
Mapping of Data-Sharing Repositories for Paediatric Clinical Research—A Rapid Review
 , , , , , , , , ,
, , , , , , , , ,
Abstract
:1. Introduction
2. Methods
- Relevance was assessed as the ability of each DSR to provide access to the IPD of the subjects included in the CTs.
- Paediatric specificity was evaluated based on the ability to filter by a generic age group (e.g., 0–6, 6–12, 6–18) or through the availability of specific keywords (e.g., paediatric, neonate).
- Access to IPD was evaluated on the basis of the type of access. Three different access types were identified:
- ○
- Direct sharing: Data are provided after a data-sharing agreement outlining the rules for data utilization has been signed by the user. No other action is required.
- ○
- Controlled access: Access is permitted after the user submits a formal application requesting data access. The data requestor may need to provide a research protocol and analysis plan, including information on data management and plans for publication of results. The data can only be accessed and analysed within the DSR’s workspace and not on the user’s computer. A data-sharing agreement must be signed by the user.
- ○
- Open access: There is no formal process to access data. Researchers may explore but not download the data without a specific request.
- Different de-identification measures are adopted to protect the privacy of data subjects, e.g., pseudonymization or anonymization. An adequate de-identification (or encryption) measure is key to protecting study participants from reidentification. In the de-identification process, the participant’s identifiable information is removed or replaced with a code, usually a random code number.
- Pseudonymization processes personal data in such a way that it can no longer be attributed to a specific data subject without the use of additional information (e.g., a specifically created confidential key). Anonymization is a process that destroys any link to an identified or identifiable person via a pseudonym.
3. Results
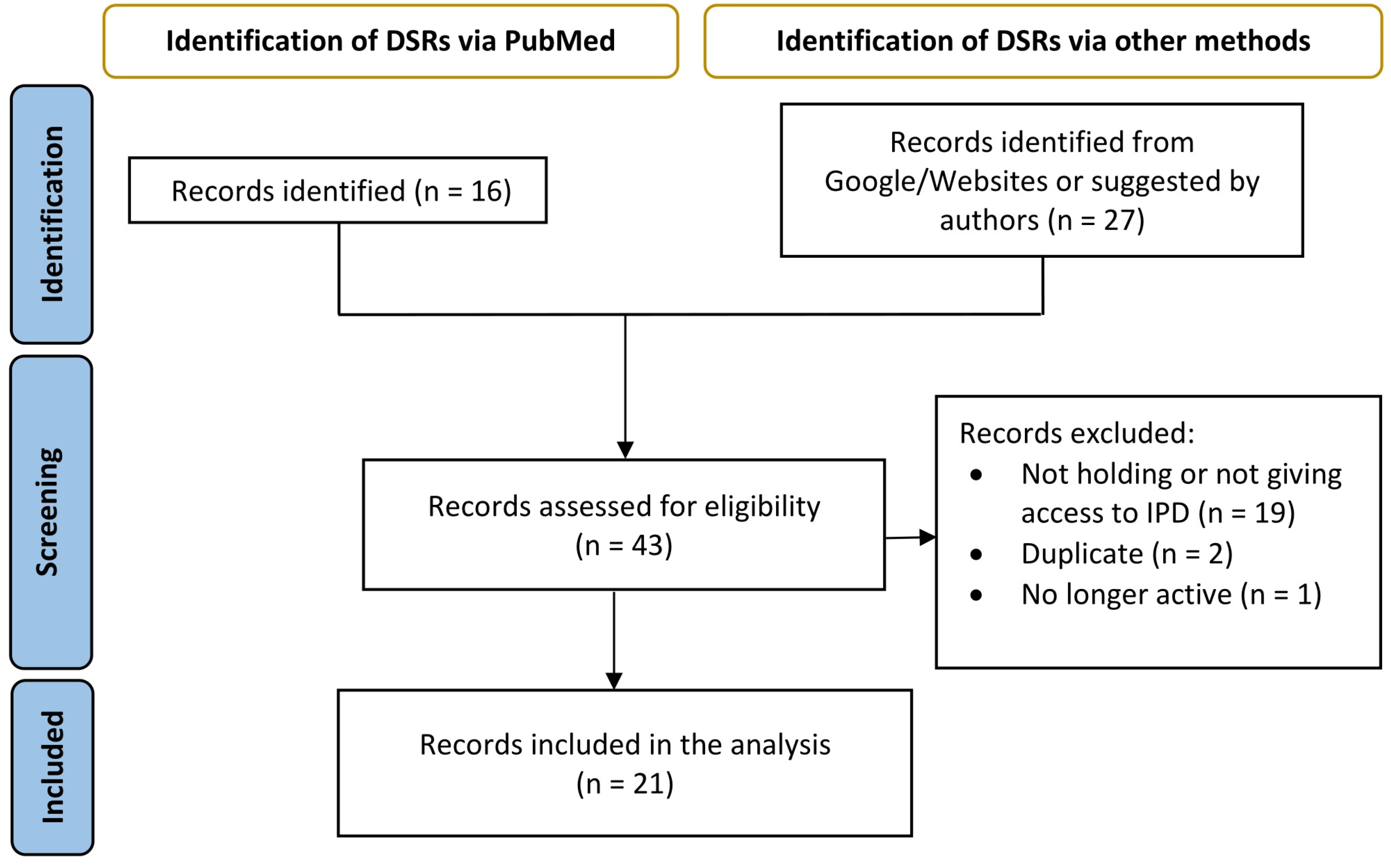
3.1. Literature Search
3.2. DSRs Selection
3.3. Data-Sharing Repositories’ Characteristics
3.4. Analysis of the Eight Indicators
- Relevance and Paediatric Specificity
- 2.
- Instructions for data owners/data submitters
- 3.
- Instructions for prospective data users
- 4.
- Guidance on data composition/structure/format for data owners/submitters
- 5.
- Data Protection
- 6.
- Procedures for Patient-Level Data Access
- Data sharing is adopted in six DSRs.
- The controlled access model is adopted by twelve DSRs.
- Open access is adopted only by one DSR.
- 7.
- IT Security Measures/Protocols
- 8.
- Sustainability
3.5. Cluster Analysis
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| Analysis Data Model (ADaM) |
| Artificial Intelligence (AI) |
| Best Pharmaceuticals for Children Act (BPCA) |
| Biologic Specimen and Data Repository Information Coordinating Center (BioLINCC) |
| Case Report Forms (CRFs) |
| Clinical Data Acquisition Standards Harmonization (CDASH) |
| Clinical Data Interchange Standards Consortium (CDISC) |
| Clinical Research Data Sharing Alliance (CRDSA) |
| Clinical Study Data Request (CSDR) |
| Clinical trials (CTs) |
| Coordinated Research Infrastructures Building Enduring Life-science (CORBEL) |
| Comma-Separated Values (CSV) |
| connect4children (c4c) |
| Data and Specimen Hub (DASH) |
| Data-sharing repositories (DSRs) |
| Data-sharing repository (DSR) |
| European Federation of Pharmaceutical Industries and Associations (EFPIA) |
| European Genome-phenome Archive (EGA) |
| European Medicines Agency (EMA) |
| European Union (EU) |
| Findable, Accessible, Interoperable, Reusable (FAIR) |
| Food and Drug Administration Amendments Act (FDAAA) |
| Food and Drug Administration Modernization Act (FDAMA) |
| Genomic Data Commons (GDC) |
| Health and Human Services (HHS) |
| International Business Machines Corporation Statistical Package for the Social Sciences (IBM SPSS) |
| International Committee of Medical Journal Editors (ICMJE) |
| Image & Data Archive (IDA) |
| Infectious Diseases Data Observatory (IDDO) |
| Immune Tolerance Network (ITN) |
| Immunology Database and Analysis Portal (ImmPort) |
| IMProving Access to Clinical Trial data (IMPACT) |
| Independent Review Panel (IRP) |
| Institute of Medicine (IOM) |
| Innovative Medicines Initiative 2 (IMI2) |
| International Business Machines Corporation (IBM) |
| Individual Paediatric patient data (IPD) |
| National Cancer Institute (NCI) |
| National Institutes of Health (NIH) |
| National Heart, Lung, and Blood Institute (NHLBI) |
| National Institute of Allergy and Infectious Diseases (NIAID) |
| National Institute of Child Health and Human Development (NICHD) |
| National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) |
| National Institute of Environmental Health Sciences (NIEHS) |
| National Institute of Mental Health (NIMH) |
| National Institute of Neurological Disorders and Stroke (NINDS) |
| National Institute on Drug Abuse (NIDA) |
| National Sleep Research Resource (NSRR) |
| Pediatric Cancer Data Commons (PCDC) |
| Paediatric Trials Network (PTN) |
| Pharmaceutical Research and Manufacturers of America (PhRMA) |
| Project Data Sphere (PDS) |
| Rare Disease Cures Accelerator–Data Analytical Platform (RDCA-DAP) |
| Statistical Analysis System (SAS) |
| Schwarz’s Bayesian Information Criterion (SBIC) |
| Study Data Tabulation Model (SDTM) |
| United Kingdom Research and Innovation (UKRI) |
| Yale University Open Data Access (YODA) |
References
- Wan, M.; Alessandrini, E.; Brogan, P.; Eleftheriou, D.; Warris, A.; Brüggemann, R.; Turner, M. Risk-Proportionate Approach to Paediatric Clinical Trials: The Legal Requirements, Challenges, and the Way Forward under the European Union Clinical Trials Regulation. Clin. Trials 2022, 19, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.A.; Hildebrand, H.; Fernandes, R.M.; De Wildt, S.N.; Mahler, F.; Hankard, R.; Leary, R.; Bonifazi, F.; Nobels, P.; Cheng, K.; et al. The conect4children (c4c) Consortium: Potential for Improving European Clinical Research into Medicines for Children. Pharm. Med. 2021, 35, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Chiaruttini, G.; Felisi, M.; Bonifazi, D. Challenges in Paediatric Clinical Trials: How to Make It Feasible. In The Management of Clinical Trials; Abdeldayem, H., Ed.; InTech: London, UK, 2018; p. 90. ISBN 978-1-78923-238-7. [Google Scholar]
- Weiss, E.M.; Porter, K.M.; Sullivan, T.R.; Sotelo Guerra, L.J.; Anderson, E.E.; Garrison, N.A.; Baker, L.; Smith, J.M.; Kraft, S.A. Equity Concerns Across Pediatric Research Recruitment: An Analysis of Research Staff Interviews. Acad. Pediatr. 2023, 24, 318–329. [Google Scholar] [CrossRef] [PubMed]
- Brewster, R.; Wong, M.; Magnani, C.J.; Gunningham, H.; Hoffer, M.; Showalter, S.; Tran, K.; Steinberg, J.R.; Turner, B.E.; Goodman, S.N.; et al. Early Discontinuation, Results Reporting, and Publication of Pediatric Clinical Trials. Pediatrics 2022, 149, e2021052557. [Google Scholar] [CrossRef] [PubMed]
- Goldacre, B.; Lane, S.; Mahtani, K.R.; Heneghan, C.; Onakpoya, I.; Bushfield, I.; Smeeth, L. Pharmaceutical Companies’ Policies on Access to Trial Data, Results, and Methods: Audit Study. BMJ 2017, 358, j3334. [Google Scholar] [CrossRef]
- Bertagnolli, M.M.; Sartor, O.; Chabner, B.A.; Rothenberg, M.L.; Khozin, S.; Hugh-Jones, C.; Reese, D.M.; Murphy, M.J. Advantages of a Truly Open-Access Data-Sharing Model. N. Engl. J. Med. 2017, 376, 1178–1181. [Google Scholar] [CrossRef] [PubMed]
- Taichman, D.B.; Sahni, P.; Pinborg, A.; Peiperl, L.; Laine, C.; James, A.; Hong, S.-T.; Haileamlak, A.; Gollogly, L.; Godlee, F.; et al. Data Sharing Statements for Clinical Trials. BMJ 2017, 357, j2372. [Google Scholar] [CrossRef] [PubMed]
- Welsh, J.; Lu, Y.; Dhruva, S.S.; Bikdeli, B.; Desai, N.R.; Benchetrit, L.; Zimmerman, C.O.; Mu, L.; Ross, J.S.; Krumholz, H.M. Age of Data at the Time of Publication of Contemporary Clinical Trials. JAMA Netw. Open 2018, 1, e181065. [Google Scholar] [CrossRef]
- Committee on Strategies for Responsible Sharing of Clinical Trial Data; Board on Health Sciences Policy; Institute of Medicine Guiding Principles for Sharing Clinical Trial Data. Sharing Clinical Trial Data: Maximizing Benefits, Minimizing Risk; National Academies Press: Washington, DC, USA, 2015; p. 290. ISBN 978-0-309-31629-3. [Google Scholar]
- International Coalition of Medicines Regulatory Authorities (ICMRA) and the World Health Organization (WHO) Joint Statement on Transparency and Data Integrit. Available online: Https://Www.Icmra.Info/Drupal/En/Covid-19/Joint_statement_on_transparency_and_data_integrity (accessed on 3 October 2023).
- U.S. Food and Drug Administration Pediatric Research Equity Act | PREA. Available online: Https://Www.Fda.Gov/Drugs/Development-Resources/Pediatric-Research-Equity-Act-Prea (accessed on 3 October 2023).
- U.S. Food and Drug Administration Best Pharmaceuticals for Children Act (BPCA). Available online: Https://Www.Fda.Gov/Drugs/Development-Resources/Best-Pharmaceuticals-Children-Act-Bpca (accessed on 3 October 2023).
- European Parliament, the Council of the European Union Regulation (EC) No 1901/2006 of The European Parliament and of the Council of 12 December 2006 on Medicinal Products for Paediatric Use, and Regulation (EC) No 1902/2006 Amending Regulation in Which Changes to the Original Text Were Introduced Relating to Decision Procedures for the European Commission. 2006. Available online: https://www.ema.europa.eu/en/human-regulatory-overview/paediatric-medicines-overview/paediatric-regulation (accessed on 11 March 2024).
- European Commission. Evaluation of Medicines for Rare Diseases and Children Legislation. European Commission. 2020. Available online: https://health.ec.europa.eu/medicinal-products/medicines-children/evaluation-medicines-rare-diseases-and-children-legislation_en (accessed on 11 March 2024).
- European Parliament, the Council of the European Union REGULATION (EU) No 536/2014 of the European Parliament and of the Council of 16 April 2014 on Clinical Trials on Medicinal Products for Human Use, and Repealing Directive 2001/20/EC. 2020. Available online: Https://Eur-Lex.Europa.Eu/Eli/Reg/2014/536/Oj (accessed on 3 October 2023).
- Pisani, E.; Aaby, P.; Breugelmans, J.G.; Carr, D.; Groves, T.; Helinski, M.; Kamuya, D.; Kern, S.; Littler, K.; Marsh, V.; et al. Beyond Open Data: Realising the Health Benefits of Sharing Data: Table 1. BMJ 2016, 355, i5295. [Google Scholar] [CrossRef]
- Ohmann, C.; Banzi, R.; Canham, S.; Battaglia, S.; Matei, M.; Ariyo, C.; Becnel, L.; Bierer, B.; Bowers, S.; Clivio, L.; et al. Sharing and Reuse of Individual Participant Data from Clinical Trials: Principles and Recommendations. BMJ Open 2017, 7, e018647. [Google Scholar] [CrossRef]
- Kiley, R.; Peatfield, T.; Hansen, J.; Reddington, F. Data Sharing from Clinical Trials—A Research Funder’s Perspective. N. Engl. J. Med. 2017, 377, 1990–1992. [Google Scholar] [CrossRef] [PubMed]
- Antman, E. Data Sharing in Research: Benefits and Risks for Clinicians. BMJ 2014, 348, g237. [Google Scholar] [CrossRef] [PubMed]
- Sardanelli, F.; Alì, M.; Hunink, M.G.; Houssami, N.; Sconfienza, L.M.; Di Leo, G. To Share or Not to Share? Expected Pros and Cons of Data Sharing in Radiological Research. Eur. Radiol. 2018, 28, 2328–2335. [Google Scholar] [CrossRef] [PubMed]
- Hrynaszkiewicz, I.; Norton, M.L.; Vickers, A.J.; Altman, D.G. Preparing Raw Clinical Data for Publication: Guidance for Journal Editors, Authors, and Peer Reviewers. Trials 2010, 11, 9. [Google Scholar] [CrossRef] [PubMed]
- Mello, M.M.; Lieou, V.; Goodman, S.N. Clinical Trial Participants’ Views of the Risks and Benefits of Data Sharing. N. Engl. J. Med. 2018, 378, 2202–2211. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.-W.; Da Silva Santos, L.B.; Bourne, P.E.; et al. The FAIR Guiding Principles for Scientific Data Management and Stewardship. Sci Data 2016, 3, 160018. [Google Scholar] [CrossRef] [PubMed]
- InfoScipedia-IGI Global Publishing House. Available online: https://Www.Igi-Global.Com/Dictionary/Digital-Repositories/7693 (accessed on 3 October 2023).
- Banzi, R.; Canham, S.; Kuchinke, W.; Krleza-Jeric, K.; Demotes-Mainard, J.; Ohmann, C. Evaluation of Repositories for Sharing Individual-Participant Data from Clinical Studies. Trials 2019, 20, 169. [Google Scholar] [CrossRef] [PubMed]
- Forero, D.A.; Curioso, W.H.; Patrinos, G.P. The Importance of Adherence to International Standards for Depositing Open Data in Public Repositories. BMC Res. Notes 2021, 14, 405. [Google Scholar] [CrossRef] [PubMed]
- Speer, E.M.; Lee, L.K.; Bourgeois, F.T.; Gitterman, D.; Hay, W.W.; Davis, J.M.; Javier, J.R. The State and Future of Pediatric Research—An Introductory Overview: The State and Future of Pediatric Research Series. Pediatr. Res. 2023, 1–5. [Google Scholar] [CrossRef]
- Cook, D.A.; Beckman, T.J. Current Concepts in Validity and Reliability for Psychometric Instruments: Theory and Application. Am. J. Med. 2006, 119, 166.e7–166.e16. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater Reliability: The Kappa Statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Morey, L.C.; Blashfield, R.K.; Skinner, H.A. A Comparison of Cluster Analysis Techniques Withing a Sequential Validation Framework. Multivar. Behav. Res. 1983, 18, 309–329. [Google Scholar] [CrossRef] [PubMed]
- Hartigan, J.A.; Wong, M.A. Algorithm AS 136: A K-Means Clustering Algorithm. Appl. Stat. 1979, 28, 100–108. [Google Scholar] [CrossRef]
- Schwarz, G. Estimating the Dimension of a Model. Ann. Statist. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- International Committee of Medical Journal Editors (ICMJE) International Committee of Medical Journal Editors (ICMJE): Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publication. Haematologica 2004, 89, 264.
- United States Congress. Senate Bill S. 558 PUBLIC LAW 110–85—SEPT. 27, 2007. Available online: Https://Www.Govinfo.Gov/Content/Pkg/PLAW-110publ85/Pdf/PLAW-110publ85.Pdf#page=82 (accessed on 3 October 2023).
- Summaries of Clinical Trial Results for Laypersons. Available online: https://health.ec.europa.eu/system/files/2020-02/2017_01_26_summaries_of_ct_results_for_laypersons_0.pdf (accessed on 3 October 2023).
- European Medicines Agency External Guidance on the Implementation of the European Medicines Agency Policy on the Publication of Clinical Data for Medicinal Products for Human Use. Available online: Https://Www.Ema.Europa.Eu/En/Documents/Regulatory-Procedural-Guideline/External-Guidance-Implementation-European-Medicines-Agency-Policy-Publication-Clinical-Data_en-1.Pdf (accessed on 3 October 2023).
- Siebert, M.; Gaba, J.F.; Caquelin, L.; Gouraud, H.; Dupuy, A.; Moher, D.; Naudet, F. Data-Sharing Recommendations in Biomedical Journals and Randomised Controlled Trials: An Audit of Journals Following the ICMJE Recommendations. BMJ Open 2020, 10, e038887. [Google Scholar] [CrossRef] [PubMed]
- Nosek, B.A.; Alter, G.; Banks, G.C.; Borsboom, D.; Bowman, S.D.; Breckler, S.J.; Buck, S.; Chambers, C.D.; Chin, G.; Christensen, G.; et al. Promoting an Open Research Culture. Science 2015, 348, 1422–1425. [Google Scholar] [CrossRef] [PubMed]
- Anthony, N.; Pellen, C.; Ohmann, C.; Moher, D.; Naudet, F. Social Media Attention and Citations of Published Outputs from Re-Use of Clinical Trial Data: A Matched Comparison with Articles Published in the Same Journals. BMC Med. Res. Methodol. 2021, 21, 119. [Google Scholar] [CrossRef] [PubMed]
- Ohmann, C.; Moher, D.; Siebert, M.; Motschall, E.; Naudet, F. Status, Use and Impact of Sharing Individual Participant Data from Clinical Trials: A Scoping Review. BMJ Open 2021, 11, e049228. [Google Scholar] [CrossRef] [PubMed]
- Clinical Research Data Sharing Alliance: CRDSA, Work Group: Data Protection A Review of Biopharma Sponsor Data Sharing Policies and Protection Methodologies 2023—Version: 2.0 2023. Available online: https://crdsalliance.org/?smd_process_download=1&download_id=469 (accessed on 3 October 2023).
- McMurry, A.J.; Murphy, S.N.; MacFadden, D.; Weber, G.; Simons, W.W.; Orechia, J.; Bickel, J.; Wattanasin, N.; Gilbert, C.; Trevvett, P.; et al. SHRINE: Enabling nationally scalable multi-site disease studies. PLoS ONE 2013, 8, e55811. [Google Scholar] [CrossRef]
- Nabbout, R.; Zanello, G.; Baker, D.; Black, L.; Brambilla, I.; Buske, O.J.; Conklin, L.S.; Davies, E.H.; Julkowska, D.; Kim, Y.; et al. Towards the international interoperability of clinical research networks for rare diseases: Recommendations from the IRDiRC Task Force. Orphanet J. Rare Dis. 2023, 18, 109. [Google Scholar] [CrossRef]
- Loudon, K.; Treweek, S.; Sullivan, F.; Donnan, P.; Thorpe, K.E.; Zwarenstein, M. The PRECIS-2 tool: Designing trials that are fit for purpose. BMJ 2015, 350, h2147. [Google Scholar] [CrossRef] [PubMed]
- Lehne, M.; Sass, J.; Essenwanger, A.; Schepers, J.; Thun, S. Why digital medicine depends on interoperability. NPJ Digit. Med. 2019, 2, 79. [Google Scholar] [CrossRef] [PubMed]
- Hodson, S.; Jones, S.; Collins, S.; Genova, F.; Harrower, N.; Mietchen, D.; Petrauskaité, R.; Wittenburg, P. FAIR Data Action Plan: Interim Recommendations and Actions from the European Commission Expert Group on FAIR Data; Zenodo: City, Country, 2018. [Google Scholar] [CrossRef]


{kind=link}
| General features |
|
|
|
|
|
|
|
| Data and document features |
|
|
|
|
|
| Paediatric specificity |
|
|
| Legal provisions |
|
|
|
|
| ITs |
|
| Score | 1. Relevance and Paediatric Specificity | 2. Instructions for Data Owners/Data Submitters | 3. Instructions for Prospective Data Users | 4. Guidance on Data Composition/Structure/Format, for Data Owners/Submitters | 5. Data Protection | 6. Procedures for Patient-Level Data Access | 7. It | 8. Sustainability |
|---|---|---|---|---|---|---|---|---|
| 0 | If the DSR currently contains paediatric CT data but there is no chance * to filter and download/access only paediatric data. | If no instructions are available * for data owners/submitters to advise on what data are in scope and how to submit their data. | If no clear instructions for prospective data users are publicly available. * | If the DSR has no publicly available guidance or recommendations for data owners/submitters on specific models, standards, or formats for data OR for metadata. * | If there is no public mention of data protection. * | If measures or procedures to access data are not reported. * | If no security protocol or safety measures are publicly mentioned on the website. * | If funding is not currently available and the sustainability of the DSR appears uncertain. * |
| 1 | If the DSR currently contains paediatric CT data but limited filtering options are available: (e.g., filters for generic age groups only, such as paediatric, adults, geriatric). * | If only basic ‘how-to upload’ instructions are publicly available (and/or if detailed instructions on what is in scope and how data should be submitted DO exist but are not publicly available). * | If only basic instructions on ‘how to access/download/analyse’ data are available publicly, or if detailed instructions are available but are not publicly visible. * | If some guidance or recommendations are provided for data owners/submitters concerning specific models, standards, or formats for data OR for metadata but this guidance is not exhaustive. * | If data protection measures are mentioned generally, but no data protection policy is specified or made publicly available. * | If measures or procedures to access individual patient data are generally mentioned but not clearly explained. * | If the DSR makes available on the website only a summary protocol for regularly testing, assessing, and evaluating the effectiveness of technical and organizational measures to ensure the security of the processing is in place. * | If the DSR has no regular/sustained funding but has business continuity measures in place. * |
| 2 | If the DSR currently contains paediatric CT data which can easily be filtered by specific paediatric age groups (e.g., below 2, between 5 and 10 years, etc). | If the DSR provides clear instructions for data owners/submitters on what data are in scope and how to submit their data (including information on any specific formats or schemas requested) and makes these instructions publicly available. | If the DSR has—and makes publicly available—clear instructions for prospective data users on how to access and/or analyse data, including. | If the DSR provides clear guidance or recommendations for data owners/submitters on specific models, standards, or formats for data OR for metadata. | If a data protection policy for the DSR is publicly available. | If procedures and materials relating to individual patient data access agreements are clearly presented and/or a data access agreement template is proposed for adoption. | If the DSR has a security protocol for regularly testing, assessing, and evaluating the effectiveness of technical and organizational measures to ensure the security of the processing in place and the protocol is available on the website. | If the DSR receives regular/sustained funding and can demonstrate business continuity measures. |
| Name | Year of Establishment | Location | Funding Source | Data Access Type (Direct Sharing, Controlled Access, Open Access) | URL |
|---|---|---|---|---|---|
| BioCelerate (TransCelerate) | 2018 | US | Private: TransCelerate BioPharma (not-for-profit) | Controlled access | https://www.transceleratebiopharmainc.com/initiatives/datacelerate/ (accessed on 3 October 2023) |
| BioLINCC | 2000 | US | Public: US Government’s National Institutes of Health—National Heart, Lung, and Blood Institute (NHLBI) | Controlled access | https://biolincc.nhlbi.nih.gov/home/ (accessed on 3 October 2023) |
| Clinical Study Data Request (CSDR) | 2016 | US | Private: Astellas, Bayer, Bill and Melinda gates, Boehringer Ingelheim, Cancer Research UK, Chugai/Roche, Daiichi-Sankyo, Eisai, gsk, Lilly, etc. | Controlled access | https://www.clinicalstudydatarequest.com (accessed on 3 October 2023) |
| Dryad Digital DSR | 2008 | US | Public sponsor: National Science Foundation to the National Evolutionary Synthesis Center and other partners in the US | Controlled access | https://datadryad.org/ (accessed on 3 October 2023) |
| European Genome-phenome Archive (EGA) | 2008 | EU | Public: ELIXIR infrastructure | Direct sharing | https://ega-archive.org/ (accessed on 3 October 2023) |
| Health Data Research Innovation Gateway | 2020 | EU | Public: UK Research and Innovation’s (UKRI) Industrial Strategy Challenge Fund | Direct sharing | https://www.healthdatagateway.org/about/our-mission-and-purpose (accessed on 3 October 2023) |
| Infectious Diseases Data Observatory (IDDO) | 2009 | EU | Public sponsor: Oxford University | Controlled access | https://www.iddo.org/about-us/about-iddo (accessed on 3 October 2023) |
| Immunology Database and Analysis Portal (ImmPort) | 2017 | US | Public: National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), Health and Human Services (HHS) | Open access | https://www.immport.org/shared/ (accessed on 3 October 2023) |
| Immune Tolerance Network (ITN) TrialShare | 2017 | US | Public: NIAID, NIH | Controlled Access | Sign In: /home (itntrialshare.org) (accessed on 3 October 2023) |
| Laboratory of Neuroimaging Image & Data Archive (IDA) | 2003 | US | Public: National Institutes of Health, National Institute of Biomedical Imaging and Bioengineering | Controlled Access | https://ida.loni.usc.edu/login.jsp (accessed on 3 October 2023) |
| National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Central DSR | 2003 | US | Public | Direct sharing | https://DSR.niddk.nih.gov/home/ (accessed on 3 October 2023) |
| National Institute on Drug Abuse (NIDA) | 2014 | US | Public: National Institutes of Health (NIH) | Direct sharing | https://datashare.nida.nih.gov/ (accessed on 3 October 2023) |
| National Sleep Research Resource (NSRR) | 2014 | US | Public: National Heart, Lung, and Blood Institute (NHLBI) | Controlled access | https://sleepdata.org/ (accessed on 3 October 2023) |
| Pediatric Cancer Data Commons (PCDC) | 2015 | US | Public: Collaborative grant from the University of Chicago, philanthropic support, and contracts from The National Cancer Institute (NCI) | Controlled access | https://portal.pedscommons.org/ (accessed on 3 October 2023) |
| Paediatric Trials Network (PTN)/DASH (data and specimen hub) | 2010 | US | Public: Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) | Direct sharing | https://www.pediatrictrials.org/ (accessed on 3 October 2023) |
| Project Data Sphere (PDS) | 2014 | US | Public: CEO Roundtable on Cancer, Inc. (non-profit organization) | Controlled access | https://www.projectdatasphere.org/projectdatasphere/html/home (accessed on 3 October 2023) |
| Rare Disease Cures Accelerator–Data Analytical Platform (RDCA-DAP) | 2021 | US | Collaborative grant from the FDA | Controlled access | https://c-path.org/programs/rdca-dap/ (accessed on 3 October 2023) |
| The National Cancer Institute’s Genomic Data Commons (GDC) | 2016 | US | Public | Controlled access | https://gdc.cancer.gov/ (accessed on 3 October 2023) |
| The National Institute of Mental Health (NIMH) Data Archive | 2014 | US | Public: National Institute of Mental Health (NIMH); National Institute of Neurological Disorders and Stroke (NINDS); National Institute of Environmental Health Sciences (NIEHS); The Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) | Controlled access | https://nda.nih.gov/ (accessed on 3 October 2023) |
| Vivli | 2017 | US | Private non-profit: Doris Duke charitable Foundation; Lyda Hill Foundation; The Leona M. and Harry B. Helmsley charitable trust; Laura and John Arnold Foundation Private profit: PhRMa | Direct sharing | http://vivli.org/ (accessed on 3 October 2023) |
| YODA project | 2014 | US | Private: Johnson & Johnson Medtronic, Inc.; Queen Mary University of London; SI-BONE, Inc. | Direct sharing | http://yoda.yale.edu/ (accessed on 3 October 2023) |
| DSR | 1. Relevance and Paediatric Specificity | 2. Instructions for Data Owners/Data Submitters | 3. Instructions for Prospective Data Users | 4. Guidance on Data Composition/Structure/Format, for Data Owners/Submitters | 5. Data Protection | 6. Procedures for Patient-Level Data Access | 7. IT Security Measures/Protocols | 8. Sustainability | |
|---|---|---|---|---|---|---|---|---|---|
| Biocelerate (Transcelerate) | + | ++ | ++ | ++ | + | ++ | + | +++ | |
| BioLINCC | + | +++ | + | +++ | + | +++ | + | +++ | |
| ClinicalStudyDataRequest (CSDR) | + | + | +++ | + | + | +++ | ++ | +++ | |
| Dryad Digital DSR | ++ | +++ | + | +++ | ++ | + | +++ | +++ | |
| European Genome-phenome Archive (EGA) | + | +++ | +++ | + | ++ | +++ | +++ | +++ | |
| Health Data Research Innovation Gateway | ++ | ++ | +++ | + | + | +++ | + | +++ | |
| Infectious Diseases Data Observatory (IDDO) | ++ | +++ | +++ | +++ | + | +++ | + | +++ | |
| Immunology Database and Analysis Portal (ImmPort) | +++ | +++ | +++ | ++ | + | +++ | ++ | +++ | |
| Immune Tolerance Network (ITN) TrialShare | ++ | +++ | +++ | + | ++ | ++ | + | +++ | |
| Laboratory of Neuroimaging Image & Data Archive (IDA) | + | +++ | +++ | + | + | +++ | ++ | +++ | |
| National Institute on Drug Abuse (NIDA) | +++ | + | +++ | + | ++ | +++ | ++ | +++ | |
| National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Central DSR | + | + | +++ | + | + | + | + | +++ | |
| National Sleep Research Resource (NSRR) | + | +++ | + | + | ++ | +++ | ++ | +++ | |
| Pediatric Cancer Data Commons (PCDC) | +++ | + | +++ | + | + | +++ | ++ | ++ | |
| Paediatric Trials Network (PTN)/DASH (data and specimen hub) | +++ | +++ | +++ | +++ | ++ | +++ | + | +++ | |
| Project Data Sphere (PDS) | + | + | +++ | + | + | +++ | + | +++ | |
| Rare Disease Cures Accelerator–Data Analytical Platform (RDCA-DAP) | +++ | +++ | +++ | +++ | +++ | +++ | +++ | ++ | |
| The National Cancer Institute’s Genomic Data Commons (GDC) | + | +++ | +++ | +++ | ++ | +++ | + | +++ | |
| The National Institute of Mental Health Data Archive (NDA) | ++ | +++ | +++ | +++ | +++ | +++ | ++ | +++ | |
| Vivli | ++ | +++ | +++ | ++ | +++ | +++ | ++ | +++ | |
| YODA project | ++ | + | +++ | + | ++ | +++ | ++ | +++ | |
| Legend | |||||||||
| SCORE | 0 | 1 | 2 | ||||||
| Level | + | ++ | +++ | ||||||
| Repository | Cluster |
|---|---|
| Immunology Database and Analysis Portal (ImmPort) | 1 |
| Paediatric Trials Network (PTN)/DASH (data and specimen hub | |
| Rare Disease Cures Accelerator – Data Analytical Platform (RDCA-DAP) | |
| The National Institute of Mental Health (NIMH) Data Archive | |
| Vivli | |
| Biocelerate (Transcelerate) | 2 |
| BioLINCC | |
| Clinical Study Data Request (CSDR) | |
| Dryad Digital Repository | |
| European Genome-phenome Archive (EGA) | |
| Health Data Resaerch Innovation Gateway | |
| IDDO Infectious Diseases Data Observatory | |
| ITN TrialShare | |
| Laboratory of Neuroimaging Image & Data Archive (IDA) | |
| National Sleep Research Resource (NSRR) | |
| NIDA | |
| NIDDK Central Repository | |
| Pediatric Cancer Data Common (PCDC) | |
| Project Data Spere (PDS) | |
| The National Cancer Institute’s Genomic Data Commons | |
| YODA project |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Felisi, M.; Bonifazi, F.; Toma, M.; Pansieri, C.; Leary, R.; Hedley, V.; Cornet, R.; Reggiardo, G.; Landi, A.; D’Ercole, A.; et al. Mapping of Data-Sharing Repositories for Paediatric Clinical Research—A Rapid Review. Data 2024, 9, 59. https://doi.org/10.3390/data9040059
Felisi M, Bonifazi F, Toma M, Pansieri C, Leary R, Hedley V, Cornet R, Reggiardo G, Landi A, D’Ercole A, et al. Mapping of Data-Sharing Repositories for Paediatric Clinical Research—A Rapid Review. Data. 2024; 9(4):59. https://doi.org/10.3390/data9040059
Chicago/Turabian StyleFelisi, Mariagrazia, Fedele Bonifazi, Maddalena Toma, Claudia Pansieri, Rebecca Leary, Victoria Hedley, Ronald Cornet, Giorgio Reggiardo, Annalisa Landi, Annunziata D’Ercole, and et al. 2024. "Mapping of Data-Sharing Repositories for Paediatric Clinical Research—A Rapid Review" Data 9, no. 4: 59. https://doi.org/10.3390/data9040059