
A Simplified Technique for Implant-Abutment Level Impression after Soft Tissue Adaptation around Provisional Restoration

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
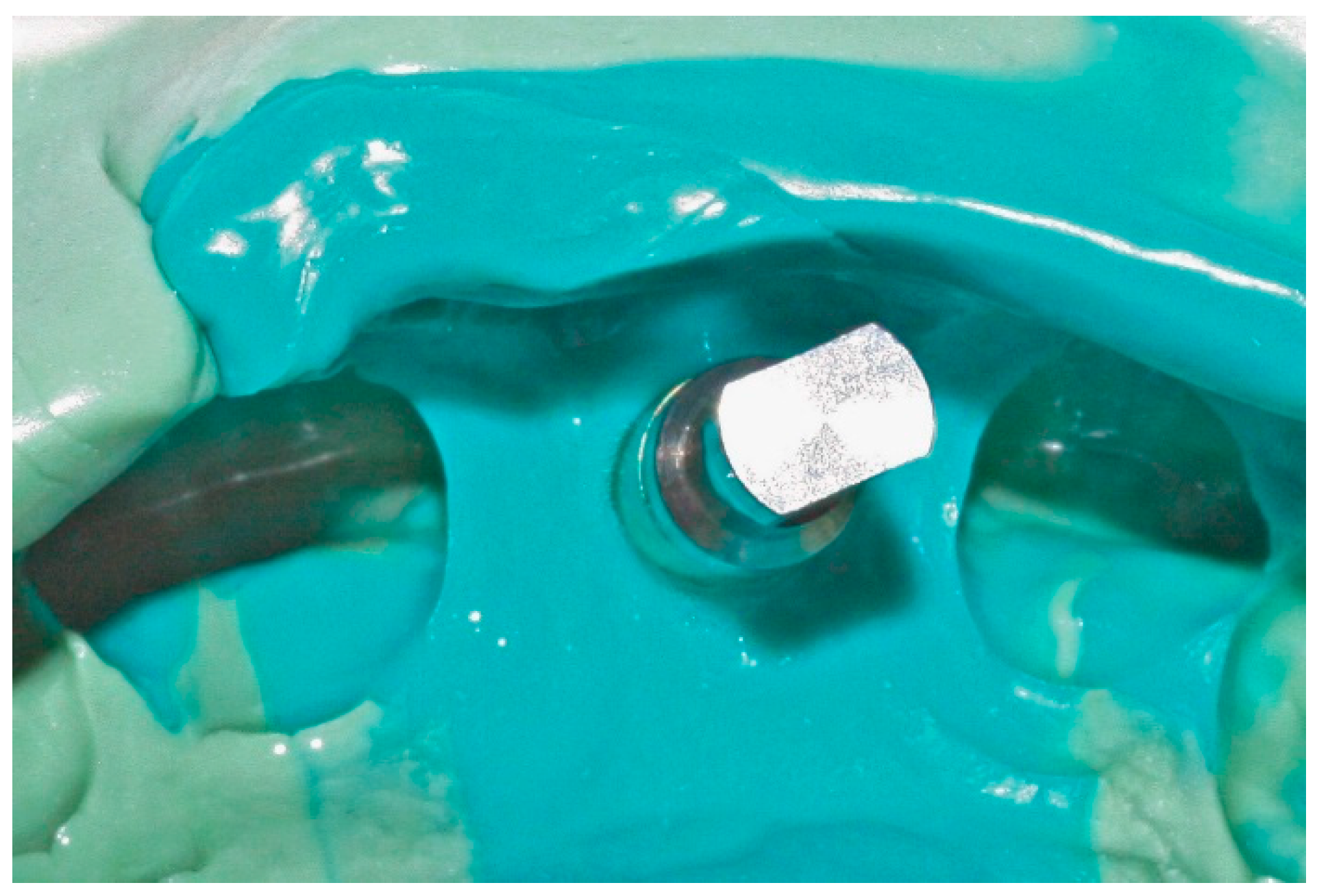
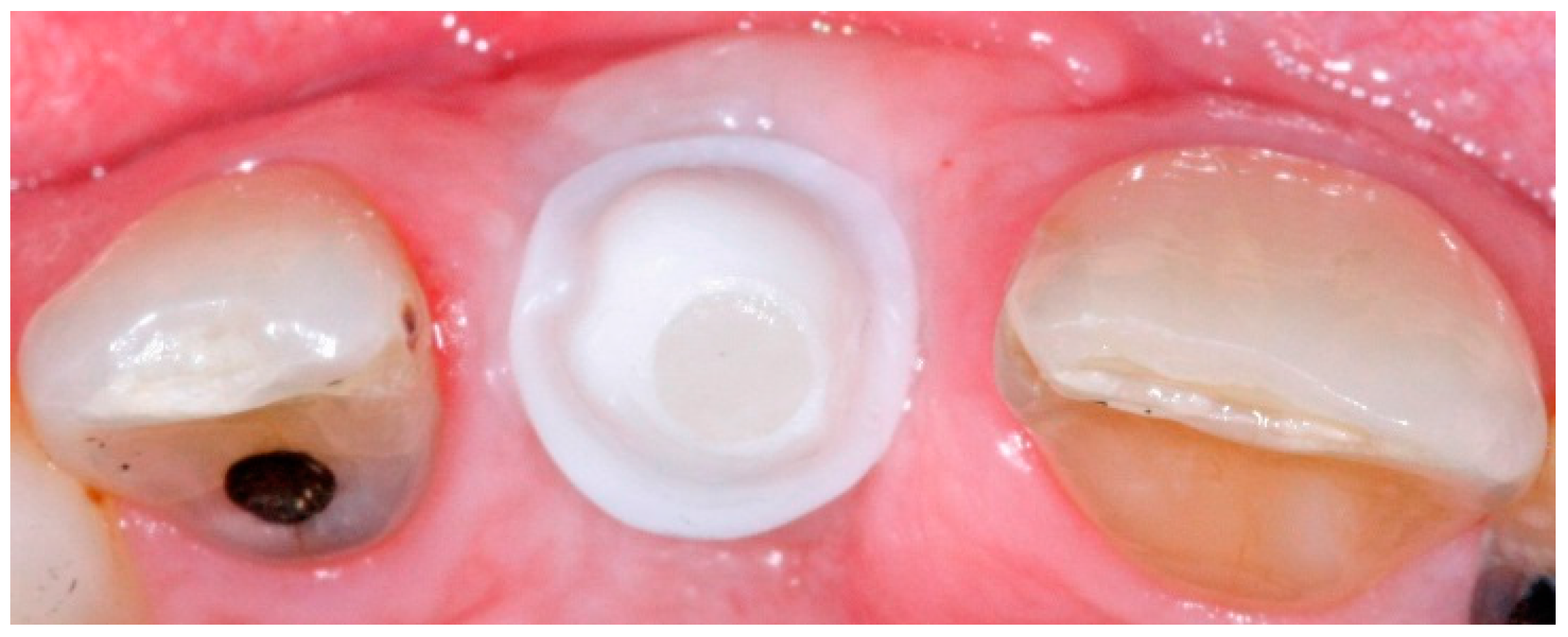
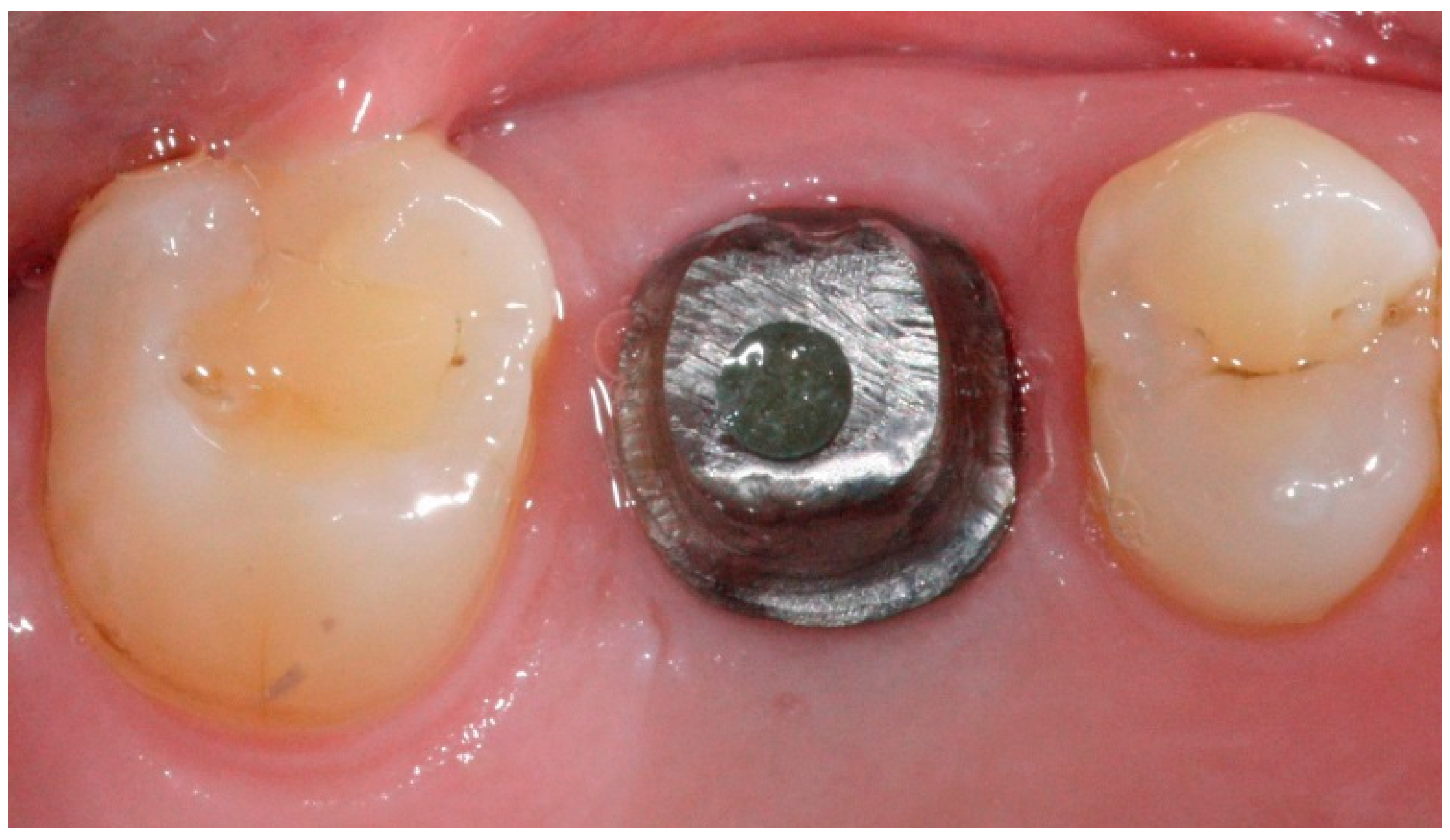
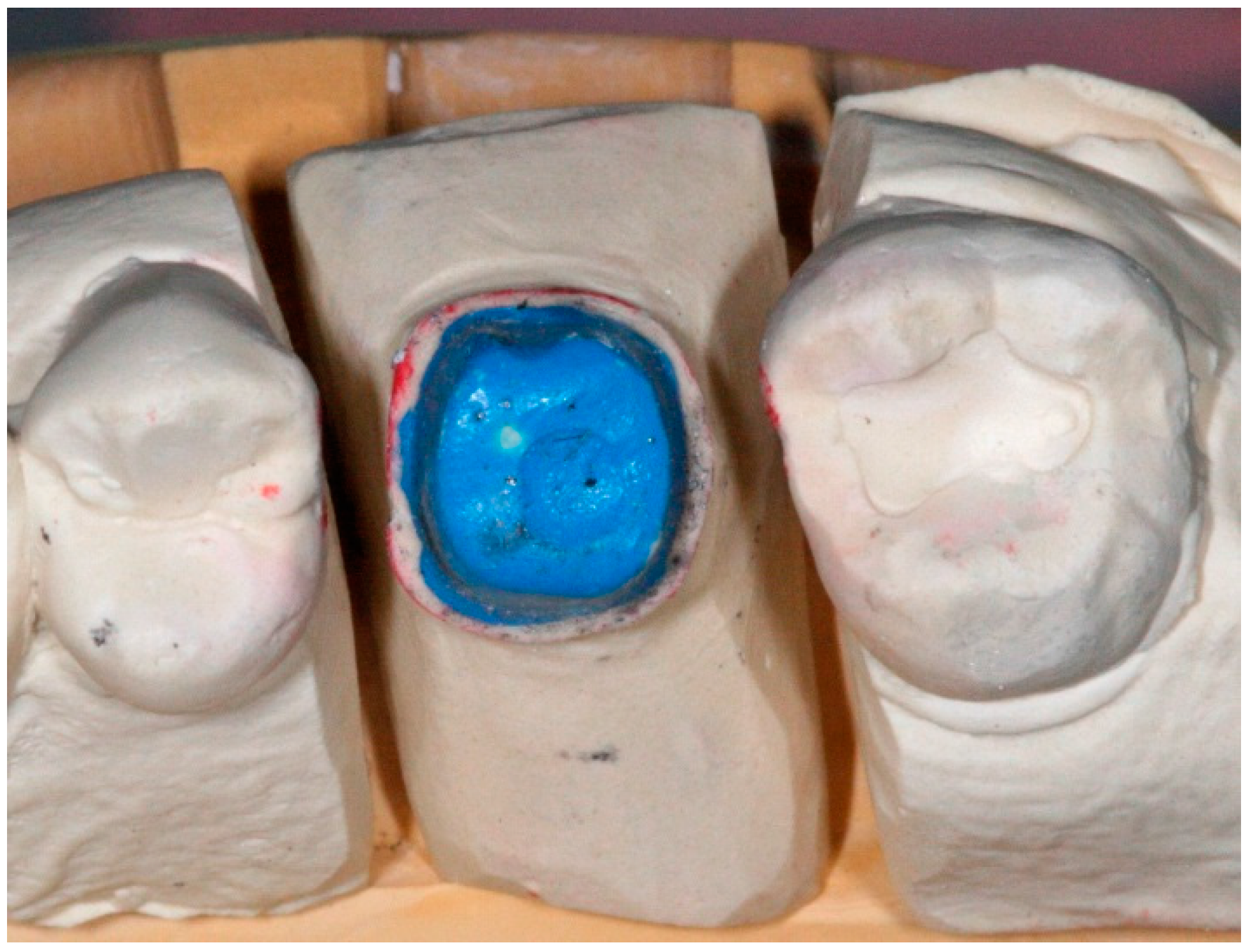
2. Impression Technique
3. Discussion
4. Conclusions
- Peri-implant soft tissue stability around provisional restoration insures optimum esthetic outcomes.
- Employing well-known familiar impression techniques allow for the recording of optimum finish line positions after the appropriate adaptation of soft tissue around provisional implant restorations.
- This variation to the use of prefabricated impression copings allows the production of predictable restorations that are esthetically acceptable to the patient.
Author Contributions
Conflicts of Interest
References
- American College of Prosthodontics Messenger. Available online: https://www.prosthodontics.org/acp-publications/acp-messenger/ (accessed on May 2012).
- Millennium Research Group. Annual Industry Report US Markets for Dental Implants: Executive Summary. Impl. Dent. 2003, 12, 108–111. [Google Scholar]
- Fernandez, M.A.; Paez de Mendoza, C.Y.; Platt, J.A.; Levon, J.A.; Hovijitra, S.T.; Nimmo, A. A comparative study of the accuracy between plastic and metal impression transfer copings for implant restorations. J. Prosthodontics 2013, 22, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Rashidan, N.; Alikhasi, M.; Samadizadeh, S.; Beyabanaki, E.; Kharazifard, M.J. Accuracy of implant impressions with different impression coping types and shapes. Clin. Implant Dent. Relat. Res. 2012, 14, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Small, P.N.; Tarnow, D.P. Gingival recession around implants: A 1-year longitudinal prospective study. Int. J. Oral Maxillofac. Implants. 2000, 15, 527–532. [Google Scholar] [PubMed]
- Grunder, U. Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. Int. J. Periodontics Restor. Dent. 2000, 20, 11–17. [Google Scholar]
- Kutkut, A.; Abu-Hammad, O.; Mitchell, R. Esthetic considerations for reconstructing implant emergence profile using titanium and zirconia custom implant abutments: Fifty case series report. J. Oral Implantol. 2013, 41, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.L.; Kurtzman, G.M. Simplifying single-stage solid abutments: Techniques for impressioning and temporization. Dent. Today. 2004, 23, 114–117. [Google Scholar] [PubMed]
- Charters, R.T. Restoration of a modified solid abutment of the ITI dental implant system: One of the most unique systems in implant dentistry. J. Dent. Technol. 2001, 18, 10–12. [Google Scholar] [PubMed]
- Chee, W.; Jivraj, S. Impression techniques for implant dentistry. Br. Dent. J. 2006, 201, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; So, J.S.; Hochstedler, J.L.; Ercoli, C. The accuracy of implant impressions: A systematic review. J. Prosthet. Dent. 2008, 100, 285–291. [Google Scholar] [CrossRef]
- Azer, S.S. A simplified technique for creating a customized gingival emergence profile for implant-supported crowns. J. Prosthodontics 2010, 19, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.B.; Klineberg, I. Prosthodontic considerations designed to optimize outcomes for single-tooth implants. A review of the literature. Aust. Dent. J. 2011, 56, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, M.D.; Kempen, J.; Lourenço, E.J.; Tells Dde, M. The use of CAD/CAM technology to fabricate a custom ceramic implant abutment: A clinical report. J. Prosthet. Dent. 2014, 111, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Liao, W.; Dai, N.; Tang, C. Design of a custom angled abutment for dental implants using computer-aided design and nonlinear finite element analysis. J. Biomech. 2010, 43, 1941–1946. [Google Scholar] [CrossRef] [PubMed]
- Bennani, V.; Schwass, D.; Chandler, N. Gingival retraction techniques for implants versus teeth: Current status. J. Am. Dent. Assoc. 2008, 139, 1354–1363. [Google Scholar] [CrossRef] [PubMed]
- Del’Acqua, M.A.; Arioli-Filho, J.N.; Compagnoni, M.A.; Mollo Fde, A., Jr. Accuracy of impression and pouring techniques for an implant-supported prosthesis. Int. J. Oral Maxillofac. Implants 2008, 23, 226–236. [Google Scholar] [PubMed]
- McArdle, B.F.; Clarizio, L.F. An alternative method for restoring single-tooth implants. J. Am. Dent. Assoc. 2001, 132, 1269–1273. [Google Scholar] [CrossRef] [PubMed]












© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutkut, A.; Abu-Hammad, O.; Frazer, R. A Simplified Technique for Implant-Abutment Level Impression after Soft Tissue Adaptation around Provisional Restoration. Dent. J. 2016, 4, 14. https://doi.org/10.3390/dj4020014
Kutkut A, Abu-Hammad O, Frazer R. A Simplified Technique for Implant-Abutment Level Impression after Soft Tissue Adaptation around Provisional Restoration. Dentistry Journal. 2016; 4(2):14. https://doi.org/10.3390/dj4020014
Chicago/Turabian StyleKutkut, Ahmad, Osama Abu-Hammad, and Robert Frazer. 2016. "A Simplified Technique for Implant-Abutment Level Impression after Soft Tissue Adaptation around Provisional Restoration" Dentistry Journal 4, no. 2: 14. https://doi.org/10.3390/dj4020014
APA StyleKutkut, A., Abu-Hammad, O., & Frazer, R. (2016). A Simplified Technique for Implant-Abutment Level Impression after Soft Tissue Adaptation around Provisional Restoration. Dentistry Journal, 4(2), 14. https://doi.org/10.3390/dj4020014