
Thermal Characterization and Preclinical Feasibility Verification of an Accessible, Carbon Dioxide-Based Cryotherapy System
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Device Comparison
2.2. Calorimeter Testing
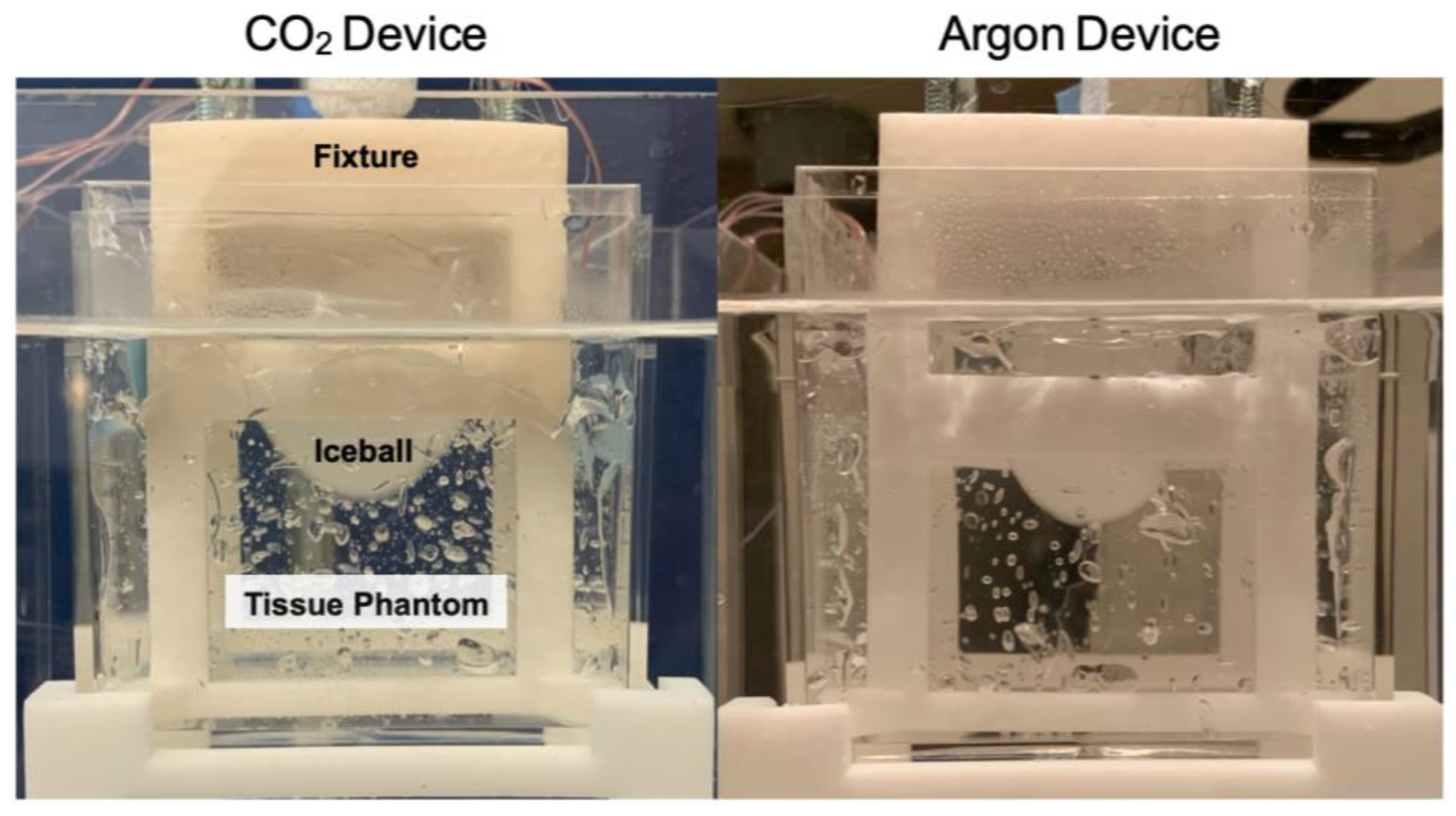
2.3. Tissue Phantom with Heat Load Testing
2.3.1. Tissue Phantom
2.3.2. Mathematical Modeling
2.4. In Vivo Testing
2.4.1. Cryotherapy Procedure in a Canine Model with Spontaneously Occurring Mammary Cancer
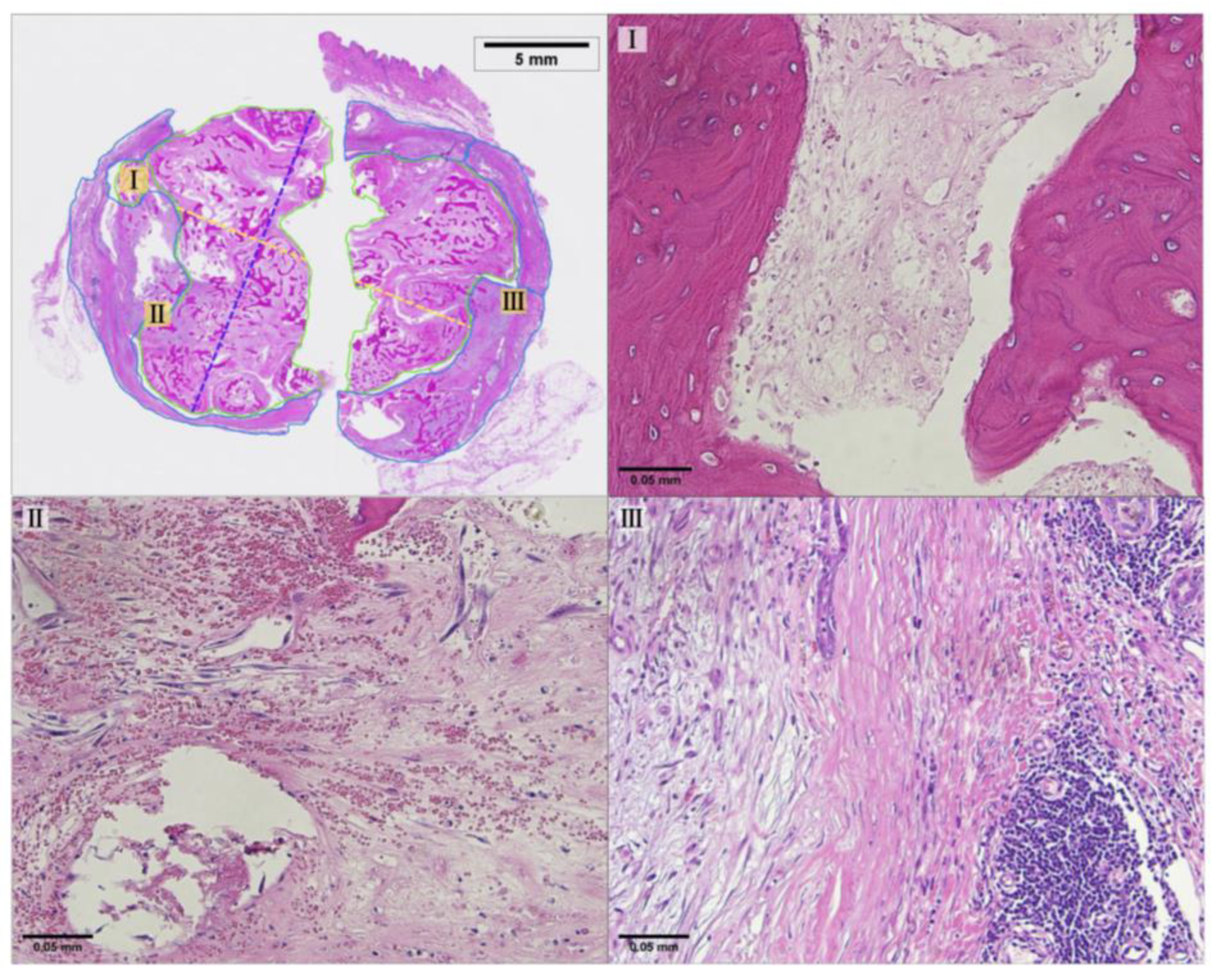
2.4.2. Pathology Methods
3. Results
3.1. Calorimeter Results
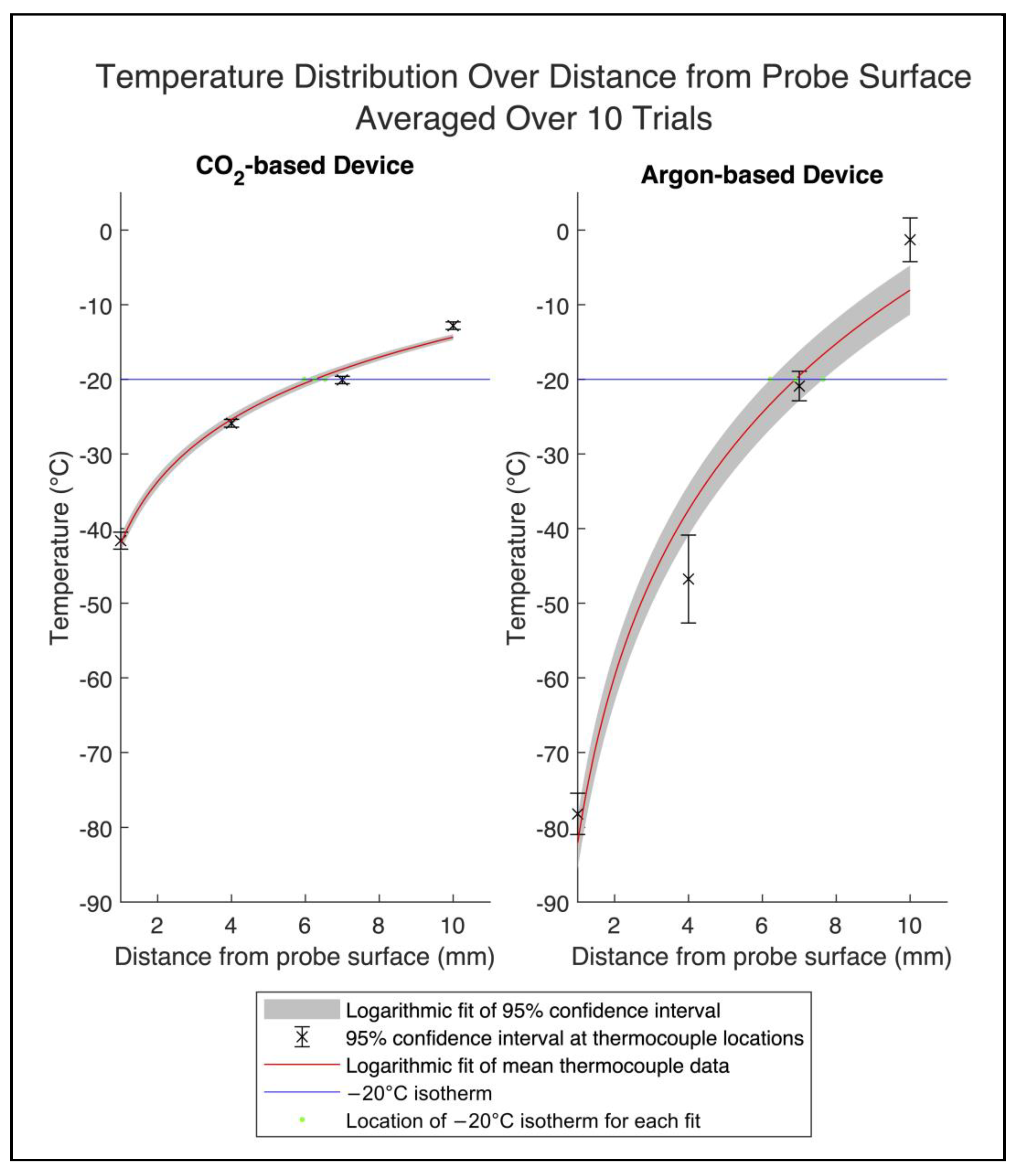
3.2. Temperature Distribution Results
3.3. Histopathology Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Sukhun, S.; Tbaishat, F.; Hammad, N. Breast cancer priorities in limited-resource environments: The price-efficacy dilemma in cancer care. Am. Soc. Clin. Oncol. Educ. Book 2022, 42, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Francies, F.Z.; Hull, R.; Khanyile, R.; Dlamini, Z. Breast Cancer in Low-Middle Income Countries: Abnormality in Splicing and Lack of Targeted Treatment Options. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7269781/ (accessed on 25 December 2023).
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and Future Burden of Breast Cancer: Global Statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Moo, T.-A.; Sanford, R.; Dang, C.; Morrow, M. Overview of Breast Cancer Therapy. PET Clin. 2018, 13, 339–354. [Google Scholar] [CrossRef] [PubMed]
- GlobalSurg Collaborative; National Institute for Health Research Global Health Research Unit on Global Surgery. Global variation in postoperative mortality and complications after cancer surgery: A multicentre, prospective cohort study in 82 countries. Lancet 2021, 397, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Cardone, C.; Arnold, D. The Cancer Treatment Gap in Lower- to Middle-Income Countries. Oncology 2023, 101 (Suppl. S1), 2–4. [Google Scholar] [CrossRef] [PubMed]
- Elmore, S.N.; Polo, A.; Bourque, J.-M.; Pynda, Y.; van der Merwe, D.; Grover, S.; Hopkins, K.; Zubizarreta, E.; Abdel-Wahab, M. Radiotherapy Resources in Africa: An International Atomic Energy Agency Update and Analysis of Projected Needs. Lancet Oncol. 2021, 22, e391–e399. [Google Scholar] [CrossRef]
- Shah, S.C.; Kayamba, V.; Peek, R.M.; Heimburger, D. Cancer Control in Low- and Middle-Income Countries: Is It Time to Consider Screening? J. Glob. Oncol. 2019, 5, 1–8. [Google Scholar] [CrossRef]
- Donkor, A.; Atuwo-Ampoh, V.D.; Yakanu, F.; Torgbenu, E.; Ameyaw, E.K.; Kitson-Mills, D.; Vanderpuye, V.; Kyei, K.A.; Anim-Sampong, S.; Khader, O.; et al. Financial Toxicity of Cancer Care in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Support. Care Cancer 2022, 30, 7159–7190. [Google Scholar] [CrossRef] [PubMed]
- Newman, L.A. Breast cancer screening in low and middle-income countries. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 83, 15–23. [Google Scholar] [CrossRef]
- Ferlic, D.J.; Kotula, F.T.; Amplatz, K. Mammography Apparatus. U.S. Patent 4901335, 13 February 1990. [Google Scholar]
- Souney, S.; Roeder, R. Portable Hand-Carry Satellite Diagnostic Ultrasound System for General and Cardiac Imaging. U.S. Patent US20020040186A1, 12 November 2002. [Google Scholar]
- Tran, T.T.; Hlaing, M.; Krause, M. Point-of-Care Ultrasound: Applications in Low- and Middle-Income Countries. Curr. Anesthesiol. Rep. 2021, 11, 69–75. [Google Scholar] [CrossRef]
- Becker, D.M.; Tafoya, C.A.; Becker, S.L.; Kruger, G.H.; Tafoya, M.J.; Becker, T.K. The Use of Portable Ultrasound Devices in Low- and Middle-income Countries: A Systematic Review of the Literature. Trop. Med. Int. Health 2016, 21, 294–311. [Google Scholar] [CrossRef] [PubMed]
- Bhimani, F.; Zhang, J.; Shah, L.; McEvoy, M.; Gupta, A.; Pastoriza, J.; Shihabi, A.; Feldman, S. Can the clinical utility of ibreastexam, a novel device, aid in optimizing breast cancer diagnosis? A systematic review. JCO Glob. Oncol. 2023, 9, e2300149. [Google Scholar] [CrossRef] [PubMed]
- Mokbel, K.; Kodresko, A.; Ghazal, H.; Mokbel, R.; Trembley, J.; Jouhara, H. The Evolving Role of Cryosurgery in Breast Cancer Management: A Comprehensive Review. Cancers 2023, 15, 4272. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.; Miller, S.; Douglas-Moore, J.; Miller, M. Cryotherapy and Its Applications in the Management of Urologic Malignancies: A Review of Its Use in Prostate and Renal Cancers. Urol. Oncol. Semin. Orig. Investig. 2014, 32, e19–e39. [Google Scholar] [CrossRef] [PubMed]
- Winkle, R.A.; Mead, R.H.; Engel, G.; Kong, M.H.; Patrawala, R.A. Physician-controlled costs: The choice of equipment used for atrial fibrillation ablation. J. Interv. Card. Electrophysiol. 2013, 36, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Bang, H.J.; Littrup, P.J.; Goodrich, D.J.; Currier, B.P.; Aoun, H.D.; Heilbrun, L.K.; Vaishampayan, U.; Adam, B.; Goodman, A.C. Percutaneous cryoablation of metastatic renal cell carcinoma for local tumor control: Feasibility, outcomes, and estimated cost-effectiveness for palliation. J. Vasc. Interv. Radiol. 2012, 23, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Sprenkle, P.C.; Mirabile, G.; Durak, E.; Edelstein, A.; Gupta, M.; Hruby, G.W.; Okhunov, Z.; Landman, J. The Effect of Argon Gas Pressure on Ice Ball Size and Rate of Formation. J. Endourol. 2010, 24, 1503–1507. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.M.; Dawber, R.P. The history of cryosurgery. J. R. Soc. Med. 2001, 94, 196–201. [Google Scholar] [CrossRef]
- Surtees, B.; Young, S.; Hu, Y.; Wang, G.; McChesney, E.; Kuroki, G.; Acree, P.; Thomas, S.; Blair, T.; Rastogi, S.; et al. Validation of a low-cost, carbon dioxide-based cryoablation system for percutaneous tumor ablation. PLoS ONE 2019, 14, e0207107. [Google Scholar] [CrossRef]
- Hinshaw, J.L.; Lee, F.T.; Laeseke, P.F.; Sampson, L.A.; Brace, C. Temperature isotherms during pulmonary cryoablation and their correlation with the zone of ablation. J. Vasc. Interv. Radiol. 2010, 21, 1424–1428. [Google Scholar] [CrossRef]
- Snyder, K.K.; Van Buskirk, R.G.; Baust, J.G.; Baust, J.M. Breast cancer cryoablation: Assessment of the impact of fundamental procedural variables in an in vitro human breast cancer model. Breast Cancer Basic Clin. Res. 2020, 14, 117822342097236. [Google Scholar] [CrossRef]
- Littrup, P.J.; Freeman-Gibb, L.; Andea, A.; White, M.; Amerikia, K.C.; Bouwman, D.; Harb, T.; Sakr, W. Cryotherapy for breast fibroadenomas. Radiology 2005, 234, 63–72. [Google Scholar] [CrossRef]
- Boston Scientific Corporation. Classic Needle Sell Sheet. Boston Scientific Corporation: Marlborough, MA, n.d. Available online: https://www.bostonscientific.com/content/dam/bostonscientific/pi/portfolio-group/cryoablation/visualice/Classic_Needle_Sell_Sheet.pdf (accessed on 26 February 2024).
- Savitzky, A.; Golay, M.J. Smoothing and differentiation of data by simplified least squares procedures. Anal. Chem. 1964, 36, 1627–1639. [Google Scholar] [CrossRef]
- Hossain, S.; Mohammadi, F. One-dimensional Steady-state Analysis of Bioheat Transfer Equation: Tumour Parameters Assessment for Medical Diagnosis Application. In Proceedings of the IMETI 2013-6th International Multi-Conference on Engineering and Technological Innovation, Orlando, FL, USA, 9–12 July 2013; Proceedings 2013. pp. 26–30. [Google Scholar]
- Parsons, K.; Reichanadter, T.; Vicksman, A.; Segur, H. Explicit solution for cylindrical heat conduction. Am. J. Undergrad. Res. 2016, 13, 109. [Google Scholar] [CrossRef]
- Pollheimer, M.J.; Kornprat, P.; Lindtner, R.A.; Harbaum, L.; Schlemmer, A.; Rehak, P.; Langner, C. Tumor necrosis is a new promising prognostic factor in colorectal cancer. Hum. Pathol. 2010, 41, 1749–1757. [Google Scholar] [CrossRef]
- Theodorescu, D. Cancer cryotherapy: Evolution and biology. Rev. Urol. 2004, 6 (Suppl. S4), S9–S19. [Google Scholar]
- Mazur, P. Physical-chemical factors underlying cell injury in cryosurgical freezing. In Cryosurgery; Rand, R., Rinfret, A., von Leden, H., Eds.; Charles C. Thomas: Springfield, IL, USA, 1968; pp. 32–51. [Google Scholar]
- Salmon, K.; Nellis, G.; Pfotenhauer, J. Experimental characterization of cryogenic contact resistance. Cryogenics 2022, 128, 103587. [Google Scholar] [CrossRef]
- Etheridge, M.L.; Choi, J.; Ramadhyani, S.; Bischof, J.C. Methods for characterizing convective cryoprobe heat transfer in Ultrasound Gel Phantoms. J. Biomech. Eng. 2013, 135, 021002. [Google Scholar] [CrossRef]
- Understanding the Characteristics of Pressure Regulators. Available online: https://fluidpowerjournal.com/understanding-the-characteristics-of-pressure-regulators/ (accessed on 28 December 2023).
- Erinjeri, J.P.; Clark, T.W.I. Cryoablation: Mechanism of action and Devices. J. Vasc. Interv. Radiol. 2010, 21 (Suppl. S8), S187–S191. [Google Scholar] [CrossRef] [PubMed]
- Kwak, K.; Yu, B.; Lewandowski, R.J.; Kim, D.-H. Recent progress in cryoablation cancer therapy and nanoparticles mediated cryoablation. Theranostics 2022, 12, 2175–2204. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.; Sundaram, C.P.; Bahler, C.D.; Eble, J.N.; Grignon, D.J.; Monn, M.F.; Simper, N.B.; Cheng, L. Correcting the shrinkage effects of formalin fixation and tissue processing for renal tumors: Toward standardization of pathological reporting of Tumor Size. J. Cancer 2015, 6, 759–766. [Google Scholar] [CrossRef]
- Upchurch, D.A.; Klocke, E.E.; Henningson, J.N. Amount of skin shrinkage affecting tumor versus grossly normal marginal skin of dogs for cutaneous mast cell tumors excised with curative intent. Am. J. Vet. Res. 2018, 79, 779–786. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CO2 Device | Argon Device | |
|---|---|---|
| Cooling Power | 116.9 W | 27.7 W |
| Effective Surface Area | 581.6 mm2 | 87.4 mm2 |
| Normalized Cooling Power | 0.20 W/mm2 | 0.32 W/mm2 |
| Thermocouple Location | CO2 (°C) | Argon (°C) |
|---|---|---|
| 1 mm | −41.62 ± 1.31 | −78.19 ± 3.19 |
| 4 mm | −25.89 ± 0.60 | −46.76 ± 6.79 |
| 7 mm | −20.09 ± 0.57 | −20.90 ± 2.28 |
| 10 mm | −12.81 ± 0.58 | −1.30 ± 3.376 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.; Gordon, N.; Ogg, K.; Kraitchman, D.L.; Durr, N.J.; Surtees, B. Thermal Characterization and Preclinical Feasibility Verification of an Accessible, Carbon Dioxide-Based Cryotherapy System. Bioengineering 2024, 11, 391. https://doi.org/10.3390/bioengineering11040391
Hu Y, Gordon N, Ogg K, Kraitchman DL, Durr NJ, Surtees B. Thermal Characterization and Preclinical Feasibility Verification of an Accessible, Carbon Dioxide-Based Cryotherapy System. Bioengineering. 2024; 11(4):391. https://doi.org/10.3390/bioengineering11040391
Chicago/Turabian StyleHu, Yixin, Naomi Gordon, Katherine Ogg, Dara L. Kraitchman, Nicholas J. Durr, and Bailey Surtees. 2024. "Thermal Characterization and Preclinical Feasibility Verification of an Accessible, Carbon Dioxide-Based Cryotherapy System" Bioengineering 11, no. 4: 391. https://doi.org/10.3390/bioengineering11040391