Overview of Foodborne Disease Outbreaks in Brazil from 2000 to 2018

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
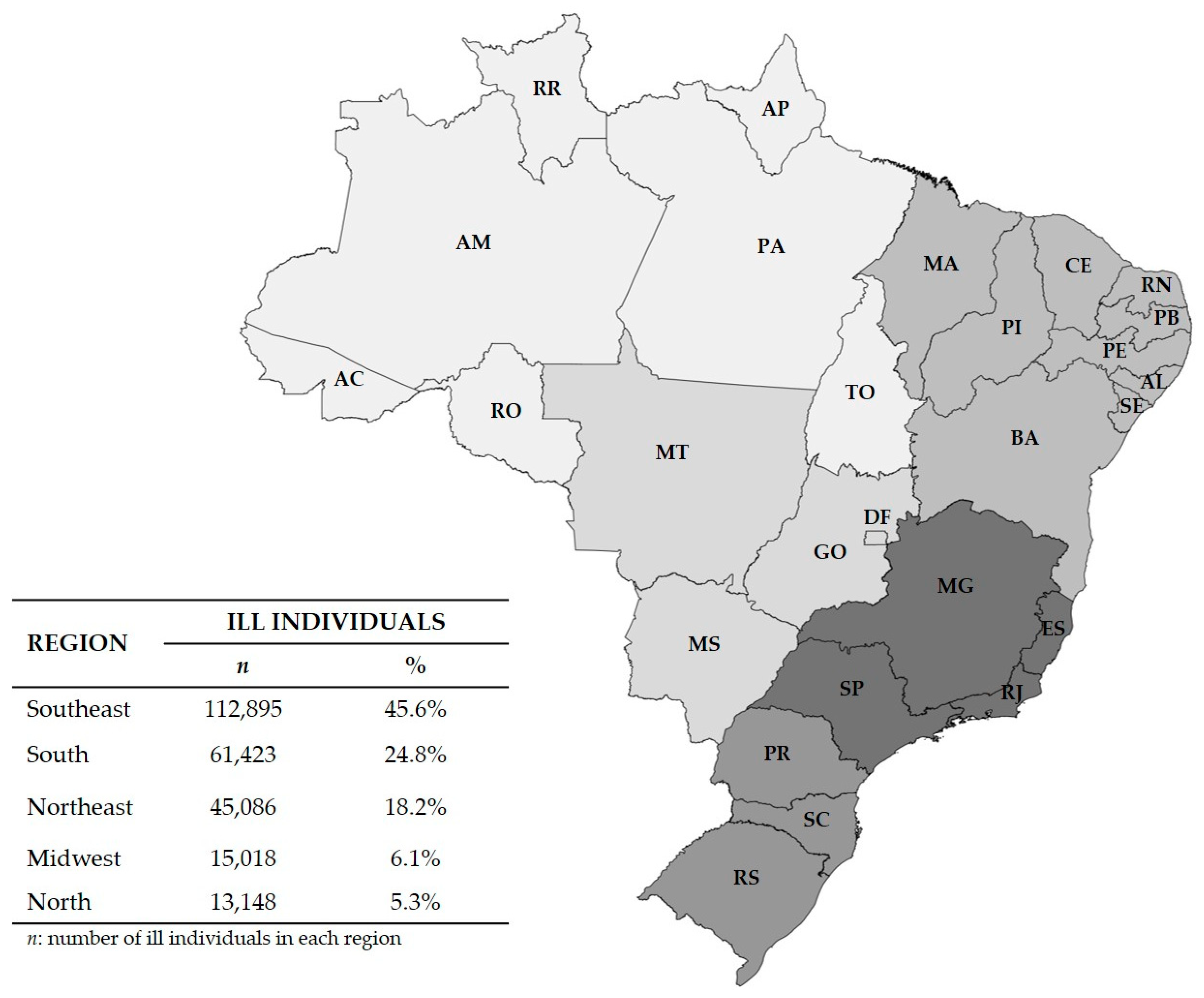
3.1. Data from the Brazilian Ministry of Health
3.2. Data from the Scientific Literature
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). Surveillance Resource Center. Estimates of Foodborne Illness in the United States. 2018. Available online: https://www.cdc.gov/foodborneburden/2011-foodborne-estimates.html (accessed on 15 January 2019).
- Brazil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Doenças Transmitidas por Alimentos: Causas, Sintomas, Tratamento e Prevenção. Brasília, DF. 2019. Available online: http://portalms.saude.gov.br/saude-de-a-z/doencas-transmitidas-por-alimentos (accessed on 27 May 2019).
- Nyachuba, D.G. Foodborne illness: Is it on the rise? Nutr. Rev. 2010, 68, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Welker, C.A.D.; Both, J.M.C.; Longaray, S.M.; Haas, S.; Soeiro, M.L.T.; Ramos, R.C. Análise microbiológica dos alimentos envolvidos em surtos de doenças transmitidas por alimentos (DTA) ocorridos no estado do Rio Grande do Sul, Brasil. Rev. Bras. Biocienc. 2010, 8, 44–48. [Google Scholar]
- World Health Organization (WHO). Food Safety. Geneva. 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/food-safety (accessed on 15 January 2019).
- Nsoesie, E.O.; Kluberg, S.A.; Brownstein, J.S. Online reports of foodborne illness capture foods implicated in official foodborne outbreak reports. Prev. Med. 2014, 67, 264–269. [Google Scholar] [CrossRef] [PubMed]
- McCabe-Sellers, B.J.; Beattie, S.E. Food safety: Emerging trends in foodborne illness surveillance and prevention. J. Am. Diet. Assoc. 2004, 104, 1708–1717. [Google Scholar] [CrossRef] [PubMed]
- Dewey-Mattia, D.; Manikonda, K.; Hall, A.J.; Wise, M.E.; Crowe, S.J. Surveillance for foodborne disease outbreaks—United States, 2009–2015. Morbidity and mortality weekly report. MMWR Surveill. Sum. 2018, 67, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Draeger, C.L.; Akutsu, R.; Zandonadi, R.; Da Silva, I.; Botelho, R.; Araújo, W. Brazilian foodborne disease national survey: Evaluating the landscape after 11 years of implementation to advance research, policy, and practice in public health. Nutrients 2019, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Garcia, D.P.; Duarte, D.A. Epidemiological profile outbreaks of foodborne illness occured in Brazil. REAS 2014, 6, 545–554. [Google Scholar]
- Silva, E.P.; Bergamini, A.M.M.; Oliveira, M.A. Alimentos e agentes etiológicos envolvidos em toxinfecções na região de Ribeirão Preto, SP, Brazil: 2005 a 2008. Bol Epidemiológico Paulista 2010, 7, 4–10. [Google Scholar]
- Rodriguez, D.M.; Suarez, M.C. Salmonella spp. in the pork supply chain: A risk approach. Rev. Colom. Cienc. Pecua. 2014, 27, 65–75. [Google Scholar]
- Brazil. Ministério da Saúde. Coordenação Geral de Doenças Transmissíveis. Unidade Técnica de Doenças de Veiculação Hídrica e Alimentar. Surtos de Doenças Transmitidas por Alimentos no Brazil—2000 a 2016; Boletim Eletrônico Epidemiológico: Brasília, Brasil, 2016. [Google Scholar]
- Brazil. Ministério da Saúde. Surtos de Doenças Transmitidas por Alimentos no Brazil—2009 a 2018. Boletim Eletrônico Epidemiológico, Brasília, DF. 2019. Available online: http://portalarquivos2.saude.gov.br/images/pdf/2019/fevereiro/15/Apresenta----o-Surtos-DTA---Fevereiro-2019.pdf (accessed on 15 January 2019).
- World Health Organization (WHO). WHO Estimates of the Global Burden of Foodborne Diseases: Foodborne Disease Burden Epidemiology Reference Group 2007–2015. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/199350/9789241565165_eng.pdf?sequence=1 (accessed on 23 June 2019).
- Public Health Agency of Canada (PHAC). Yearly Food-Borne Illness Estimates for Canada. Available online: https://www.canada.ca/en/public-health/services/foodborne-illness-canada/yearly-food-borne-illness-estimates-canada.html (accessed on 11 September 2019).
- Archer, B.; Astridge, K.; Bell, R.; Combs, B.; Corvisy, R.; Draper, A.; Furlong, C. Monitoring the incidence and causes of diseases potentially transmitted by food in Australia: Annual report of the OzFoodNet network, 2012. Commun. Dis. Intell. 2018, 42, S2209–S6051. [Google Scholar]
- Li, Y.; Huang, Y.; Yang, J.; Liu, Z.; Li, Y.; Yao, X.; Wei, B.; Tang, Z.; Chen, S.; Liu, D.; et al. Bacteria and poisonous plants were the primary causative hazards of foodborne disease outbreak: A seven-year survey from Guangxi, South China. BMC Public Health 2018, 18, 519. [Google Scholar] [CrossRef] [PubMed]
- Ritter, A.; Tondo, E. Review article foodborne illnesses in Brazil: Control measures for 2014 FIFA world cup travelers. J. Infect. Dev. Ctries. 2014, 8, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Forsythe, S.J. Microbiologia da Segurança dos Alimentos, 2nd ed.; Artmed: Porto Alegre, Brasil, 2013; pp. 1–607. [Google Scholar]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico. 2010. Available online: http://www.ibge.gov.br/home/estatistica/populacao/censo2010/default.shtm (accessed on 8 March 2017).
- Brazil. Ministério da Saúde. Portaria de Consolidação nº 5, de 28 de Setembro de 2017. Consolidação das Normas Sobre as Ações e os Serviços de Saúde do Sistema Único de Saúde. Diário Oficial da União, Brasília, DF. 2017. Available online: http://portalarquivos2.saude.gov.br/images/pdf/2018/marco/29/PRC-5-Portaria-de-Consolida----o-n---5--de-28-de-setembro-de-2017.pdf (accessed on 5 July 2019).
- Sistema Nacional de Informações sobre Saneamento (SNIS). Ministério do Desenvolvimento Regional. 2017. Available online: http://www.snis.gov.br/ (accessed on 30 July 2019).
- Merussi, G.D.; Maffei, D.F.; Catanozi, M.P.L.M. Outbreaks of gastroenteritis related to dairy products intake in the state of Sao Paulo from 2000 to 2010. Alim. Nutr. 2012, 23, 639–645. [Google Scholar]
- Silva, S.S.O.; Nova, P.A.C.; Pinto, A.T. Caracterização de surtos de toxinfecções alimentares confirmados, no município de Porto Alegre, entre 2005 e 2009. Hig. Alim. 2014, 28, 238–239. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Salmonella and Food. 2018. Available online: https://www.cdc.gov/features/salmonella-food/index.html (accessed on 10 February 2019).
- Callejón, R.; Rodríguez-Naranjo, M.I.; Ubeda, C.; Hornedo-Ortega, R.; Garcia-Parrilla, M.C.; Troncoso, A.M. Reported foodborne outbreaks due to fresh produce in the United States and European Union: Trends and causes. Foodborne Pathog. Dis. 2015, 12, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Kozak, G.; Macdonald, D.; Landry, L.; Farber, J. Review foodborne outbreaks in Canada linked to produce: 2001 through 2009. J. Food Prot. 2013, 76, 173–183. [Google Scholar] [CrossRef]
- Hull-Jackson, C.; Adesiyun, A.A. Foodborne disease outbreaks in Barbados (1998–2009): A 12-year review. J. Infect. Dev. Ctries. 2019, 13, 1–10. [Google Scholar] [CrossRef]
- Scallan, E.; Hoekstra, R.M.; Angulo, F.J.; Tauxe, R.V.; Widdowson, M.; Roy, S.L.; Jones, J.L.; Griffin, P.M. Foodborne illness acquired in the United States—Major pathogens. Emerg. Infect. Dis. 2011, 17, 7–15. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Scientific Report of EFSA and ECDC. The European Union Summary Report on Trends and Sources of Zoonoses, Zoonotic Agents and Food-borne Outbreaks in 2012. EFSA J. 2014, 12, 3547. [Google Scholar] [CrossRef]
- Ting-Ting, L.I. Analysis of the food poisoning in China from 2002 to 2011. J. Shanxi Med. Univ. 2012, 6, 008. [Google Scholar]
- Fernandez, A.T.; Fortes, M.L.M.; Alexandre, M.H.S.; Bastos, C.S.P.; Viana, E.P.L. Ocorrência de surtos de doenças transmitidas por alimentos na cidade do Rio de Janeiro. Hig. Alim. 2003, 17, 58–63. [Google Scholar]


{kind=link}
| Year | Outbreaks | Exposed Individuals | Sick Individuals | Dead Individuals |
|---|---|---|---|---|
| 2000 | 545 | 31,943 | 9613 | 4 |
| 2001 | 897 | 211,228 | 15,706 | 5 |
| 2002 | 823 | 116,962 | 12,402 | 5 |
| 2003 | 620 | 688,742 | 17,981 | 4 |
| 2004 | 645 | 368,158 | 21,781 | 21 |
| 2005 | 923 | 241,991 | 17,279 | 12 |
| 2006 | 577 | 49,044 | 10,356 | 8 |
| 2007 | 683 | 25,195 | 11,635 | 11 |
| 2008 | 641 | 23,275 | 8736 | 26 |
| 2009 | 594 | 24,014 | 9407 | 12 |
| 2010 | 498 | 23,954 | 8628 | 11 |
| 2011 | 795 | 52,640 | 17,884 | 4 |
| 2012 | 863 | 42,138 | 14,670 | 10 |
| 2013 | 861 | 64,340 | 17,455 | 8 |
| 2014 | 886 | 124,359 | 15,700 | 9 |
| 2015 | 673 | 35,826 | 10,676 | 17 |
| 2016 | 538 | 200,896 | 9935 | 7 |
| 2017 | 598 | 47,218 | 9320 | 12 |
| 2018 | 503 | 57,297 | 8406 | 9 |
| Total | 13,163 | 2,429,220 | 247,570 | 195 |
| Component | Individuals | |
|---|---|---|
| n | % | |
| Confirmatory criteria | ||
| Inconclusive | 111,914 | 45.2 |
| Epidemiological survey | 56,203 | 22.7 |
| Clinical analyses | 32,693 | 13.2 |
| Bromatological analyses | 24,969 | 10.1 |
| Epidemiological-clinical-bromatological analyses | 21,791 | 8.8 |
| Foods implicated | ||
| Not identified | 113,571 | 45.9 |
| Water | 29,690 | 12.0 |
| Mixed foods | 25,834 | 10.4 |
| Multiple foods | 24,206 | 9.8 |
| Eggs/egg products | 17,075 | 6.9 |
| Red meats | 8772 | 3.5 |
| Others * | 28,422 | 11.5 |
| Etiological agents | ||
| Not identified | 93,981 | 38.0 |
| Salmonella spp. | 35,743 | 14.4 |
| Rotavirus | 24,434 | 9.9 |
| Escherichia coli | 18,398 | 7.4 |
| Staphylococcus aureus | 15,724 | 6.4 |
| Bacillus cereus | 8213 | 3.3 |
| Inconclusive | 8135 | 3.3 |
| Norovirus | 6076 | 2.5 |
| Clostridium perfringes | 5761 | 2.3 |
| Shigella sonnei | 5035 | 2.0 |
| Others ** | 26,070 | 10.5 |
| Sites of occurrence | ||
| Homes | 30,964 | 12.5 |
| Daycare/school | 26,143 | 10.6 |
| Restaurants/bakeries | 22,965 | 9.3 |
| Not identified | 20,305 | 8.2 |
| Events | 18,898 | 7.6 |
| Hospitals | 7615 | 3.1 |
| Asylums | 1106 | 0.4 |
| Scattered sites | 119,574 | 48.3 |
| Component | Studies | |
|---|---|---|
| n | % | |
| Foods implicated | ||
| Mixed foods | 18 | 31.6 |
| Water | 12 | 21.1 |
| Uninformed | 8 | 14.0 |
| Red meats and poultry | 6 | 10.5 |
| Fish and seafood | 4 | 7.0 |
| Acai/acai juice | 4 | 7.0 |
| Eggs/egg products | 2 | 3.5 |
| Vegetables | 2 | 3.5 |
| Sugarcane juice | 1 | 1.8 |
| Etiological agents | ||
| Salmonella spp. | 13 | 22.8 |
| Trypanosoma cruzi | 8 | 14.0 |
| Norovirus | 7 | 12.3 |
| Virus da Hepatite A | 4 | 7.0 |
| Fish Toxin | 4 | 7.0 |
| Rotavirus | 3 | 5.3 |
| Clostridium botulinum | 3 | 5.3 |
| Uninformed | 3 | 5.3 |
| Bacillus cereus | 3 | 5.3 |
| Others * | 9 | 15.8 |
| Sites of occurrence | ||
| Residences | 26 | 45.6 |
| Uninformed | 18 | 31.6 |
| Restaurants | 4 | 7.0 |
| Workplaces | 4 | 7.0 |
| Events | 2 | 3.5 |
| Hospitals | 1 | 1.8 |
| Asylums | 1 | 1.8 |
| Ships | 1 | 1.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finger, J.A.F.F.; Baroni, W.S.G.V.; Maffei, D.F.; Bastos, D.H.M.; Pinto, U.M. Overview of Foodborne Disease Outbreaks in Brazil from 2000 to 2018. Foods 2019, 8, 434. https://doi.org/10.3390/foods8100434
Finger JAFF, Baroni WSGV, Maffei DF, Bastos DHM, Pinto UM. Overview of Foodborne Disease Outbreaks in Brazil from 2000 to 2018. Foods. 2019; 8(10):434. https://doi.org/10.3390/foods8100434
Chicago/Turabian StyleFinger, Jéssica A. F. F., Wilma S. G. V. Baroni, Daniele F. Maffei, Deborah H. M. Bastos, and Uelinton M. Pinto. 2019. "Overview of Foodborne Disease Outbreaks in Brazil from 2000 to 2018" Foods 8, no. 10: 434. https://doi.org/10.3390/foods8100434
APA StyleFinger, J. A. F. F., Baroni, W. S. G. V., Maffei, D. F., Bastos, D. H. M., & Pinto, U. M. (2019). Overview of Foodborne Disease Outbreaks in Brazil from 2000 to 2018. Foods, 8(10), 434. https://doi.org/10.3390/foods8100434