
The Overall Survival, Complication-Free Survival, and Related Complications of Combined Tooth-Implant Fixed Partial Dentures: A Literature Review


Abstract
:1. Introduction
- mobility of the natural tooth;
- number of teeth and implants to be connected;
- occlusal forces including:
- ○
- magnitude,
- ○
- duration,
- ○
- distribution, and
- ○
- direction;
- the force absorbing properties of the veneering material;
- rigidity of the prosthesis including length, thickness, and connectors (rigid or non-rigid);
- type of bone.
- (a)
- Retrievability: If a NRC is used with screw retention on the implant, then the implant portion of the reconstruction can easily be removed. If, on the other hand, a rigid construction is necessary, a one-piece casting will reduce retrievability because of the cement retention on the natural tooth abutment. To have a rigid restoration and maintain retrievability, a “screw-locked connector” may be installed in the restoration or a one-piece casting used with a telescopic crown on the natural tooth. This would be retained through the use of temporary cement or a locking screw.
- (b)
- Implant screw loosening: The constant bending of the prosthesis caused by the disparity in implant and natural tooth mobility may result in the loosening of the screw or ultimately fatigue fracture [39].
- (c)
- Framework and veneer fracture: Similarly, the constant bending of the restoration may lead to fracture of the framework and veneering material. The preference to keep the framework connectors narrow to increase the flexibility of framework must be balanced with the need for fracture resistance. The veneering material should also be flexible and preferably absorb some of the occlusal load without compromising material strength.
- (d)
- Tooth intrusion: Possible reasons have been described, including diffuse atrophy, differential energy dissipation, mandibular flexure, fixed partial denture flexure, impaired rebound memory, debris impaction or microjamming, and the ratchet effect [38], yet the etiology for this phenomenon is not fully understood.
- (e)
2. Aims and Objectives
2.1. Aims
2.2. Objectives
- To assess which clinical situations are best suited for TIFPs.
- To determine overall survival and complication-free survival for TIFPs.
- To determine whether rigid or non-rigid connectors are the better option when connecting teeth to implants.
- To determine the potential of periodontally compromised and structurally compromised teeth to be used as abutments for TIFPs.
- To determine the best ways of attaching the framework to the natural teeth.
- To determine the ideal construction of TIFPs, including connectors, framework, and veneering.
3. Methodology
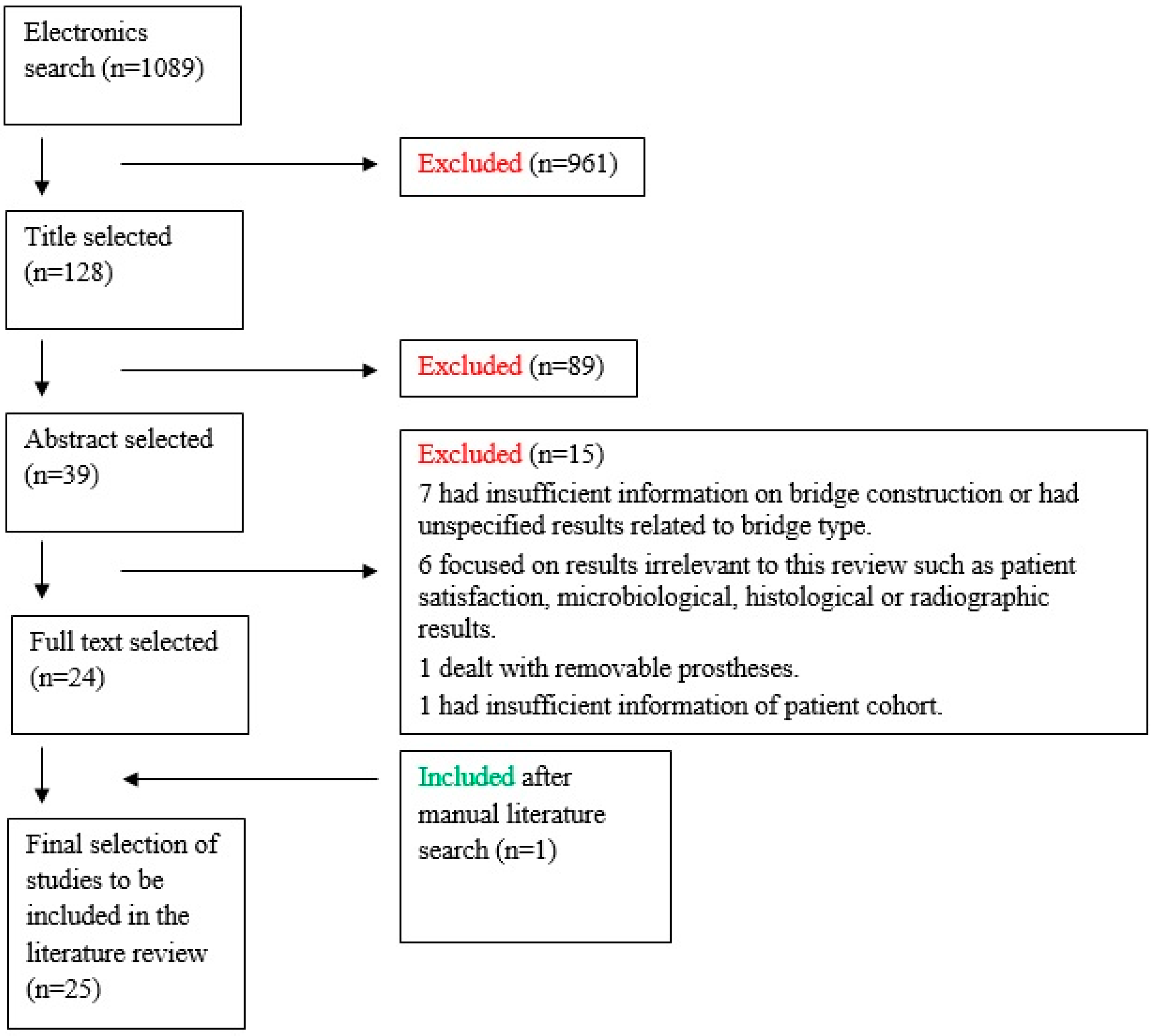
3.1. Search Strategy
TITLE: (tooth* or teeth* or partial*) AND TITLE: (implant* or implants* or fixture* or fixtures*) AND TITLE: (fixed partial denture* or prostheses* or prosthesis* or connected* or connection* or bridge* or partial*).
3.2. Types of Studies Included
- Studies published in peer-reviewed journals in English;
- Studies with at least ten participants;
- Randomized control studies;
- Prospective cohort studies;
- Retrospective cohort studies;
- Clinical trials including prospective and retrospective, controlled or uncontrolled and multi-center studies;
- Only studies utilizing commercially pure titanium implants were included.
3.3. Types of Participants
- Patients requiring tooth-to-implant fixed prosthesis treatment;
- Partially edentulous adult male and female patients, including smokers;
- Patients with fixed or removable opposing dentitions;
- Patients free from active periodontal disease.
3.4. Types of Intervention
- Tooth-to-implant fixed prostheses treatment in the maxilla and mandible;
- Tooth-to-implant connection with rigid and non-rigid connectors;
- Tooth connection utilizing telescopic crowns;
- Applications of temporary and permanent cements in tooth-to-implant cases;
- Sectional and full-arch cases;
- Application of different framework and veneering material for tooth-to-implant prostheses;
- Treatment utilizing vital and RCT teeth.
3.5. Outcomes Recorded
- Prosthetic complications including: veneer/framework fracture, abutment/implant fracture, cement failure, screw loosening, and loss of prosthesis;
- Biological complications including: tooth intrusion, dental caries, dental periapical pathology, tooth fracture, tooth bone loss, dental mobility, fixture bone loss, plaque deposits, and bleeding on probing.
3.6. Types of Excluded Studies/Exclusion Criteria
- in vitro experiments;
- animal studies;
- case reports;
- literature reviews;
- studies making use of immediate implants or immediate loading of implants.
3.7. Study Selection
3.8. Study Validity and Clinical Relevance
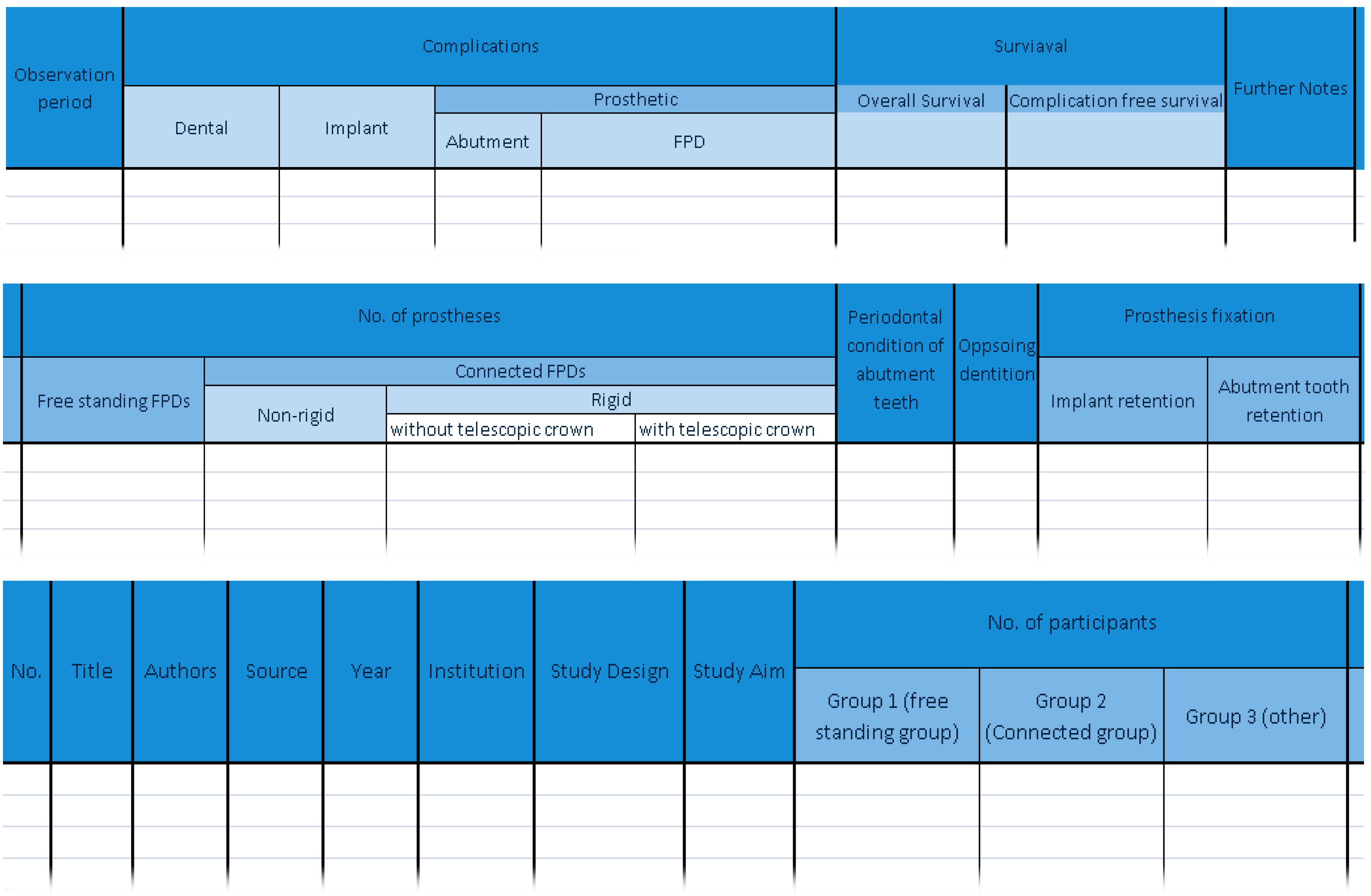
3.9. Data Extraction and Analysis
- study title, author names, publishing journal, and year of publication;
- institution where the study was conducted;
- type of study design;
- study aim;
- number of participants;
- number and type of prostheses, whether implant or tooth and implant-supported;
- bridge constructions;
- the periodontal condition of the teeth involved;
- the quality of the opposing dentition;
- method of prosthesis fixation to the supporting teeth and implants;
- observation period;
- biological and prosthetic complications.
3.10. Study Quality Assessment and Risk of Bias
- Reporting;
- External validity—addressing the relevance of the findings to the general population;
- Bias—addressing bias in measuring the intervention and the measurement of the outcome;
- Selection bias—which addresses bias in subject selection;
- Power—attempting to determine whether the negative findings may be due to chance.
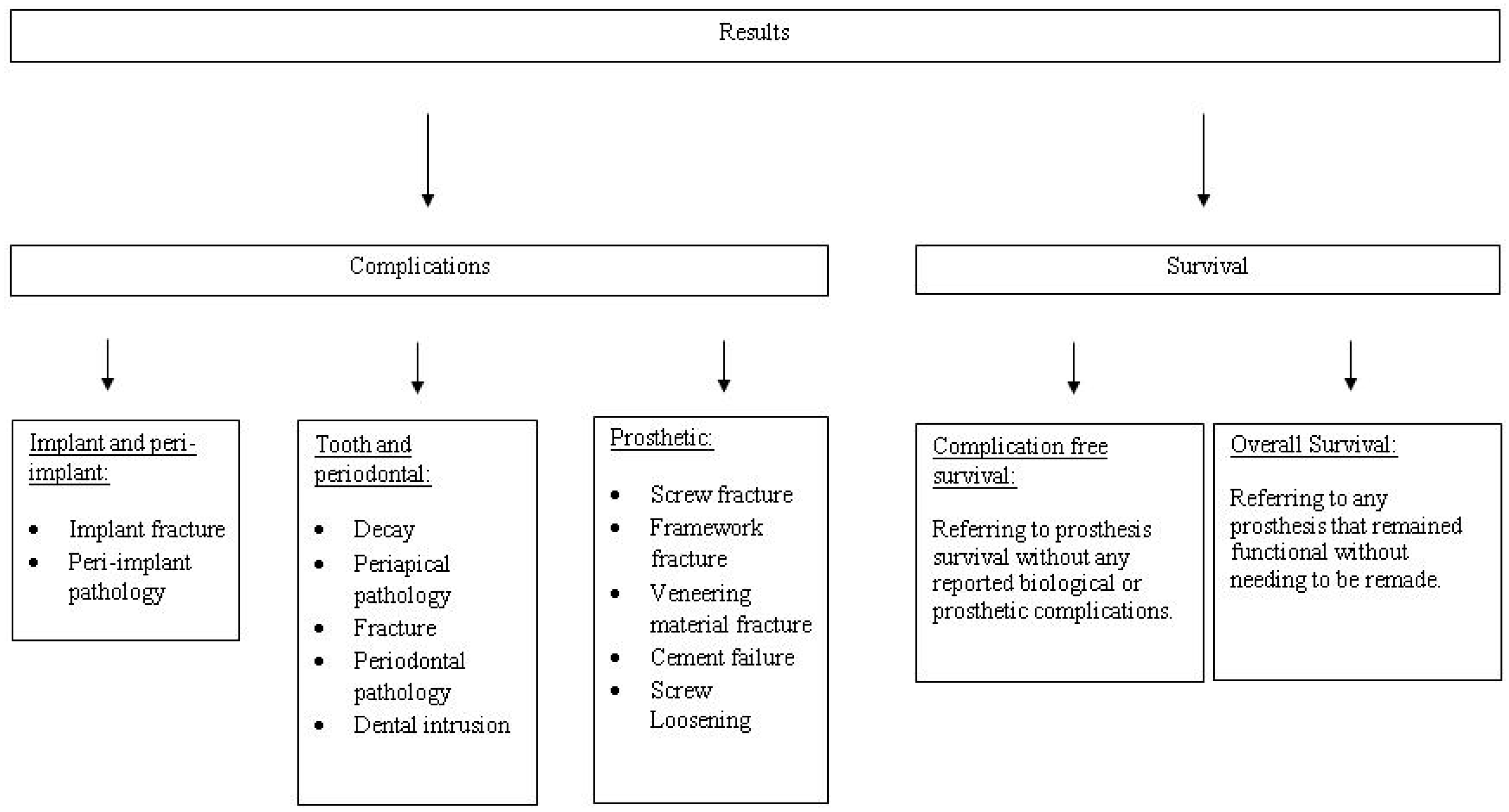
4. Results
4.1. Complications
4.1.1. Implant and Peri-Implant Complications
4.1.2. Natural Tooth and Periodontal Complications
4.1.3. Prosthetic Complications
4.2. Survival
4.2.1. Overall Survival
4.2.2. Complication-Free Survival
5. Discussion
6. Conclusions
Conflicts of Interest
Appendix 1: Data Extraction Spreadsheet

References
- Adell, R.; Lekholm, U.; Rockler, B.; Branemark, P. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef]
- Johns, R.; Jemt, T.; Heath, M.; Hutton, J.; McKenna, S.; McNamara, D.; van Steenberghe, D.; Taylor, R.; Watson, R.; Herrmann, I. A multicenter study of overdentures supported by Branemark implants. Int. J. Oral Maxillofac. Implants 1992, 7, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implants Res. 2012, 23, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002, 29, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Janner, S.; Wittneben, J.; Bragger, U.; Ramseier, C.; Salvi, G. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: A retrospective study in 303 partially edentulous patients. Clin. Implant Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Spear, F. Connecting teeth to implants The truth about a debated technique. J. Am. Dent. Assoc. 2009, 140, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, I.; Lekholm, U.; Branemark, P.; Lindhe, J.; Glantz, P.; Nyman, S. A Clinical-evaluation of fixed-bridge restorations supported by the combination of teeth and osseointegrated titanium implants. J. Clin. Periodontol. 1986, 13, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Palmer, R.; Howe, L.; Palmer, P. A prospective 3-year study of fixed bridges linking Astra Tech ST implants to natural teeth. Clin. Oral Implants Res. 2005, 16, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Akca, K.; Cehreli, M. 2-year prospective follow-up of implant/tooth-supported versus freestanding implant-supported fixed partial dentures. Int. J. Periodontics Restor. Dent. 2008, 28, 593–599. [Google Scholar]
- Nickenig, H.; Spiekermann, H.; Wichmann, M.; Andreas, S.; Eitner, S. Survival and complication rates of combined tooth-implant-supported fixed and removable partial dentures. Int. J. Prosthodont. 2008, 21, 131–137. [Google Scholar] [PubMed]
- Rammelsberg, P.; Schwarz, S.; Schroeder, C.; Bermejo, J.; Gabbert, O. Short-term complications of implant-supported and combined tooth-implant-supported fixed dental prostheses. Clin. Oral Implants Res. 2013, 24, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Iacono, V.; Cochran, D. State of the science on implant dentistry: A workshop developed using an evidence-based approach. Int. J. Oral Maxillofac Implants 2007, 22, 7–10. [Google Scholar] [PubMed]
- Lang, N.; Berglundh, T.; Heitz-Mayfield, L.; Pjetursson, B.; Salvi, G.; Sanz, M. Consensus statements and recommended clinical procedures regarding implant survival and complications. Int. J. Oral Maxillofac Implants 2004, 19, 150–154. [Google Scholar] [PubMed]
- Salvi, G.; Bragger, U. Mechanical and technical risks in implant therapy. Int. J. Oral Maxillofac Implants 2009, 24, 69–85. [Google Scholar] [PubMed]
- Ghodsi, S.; Rasaeipour, S. Tooth-implant connection: A literature review. World J. Dent. 2012, 3, 213–219. [Google Scholar] [CrossRef]
- Cavicchia, F.; Bravi, F. Free-standing vs tooth-connected implant supported fixed partial restorations: A comparative retrospective clinical study of the prosthetic results. Int. J. Oral Maxillofac Implants 1994, 9, 711–718. [Google Scholar]
- Sekine, H.; Komiyama, Y.; Potta, H.; Yoshida, K. Mobility characteristics and tactile sensitivity of osseointegrated fixture-supporting systems. In Tissue Integration in Oral Maxillofacial Reconstruction; van Steenberghe, D.M., Ed.; Elsiver: Amsterdam, The Netherlands, 1986; pp. 326–332. [Google Scholar]
- Natali, A.; Pavan, P.; Scarpa, C. Numerical analysis of tooth mobility: Formulation of a non-linear constitutive law for the periodontal ligament. Dent. Mater. J. 2004, 20, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Komiyama, Y. Clinical and research experience with osseointegrated implants in Japan. In The Branemark Osseointegrated Implant; Albrektsson, T., Zarb, G., Eds.; Quintessence Publ Co., Inc.: Chicago, IL, USA, 1989; pp. 197–214. [Google Scholar]
- Skalak, R. Biomechanical considerations in osseointegrated prostheses. J. Prosthet. Dent. 1983, 49, 843–848. [Google Scholar] [CrossRef]
- Finger, I.; Guerra, L. Prosthetic considerations in reconstructive implantology. Dent. Clin. North Am. 1986, 30, 69–83. [Google Scholar] [PubMed]
- Sullivan, D. Prosthetic considerations for the utilization of osseointegrated fixtures in the partially edentulous arch. Int. J. Oral Maxillofac Implants 1986, 1, 39–45. [Google Scholar] [PubMed]
- Gross, M.; Laufer, B. Splinting osseointegrated implants and natural teeth in rehabilitation of partially edentulous patients. 1: Laboratory and clinical studies. J. Oral Rehabil. 1997, 24, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.; Pjetursson, B.; Tan, K.; Bragger, U.; Egger, M.; Zwahlen, M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years-II. Combined tooth-implant-supported FPDs. Clin. Oral Implants Res. 2004, 15, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Misch, C. Contemporary Implant Dentistry, 3rd ed.; Mosby: Maryland Heights, MO, USA, 2008. [Google Scholar]
- Rangert, B.; Gunne, J.; Sullivan, D. Mechanical aspects of a branemark implant connected to a natural tooth an in vitro study. Int. J. Oral Maxillofac Implants 1991, 6, 177–186. [Google Scholar] [PubMed]
- Rangert, B.; Gunne, J.; Glantz, P.; Svensson, A. Vertical load distribution on a 3-unit prosthesis supported by a natural tooth and a single branemark implant-an in vitro study. Clin. Oral Implants Res. 1995, 6, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Michalakis, K.; Calvani, P.; Hirayama, H. Biomechanical considerations on tooth-implant supported fixed partial dentures. J. Dent. Biomech. 2012, 3, 1758736012462025. [Google Scholar] [CrossRef] [PubMed]
- Hosny, M.; Duyck, J.; van Steenberghe, D.; Naert, I. Within-subject comparison between connected and nonconnected tooth-to-implant fixed partial prostheses: Up to 14-year follow-up study. Int. J. Prosthodont. 2000, 13, 340–346. [Google Scholar] [PubMed]
- Naert, I.; Duyck, J.; Hosny, M.; Quirynen, M.; van Steenberghe, D. Freestanding and tooth-implant connected prostheses in the treatment of partially edentulous patients Part II: An up to 15-years radiographic evaluation. Clin. Oral Implants Res. 2001, 12, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Block, M.; Lirette, D.; Gardiner, D.; Li, L.; Finger, I.; Hochstedler, J.; Evans, G.; Kent, J.; Misiek, D.; Mendez, A.; et al. Prospective evaluation of implants connected to teeth. Int. J. Oral Maxillofac Implants 2002, 17, 473–487. [Google Scholar] [PubMed]
- Richter, E.; Orschall, B.; Jovanovic, S. Dental implant abutment resembling the 2-phase tooth mobility. J. Biomech. 1990, 23, 297–306. [Google Scholar] [CrossRef]
- Vanrossen, I.; Braak, L.; Deputter, C.; Degroot, K. Stress-absorbinelements in dental implants. J. Prosthet. Dent. 1990, 64, 198–205. [Google Scholar] [CrossRef]
- Cordaro, L.; Ercoli, C.; Rossini, C.; Torsello, F.; Feng, C. Retrospective evaluation of complete-arch fixed partial dentures connecting teeth and implant abutments in patients with normal and reduced periodontal support. J. Prosthet. Dent. 2005, 94, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Nickenig, H.; Schaefer, C.; Spiekermann, H. Survival and complication rates of combined tooth-implant-supported fixed partial dentures. Clin. Oral Implants Res. 2006, 17, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Wang, J.; Chang, W. Biomechanical interactions in tooth-implant-supported fixed partial dentures with variations in the number of splinted teeth and connector type: A finite element analysis. Clin. Oral Implants Res. 2008, 19, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Chee, W.; Mordohai, N. Tooth-to-implant connection: A systematic review of the literature and a case report utilizing a new connection design. Clin. Implant Dent. Relat. Res. 2010, 12, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Pesun, I. Intrusion of teeth in the combination implant-to-natural-tooth fixed partial denture: A review of the theories. J. Prosthodont. 1997, 6, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Noda, K.; Arakawa, H.; Maekawa, K.; Hara, E.; Yamazaki, S.; Kimura-Ono, A.; Sonoyama, W.; Minakuchi, H.; Matsuka, Y.; Kuboki, T. Identification of risk factors for fracture of veneering materials and screw loosening of implant-supported fixed partial dentures in partially edentulous cases. J. Oral Rehabil. 2013, 40, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Lindh, T.; Back, T.; Nystrom, E.; Gunne, F. Implant versus tooth-implant supported prostheses in the posterior maxilla: A 2-year report. Clin. Oral Implants Res. 2001, 12, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Astrand, P.; Borg, K.; Gunne, J.; Olsson, M. Combination of natural teeth and osseointegrated implants as prosthesis abutments: A 2-year longitudinal study. Int. J. Oral Maxillofac Implants 1991, 6, 305–312. [Google Scholar] [PubMed]
- Gunne, J.; Astrand, P.; Ahlen, K.; Borg, K.; Olsson, M. Implants in partially edentulous patients. A longitudinal study of bridges supported by both implants and natural teeth. Clin. Oral Implants Res. 1992, 3, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Olsson, M.; Gunne, J.; Astrand, P.; Borg, K. Bridges supported by freestanding implants versus bridges supported by tooth and implant a 5-year prospective study. Clin. Oral Implants Res. 1995, 6, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Gunne, J.; Astrand, P.; Lindh, T.; Borg, K.; Olsson, M. Tooth-implant and implant supported fixed partial dentures: A 10-year report. Int. J. Prosthodont. 1999, 12, 216–221. [Google Scholar] [PubMed]
- Downs, S.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community H 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Naert, I.; Quirynen, M.; Schepers, E.; Vansteenberghe, D.; Darius, P. A 6-year prosthodontic study of 509 consecutively inserted implants for the treatment of partial edentulism. J. Prosthet. Dent. 1992, 67, 236–245. [Google Scholar] [CrossRef]
- Kindberg, H.; Gunne, J.; Kronstrom, M. Tooth- and implant-supported prostheses: A retrospective clinical follow-up up to 8 years. Int. J. Prosthodont. 2001, 14, 575–581. [Google Scholar] [PubMed]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac Implants 1986, 1, 11–25. [Google Scholar] [PubMed]
- Koczorowski, R.; Surdacka, A. Evaluation of bone loss at single-stage and two-stage implant abutments of fixed partial dentures. Adv. Med. Sci. 2006, 51 (Suppl. 1), 43–45. [Google Scholar]
- Lindh, T.; Dahlgren, S.; Gunnarsson, K.; Josefsson, T.; Nilson, H.; Wilhelmsson, P.; Gunne, J. Tooth-implant supported fixed prostheses: A retrospective multicenter study. Int. J. Prosthodont. 2001, 14, 321–328. [Google Scholar] [PubMed]
- Bragger, U.; Karoussis, I.; Persson, R.; Pjetursson, B.; Salvi, G.; Lang, N. Technical and biological complications/failures with single crowns and fixed partial dentures on implants: A 10-year prospective cohort study. Clin. Oral Implants Res. 2005, 16, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Tangerud, T.; Gronningsaeter, A.; Taylor, A. Fixed partial dentures supported by natural teeth and Branemark system implants: A 3-year report. Int. J. Oral Maxillofac Implants 2002, 17, 212–219. [Google Scholar]
- Ozkan, Y.; Akoglu, B.; Kulak-Ozkan, Y. Five-year treatment outcomes with four types of implants in the posterior maxilla and mandible in partially edentulous patients: A retrospective study. Int. J. Oral Maxillofac Implants 2011, 26, 639–647. [Google Scholar] [PubMed]
- Romeo, E.; Lops, D.; Margutti, E.; Ghisolfi, M.; Chiapasco, M.; Vogel, G. Long-term survival and success of oral implants in the treatment of full and partial arches: A 7-year prospective study with the ITI dental implant system. Int. J. Oral Maxillofac Implants 2004, 19, 247–259. [Google Scholar] [PubMed]
- Heinemann, F.; Mundt, T.; Biffar, R. Retrospective evaluation of temporary cemented, tooth and implant supported fixed partial dentures. J. Craniomaxillofac. Surg. 2006, 34, 86–90. [Google Scholar] [CrossRef]
- Mundt, T.; Heinemann, F.; Schankath, C.; Schwahn, C.; Biffar, R. Retrospective and clinical evaluation of retrievable, tooth-implant supported zirconia-ceramic restorations. Acta Odontol. Scand. 2013, 71, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.; Pjetursson, B.; Lang, N.; Chan, E. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years-III. Conventional FPDs. Clin. Oral Implants Res. 2004, 15, 654–666. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.; Tan, K.; Lang, N.; Bragger, U.; Egger, M.; Zwahlen, M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years-I. Implant-supported FPDs. Clin. Oral Implants Res. 2004, 15, 625–642. [Google Scholar] [CrossRef] [PubMed]
- Wennstrom, J.; Zurdo, J.; Karlsson, S.; Ekestubbe, A.; Grondahl, K.; Lindhe, J. Bone level change at implant-supported fixed partial dentures with and without cantilever extension after 5 years in function. J. Clin. Periodontol. 2004, 31, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Haelg, G.; Schmid, J.; Haemmerle, C. Bone level changes at implants supporting crowns or fixed partial dentures with or without cantilevers. Clin. Oral Implants Res. 2008, 19, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Romeo, E.; Tomasi, C.; Finini, I.; Casentini, P.; Lops, D. Implant-supported fixed cantilever prosthesis in partially edentulous jaws: A cohort prospective study. Clin. Oral Implants Res. 2009, 20, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Torrecillas-Martinez, L.; Monje, A.; Lin, G.; Suarez, F.; Ortega-Oiler, I.; Galindo-Moreno, P.; Wang, H. Effect of cantilevers for implant-supported prostheses on marginal bone loss and prosthetic complications: Systematic review and meta-analysis. Int. J. Oral Maxillofac Implants 2014, 29, 1315–1321. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Participants | Partially Edentulous Patients Requiring Tooth-Implant Fixed Prostheses (TIPFs) Treatment |
|---|---|
| Interventions | Rigid/non-rigid tooth-to-implant connection. |
| Permanent/temporary cement use for tooth cementation. | |
| Screw/cement retained for tooth/implant fixation. | |
| Different framework and veneering materials. | |
| Comparison | Studies with similar interventions on tooth supported by FSFPs. |
| Outcomes | Complications, complication-free survival, and overall survival of different tooth-to-implant fixed prosthesis treatment modalities. |
| No. | Authors | Title | Source | Institute | Study Design | No. of Patients | Study Aim | Observation Period |
|---|---|---|---|---|---|---|---|---|
| 1 | Akca K, Cehreli MC. | Two-Year Prospective Follow-up of Implant/Tooth-Supported Versus Freestanding Implant-Supported Fixed Partial Dentures. | Int J Periodontics Restorative Dent. 2008, 28, 593–599 | Faculty of Dentistry, Hacettepe, University, Ankara, Turkey | Prospective case study | 29 | To Compare prosthetic outcomes of rigidly connected short-span TIFPs and FSFPs. | 24 months |
| 2 | Åstrand P, Borg K, Gunne J, Olsson M. | Combination of Natural Teeth and Osseointegrated Implants as Prosthesis Abutments: A 2-Year Longitudinal Study | Int J Oral Maxillofac Implants 1991, 6, 305–312. | Maxillofacial Unit at the University of Umeå | Prospective case study with cross-arch control; Randomized | 23 | To perform cross-arch comparisons between FSFPs and TIFPs. | 24 months |
| 3 | J Gunne, Astrand P, Ahlen K, Borg K, Olsson M. | Implants in partially edentulou patients. A longitudinal study of bridges supported by both implants and natural teeth | Clin. Oral. Impl. Res. 1992, 3, 49–56 | Maxillofacial Unit at the University of Umeå | Prospective case study with cross-arch control; Randomized | 23 | To compare the outcomes of FSFPs with TIFPs. | 36 months |
| 4 | Olsson M, Gunne J, Astrand P, Borg K. | Bridges supported by free-standing implants versus bridges supported by tooth and implant | Clin. Oral. Impl. Res. 1995, 6, 114–121 | Maxillofacial Unit at the University of Umeå | Prospective case study with cross-arch control; Randomized | 23 | To evaluate the same bridges as those presented in 1991 after 5 years in function. | 60 months |
| 5 | Gunne F, Ástrand P, Lindh T, Borg K, Olsson M. | Tooth-Implant and Implant Supported Fixed Partial Dentures: A 10-Year Report | Int J Prosthodont 1999, 12, 216–221. | Maxillofacial Unit at the University of Umeå | Prospective case study with cross-arch control; Randomized | 23–20 attending at 10 years | To compare FSFPs with TIFPs after 10 years of function. | 120 months |
| 6 | Block MS, Lirette D, Gardiner D, Li L, Finger IM, et al. | Prospective Evaluation of Implants Connected to Teeth. | Int J Oral Maxillofac Implants. 2002, 17, 473–487 | Authors affiliated with the Department of Oral and Maxillofacial Surgery, Louisiana State University | Prospective case study with cross-arch control; Randomized | 40 | To examine the effect on teeth and implants when rigidly or non-rigidly connected in a cross-arch study. | 60 months |
| 7 | Bragger U, Karoussis I, Persson R, Pjetursson B, Salvi G, et al. | Technical and biological complications/failures with single crowns and fixed partial dentures on implants: a 10-year prospective cohort study. | Clin. Oral Impl. Res. 2005, 16, 326–334 | Clinic for Periodontology and Fixed Prosthodontics University of Bern | Prospective case study | 21 | To assess the incidences of technical and/or biological complications and failures occurring in partially edentulous patients with fixed reconstructions on implants over 10 years. | 120 months |
| 8 | Cordaro L, Ercoli C, Rossini C, Torsello F, Feng C. | Retrospective evaluation of complete-arch fixed partial dentures connecting teeth and implant abutments in patients with normal and reduced periodontal support. | J Prosthet Dent 2005, 94, 313–320 | Authors affiliated with the Eastman Dental Hospital, Rome, Italy; Eastman Dental Center Rochester, NY. | Retrospective case study | 20 | The aim of this retrospective study was to evaluate the clinical outcomes of complete-arch TIFPs in patients demonstrating normal or reduced periodontal support. | 24–94 months average of 36.5 months |
| 9 | Ericsson I, Lekholm U, Branemark PI, Lindhe J, Glantz PO, et al. | A clinical evaluation of fixed-bridge restorations supported by the combination of teeth and osseointegrated titanium implants. | J Clin Periodontol 1986, 13, 307–312 | Department of Periodontology, University of Gothenburg, | Prospective case study | 10 | To investigate whether titanium fixtures could be used as combined abutments with teeth in fixed bridgework. | 6–30 months average of 17.4 months |
| 10 | Heinemann F, Mundt T, Biffar R. | Retrospective evaluation of temporary cemented, tooth and implant supported fixed partial dentures | Journal of Cranio-Maxillofacial Surgery 2006, 34, Suppl. 2, 86–90 | Private practice in Germany. | Retrospective case study | 47 | The aim of this study was to evaluate TIFPs, and determine which cement is best suited for temporary cementation. | 48 months |
| 11 | Hosny M, Duyck J, van Steenberghe D, Naert I. | Within-Subject Comparison Between Connected and Non connected TIFP: Up to 14-Year Follow-up Study | Int J Prosthodont. 2000, 13, 340–346. | University Hospitals of Catholic, University of Leuven, Belgium | Retrospective, case study with cross-arch control | 18 | This long-term follow-up study aimed to compare the outcome of TIFPs and FSFPs. | 168 months |
| 12 | Kindberg H, Gunne J, Kronström M. | Tooth- and Implant-Supported Prostheses: A Retrospective Clinical Follow-up up to 8 Years | Int J Prosthodont 2001, 14, 575–581 | Department of Prosthetic Dentistry, Central Hospital, Skövde, Sweden | Retrospective case study | 36 | To evaluate clinical treatment outcomes of fixed prostheses in different sizes and with combinations of different numbers of teeth and implants as abutments | 14 months to 106 months |
| 13 | KoczorowskiR, Surdacka A. | Evaluation of bone loss at single-stage and two-stage implant abutments of fixed partial dentures | Adv Med Sci. 2006, 51 Suppl. 1, 43–45. | Authors affiliated with the University of Medical Sciences in Poznan | Prospective case study | 32 | To evaluate alveolar bone loss at single-stage and two-stage implants as abutments of fixed partial dentures used to replace missing teeth. | 76 implants reviewed at 24 months, 50 reviewed up to 72 months |
| 14 | Lindh T, Bäck T, Nyström E, Gunne J. | Implant versus tooth-implant supported prostheses in the posterior maxilla: a 2-year report | Clin. Oral Impl. Res. 2001, 12, 441–449. | Department of Prosthetic Dentistry at Umeå University. | Prospective clinical study with cross-arch control | 26 | To compare the biological and mechanical consequences of implants placed in the posterior maxilla connected to teeth, or when used in FSFPs. | 24 months |
| 15 | Lindh T, Dahlgren S, Gunnarsson K, Josefsson T, Nilson H, et al. | Tooth-Implant Supported Fixed Prostheses: A Retrospective Multicenter Study | Int J Prosthodont 2001, 14, 321–328. | Multi-centre (6 centres) | Retrospective case study | 111 | To investigate the implant survival rate and loss of marginal bone, as well as indications and complications pertinent to TIFP treatment. | 36 months |
| 16 | Mundt T, Hinemann F, Schankath C, Schwahn C, Biffar R. | Retrospective and clinical evaluation of retrievable, tooth-implant supported zirconia-ceramic restorations | Acta Odontol Scand 2013, 71(5), 1326–1334 | Private practice, Germany | Retrospective case study | 23 | To assess retrievable TIFPs made of veneered zirconia cores as a viable treatment option. | 12.7–47.9 average of 28.8 months |
| 17 | Naert I, Quirynen M, Van Steenberghe D, Darius P. | A six-year prosthodontic study of 509 consecutively inserted implants for the treatment of partial edentulism. | J Prosthet Dent 1992, 67, 236–245. | Leuven University Clinic. | Retrospective case study | 146 (80 tooth-to-implant bridges) | To investigate the connection between teeth and implants and its possible harmful effects on fixture loss and bone loss as well as to investigate the use of composites or porcelain on the occlusal surfaces of TIFPs. | 2 to 77 months |
| 18 | Naert I, Duyck J, Hosny M, van Steenberghe D. | Freestanding and tooth-implant connected prostheses in the treatment of partially edentulous patients Part I: An up to 15-years clinical evaluation. | Clin. Oral Impl. Res. 2001, 12, 237–244 | Dept. of Periodontology and of Prosthetic Dentistry at the Hospitals of the Catholic University of Leuven. | Retrospective case study with cross-arch control | 123 | To compare TIFP and FSFP treatment modalities with each other based on implant, tooth and prosthesis complications. | 18–180 months |
| 19 | Nickenig HJ, Schafer C, Spiekermann H. | Survival and complication rates of combined tooth–implant-supported fixed partial dentures | Clin. Oral Impl. Res. 2006, 17, 506–511 | Based on the treatment documentations of a Bundeswehr dental clinic (Cologne-Wahn German Air Force Garrison) | Retrospective case study | 83 patients | To review the incidence of biological and technical complications in case of TIFP treatment on the basis of survival data regarding clinical cases. | 26.4–99.6 average of 56.8 months. |
| 20 | Noda K, Arakawa H, Maekawa K, Hara ES, Yamazaki S. | Identification of risk factors for fracture of veneering materials and screw loosening of implant-supported fixed partial dentures in partially edentulous cases | Journal of Oral Rehabilitation 2013, 40, 214–220 | Fixed Prosthodontic Clinic of Okayama University Dental Hospital, Okayama, Japan | Retrospective case study | 120 for veneer fracture, 81 for abutment screw loosening. | To identify the risk factors for fracture of veneering materials and screw loosening of implant-supported fixed partial dentures in partially edentulous cases. | Average of 48 months for screw loosening group and 30 months for veneer fracture group. |
| 21 | Özkan Y, Akoğlu B, Kulak-Özkan Y. | Five-year Treatment Outcomes with Four Types of Implants in the Posterior Maxilla and Mandible in Partially Edentulous Patients: A Retrospective Study | Int J Oral Maxillofac Implants 2011, 26, 639–647 | University of Marmara, Department of Oral Surgery and Depart-ment of Prosthetic Dentistry, Istanbul, Turkey, | Retrospective case study | 83 | To evaluate the clinical and radiologic outcomes of four types of implants and their suprastructures in the posterior maxilla and mandible in partially edentulous patients after 5 years of functional loading. | 60 months |
| 22 | Palmer RM, Howe LC, Palmer PJ. | A prospective 3-year study of fixed bridges linking Astra Tech ST implants to natural teeth | Clin. Oral Impl. Res. 2005, 16, 302–307 | Authors affiliation: Departments of Perio. and Prosth. GKT Dental Institute, King’s College, London. | Prospective case study | 19 | To assess the clinical and radiographic performance of the teeth and implants used to support three-unit fixed bridges subjected to normal functional loads. | 36 months |
| 23 | Rammelsberg P, Schwarz S, Schroeder C, Bermejo J, Gabbert O. | Short-term complications of implant-supported and combined tooth-implant-supported fixed dental prostheses | Clin. Oral Impl. Res. 2013, 24, 758–762 | Department of Prosthodontics at the University Hospital of Heidelberg. | Retrospective case study | 132 | To investigate the complications of metal-ceramic and all-ceramic FDPs supported by implants or by a combination of teeth and implants. | Average of 28 months. |
| 24 | Romeo E, Lops D, Margutti E, Ghisolfi M, Chiapasco M, et al. | Long-term Survival and Success of Oral Implants in the Treatment of Full and Partial Arches: A 7-year Prospective Study with the ITI Dental Implant System | Int J Oral Maxillofac Implants 2004, 19, 247–259 | Dental Clinic, Department of Medicine Surgery and Medicine, University of Milan, Italy. | Prospective case study | 201 | To evaluate the medium- to long-term survival and success of different implant-supported prostheses supported by ITI implants and to determine whether significant differences in survival and success could be observed for different implant placement sites. | 46.2 months |
| 25 | Tangerud T, Grønningsæter AG, Taylor A. | Fixed Partial Dentures Supported by Natural Teeth and Brånemark System Implants: A 3-year Report | Int J Oral Maxillofac Implants 2002, 17, 212–219 | Dental School, University of Bergen, Norway | Prospective case study | 30 | To evaluate TIFPs in a variety of clinical situations. | 36 months |
| Author/Year | Methodology | Implant Brand | Number of Connected Implants | Connected Implants Lost | Peri-Implant Bone Changes | Observation Period |
|---|---|---|---|---|---|---|
| (Akca and Cehreli 2008) | Prospective study comparing TIFPs and FSFPs. | ITI/Straumann | 34 | 0 | +0.19 mm (±0.52 mm) change in bone level which was significantly less bone loss than in FSFPs. | 24–30 months (mean 26 months) |
| (Astrand et al. 1991, Gunne et al. 1992, Olsson et al. 1995, Gunne et al. 1999) | Prospective study comparing TIFPs and FSFPs, randomized cross-arch control studt. | Nobel Biocare | 23 | 2 | −0.5–0.7 mm over 10 years not statistically significant to the contralateral side supporting FSFP implants. | 120 months |
| (Block et al. 2002) | Prospective study comparing rigid and non-rigid TIFPs, randomized cross-arch study. | Omniloc | 60 | 1 | 0.91 mm Average bone loss. No significant difference in bone loss around rigidly and non-rigidly connected implants. Four implants developed bone loss >2 mm. | 60 months |
| (Bragger et al. 2005) | Prospective study following single crown, FSFP and TIFP restorations. | ITI/Straumann | 22 | 3 | Three implants lost due to excessive bone loss. | 120 months |
| (Cordaro et al. 2005) | Retrospective study analyzing the performance of full-arch TIFPs. | 3i Implant and ITI/Straumann | 90 | 1 | 87 implants had stable bone levels during the observation period while 3 had bone loss than >2 mm. | 24–94 months (mean 36.5 months) |
| (Ericsson et al. 1986) | Prospective study following implants rigidly and non-rigidly connected to teeth. | Branemark | 41 | 0 | <1 mm marginal bone loss round most implants; 1–3 mm bone loss around 3 fixtures and >3 mm bone loss around2 implants in one patient and with rigid connection. | 6–30 months (mean 17.4 months) |
| (Heinemann et al. 2006) | Retrospective evaluation of different temporary cements in TIFP cases. | Tiolox | 155 | 1 | Two implants developed peri-implantitis of which one was lost. | 48 months |
| (Hosny et al. 2000) | Retrospective study of TIFPs with cross-arch FSFP control. | Branemark | 30 | 0 | 1.9 mm: Average bone loss over 15 years (2.2 mm/year for the first 6 months, 0.015 mm/year thereafter); More bone loss in FSFP group; however, difference not significant. | 15–168 months (mean 78 months) |
| (Kindberg et al. 2001) | Retrospective analysis of implants rigidly or non-rigidly connected to teeth. | Nobel Biocare | 112 | 6 | After 1 year, 46 implants showed marginal bone loss, 31 up to one thread, 11 up to two threads, 2 up to three threads and 2 up to four threads, for the three and five year examination progression of bone loss was minimal. | 14–107 months (mean 58.3 months) |
| (Koczorowski and Surdacka 2006) | Prospective evaluation of posterior implants connected to teeth. | Osteoplant | 76 | 0 | −0.70 mm ±0.50 after two years and −1.73 mm ±0.41 after six years of mean marginal bone loss. | 24–72 months (mean 43 months) |
| (Lindh et al. 2001a) | Prospective study of TIFPs with cross-arch control FSFPs in Kennedy Class I patients. | Nobel Biocare | 26 | 1 | −0.09 ± 0.52 mm around the posterior connected implant. The difference in bone loss from loading to 24 months was significant for posterior implant in FSFPs but not significant for posterior implants in TISP. | 24 months |
| (Lindh et al. 2001b) | Multi-centre retrospective study following TIFPs. | Nobel Biocare and Straumann | 185 | 5 | 1.7 mm, SD 0.8 mm bone loss at 12 months in 9 of the 74 implants reviewed for the whole 3 years, 0.3 mm, SD 0.7 many more bone loss in the other 65 implants. The subsequent loss of marginal bone during the second and third years for these two groups of implants was lower (n = 9: 0.3 mm, SD 0.9 mm; n = 65: 0.1 mm, SD 0.5 many more). | 36 months |
| (Mundt et al. 2013) | Retrospective study assessing zirconia TIFPs. | 38 Tiolox, 8 Ankylos, 5 Straumann | 51 | 0 | No marginal bone loss measurements however, by the end of the examination period only one implant had bleeding on probing. | 12.7–47.9 months (mean: 28.8 months) |
| (Naert et al. 1992) | Retrospective analysis of FSFPs and TIFPs. | Branemark | 80 | 5 | 1.02 mm mean bone loss in Year 1 followed by 0.10 mm bone gain in year two. No statistical difference between bone loss around the ditstal implant in connected and non-connected cases. | 72 months |
| (Naert et al. 2001) | Retrospective analysis of TIFPs compared to a control group of similar FSFPs. | Branemark | 339 | 10 | No statistical difference from 0 to 6 months between FS, non-rigid and rigid group, there was no statistical difference in bone loss from 6 to 180 years between the FSFP group 0.02 mm a year and non-rigid group 0.04 mm a year. There was, however, a statistical significant difference between the rigid group 0.09 mm a year and the FSFP group (p = 0.004). | 18–180 months (mean 78 months) |
| (Nickenig et al. 2006) | Retrospective analysis of implants rigidly and non-rigidly connected to teeth. | 85% Branemark and Straumann; 15% including Replace, Friadent, Ankylos and others | 142 | 0 | 5 mm probing depths were found in <1% of implants after 5 years. | 26–100 months (mean 56.8 months) |
| (Ozkan et al. 2011) | A retrospective study of single implant crowns, TIFPs and FSFPs. | Straumann, swiss plus, camlog, Friadent. | 9 | 0 | All implants met the criteria for success. All implants were surrounded by stable healthy tissue with crestal bone level changes not significantly different between TIFP and FSFP implants. | 60 months |
| (Palmer et al. 2005) | A prospective study of rigidly connected teeth and implants via short-span bridges in Kennedy Class II cases | Astra tech | 19 | 0 | Up to 1.2 mm of bone loss seen in 9 patients; 10 patients experienced no change or an increase in bone level around connected implants. | 36 months |
| (Romeo et al. 2004) | A prospective study of various types of implant-supported prostheses designs. | ITI | 31 | 3 | N/A | 16–84 months (mean 46.2 months) |
| (Tangerud et al. 2002) | Prospective study monitoring 30 rigid TIFPs. | Branemark | 85 | 2 | Bone loss of 0.8 mm ± 1.1 mm around connected implants from time of loading to 3 years review. | 36 months |
| Author/Year | Location of Failed Implant | Opposing Dentition | Connection Type | Reconstruction Length | FPD Retention | Time after Loading | Implant Brand | Reason for Failure |
|---|---|---|---|---|---|---|---|---|
| (Astrand et al., 1991, Gunne et al., 1992, Olsson et al., 1995, Gunne et al., 1999) | Posterior mandible | Complete Removable | Rigid | 3-unit | Screw | Within 18 months | Nobel Biocare | Loss of integration |
| Posterior mandible | Complete Removable | Rigid | 3-unit | Screw | Within 18 months | Nobel Biocare | Loss of integration | |
| (Block et al. 2002) | Posterior mandible | Complete Removable | Rigid | 3-unit | Screw | 36 months | Omniloc | Loss of integration without inflammation |
| (Bragger et al. 2005) | N/A | Fixed | Rigid | N/A | N/A | Within 60 months | ITI/Straumann | Primary biological complication |
| N/A | Fixed | Rigid | N/A | N/A | Within 60 months | ITI/Straumann | Bony defect followed by fracture | |
| N/A | Fixed | Rigid | N/A | N/A | Within 120 months | ITI/Straumann | Loss of integration | |
| (Cordaro et al. 2005) | Posterior Maxilla | Combined fixed removable prosthesis | Non rigid | 12-unit | Permanent Cement | 7 months | Straumann | Mobility |
| N/A | N/A | Rigid | N/A | Temporary Cement | N/A | Tiolox | Peri-implant disease | |
| (Kindberg et al. 2001) | Maxilla | N/A | Non rigid | 12-unit | Screw | 36 months | Nobel Biocare | Loss of integration |
| Maxilla | N/A | N/A | N/A | Screw | 36 months | Nobel Biocare | Loss of integration | |
| Maxilla | N/A | N/A | N/A | Screw | 36 months | Nobel Biocare | Loss of integration | |
| Maxilla | N/A | Rigid | 10-unit | Screw | 60 months | Nobel Biocare | Loss of integration | |
| Maxilla | N/A | N/A | N/A | Screw | 60 months | Nobel Biocare | Loss of integration | |
| Maxilla | N/A | N/A | N/A | Screw | 60 months | Nobel Biocare | Loss of integration | |
| (Lindh et al. 2001a) | Posterior Maxilla | N/A | Rigid | Unilateral short span | Screw | Within 3 months | Nobel Biocare | Mobility |
| (Lindh et al. 2001b) | Posterior Maxilla | N/A | N/A | N/A | N/A | 12 months | Straumann or Nobel Biocare | Loss of integration |
| Posterior Maxilla | N/A | N/A | N/A | N/A | 12 months | Straumann or Nobel Biocare | Loss of integration | |
| Maxilla | N/A | N/A | N/A | N/A | 12 months | Straumann or Nobel Biocare | Loss of integration | |
| Maxilla | N/A | N/A | N/A | N/A | 12 months | Straumann or Nobel Biocare | Loss of integration | |
| Maxilla | N/A | N/A | N/A | N/A | N/A | Straumann or Nobel Biocare | Loss of integration | |
| (Naert et al., 1992) | Posterior maxilla | N/A | Rigid | Unilateral short span | N/A | Within 36 months | Branemark | Fracture |
| Posterior maxilla | N/A | Rigid | Unilateral short span | N/A | Within 36 months | Branemark | Fracture | |
| Posterior | N/A | Rigid | Unilateral short span | N/A | Within 22 months | Branemark | Loss of integration | |
| Posterior | N/A | Rigid | Unilateral short span | N/A | Within 22 months | Branemark | Loss of integration | |
| Posterior | N/A | Rigid | Unilateral short span | N/A | Within 22 months | Branemark | Loss of integration | |
| (Naert et al. 2001) | N/A | N/A | Rigid | N/A | Screw | 25–36 months | Branemark | Mobility |
| N/A | N/A | Rigid | N/A | Screw | 25–36 months | Branemark | Mobility | |
| N/A | N/A | Rigid | N/A | Screw | 25–36 months | Branemark | Mobility | |
| N/A | N/A | Rigid | N/A | Screw | 25–36 months | Branemark | Mobility | |
| N/A | N/A | Non-rigid | N/A | Screw | 49–60 months | Branemark | Mobility | |
| N/A | N/A | Non-rigid | N/A | Screw | 49–60 months | Branemark | Mobility | |
| N/A | N/A | Rigid | N/A | Screw | 61–72 months | Branemark | Fracture | |
| N/A | N/A | Rigid | N/A | Screw | 85–96 months | Branemark | Fracture | |
| N/A | N/A | Rigid | N/A | Screw | 85–96 months | Branemark | Fracture | |
| N/A | N/A | Non-rigid | N/A | Screw | 85–96 months | Branemark | Fracture | |
| (Romeo et al. 2004) | Mandible | N/A | N/A | N/A | N/A | 72–84 months | ITI/Straumann | Peri-implant disease |
| Maxilla | N/A | N/A | N/A | N/A | 36–48 months | ITI/Straumann | Peri-implant disease | |
| Maxilla | N/A | N/A | N/A | N/A | 48–60 months | ITI/Straumann | Peri-implant disease | |
| (Tangerud et al. 2002) | Maxilla | N/A | Rigid | N/A | Screw | 12–24 months | Branemark | Mobility |
| Maxilla | N/A | Rigid | N/A | Screw | 24–36 months | Branemark | Peri-implant bone loss |
| Author/Year | Methodology | No. of Connected Teeth | Initial Periodontal Condition | Initial Endodontic Condition | Method of Fixation | Lost to Dental Caries | Lost to Periapical Pathology | Lost to Tooth Fracture | Periodontal Bone Changes | Tooth Intrusion | Observation Period |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (Akca and Cehreli 2008) | Prospective study comparing TIFPs and FSFPs. | 34 | crown root ratio 2:3. | 4 RCT, 30 Vital | Permanent cement | 0 | 0 | 0 | N/A | 0 | 24–30 months (mean 26 months) |
| (Astrand et al. 1991, Gunne et al. 1992, Olsson et al. 1995, Gunne et al. 1999) | Prospective study comparing TIFPs and FSFPs, randomized cross-arch control. | 23 | Healthy periodontium. | 0 RCT, 23 Vital | Permanent cement | 1 | 0 | Not significantly different to control; 1 tooth developed mobility | 0 | 120 months | |
| (Block et al. 2002) | Prospective study comparing rigid and non-rigid TIFPs. | 60 | Healthy periodontium Crown root ration of at least 1:2. | 27 RCT, 33 Vital | Permanent cement for non-rigid. Temporary cement for rigid. | 0 | 0 | 2 rigid side 3 non rigid side(all RCT) | No significant bone loss | 21 non rigid cases 14 rigid cases. | 60 months |
| (Bragger et al. 2005) | Prospective study following SC, FSFP and TIFP restorations. | 24 | Supportive periodontal care given. | RCT and vital | Permanent cement | 4 | 0 | 0 | N/A | 0 | 120 months |
| (Cordaro et al. 2005) | Retrospective study of TIFPs on teeth with normal and reduced periodontal support. | 72 | 10 patients had >2/3 residual periodontium 10 patients <2/3 residual periodontium | N/A | Permanent cement for non-rigid. Temporary cement for rigid. | 0 | 0 | 0 | N/A | 4 non-rigid cases with >2/3 periodontal support | 24–94 months (mean 36.5 months) |
| (Ericsson et al. 1986) | Prospective study following implants rigidly and non-rigidly connected to teeth. | 29 | Supportive periodontal care given | N/A | N/A | 0 | 0 | 0 | No loss of alveolar bone around teeth. | 1 non-rigid case | 6–30 months (mean 17.4 months) |
| (Heinemann et al. 2006) | Retrospective evaluation of different temporary cements in TIFP cases. | 108 | N/A | N/A | Temporary or semi-permanent cement. | 0 | 2 | N/A | 0 | 48 months | |
| (Hosny et al. 2000) | Retrospective study of TIFPs with cross-arch FSFP control. | 30 | N/A | N/A | 16 Temporary cement, 14 Permanent cement | 0 | 0 | 0 | N/A | 0 | 15–168 months (mean 78 months) |
| (Kindberg et al. 2001) | Retrospective study of implants connected rigidly or non-rigidly to teeth. | 85 | Healthy periodontium | N/A | 45 screw locked, cemented or telescopic | 0 | 5 | No significant bone loss | 1 non-rigid case and 2 in rigid cases with non locked telescopic crowns. | 14–107 months (mean 58.3 months) | |
| (Lindh et al. 2001a) | 26 TIFPs with cross-arch control FSFPs in Kennedy Class I patients. | 26 | 16 intact periodontia; 10 <1/4 bone loss | 15 RCT, 11 Vital | Temporary and Permanent cement | 0 | 0 | 1 | No increased mobility reported | 0 | 24 months |
| (Lindh et al. 2001b) | Multi-centre retrospective study following TIFP | 220 | 21 lost >1/3 of their periodontal support | 49 RCT, 171 Vital | N/A | 0 | 0 | 0 | N/A | 11 all debonded from prosthesis | 36 months |
| (Mundt et al. 2013) | Retrospective study assessing zirconia TIFPs. | 40 | No BOP <4 mm probing depth | RCT or Vital | Semi-permanent cement | 0 | 0 | 0 | 3 teeth with BOP | 0 | 12.7–47.9 months (mean: 28.8 months) |
| (Naert et al. 2001) | Retrospective analysis of TIFPs compared to a control group of FSFPs. | 313 | N/A | N/A | 46 temporary cement, 94 permanent cement | 3 | 11 | 2 | N/A | 19 all debonded from prosthesis | 18–180 months (mean 78 months) |
| (Nickenig et al. 2006) | Retrospective analysis of teeth rigidly and non-rigidly connected to implants. | 132 | N/A | N/A | N/A | 0 | 3 | 0 | 10 teeth required periodontal treatment | 0 | 26.4–99.6 months (mean 56.76) |
| (Palmer et al. 2005) | Rigidly connected teeth and implants via 3-unit bridges in Kennedy Class II cases. | 19 | Healthy periodontium | Vital | Temporary cement | 0 | 0 | 0 | No significant bone loss | 0 | 36 months |
| (Tangerud et al. 2002) | Prospective study monitoring 30 rigid TIFPs. | 86 | N/A | 40 RCT, 46 Vital | Cemented | 0 | 0 | 1 RCT | Bone reduction of 0.1 mm ± 0.8 mm around teeth | 0 | 36 months |
| Author/Year | No. of Tooth-Implant Prostheses | Prostheses Length | Prostheses Construction | Method of Fixation | Veneer Fracture | Framework Fracture | CEMENT FAILURE | Implant Screw Fracture/Loosening | Opposing Dentition | Observation Period | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rigid | Non-Rigid | Tooth | Implant | |||||||||
| (Akca and Cehreli 2008) | 34 | 0 | 3-unit | Metal-ceramic | Permanent cement | Permanent cement | 0 | 0 | 0 | 0 | N/A | 24–30 months (mean 26 months) |
| (Astrand et al. 1991, Gunne et al. 1992, Olsson et al. 1995, Gunne et al. 1999) | 23 | 0 | 3-unit | Metal-acrylic | Permanent cement | Screw | 0 | 0 | 0 | 3 | Removable | 120 months |
| (Bragger et al. 2005) | 22 | 0 | 10 3-unit; 6 4-unit; 4 5-unit; 2 10-unit; | Metal-ceramic | Permanent cement | 10 cement 12 screw | 2 | 0 | 4 | 4 | Fixed | 120 months |
| (Cordaro et al. 2005) | 6 | 13 | 10–14-unit | 15 Metal-ceramic; 4 Metal-composite | Permanent/Temporary cement | 12 Permanent/Temporary cement; 7 screw | 1 (composite) | 0 | N/A | 0 | 14 Fixed; 1 Removable; 4 Mixed | 24–94 months (mean 36.5 months) |
| (Heinemann et al. 2006) | 65 | 0 | Most four abutments; 12 2–3 abutments; 13 >4 abutments | Metal-ceramic | Semi-permanent/ Temporary cement | Semi-permanent/ Temporary cement | 5 | 0 | 80 with temp cement; 4 with semi-permanent cement | N/R | N/A | 48 months |
| (Hosny et al. 2000) | 14 | 4 | 6 3-unit; 6 4-unit; 2 5-unit; 3 6-unit; 1 8-unit | 14 Metal-cerami; 4 Metal-acrylic | 14 Permanent cement; 16 Temporary cement | Screw | 0 | 0 | 0 | 0 | N/A | 15–168 months (mean 78 months) |
| (Kindberg et al. 2001) | 40 | 1 | 11 3-unit; 5 4-unit; 25 >5-unit | 20 Metal-ceramic 20 Metal-acrylic 1 Metal-composite | 45 screw locked copings. Cemented and Telescopic | Screw | 4 | 0 | 0 | 1 | N/A | 14 months to 106 months |
| (Lindh et al. 2001a) | 26 | 0 | Unilateral | Metal-ceramic | Permanent/Temporary cement | Screw | 0 | 0 | 2 with temporary cement | 1 | N/A | 24 months |
| (Lindh et al. 2001b) | 122 | 16 | Most 1 implant to 1 tooth | 131 Metal-ceramic 7 Metal-acrylic | N/A | N/A | 3 | 2(attachment fractures) | 0 | 2 (and 2 abutment screws loosened) | 119 Fixed; 19 Removable | 36 months |
| (Mundt et al. 2013) | 31 | 0 | 15 3-unit; 4 4-unit; 6 5-unit; 4 6-unit; 1 8-unit; 1 12-unit | Zirconia with ceramic veneer | Semi-permanent cement | Semi-permanent cement | 10 | 2 | 2 | 1 abutment screw loosened. | Fixed | 12.7–47.9 months (mean 28.8 months) |
| (Naert et al. 2001) | 49 | 34 | N/A | 106 Metal-ceramic 34 Metal- acrylic | 94 Permanent cement; 46 Temporary cement. | Screw | N/A | 3 | 25 | Loose screw not reported; despite 3 abutment screw fractures | N/A | 18–180 months (mean 78 months) |
| 57 | ||||||||||||
| (Noda et al. 2013) | 136 | N/A | Metal-ceramic | N/A | N/A | 22 | N/A | N/A | 4 of 58 had screw loosening | N/A | Mean of 37.3 months. | |
| (Ozkan et al. 2011) | 9 | N/A | Metal-ceramic | Permanent cement | Screw/Permanent cement | 0 | 0 | 0 | 0 | Fixed and Removable | 60 months | |
| (Palmer et al. 2005) | 19 | 0 | Unilateral | Metal-composite | Temporary cement | Temporary cement | 8 | 0 | 8 | N/R | Fixed | 36 months |
| (Rammelsberg et al., 2013) | 48 | 0 | Mostly 3–4-unit | Metal-ceramic | Permanent/Semi-permanent cement | Permanent/Semi-permanent cement | 7 | 0 | 3 | N/R | N/A | Average of 28 months. |
| (Romeo et al. 2004) | 13 | N/A | Metal-ceramic | N/A | N/A | 0 | 0 | 0 | 0 | N/A | 46.2 months | |
| (Tangerud et al. 2002) | 30 | 0 | 3–13 units, mean 8.6 | 16 Metal-ceramic, 14 Metal-composite | Cement | Screw | 8 | 0 | 0 | 0 | N/A | 36 months |
| Intrusion | Retrievability | Caries Risk | Technical Complications | |
|---|---|---|---|---|
| Temporary Cement | Likely | Good | Moderate | Low |
| Permanent Cement | Unlikely | Poor | Low | Low |
| Temporarily Cemented telescopic crowns | Possible | Good | Low | Low |
| Uncemented telescopic crowns | Likely | Good | Low | Low |
| Screw retained on coping | Possible | Good | Low | High |
| Permanent cement with locked TIFP attachment | Possible | Good | Low | High |
| Intrusion | Biological Complications | Technical Complications | |
|---|---|---|---|
| Rigid construction | Unlikely | No difference | Low |
| Non-Rigid construction | Likely | No difference | High |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borg, P.; Puryer, J.; McNally, L.; O’Sullivan, D. The Overall Survival, Complication-Free Survival, and Related Complications of Combined Tooth-Implant Fixed Partial Dentures: A Literature Review. Dent. J. 2016, 4, 15. https://doi.org/10.3390/dj4020015
Borg P, Puryer J, McNally L, O’Sullivan D. The Overall Survival, Complication-Free Survival, and Related Complications of Combined Tooth-Implant Fixed Partial Dentures: A Literature Review. Dentistry Journal. 2016; 4(2):15. https://doi.org/10.3390/dj4020015
Chicago/Turabian StyleBorg, Peter, James Puryer, Lisa McNally, and Dominic O’Sullivan. 2016. "The Overall Survival, Complication-Free Survival, and Related Complications of Combined Tooth-Implant Fixed Partial Dentures: A Literature Review" Dentistry Journal 4, no. 2: 15. https://doi.org/10.3390/dj4020015