Figure 1.
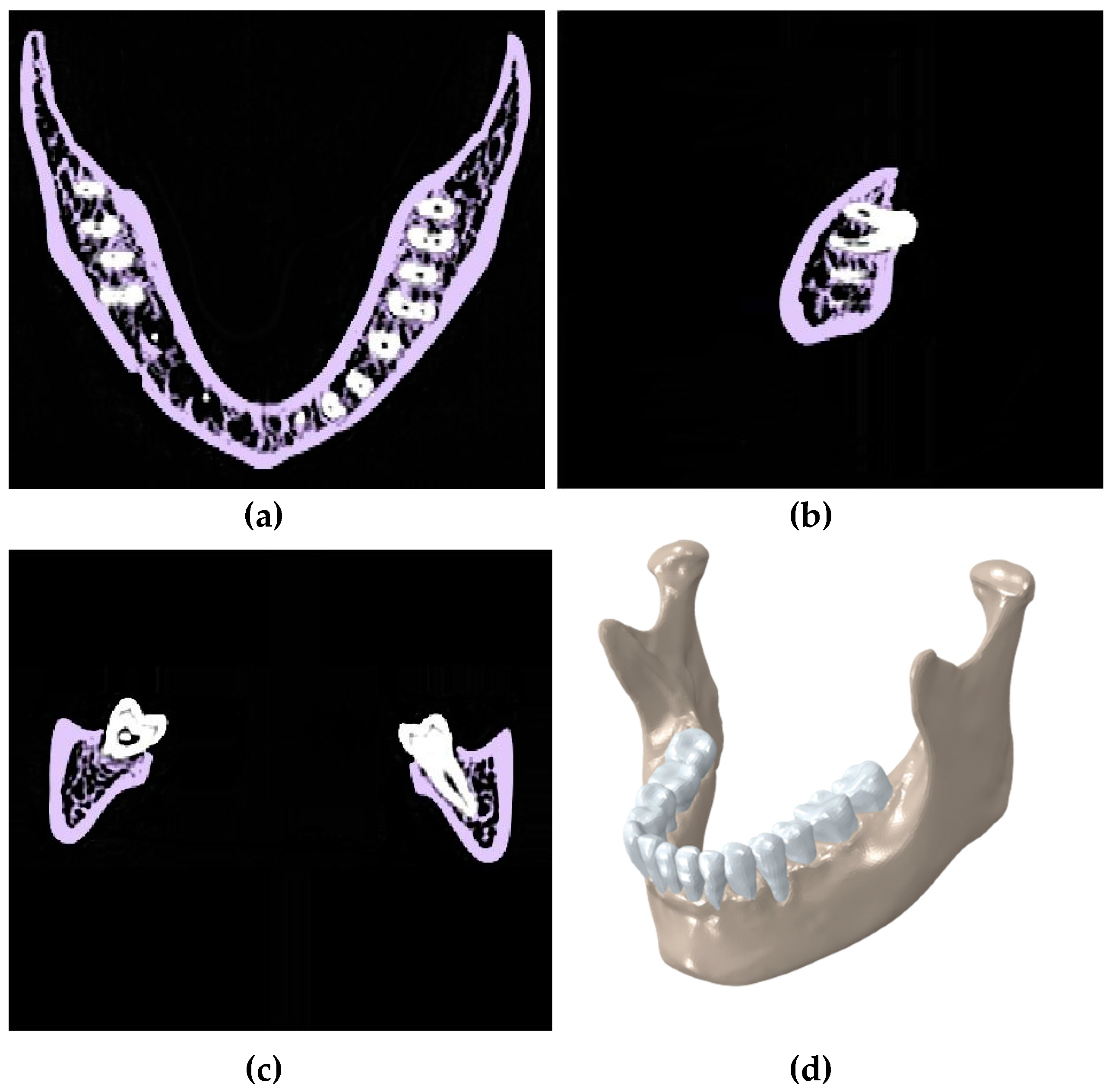
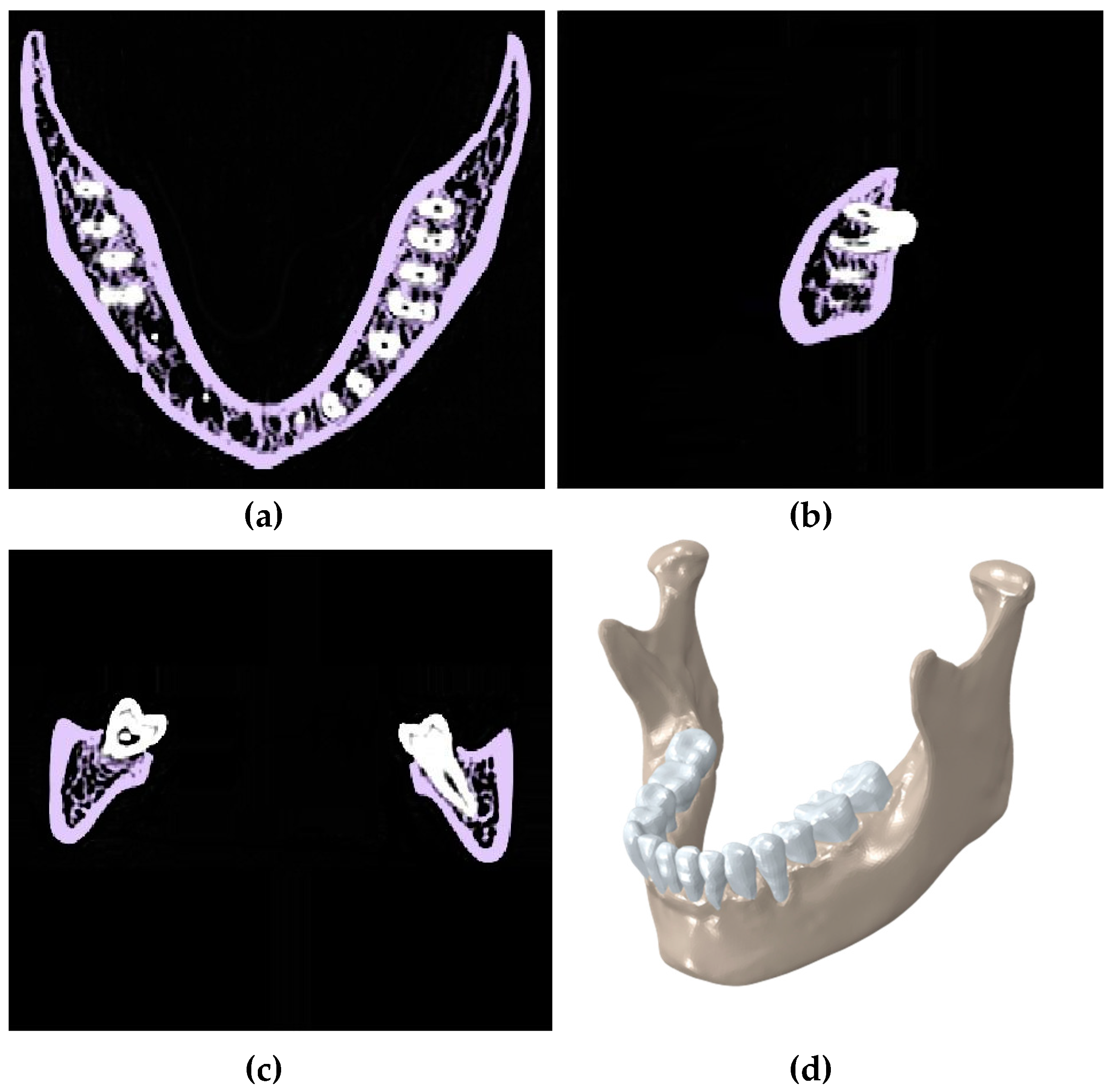
Segmentation of CT scan of a healthy mandible showing the (a) transverse plane; (b) sagittal plane; and (c) coronal plane; (d) a 3D model in Mimics.
Figure 1.
Segmentation of CT scan of a healthy mandible showing the (a) transverse plane; (b) sagittal plane; and (c) coronal plane; (d) a 3D model in Mimics.
Figure 2.
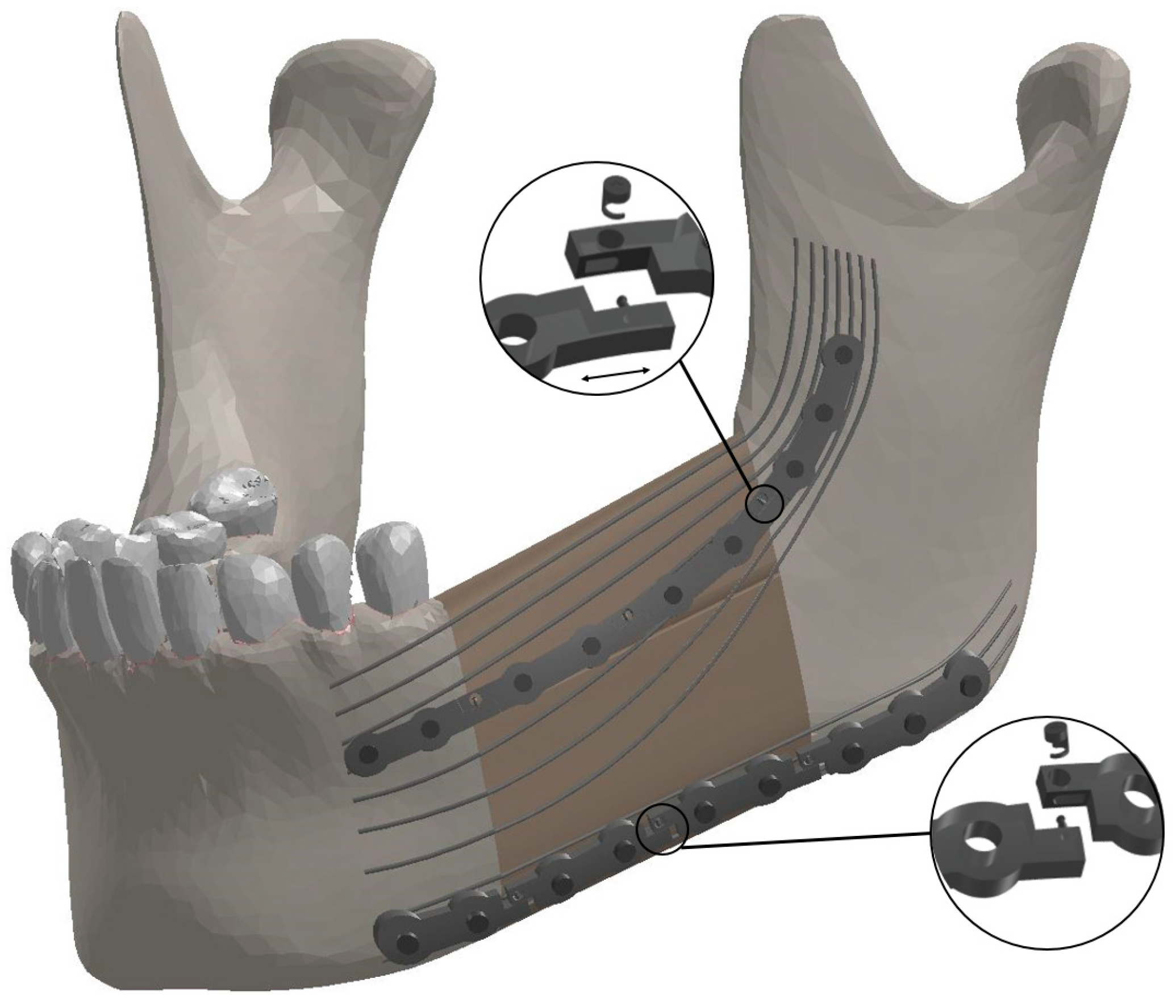
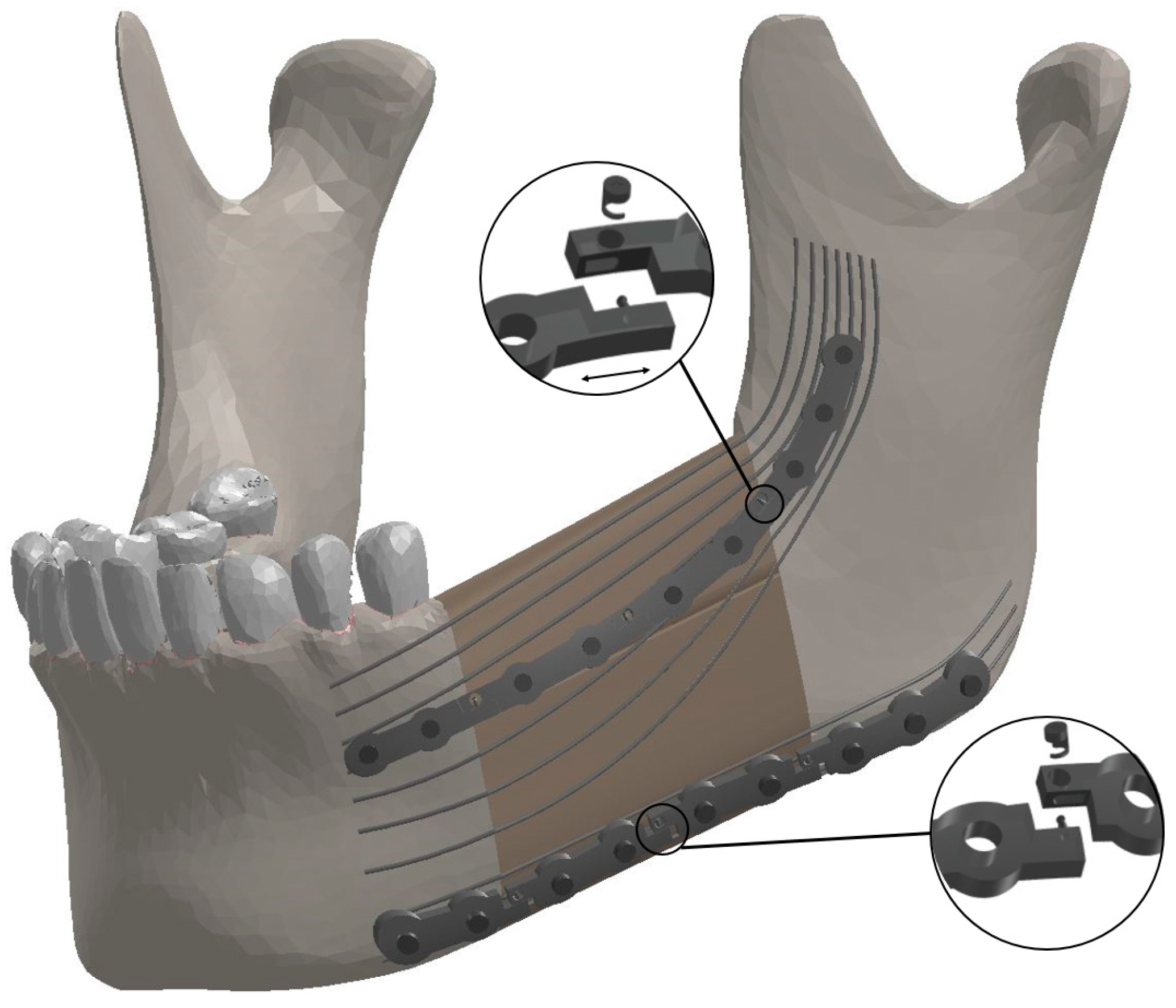
The components of the Bone Bandaid mandibular reconstruction using a releasable Ti-6Al-4V fixation device and underlying Bone Bandaid NiTi wires. The NiTi wires are affixed to the bone by tiny barbs that are not seen. Release is accomplished during a minimally invasive outpatient procedure using a sterile release microsurgical device. There are in total six release points. Since the upper fixation is under tensile loading, the mini-plates will move apart in released state, while the inferior ones get closer since they are under compressive loading.
Figure 2.
The components of the Bone Bandaid mandibular reconstruction using a releasable Ti-6Al-4V fixation device and underlying Bone Bandaid NiTi wires. The NiTi wires are affixed to the bone by tiny barbs that are not seen. Release is accomplished during a minimally invasive outpatient procedure using a sterile release microsurgical device. There are in total six release points. Since the upper fixation is under tensile loading, the mini-plates will move apart in released state, while the inferior ones get closer since they are under compressive loading.
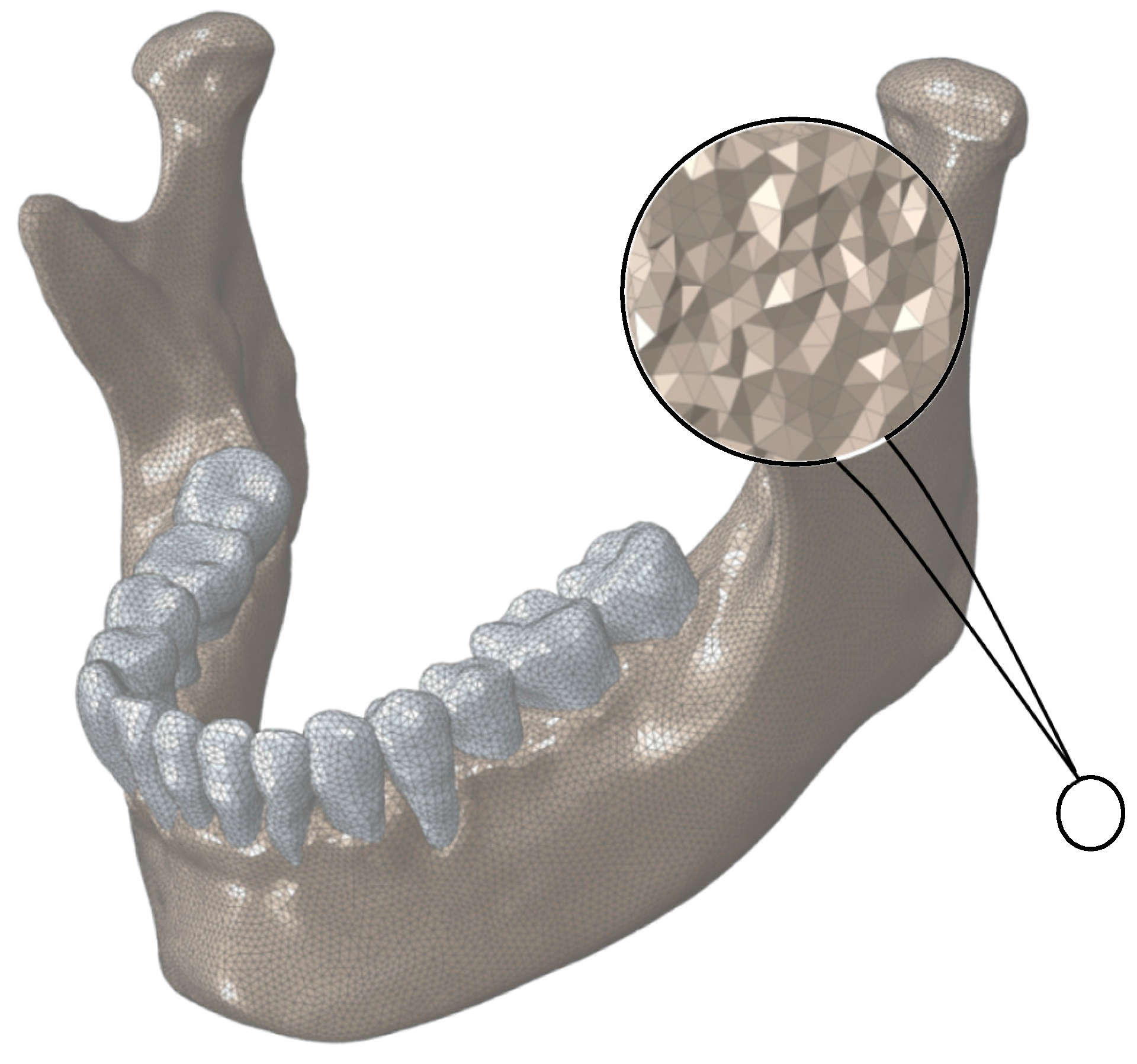
Figure 3.
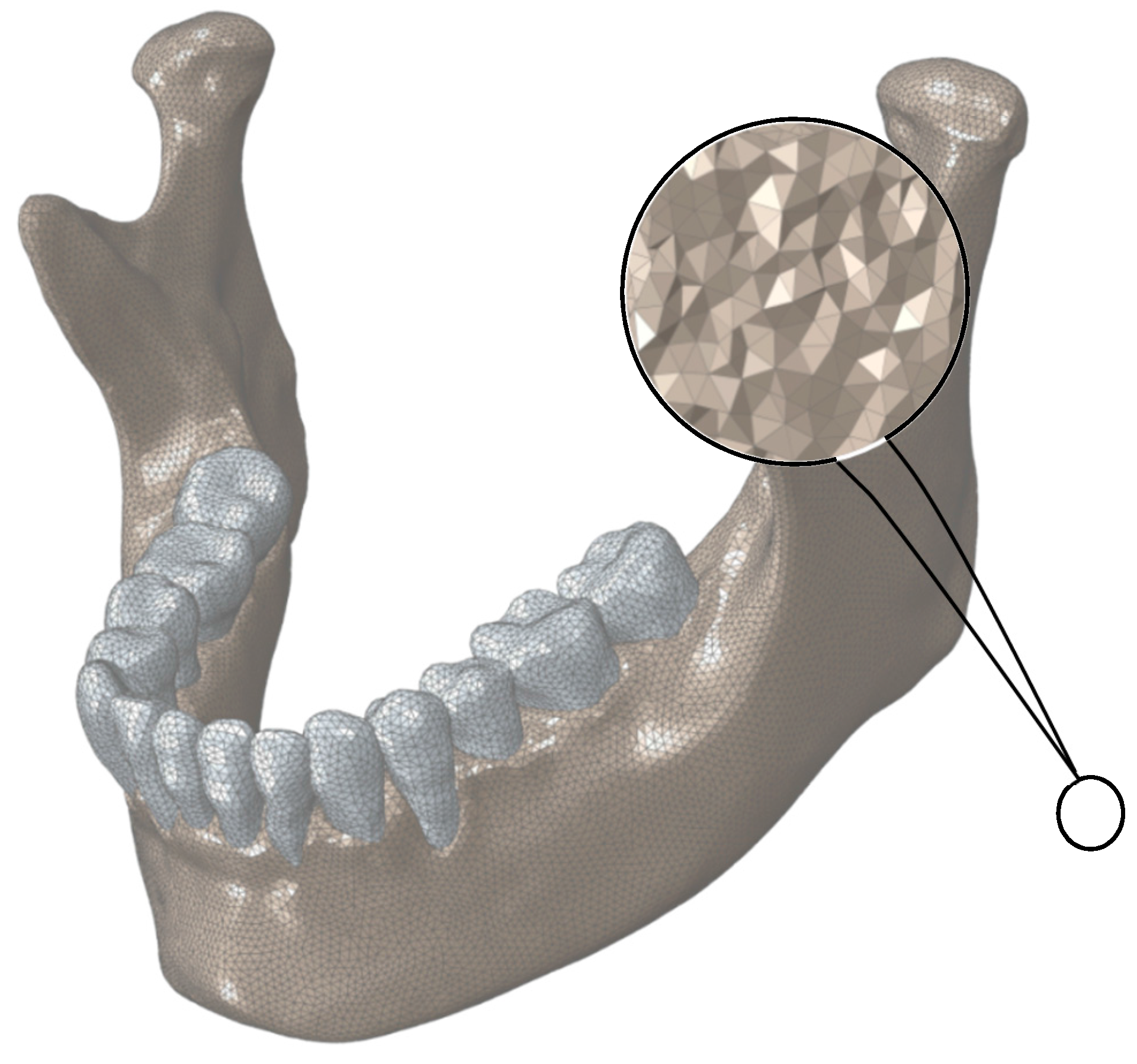
Finite Element mesh for normal mandible. The assigned mesh is 10-node tetrahedral elements (C3D10).
Figure 3.
Finite Element mesh for normal mandible. The assigned mesh is 10-node tetrahedral elements (C3D10).
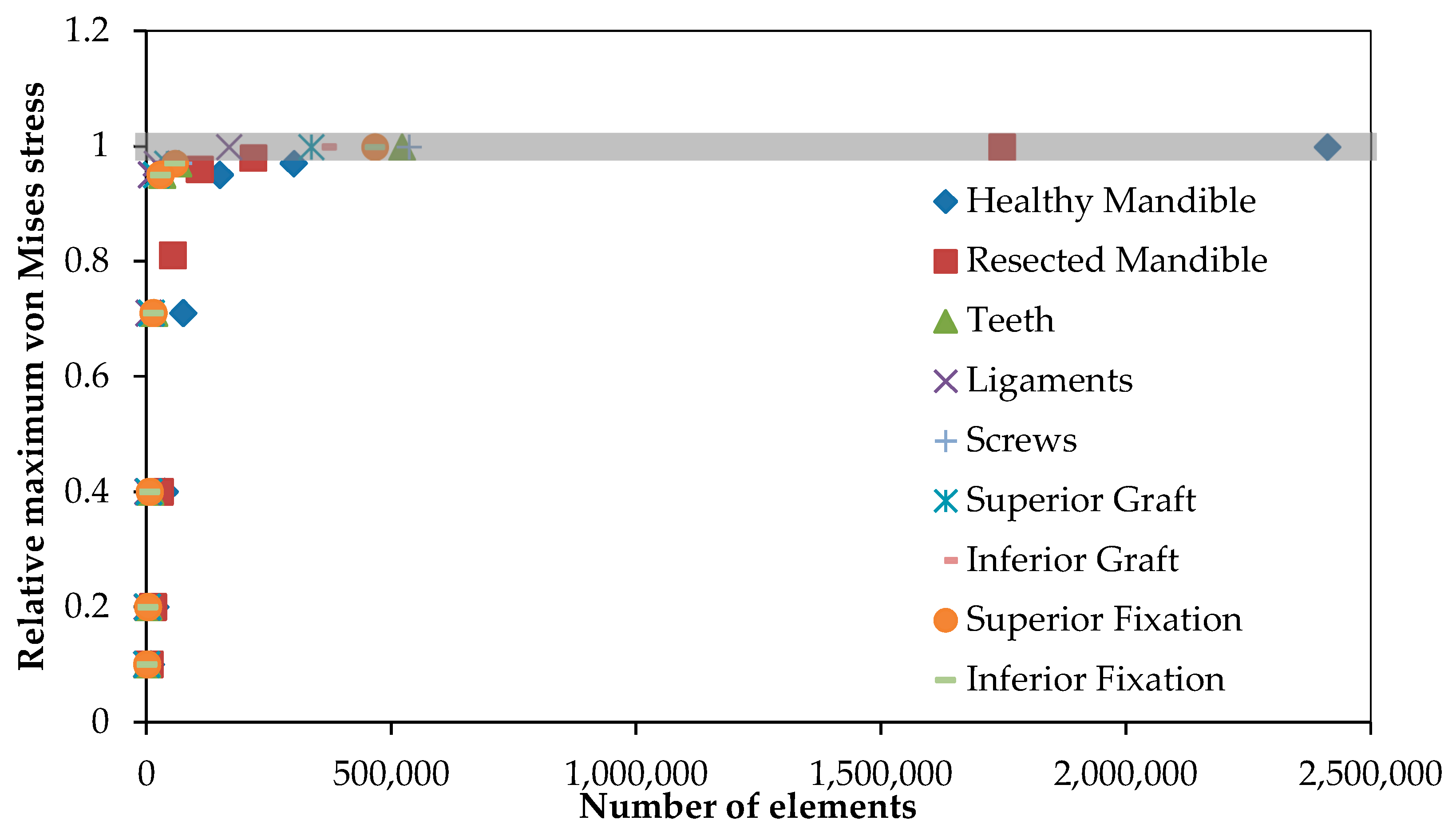
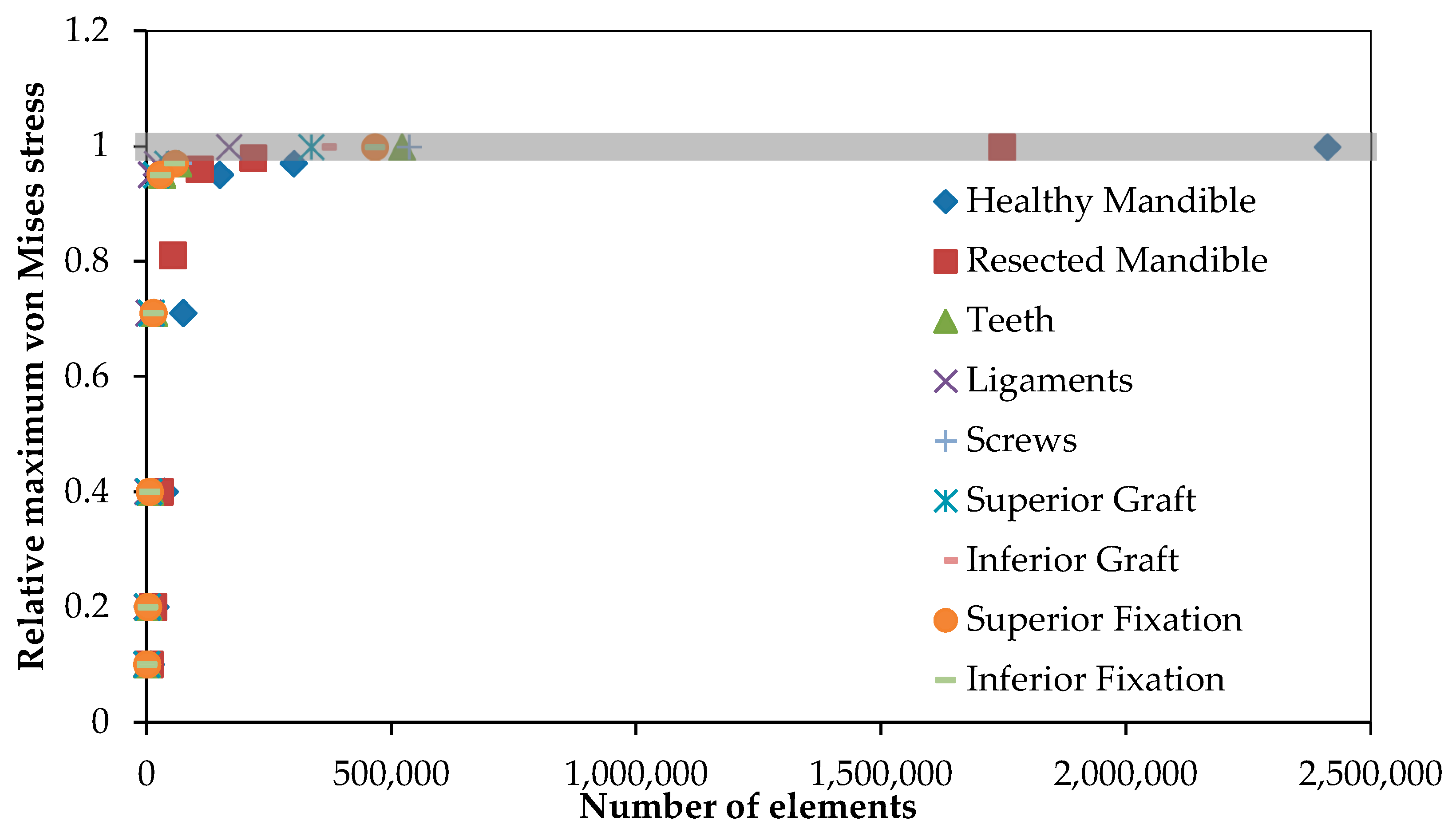
Figure 4.
The mesh convergence study was done to define the optimized number of elements for each component. The vertical axis shows the maximum von Mises stress on each component relative to the maximum von Mises stress on the same component with the highest number of elements.
Figure 4.
The mesh convergence study was done to define the optimized number of elements for each component. The vertical axis shows the maximum von Mises stress on each component relative to the maximum von Mises stress on the same component with the highest number of elements.
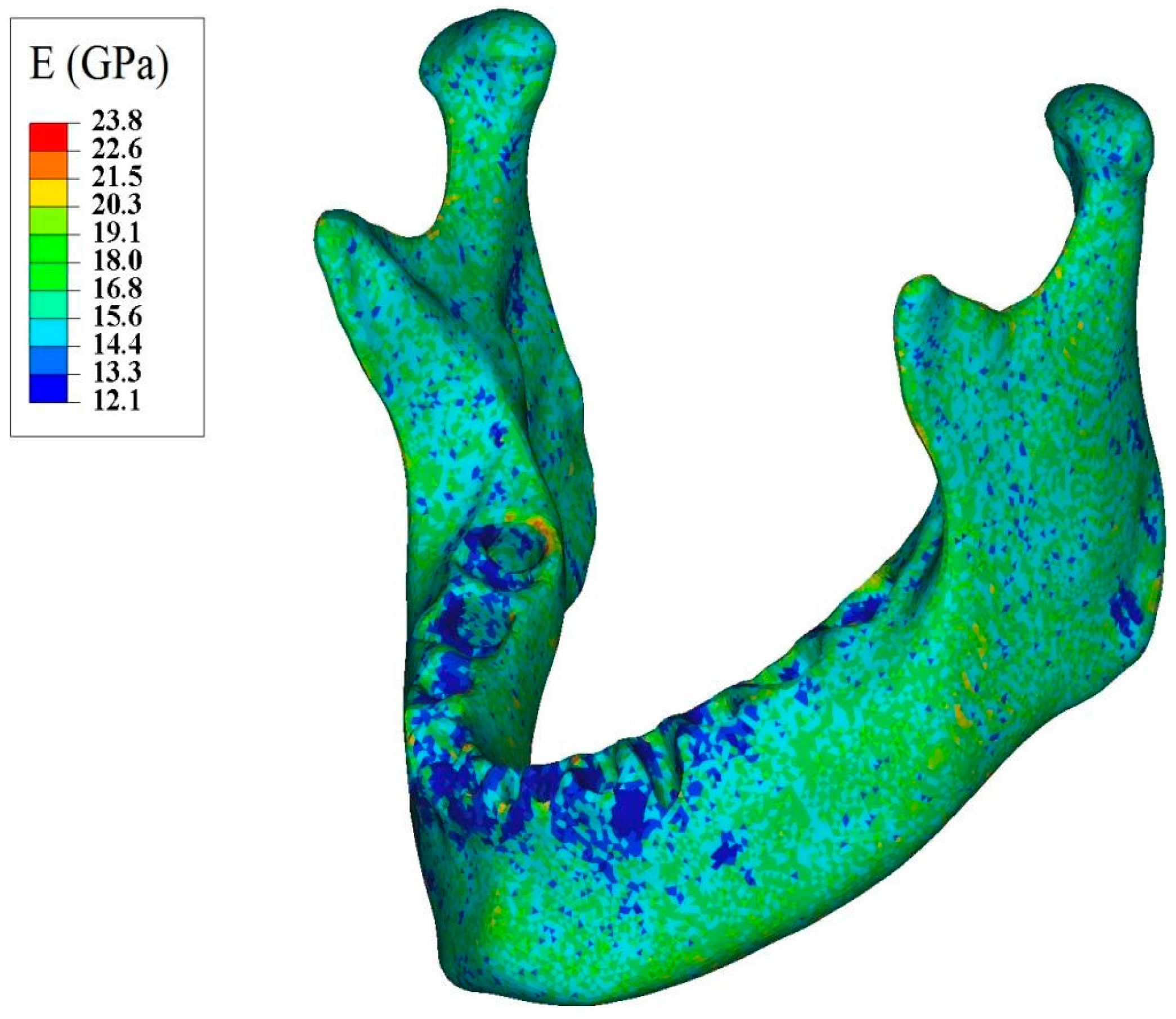
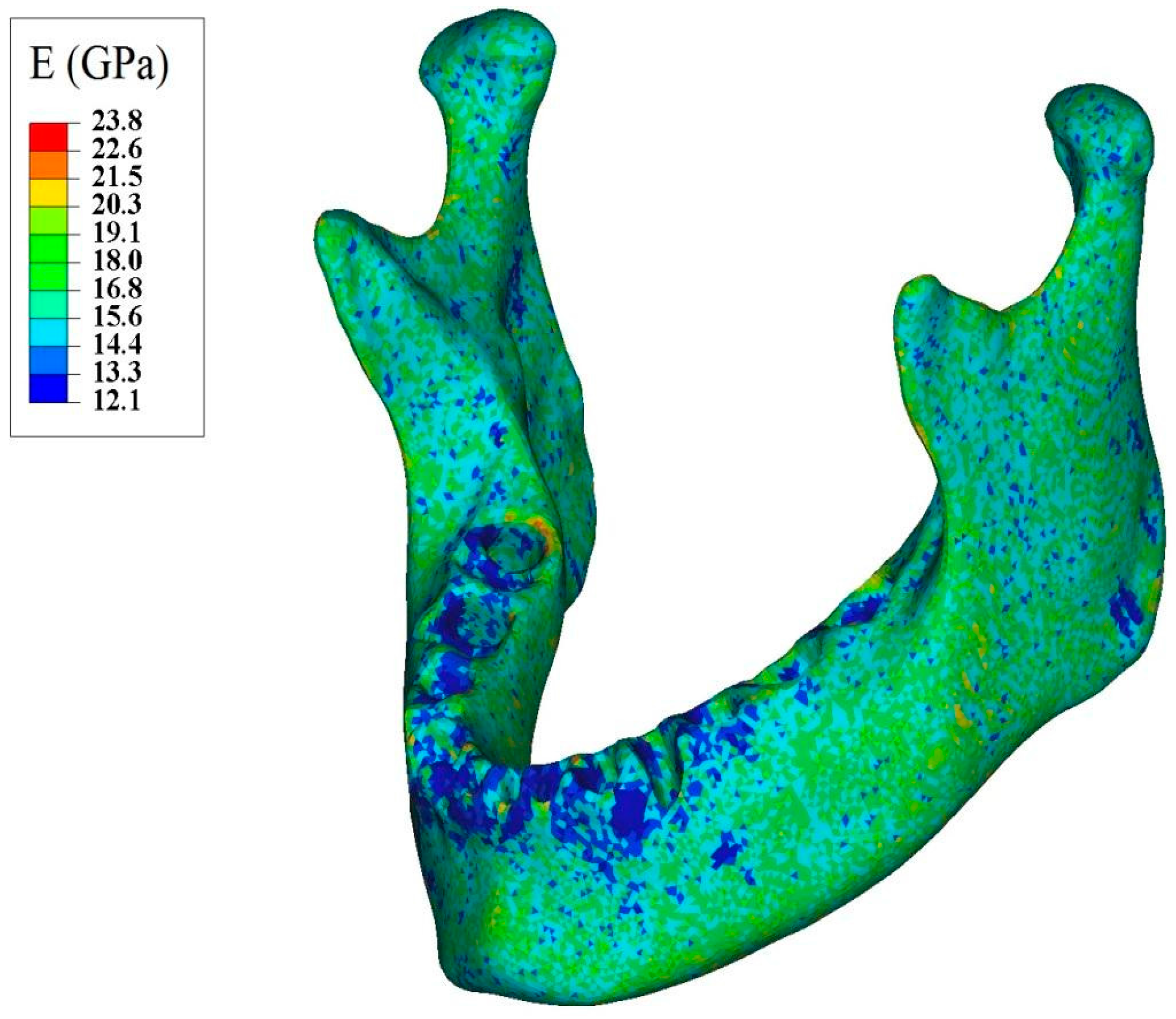
Figure 5.
Apparent modulus of elasticity distribution throughout normal mandible assigned based on the ash density.
Figure 5.
Apparent modulus of elasticity distribution throughout normal mandible assigned based on the ash density.
Figure 6.
(A) 3D structures of major masticatory muscles; (B) Each muscle is simulated by three truss elements, considering the origin and insertion points taken from the 3D structures of muscles. RT = Right temporalis, LT = Left temporalis, RMP = Right medial pterygoid, LMP = Left medial pterygoid, RM = Right masseter, and LM = Left masseter.
Figure 6.
(A) 3D structures of major masticatory muscles; (B) Each muscle is simulated by three truss elements, considering the origin and insertion points taken from the 3D structures of muscles. RT = Right temporalis, LT = Left temporalis, RMP = Right medial pterygoid, LMP = Left medial pterygoid, RM = Right masseter, and LM = Left masseter.
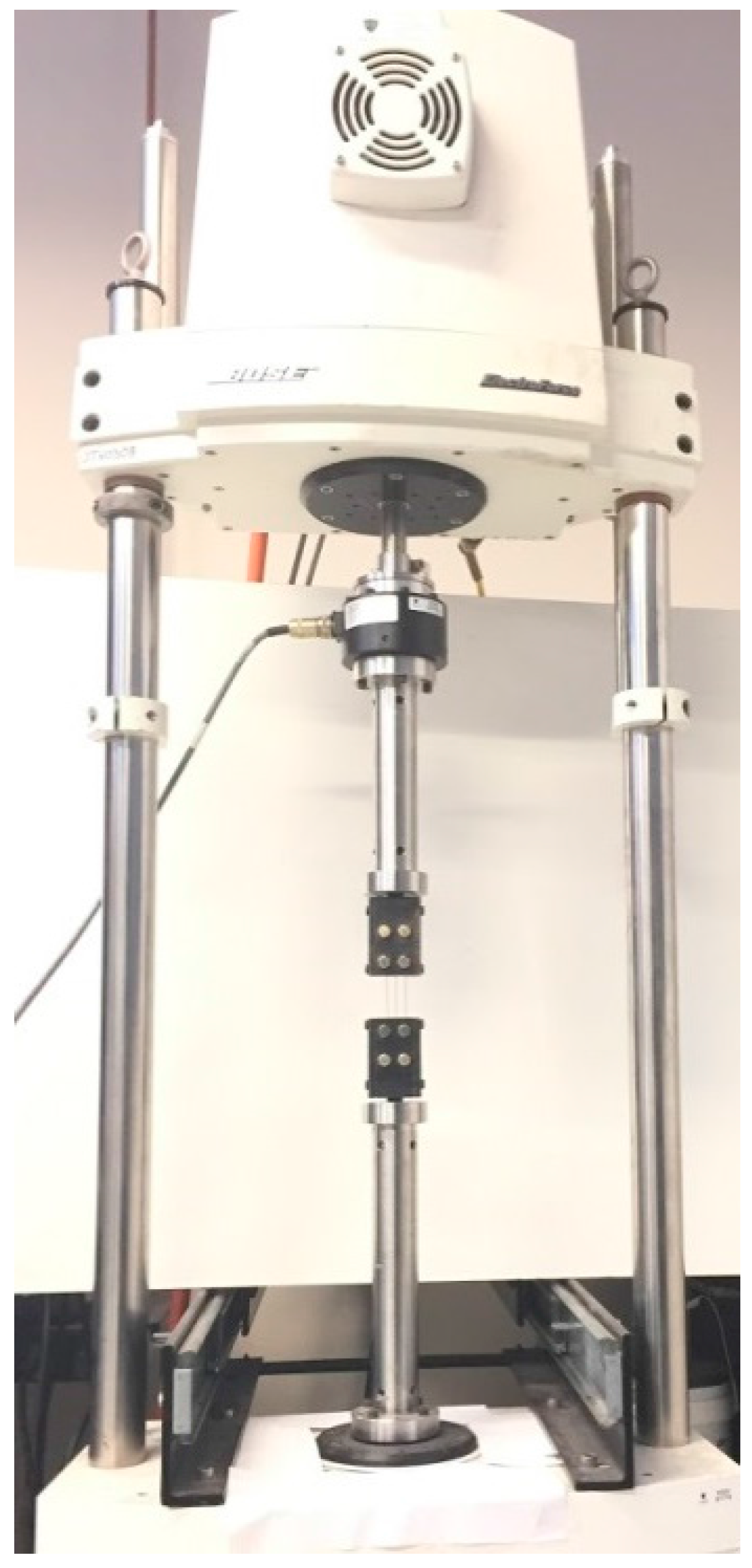
Figure 7.
The experimental setup for tensile test on a Bone Bandaid NiTi wire.
Figure 7.
The experimental setup for tensile test on a Bone Bandaid NiTi wire.
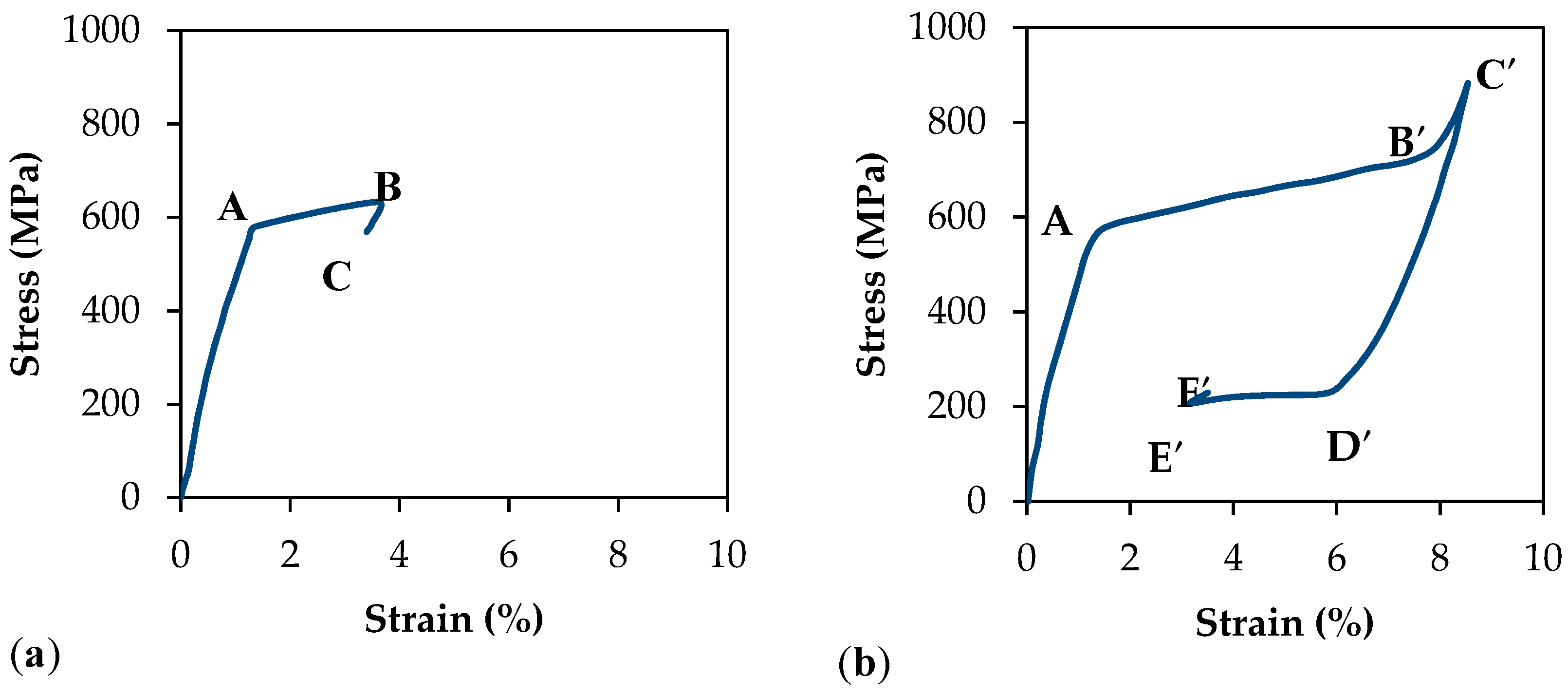
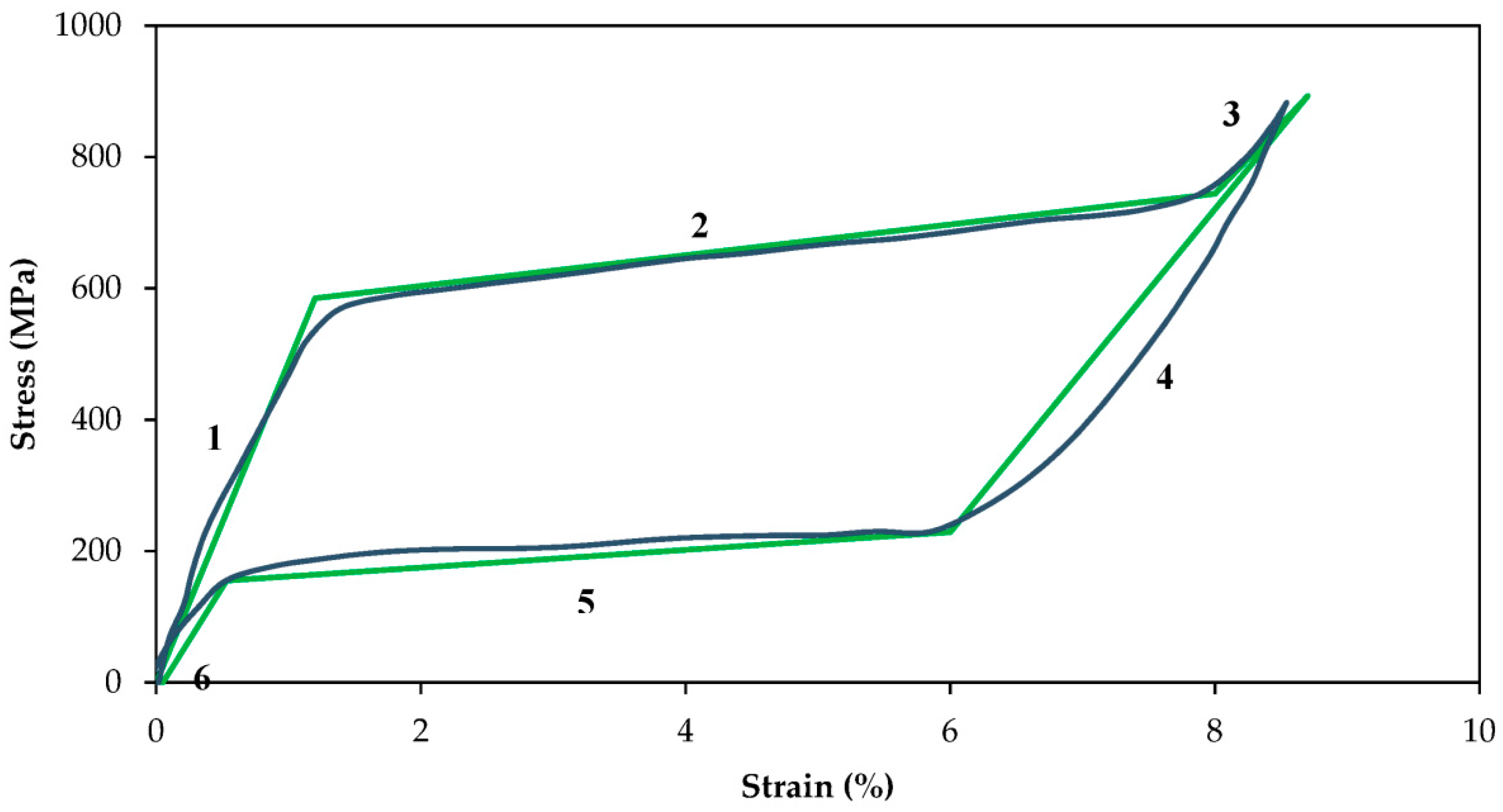
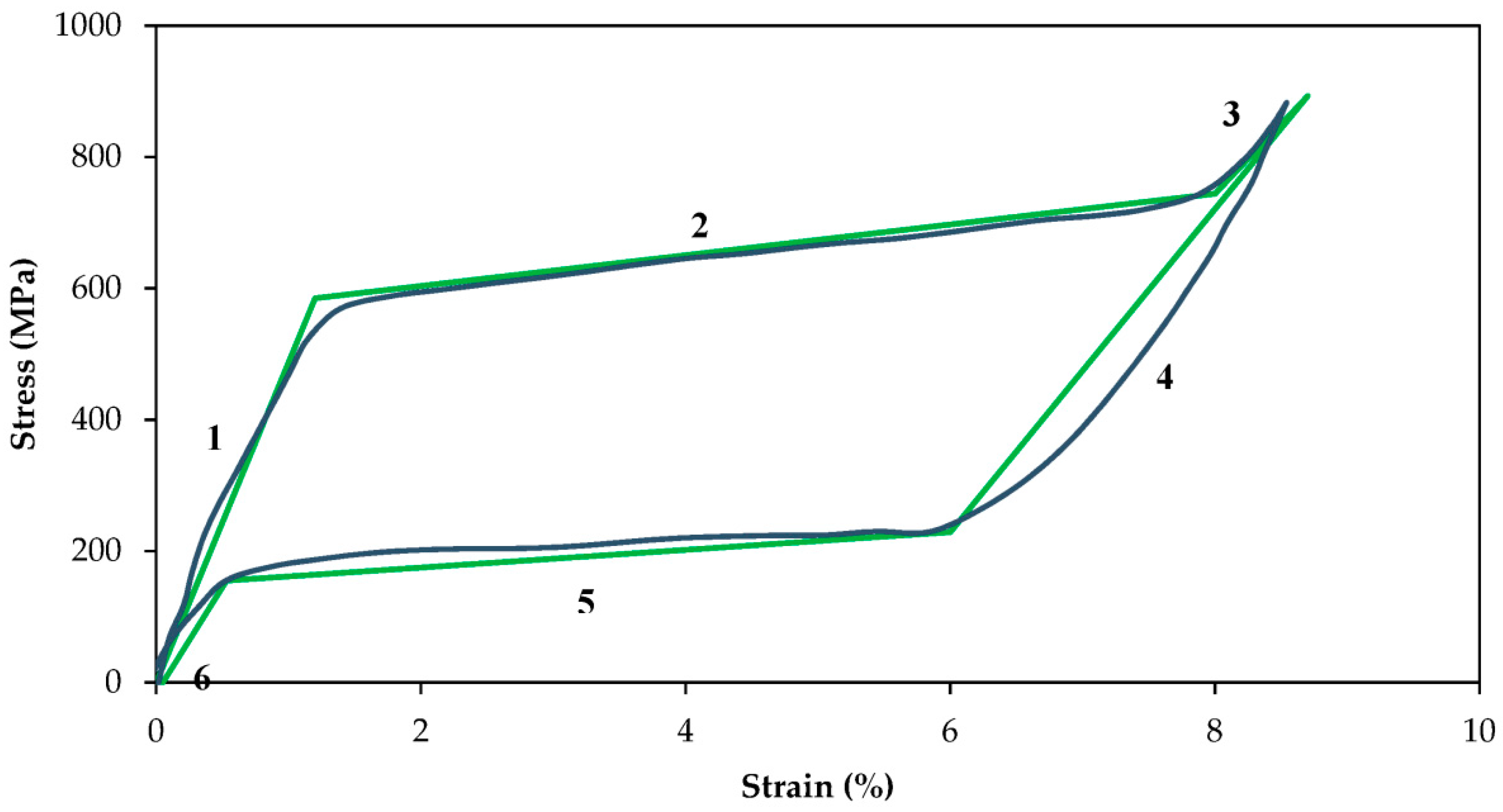
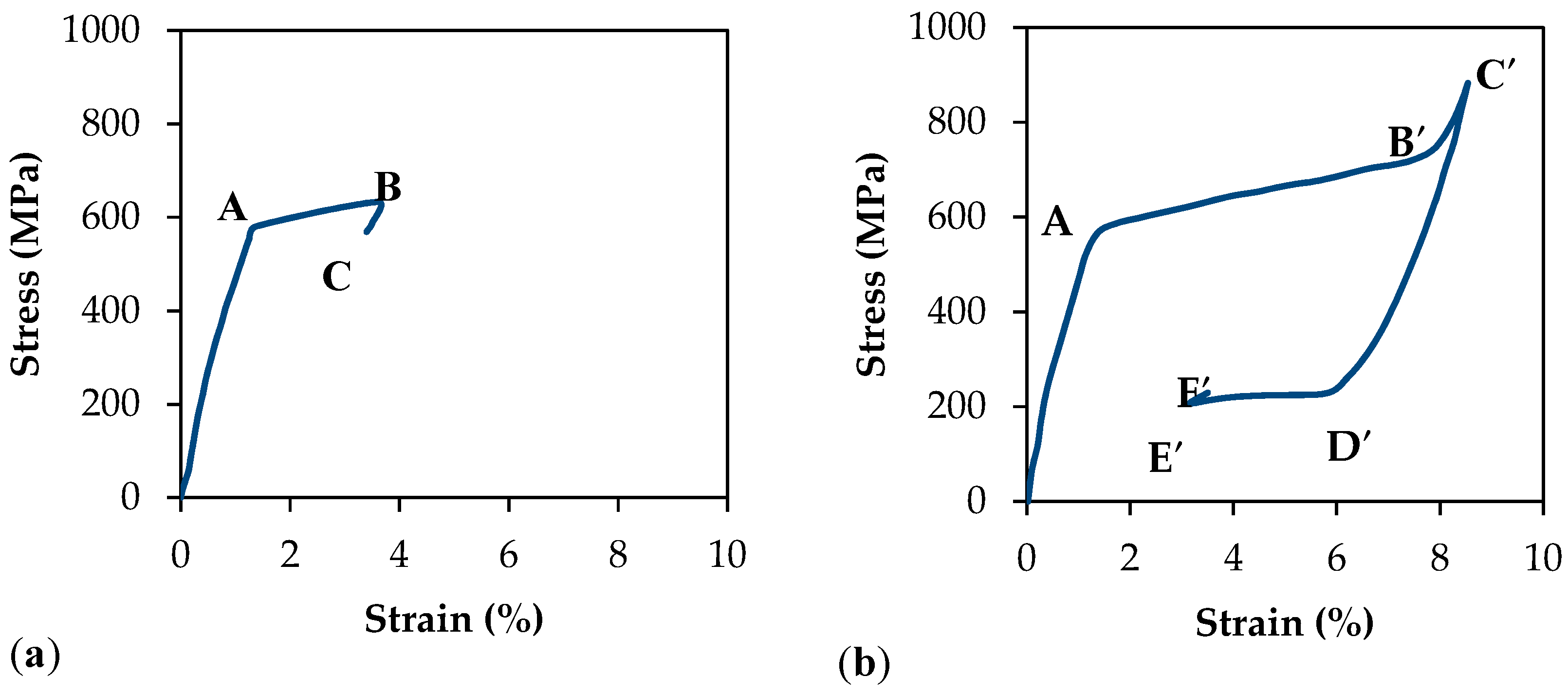
Figure 8.
Stress-strain plots of superelastic NiTi wires and the validation of the UMAT.
Figure 8.
Stress-strain plots of superelastic NiTi wires and the validation of the UMAT.
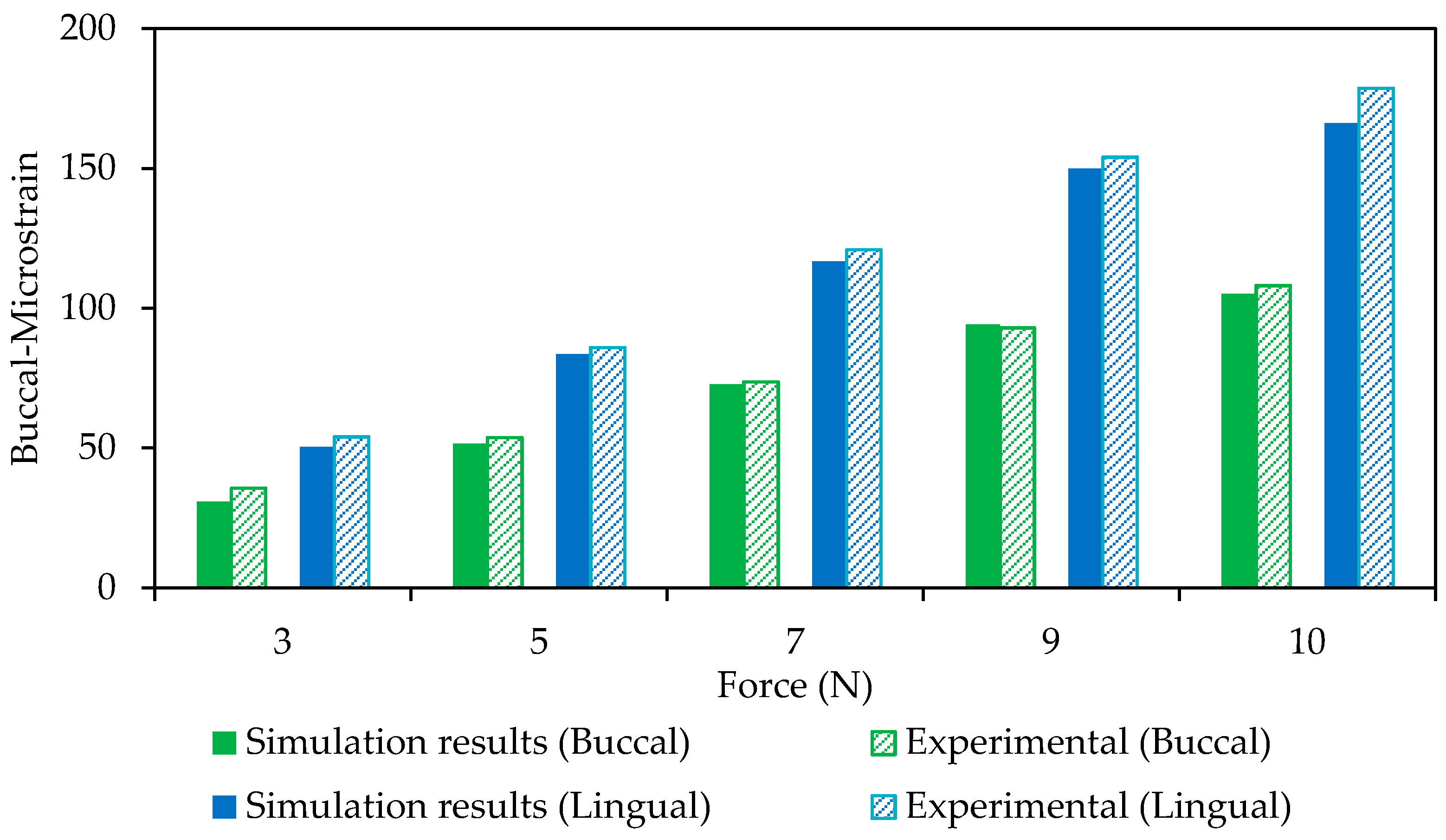
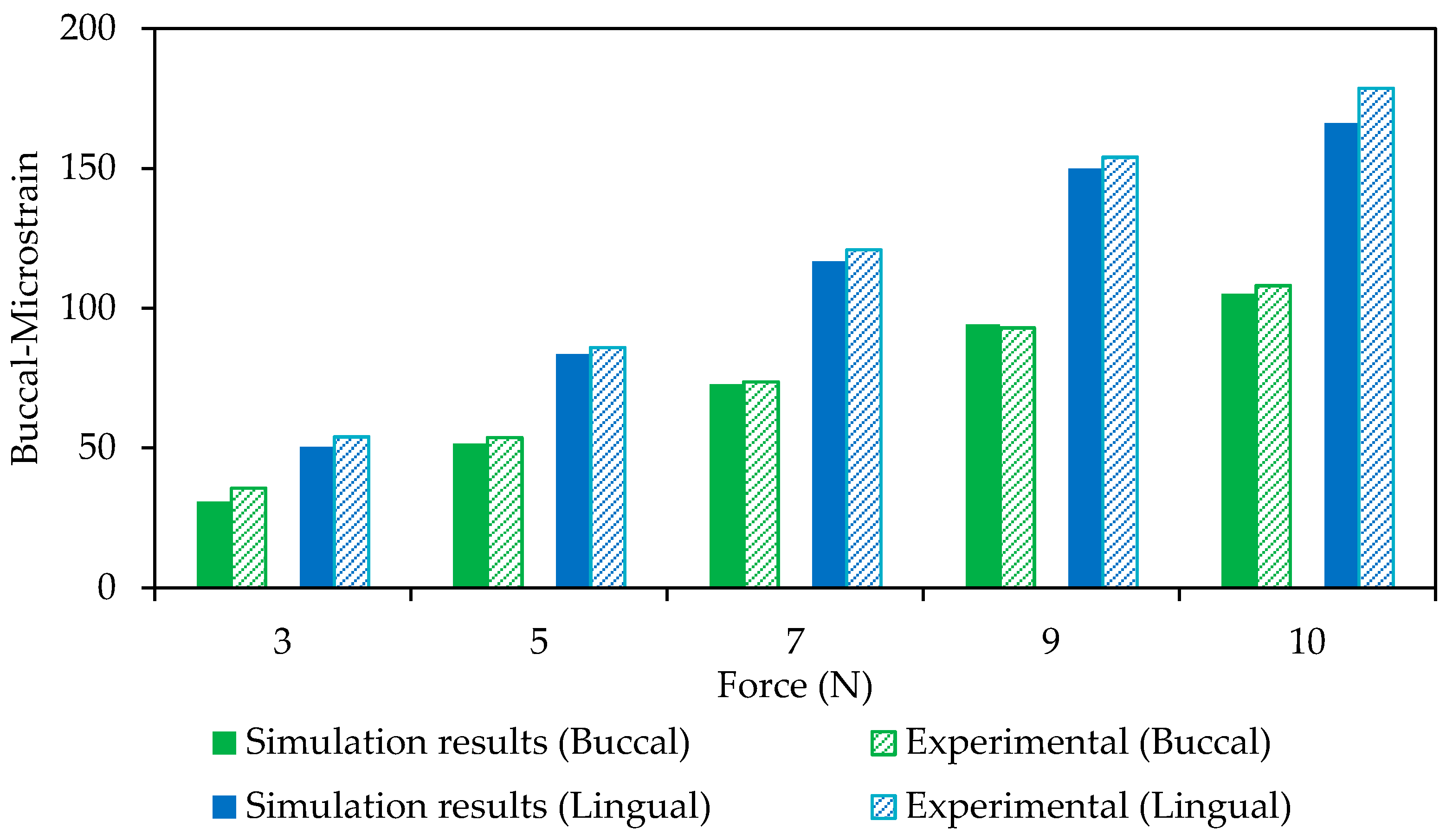
Figure 9.
A comparison between FE model and experimental data on the buccal and lingual regions (Model Validation).
Figure 9.
A comparison between FE model and experimental data on the buccal and lingual regions (Model Validation).
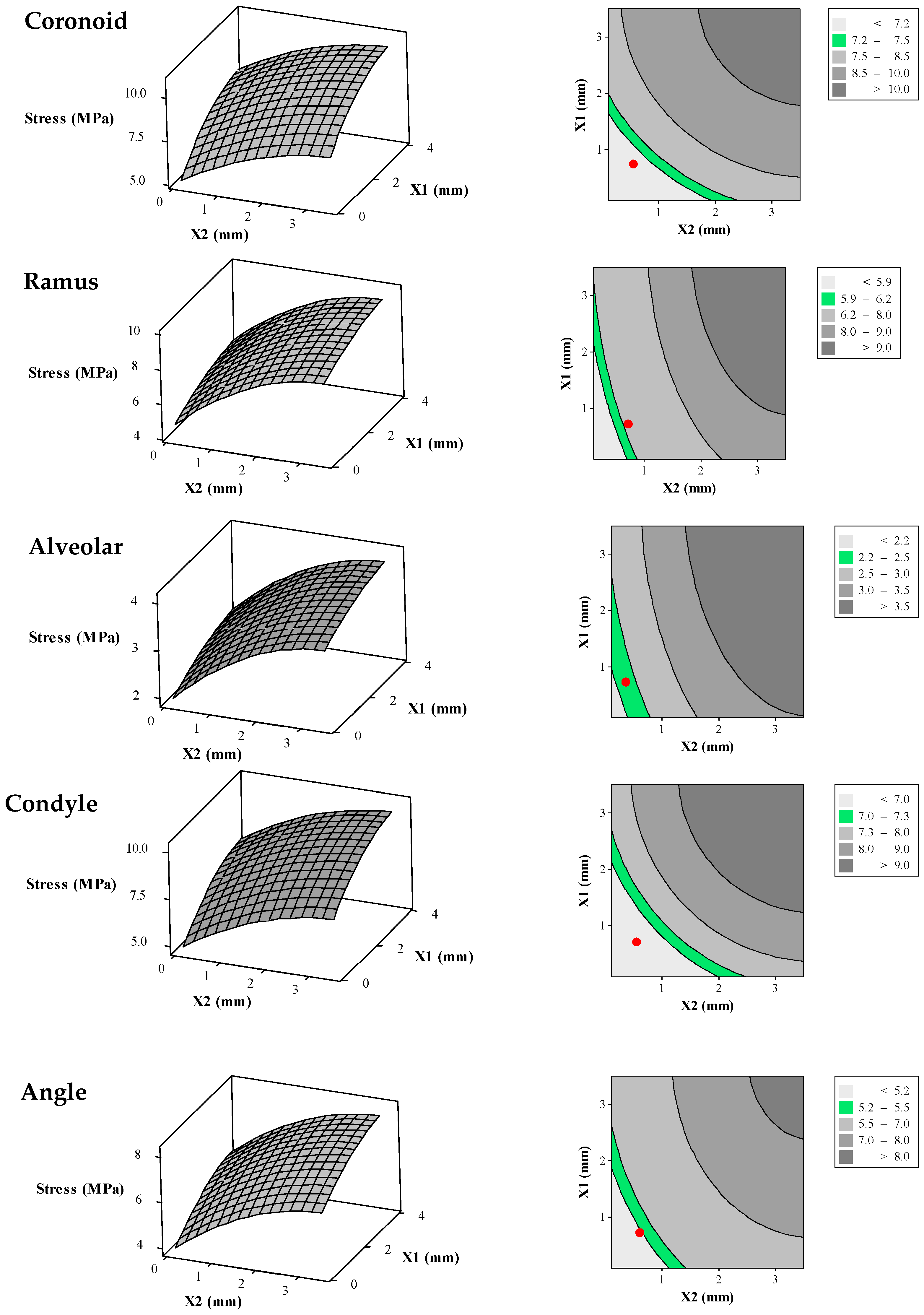
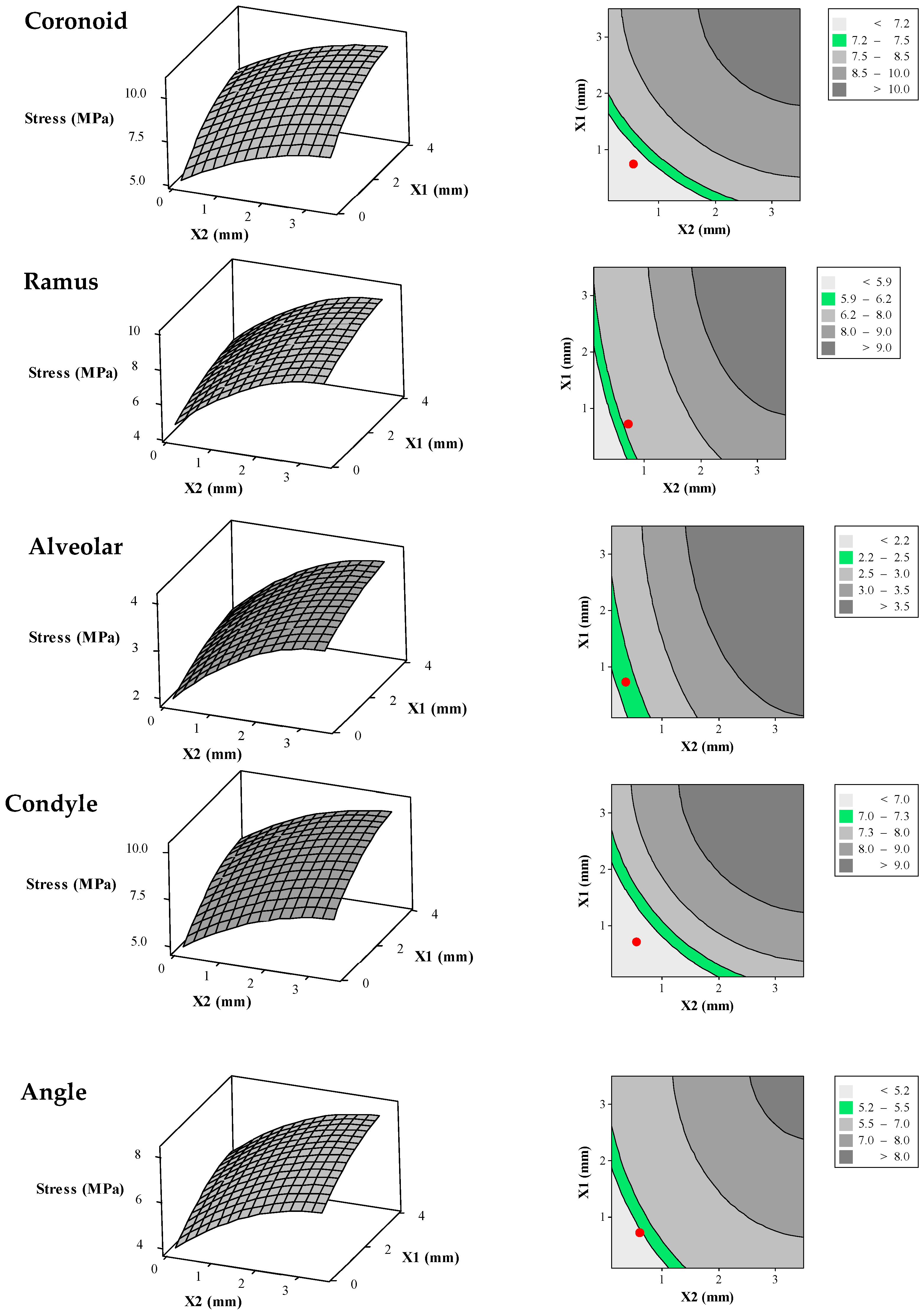
Figure 10.
Surface plots (left) and their corresponding contour plots (right) representing average von Mises stress in the different zones of the reconstructed mandible (i.e., alveolar, symphysis, body, angle, ramus, coronoid, and condyle) as a function of the diameters of superior and inferior wires of the Bone Bandaid apparatus. In the 2D contour plots (right), the desired ranges for the average von Mises stresses are presented as green areas. The red circles are representative for the average von Mises stresses resulting from the combination of optimized X1 = 1 mm and X2 = 0.65 mm.
Figure 10.
Surface plots (left) and their corresponding contour plots (right) representing average von Mises stress in the different zones of the reconstructed mandible (i.e., alveolar, symphysis, body, angle, ramus, coronoid, and condyle) as a function of the diameters of superior and inferior wires of the Bone Bandaid apparatus. In the 2D contour plots (right), the desired ranges for the average von Mises stresses are presented as green areas. The red circles are representative for the average von Mises stresses resulting from the combination of optimized X1 = 1 mm and X2 = 0.65 mm.
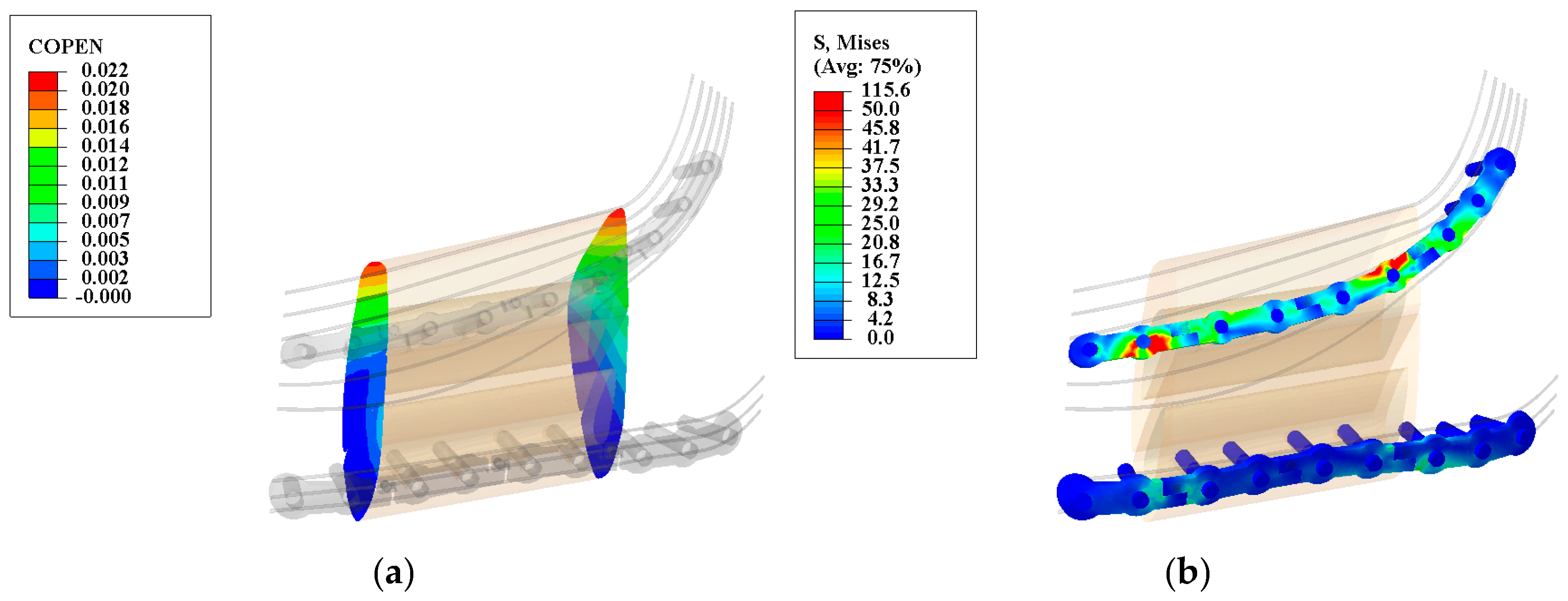
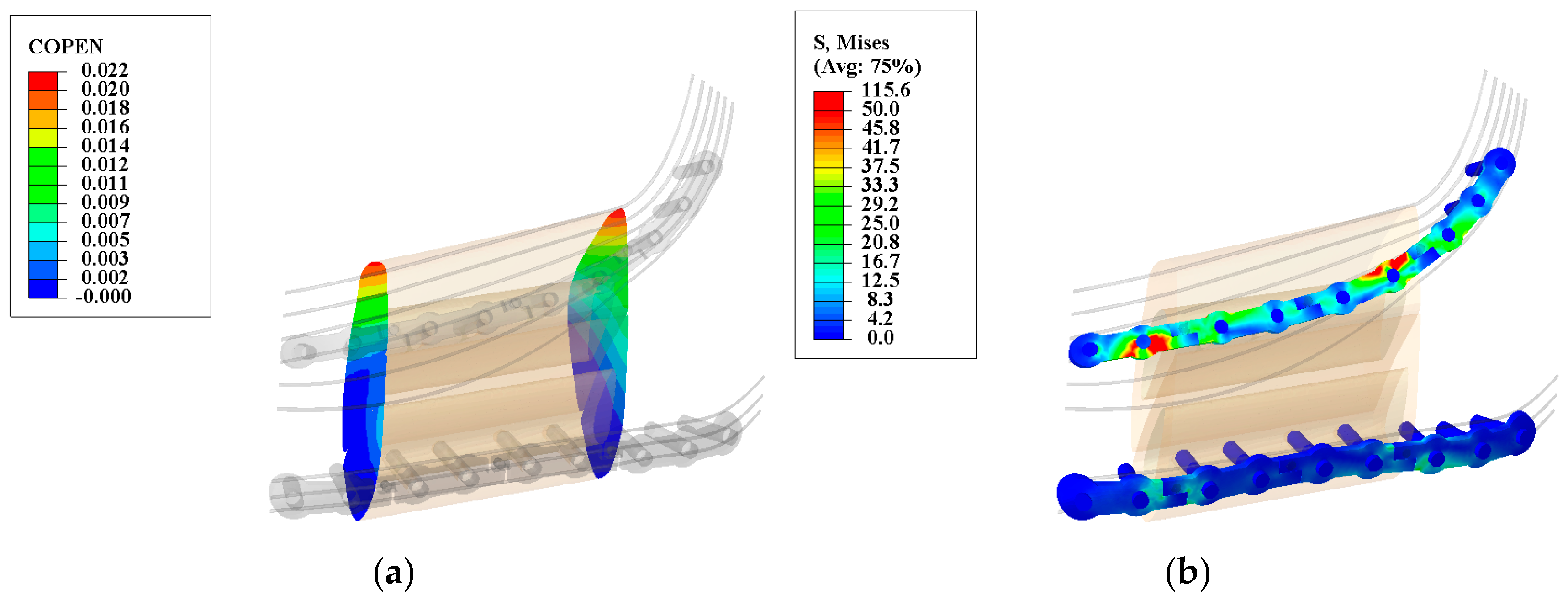
Figure 11.
Deformation map for the graft/mandible junction (a) and von Mises stress distribution along the releasable Ti-6Al-4V hardware (b) in the second stage. The observed gap is less than the allowable gap (200–400 μm) and the maximum observed von Mises stresses are less than their yielding points (superior hardware: 1186.8 MPa, and inferior hardware: 1098.6 MPa). (Units: micron (μm) and megapascal (MPa)).
Figure 11.
Deformation map for the graft/mandible junction (a) and von Mises stress distribution along the releasable Ti-6Al-4V hardware (b) in the second stage. The observed gap is less than the allowable gap (200–400 μm) and the maximum observed von Mises stresses are less than their yielding points (superior hardware: 1186.8 MPa, and inferior hardware: 1098.6 MPa). (Units: micron (μm) and megapascal (MPa)).
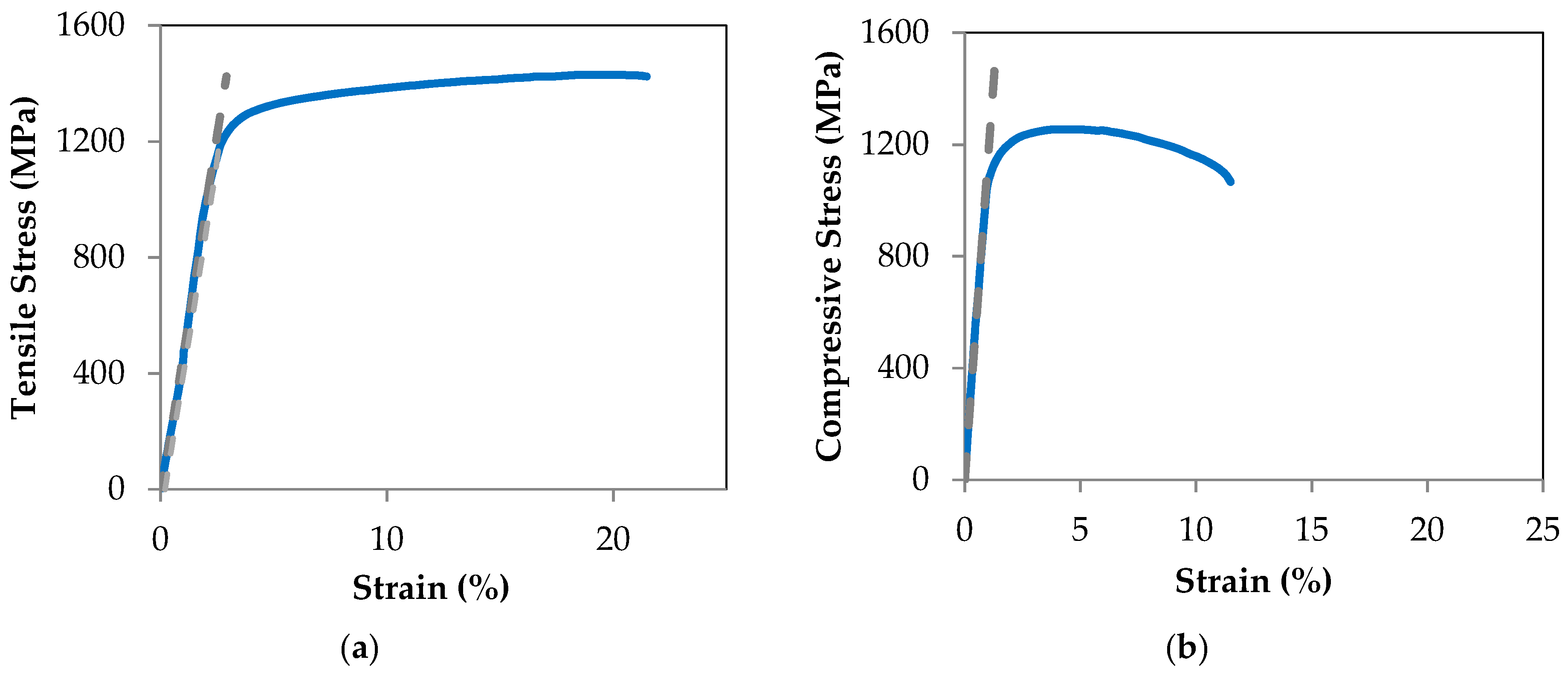
Figure 12.
Tensile (a) and compressive (b) stress-strain plots for Ti-6Al-4V hardware. The tensile and compressive yield stresses by 0.2% offset strain technique are calculated to be 1186.8 MPa and 1098.6 MPa, respectively.
Figure 12.
Tensile (a) and compressive (b) stress-strain plots for Ti-6Al-4V hardware. The tensile and compressive yield stresses by 0.2% offset strain technique are calculated to be 1186.8 MPa and 1098.6 MPa, respectively.
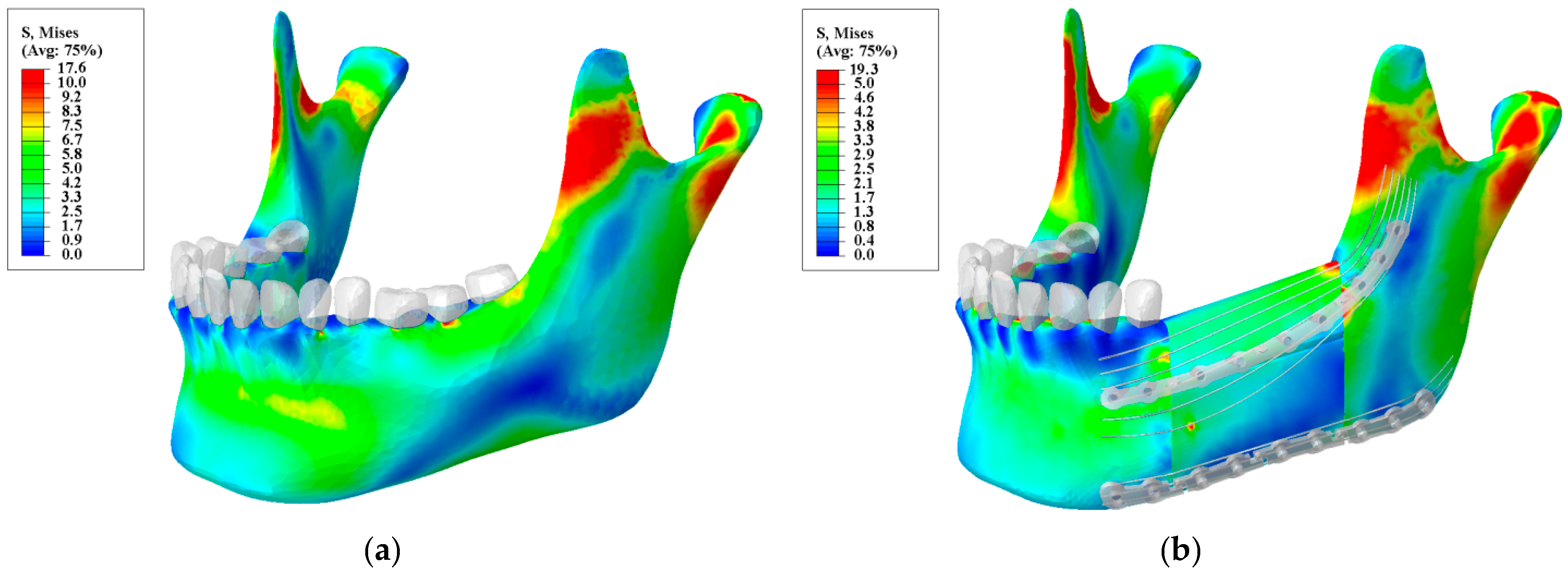
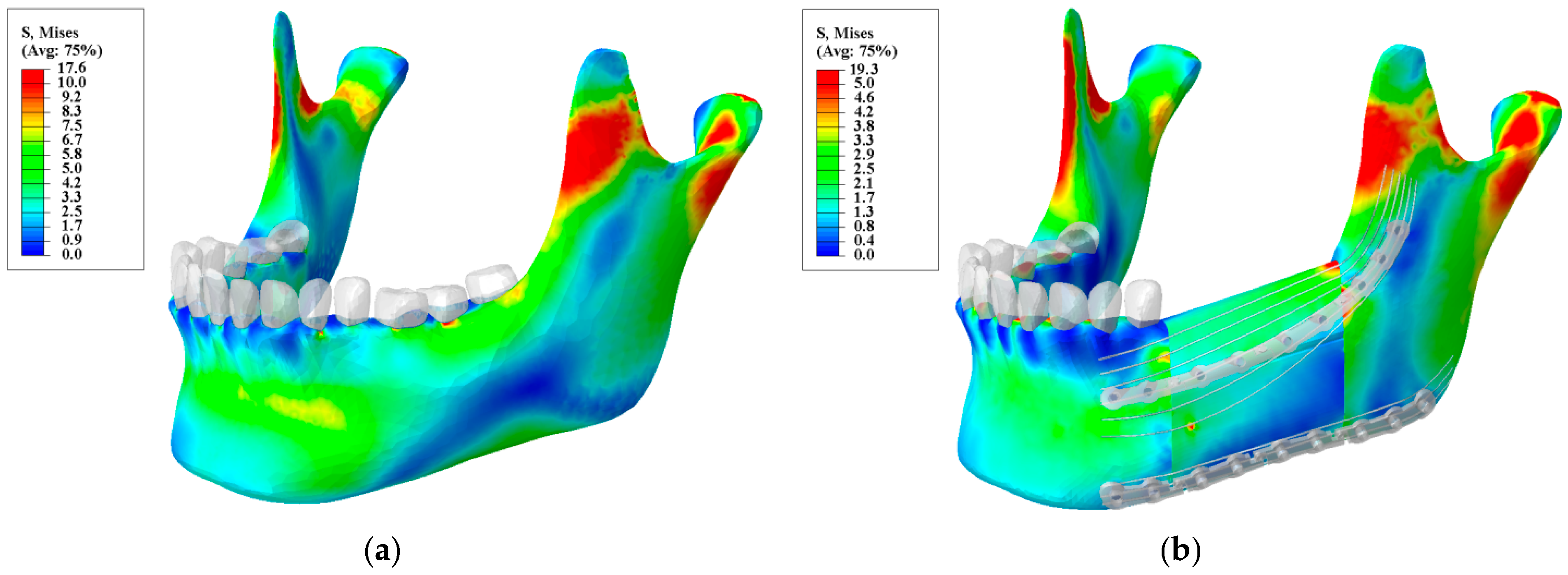
Figure 13.
Von Mises stress distribution for: (a) a normal mandible; and (b) a reconstructed mandible with releasable Ti-6Al-4V hardware and underlying optimized NiTi Bone Bandaid wires. (Unit: megapascal (MPa)).
Figure 13.
Von Mises stress distribution for: (a) a normal mandible; and (b) a reconstructed mandible with releasable Ti-6Al-4V hardware and underlying optimized NiTi Bone Bandaid wires. (Unit: megapascal (MPa)).
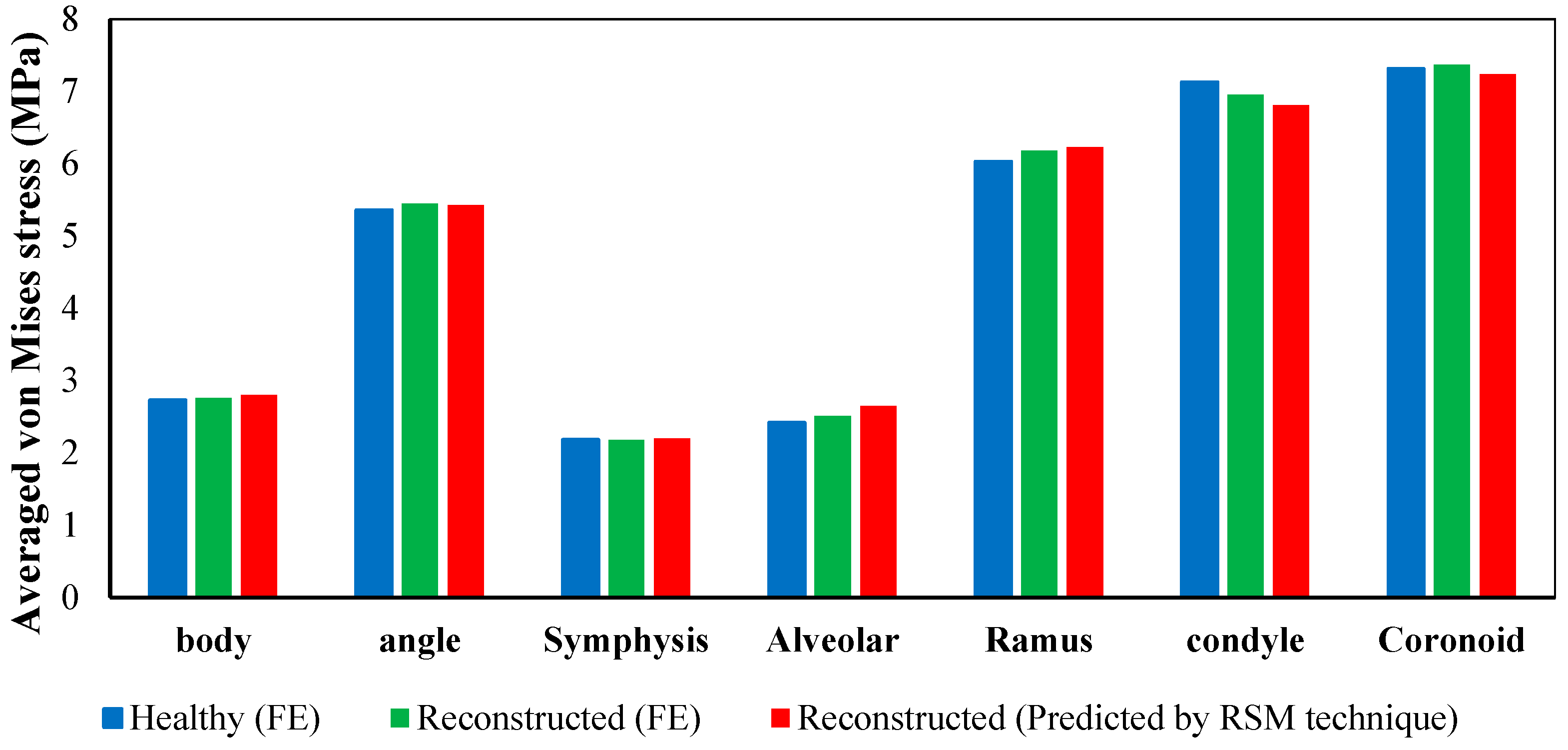
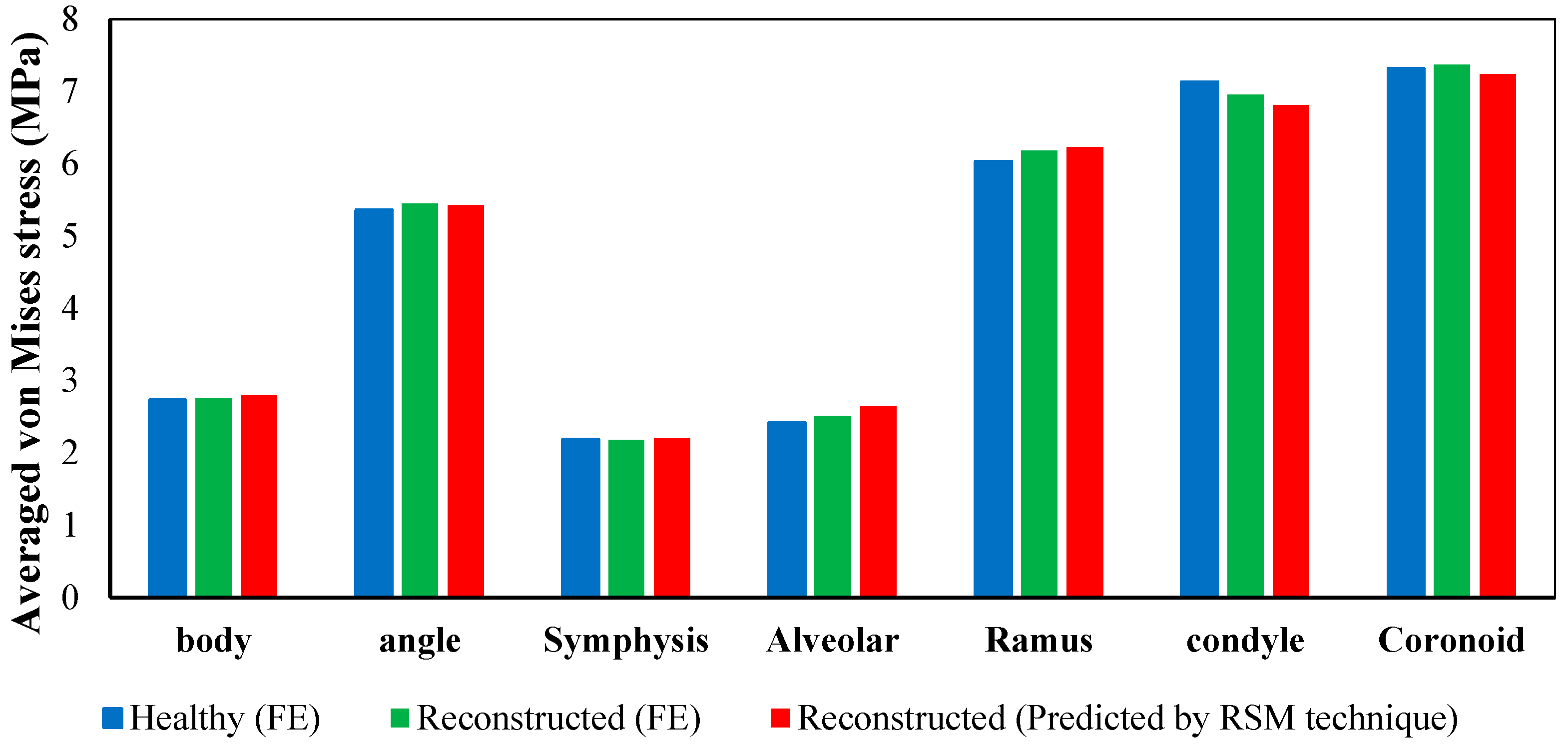
Figure 14.
Average von Mises stress in different regions obtained from finite element analysis of a normal adult mandible, finite element analysis of reconstructed mandible, and predicated values for reconstructed mandible from the second order function estimated by RSM technique.
Figure 14.
Average von Mises stress in different regions obtained from finite element analysis of a normal adult mandible, finite element analysis of reconstructed mandible, and predicated values for reconstructed mandible from the second order function estimated by RSM technique.
Table 1.
The number of elements for the Finite Element Analysis model components. The number of tetrahedral elements was determined by convergence analysis.
Table 1.
The number of elements for the Finite Element Analysis model components. The number of tetrahedral elements was determined by convergence analysis.
| Component | Number of Elements |
|---|
| Healthy mandible | 321,023 |
| Resected mandible | 218,328 |
| Teeth (13 Total) | 65,179 |
| Ligaments (13 Total) | 21,053 |
| Top Graft | 42,065 |
| Lower Graft | 45,037 |
| Fixation hardware(s) | 58,327 |
| Screws (10 Total) | 67,027 |
Table 2.
Material properties of the Finite Element Model components. (Unit: megapascal or MPa).
Table 2.
Material properties of the Finite Element Model components. (Unit: megapascal or MPa).
| Components | E (MPa) | |
|---|
| Cortical Fibular Graft | 26,800 | 0.3 |
| Cancellous Fibular Graft | 1650 | 0.3 |
| Ti-6Al-4V | 112,000 | 0.3 |
| NiTi | * 40,000 | 0.33 |
| ** 30,000 |
| Teeth | 17,600 | 0.25 |
| Periodontal Ligament | 2.7 | 0.45 |
Table 3.
The ranges of effective parameters.
Table 3.
The ranges of effective parameters.
| Variables, Unit | Factors | Range and Levels |
|---|
| −1 | 0 | 1 | |
|---|
| Inferior wires diameter (mm) | | 0.103 | 0.6 | 1.8 | 3 | 3.497 |
| Superior wires diameter (mm) | | 0.103 | 0.6 | 1.8 | 3 | 3.497 |
Table 4.
Material properties of the NiTi wires purchased from Fort Wayne Metals Ltd. (Fort Wayne, IN, USA).
Table 4.
Material properties of the NiTi wires purchased from Fort Wayne Metals Ltd. (Fort Wayne, IN, USA).
| Variables, Unit | Values |
|---|
| (MPa) | 40,000 |
| (MPa) | 30,000 |
| (°C) | −88 |
| (°C) | −65 |
| (°C) | −23 |
| (°C) | −8 |
| (MPa/°C) | 5.7 |
| (MPa/°C) | 8.6 |
| 0.039 |
Table 5.
Average von Mises stress in different regions obtained from finite element analysis of the healthy mandible vs. the reconstructed mandible (MPa).
Table 5.
Average von Mises stress in different regions obtained from finite element analysis of the healthy mandible vs. the reconstructed mandible (MPa).
| Mandible Type | Body | Angle | Symphysis | Alveolar | Ramus | Condyle | Coronoid |
|---|
| Healthy Mandible | 2.37 | 5.36 | 2.184 | 2.42 | 6.03 | 7.13 | 7.31 |
| Reconstructed | 4.17 | 8.00 | 3.27 | 3.98 | 9.65 | 9.92 | 10.52 |
Table 6.
The achieved coefficients from Response Surface Methodology (RSM) technique to predict the average von Mises stress in each zone.
Table 6.
The achieved coefficients from Response Surface Methodology (RSM) technique to predict the average von Mises stress in each zone.
| Mandible Zones | a | b | c | d | e | f |
|---|
| Body | 1.92 | 0.42 | 0.85 | −0.05 | −0.11 | −0.01 |
| Symphysis | 1.50 | 0.33 | 0.67 | −0.04 | −0.09 | −0.00 |
| Coronoid | 4.48 | 1.45 | 1.52 | −0.19 | −0.20 | 0.00 |
| Ramus | 4.44 | 0.77 | 2.18 | −0.09 | −0.30 | −0.2 |
| Alveolar | 1.83 | 0.31 | 0.90 | −0.03 | −0.12 | −0.00 |
| Condyle | 4.85 | 1.71 | 1.51 | −0.23 | −0.20 | −0.01 |
| Angle | 3.69 | 0.95 | 1.49 | −0.12 | −0.20 | −0.00 |
Table 7.
Predicted and observed values obtained from RSM technique (X1 = Inferior wires diameter, X2 = Superior wires diameter, O = Observe, i.e., calculated with Finite Element Analysis (FEA), P = Predicted, i.e., calculated by RSM).
Table 7.
Predicted and observed values obtained from RSM technique (X1 = Inferior wires diameter, X2 = Superior wires diameter, O = Observe, i.e., calculated with Finite Element Analysis (FEA), P = Predicted, i.e., calculated by RSM).
| Model Number | Factors | Average von Mises Stress in Different Zones of the Mandible |
|---|
| X1 | X2 | Body | Angle | Symphysis | Alveolar | Ramus | Condyle | Coronoid |
|---|
| O. | P. | O. | P. | O. | P. | O. | P. | O. | P. | O. | P. | O. | P. | O. | P. |
|---|
| 1 | 1.80 | 0.10 | 2.45 | 2.60 | 4.88 | 5.16 | 1.92 | 2.04 | 2.22 | 2.38 | 5.39 | 5.76 | 6.46 | 6.63 | 7.03 | 7.34 |
| 2 | 1.80 | 1.80 | 3.67 | 3.67 | 7.04 | 7.04 | 2.88 | 2.88 | 3.50 | 3.50 | 8.49 | 8.49 | 8.73 | 8.56 | 9.26 | 9.26 |
| 3 | 1.80 | 3.50 | 4.10 | 4.07 | 7.81 | 7.75 | 3.21 | 3.18 | 3.95 | 3.91 | 9.59 | 9.48 | 9.54 | 9.30 | 10.05 | 10.01 |
| 4 | 0.10 | 1.80 | 3.02 | 3.13 | 5.60 | 5.82 | 2.36 | 2.45 | 2.99 | 3.08 | 7.25 | 7.48 | 6.55 | 6.72 | 6.76 | 7.10 |
| 5 | 3.00 | 3.00 | 4.17 | 4.22 | 8.00 | 8.09 | 3.27 | 3.31 | 3.98 | 4.02 | 9.65 | 9.76 | 9.92 | 9.83 | 10.52 | 10.64 |
| 6 | 3.50 | 1.80 | 3.90 | 3.91 | 7.55 | 7.55 | 3.06 | 3.06 | 3.68 | 3.70 | 8.93 | 8.96 | 9.51 | 9.28 | 10.14 | 10.09 |
| 7 | 0.60 | 0.60 | 2.79 | 2.63 | 5.35 | 5.05 | 2.19 | 2.06 | 2.66 | 2.51 | 6.45 | 6.08 | 6.64 | 6.13 | 7.03 | 6.63 |
| 8 | 0.60 | 3.00 | 3.69 | 3.67 | 6.94 | 6.87 | 2.89 | 2.87 | 3.60 | 3.59 | 8.73 | 8.71 | 8.31 | 8.02 | 8.68 | 8.52 |
| 9 | 3.00 | 0.60 | 3.27 | 3.18 | 6.41 | 6.26 | 2.56 | 2.49 | 3.04 | 2.94 | 7.36 | 7.13 | 8.25 | 7.95 | 8.87 | 8.75 |
| R-Square | 97.53% | 97.48% | 97.53% | 97.62% | 97.64% | 97.43% | 97.46% |


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}