Abstract
The language and approach we use to describe the past can have a strong influence on the audience’s interpretation of our story. In our experiment, we explore, using 3 different conditions, how the framing, language and style of an accident report can affect the audience’s proposed solutions to manage the problems found. We find that the approach used to create an accident report can have a powerful influence on the audience’s decision making. Whether we are describing an accident in a linear manner, using a systems approach, or we are accepting of multiple stories which are not linear or coherent, the methods we use to capture and communicate the story have a profound impact on the actions decided upon by the reader.
1. Introduction
How stories are framed can greatly influence the readers’ interpretation of the event and the actions taken as a result. The analysis of accidents and the accident report style used to share the story provides a prime example of this.
The language we use to tell a story can have a profound effect on how the listener or reader interprets the story. The power of language and metaphors is showcased in the work of Thibodeau and Boroditsky [1]. In their study, Thibodeau and Boroditsky presented participants with different descriptions of the same fictional city suffering from a surge in crime. Their study sought to understand how metaphors shape understanding and reasoning, and whether the use of different metaphors to describe crime would lead to the proposal of different solutions. Their study’s results showed that when the word “beast” was used to describe crime, the proposed solutions were much more likely to be enforcement-based, while when the word “virus” was used to describe crime, the proposed solutions became much more social-reform based.
The influence of the English language on our thoughts and actions, as opposed to other languages, should not be understated either. In the description of accidents, the English language consistently uses the agent of causality to describe the event e.g., “John dropped the vase”. Conversely, when describing accidents in Spanish or Japanese, the agent of causality is dropped, “The vase broke itself” [2]. This showcases how those of us who speak the English language are more likely to naturally focus upon human error because of our instinctive way of describing the world we see. When this is refined to how we normally hear about accidents, which is usually in a headline format to keep it sharp and simple, the accident becomes more about the individual than about the system issues which have led to it occurring due to how we tell the story. This can often unintentionally assist the creation of a blame culture and can have a serious impact on an organisation’s ability to learn.
Although the world of academia has generally accepted that most industrial accidents occur due to complex system issues [3] and that human error is but a symptom of a larger problem within the organisational system [4], many organisations, and society, remain deeply focussed on the front-line operator after an accident has occurred. Many accident reports still cite human error as a primary cause [5]. Reports for notable accidents such as the Bhopal chemical plant [6], the Herald of Free Enterprise [7] and the Kegworth air crash [8] have all highlighted human error as a key factor in the accident’s occurrence. All 3 of these accidents are used within safety training curriculum as examples of how things go wrong to this very day. This leads organisations to believe that it is the operator who is the main contributor to accidents and it is the operator who is the problem within their system which requires rectification. Today, almost every accident is followed by questions focussed on ‘‘whose fault?’’ [9] It seems as if every accident must be charged to somebody’s account [10]. This often results in someone being blamed and punished for an accident which was essentially created by complex system problems which arose from various relationships and interactions within the system [11].
The use of punitive or blame methods to manage mistakes or errors can be not only harmful to the worker [12] but also to an organisation’s learning ability [13]. Workforces are much less likely to report mistakes for fear of retribution [14,15], creating an organisational culture where a chief executive officer (CEO) only learns of the problems within their organisation after a person is seriously injured. Using punishment to deal with error is likely to create a culture where the workforce resent the very system that was supposed to enable them to work safely because of it using them as the sacrificial lamb to appease society when something goes wrong. The greatest impediment to learning from mistakes is the use of punishment [16] as you cannot have a system which punishes those who make mistakes while also trying to maintain a learning culture [17] which needs people to be open and honest when an error is made.
To counter these harms within our systems, the use of restorative mechanisms has been promoted as a more beneficial alternative to manage failure in the workplace and to achieve justice. Rather than continuing to use solely retributive mechanisms that will create long-lasting workplace wounds, the use of restorative mechanisms is proposed as a means of “addressing the harms that have been done and addressing the causes of these harms” [18]. Using this approach, the line of questioning following an accident would no longer be who is responsible, but what [19], and how can we fix the issue; not the person. The restorative principles, particular those put forward by Zehr and Gohar, are aligned with the work of Doctor Albert Wu and his Second Victim Theory [12]. Wu’s theory highlights the impact an accident has upon those who feel personally responsible for the accident’s occurrence and the need for organisations to help these individuals to recover from their mistake, rather than vilify and ostracise them.
The accident model and writing style chosen by the accident facilitator play a critical role in the level of learning achieved by an organisation following an accident. There are many accident models available today, with several having contrasting styles. Some follow the root cause analysis approach, where the use of reductionism can often lead to a form of human error as a conclusion. Other models are more systems-orientated, placing the focus more on system relationships and emergent risk. For the accident facilitator, “what you look for is what you find” [20]. If you are looking for someone to blame, they are easily found, particularly in hindsight. The style of model used may dictate the information provided to the reader. For an organisation deciding upon the actions to prevent a similar reoccurrence, “what you see is all there is” [21]. The reader’s understanding of the event and their opinion of the actors involved is heavily reliant upon the information provided within the accident report and the framing and language used by the accident facilitator.
In this paper, we empirically analyse whether using different metaphors and writing styles to tell the accident story leads the reader to focus on different aspects of the accident report and to propose different solutions. Will the solutions vary in line with the writing style? Will the metaphors used encourage people to reason about the event in a consistent manner with the underlying perception of these metaphors? For example, if we use language which is consistent with how law enforcement describes a crime, will people treat the event in a similar manner to how crime is dealt with in society? Will the focus of the accident analysis facilitator and their chosen facts influence the reader? Or if the event is told in a way which is aimed towards a learning outcome, will the solutions proposed be consistent with the aims of the storyteller?
2. Materials and Methods (A Study of an Accident Report Interpretation (Griffith University Ethics Approval Ref. No.: 2017/839))
2.1. Participants
For this experiment, we used a sample population of 93 people, all of whom work for construction companies. The study was issued to the operational staff members of three different companies and the studies were issued in alphabetical order using each organisation’s distribution list. Our sample population included various sub-populations such as engineers, construction managers, human capital personnel and safety advisors. This allowed us to sample a broad cross section of the production support team. This was necessary as people’s conceptions of workplace accidents may differ depending on their past experiences, their role and their exposure to the accident process.
The data was collected using both paper and online anonymous surveys and there was no incentive to participate. To preserve the confidentiality of the participants, no individually identifiable information, including the participant’s organisation role, was collected.
2.2. Materials
The experiment involved 3 conditions, titled “Report Variants”. Each participant was randomly allocated 1 of 3 accident reports, such that each report was reviewed by one-third (31) of the participants. In each of the 3 reports, participants were presented with a description of an event which had the potential to cause life-altering harm to human life. Each report described the same event. The reports differed in their language, structure and style. Report Variant 1 used a reductionist approach to create a linear story; Report Variant 2 focussed on issues existing within the organisation’s system; and Report Variant 3 focussed on the provision of multiple accounts.
The facts included in the reports used were all taken from a real-life accident. Due to the different report styles used, not all facts are captured in each report. This was natural rather than forced due to the accident report style dictating the information captured and the way it was presented.
Each report information sheet requested the participants to “review an accident report and provide 3 recommendations based on the information provided”. The heading above the 3 blank boxes provided asked the participant to “identify preventative/corrective actions”.
Participants could access the report and submit their response in either paper or electronic format.
2.3. Conditions
2.3.1. Report Variant 1
The search for human error following an accident has long been a goal of many accident analysers. One of the factors which greatly increased the focus on human error following an accident was the event that occurred at Three Mile Island and the use of the label “human error” in the subsequent report [22]. The spotlight on human error within the world of accident analysis intensified in recent decades because of human error-focussed research, such as that of Stanton and Glendon’s work on individual attitudes to risk taking [23]. This led those within the field of accident analysis to place a disproportionate amount of time focussing on human issues and viewing them as the main cause of accidents. Another influencing factor in industry choosing this trajectory for the analysis of accidents was the work of Heinrich, who declared that 88% of all accidents are the result of human error [24]. A key issue with focussing upon the symptoms of human error is the underlying causes which helped create the error are ignored [25], as well as the weaknesses in the organisational and regulatory system which created the environment for the error [26]. These less direct forms of human failure help to establish the working practices that result in operator error [27].
The report used for Report Variant 1 was a real accident report written after an accident occurred on a construction project. It was modified only by removing identifying details. The writing style used by the original report’s author is human-error focussed, with minimal focus on the underlying causes of the errors [Appendix B]. In creating the report, the accident analysis facilitator reviewed the interviews of those involved and selected the information they believed to be relevant to the report.
2.3.2. Report Variant 2
There are many safety researchers who encourage the operational world to move away entirely from a focus on human error and towards a complete system focus. Accidents today are much too complex to understand through traditional accident analysis, which aspired to find individual broken components such as human error [11]. System behaviour cannot be deduced from component behaviour [28] as “simple entities, because of their interaction, cross-adaption and cumulative change, can produce far more complex behaviours as a collective” [29].
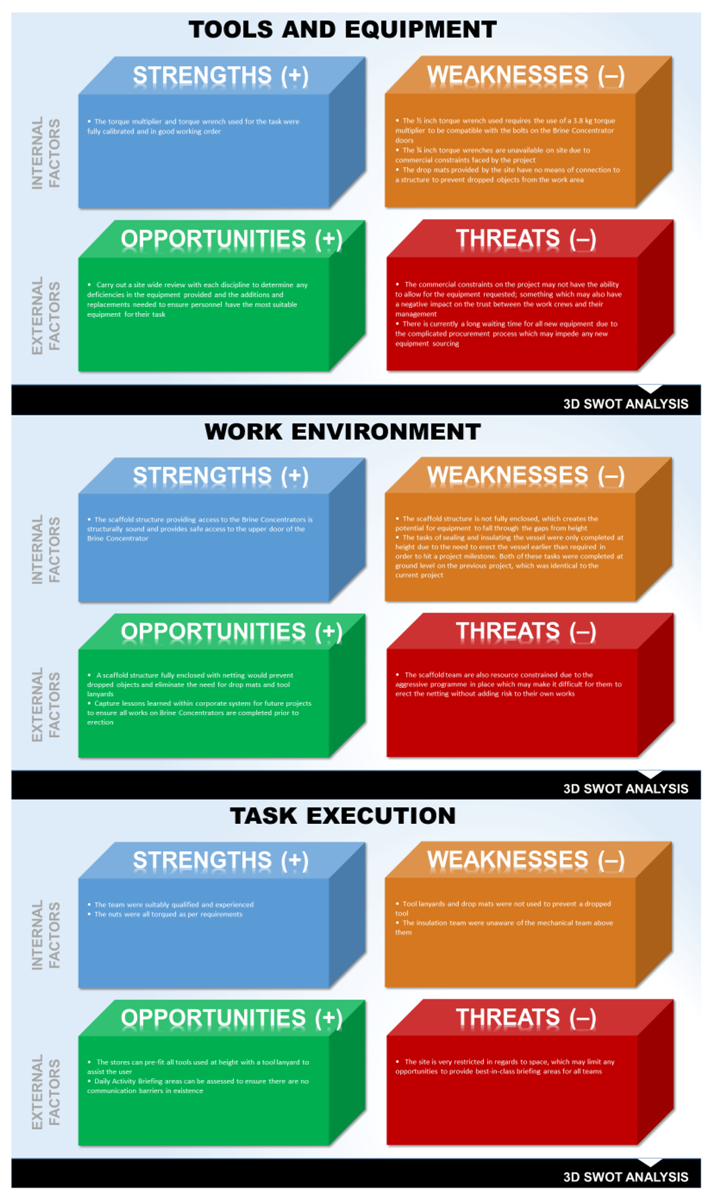
There are many methods used in the world today to analyse accidents using a systems approach. The Functional Resonance Analysis Method (FRAM) [30], Accimaps [3], Systems Theoretic Accident Model and Processes (STAMP) [11] and Strengths, Weaknesses, Opportunities and Threats (SWOT) Analysis are just some of the processes used to better understand complex accidents.
The report used for Report Variant 2 was based on the same accident used for Report Variant 1. This report was written by the first author for this experiment and contains information which was not included in Report Variant 1 because of the writing style chosen. This additional information is also factual. Participants were provided with a one paragraph summary of the accident followed by a SWOT Analysis of the 5 elements deemed necessary to achieve success [Appendix C].
These elements were:
- Daily activity briefing;
- Personnel;
- Tools and equipment;
- Work environment;
- Task execution.
2.3.3. Report Variant 3
Traditionally, accident reports consisted of a singular narrative describing the event. The role of the accident analysis facilitator was to objectively collate the facts related to the event and to provide a story for others to better understand what happened and how. The accident analysis facilitator would choose what they believed to be the important aspects from each statement of those involved in the event and use this information to create a linear story. A key failure in this approach is that it is impossible for the facilitator to avoid hindsight bias using this method, given that they are aware of the outcome of the event. Hindsight allows observers to change past indeterminacy and complexity into order, structure, and oversimplified causality [31]. The facilitator regularly omits background information within each actor’s story from the final report to help create the story they believe to be true. This story is often littered with counterfactuals highlighting what the operators could or should have done. However, saying what people could have done to prevent a specific outcome does not explain why they did what they did [32].
The report used for Report Variant 3 again communicated the same accident as Report Variant 1 and 2. This report, written by the first author for this experiment, used the “multiple stories” approach [Appendix D]. This report, like Report Variant 2, contains information which was not included in Report Variant 1 because of the writing style chosen. This additional information is also factual. Each actor’s account was recounted verbatim in the final report to ensure everyone’s voice was heard, whether conflicting or not, and this became the accident report. The issues and constraints faced by those involved and captured in their story were listed as contributing factors to the accident.
3. Results
Overall, there were 298 corrective actions proposed by the participants across the 3 conditions; 99, 100 and 99.
3.1. Coding
Proposed corrective actions were coded into 2 categories: (1) Human/blame-focussed; and (2) system-focussed. Each category was further broken down into sub-categories. Human/blame-focussed was divided into the following elements: (1) punish the people involved; (2) non-punitive action focussed on the people involved (e.g., training, reinforcement of correct behaviour). System-focussed was divided into the following groups: (1) one-off actions such as communicating about the accident or reviewing the risk register considering the accident; (2) changes to the physical workplace; (3) reinforcement or change to the work practices specifically involved in the accident; (4) reinforcement or change to practices not directly involved in the accident; and (5) changes to documents. A separate category was provided for any counterfactual statement found. This category was then separately coded using the 2 main categories.
Each participant’s response was weighted equally—as a single point towards the analysis.
Participants’ corrective action suggestions were coded blindly by two coders. Cronbach’s Alpha—a measure of reliability—was 0.957759, indicating good agreement between the coders. The coding made by the first author was used for the remainder of the analysis.
3.2. Findings
Overall, participants were more likely to propose system-focussed corrective actions (255 actions, 86.44%) than human error-focussed (40 actions, 13.56%). However, the actions participants proposed to manage the issues which led to the accident varied greatly depending on the style of the report, the framing of the story and the language used to describe the event. Participants provided with the traditional approach report were more likely to suggest actions with a human error/blame-focus (27 actions, 27.55%) than those provided with the systems approach report (8 actions, 8%) or the multiple stories approach (5 actions, 5.15%) reports, χ2 = 25.39, p < 0.001, see Figure 1.
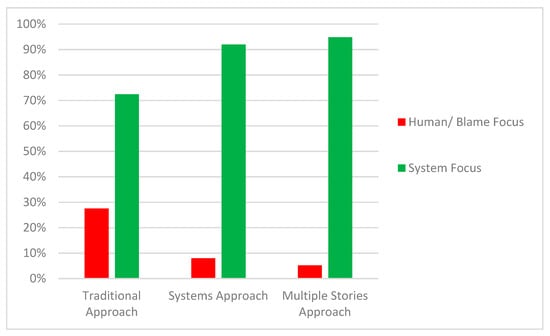
Figure 1.
The figure above displays the percentage of human/blame-focussed recommendations against the percentage of system-focussed recommendations provided for each report variant.
As seen in Table 1, readers of Report Variant 1 were the only participants from all 3 reports who requested punishment for the individuals involved (4 actions, 4.04%).

Table 1.
The table below displays the distribution of accident classifications across the 3 report variants.
Appendix A contains examples of the recommended actions in each classification.
4. Discussion
4.1. Interpretation of Results
The results show that participants presented with Report Variant 1 were more likely to recommend actions that are directed at front-line operators than participants presented with Report Variants 2 and 3. Only readers of Report Variant 1 chose punishment as an action. Although the number of such cases is small (4), it is significant that none of the readers of Report Variants 2 or 3 chose this type of action.
In terms of reaching a conclusion from our results, there are 3 possibilities:
- The results are random and do not mean anything.
- Different information within each report influenced the participants.
- Different styles used to present the story influenced the actions decided upon.
The reports were issued to a wide range of individuals each of whom operate within a specific discipline in the construction organisation. Each participant will have had some form of exposure to a workplace accident prior to participation in this study as all of the disciplines were chosen based on their exposure and influence upon the accident process within the organisation. The results, rather than having been influenced by the style or language of the reports, may have been instead dependent on the reader’s personal opinion of accident causation and the type of action required following any event. The reader may have used their previous knowledge and experience to assess the information provided and chose their actions accordingly. The actions which were human and punishment-based may have been chosen by the participants who believed their selected actions would help the organisation and the people involved. It may have been by chance that many of the participants who believe a focus on the human is beneficial received Report Variant 1 rather than Report Variant 2 or 3.
When carrying out these type of experiments, a participant’s past experience and their personal beliefs will have some form of influence upon their decisions and actions. For example, a reader may see similarities between the accident report information and a previous accident they were involved in and decide upon similar actions because they believe these actions were successful previously. The participant’s beliefs may also play a role. A person’s beliefs are shaped by society, religion and previous experience. It is a strongly held belief among many that a mistake which did or could have caused serious harm requires retributive action to ensure the human involved pays what they owe.
Whilst past experience and personal beliefs may indeed affect decision making, this is insufficient to explain the results. Out of the 3 reports, only Report Variant 1 is human error-focussed. This report was also the only report to be provided with actions that recommended the use of punishment. Although the number of punishment recommendations was small, this is still statistically significant. Were the results truly random and based only on past experience and personal beliefs, there would be a high likelihood that the human-focussed actions would be more evenly distributed or higher in Report Variants 2 or 3 as opposed to Report Variant 1.
Report Variants 2 and 3 both have background information provided within them that does not appear within Report Variant 1. The provision of these additional opinions and facts may have helped sway their readers’ focus from the individuals involved towards system fragilities. Conversely, had this information been provided within Report Variant 1, the number of actions focussed on the front-line operatives may have dramatically decreased, as the reader would have been given a more comprehensive picture of the accident and the reasons why people did what they did.
Report Variants 2 and 3 did have additional background information provided in several areas where Report Variant 1 did not. A key reason for this is that the accident report style chosen dictates the content of the report. The style of Report Variant 1 is heavily reliant on the accident facilitator’s perception and interpretation of “important” facts. Given that as humans we are naturally susceptible to hindsight and confirmation bias when analysing past events, the style of Report Variant 1 makes it more vulnerable to omitted information than Report Variants 2 or 3, as any conflicting information creates a choice for the facilitator to ensure a linear story is achieved. As the key goal of Report Variant 1 is to put forward the proven facts as the facilitator sees them, the background information captured within Report Variants 2 and 3 is often written off as opinion and hearsay. Reports based on provable facts can help an organisation understand what happened, but they are far less effective in helping us understand why. Human error is easy to “prove” in hindsight and with the help of post-accident procedure reviews, whereas problems within a system can be much more difficult to label as “broken” because often system issues exist among a variety of systems that are individually working as designed. It is only their interactions with other systems that are creating the unmanaged risk.
The accident is presented in 3 very different styles. Report Variant 1 prioritises facts and minimises any background information deemed irrelevant by the author. Report Variant 2 delves into different facets of the system and the elements that were successful against those which were creating unmanaged risk. Report Variant 3 seeks to allow the various actors involved in the accident to be heard to ensure the reader has a full understanding of what happened and the constraints faced by each of the actors. The report style chosen has influenced the focus of attention. Report Variant 1, due to its focus upon what went wrong, places a strong focus upon the front-line operatives which may have led to the some of the report’s readers to decide that the accident was the result of careless workers. With Report Variant 2, the focus migrates from the human to the system. The description of the issues found are more focussed on the “what” than the “who”. This in turn may have led the reader to provide actions based around what needs rectification, rather than who. Like Report Variant 2, Report Variant 3 ensures the human is not the focus of attention. Each actor’s story, and the constraints they faced leading up to the accident, is heard in full to ensure these people are understood and the reader gains a deep understanding of the world these people operated within at the time of the event.
Although these reports are related to the same accident, each of them has slightly different objectives. Report Variant 1 uses a reductionist-style approach to find the broken parts that caused the accident and to fix them. Each fact is assessed against the safety management system to determine whether it is “broken” or not. This creates a binary view of the accident and the actions of those involved. This in turn can lead to a “guilty” or “not guilty” description of the actions of those involved. Report Variant 2 focuses solely upon the system and the various relationships and issues that exist within it. A human mistake is viewed as something that has been caused by a bigger issue which exists within the system. In a similar manner to Report Variant 1, this report can transform what began as an accident which was highly personal to all of those involved into an objective, lifeless narrative which fails to capture the mindset of the accident’s actors. Report Variant 3 is focussed upon allowing the actors to be heard so that any damage suffered by them can be healed through the disclosure of their story. The front-line operatives are viewed as victims who require support. These differences in objectives can have a substantial impact on the type of actions determined by the reader. One of the consequences of the different styles of reporting is both the author and the reader being drawn to different information. Report Variant 1 is over-reliant on the author needing to view information sourced from those involved in the accident as important for it to be included within the final report, whereas Report Variant 3 is much less reliant on the author’s own views and is accepting of contradictory facts without resolving to a single conclusion. This highlights how careful organisations need to be when selecting their accident report style and whether the style aligns with their objectives. The results of our study suggest that information viewed as unimportant, not relevant or otherwise by the report’s author, can have serious implications for those involved in accidents and the ability for the organisation to learn from its mistakes.
A limitation of this study is the fact that it was conducted in abstract, as the participants were engaged in an experiment rather than a real accident review. This creates the potential for participants to respond differently to how they would respond to an accident report within their workplace because of the removal of any socio-political aspects which may exist in their organization.
4.2. Implications for Practice
The findings in this study suggest that the accident report style and model selected by an organisation or the accident analysis facilitator to analyse the accident can have a significant impact on the outcomes of the accident analysis. This has important implications for any organisation seeking to achieve a “just” culture. The accident process is a core element in establishing and maintaining a learning culture within an organisation. Learning from accidents, particularly those with serious consequences, often influences an organisation’s future safety strategy. The treatment of those involved in accidents can create or destroy the foundation of trust needed to support a positive reporting culture and the sharing of critical information within an organisation. Facilitators of accident analyses must accept that the accident report style chosen has serious implications for those involved and the future ability of the organisation to learn. Our results suggest that the pursuit of a linear report based only on facts determined as important by the author may increase the potential for recommended actions to be blame-focussed and impede the organisation from dealing with more serious issues which have been deemed irrelevant by the author. The omission of background information provided by the actors involved in the event from the final report can have severe repercussions for these actors and for future reporting within the organisation.
This study raises legitimate concerns that researchers need to do more work in the area of accident analysis to provide better advice to safety practitioners in future. As with accident reports themselves, readers should take care in under or over interpreting the results from this study. The results are strongly suggestive that accident report style influences accident analysis outcomes—but alternate interpretations can be drawn from the results. Further work is needed to establish conclusive relationships between the facts, methods, styles and outcomes of accident reporting.
Author Contributions
For this research article, members of the research team made the following contributions; Conceptualisation—D.H., A.R. and S.D.; Methodology—D.H., A.R. and S.D.; Resources—D.H.; Data Curation—D.H.; Formal Analysis—D.H. and A.R.; Writing—original draft preparation—D.H.; Writing—review and editing—A.R.; Supervision—A.R. and S.D.
Funding
This research received no external funding.
Acknowledgments
The authors would like to thank Martin Westbury, Robert Jordan, Stuart Griffiths, John Phillips, Russell Lang and Alex McTaggart for their support in achieving this study.
Conflicts of Interest
The first author is an employee in one of the organisations in which the research was carried out. To minimize any risk associated with this, the second author provided oversight and all data collected was classified independently by both authors before being tested using Cronbach’s Alpha.
Appendix A. Examples of Recommendations Made by the Participants
Table A1.
Examples of human-focussed recommendations.
Table A1.
Examples of human-focussed recommendations.
| Report Variant | Classification | Recommended Action |
|---|---|---|
| 1 | Punish the people involved | Disciplinary action against supervisors for improper briefing |
| 1 | Punish the people involved | Immediate dismissal of mechanical crew |
| 1 | Non-punitive action focussed on the people involved | Training/re-briefing to teams on working procedures |
| 1 | Non-punitive action focussed on the people involved | Brief/retrain operatives to comply with approved Risk Assessment and Method Statement (RAMS). Brief/retrain supervisor on is duties to ensure compliance with RAMS i.e., Correct equipment available, fit for purpose, ensure operatives understand and comply |
| 2 | Non-punitive action focussed on the people involved | Better training or the appropriate tools for the task |
| 2 | Non-punitive action focussed on the people involved | Provide adequate training to update existing skills |
| 3 | Non-punitive action focussd on the people involved | Point of Work Risk Assessment (POWRA)—retraining is required. A POWRA should only be done at the point of work. If done correctly the lack of correct tools, unsuitable mats, not used lanyards and incomplete scaffold—this should have prevented the job being started until all these aspects were solved |
Table A2.
Examples of system-focussed recommendations.
Table A2.
Examples of system-focussed recommendations.
| Report Variant | Classification | Recommended Action |
|---|---|---|
| 1 | Reinforcement or change to the work practices specifically involved in accident (in this protecting against dropped tools) | Given the scope of the overall works, all tools should be fitted with lanyards and their use made compulsory with recorded training given to all operatives |
| 1 | Change to induction training | Reinforcement or change to practices not directly involved in the incident (e.g., toolbox talks, site coordination, competency management) |
| 1 | Changes in documents | HOLD POINT in RAMS. Appointed supervisory staff (person in charge) should check and confirm risk assessments have been read, that all safeguards and risk prevention/mitigation measures are in place prior to the work commencing (mats, nets, barriered impact areas below, lanyards, tools), and are signed off before commencement, especially high risk and safety critical works. |
| 2 | Reinforcement or change to the work practices specifically involved in accident (in this protecting against dropped tools) | Competent scaffold inspection should be done weekly |
| 2 | Reinforcement or change to practices not directly involved in the accident (e.g., toolbox talks, site coordination, competency management) | Introduce pre-start briefs between different trade team leaders to achieve better communication |
| 2 | Changes to the physical workplace | Adequate protection of assets should be applied to equipment |
| 3 | Reinforcement or change to the work practices specifically involved in accident (in this protecting against dropped tools) | Apply exclusion zones below teams working on scaffoldings. Rotate teams working so that always an area is available to work. Tag scaffolds when complete and safe to use, install signage, improve communication |
| 3 | Reinforcement or change to practices not directly involved in the accident (e.g., toolbox talks, site coordination, competency management) | Managers to re-consider commercial embargos when relates to safety as low costs that are avoided might cause great losses following an accident |
| 3 | One-off actions such as communicating about the accident, or reviewing the risk register considering the accident | Use this adverse event to highlight to management the potential consequences that upstream commercial/programme decisions can have on downstream operations—introduces additional variables—“blindsided” |
Table A3.
Examples of counterfactual recommendations.
Table A3.
Examples of counterfactual recommendations.
| Report Variant | Counterfactual Classification | Recommended Action |
|---|---|---|
| 1 | Human | Workers should have used the tool lanyards |
| 1 | System | Have the correct tools for the job. If the correct sized torque tool been available there would have been no need for the torque multiplier. This would have meant that there would only have been a single tool for Jim to work with, reducing the chance of dropping it |
| 2 | Human | Badly layed out platform/work area |
| 2 | System | Money was a problem which led to corners being cut |
| 3 | Human | Rushing, lack of communication, badly briefed, bad supervision, briefings should have been held in a better place |
| 3 | System | Change the culture associated with safety paperwork. Both operatives stated that the POWRA would be used ‘against them’ if something went wrong. POWRA are there to prevent accidents, not apportion blame. Form should have also been amended to reflect the actual method of work |
Appendix B. Accident Report 1 (All Names Used in These Reports Have Been Falsified to Provide Anonymity for Those Involved in the Real-Life Accident That Forms the Basis of This Study)
| Incident/Incident No.: | 11111 | Incident Date: | 22-09-2017 | ||||||
| DETAILS OF PERSONS INVESTIGATING INCIDENT | |||||||||
| Team Leader Name | John Smith | Position | Project Safety Manager | Contact No. | 555-1234 | ||||
| Team Leader Name | Peter Parker | Position | Senior Safety Advisor | Contact No. | 555-2345 | ||||
| BASIC INCIDENT DETAILS | |||||||||
| Incident Date (dd/mm/yy) | 22-09-2017 | Incident Time (24 h) | 09:00 a.m. | ||||||
| Incident Site Address | London | ||||||||
| Location of Incident on Site | Brine Concentrator 1 | ||||||||
| Person Responsible for Workplace | Mark Masterson | ||||||||
| Step 1: Incident Level Classification | |||||||||
| Actual Injury | The class of actual injury was—Nil | ||||||||
| Potential Injury | The maximum reasonable potential class of injury was—High | ||||||||
| STEP 2: Observation/Information Gathering | |||||||||
| Instructions for Gathering Information Our first priority is to understand the incident and how the damage was sustained.
| |||||||||
| List of Persons Involved (Full name and contact phone number) | |||||||||
| Name | Contact Phone | Position | Employer | Witness | Statement Attached | ||||
| Yes | No | Yes | No | ||||||
| Jim Johnson | 555-3456 | Mechanical Fitter | Perfect Construction Ltd. | ⊠ | ☐ | ⊠ | ☐ | ||
| Ben Benson | 555-4567 | Mechanical Fitter | Perfect Construction Ltd. | ⊠ | ☐ | ⊠ | ☐ | ||
| Lionel Leslie | 555-5678 | Cladding Specialist | Superior Insulation | ⊠ | ☐ | ⊠ | ☐ | ||
| Mike Michaels | 555-6789 | Mechanical Supervisor | Perfect Construction Ltd. | ☐ | ⊠ | ⊠ | ☐ | ||
| Clive Conlan | 555-8901 | Scaffold Working Supervisor | Perfect Construction Ltd. | ⊠ | ⊠ | ☐ | ☐ | ||
| STEP 3: Give a DETAILED DESCRIPTION of the incident | |||||||||
| On Friday the 22nd of September 2017 at the 07:30 a.m. Daily Activity Briefing (DAB), Mike Michaels, the Mechanical Supervisor, tasked Jim Johnson and Ben Benson with carrying out works at the top of Brine Concentrator 1. It was also addressed by Mike Michaels at his pre-start that Superior Insulation would be working in the same area, though the workers associated with the incident later reported that they did not hear this advice. | |||||||||
 Brine concentrator 1. | |||||||||
| Jim and Ben set off after their DAB to get the tools required for their task, which was to torque the bolts to the flange on the man way covers on BC1. Once they had acquired the torque wrench that they required for their task, they proceeded back to the base of BC1. They then went their separate ways as Jim went to the Main Process Building in order to get a torque multiplier and Ben went down to the Lime Silos in order to get tool lanyards for their task. These lanyards were items that he owned. They were not issued by the stores. Jim stated that he would have preferred to use a ¾ inch drive torque wrench but there were only ½ inch drive torque wrenches available. ¾ inch drive torque wrenches were requested but were unavailable due to commercial reasons. This then necessitated the requirement to use a torque multiplier. | |||||||||
 Torque multiplier. | |||||||||
| Once they had both collected their required tools, they again reconvened below BC1 where they met Steve Stevenson from UK Gas Ltd., who was there to carry out a visual inspection to confirm the cleanliness of the flood box inside BC 1. They received Clive Conlan’s permission by radio for access to BC1 before making their way to the top of BC1; as read by the access procedure in force. Ben Benson saw Superior Insulation workers working on the scaffold as he was walking up to his work area and he never communicated to them that he would be working above them. Once Jim Johnson, Ben Benson and Steve Stevenson reached the top floor, they showed Steve the inside of the BC before closing up the door. Steve then left the area. | |||||||||
 Brine concentrator door. | |||||||||
| Both Jim and Ben commenced work on the door. The nuts, bolts and washers were installed and hand tightened. The bolts on the door way were then numbered sequentially. Ben took the torque multiplier from its box, carried out some required calculations, set the tool up and then handed the tool to Jim. Jim then placed the multiplier over nut number 1. He asked Ben to hand him the torque wrench. It was at this moment that he knocked the multiplier off of the bolt and it bounced on the scaffold before falling 8 floors (16 m) below. There had been no lanyard on the tool and no drop mats in place, despite the worker’s Point of Work Risk Assessment (POWRA) highlighting both of these controls. The lanyards had remained in Ben Benson’s bag, which was at the work front. There was also the fact that Ben Benson did not sign onto the task POWRA. | |||||||||
 Work area with visible gaps. | |||||||||
 Damage to brine concentrator—post-impact. | |||||||||
| No catch net had been taken from the stores up to the work front. The tool that fell weighed 3.8 kg and hit with a force of approximately 607 kg, based on subsequent calculations. After the event, Ben proceeded down the scaffold stairs before finding the tool 8 floors below. It was lying next to the Superior Insulation crew. At the time of the event, they had been standing approximately 3 m away. Once Ben had seen that Superior Insulations’ workers were not injured, he alerted Jim, who came down and apologized. Jim then called Mike and alerted him of the incident. Once Mike arrived, he secured the scene before calling the site Safety Manager. John Smith then began an investigation. Both workers returned negative results when drug and alcohol tested. | |||||||||
| STEP 4: BASIC LEVEL INCIDENT ANALYSIS | |||||||||
| 1. List Elements List the “people”, “equipment”, and “environment” elements involved in the incident | |||||||||
| PEOPLE | EQUIPMENT | ENVIRONMENT | |||||||
| Jim Johnson | Norbar Torque Wrench Multiplier HT3 3/4 | Time | 09:00 a.m. | ||||||
| Ben Benson | Torque Wrench | Lighting | Good | ||||||
| Lionel Leslie | Tool Lanyards | Climate | Warm | ||||||
| Mike Michaels | - | - | - | ||||||
| Justin James | - | - | - | ||||||
| Clive Conlan | - | - | - | ||||||
| Kevin Kelvin | - | - | - | ||||||
| 2. List Factors For each element listed above identify essential and contributing factors based on the focussing questions in the left-hand column. Essential = Factor is essential for damage to occur. Contributing = Factor increases the likelihood damage occurs but removal may not interrupt incident | |||||||||
| ESSENTIAL AND CONTRIBUTING FACTORS | |||||||||
| Both superior insulation and the mechanical crew were told at the daily activity brief that there would be other work crews in their area but they advised that this message had not been heard by them. | |||||||||
| The mechanical crew did not communicate with the superior insulation crew before carrying out works above them. | |||||||||
| The workers stated on their POWRA that drop mats and tool lanyards were required but these controls were not implemented. | |||||||||
| The workers had the tool lanyards at the job front but did not use them. | |||||||||
| The RAMS stated the requirement for drop mats when working at height. | |||||||||
| The most suitable tool for the task, a ¾ torque wrench, was unavailable to the workers at the time of the incident. | |||||||||
| 3. List Recommendations From the effectively controllable factors, identified above, list corrective/preventative actions to manage this incident into the future. | |||||||||
| CORRECTIVE/PREVENTATIVE ACTIONS REQUIRED | |||||||||
| 1 | - | ||||||||
| 2 | - | ||||||||
| 3 | - | ||||||||
Appendix C. Accident Report 2
| Exploration No.: | 11111 | Accident Date: | 22-09-2017 | ||||||
| DETAILS OF PERSONS EXPLORING ACCIDENT | |||||||||
| Team Leader Name | John Smith | Position | Project Safety Manager | Contact No. | 555-1234 | ||||
| Team Leader Name | Peter Parker | Position | Senior Safety Advisor | Contact No. | 555-2345 | ||||
| BASIC ACCIDENT DETAILS | |||||||||
| Accident Date (dd/mm/yy) | 22-09-2017 | Accident Time (24 h) | 09:00 a.m. | ||||||
| Accident Site Address | London | ||||||||
| Location of Accident on Site | Brine Concentrator 1 | ||||||||
| Person Responsible for Workplace | Mark Masterson | ||||||||
| Step 1: Accident Level Classification | |||||||||
| Actual Injury | The class of actual injury was—Nil | ||||||||
| Potential Injury | The maximum reasonable potential class of injury was—High | ||||||||
| STEP 2: Observation/Information Gathering | |||||||||
| Instructions for Gathering Information Our first priority is to understand the accident and how the damage was sustained.
| |||||||||
| List of Persons Involved (Full name and contact phone number) | |||||||||
| Name | Contact Phone | Position | Employer | Witness | Discovery Sessions Attached | ||||
| Yes | No | Yes | No | ||||||
| Jim Johnson | 555-3456 | Mechanical Fitter | Perfect Construction Ltd. | ⊠ | ☐ | ⊠ | ☐ | ||
| Ben Benson | 555-4567 | Mechanical Fitter | Perfect Construction Ltd. | ⊠ | ☐ | ⊠ | ☐ | ||
| Lionel Leslie | 555-5678 | Cladding Specialist | Superior Insulation | ⊠ | ☐ | ⊠ | ☐ | ||
| Mike Michaels | 555-6789 | Mechanical Supervisor | Perfect Construction Ltd. | ☐ | ⊠ | ⊠ | ☐ | ||
| Clive Conlan | 555-8901 | Scaffold Working Supervisor | Perfect Construction Ltd. | ☐ | ⊠ | ⊠ | ☐ | ||
| STEP 3: Give a DETAILED DESCRIPTION of the accident | |||||||||
| On Friday the 22nd of September 2017, a work crew were sealing a door closed on a Brine Concentrator (BC) via a scaffold structure 30 m high when the torque multiplier being used to torque the bolts dropped through a gap in the scaffold structure to an area 16 m below. The object struck the BC vessel approximately 3 m from an insulation team’s work area. | |||||||||
| Brine concentrator 1. | |||||||||
| Torque multiplier. | |||||||||
| Brine concentrator door. | |||||||||
| Work area with visible gaps. | |||||||||
| Damage to brine concentrator—post-impact. | |||||||||
| SWOT Analysis | |||||||||
  | |||||||||
| CORRECTIVE/PREVENTATIVE ACTIONS REQUIRED | |||||||||
| 1 | - | ||||||||
| 2 | - | ||||||||
| 3 | - | ||||||||
Appendix D. Accident Report 3
| Exploration No.: | 11111 | Accident Date: | 22-09-2017 | ||||||
| DETAILS OF PERSONS EXPLORING THE ACCIDENT | |||||||||
| Team Leader Name | John Smith | Position | Project Safety Manager | Contact No. | 555-1234 | ||||
| Team Leader Name | Peter Parker | Position | Senior Safety Advisor | Contact No. | 555-2345 | ||||
| BASIC ACCIDENT DETAILS | |||||||||
| Accident Date (dd/mm/yy) | 22-09-2017 | Accident Time (24 h) | 09:00 a.m. | ||||||
| Accident Site Address | London | ||||||||
| Location of Accident on Site | Brine Concentrator 1 | ||||||||
| Person Responsible for Workplace | Mark Masterson | ||||||||
| Step 1: Accident Level Classification | |||||||||
| Actual Injury | The class of actual injury was—Nil | ||||||||
| Potential Injury | The maximum reasonable potential class of injury was—High | ||||||||
| STEP 2: Observation/Information Gathering | |||||||||
| Instructions for Gathering Information Our first priority is to understand the incident and how the damage was sustained.
| |||||||||
| List of Persons Involved (Full name and contact phone number) | |||||||||
| Name | Contact Phone | Position | Employer | Witness | Statement Attached | ||||
| Yes | No | Yes | No | ||||||
| Jim Johnson | 555-3456 | Mechanical Fitter | Perfect Construction Ltd. | ⊠ | ☐ | ⊠ | ☐ | ||
| Ben Benson | 555-4567 | Mechanical Fitter | Perfect Construction Ltd. | ⊠ | ☐ | ⊠ | ☐ | ||
| Lionel Leslie | 555-5678 | Cladding Specialist | Superior Insulation | ⊠ | ☐ | ⊠ | ☐ | ||
| Mike Michaels | 555-6789 | Mechanical Supervisor | Perfect Construction Ltd. | ☐ | ⊠ | ⊠ | ☐ | ||
| Clive Conlan | 555-8901 | Scaffold Working Supervisor | Perfect Construction Ltd. | ☐ | ⊠ | ⊠ | ☐ | ||
| STEP 3: Give a DETAILED DESCRIPTION of the accident | |||||||||
| On Friday the 23rd of September 2017, the door of a Brine Concentrator was being secured with nuts when an accident occurred where the tool being used, a torque multiplier weighing 3.8 kg, slipped from the nut it was being used to tighten and fell through a gap in the scaffold deck onto a level 16 m below, where a team on insulators were carrying out works. Below are the accounts of those involved: Jim Johnson—Mechanical Fitter At our morning briefing, Mike, our supervisor, tasked Ben and I with helping Steve from UK Gas Ltd. carry out an inspection of the inside of Brine Concentrator (BC) 1 prior to its top entrance being sealed. Steve, who was also attending our briefing, said that he would meet us at the BC 1 gate at around 08:30 a.m. Apparently Mike also told us at the briefing about Superior Insulation also working on BC1 on a lower level than us but I definitely didn’t hear that. In saying that, that doesn’t mean he didn’t say as it wouldn’t be the first time we didn’t hear some of Mike’s announcements due to that stupid generator running right behind our briefing area. | |||||||||
| Brine concentrator 1. | |||||||||
| Once the briefing was over, Ben and I headed over to the stores to get the gear we needed to carry out the job. We were only able to get the ½ inch drive torque wrench from Al the store man as all of the torque multipliers were in the field. Really and truly, what we really needed was a ¾ inch drive torque wrench for this kind of job as this would have meant not having to use a heavy and awkward torque multiplier at height. Unfortunately, when we asked about buying some, Mike told us that the financial problems faced by the project meant that there was a freeze on buying any new equipment which meant we just had to make do with what we had. Without the torque multiplier, there was no way of doing the job but luckily enough I knew one of the guys who had one out from the stores. | |||||||||
| Torque multiplier. | |||||||||
| Ben and I headed over to the BC1 gate to drop off the torque wrench at the base. While there, we also carried out our Point of Work Risk Assessment (POWRA) to get it out of the way. I then headed off to the Main Process Building (MPB) to borrow the torque multiplier for the job while Ben headed to the Lime Silo area as he had left his tool lanyards down there the day before when we were down there installing the internal hopper. By the time we both got back to BC1, Steve from UK Gas was waiting on us at the gate. Before entering, we were required to gain permission from the area owner, who at the time was Justin James, the Scaffold Superintendent. Justin being the area owner, created 2 problems:
Steve, armed with a torch, stepped into the vessel and carried out his inspection. After giving us the thumbs up, Steve headed off back down the scaffold stairs. We were glad to get the inspection out of the way as it was a BC1 hold point and we were already a week behind program already and the milestone only round the corner in November. With Steve now gone, Ben and I gave the POWRA a final look to ensure we didn’t miss anything we could be pinged for afterwards. We did write down the use of rubber mats to prevent dropped objects but the problem we had was the site bought cheap mats which are useless in preventing a dropped object because they don’t have the metal rings that the good ones have which allow you to connect them to a railing. Anything that hits the site mats just falls through as the mat isn’t secured. To be honest, on any other job I’ve been on that has a lot of working at heights on a scaffold, the scaffold is usually fully insulated with netting to prevent anything from dropping. We then pushed the door of the BC shut and set up our work area, with the tools well away from the gaps in the scaffold. We first placed all of the nuts on the door bolts. This was a job that we had to be really careful with as one slip of the finger could have meant a nut dropping to the floors below. | |||||||||
| Brine concentrator door. | |||||||||
| Once all the nuts were on and numbered correctly, we moving to the torque phase. I was lead and Ben was support. Ben handed me the torque multiplier and I placed it carefully on the bolt number 1. I never even noticed that it didn’t have a lanyard attached. Ben then handed me the torque wrench but as he did, my other arm made contact with torque multiplier and it slipped from the nut and fell below. I froze for a second while Ben ran down the scaffold to see where it landed. After a few seconds I came to my senses when I heard shouting from below. | |||||||||
| Work area with visible gaps. | |||||||||
| I ran down the scaffold stairs and found Ben 6–7 floors below talking to the Superior Insulation guys who looked in shock. The torque multiplier had landed only yards from where they were working but luckily no one was hurt. I apologies profusely for my mistake to the guys. I then called Mike and told him about the accident. Mike arrived a few minutes later and secured the scene before calling John, the Safety Manager. Once John came, Ben and I were sent for D and A tests and sat in a room waiting on you. | |||||||||
| Damage to brine concentrator—post-impact. | |||||||||
| Ben Benson—Mechanical Fitter We started off our day at our morning briefing with Mike, our supervisor. Jim and I were given the task of babysitting Steve from UK Gas while he inspected the inside of BC1. We were then to immediately secure the door and torque the bolts. The issue we immediately saw was the bolts on the door needed a ½ inch drive torque wrench but we only had ¾ inch drive torque wrenches. The reason for this was because site refused to buy them due to additional costs and the current buying freeze due the project loosing shit loads of money. We met Steve from UK Gas after the briefing and we agreed to meet at the BC1 access gate at 08:30 a.m. We then headed off to the stores to get our torque wrench and a torque multiplier. When we got there, Al the store man told us that he was all out of torque multipliers but he had the ¾ inch torque wrench. Luckily, Jim knew that Mark in the MPB had one and, since Mark owed him a few favours by now, he would use this to cash one in. I didn’t bother getting any tool lanyards from Al as the quality of his were poor and my own, which were in the Lime Silo area, were much more suitable for holding a 4 kg tool in place. When we had gotten what we needed from Al, we walked back to the BC1 gate and dropped off the torque wrench and wrote up our POWRA for the planned job. Jim then headed towards the MPB to collect his torque multiplier while I headed to the Lime Silos to collect my tool lanyards. While down at the Silos I also saw the rubber mats I had used for the job we had done there the day before on the hopper. I didn’t bother bringing them with me as they were useless in stopping anything from dropping as they had no way of securing them to anything. Jim and I reconvened at the BC1 gate where Steve from UK Gas was now waiting for us. We tried calling Justin, the area owner, but as usual he didn’t answer. Jim then called Clive, his blue hat, and he came over and allowed us in. The usual protocol is for the area owner to walk out the task with the guys before authorizing but poor Clive clearly didn’t have time for this as his scaffold team was behind. The milestone targets that were agreed for these BCs were ridiculous which meant that everybody was chasing their tail trying to hit dates they never agreed to in the first place. Jim and I, with our tools with us, headed up the scaffold with Steve. We walked past Superior Insulation but at the time I never even noticed that they were there. Once we reached the BC door, Steve gave the inside of the BC a swift inspection before giving us the thumbs up and heading off. As always, we gave the POWRA a quick once over to ensure we hadn’t missed anything that could be used against us later. In hindsight, I probably should have removed the rubber mats from it but it didn’t cross my mind at the time. We set up our work space so that there was minimal movement for us to do. We were well aware of the gaps in the scaffold so we had to keep all of our gear well away from these. Instead of leaving the bucket of nuts under Jim while he placed them, we kept them beside me behind him and I handed them to him. A bucket of nuts falling through a gap can cause a lot of damage! When all the nuts were placed and numbered, Jim asked me to hand him the torque multiplier. I instinctively reached for it and handed to him. He carefully placed it on bolt number 1 before reaching back for the torque wrench I was about to hand him. It was then I heard a noise and Jim said “oh shit”. I looked to where the multiplier was and all that was left was the bolt and nut and then we heard a bang. My first thought was, “I forgot to put the lanyard on the multiplier.” The only reason I can think of that caused this was fatigue. Due to manpower shortages, I worked through my last R&R and Friday was my 19th day straight on site and these 12 h days take their toll. I instinctively ran down the stairs and about 7 rows down I found the tool lying beside the Superior Insulation guys, who up until that point, I didn’t even know were there. They were both quite ashen faced and when I asked them if they were ok, all I got was a mumble. I looked around at the BC and saw a big dent where the tool had made contact. Jim came down after me and when he saw the Superior Insulation guys he apologized profusely. He then rang Mike to come down. When Mike arrived, he had a look at what happened and had a quick chat with the insulation guys to ensure they were ok. He then rang John, the Safety Mgr., to come down and have a look. When John arrived, Jim and I were sent for D and A. Mike Michaels—Works Supervisor As usual, we started off with our morning brief. I gave all the boys their tasks and I asked if there were any issues from the previous day. The only issue raised was the noise of the generator behind us and how it made it difficult to hear what I was saying. Unfortunately, this was the only area we could use for the briefing and the generator was required to run 24/7 to power the welfare facilities. I then ran through the areas where there was specific risk. One of them was the Superior Insulation boys working a few floors under Jim and Ben. After the briefing was over, I headed over to the induction room to meet my 2 new starters. We’re under manned at the moment and I’m finding it impossible to hit the targets set by Project Controls, (none of whom have ever built a treatment plant). The new starters were badly needed but it meant half my day was going to be taken up with getting them the basics so they could work onsite. I got a phone call around 9 a.m. about the accident. I went over straight away to see how bad it was. When I arrived, I saw that it was pretty bad. Jim’s torque multiplier had fallen through a scaffold gap and landed 8 floors below near the Superior Insulation guys. When I saw what had happened and how it had happened, I was angry. The original design of the scaffold structure included the requirement for the scaffold to be fully meshed and with drop nets to cover the gap between the scaffold and the BC. This never got done because the scaffold team is under resourced and they were told to move to BC2 as soon as the basic scaffold structure was erected to ensure we hit the milestone. The milestone is the 1st of November and if we don’t hit it, the project loses out on £20 million. The tool which dropped should never have had to be used either. You only have to use a multiplier when the torque wrench being used doesn’t suit the bolt being torqued. The boys asked me for ½ inch drive torque wrenches months ago but when I put in the purchase order, it was rejected because our corporate commercial team had put a freeze on the ordering off new equipment due to the money being lost on the project. After a chat with the insulation boys to see if they were ok, I rang John Smith, the Safety Mgr. and told him what had happened. He came down shortly afterwards and assessed the area. He then sent Jim and Ben away for D and A while I rang Mark, the Project Director and told him the bad news and that his BC works would be delayed. Lionel Leslie—Cladding Specialist I attended Mike’s morning briefing and listened as he allocated his team their tasks. I didn’t really hear much of what he was saying as the generator beside us is extremely noisy and smothers a lot of the conversation. Someone told me after the accident that he spoke about Jim and Ben working above us but I never heard this; probably because of the noise. Pete and I grabbed our tools and headed off to BC1. Clive was just at the gate with his own guys and he signed us into the area. On floor 3, we started carrying out repair work at the back of the BC, with the staircase on the opposite side. We slowly made our way around the vessel. At around 09:00 a.m., we heard a loud bang and a tool bounced off the BC and landed on the scaffold floor beside us. I was in shock as I didn’t know anyone was above us and I hadn’t seen anyone walk by. After a minute or so of silence, Ben Benson came running down and looked towards the tool. He then began apologizing for what had happened. A minute or so later, Jim Johnson appeared and again began apologizing profusely for what had happened. I couldn’t say much at the time as I was still thinking about how close I had come to being smashed by a tool. Mike arrived soon after and again asked us if we were ok. Soon after the Safety Manager came and began asking questions. Clive Conlan—Scaffold Working Supervisor I got a call from Jim Johnson at about 08:30 a.m. about getting onto the BC1 scaffold. I was on BC2 at the time and as we are behind schedule and I’m a few men down, I had to rush them through the sign in and didn’t have time to talk them through the other works in the area, which I would normally do. I am not even supposed to be the area owner but my supervisor was unreachable so I got stuck with doing it on the day. At around 09:30, I heard they had an accident but nobody was hurt. The tool would never have fallen through the gap had we been given time to install the mesh and the nets like we were supposed to. Instead we were rushed over to BC2 to start the scaffold on it. These milestone targets will be the death of someone. | |||||||||
| STEP 4: BASIC LEVEL INCIDENT ANALYSIS | |||||||||
| 1. List Elements List the “people”, “equipment”, and “environment” elements involved in the incident | |||||||||
| PEOPLE | EQUIPMENT | ENVIRONMENT | |||||||
| Jim Johnson | Norbar Torque Wrench Multiplier HT3 3/4 | Time | 09:00 a.m. | ||||||
| Ben Benson | Torque Wrench | Lighting | Good | ||||||
| Lionel Leslie | Tool Lanyards | Climate | Warm | ||||||
| Mike Michaels | - | - | - | ||||||
| Justin James | - | - | - | ||||||
| Clive Conlan | - | - | - | ||||||
| Kevin Kelvin | - | - | - | ||||||
| 2. List Factors For each element listed above identify essential and contributing factors based on the focussing questions in the left-hand column. Essential = Factor is essential for damage to occur. Contributing = Factor increases the likelihood damage occurs but removal may not interrupt incident | |||||||||
| ESSENTIAL AND CONTRIBUTING FACTORS | |||||||||
| The location of the briefing area next to a generator led to critical information being missed by the work parties. | |||||||||
| Programme pressures led to essential dropped object prevention systems being omitted from the final design of the BC scaffold structure. | |||||||||
| A commercial embargo led to an essential tool from being procured and a tool not suitable for the task being used. | |||||||||
| The £20 million milestone achievement reward created an environment of time and resource constraints due to the creation of an unrealistic target date. | |||||||||
| Time pressures led to critical information not being communicated during the sign in stage within the BC area. | |||||||||
| The rubber mats available on site were useless when used to insulate a work area to prevent dropped objects as they had no means of connection to a structure. | |||||||||
| A failure in the fatigue management system led to a worker being exposed to an excessive work pattern. | |||||||||
| 3. List Recommendations From the effectively controllable factors, identified above, list corrective/preventative actions to manage this incident into the future. | |||||||||
| CORRECTIVE/PREVENTATIVE ACTIONS REQUIRED | |||||||||
| 1 | - | ||||||||
| 2 | - | ||||||||
| 3 | - | ||||||||
References
- Thibodeau, P.H.; Boroditsky, L. Metaphors we think with: The role of metaphor in reasoning. PLoS ONE 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Boroditsky, L. How language shapes thought—The languages we speak affect our perceptions of the world. Sci. Am. 2011, 304, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, J. Risk management in a dynamic society: A modelling problem. Saf. Sci. 1997, 27, 183–213. [Google Scholar] [CrossRef]
- Reason, J. Human error: Models and management. BMJ Br. Med. J. 2000, 320, 768–770. [Google Scholar] [CrossRef]
- Johnson, C.W. Visualizing the relationship between human error and organizational failure. In Proceedings of the 17th International Systems Safety Conference, Phoenix, AZ, USA, 13–17 August 1999; pp. 101–110. [Google Scholar]
- Morehouse, W.; Subamaniam, M.A. The Bhopal Tragedy; Technical Report; Council for International and Public Affairs: New York, NY, USA, 1986. [Google Scholar]
- UK Department of Transport. Formal Investigation into the Sinking of the MV Herald of Free Enterprise; Report of Court 8074; Her Majesty’s Stationery Office: London, UK, 1987.
- Air Accidents Investigations Branch, Department of Transport. Report on the Accident to Boeing 737-400 G-OBME Near Kegworth, Leicestershire, on 8 January 1989; Her Majesty’s Stationery Office: London, UK, 1990.
- Dekker, S.W.A. Just culture: Who gets to draw the line. Cognit. Technol. Work 2009, 11, 177–185. [Google Scholar] [CrossRef]
- Douglas, M. Risk and Blame: Essays in Cultural Theory; Routledge: London, UK, 1992. [Google Scholar]
- Leveson, N. A new model for engineering safer systems. Saf. Sci. 2004, 42, 237–270. [Google Scholar] [CrossRef]
- Wu, A.W. Medical error: The Second Victim. BMJ 2000, 320, 812. [Google Scholar] [CrossRef]
- Ruitenberg, B. Court case against Dutch controllers. Controller 2002, 41, 22–24. [Google Scholar]
- Merry, A.F.; McCall Smith, A. Errors, Medicine and the Law; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- Chapman, C. Dispensing errors: A criminal mistake? Chem. Drug. 2009. Available online: http://www.chemistanddruggist.co.uk/cotent/dispensing-errors-criminal-mistake (accessed on 20 September 2018).
- Leape, L.L. Error in medicine. J. Am. Med. Assoc. 1994, 272, 1851–1857. [Google Scholar] [CrossRef]
- Dekker, S.W.A. The Field Guide to Human Error Investigations; Cranfield University: Cranfield, UK, 2002. [Google Scholar]
- Zehr, H.; Gohar, A. The Little Book of Restorative Justice; Good Books: New York, NY, USA, 2002. [Google Scholar]
- Dekker, S.W.A. Just Culture: Balancing Safety and Accountability, 2nd ed.; Ashgate: Farnham, UK, 2012. [Google Scholar]
- Hollnagel, E. Safety I and Safety II: The Past and Future of Safety Management; Routledge: Abingdon, UK, 2014. [Google Scholar]
- Kahneman, D. Thinking, Fast and Slow; Farrar, Straus and Giroux: New York, NY, USA, 2011. [Google Scholar]
- Woods, D.D.; Johannesen, L.J.; Cook, R.J.; Sarter, N.B. Behind Human Error: Cognitive Systems, Computers and Hindsight; DTIC: Fort Belvoir, VA, USA, 1994. Available online: http://www.dtic.mil/dtic/tr/fulltext/u2/a492127.pdf (accessed on 22 March 2018).
- Stanton, N.; Glendon, I. Risk homeostasis and risk assessment. J. Saf. Sci. 1996, 22, 1–13. [Google Scholar] [CrossRef]
- Heinrich, H.W. Industrial Accident Prevention: A Scientific Approach; McGraw-Hill: New York, NY, USA, 1931. [Google Scholar]
- Van Vuuren, W.; Shea, C.E.; Van Der Schaaf, T.W. The Development of an Incident Analysis Tool for the Medical Field; Technical Report EUT/BDK/85; Eindhoven University of Technology, Faculty of Technology Management: Eindhoven, The Netherlands, 1997. [Google Scholar]
- Hale, H.; Wilbert, B.; Freitag, M. After the Event: From Accident to Organizational Learning; Pergamon Press: New York, NY, USA, 1997. [Google Scholar]
- Reason, J. Managing the Risk of Organizational Accidents; Ashgate: Aldershot, UK, 1997. [Google Scholar]
- Shorrock, S.; Leonhardt, J.; Lieu, T.; Peters, C. Systems Thinking for Safety: A White Paper; European Organisation for the Safety of Air Navigation (EUROCONTROL): Brussels, Belgium, 2014; Available online: https://www.skybrary.aero/bookshelf/books/2882.pdf (accessed on 10 May 2018).
- Woods, D.D.; Dekker, S.; Cook, R.; Johannsen, L.; Sarter, N. Behind Human Error; Ashgate: Farnham, UK, 2010. [Google Scholar]
- Hollnagel, E. FRAM: Functional Resonance Analysis Method; Ashgate: Farnham, UK, 2012. [Google Scholar]
- Reason, J. Human Error; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Dekker, S.W.A. Reconstructing human contributions to accidents: The new view on error and performance. J. Saf. Res. 2002, 33, 371–385. [Google Scholar] [CrossRef]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).