


In Vivo Evaluation of Regenerative Osteogenic Potential Using a Human Demineralized Dentin Matrix for Dental Application


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Dentin Particles
2.2. Preparation of SA Solution
2.3. Preparation of SA Hydrogel, DDMH and NHH
2.4. Characterization of the Formulated Hydrogels
2.5. Experimental Animals
2.5.1. Sample Size Calculation
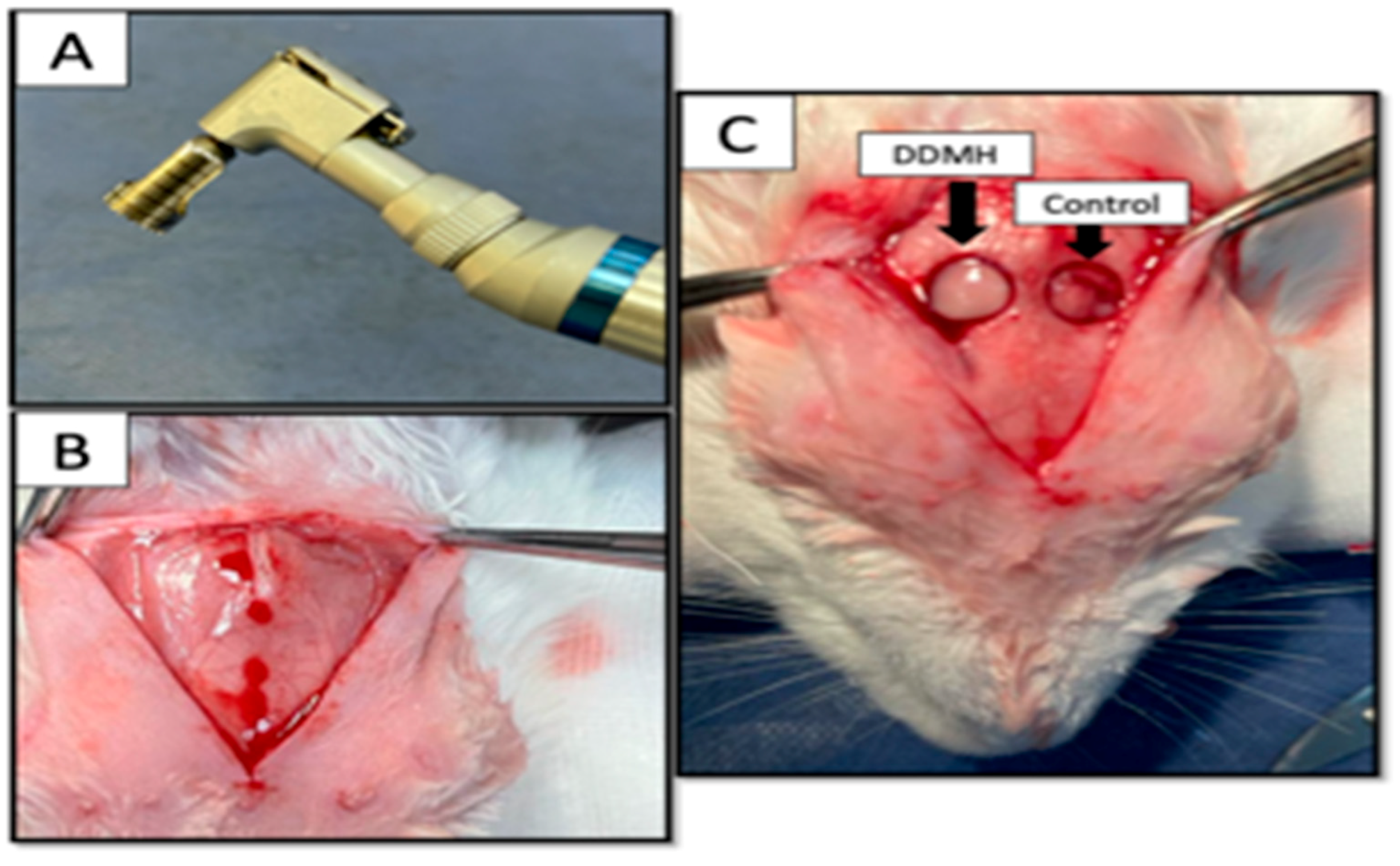
2.5.2. Surgery of Experimental Animals
2.5.3. Postoperative Care
2.5.4. Histological Analysis
2.5.5. Immunohistochemical Staining
2.5.6. Image Analysis
2.5.7. Study Design and Grouping
2.5.8. Statistical Analysis
3. Results
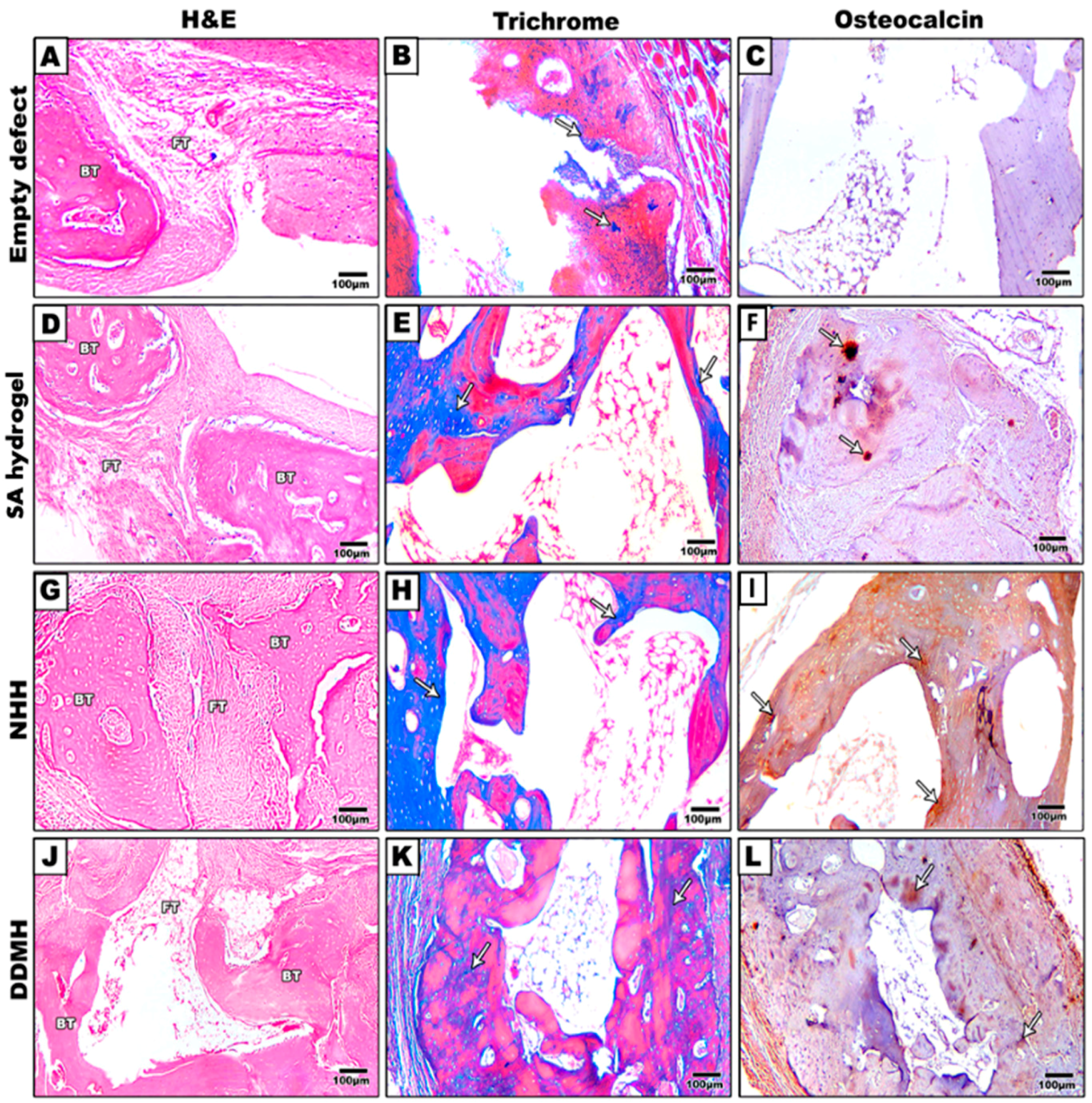
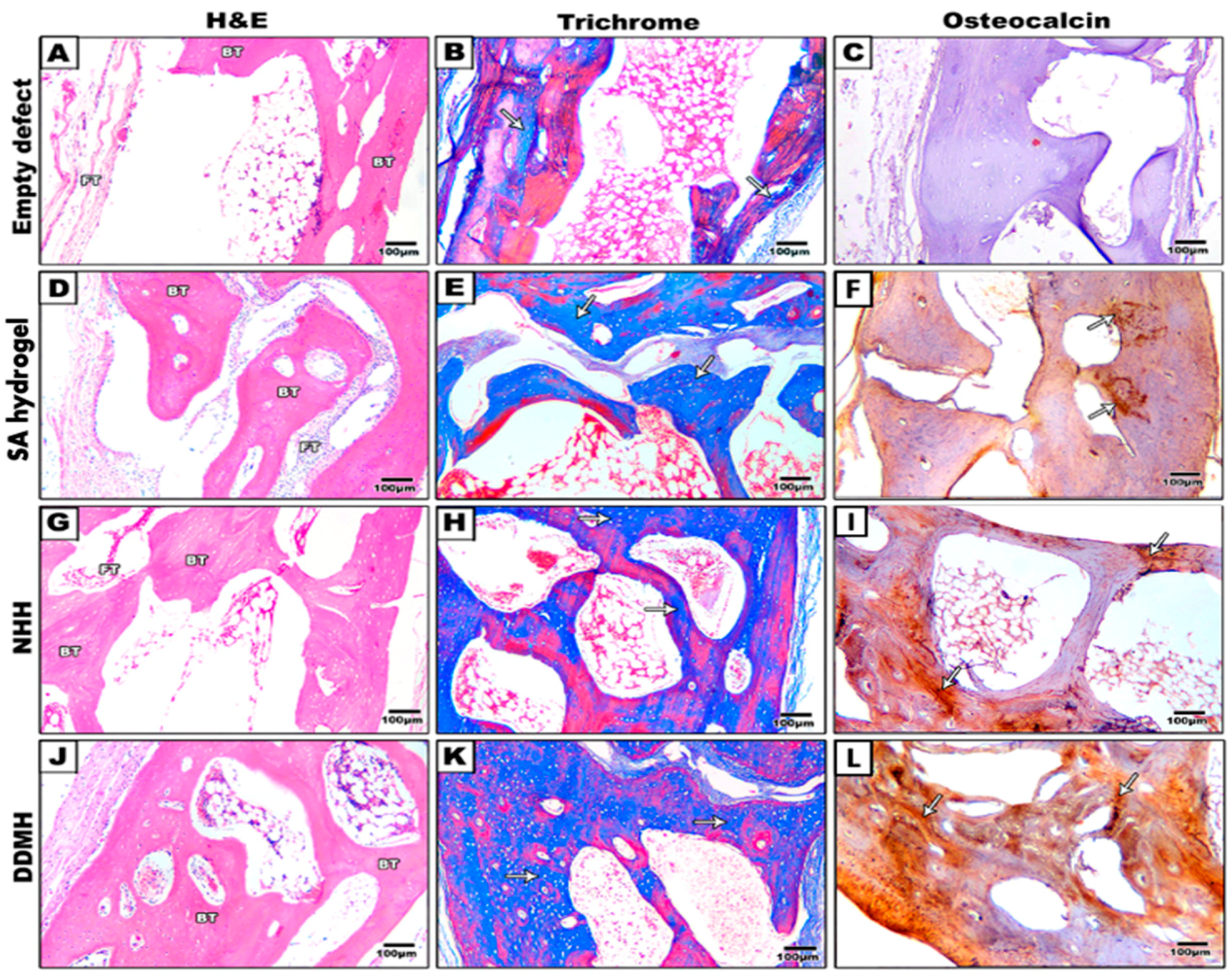
3.1. Histological Results
3.1.1. H&E Results
After 4 Weeks
After 8 Weeks
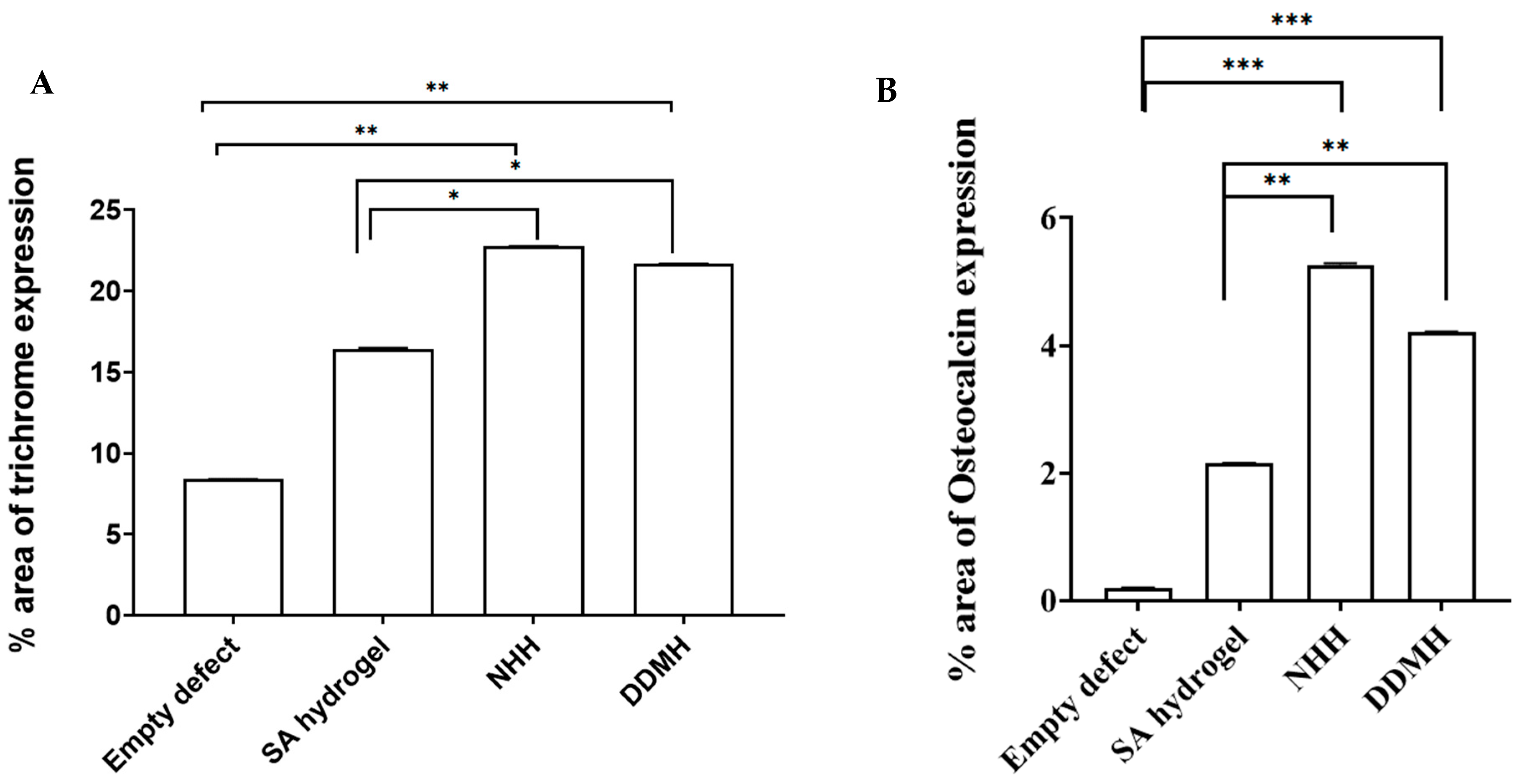
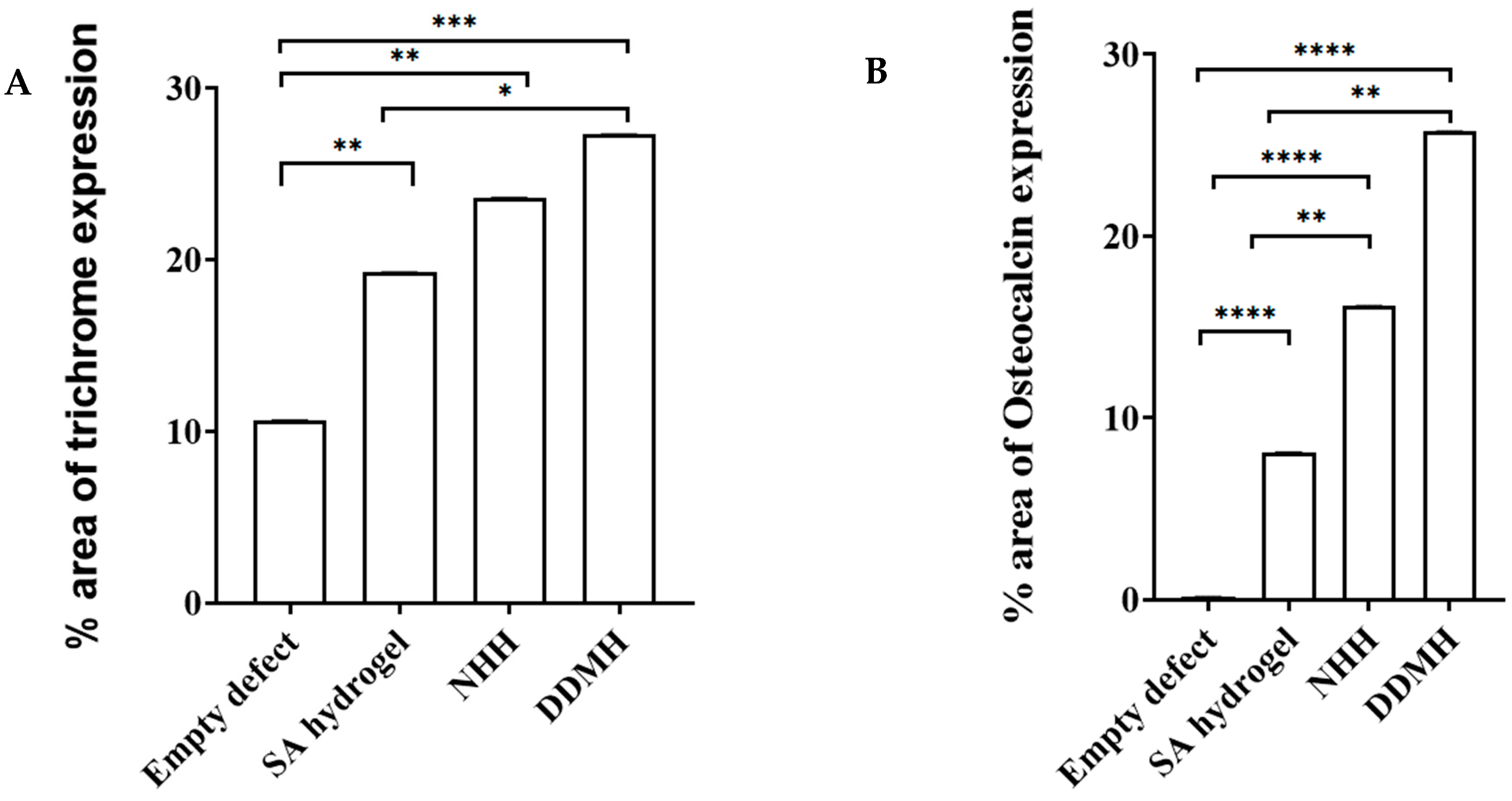
3.1.2. Masson Trichrome Staining Results
After 4 Weeks
After 8 Weeks
3.1.3. Immunohistochemical Staining
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaito, T.; Hosono, N.; Makino, T.; Kaneko, N.; Namekata, M.; Fuji, T. Postoperative displacement of hydroxyapatite spacers implanted during double-door laminoplasty. J. Neurosurg. Spine 2009, 6, 551–556. [Google Scholar] [CrossRef]
- Korkusuz, F.; Timuçin, M.; Korkusuz, P. Nanocrystalline apatite-based biomaterials and stem cells in orthopaedics. In Advances in Calcium Phosphate Biomaterials; Springer: Berlin/Heidelberg, Germany, 2014; pp. 373–390. [Google Scholar]
- Ferreira, A.M.; Gentile, P.; Chiono, V.; Ciardelli, G. Collagen for bone tissue regeneration. Acta Biomater. 2012, 9, 3191–3200. [Google Scholar] [CrossRef]
- Zizzari, V.L.; Zara, S.; Tetè, G.; Vinci, R.; Gherlone, E.; Cataldi, A. Biologic and clinical aspects of integration of different bone substitutes in oral surgery: A literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 4, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Agrali, O.B.; Yildirim, S.; Ozener, H.O.; Köse, K.N.; Ozbeyli, D.; Soluk-Tekkesin, M.; Kuru, L. Evaluation of the effectiveness of esterified hyaluronic acid fibers on bone regeneration in rat calvarial defects. BioMed Res. Int. 2018, 2018, 3874131. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Guo, W.; Yang, B.; Guo, L.; Sheng, L.; Chen, G.; Tian, W. Human treated dentin matrix as a natural scaffold for complete human dentin tissue regeneration. Biomaterials 2011, 20, 4525–4538. [Google Scholar] [CrossRef]
- Maureira, M.; Cuadra, F.; Cádiz, M.; Torres, M.; von Marttens, A.; Covarrubias, C. Preparation and osteogenic properties of nanocomposite hydrogel beads loaded with nanometric bioactive glass particles. Biomed. Mater. 2021, 4, 045043. [Google Scholar] [CrossRef]
- Jayash, S.N.; Hashim, N.M.; Misran, M.; Ibrahim, N.; Al-Namnam, N.M.; Baharuddin, N.A. Analysis on efficacy of chitosan-based gel on bone quality and quantity. Front. Mater. 2021, 8, 640950. [Google Scholar] [CrossRef]
- Jayash, S.N.; Cooper, P.R.; Shelton, R.M.; Kuehne, S.A.; Poologasundarampillai, G. Novel chitosan-silica hybrid hydrogels for cell encapsulation and drug delivery. Int. J. Mol. Sci. 2021, 22, 12267. [Google Scholar] [CrossRef]
- Sultan, N.; Jayash, S.N. Evaluation of osteogenic potential of demineralized dentin matrix hydrogel for bone formation. BMC Oral Health 2023, 23, 247. [Google Scholar] [CrossRef]
- Jing, X.; Xie, B.; Li, X.; Dai, Y.; Nie, L.; Li, C. Peptide decorated demineralized dentin matrix with enhanced bioactivity, osteogenic differentiation via carboxy- methyl chitosan. Dent. Mater. 2021, 1, 19–29. [Google Scholar] [CrossRef]
- Holiel, A.A.; Mahmoud, E.M.; Abdel-Fattah, W.M.; Kawana, K.Y. Histological evaluation of the regenerative potential of a novel treated dentin matrix hydrogel in direct pulp capping. Clin. Oral Investig. 2021, 4, 2101–2112. [Google Scholar] [CrossRef]
- Eshkol-Yogev, I.; Kaufman, A.; Haddad, M.; Zilberman, M. Cell viability of novel composite hydrogels loaded with hydroxyapatite for oral and maxillofacial bone regeneration. Odontology 2022, 110, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Kim, S.K.; Lee, J.H. Bone regeneration of demineralized dentin matrix with platelet-rich fibrin and recombinant human bone morphogenetic protein-2 on the bone defects in rabbit calvaria. Maxillofac. Plast. Reconstr. Surg. 2021, 43, 34. [Google Scholar] [CrossRef]
- Gomes, P.S.; Fernandes, M.H. Rodent models in bone-related research: The relevance of calvarial defects in the assessment of bone regeneration strategies. Lab. Anim. 2011, 45, 14–24. [Google Scholar] [CrossRef]
- Takagi, K.; Urist, M.R. The reaction of the dura to bone morphogenetic protein (BMP) in repair of skull defects. Ann. Surg. 1982, 1, 100. [Google Scholar] [CrossRef]
- Shiu, S.T.; Lee, W.F.; Chen, S.M.; Hao, L.T.; Hung, Y.T.; Lai, P.C.; Feng, S.W. Effect of different bone grafting materials and mesenchymal stem cells on bone regeneration: A micro-computed tomography and histomorphometric study in a rabbit calvarial defect model. Int. J. Mol. Sci. 2021, 22, 8101. [Google Scholar] [CrossRef] [PubMed]
- Ranganath, S.K.; Schlund, M.; Delattre, J.; Ferri, J.; Chai, F. Bilateral double site (calvarial and mandibular) critical-size bone defect model in rabbits for evaluation of a craniofacial tissue engineering constructs. Mater. Today Bio 2022, 14, 100267. [Google Scholar]
- Naguib, G.H.; Abd El-Aziz, G.S.; Almehmadi, A.; Bayoumi, A.; Mira, A.I.; Hassan, A.H.; Hamed, M.T. Evaluation of the time-dependent osteogenic activity of glycerol incorporated magnesium oxide nanoparticles in induced calvarial defects. Heliyon 2023, 9, e18757. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, P.; Lee, J.H.; Zhao, B.C.; Cai, H.; Rim, J.S.; Jang, H.S.; Lee, E.S. Microcomputed tomography and histological study of bone regeneration using tooth biomaterial with BMP-2 in rabbit calvarial defects. Scanning 2021, 2021, 6690221. [Google Scholar] [CrossRef]
- Um, I.W.; Ku, J.K.; Lee, B.K.; Yun, P.Y.; Lee, J.K.; Nam, J.H. Postulated release profile of recombinant human bone morphogenetic protein-2 (rhBMP-2) from demineralized dentin matrix. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 123. [Google Scholar] [CrossRef]
- Nam, J.W.; Kim, M.Y.; Han, S.J. Cranial bone regeneration according to different particle sizes and densities of demineralized dentin matrix in the rabbit model. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 27. [Google Scholar] [CrossRef]
- Xu, J.; Liu, Y.; Hsu, S.H. Hydrogels Based on Schiff Base Linkages for Biomedical Applications. Molecules 2019, 24, 3005. [Google Scholar] [CrossRef]
- Zheng, A.; Cao, L.; Liu, Y.; Wu, J.; Zeng, D.; Hu, L.; Jiang, X. Biocompatible silk/calcium silicate/sodium alginate composite scaffolds for bone tissue engineering. Carbohydr. Polym. 2018, 199, 244–255. [Google Scholar] [CrossRef]
- Venkatesan, J.; Bhatnagar, I.; Manivasagan, P.; Kang, K.H.; Kim, S.K. Alginate composites for bone tissue engineering: A review. Int. J. Biol. Macromol. 2015, 72, 269–281. [Google Scholar] [CrossRef]
- García-García, P.; Reyes, R.; Pérez-Herrero, E.; Arnau, M.R.; Évora, C.; Delgado, A. Alginate-hydrogel versus alginate-solid system. Efficacy in bone regeneration in osteoporosis. Mater. Sci. Eng. C 2020, 115, 111009. [Google Scholar] [CrossRef] [PubMed]
- Kamal, M.; Andersson, L.; Al-Asfour, A.; Bartella, A.K.; Gremse, F.; Rosenhain, S.; Gabato, S.; Hölzle, F.; Kessler, P.; Lethaus, B. Bone regeneration in rabbit calvarial critical-sized defects filled with composite in situ formed xenogenic dentin and biphasic tricalcium phosphate/hyroxyapatite mixture. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 3, 773–782. [Google Scholar] [CrossRef]
- Mordenfeld, A.; Hallman, M.; Lindskog, S. Tissue reactions to subperiosteal onlays of demineralized xenogenous dentin blocks in rats. Dent. Traumatol. 2011, 27, 446–451. [Google Scholar] [CrossRef]
- Al-Asfour, A.; Andersson, L.; Kamal, M.; Joseph, B. New bone formation around xenogenic dentin grafts to rabbit tibia marrow. Dent. Traumatol. 2013, 29, 455–460. [Google Scholar] [CrossRef]
- Andersson, L. Dentin xenografts to experimental bone defects in rabbit tibia are ankylosed and undergo osseous replacement. Dent. Traumatol. 2010, 26, 398–402. [Google Scholar] [CrossRef]
- Andersson, L.; Ramzi, A.; Joseph, B. Studies on dentin grafts to bone defects in rabbit tibia and mandible; development of an experimental model. Dent. Traumatol. 2009, 25, 78–83. [Google Scholar] [CrossRef]
- Fricain, J.C.; Schlaubitz, S.; Le Visage, C.; Arnault, I.; Derkaoui, S.M.; Siadous, R.; Catros, S.; Lalande, C.; Bareille, R.; Renard, M.; et al. A nano-hydroxyapatite–pullulan/dextran polysaccharide composite macroporous material for bone tissue engineering. Biomaterials 2013, 34, 2947–2959. [Google Scholar] [CrossRef]
- Fu, S.; Ni, P.; Wang, B.; Chu, B.; Peng, J.; Zheng, L.; Zhao, X.; Luo, F.; Wei, Y.; Qian, Z. In vivo biocompatibility and osteogenesis of electrospun poly (ε-caprolactone)–poly (ethylene glycol)–poly (ε-caprolactone)/nano-hydroxyapatite composite scaffold. Biomaterials 2012, 33, 8363–8371. [Google Scholar] [CrossRef]
- Liu, W.; Wei, Y.; Zhang, X.; Xu, M.; Yang, X.; Deng, X. Lower extent but similar rhythm of osteogenic behavior in hBMSCs cultured on nanofibrous scaffolds versus induced with osteogenic supplement. ACS Nano 2013, 7, 6928–6938. [Google Scholar] [CrossRef] [PubMed]
- Galle, J.; Bader, A.; Hepp, P.; Grill, W.; Fuchs, B.; Kas, J.A.; Krinner, A.; MarquaB, B.; Muller, K.; Schiller, J.; et al. Mesenchymal stem cells in cartilage repair: State of the art and methods to monitor cell growth, differentiation and cartilage regeneration. Curr. Med. Chem. 2010, 17, 2274–2291. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Feng, X.; Cao, G.; She, Z.; Tan, R.; Aifantis, K.E.; Zhang, R.; Li, X. The effect of carbon nanotubes on osteogenic functions of adipose-derived mesenchymal stem cells in vitro and bone formation in vivo compared with that of nano-hydroxyapatite and the possible mechanism. Bioact. Mater. 2021, 6, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Xu, G.; Gao, Z.; Liu, Z.; Xu, J.; Wang, J.; Zhang, C.; Wang, S. Demineralized Dentin Matrix Induces Odontoblastic Differentiation of Dental Pulp Stem Cells. Cells Tissues Organs 2016, 201, 65–76. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sultan, N.; Jayash, S.N. In Vivo Evaluation of Regenerative Osteogenic Potential Using a Human Demineralized Dentin Matrix for Dental Application. Dent. J. 2024, 12, 76. https://doi.org/10.3390/dj12030076
Sultan N, Jayash SN. In Vivo Evaluation of Regenerative Osteogenic Potential Using a Human Demineralized Dentin Matrix for Dental Application. Dentistry Journal. 2024; 12(3):76. https://doi.org/10.3390/dj12030076
Chicago/Turabian StyleSultan, Nessma, and Soher Nagi Jayash. 2024. "In Vivo Evaluation of Regenerative Osteogenic Potential Using a Human Demineralized Dentin Matrix for Dental Application" Dentistry Journal 12, no. 3: 76. https://doi.org/10.3390/dj12030076