how to increase efficiency and the ability to improve an inhabitant's quality of life. |
| [37] | 2012 | Development of a technological platform to support innovative care provision allowing remote health and physical monitoring as well as cognitive and behavioral assessment. |
| [38] | 2014 | Development and demonstration of the general feasibility, scientific or technical effectiveness, social or legal plausibility, and the acceptability by end-users of cooperating robots integrated with smart environments and acting in heterogeneous environments such as homes, condominiums and the outdoors. |
| [39] | 2015 | Biofeedback system to prevent inactivity (often associated with blue moods and depression, atrophy and a rapid decrease of the plasticity of the brain and the aging of neural cells). |
| [40] | 2016 | Development of a mechatronic system to withdraw patients from their beds for bathing and basic healthcare as well as the development of a Medical Care Terminal (MCT) to collect physiological data from the patient. |
| Area | Articles |
|---|---|
| Conceptual articles | [9] |
| Technologies | - |
| Architecture | [10,22,25,26] |
| Sensors network | [32] |
| Development methods | [11,12,27,29,30] |
| User interaction | [20,23,24,35,36] |
| Systems | - |
| Home monitoring | [9,13,14,28,31,33,34,37,39] |
| Other health care applications | [15,16,17,21] |
| Participation | [18,19] |
| Evaluation Type | Article (Presence of User Involvement) |
|---|---|
| Functional requirements | [14,15,18,19,31,35,37,39] |
| Conceptual validation | [15,16,19,24,25,26,28,36] |
| Prototype | [11,12,15,16,17,18,19,24,25,28,30,31,35,38,40] |
| Pilot | [9,13,14,18,19,24,25,28,29,30,31,32,33,34] |
| Time | Prototype | Pilot |
|---|---|---|
| Not referred | 23 | 16 |
| <1 month | 2 | 2 |
| >1 month And <3 months | 1 | 0 |
| >3 months And <3 months | 1 | 0 |
| >6 months And <3 months | 0 | 1 |
| >12 months | 0 | 2 |
| Phase | Article | Evaluation Techniques |
|---|---|---|
| Functional requirements | [37] | Instruments to measure ADL and IADL, WHOQOL-OLD and questionnaires |
| [39] | Questionnaires | |
| [18] | Focus group | |
| Conceptual validation | [28] | Brainstorming |
| Prototype | [19] | Interviews and questionnaires |
| [17] | Questionnaires | |
| [25] | Personas and scenarios, focus group and questionnaires | |
| [26] | Scenarios | |
| [12] | PHQ-9 | |
| [18] | Usability tests, 10-min walking test, TUG and inverted L exercise | |
| [27] | Simulation | |
| Pilot | [19] | Connectedness questionnaires, usability tests (adapted questionnaire), expectation questionnaires |
| [28] | Usability tests (heuristic evaluation) | |
| [33] | MMSE, WHOQOL-BREF, WHOQOL-OLD, EQ5D, focus groups, TAEG, usability tests, interviews, perceived system satisfaction, frequency of usage (technical analysis), sociodemographic parameters, health threatening event in the past and support for limitations | |
| [14] | Wellbeing questionnaire, interviews, CES-D, HADS, MOCA, SF-36, DE Jong scale and PSQI | |
| [34] | Wellbeing questionnaire, interviews, CES-D, HADS, MOCA, SF-36, DE Jong scale and PSQI |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Queirós, A.; Dias, A.; Silva, A.G.; Rocha, N.P. Ambient Assisted Living and Health-Related Outcomes—A Systematic Literature Review. Informatics 2017, 4, 19. https://doi.org/10.3390/informatics4030019
Queirós A, Dias A, Silva AG, Rocha NP. Ambient Assisted Living and Health-Related Outcomes—A Systematic Literature Review. Informatics. 2017; 4(3):19. https://doi.org/10.3390/informatics4030019
Chicago/Turabian StyleQueirós, Alexandra, Ana Dias, Anabela G. Silva, and Nelson Pacheco Rocha. 2017. "Ambient Assisted Living and Health-Related Outcomes—A Systematic Literature Review" Informatics 4, no. 3: 19. https://doi.org/10.3390/informatics4030019