
Evaluation of a Granular Bone Substitute for Bone Regeneration Using an Optimized In Vivo Alveolar Cleft Model
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Isolation and Culture
2.2. Phenotypic Characterization
2.3. Differientiation Capacities
2.4. Biomaterial
2.5. Animals
2.6. Surgical Procedures and Material Placement
2.7. Tomodensitometric Analyses
2.8. Statistical Analysis
3. Results
3.1. Cell Analysis
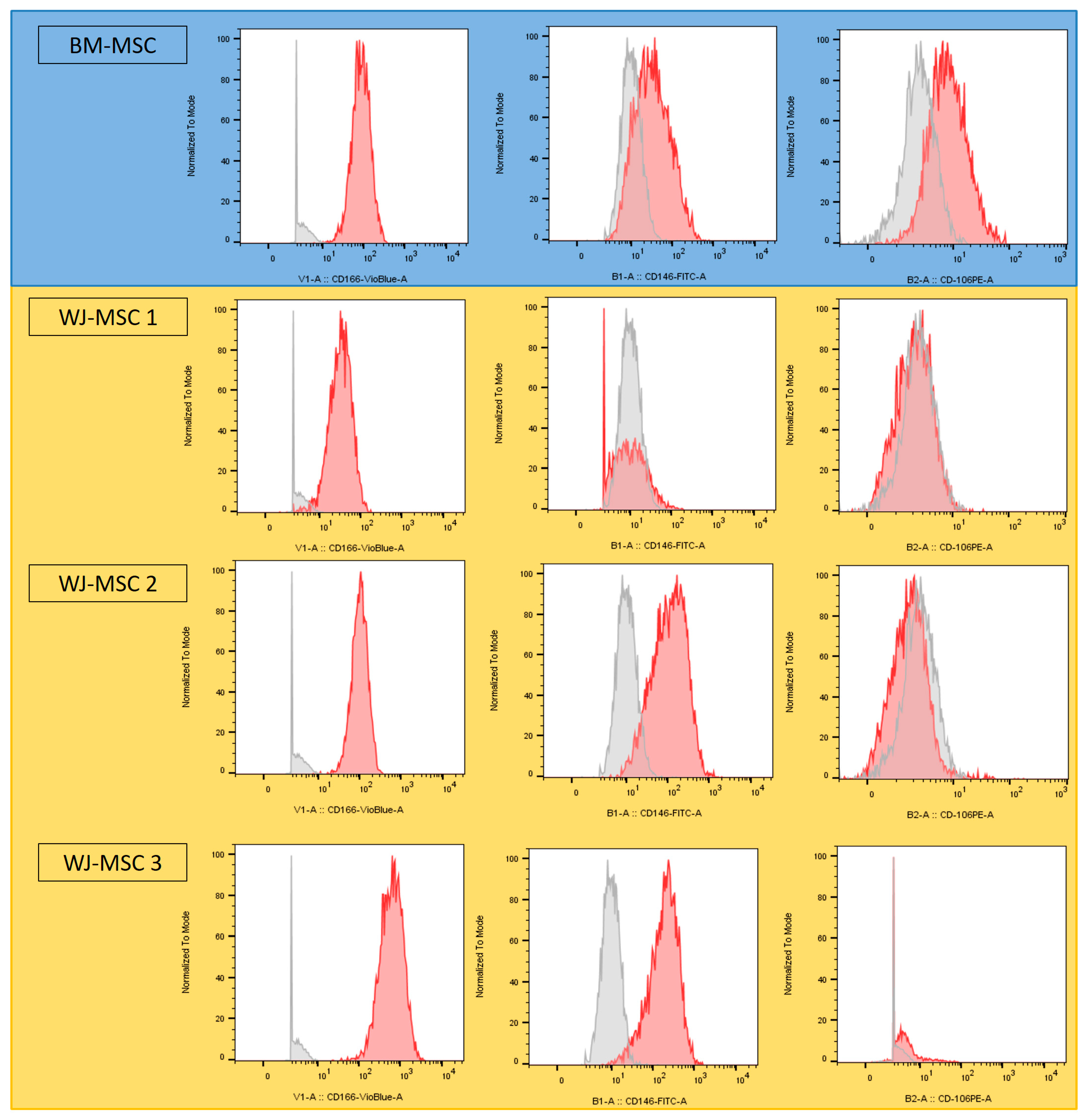
3.1.1. Phenotype Analysis
3.1.2. Differentiation Capacity Analysis
3.2. Cleft Model Optimization
3.2.1. Surgical Procedure
3.2.2. Computed Tomography Analysis
3.3. Bone Regeneration Study
3.3.1. Biomaterial Implantation
3.3.2. Computed Tomography Analysis
3.3.3. Bone Volume and Bone Mineral Density
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Miltenyi Biotec Reference | Panel | ||||||
|---|---|---|---|---|---|---|---|---|
| CD44-BV2011 | 562,890 | 1 | ||||||
| CD90-FITC | 559,869 | 1 | ||||||
| CD34-PE | 555,822 | 1 | ||||||
| CD73-PECy7 | 561,258 | 1 | ||||||
| CD105-APC | 562,408 | 1 | ||||||
| CD45-APCH7 | 557,833 | 1 | ||||||
| CD166-BV421 | 562,936 | 2 | ||||||
| CD146-FITC | 560,846 | 2 | ||||||
| CD106-PE | 555,647 | 2 | ||||||
| CD39-APCH7 | 560,239 | 2 | ||||||
| Channel | V1 | V2 | B1 | B2 | B3 | B4 | R1 | R2 |
| Panel 1 | CD44 | Viability | CD90 | CD34 | CD73 | CD105 | CD45 | |
| Panel 2 | CD166 | Viability | CD146 | CD106 | CD19 | CD39 | ||
| Empty | Biomaterial | Biomaterial + MSCs | ||||
|---|---|---|---|---|---|---|
| Week 4 | Week 8 | Week 4 | Week 8 | Week 4 | Week 8 | |
| 65.4870226 | 71.1397164 | 103.679512 | 107.26423 | 84.7664404 | 88.7551674 | |
| 58.872241 | 63.4156236 | 88.8578814 | 92.1241866 | 79.3924439 | 90.3266916 | |
| 75.1626814 | 80.8667322 | 61.5975858 | 71.5300296 | 66.5312816 | 71.420468 | |
| 81.914415 | 88.9777144 | 87.2144574 | 92.1070676 | 89.8781738 | 92.0591344 | |
| 56.1777104 | 67.3358746 | 92.3843954 | 88.2689878 | 88.2039356 | 89.1180902 | |
| 65.5554986 | 75.9980886 | 86.9713676 | 84.0474424 | 85.3176722 | 71.5300296 | |
| 74.673078 | 81.794582 | 97.8727468 | 101.584146 | 100.457716 | 89.1317854 | |
| 74.0328274 | 74.29646 | 94.000429 | 101.827236 | 98.5301164 | 108.753583 | |
| 76.6451868 | 80.9454796 | 97.355753 | 100.440597 | 105.463311 | 101.337632 | |
| N/A | N/A | 85.492286 | 94.7742078 | N/A | 110.845525 | |
| N/A | N/A | 96.7771308 | 107.099888 | N/A | N/A | |
| Mean | 69.836 | 76.086 | 90.200 | 94.643 | 88.727 | 91.328 |
| SD | 8.701 | 7.985 | 11.026 | 10.713 | 11.845 | 13.295 |
| Empty | Biomaterial | Biomaterial + MSCs | ||||
|---|---|---|---|---|---|---|
| Week 4 | Week 8 | Week 4 | Week 8 | Week 4 | Week 8 | |
| 18.74994 | 34.0908 | 87.49972 | 85.79518 | 82.95428 | 84.09064 | |
| 47.72712 | 23.29538 | 80.68156 | 85.227 | 69.31796 | 93.7497 | |
| 52.27256 | 65.90888 | 20.45448 | 43.74986 | 34.65898 | 42.6135 | |
| 63.06798 | 73.29522 | 88.0679 | 96.5906 | 93.18152 | 93.7497 | |
| 14.2045 | 41.47714 | 96.5906 | 86.93154 | 89.77244 | 91.47698 | |
| 32.38626 | 55.68164 | 80.11338 | 79.5452 | 78.40884 | 67.04524 | |
| 55.68164 | 68.1816 | 97.15878 | 130.11322 | 106.81784 | 81.81792 | |
| 47.72712 | 49.99984 | 90.9088 | 113.636 | 105.68148 | 124.43142 | |
| 44.31804 | 52.84074 | 106.81784 | 111.93146 | 125.56778 | 120.45416 | |
| N/A | N/A | 77.27248 | 99.4315 | N/A | 130.6814 | |
| N/A | N/A | 99.4315 | 124.43142 | N/A | N/A | |
| Mean | 41.793 | 51.641 | 84.091 | 96.126 | 87.373 | 93.011 |
| SD | 16.631 | 16.513 | 22.970 | 24.191 | 26.020 | 27.043 |


References
- Degner, D.A. Facial reconstructive surgery. Clin. Tech. Small Anim. Pract. 2007, 22, 82–88. [Google Scholar] [CrossRef]
- Krüger, E. Reconstruction of bone and soft tissue in extensive facial defects. J. Oral Maxillofac. Surg. 1982, 40, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, D.A. Fibula free flap mandibular reconstruction. Clin. Plast. Surg. 1994, 21, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Sassano, P.; Gennaro, P.; Chisci, G.; Gabriele, G.; Aboh, I.V.; Mitro, V.; di Curzio, P. Calvarial onlay graft and submental incision in treatment of atrophic edentulous mandibles: An approach to reduce postoperative complications. J. Craniofacial Surg. 2014, 25, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Myeroff, C.; Archdeacon, M. Autogenous bone graft: Donor sites and techniques. J. Bone Jt. Surg. Am. 2011, 93, 2227–2236. [Google Scholar] [CrossRef] [PubMed]
- Mossey, P.A.; Modell, B. Epidemiology of oral clefts 2012: An international perspective. Front. Oral Biol. 2012, 16, 1–18. [Google Scholar] [CrossRef]
- De Bérail, A.; Lauwers, F.; Noirrit Esclassan, E.; Woisard Bassols, V.; Gardini, B.; Galinier, P. Épidémiologie des malformations associées aux fentes labiales et palatines à propos d’une étude rétrospective de 324 cas [Epidemiology of malformations associated with cleft lip and palate: A retrospective study of 324 cases]. Arch. Pediatr. 2015, 22, 816–821. [Google Scholar] [CrossRef]
- Farronato, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Giannini, L.; Galbiati, G.; Maspero, C. Cleft lip and/or palate: Review. Minerva Stomatol. 2014, 63, 111–126. (In Italian) [Google Scholar]
- Worley, M.L.; Patel, K.G.; Kilpatrick, L.A. Cleft Lip and Palate. Clin. Perinatol. 2018, 45, 661–678. [Google Scholar] [CrossRef]
- Rodman, R.E.; Tatum, S. Controversies in the Management of Patients with Cleft Lip and Palate. Facial Plast. Surg. Clin. N. Am. 2016, 24, 255–264. [Google Scholar] [CrossRef]
- Shaw, W.C.; Semb, G.; Nelson, P.; Brattström, V.; Mølsted, K.; Prahl-Andersen, B.; Gundlach, K.K. The Eurocleft project 1996–2000: Overview. J. Craniomaxillofac. Surg. 2001, 29, 131–140; discussion 141–142. [Google Scholar] [CrossRef] [PubMed]
- Schalet, G.; Langlie, J.; Kim, M.; Thaller, S. The Rule of 10s for Cleft Repair: A Historical Review of the Literature. J. Craniofacial Surg. 2023, 34, 884–887. [Google Scholar] [CrossRef] [PubMed]
- Fisher, D.M. Unilateral cleft lip repair: An anatomical subunit approximation technique. Plast. Reconstr. Surg. 2005, 116, 61–71. [Google Scholar] [CrossRef]
- Millard, D.R., Jr. Closure of bilateral cleft lip and elongation of columella by two operations in infancy. Plast. Reconstr. Surg. 1971, 47, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Mohler, L.R. Unilateral cleft lip repair. Plast. Reconstr. Surg. 1987, 80, 511–517. [Google Scholar] [CrossRef]
- Noordhoff, M.S. Reconstruction of vermilion in unilateral and bilateral cleft lips. Plast. Reconstr. Surg. 1984, 73, 52–61. [Google Scholar] [CrossRef]
- Dissaux, C.; Bodin, F.; Grollemund, B.; Bridonneau, T.; Kauffmann, I.; Mattern, J.F.; Bruant-Rodier, C. Evaluation of success of alveolar cleft bone graft performed at 5 years versus 10 years of age. J. Craniomaxillofac. Surg. 2016, 44, 21–26. [Google Scholar] [CrossRef]
- Weissler, E.H.; Paine, K.M.; Ahmed, M.K.; Taub, P.J. Alveolar Bone Grafting and Cleft Lip and Palate: A Review. Plast. Reconstr. Surg. 2016, 138, 1287–1295. [Google Scholar] [CrossRef]
- Kang, N.H. Current Methods for the Treatment of Alveolar Cleft. Arch. Plast. Surg. 2017, 44, 188–193. [Google Scholar] [CrossRef]
- Bajaj, A.K.; Wongworawat, A.A.; Punjabi, A. Management of alveolar clefts. J. Craniofacial Surg. 2003, 14, 840–846. [Google Scholar] [CrossRef]
- Rawashdeh, M.A.; Telfah, H. Secondary alveolar bone grafting: The dilemma of donor site selection and morbidity. Br. J. Oral Maxillofac. Surg. 2008, 46, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Rawashdeh, M.A. Morbidity of iliac crest donor site following open bone harvesting in cleft lip and palate patients. Int. J. Oral Maxillofac. Surg. 2008, 37, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Berthiaume, F.; Maguire, T.J.; Yarmush, M.L. Tissue engineering and regenerative medicine: History, progress, and challenges. Annu. Rev. Chem. Biomol. Eng. 2011, 2, 403–430. [Google Scholar] [CrossRef] [PubMed]
- Jordana, F.; Le Visage, C.; Weiss, P. Substituts osseux [Bone substitutes]. Med. Sci. 2017, 33, 60–65. (In French) [Google Scholar] [CrossRef]
- Chisci, G.; Fredianelli, L. Therapeutic Efficacy of Bromelain in Alveolar Ridge Preservation. Antibiotics 2022, 11, 1542. [Google Scholar] [CrossRef]
- Covani, U.; Giammarinaro, E.; Panetta, D.; Salvadori, P.A.; Cosola, S.; Marconcini, S. Alveolar Bone Remodeling with or without Collagen Filling of the Extraction Socket: A High-Resolution X-ray Tomography Animal Study. J. Clin. Med. 2022, 11, 2493. [Google Scholar] [CrossRef]
- Barre, A.; Naudot, M.; Colin, F.; Sevestre, H.; Collet, L.; Devauchelle, B.; Lack, S.; Marolleau, J.P.; Le Ricousse, S. An Alginate-Based Hydrogel with a High Angiogenic Capacity and a High Osteogenic Potential. BioRes. Open Access 2020, 9, 174–182. [Google Scholar] [CrossRef]
- Hollý, D.; Klein, M.; Mazreku, M.; Zamborský, R.; Polák, Š.; Danišovič, Ľ.; Csöbönyeiová, M. Stem Cells and Their Derivatives-Implications for Alveolar Bone Regeneration: A Comprehensive Review. Int. J. Mol. Sci. 2021, 22, 11746. [Google Scholar] [CrossRef]
- Naudot, M.; Garcia Garcia, A.; Jankovsky, N.; Barre, A.; Zabijak, L.; Azdad, S.Z.; Collet, L.; Bedoui, F.; Hébraud, A.; Schlatter, G.; et al. The combination of a poly-caprolactone/nano-hydroxyapatite honeycomb scaffold and mesenchymal stem cells promotes bone regeneration in rat calvarial defects. J. Tissue Eng. Regen. Med. 2020, 14, 1570–1580. [Google Scholar] [CrossRef]
- Naudot, M.; Davrou, J.; Djebara, A.E.; Barre, A.; Lavagen, N.; Lardière, S.; Azdad, S.Z.; Zabijak, L.; Lack, S.; Devauchelle, B.; et al. Functional Validation of a New Alginate-based Hydrogel Scaffold Combined with Mesenchymal Stem Cells in a Rat Hard Palate Cleft Model. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2743. [Google Scholar] [CrossRef]
- Yamada, T.; Mishima, K.; Fujiwara, K.; Imura, H.; Sugahara, T. Cleft lip and palate in mice treated with 2,3,7,8-tetrachlorodibenzo-p-dioxin: A morphological in vivo study. Congenit. Anom. 2006, 46, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Huang, Z.; Wang, L.; Li, H.; Zhang, Y.; Shao, M.; Chen, Y. Tamoxifen exposure induces cleft palate in mice. Br. J. Oral Maxillofac. Surg. 2021, 59, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Juriloff, D.M.; Harris, M.J. Mouse genetic models of cleft lip with or without cleft palate. Birth Defects Res. A Clin. Mol. Teratol. 2008, 82, 63–77. [Google Scholar] [CrossRef]
- Gong, S.G.; White, N.J.; Sakasegawa, A.Y. The Twirler mouse, a model for the study of cleft lip and palate. Arch. Oral Biol. 2000, 45, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xu, W.; Chen, Y.; Wang, J. Alveolar bone repair of rhesus monkeys by using BMP-2 gene and mesenchymal stem cells loaded three-dimensional printed bioglass scaffold. Sci. Rep. 2019, 9, 18175. [Google Scholar] [CrossRef] [PubMed]
- Yuanzheng, C.; Yan, G.; Ting, L.; Yanjie, F.; Peng, W.; Nan, B. Enhancement of the repair of dog alveolar cleft by an autologous iliac bone, bone marrow-derived mesenchymal stem cell, and platelet-rich fibrin mixture. Plast. Reconstr. Surg. 2015, 135, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Du, C.; Ma, L. Construction of a Pig Alveolar Cleft Model in Imitation of Cleft Lip and Palate Congenital Deformity. Tissue Eng. Part C Methods 2022, 28, 127–135. [Google Scholar] [CrossRef]
- De Ruiter, A.; Meijer, G.; Dormaar, T.; Janssen, N.; van der Bilt, A.; Slootweg, P.; de Bruijn, J.; van Rijn, L.; Koole, R. β-TCP versus autologous bone for repair of alveolar clefts in a goat model. Cleft Palate Craniofacial J. 2011, 48, 654–662. [Google Scholar] [CrossRef]
- Martín-Del-Campo, M.; Rosales-Ibañez, R.; Rojo, L. Biomaterials for Cleft Lip and Palate Regeneration. Int. J. Mol. Sci. 2019, 20, 2176. [Google Scholar] [CrossRef]
- Nguyen, P.D.; Lin, C.D.; Allori, A.C.; Ricci, J.L.; Saadeh, P.B.; Warren, S.M. Establishment of a critical-sized alveolar defect in the rat: A model for human gingivoperiosteoplasty. Plast. Reconstr. Surg. 2009, 123, 817–825. [Google Scholar] [CrossRef]
- Jelusic, D.; Zirk, M.L.; Fienitz, T.; Plancak, D.; Puhar, I.; Rothamel, D. Monophasic ß-TCP vs. biphasic HA/ß-TCP in two-stage sinus floor augmentation procedures—A prospective randomized clinical trial. Clin. Oral Implants Res. 2017, 28, e175–e183. [Google Scholar] [CrossRef]
- De Oliveira, J.M., Jr.; Montagner, P.G.; Carrijo, R.C.; Martinez, E.F. Physical characterization of biphasic bioceramic materials with different granulation sizes and their influence on bone repair and inflammation in rat calvaria. Sci. Rep. 2021, 11, 4484. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, N.Z.; Doschak, M.R.; Major, P.W.; Talwar, R. Reliable critical sized defect rodent model for cleft palate research. J. Craniomaxillofac. Surg. 2014, 42, 1840–1846. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.L.; Medicetty, S.; Bledsoe, A.R.; Rachakatla, R.S.; Choi, M.; Merchav, S.; Luo, Y.; Rao, M.S.; Velagaleti, G.; Troyer, D. Human umbilical cord matrix stem cells: Preliminary characterization and effect of transplantation in a rodent model of Parkinson’s disease. Stem Cells 2006, 24, 781–792. [Google Scholar] [CrossRef]
- Cabrera-Pérez, R.; Monguió-Tortajada, M.; Gámez-Valero, A.; Rojas-Márquez, R.; Borràs, F.E.; Roura, S.; Vives, J. Osteogenic commitment of Wharton’s jelly mesenchymal stromal cells: Mechanisms and implications for bioprocess development and clinical application. Stem Cell Res. Ther. 2019, 10, 356. [Google Scholar] [CrossRef]
- Seshareddy, K.; Troyer, D.; Weiss, M.L. Method to isolate mesenchymal-like cells from Wharton’s Jelly of umbilical cord. Methods Cell Biol. 2008, 86, 101–119. [Google Scholar] [CrossRef]
- Kikuchi-Taura, A.; Taguchi, A.; Kanda, T.; Inoue, T.; Kasahara, Y.; Hirose, H.; Sato, I.; Matsuyama, T.; Nakagomi, T.; Yamahara, K.; et al. Human umbilical cord provides a significant source of unexpanded mesenchymal stromal cells. Cytotherapy 2012, 14, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Samsonraj, R.M.; Raghunath, M.; Nurcombe, V.; Hui, J.H.; van Wijnen, A.J.; Cool, S.M. Concise Review: Multifaceted Characterization of Human Mesenchymal Stem Cells for Use in Regenerative Medicine. Stem Cells Transl. Med. 2017, 6, 2173–2185. [Google Scholar] [CrossRef]
- Sun, J.; Xu, Y.; Chen, Z. Establishment of a rat model for alveolar cleft with bone wax. J. Oral Maxillofac. Surg. 2015, 73, 733.e1–733.e10, Erratum in J. Oral Maxillofac. Surg. 2015, 73, 1440. [Google Scholar] [CrossRef]







| ID | Length (mm) | Width (mm) | Height (mm) |
|---|---|---|---|
| FLAP 1-02 | 6.600 | 1.970 | 2.333 |
| FLAP 1-03 | 7.053 | 2.146 | 2.322 |
| FLAP 1-04 | 6.139 | 1.987 | 1.811 |
| FLAP 1-06 | 5.664 | 2.181 | 2.216 |
| FLAP 1-07 | 6.103 | 1.899 | 2.286 |
| FLAP 1-08 | 7.194 | 2.005 | 2.321 |
| FLAP 1-09 | 6.402 | 2.040 | 1.900 |
| Mean | 6.450 | 2.033 | 2.170 |
| SD | 0.544 | 0.100 | 0.220 |
| ID | Length (mm) | Width (mm) | Height (mm) |
|---|---|---|---|
| FLAP 2-01 | 7.2 | 2.1 | 2.4 |
| FLAP 2-02 | 6.4 | 2.1 | 2.6 |
| FLAP 2-04 | 6.9 | 2.9 | 2.2 |
| FLAP 2-05 | 7.1 | 2.24 | 3.3 |
| FLAP 2-06 | 7.4 | 2.2 | 2.1 |
| FLAP 2-07 | 6.1 | 2.3 | 2.1 |
| FLAP 2-08 | 7.7 | 2.3 | 3.4 |
| FLAP 2-09 | 6.8 | 2 | 3 |
| FLAP 2-10 | 6.3 | 2.7 | 4.3 |
| FLAP 2-11 | 7.1 | 2.7 | 4.8 |
| FLAP 2-12 | 8.6 | 2.3 | 3.1 |
| FLAP 2-13 | 7.1 | 2.8 | 2.6 |
| FLAP 2-14 | 8.1 | 3.1 | 3.6 |
| FLAP 2-15 | 7.4 | 2.6 | 2.9 |
| FLAP 2-16 | 7.3 | 2.3 | 3.5 |
| FLAP 2-17 | 7.7 | 3.1 | 3.4 |
| FLAP 2-18 | 7.5 | 3.1 | 3.6 |
| FLAP 2-20 | 6.5 | 2 | 2.7 |
| FLAP 2-21 | 6.8 | 2 | 2.4 |
| FLAP 2-22 | 6.9 | 2.1 | 3 |
| FLAP 2-25 | 6.4 | 2 | 2 |
| FLAP 2-26 | 8.4 | 2.4 | 2.3 |
| FLAP 2-27 | 7.8 | 2.4 | 2.5 |
| FLAP 2-29 | 7 | 2.4 | 2 |
| FLAP 2-30 | 7.6 | 2.3 | 2.5 |
| FLAP 2-31 | 6.6 | 2.2 | 2.1 |
| FLAP 2-33 | 6.6 | 2.3 | 3.2 |
| FLAP 2-34 | 7.1 | 3.1 | 3 |
| FLAP 2-35 | 7.2 | 2.9 | 2.8 |
| FLAP 2-36 | 8.5 | 2.1 | 2.4 |
| Mean | 7.203 | 2.435 | 2.860 |
| SD | 0.648 | 0.370 | 0.679 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Destrez, A.; Colin, E.; Testelin, S.; Devauchelle, B.; Dakpé, S.; Naudot, M. Evaluation of a Granular Bone Substitute for Bone Regeneration Using an Optimized In Vivo Alveolar Cleft Model. Bioengineering 2023, 10, 1035. https://doi.org/10.3390/bioengineering10091035
Destrez A, Colin E, Testelin S, Devauchelle B, Dakpé S, Naudot M. Evaluation of a Granular Bone Substitute for Bone Regeneration Using an Optimized In Vivo Alveolar Cleft Model. Bioengineering. 2023; 10(9):1035. https://doi.org/10.3390/bioengineering10091035
Chicago/Turabian StyleDestrez, Alban, Emilien Colin, Sylvie Testelin, Bernard Devauchelle, Stéphanie Dakpé, and Marie Naudot. 2023. "Evaluation of a Granular Bone Substitute for Bone Regeneration Using an Optimized In Vivo Alveolar Cleft Model" Bioengineering 10, no. 9: 1035. https://doi.org/10.3390/bioengineering10091035