
Long-Term Volumetric Stability of Maxillary Sinus Floor Augmentation Using a Xenograft Bone Substitute and Its Combination with Autologous Bone: A 6+ Year Retrospective Follow-Up Study Using Cone Beam Computed Tomography

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection Criteria
2.2. Maxillary Sinus Floor Augmentation (MSFA)
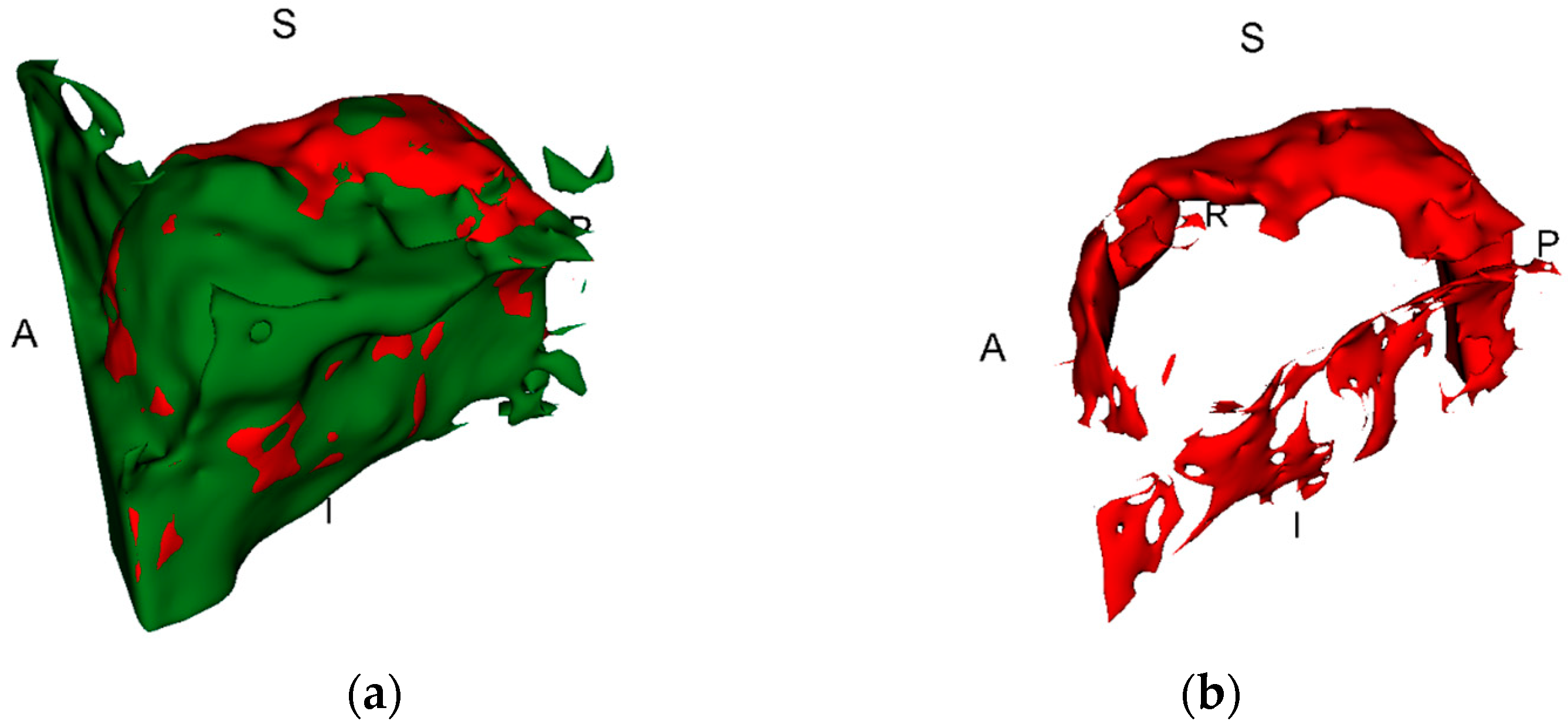
2.3. Evaluation of Volumetric Change
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iezzi, G.; Perrotti, V.; Felice, P.; Barausse, C.; Piattelli, A.; Del Fabbro, M. Are <7-mm long implants in native bone as effective as longer implants in augmented bone for the rehabilitation of posterior atrophic jaws? A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2020, 22, 552–566. [Google Scholar] [CrossRef]
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar] [PubMed]
- Starch-Jensen, T.; Deluiz, D.; Vitenson, J.; Bruun, N.H.; Tinoco, E.M.B. Maxillary Sinus Floor Augmentation with Autogenous Bone Graft Compared with a Composite Grafting Material or Bone Substitute Alone: A Systematic Review and Meta-Analysis Assessing Volumetric Stability of the Grafting Material. J. Oral Maxillofac. Res. 2021, 12, e1. [Google Scholar] [CrossRef]
- Sakkas, A.; Wilde, F.; Heufelder, M.; Winter, K.; Schramm, A. Autogenous bone grafts in oral implantology-is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int. J. Implant. Dent. 2017, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.; Schou, S.; Stavropoulos, A.; Terheyden, H.; Holmstrup, P. Maxillary sinus floor augmentation with Bio-Oss or Bio-Oss mixed with autogenous bone as graft: A systematic review. Clin. Oral Implant. Res. 2012, 23, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Starch-Jensen, T.; Deluiz, D.; Duch, K.; Tinoco, E.M.B. Maxillary Sinus Floor Augmentation With or Without Barrier Membrane Coverage of the Lateral Window: A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Res. 2019, 10, e1. [Google Scholar] [CrossRef] [PubMed]
- Rakhmatia, Y.D.; Ayukawa, Y.; Furuhashi, A.; Koyano, K. Current barrier membranes: Titanium mesh and other membranes for guided bone regeneration in dental applications. J. Prosthodont. Res. 2013, 57, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhou, Z.; Yun, J.; Liu, R.; Li, J.; Chen, Y.; Cai, H.; Jiang, H.B.; Lee, E.S.; Han, J.; et al. Effect of Different Membranes on Vertical Bone Regeneration: A Systematic Review and Network Meta-Analysis. Biomed Res. Int. 2022, 2022, 7742687. [Google Scholar] [CrossRef]
- Codari, M.; de Faria Vasconcelos, K.; Ferreira Pinheiro Nicolielo, L.; Haiter Neto, F.; Jacobs, R. Quantitative evaluation of metal artifacts using different CBCT devices, high-density materials and field of views. Clin. Oral Implant. Res. 2017, 28, 1509–1514. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Jacobs, R.; Singer, S.R.; Mupparapu, M. CBCT-based bone quality assessment: Are Hounsfield units applicable? Dentomaxillofac. Radiol. 2015, 44, 20140238. [Google Scholar] [CrossRef]
- Fontenele, R.C.; Nascimento, E.H.; Vasconcelos, T.V.; Noujeim, M.; Freitas, D.Q. Magnitude of cone beam CT image artifacts related to zirconium and titanium implants: Impact on image quality. Dentomaxillofac. Radiol. 2018, 47, 20180021. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Maxillary sinus augmentation for endosteal implants: Organized alternative treatment plans. Int. J. Oral Implantol. 1987, 4, 49–58. [Google Scholar] [PubMed]
- Jamovi. The Jamovi Project (Version 2.3) [Computer Software]. 2022. Available online: https://www.jamovi.org (accessed on 1 December 2023).
- Mazzocco, F.; Lops, D.; Gobbato, L.; Lolato, A.; Romeo, E.; del Fabbro, M. Three-dimensional volume change of grafted bone in the maxillary sinus. Int. J. Oral Maxillofac. Implant. 2014, 29, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Shanbhag, V.; Stavropoulos, A. Volume changes of maxillary sinus augmentations over time: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 881–892. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Aludden, H.; Hallman, M.; Dahlin, C.; Christensen, A.E.; Mordenfeld, A. A systematic review and meta-analysis of long-term studies (five or more years) assessing maxillary sinus floor augmentation. Int. J. Oral Maxillofac. Surg. 2018, 47, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Raghoebar, G.M.; Onclin, P.; Boven, G.C.; Vissink, A.; Meijer, H.J.A. Long-term effectiveness of maxillary sinus floor augmentation: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 307–318. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Stelzle, F. Clinical outcomes of sinus floor augmentation for implant placement using autogenous bone or bone substitutes: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. S4), 124–133. [Google Scholar] [CrossRef] [PubMed]
- Pesce, P.; Menini, M.; Canullo, L.; Khijmatgar, S.; Modenese, L.; Gallifante, G.; Del Fabbro, M. Radiographic and Histomorphometric Evaluation of Biomaterials Used for Lateral Sinus Augmentation: A Systematic Review on the Effect of Residual Bone Height and Vertical Graft Size on New Bone Formation and Graft Shrinkage. J. Clin. Med. 2021, 10, 4996. [Google Scholar] [CrossRef]
- Hatano, N.; Shimizu, Y.; Ooya, K. A clinical long-term radiographic evaluation of graft height changes after maxillary sinus floor augmentation with a 2:1 autogenous bone/xenograft mixture and simultaneous placement of dental implants. Clin. Oral Implant. Res. 2004, 15, 339–345. [Google Scholar] [CrossRef]
- Park, W.B.; Han, J.Y.; Kang, K.L. Long-Term Comparison of Survival and Marginal Bone of Implants with and without Sinus Augmentation in Maxillary Molars within the Same Patients: A 5.8- to 22-Year Retrospective Study. J. Clin. Med. 2021, 10, 1360. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Ramaglia, L.; Guidetti, F.; Sbordone, L.; Martuscelli, R. A 5-year clinical and computerized tomographic implant follow-up in sinus-lifted maxillae and native bone. Clin. Oral Implant. Res. 2014, 25, 1056–1064. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Martuscelli, R.; Guidetti, F.; Sbordone, L.; Ramaglia, L. A 5-Year Implant Follow-Up in Maxillary and Mandibular Horizontal Osseous Onlay Grafts and Native Bone. J. Oral Implantol. 2015, 41, 570–578. [Google Scholar] [CrossRef]
- Hallman, M.; Zetterqvist, L. A 5-year prospective follow-up study of implant-supported fixed prostheses in patients subjected to maxillary sinus floor augmentation with an 80:20 mixture of bovine hydroxyapatite and autogenous bone. Clin. Implant. Dent. Relat. Res. 2004, 6, 82–89. [Google Scholar] [CrossRef]
- Nyström, E.; Ahlqvist, J.; Gunne, J.; Kahnberg, K.E. 10-year follow-up of onlay bone grafts and implants in severely resorbed maxillae. Int. J. Oral Maxillofac. Surg. 2004, 33, 258–262. [Google Scholar] [CrossRef]
- Nyström, E.; Ahlqvist, J.; Legrell, P.E.; Kahnberg, K.E. Bone graft remodelling and implant success rate in the treatment of the severely resorbed maxilla: A 5-year longitudinal study. Int. J. Oral Maxillofac. Surg. 2002, 31, 158–164. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Guidetti, F.; Califano, L.; Santoro, A.; Sbordone, L. Volume changes of iliac crest autogenous bone grafts after vertical and horizontal alveolar ridge augmentation of atrophic maxillas and mandibles: A 6-year computerized tomographic follow-up. J. Oral Maxillofac. Surg. 2012, 70, 2559–2565. [Google Scholar] [CrossRef]
- Cansiz, E.; Haq, J.; Manisali, M.; Cakarer, S.; Gultekin, B.A. Long-term evaluation of three-dimensional volumetric changes of augmented severely atrophic maxilla by anterior iliac crest bone grafting. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 665–671. [Google Scholar] [CrossRef]
- Schlegel, A.K.; Donath, K. BIO-OSS—A resorbable bone substitute? J. Long Term Eff. Med. Implant. 1998, 8, 201–209. [Google Scholar]
- Iezzi, G.; Degidi, M.; Scarano, A.; Petrone, G.; Piattelli, A. Anorganic bone matrix retrieved 14 years after a sinus augmentation procedure: A histologic and histomorphometric evaluation. J. Periodontol. 2007, 78, 2057–2061. [Google Scholar] [CrossRef]
- Ferreira, C.E.; Novaes, A.B.; Haraszthy, V.I.; Bittencourt, M.; Martinelli, C.B.; Luczyszyn, S.M. A clinical study of 406 sinus augmentations with 100% anorganic bovine bone. J. Periodontol. 2009, 80, 1920–1927. [Google Scholar] [CrossRef]
- Imai, H.; Prati, C.; Zamparini, F.; Iezzi, G.; Botticelli, D.; Gandolfi, M.G.; Baba, S. ESEM-EDX Mineralization and Morphological Analysis of Human Retrieved Maxillary Sinus Bone Graft Biopsies before Loading. J. Funct. Biomater. 2023, 14, 391. [Google Scholar] [CrossRef]
- Demirturk Kocasarac, H.; Koenig, L.J.; Ustaoglu, G.; Oliveira, M.L.; Freitas, D.Q. CBCT image artefacts generated by implants located inside the field of view or in the exomass. Dentomaxillofac. Radiol. 2022, 51, 20210092. [Google Scholar] [CrossRef]
- Ludlow, J.B.; Timothy, R.; Walker, C.; Hunter, R.; Benavides, E.; Samuelson, D.B.; Scheske, M.J. Effective dose of dental CBCT-a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac. Radiol. 2015, 44, 20140197. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Sex | Age at T1 (years) | Days between MFBA and T1 | Material Used for MFBA | Membrane | Bone Volume at T1 (mm3) | Bone Volume at T2 (mm3) | T1-T2 (Including Artefacts) * | True Bone Volume Change (mm3) | True Bone Volume Change (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 57 | 236 | XG | Ti | 7908 | 6204 | 1704 | 1351 | 17% |
| 2 | M | 54 | 159 | XG + AB | - | 4900 | 3977 | 923 | 477 | 10% |
| 3 | F | 30 | 273 | XG | Ti | 6333 | 5529 | 804 | 862 | 14% |
| 4 | F | 41 | 205 | XG + AB | Ti | 3192 | 3767 | −575 | 0 | 0% |
| 5 | F | 41 | 205 | XG + AB | Ti | 3643 | 3437 | 206 | 198 | 5% |
| 6 | F | 50 | 349 | XG + AB | - | 6116 | 5536 | 580 | 263 | 4% |
| 7 | F | 51 | 680 | XG | - | 4655 | 5005 | −350 | 0 | 0% |
| 8 | M | 58 | 313 | XG | Ti | 4495 | 4653 | −158 | 39 | 1% |
| 9 | F | 38 | 353 | XG | Ti | 3526 | 2927 | 599 | 317 | 9% |
| 10 | F | 53 | 189 | XG | - | 5002 | 5135 | −133 | 165 | 3% |
| 11 | F | 56 | 277 | XG + AB | - | 5817 | 4276 | 1541 | 423 | 7% |
| 12 | F | 39 | 185 | XG | BG | 3947 | 3626 | 321 | 53 | 1% |
| 13 | M | 49 | 217 | XG | BG | 23,688 | 25,802 | −2114 | 119 | 1% |
| 14 | M | 49 | 217 | XG | BG | 23,688 | 25,802 | −2114 | 304 | 1% |
| 15 | M | 47 | 138 | XG | Ti | 5169 | 4743 | 426 | 17 | 0% |
| 16 | F | 56 | 167 | XG | Ti | 4763 | 4831 | −68 | 23 | 0% |
| Median: | 217 | Median: | 4951 | 4787 | 263.5 | 181.5 | 2% | |||
| Q1–Q3: | 188–286 | Q1–Q3: | 4358–6170 | 3924–5531 | −302–752.75 | 35–344 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamure-Damberga, L.; Radzins, O.; Salms, G.; Zolovs, M.; Bokvalde, Z.; Neimane, L. Long-Term Volumetric Stability of Maxillary Sinus Floor Augmentation Using a Xenograft Bone Substitute and Its Combination with Autologous Bone: A 6+ Year Retrospective Follow-Up Study Using Cone Beam Computed Tomography. Dent. J. 2024, 12, 121. https://doi.org/10.3390/dj12050121
Zamure-Damberga L, Radzins O, Salms G, Zolovs M, Bokvalde Z, Neimane L. Long-Term Volumetric Stability of Maxillary Sinus Floor Augmentation Using a Xenograft Bone Substitute and Its Combination with Autologous Bone: A 6+ Year Retrospective Follow-Up Study Using Cone Beam Computed Tomography. Dentistry Journal. 2024; 12(5):121. https://doi.org/10.3390/dj12050121
Chicago/Turabian StyleZamure-Damberga, Liene, Oskars Radzins, Girts Salms, Maksims Zolovs, Zanda Bokvalde, and Laura Neimane. 2024. "Long-Term Volumetric Stability of Maxillary Sinus Floor Augmentation Using a Xenograft Bone Substitute and Its Combination with Autologous Bone: A 6+ Year Retrospective Follow-Up Study Using Cone Beam Computed Tomography" Dentistry Journal 12, no. 5: 121. https://doi.org/10.3390/dj12050121