
AI-Enabled Electrocardiogram Analysis for Disease Diagnosis



Department of Electrical and Computer Engineering, Tennessee Technological University, Cookeville, TN 38505, USA
*
Author to whom correspondence should be addressed.
Appl. Syst. Innov. 2023, 6(5), 95; https://doi.org/10.3390/asi6050095
Submission received: 5 September 2023
/
Revised: 14 October 2023
/
Accepted: 18 October 2023
/
Published: 20 October 2023
(This article belongs to the Section Medical Informatics and Healthcare Engineering)
Abstract
:Contemporary methods used to interpret the electrocardiogram (ECG) signal for diagnosis or monitoring are based on expert knowledge and rule-centered algorithms. In recent years, with the advancement of artificial intelligence, more and more researchers are using deep learning (ML) and deep learning (DL) with ECG data to detect different types of cardiac issues as well as other health problems such as respiration rate, sleep apnea, and blood pressure, etc. This study presents an extensive literature review based on research performed in the last few years where ML and DL have been applied with ECG data for many diagnoses. However, the review found that, in published work, the results showed promise. However, some significant limitations kept that technique from implementation in reality and being used for medical decisions; examples of such limitations are imbalanced and the absence of standardized dataset for evaluation, lack of interpretability of the model, inconsistency of performance while using a new dataset, security, and privacy of health data and lack of collaboration with physicians, etc. AI using ECG data accompanied by modern wearable biosensor technologies has the potential to allow for health monitoring and early diagnosis within reach of larger populations. However, researchers should focus on resolving the limitations.
1. Introduction
The electrocardiogram (ECG) is a standard tool in clinical practice due to its low cost, quick measurement time, and simplicity. ECG is a noninvasive tool, meaning using it does not require any cut or incision; the only requirement is placing the electrodes in specific positions on the body with or without gel for better conductivity. Also, ECG data acquisition is relatively quick and easy if perfromed with a professional physician; simultaneously, since it captures the heart’s activity, even slight abnormality keeps a trace in the ECG. It provides physiological, electrical, and mechanical activities of the heart for a specific window of time, which contains vast information, including symptoms for different diseases or heart conditions. Besides being user-friendly to doctors, ECG’s usefulness in medical diagnosis is very significant in the case of diagnosing heart conditions such as arrhythmia, heart attack, stroke, heart failure, etc., which are all prevalent worldwide. Even when it comes to monitoring the heart condition of elderly or heart patients, ECG is the primary choice for frequent measurement. Also, while treating any patient during surgery or any medical procedure, keeping track of ECG is a standard preparation to monitor vital health. Even for preoperative evaluation, ECG is popular to ensure no underlying heart conditions might change the course of action during or before the operation.
Until now, apart from the heart rate calculation, the other types of ECG diagnosis typically depend on the physician’s expertise, so consistency and accuracy of the diagnosis varies a lot [1]. ECG has expanded beyond its conventional use and has shown significant promise in diagnosing illnesses unrelated to the heart. Notably, by spotting abnormal breathing patterns while sleeping, ECG data have proven useful in detecting sleep apnea. ECG measurements can be used in epilepsy diagnosis to identify specific electrical patterns and seizures. Furthermore, pulmonary illnesses can be detected by ECG since variations in waveform features might indicate diseases such as chronic obstructive pulmonary disease (COPD). Surprisingly, heart rate variability analysis helps determine stress levels and emotional reactions. Therefore, the ECG’s scope also includes emotional states. This wide-ranging use of ECG highlights its adaptability as a diagnostic tool, moving beyond its originally cardiac-centric focus. Healthcare practitioners glean vital insights into various physiological and psychological conditions by harnessing the heart’s electrical signals. The use of ECG technology in non-cardiac diagnoses may increase as that technology develops, possibly changing medical procedures. This flexibility highlights the value of the ECG as a multifaceted tool for developing thorough and informative healthcare diagnostics across various medical specialties.
Computer-aided diagnosis based on heart rate has been widely used for several years, depending on the device’s rules or pattern recognition algorithm. However, with the advancement of artificial intelligence, such as machine learning and deep learning algorithms, the ECG data, image, and the features acquired from it can be used as input and classified with different output classes, such as different heart disease and other health conditions [2,3,4,5]. Recently, researchers trained and tested computer models that could interpret ECG patterns using internet data. When given the same input data as clinicians, the algorithms could identify some cardiac problems with the same level of accuracy [5,6]. However, there are still some challenges keeping the model or algorithms from being used in clinical settings, such as accuracy, reliability, consistency, interpretability, etc. [7,8,9,10,11,12]. Unless these shortcomings are solved, the experimental accuracy or good performance metrics found by the researchers with a chosen dataset will not impact real life. The advancement in sensor technology and wearable devices made it possible to acquire vital data such as ECG with less noise and for a longer duration, which was necessary with frequent monitoring [13,14,15,16,17]. The invention of high-performance microcontrollers also made it possible to complete complex and vast calculations required to process a large amount of data in real-time [18,19,20]. Therefore, these issues and recent advancements justify the need to review the current literature, which discusses the present research advancement in the field of AI in ECG for diagnosis to determine the challenges and shortcomings for future research directions.
1.1. Current Literature Survey
This subsection discusses the relevant systematic survey and review work that has been conducted on the use of ECG with artificial intelligence for the purpose of diagnosis. These studies accumulated and summarized here are based on three aspects:
- Is ECG the main or only vital sign considered in the literature survey?
- Is artificial intelligence the focus technology for interpreting ECG?
- Were there significant challenges and future directions discussed?
Table 1 contains the list of literature survey or review papers published in recent years, along with their title and discussion summaries.
The existing review papers on the application of ECG and AI in the field of diagnosis have primarily focused on specific types of heart diseases or diseases related to particular organs. As a result, the current body of literature lacks a more comprehensive and integrated approach to diagnosis using ECG and AI. To address this limitation, a new review work was developed that takes a more holistic perspective by comprehensively integrating ECG and AI. This approach is intended to provide a complete understanding of the potential for using ECG and AI to diagnose various cardiac and other diseases and health conditions. The review covers other essential aspects of the ECG and AI techniques, such as the preprocessing of ECG signals and the current datasets available for research. Various new deep learning techniques appear as AI develops, but the possibility of their use in the real world is constrained by technical issues. This study explores these issues and constraints while highlighting prospective research lines to raise the precision and utility of these approaches in real-world applications.
1.2. Survey Goal
With the ever-evolving sensor technology, signal processing capability, and machine learning/deep learning algorithms, it is essential to incorporate these advancements into the latest survey paper. This survey paper aims to provide a comprehensive overview of the research conducted in electrocardiogram (ECG) analysis using machine learning and deep learning techniques for clinical diagnosis. To begin, section two presents a framework for searching relevant and recent materials for this survey. The third section discusses the ECG signal analysis techniques, which include signal processing methods like noise reduction, filtering, and feature extraction. The fourth section elaborates on using machine learning with ECG for clinical analysis, including classification, clustering, and regression techniques. This paper delves deeper into the clinical analysis of heart diseases using ECG signals. The first part of this analysis is based on heart disease discussions, including coronary artery disease, arrhythmia, and heart failure. The second part of the clinical analysis focuses on discussing other diseases, followed by an analysis of the application of deep learning using ECG for diagnosis. DL algorithms have great potential in ECG analysis, especially in arrhythmia detection and classification. Section five discusses the challenges and future recommendations.
The literature survey aimed to address three primary research questions related to using electrocardiogram (ECG) with artificial intelligence (AI) for diagnostic purposes.
- What is the preprocessing required for ECG signal before using it with AI techniques?
- What are the ML/DL techniques applied in ECG-based heart diseases and other health issues?
- Are there any limitations and challenges in using ECG signals for ML/DL-based disease classification?
2. Framework for Reference Search and Selection Process
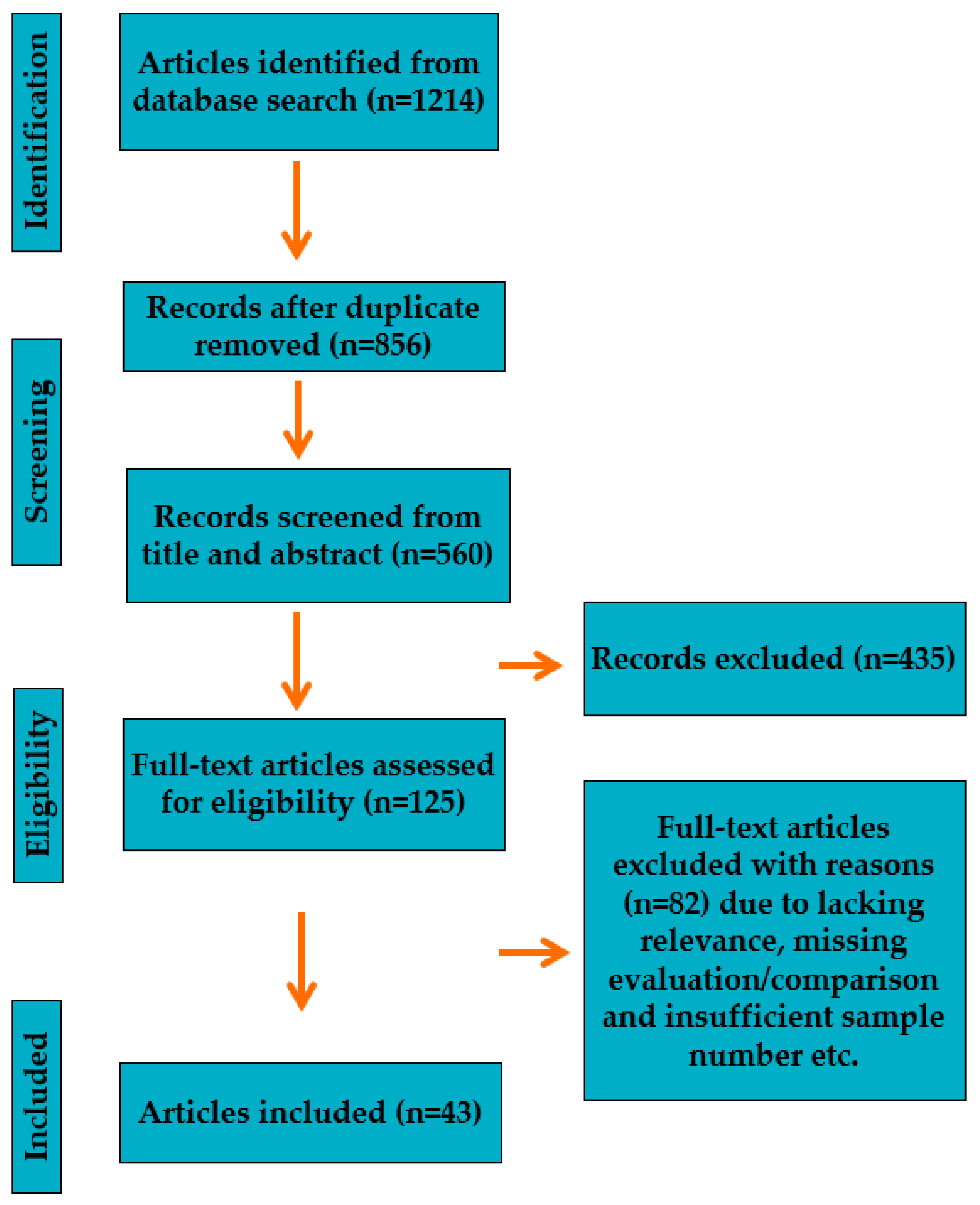
For a thorough survey, the search process was implemented to find the relevant research on using ECG for diagnosis with the help of artificial intelligence. Google Scholar and PubMed were used to find the studies or experiments performed and published, using a timeline from 2018 to 2023. The following terms were used to search: (“ECG” or “electrocardiogram”, “EKG” or “biomedical signals”, “vital signs”) and (“heart disease” or “cardiovascular disease” or “Arrhythmia” or “health monitoring”) or (“machine learning” or “ML” or “deep learning” or “DL” or “artificial neural network” or “convolutional neural network” or “ANN” or “CNN” or “LSTM”). The number of articles found after using these search terms was significantly large. Therefore, a work plan had to be established to sort out the relevant ones. Figure 1 visually represents the article selection process used for this literature review. This process involved four stages: identification, screening, eligibility, and inclusion.
The first stage, identification, involved searching for articles on Google Scholar and PubMed, retrieving 1214 articles. After removing duplicates, the number of articles was reduced to 856. These articles were subjected to the second stage of the selection process, screening. At this stage, the conference abstracts and articles with access restrictions were removed (from 856 to 560). Second, the titles and abstracts of the articles were reviewed to identify articles irrelevant to the study or outside the scope of the research. Four hundred thirty-five articles were removed during this stage (from 560 to 125). The third stage of the selection process involved a thorough review of the full texts of the remaining 125 articles identified as potentially relevant during the screening stage. During this review, 82 more articles were eliminated due to missing evaluations or assessments, inadequate dataset or sample numbers, the deficient rationale behind evaluations, and sketchy details of the experiment or method used. Finally, 43 articles were deemed relevant to the literature review after completing the eligibility stage. They met all the criteria specified in the framework. This rigorous selection process ensured that only high-quality, relevant articles were included in the final review, which would help to provide accurate and reliable findings.
3. ECG Signal Analysis
Before using ECG signal information as input for any artificial intelligence algorithm, ECG data must be processed to make it suitable. Without a signal analysis and processing, the ECG data might contain unwanted artifacts, noise, unusual spikes or abnormal characteristics, etc., which might result in the inaccurate result of ML/DL algorithms or under/overfitting. The typical steps or stages for ECG signal analysis and processing are filtering, feature extraction, and feature selection. In this section, the conventional techniques implemented using ECG are discussed.
The signal-to-noise ratio for ECG is not high, so the raw ECG becomes unusable without proper denoising. Since it is a biomedical signal, there are chances of noise from biological, mechanical, and electrical aspects. The first noise to be discussed here is the electromyogram (EMG), which comes as a result of the electrical activity of the body muscle. Since the frequency spectra for EMG and ECG overlap, using ordinary filters does not work [35,36]. Also, although the EMG noise is minimal at resting position, during activity, such as under stress or during exercise, the effect is significant. Adaptive filters, wavelet transformation, and low-pass filters were tried to remove EMG noise. Using those filters appears to affect the peak shapes of ECG [36,37]. Two more common noises are baseline wanderer and power line interference. The fixed range (50–60 Hz) makes removing power line interference easier. The typical solution is using a notch filter and their variant with the downside of adding a ripple to the ECG wave [38,39,40,41]. Some other solutions are adaptive filters, such as the Hilbert Huang Transform adaptive filter; the downside, in this case, is the requirement of a reference signal [42,43,44,45,46]. The electrocardiogram (ECG) waveform may exhibit baseband wander, which is extra low-frequency noise or movement that gradually shifts or drifts the baseline. It frequently results from electrode or patient movement, breathing, or muscular activation. Techniques including correct electrode placement, patient positioning, signal filtering, and cutting-edge artifact removal technologies are used to reduce baseband wander’s adverse effects on the precision and interpretation of the ECG signal. Different filters were applied to remove baseband wander, such as high pass filters, adaptive filters, wavelet transformation, etc. [47,48,49,50]. In Figure 2, a typical ECG wave is depicted, and in Figure 3, an example of baseband wander is shown.
There are three different domains from which aspect the features are extracted.
- Time domain: The most significant is the time domain since the ECG presents the physical movement of the heart’s activities. However, the frequency and statistical domains provide helpful information that can remain unnoticed in time domain information. The time domain characteristics of the ECG waveform delineate its features based on time, which consist of amplitude, duration, P-wave duration, QRS duration, the QT interval, the RR interval, and the PR interval [52,53,54,55,56,57,58,59]. The height of the waveform, known as the amplitude, represents the strength of the electrical signal generated by the heart. Duration denotes the time the waveform takes to complete one cycle, calculated from the beginning of one waveform to the beginning of the next. P-wave duration measures the time taken for the first positive deflection of the waveform that shows atrial depolarization. QRS duration determines the time taken for the QRS complex, which displays ventricular depolarization. The QT interval represents the duration between the start of the QRS complex and the end of the T-wave, signifying the entire length of ventricular depolarization and repolarization. The RR interval indicates the duration between two consecutive R waves corresponding to the time between two heartbeats. Finally, the PR interval shows the time the electrical signal travels from the atria to the ventricles. These features provide crucial information about the heart’s electrical activity and help diagnose and monitor several cardiac conditions.
- Frequency domain: Frequency domain features of ECG refer to the characteristics of the ECG waveform in terms of frequency, obtained by converting the ECG signal from the time domain to the frequency domain using techniques like Fourier transform [59,60,61]. ECG’s most common frequency domain features are power spectral density (PSD), frequency bands, and heart rate variability (HRV). PSD measures the ECG signal’s power at different frequencies and provides information about the signal’s energy distribution over a broad range of frequencies. The frequency bands associated with ECG signals are shallow frequency (VLF), low frequency (LF), and High frequency (HF). VLF power is linked to long-term heart rate and blood pressure fluctuations. The autonomic nervous system’s sympathetic and parasympathetic branches control several physiological processes, including heart rate variability (HRV). Frequency domain methods, such as spectral analysis, which divides the HRV signal into several frequency bands, are frequently used to investigate HRV. In HRV analysis, the high-frequency (HF) band (usually 0.15–0.4 Hz) is linked to parasympathetic (vagal) activity, while the low-frequency (LF) band (generally 0.04–0.15 Hz) is thought to represent a combination of sympathetic and parasympathetic impulses. HRV measures the time intervals between successive heartbeat variations, helps to assess the risk of arrhythmia, and provides information about the autonomic nervous system’s function. By analyzing the ECG’s frequency domain features, medical professionals can gain insights into the heart’s functioning and the autonomic nervous system.
- Statistical domain: The statistical features of ECG are parameters that describe the distribution of the ECG signal in the time and frequency domains. These features include measures of central tendency, such as mean and median, measures of variability, such as variance and standard deviation, and measures of distribution, such as skewness and kurtosis. The mean of the ECG signal represents the average amplitude of the waveform over a specific time interval. At the same time, the variance measures the spread of the signal around the mean. High variability can indicate that the signal has many variabilities, while low variability indicates that the signal is relatively stable. Skewness measures the degree of asymmetry of the distribution, while kurtosis measures the degree of the peakedness of the distribution. Heart rate, also known as rate, is another statistical feature of ECG that describes the number of heartbeats per minute. This feature can assess the cardiovascular system’s overall health and detect rapid or slow heart rate abnormalities. These statistical features can be used to diagnose and monitor cardiovascular diseases by extracting them through mathematical techniques like signal processing and machine learning algorithms. They can also be used to develop automated ECG analysis tools for clinical applications.
The feature selection stage is mandatory because, based on the objective, target variable, or outcome, the requirement of several features and a choice of feature changes. The features can be ranked based on the correlation with the class variable, and a threshold can be used to choose a certain number of features. Usually, there are three types of feature selection techniques:
- Filter-based: The filter-based method [62] evaluates each feature’s relevance independently of the machine learning algorithm by analyzing the correlation between each feature and the target variable. Filter-based methods include correlation-based feature selection (CFS), mutual information, and variance threshold.
- Wrapper-based methods assess the relevance of a subset of features by training and evaluating the machine learning algorithm on various feature subsets [62]. Although these methods are computationally expensive, they can yield better accuracy than filter-based methods. Recursive feature elimination (RFE) is a well-known wrapper-based method that recursively eliminates the least essential features until the desired number of features is selected.
- Embedded-based: Embedded-based methods are a combination of filter-based and wrapper-based methods. These methods perform feature selection during the machine learning algorithm’s training process [62]. Lasso (Least Absolute Shrinkage and Selection Operator) and Ridge regression are typical examples of embedded-based methods that use regularization techniques. Recently, there have been evolutionary algorithms that have been used for the selection of ECG features, some of the algorithms are genetic algorithm [63], particle swarm optimizer [64], firefly algorithm [64].
4. Use of ECG with AI for Clinical Analysis and Diagnosis
This section discusses the use of information acquired from ECG signals with different machine learning algorithms. The significant part of discussion focuses on the diagnosis of different heart diseases. Still, at the same time, some other uses of ECG signals are discussed to monitor various health parameters and characteristics.
4.1. Use of ML with ECG for Heart Health Diagnosis
The electrocardiogram (ECG), a crucial cardiovascular health diagnostic tool, offers thorough information on cardiac function. Waveform or tabular ECG data are processed by machine learning algorithms, which then extract and choose the most pertinent characteristics for study. The machine learning algorithms, such as regression, support vector machine, decision tree, etc., are being trained using the finalized features. Once the model performance is acceptable, that model can be used to validate and later evaluate using new ECG data for diagnosis purposes. Some recent and relevant studies related to using ECG with machine learning for heart disease diagnosis are listed in Table 2.
A framework for machine learning using ECG data for disease diagnosis is depicted in Figure 4. The process of using ECG data with machine learning (ML) for illness diagnosis is shown in the flow diagram. The first step is gathering ECG data in many formats, including tabular, waveform, picture, and video. The data are then split into two sets to train and assess the ML model: training and testing datasets.
The next step is to create and train prediction models using various ML algorithms on the training dataset. In order to compare various models and improve the ML algorithms, the assessment process is carried out iteratively. The goal is to find the model that performs the best and most correctly forecasts the target illness. The flow diagram moves to the final model selection phase after the assessment. The final illness prediction model is selected based on its performance and accuracy. This model may be ready for application and captures the discovered correlations and patterns in the ECG data. This section aims to divert attention away from a comparison based on high accuracy or other performance indicators to the extent of ongoing research efforts in utilizing machine learning algorithms to diagnose heart diseases. While comparative analysis is frequently used to assess the efficacy of various algorithms or methodologies, it may not necessarily be the best strategy for applying machine learning to diagnose cardiac conditions. The reasons behind avoiding performance metrics are the following: first, there is no generalized protocol to evaluate a machine learning model while using ECG for heart disease diagnosis. Second, there is no standardized dataset, and people use different datasets for evaluation, making it hard to compare different models. The quantity, diversity, quality, and inclusion standards of the heart disease datasets utilized in various research may differ. Because of these variances, comparing machine learning algorithms conclusively using only accuracy or other criteria can be challenging. Third, different research papers on applying machine learning algorithms to diagnose cardiac disorders may present distinct circumstances, such as patient demographics or experimental setups. Direct comparisons might be incorrect or misleading due to these contextual variations, which substantially influence performance indicators and results. Although the research is ongoing and researchers produce excellent, accurate models, real-life implementation and usability in medical setups remain in question. Machine learning algorithms have been primarily used for heart rate-related problems and other heart diseases such as myocardial infarction or general heart diseases such as “yes” or “no” scenarios.
Here are some potential paths for future study in the use of ECG for diagnosis using machine learning for heart disease diagnosis:
- Develop more robust machine learning algorithms: Often, the machine learning algorithms used today to diagnose ECGs are not resistant to signal noise and distortions. This is a significant drawback since real-world ECG recordings frequently contain noise and artifacts. Developing more robust machine learning algorithms that can better tolerate noise and artifacts should be the primary goal of future research.
- Use more extensive and diverse datasets: Most research on machine learning for ECG diagnosis has relied on relatively small datasets. The results’ generalizability is so constrained. Future research should use more extensive and varied datasets to increase the generalizability of the findings. A benchmark dataset should contain a sufficient number of features that are relevant to the class variable as well as a large number of samples from varied characteristics of patients.
- Integrate machine learning with other clinical data: Clinical data other than ECG signals can also be utilized to identify cardiac disorders. Information from patient medical records, lab results, and imaging investigations may also be utilized. Future studies should look at ways to better diagnose heart disease by combining machine learning with other clinical data.
- Develop mobile and wearable ECG devices: ECG equipment is becoming more wearable and portable. This enables the collection of ECG data outside of a hospital environment. Future studies should look at ways to enhance the early diagnosis of cardiac problems using mobile and wearable ECG sensors.
- Make machine learning algorithms more interpretable: Black boxes characterize many current machine learning techniques for ECG diagnosis. As a result, it is challenging to comprehend how the algorithms generate their predictions. Future studies should concentrate on creating interpretable machine learning algorithms so physicians can better comprehend the outcomes of the forecasts.
4.2. Use of DL with ECG for Heart Health Diagnosis
With the advancement of deep learning algorithms such as artificial neural network (ANN), convolutional neural networks (CNN), long short-term memory (LSTM), recurrent neural network (RNN), etc., along with tabular and waveform type of data, the image of ECG came in the front. Because neural networks may link characteristics that are challenging to comprehend with the human eye or conventional machine learning approaches, recent research has concentrated chiefly on deep learning [85,86]. The input was raw data, and the output was disease classification. The first research worked with ECG data to classify them into different arrhythmia types. The second research worked with ECG data to detect ventricular systolic dysfunction. In both types of research, the accuracy of models was better than that of contemporary research using machine learning algorithms without neural networks or DL. The significant advantage of DNN is that there is no need to work with feature extraction or feature selection. Major disadvantages are heavy on calculation and require a significantly large amount of data. Some recent and relevant studies related to using ECG with deep learning for heart disease diagnosis are listed in Table 3.
Based on the literature review on deep learning using ECG for heart disease diagnosis, the most popular algorithms among researchers are convolutional neural network (CNN) and long short-term memory (LSTM). Similar to the reasons stated in the previous subsection, the review does not discuss the performance of deep neural networks. Instead, the review discusses the potential use of DL for diagnosis. Like the current scenario using machine learning algorithms, deep learning algorithms are strictly limited to studies or experiments; none of the studies have been implemented in any commercial product or can be used reliably in medical setups. However, from the existing experiments, it is evident that the future holds significant promises once the questions with reliability and consistency can be solved. This was primarily concluded because deep learning can train a model by fusing several characteristics in a sophisticated network. This aids the model’s learning and comprehension of intricate correlations and patterns in the data. However, because of how intricate these linkages are, it is tough for people to comprehend or duplicate how the model decides entirely. Deep learning algorithms can manage enormous volumes of data and extract useful information from them, surpassing what humans can, in some instances, examine and comprehend.
Since ECG data is one-dimensional, 1D CNN can be used instead of 2D CNN [106,107,108]. Also, the 2D CNN can be applied when using a time-frequency spectrogram. Also, the image of ECG can be used as input for a standard CNN algorithm. The complexity of the calculation capacity requirement varies based on the neural network’s depth. However, it has performed excellently in studies with arrhythmia and atrial fibrillation [109,110,111]. Recurrent neural network (RNN) has the advantage of using time series data and has proven excellent performance [112,113,114]. The LSTM part from RNN can analyze the sequential relation in ECG data and be used with CNN. Also, “Bidirectional LSTM” may simultaneously examine the context before and after a certain point in the data. In order to grasp the whole context and make more precise predictions, gathering information from past and future points in the ECG data is highly helpful [115,116]. Also, using the advantage of the attention module of locating the most informative part and the ability to length the ECG window with LSTM-CNN can improve efficiency [114]. The only downside of these techniques is that computational cost is very high since they need to work with many parameters.
4.3. Use of ML/DL with ECG for Other Health Issues
With the advancement of machine learning and deep learning with ECG data in tabular, waveform, image, or video format, the impact of using ECG on some other health conditions or diseases can be assessed or detected more accurately than the typical rule-based or threshold-based clinical diagnosis. Based on recent research findings, the other areas where the analysis of ECG has an impact are sleep apnea detection, respiration rate detection, fetal ECG monitoring, and blood pressure monitoring. In Table 4, the information on use of ML and DL with ECG data for the diagnosis of diseases other than cardiac issues is listed.
Sleep apnea happens when obstruction occurs during airflow while sleeping and disturbs breathing. It increases cardiac disease by threefold and makes a person prone to accidents. Left unnoticed or untreated, it may result in severe CVD. The conventional way of diagnosing sleep apnea is by attaching an electrode while sleeping, which is uncomfortable; researchers in recent years have used single lead ECG measurement and classification using machine learning into sleep apnea or normal conditions. The ECG measurement can be turned into a respiratory signal using signal processing techniques since the latter is hidden in the former. Since ECG signal acquisition is cheaper and more accessible, respiration, another crucial vital sign, can be measured simultaneously while monitoring heart health conditions. The fetal heart rate can be achieved by recording abdominal ECG by placing ECG lead over the abdomen of a pregnant woman. From that fetal heart rate, the possible arrhythmia of the fetus and probable congenital disease information can be observed, as suggested by several studies. Finally, measuring blood pressure in a noninvasive way without a cuff can be achieved using ECG and PPG signals [129,130,131,132]. The pulse transit time can be calculated from those two signals. That parameter is inversely related to the change in blood pressure.
Accurate and effective stroke detection is essential for prompt treatment and better patient outcomes. A potential method for stroke diagnosis has evolved that combines artificial intelligence (AI) methods with electrocardiograms (ECG) [133]. ECG analysis and cutting-edge AI algorithms can offer doctors important information about stroke diagnosis. Atrial fibrillation (AF) detection utilizing ECG and AI is one of the essential components of the process. AF, an irregular heartbeat, considerably increases the risk of stroke. AI systems can automatically identify the existence of AF by reviewing ECG data, enabling the early detection of those at risk for stroke [134]. The ST-segment alterations in an ECG can be a valuable indicator of an ischemic stroke. Lack of oxygen delivery to the heart causes an ischemic stroke characterized by distinctive abnormalities in the ST segment of the ECG [135]. These ST-segment variations may be analyzed by AI algorithms, which then categorize them as signs of stroke, assisting medical practitioners in making quick and precise diagnoses. ECG signal analysis of the QRS complexes aids in stroke detection. Artificial intelligence (AI) systems can spot abnormalities in these complexes to provide effective stroke detection. AI may also evaluate heart rate variability (HRV) produced from ECG readings to find patterns associated with stroke risk to detect stroke [136]. Early identification of strokes and the evaluation of stroke risk are improved by combining HRV analysis with other clinical data.
Convulsions, loss of consciousness, sensory problems, and periods of aberrant electrical activity in the brain are just a few symptoms that can result from seizures. Growing interest has been shown in the application of AI and ECG for epilepsy detection in recent years. ECG data may be analyzed using AI algorithms to find patterns connected to epilepsy. These patterns can be utilized to create AI-based tools that assist physicians in making earlier and more accurate diagnoses of epilepsy [137,138]. The combination of ML/DL and ECG has the potential to completely transform healthcare by enabling the early and precise identification of a wide range of medical disorders outside of heart diseases. These strategies might improve patient care, enable individualized therapy, and aid in the general growth of healthcare systems with more study and development.
5. Challenges and Future Recommendations
The advancements in artificial intelligence are allowing researchers the use of ECG data, whether the format is tabular, waveform, image or video, etc., for the diagnosis of different health issues along with cardiac problems. Although the performance is presentable during the experiment for those studies, accuracy for a different dataset for which the model has not been trained and reliability remains questionable. This section discusses the current challenges, limitations, and probable future research directions.
- External evaluation/standard system for evaluation: The first limitation of the current studies is an external evaluation or a standard system for evaluating the performance of the models produced by the researcher to create an acceptable benchmark. Also, when the disease differs between race and geographical area, the models do not have any answer or options for modification for those terms.
- Ability to be applied in clinical setups: Despite excellent experiment performance, none of the algorithms made it to a medical setup. The main reason behind this conclusion is that the use of ECG in most cases cannot be the only data source to achieve a conclusive diagnosis. Also, medical professionals are less likely to accept it for diagnosis unless the model’s performance is consistent over a different dataset with different characteristics and there is no regulatory problem.
- Limited resource in wearables for computation: The use of deep learning techniques in wearables, which use substantial neural networks, has another disadvantage. Significant computational resources are needed to handle and evaluate the data from these networks. This can be difficult for wearable technology or other edge computing devices since they do not have the capabilities to carry out such computationally demanding activities locally. In these circumstances, relying on cloud-based programs or distant servers to process data and make decisions can be necessary. This drawback emphasizes how crucial it is to consider the computing capabilities and resource needs when developing deep learning algorithms for ECG analysis in wearable technology or other situations with limited resources. Also, at the same time, using the cloud as an option to take care of the computation question comes to form the front of privacy and security. Sending personal information over the cloud makes it vulnerable to attacks or leaks. Therefore, the infrastructure needs to be there with proper security and privacy protocol before the data can be moved to another location for analysis or diagnosis.
- Imbalanced and limited labeled datasets: Imbalanced datasets are a big concern. Training deep learning algorithms requires significantly large amounts of data. However, not all cases or classes of diseases or health conditions have a large dataset with a balanced format. Therefore, the unavailability of a balanced dataset may provide accurate results, but that cannot be taken as a general rule and can result in overfitting or underfitting.
- Interpretability and transparency: In utilizing deep learning algorithms for ECG analysis to diagnose disorders, interpretability and transparency are significant problems. Convolutional neural networks (CNNs) are an example of a sophisticated deep learning model that is sometimes called a “black box” since it lacks explicit rules or explanations that humans can understand. It raises questions about the validity and dependability of the diagnostic judgments made by these models due to this lack of interpretability. Clinicians in conventional medicine rely on interpretability to comprehend the underlying causes of a diagnosis. They must be able to describe how specific characteristics or patterns in the ECG signal help to identify a particular condition. To track down and comprehend the precise elements or patterns that lead to a given diagnosis, deep learning models function by learning sophisticated representations from enormous volumes of data. Their lack of interpretability may hamper the acceptability and use of AI-based diagnostic tools in clinical settings.
Based on the limitations and challenges stated above, there are several aspects that future research should focus on, as shown in Figure 5.
6. Conclusions
The ECG is an essential tool that can be used to determine cardiac issues through the help of artificial intelligence. Also, the advancement of ML and DL provides opportunities to use ECG for other health signs measurements, such as blood pressure measurement, fetal ECG, respiration rate, sleep apnea detection, etc. This review provided a detailed discussion about recent updates and notable research on the depth of diagnosis using AI techniques on information extracted from ECG signals. Although the processing of ECG signals using AI techniques started with only machine learning algorithms, deep learning algorithms such as CNN and RNN (LSTM) have dominated the studies in recent years. Although the performance from the recent studies showed excellent improvement over previous ones, there has been minimal progress in bringing those solutions to real life or any medical setup. Also, the practical use of AI with ECG remains limited in wearable devices, only for heart rate or arrhythmia. More studies are required to improve the usability and applicability of AI with ECG applications in actual medical situations. It is vital to concentrate on improving the interpretability of AI models so that medical practitioners can comprehend and believe the models’ diagnostic choices. Developing a standard assessment process and a standard dataset is crucial to guarantee consistent and dependable performance across several investigations. By focusing on these study areas, we may overcome the barriers to the mainstream use of AI in ECG analysis and expand its application in various healthcare situations.
Author Contributions
Conceptualization, M.M.R.K.M.; methodology, M.M.R.K.M.; software, M.M.R.K.M.; validation, M.M.R.K.M.; formal analysis, M.M.R.K.M.; investigation, M.M.R.K.M.; resources, M.M.R.K.M.; data curation, M.M.R.K.M.; writing—original draft preparation, M.M.R.K.M.; writing—review and editing, M.M.R.K.M. and T.E.; visualization, M.M.R.K.M.; supervision, T.E.; project administration, T.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The author declares no conflict of interest.
References
- Shintomi, A.; Izumi, S.; Yoshimoto, M.; Kawaguchi, H. Effectiveness of the heartbeat interval error and compensation method on heart rate variability analysis. Healthc. Technol. Lett. 2022, 9, 9–15. [Google Scholar] [CrossRef]
- El-Baz, A.; Giridharan, G.A.; Shalaby, A.; Mahmoud, A.H.; Ghazal, M. Special Issue “Computer Aided Diagnosis Sensors”. Sensors 2022, 22, 8052. [Google Scholar] [CrossRef]
- Simegn, G.L.; Gebeyehu, W.B.; Degu, M.Z. Computer-Aided Decision Support System for Diagnosis of Heart Diseases. Res. Rep. Clin. Cardiol. 2022, 13, 39–54. [Google Scholar] [CrossRef]
- Marques, J.A.L.; Gois, F.N.B.; Madeiro, J.P.D.V.; Li, T.; Fong, S.J. Artificial neural network-based approaches for computer-aided disease diagnosis and treatment. In Cognitive and Soft Computing Techniques for the Analysis of Healthcare Data; Academic Press: Cambridge, MA, USA, 2022; pp. 79–99. [Google Scholar]
- He, Y.; Ren, K.; Shan, S. Design of Microcontroller-Based Heart Rate and Temperature Detection System. In Proceedings of the 2022 IEEE 5th International Conference on Information Systems and Computer Aided Education (ICISCAE), Dalian, China, 23–25 September 2022; pp. 22–25. [Google Scholar]
- Mamun, M.M.R.K.; Alouani, A. Arrhythmia Classification Using Hybrid Feature Selection Approach and Ensemble Learning Technique. In Proceedings of the 2021 IEEE Canadian Conference on Electrical and Computer Engineering (CCECE), Virtual, 12–17 September 2021; pp. 1–6. [Google Scholar]
- Mamun, M.M.R.K.; Alouani, A. Automatic Detection of Heart Diseases Using Biomedical Signals: A Literature Review of Current Status and Limitations. In Future of Information and Communication Conference; Springer: Cham, Switzerland, 2022; pp. 420–440. [Google Scholar]
- Rajpurkar, P.; Chen, E.; Banerjee, O.; Topol, E.J. AI in health and medicine. Nat. Med. 2022, 28, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Tadesse, G.A.; Ho, D.; Fei-Fei, L.; Zaharia, M.; Zhang, C.; Zou, J. Advances, challenges and opportunities in creating data for trustworthy AI. Nat. Mach. Intell. 2022, 4, 669–677. [Google Scholar] [CrossRef]
- Farina, E.; Nabhen, J.J.; Dacoregio, M.I.; Batalini, F.; Moraes, F.Y. An overview of artificial intelligence in oncology. Futur. Sci. OA 2022, 8, FSO787. [Google Scholar] [CrossRef]
- Benda, N.C.; Novak, L.L.; Reale, C.; Ancker, J.S. Trust in AI: Why we should be designing for APPROPRIATE reliance. J. Am. Med. Inform. Assoc. 2021, 29, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Busnatu, A.; Niculescu, A.; Bolocan, G.E.; Petrescu, D.N.; Păduraru, I.; Năstasă, M.; Lupușoru, M.; Geantă, O.; Andronic, A.M. Grumezescu Clinical Applications of Artificial Intelligence—An Updated Overview. J. Clin. Med. 2022, 11, 2265. [Google Scholar] [CrossRef] [PubMed]
- Chidambaram, S. IoT-based ECG monitoring system for smart healthcare data applications. In Recent Advancement of IoT Devices in Pollution Control and Health Applications; Woodhead Publishing: Sawston, UK, 2023; pp. 109–125. [Google Scholar]
- Devi, D.H.; Duraisamy, K.; Armghan, A.; Alsharari, M.; Aliqab, K.; Sorathiya, V.; Das, S.; Rashid, N. 5G Technology in Healthcare and Wearable Devices: A Review. Sensors 2023, 23, 2519. [Google Scholar] [CrossRef]
- Hughes, A.; Shandhi, M.H.; Master, H.; Dunn, J.; Brittain, E. Wearable Devices in Cardiovascular Medicine. Circ. Res. 2023, 132, 652–670. [Google Scholar] [CrossRef]
- Gawali, D.H.; Wadhai, V.M.; Patil, M.; Chanchlani, A.S. A Wearable ECG Sensor for Intelligent Cardiovascular Health Informatics. In Designing Intelligent Healthcare Systems, Products, and Services Using Disruptive Technologies and Health Informatics; CRC Press: Boca Raton, FL, USA, 2022; pp. 109–129. [Google Scholar]
- Gomes, N.; Pato, M.; Lourenço, A.R.; Datia, N. A Survey on Wearable Sensors for Mental Health Monitoring. Sensors 2023, 23, 1330. [Google Scholar] [CrossRef] [PubMed]
- Shumba, A.; Montanaro, T.; Sergi, I.; Fachechi, L.; De Vittorio, M.; Patrono, L. Leveraging IoT-Aware Technologies and AI Techniques for Real-Time Critical Healthcare Applications. Sensors 2022, 22, 7675. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.-W.; Lee, W.; Kim, Y.-J. A Real-Time Wearable Physiological Monitoring System for Home-Based Healthcare Applications. Sensors 2021, 22, 104. [Google Scholar] [CrossRef]
- Ouda, H.; Badr, A.; Rashwan, A.; Hassanein, H.S.; Elgazzar, K. Optimizing Real-Time ECG Data Transmission in Constrained Environments. In Proceedings of the ICC 2022—IEEE International Conference on Communications, Seoul, Republic of Korea, 16–20 May 2022; pp. 2114–2119. [Google Scholar]
- Mincholé, A.; Camps, J.; Lyon, A.; Rodríguez, B. Machine learning in the electrocardiogram. J. Electrocardiol. 2019, 57, S61–S64. [Google Scholar] [CrossRef] [PubMed]
- Wasimuddin, M.; Elleithy, K.; Abuzneid, A.-S.; Faezipour, M.; Abuzaghleh, O. Stages-Based ECG Signal Analysis From Traditional Signal Processing to Machine Learning Approaches: A Survey. IEEE Access 2020, 8, 177782–177803. [Google Scholar] [CrossRef]
- Hong, S.; Zhou, Y.; Shang, J.; Xiao, C.; Sun, J. Opportunities and challenges of deep learning methods for electrocardiogram data: A systematic review. Comput. Biol. Med. 2020, 122, 103801. [Google Scholar] [CrossRef]
- Somani, S.; Russak, A.J.; Richter, F.; Zhao, S.; Vaid, A.; Chaudhry, F.; De Freitas, J.K.; Naik, N.; Miotto, R.; Nadkarni, G.N.; et al. Deep learning and the electrocardiogram: Review of the current state-of-the-art. Europace 2021, 23, 1179–1191. [Google Scholar] [CrossRef]
- Saini, S.K.; Gupta, R. Artificial intelligence methods for analysis of electrocardiogram signals for cardiac abnormalities: State-of-the-art and future challenges. Artif. Intell. Rev. 2021, 55, 1519–1565. [Google Scholar] [CrossRef]
- Siontis, K.C.; Noseworthy, P.A.; Attia, Z.I.; Friedman, P.A. Artificial intelligence-enhanced electrocardiography in cardiovascular disease management. Nat. Rev. Cardiol. 2021, 18, 465–478. [Google Scholar] [CrossRef]
- Liu, X.; Wang, H.; Li, Z.; Qin, L. Deep learning in ECG diagnosis: A review. Knowl.-Based Syst. 2021, 227, 107187. [Google Scholar] [CrossRef]
- Chung, C.T.; Lee, S.; King, E.; Liu, T.; Armoundas, A.A.; Bazoukis, G.; Tse, G. Clinical significance, challenges and limitations in using artificial intelligence for electrocardiography-based diagnosis. Int. J. Arrhythmia 2022, 23, 24. [Google Scholar] [CrossRef] [PubMed]
- Petmezas, G.; Stefanopoulos, L.; Kilintzis, V.; Tzavelis, A.; Rogers, J.A.; Katsaggelos, A.K.; Maglaveras, N. State-of-the-Art Deep Learning Methods on Electrocardiogram Data: Systematic Review. JMIR Med. Inform. 2022, 10, e38454. [Google Scholar] [CrossRef] [PubMed]
- Rjoob, K.; Bond, R.; Finlay, D.; McGilligan, V.; Leslie, S.J.; Rababah, A.; Iftikhar, A.; Guldenring, D.; Knoery, C.; McShane, A. Machine learning and the electrocardiogram over two decades: Time series and meta-analysis of the algorithms, evaluation metrics and applications. Artif. Intell. Med. 2022, 132, 102381. [Google Scholar] [CrossRef]
- Ayano, Y.M.; Schwenker, F.; Dufera, B.D.; Debelee, T.G. Interpretable Machine Learning Techniques in ECG-Based Heart Disease Classification: A Systematic Review. Diagnostics 2022, 13, 111. [Google Scholar] [CrossRef] [PubMed]
- Merdjanovska, E.; Rashkovska, A. Comprehensive survey of computational ECG analysis: Databases, methods and applications. Expert Syst. Appl. 2022, 203, 117206. [Google Scholar] [CrossRef]
- Denysyuk, H.V.; Pinto, R.J.; Silva, P.M.; Duarte, R.P.; Marinho, F.A.; Pimenta, L.; Gouveia, A.J.; Gonçalves, N.J.; Coelho, P.J.; Zdravevski, E.; et al. Algorithms for automated diagnosis of cardiovascular diseases based on ECG data: A comprehensive systematic review. Heliyon 2023, 9, e13601. [Google Scholar] [CrossRef]
- Pradhan, B.K.; Neelappu, B.C.; Sivaraman, J.; Kim, D.; Pal, K. A Review on the Applications of Time-Frequency Methods in ECG Analysis. J. Healthc. Eng. 2023, 2023, 3145483. [Google Scholar] [CrossRef]
- Marouf, M.; Saranovac, L.; Vukomanovic, G. Algorithm for EMG noise level approximation in ECG signals. Biomed. Signal Process. Control 2017, 34, 158–165. [Google Scholar] [CrossRef]
- Christov, I.I.; Daskalov, I.K. Filtering of electromyogram artifacts from the electrocardiogram. Med. Eng. Phys. 1999, 21, 731–736. [Google Scholar] [CrossRef]
- Joy, J.; Manimegalai, P. Wavelet based EMG artifact removal from ECG signal. J. Eng. Comp. Appl. Sci. 2013, 2, 55–58. [Google Scholar]
- Belgurzi, A.N.S.; Elshafiey, I. A Power Line Interference Canceler using Wavelet Transform and Adaptive Filter for ECG Signal. In Proceedings of the 2017 International Conference on Computer and Applications (ICCA), Doha, United Arab Emirates, 6–7 September 2017; pp. 206–210. [Google Scholar]
- Dobrev, D.; Neycheva, T.; Krasteva, V.; Iliev, I. High-Q comb FIR filter for mains interference elimination. Annu. J. Electron. 2010, 4, 126–129. [Google Scholar]
- Kocoń, S.; Piskorowski, J. Digital finite impulse response notch filter with non-zero initial conditions, based on an infinite impulse response prototype filter. Metrol. Meas. Syst. 2012, 19, 767–776. [Google Scholar] [CrossRef]
- Rieta, J.J.; Zarzoso, V.; Millet-Roig, J.; Garcia-Civera, R.; Ruiz-Granell, R. Atrial activity extraction based on blind source separation as an alternative to QRST cancellation for atrial fibrillation analysis. In Computers in Cardiology 2000. Vol.27 (Cat. 00CH37163); IEEE: Piscataway, NJ, USA, 2020. [Google Scholar] [CrossRef]
- Warmerdam, G.J.J.; Vullings, R.; Schmitt, L.; Van Laar, J.O.E.H.; Bergmans, J.W.M. A Fixed-Lag Kalman Smoother to Filter Power Line Interference in Electrocardiogram Recordings. IEEE Trans. Biomed. Eng. 2016, 64, 1852–1861. [Google Scholar] [CrossRef]
- Marques, J.A.L.; Cortez, P.C.; Madeiro, J.P.D.V.; Fong, S.J.; Schlindwein, F.S.; De Albuquerque, V.H.C. Automatic Cardiotocography Diagnostic System Based on Hilbert Transform and Adaptive Threshold Technique. IEEE Access 2019, 7, 73085–73094. [Google Scholar] [CrossRef]
- Hamilton, P. A comparison of adaptive and nonadaptive filters for reduction of power line interference in the ECG. IEEE Trans. Biomed. Eng. 1996, 43, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Taralunga, D.D.; Gussi, I.; Strungaru, R. Fetal ECG enhancement: Adaptive power line interference cancellation based on Hilbert Huang Transform. Biomed. Signal Process. Control 2015, 19, 77–84. [Google Scholar] [CrossRef]
- Levkov, C.; Mihov, G.; Ivanov, R.; Daskalov, I.; Christov, I.; Dotsinsky, I. Removal of power-line interference from the ECG: A review of the subtraction procedure. Biomed. Eng. Online 2005, 4, 50. [Google Scholar] [CrossRef]
- Rieta, J.; Castells, F.; Sanchez, C.; Zarzoso, V.; Millet, J. Atrial Activity Extraction for Atrial Fibrillation Analysis Using Blind Source Separation. IEEE Trans. Biomed. Eng. 2004, 51, 1176–1186. [Google Scholar] [CrossRef]
- von Borries, R.; Pierluissi, J.; Nazeran, H. Wavelet Transform-Based ECG Baseline Drift Removal for Body Surface Potential Mapping. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 31 August–3 September 2005; pp. 3891–3894. [Google Scholar]
- Sayadi, O.; Shamsollahi, M.B. Multiadaptive Bionic Wavelet Transform: Application to ECG Denoising and Baseline Wandering Reduction. EURASIP J. Adv. Signal Process. 2007, 2007, 041274. [Google Scholar] [CrossRef]
- Tinati, B.M.A. ECG baseline wander elimination using wavelet packets. World Acad. Sci. Eng. Technol. 2005, 3, 14–16. [Google Scholar]
- Mamun, M.M.R.K.; Alouani, A.T. Cuffless Blood Pressure Measurement Using Linear and Nonlinear Optimized Feature Selection. Diagnostics 2022, 12, 408. [Google Scholar] [CrossRef]
- Petrenas, A.; Marozas, V.; Sornmo, L.; Lukosevicius, A. An Echo State Neural Network for QRST Cancellation During Atrial Fibrillation. IEEE Trans. Biomed. Eng. 2012, 59, 2950–2957. [Google Scholar] [CrossRef]
- Guzik, P.; Piskorski, J.; Krauze, T.; Wykretowicz, A.; Wysocki, H. Heart rate asymmetry by Poincaré plots of RR intervals. Biomed. Eng. 2006, 51, 272–275. [Google Scholar] [CrossRef]
- Yakut, Ö.; Bolat, E.D. An improved QRS complex detection method having low computational load. Biomed. Signal Process. Control 2018, 42, 230–241. [Google Scholar] [CrossRef]
- Park, J.; Lee, S.; Jeon, M. Atrial fibrillation detection by heart rate variability in Poincare plot. Biomed. Eng. Online 2009, 8, 38. [Google Scholar] [CrossRef]
- Lin, C.-C.; Chang, H.-Y.; Huang, Y.-H.; Yeh, C.-Y. A Novel Wavelet-Based Algorithm for Detection of QRS Complex. Appl. Sci. 2019, 9, 2142. [Google Scholar] [CrossRef]
- Lee, J.S.; Lee, S.J.; Choi, M.; Seo, M.; Kim, S.W. QRS detection method based on fully convolutional networks for capacitive electrocardiogram. Expert Syst. Appl. 2019, 134, 66–78. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, BME-32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.F.; Kumar, N.A.; Burbano-Fernandez, M.; Ramirez-Gonzalez, G.; Abdulhay, E.; De Albuquerque, V.H.C. An Automated Remote Cloud-Based Heart Rate Variability Monitoring System. IEEE Access 2018, 6, 77055–77064. [Google Scholar] [CrossRef]
- Marinho, L.B.; Nascimento, N.d.M.; Souza, J.W.M.; Gurgel, M.V.; Filho, P.P.R.; de Albuquerque, V.H.C. A novel electrocardiogram feature extraction approach for cardiac arrhythmia classification. Futur. Gener. Comput. Syst. 2019, 97, 564–577. [Google Scholar] [CrossRef]
- Nascimento, N.M.M.; Marinho, L.B.; Peixoto, S.A.; Madeiro, J.P.D.V.; de Albuquerque, V.H.C.; Filho, P.P.R. Heart Arrhythmia Classification Based on Statistical Moments and Structural Co-occurrence. Circuits Syst. Signal Process. 2019, 39, 631–650. [Google Scholar] [CrossRef]
- Mahajan, R.; Kamaleswaran, R.; Howe, J.A.; Akbilgic, O. Cardiac Rhythm Classification from a Short Single Lead ECG Recording via Random Forest. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Kora, P. ECG based Myocardial Infarction detection using Hybrid Firefly Algorithm. Comput. Methods Programs Biomed. 2017, 152, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Goharrizi, M.A.B.; Teimourpour, A.; Falah, M.; Hushmandi, K.; Isfeedvajani, M.S. Multi-lead ECG heartbeat classification of heart disease based on HOG local feature descriptor. Comput. Methods Programs Biomed. Update 2023, 3, 100093. [Google Scholar]
- Nandanwar, J.; Singh, J.; Patidar, S. ECG Signals- Early detection of Arrhythmia using Machine Learning approaches. In Proceedings of the 2023 13th International Conference on Cloud Computing, Data Science & Engineering (Confluence), Noida, India, 19–20 January 2023; pp. 32–38. [Google Scholar]
- Dhanamjayulu, C.; Suraj, G.V.; Nikhil, M.; Kaluri, R.; Koppu, S. A Machine Learning Algorithm-Based IoT-Based Message Alert System for Predicting Coronary Heart Disease. In International Conference on Advancements in Smart Computing and Information Security; Springer: Cham, Switzerland, 2022; pp. 362–376. [Google Scholar]
- Ahamad, G.N.; Shafiullah; Fatima, H.; Imdadullah; Zakariya, S.M.; Abbas, M.; Alqahtani, M.S.; Usman, M. Influence of Optimal Hyperparameters on the Performance of Machine Learning Algorithms for Predicting Heart Disease. Processes 2023, 11, 734. [Google Scholar] [CrossRef]
- Geweid, G.G.; Chen, J.D. Automatic classification of atrial fibrillation from short single-lead ECG recordings using a Hybrid Approach of Dual Support Vector Machine. Expert Syst. Appl. 2022, 198, 116848. [Google Scholar] [CrossRef]
- Mazidi, M.H.; Eshghi, M.; Raoufy, M.R. Premature Ventricular Contraction (PVC) Detection System Based on Tunable Q-Factor Wavelet Transform. J. Biomed. Phys. Eng. 2022, 12, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Fu, G.; Struppa, D.; Abudayyeh, I.; Contractor, T.; Anderson, K.; Chu, H.; Rakovski, C. A High Precision Machine Learning-Enabled System for Predicting Idiopathic Ventricular Arrhythmia Origins. Front. Cardiovasc. Med. 2022, 9, 809027. [Google Scholar] [CrossRef]
- He, K.; Liang, W.; Liu, S.; Bian, L.; Xu, Y.; Luo, C.; Li, Y.; Yue, H.; Yang, C.; Wu, Z. Long-term single-lead electrocardiogram monitoring to detect new-onset postoperative atrial fibrillation in patients after cardiac surgery. Front. Cardiovasc. Med. 2022, 9, 1001883. [Google Scholar] [CrossRef]
- Naz, M.; Shah, J.H.; Khan, M.A.; Sharif, M.; Raza, M.; Damaševičius, R. From ECG signals to images: A transformation based approach for deep learning. PeerJ Comput. Sci. 2021, 7, e386. [Google Scholar] [CrossRef]
- Grogan, M.; Lopez-Jimenez, F.; Cohen-Shelly, M.; Dispenzieri, A.; Attia, Z.I.; Ezzedine, O.F.A.; Lin, G.; Kapa, S.; Borgeson, D.D.; Friedman, P.A.; et al. Artificial Intelligence–Enhanced Electrocardiogram for the Early Detection of Cardiac Amyloidosis. Mayo Clin. Proc. 2021, 96, 2768–2778. [Google Scholar] [CrossRef]
- Wang, X.; Li, R.; Wang, S.; Shen, S.; Zhang, W.; Zhou, B.; Wang, Z. Automatic diagnosis of ECG disease based on intelligent simulation modeling. Biomed. Signal Process. Control 2021, 67, 102528. [Google Scholar] [CrossRef]
- Houssein, E.H.; Ibrahim, I.E.; Neggaz, N.; Hassaballah, M.; Wazery, Y.M. An efficient ECG arrhythmia classification method based on Manta ray foraging optimization. Expert Syst. Appl. 2021, 181, 115131. [Google Scholar] [CrossRef]
- Chumrit, N.; Weangwan, C.; Aunsri, N. ECG-based Arrhythmia Detection using Average Energy and Zero-crossing Features with Support Vector Machine. In Proceedings of the 2020 5th International Conference on Information Technology (InCIT), Chonburi, Thailand, 21–22 October 2020; pp. 282–287. [Google Scholar]
- Mazaheri, V.; Khodadadi, H. Heart arrhythmia diagnosis based on the combination of morphological, frequency and nonlinear features of ECG signals and metaheuristic feature selection algorithm. Expert Syst. Appl. 2020, 161, 113697. [Google Scholar] [CrossRef]
- Subramanian, K.; Prakash, N.K. Machine Learning based Cardiac Arrhythmia detection from ECG signal. In Proceedings of the 2020 Third International Conference on Smart Systems and Inventive Technology (ICSSIT), Tirunelveli, India, 20–22 August 2020; pp. 1137–1141. [Google Scholar]
- Wang, Z.; Qian, L.; Han, C.; Shi, L. Application of multi-feature fusion and random forests to the automated detection of myocardial infarction. Cogn. Syst. Res. 2019, 59, 15–26. [Google Scholar] [CrossRef]
- Yang, W.; Si, Y.; Wang, D.; Zhang, G.; Liu, X.; Li, L. Automated intra-patient and inter-patient coronary artery disease and congestive heart failure detection using EFAP-Net. Knowl.-Based Syst. 2020, 201, 106083. [Google Scholar] [CrossRef]
- Bashar, S.K.; Ding, E.; Albuquerque, D.; Winter, M.; Binici, S.; Walkey, A.J.; McManus, D.D.; Chon, K.H. Atrial Fibrillation Detection in ICU Patients: A Pilot Study on MIMIC III Data. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 298–301. [Google Scholar]
- Kong, D.; Zhu, J.; Wu, S.; Duan, C.; Lu, L.; Chen, D. A novel IRBF-RVM model for diagnosis of atrial fibrillation. Comput. Methods Programs Biomed. 2019, 177, 183–192. [Google Scholar] [CrossRef]
- Mahmood, I.S.; Abdelrahman, I.A.M. A Comparison between Different Classifiers for Diagnoses of Atrial Fibrillation. In Proceedings of the 2019 International Conference on Computer, Control, Electrical, and Electronics Engineering (ICCCEEE), Khartoum, Sudan, 21–23 September 2019; pp. 1–6. [Google Scholar]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef]
- Attia, Z.I.; Kapa, S.; Lopez-Jimenez, F.; McKie, P.M.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Enriquez-Sarano, M.; Noseworthy, P.A.; Munger, T.M.; et al. Screening for cardiac contractile dysfunction using an artificial intelligence–enabled electrocardiogram. Nat. Med. 2019, 25, 70–74. [Google Scholar] [CrossRef]
- Lokhande, P.P.; Chinnaiah, K. Cardiac Disease Detection Using IoT-Enabled ECG Sensors and Deep Learning Approach. In International Conference on Advanced Communication and Intelligent Systems; Springer: Cham, Switzerland, 2022; pp. 195–204. [Google Scholar]
- Wang, Z.; Stavrakis, S.; Yao, B. Hierarchical deep learning with Generative Adversarial Network for automatic cardiac diagnosis from ECG signals. Comput. Biol. Med. 2023, 155, 106641. [Google Scholar] [CrossRef]
- Akbilgic, O.; Karabayir, I.; Butler, L.; Güntürkün, F.; Chinthala, L.; Jefferies, J.L.; Baykaner, T.; Herrington, D.M.; Soliman, E.Z.; Davis, R. A real world evidence for the performance of an ecg-ai based heart failure risk predictor. J. Am. Coll. Cardiol. 1985, 81 (Suppl. S8), 727. [Google Scholar] [CrossRef]
- Munawar, S.; Angappan, G.; Konda, S. Arrhythmia Classification Based on Bi-Directional Long Short-Term Memory and Multi-Task Group Method. Int. J. E-Collab. 2023, 19, 1–18. [Google Scholar] [CrossRef]
- Li, Y.; Luo, J.-H.; Dai, Q.-Y.; Eshraghian, J.K.; Ling, B.W.-K.; Zheng, C.-Y.; Wang, X.-L. A deep learning approach to cardiovascular disease classification using empirical mode decomposition for ECG feature extraction. Biomed. Signal Process. Control 2023, 79, 104188. [Google Scholar] [CrossRef]
- Bhaskarpandit, S.; Gade, A.; Dash, S.; Dash, D.K.; Tripathy, R.K.; Pachori, R.B. Detection of Myocardial Infarction From 12-Lead ECG Trace Images Using Eigendomain Deep Representation Learning. IEEE Trans. Instrum. Meas. 2023, 72, 1–12. [Google Scholar] [CrossRef]
- Mahajan, R.; Pundir, P.; Gambhir, A.; Adumala, S. ECG-based deep learning framework to identify ventricular arrhythmias in patients monitored with mct. J. Am. Coll. Cardiol. 2023, 81, 2176. [Google Scholar] [CrossRef]
- Leema, A.; Nagaraj, J. A deep learning framework for automatic cardiovascular classification from Electrocardiogram Images. Res. Sq. 2023. [Google Scholar] [CrossRef]
- Wang, Z.; Jin, B.; Li, S.; Zhang, F.; Zhang, W. ECG-grained Cardiac Monitoring Using UWB Signals. Proc. Acm Interact. Mob. Wearable Ubiquitous Technol. 2022, 6, 1–25. [Google Scholar] [CrossRef]
- Ismail, A.R.; Jovanovic, S.; Ramzan, N.; Rabah, H. ECG Classification Using an Optimal Temporal Convolutional Network for Remote Health Monitoring. Sensors 2023, 23, 1697. [Google Scholar] [CrossRef] [PubMed]
- Maurya, J.P.; Manoria, M.; Joshi, S. Cardiac Arrhythmia Classification Using Cascaded Deep Learning Approach (LSTM & RNN). In Proceedings of the International Conference on Machine Learning, Image Processing, Network Security and Data Sciences, Virtual Event, 19–20 January 2023; pp. 3–13. [Google Scholar]
- Monaci, S.; Qian, S.; Gillette, K.; Puyol-Antón, E.; Mukherjee, R.; Elliott, M.K.; Whitaker, J.; Rajani, R.; O’neill, M.; Rinaldi, C.A.; et al. Non-invasive localization of post-infarct ventricular tachycardia exit sites to guide ablation planning: A computational deep learning platform utilizing the 12-lead electrocardiogram and intracardiac electrograms from implanted devices. Europace 2022, 25, 469–477. [Google Scholar] [CrossRef]
- Allam, J.P.; Samantray, S.; Ari, S. Patient-specific ECG beat classification using EMD and deep learning-based technique. In Advanced Methods in Biomedical Signal Processing and Analysis; Academic Press: Cambridge, MA, USA, 2023; pp. 87–108. [Google Scholar]
- Alsheikhy, A.; Said, Y.F.; Shawly, T.; Lahza, H. A Model to Predict Heartbeat Rate Using Deep Learning Algorithms. Healthcare 2023, 11, 330. [Google Scholar] [CrossRef]
- Zhao, X.; Huang, G.; Wu, L.; Wang, M.; He, X.; Wang, J.-R.; Zhou, B.; Liu, Y.; Lin, Y.; Liu, D.; et al. Deep learning assessment of left ventricular hypertrophy based on electrocardiogram. Front. Cardiovasc. Med. 2022, 9, 952089. [Google Scholar] [CrossRef]
- Liu, P.; Sun, X.; Han, Y.; He, Z.; Zhang, W.; Wu, C. Arrhythmia classification of LSTM autoencoder based on time series anomaly detection. Biomed. Signal Process. Control 2021, 71, 103228. [Google Scholar] [CrossRef]
- Radhakrishnan, T.; Karhade, J.; Ghosh, S.; Muduli, P.; Tripathy, R.; Acharya, U.R. AFCNNet: Automated detection of AF using chirplet transform and deep convolutional bidirectional long short term memory network with ECG signals. Comput. Biol. Med. 2021, 137, 104783. [Google Scholar] [CrossRef] [PubMed]
- Wang, J. Automated detection of premature ventricular contraction based on the improved gated recurrent unit network. Comput. Methods Programs Biomed. 2021, 208, 106284. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Paul, A.; Agarwal, A.; Jindal, S.K. Real Time Arrhythmia Detecting Wearable using a Novel Deep Learning Model. In Proceedings of the 2020 International Conference on Interdisciplinary Cyber Physical Systems (ICPS), Chennai, India, 28–29 December 2020; pp. 14–19. [Google Scholar]
- Rajpurkar, P.; Hannun, A.Y.; Haghpanahi, M.; Bourn, C.; Ng, A.Y. Cardiologist-level arrhythmia detection with convolutional neural networks. arXiv 2017, arXiv:1707.01836. [Google Scholar]
- Zhai, X.; Tin, C. Automated ECG Classification Using Dual Heartbeat Coupling Based on Convolutional Neural Network. IEEE Access 2018, 6, 27465–27472. [Google Scholar] [CrossRef]
- Huang, J.; Chen, B.; Yao, B.; He, W. ECG Arrhythmia Classification Using STFT-Based Spectrogram and Convolutional Neural Network. IEEE Access 2019, 7, 92871–92880. [Google Scholar] [CrossRef]
- Liu, W.; Huang, Q.; Chang, S.; Wang, H.; He, J. Multiple-feature-branch convolutional neural network for myocardial infarction diagnosis using electrocardiogram. Biomed. Signal Process. Control 2018, 45, 22–32. [Google Scholar] [CrossRef]
- Niu, J.; Tang, Y.; Sun, Z.; Zhang, W. Inter-Patient ECG Classification With Symbolic Representations and Multi-Perspective Convolutional Neural Networks. IEEE J. Biomed. Health Inform. 2019, 24, 1321–1332. [Google Scholar] [CrossRef]
- Acharya, U.R.; Fujita, H.; Oh, S.L.; Raghavendra, U.; Tan, J.H.; Adam, M.; Gertych, A.; Hagiwara, Y. Automated identification of shockable and non-shockable life-threatening ventricular arrhythmias using convolutional neural network. Futur. Gener. Comput. Syst. 2018, 79, 952–959. [Google Scholar] [CrossRef]
- Tan, J.H.; Hagiwara, Y.; Pang, W.; Lim, I.; Oh, S.L.; Adam, M.; Tan, R.S.; Chen, M.; Acharya, U.R. Application of stacked convolutional and long short-term memory network for accurate identification of CAD ECG signals. Comput. Biol. Med. 2018, 94, 19–26. [Google Scholar] [CrossRef]
- Yao, Q.; Wang, R.; Fan, X.; Liu, J.; Li, Y. Multi-class Arrhythmia detection from 12-lead varied-length ECG using Attention-based Time-Incremental Convolutional Neural Network. Inf. Fusion 2019, 53, 174–182. [Google Scholar] [CrossRef]
- Lih, O.S.; Jahmunah, V.; San, T.R.; Ciaccio, E.J.; Yamakawa, T.; Tanabe, M.; Kobayashi, M.; Faust, O.; Acharya, U.R. Comprehensive electrocardiographic diagnosis based on deep learning. Artif. Intell. Med. 2020, 103, 101789. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Sim, G.; Matuszewski, B. Inter-patient ECG classification with convolutional and recurrent neural networks. Biocybern. Biomed. Eng. 2019, 39, 868–879. [Google Scholar] [CrossRef]
- Andersen, R.S.; Peimankar, A.; Puthusserypady, S. A deep learning approach for real-time detection of atrial fibrillation. Expert Syst. Appl. 2018, 115, 465–473. [Google Scholar] [CrossRef]
- Liu, H.; Cui, S.; Zhao, X.; Cong, F. Detection of obstructive sleep apnea from single-channel ECG signals using a CNN-transformer architecture. Biomed. Signal Process. Control 2023, 82, 104581. [Google Scholar] [CrossRef]
- Srivastava, G.; Chauhan, A.; Kargeti, N.; Pradhan, N.; Dhaka, V.S. ApneaNet: A hybrid 1DCNN-LSTM architecture for detection of Obstructive Sleep Apnea using digitized ECG signals. Biomed. Signal Process. Control 2023, 84, 104754. [Google Scholar] [CrossRef]
- Tyagi, P.K.; Agrawal, D. Automatic detection of sleep apnea from single-lead ECG signal using enhanced-deep belief network model. Biomed. Signal Process. Control 2023, 80, 104401. [Google Scholar] [CrossRef]
- Yue, H.; Li, P.; Li, Y.; Lin, Y.; Huang, B.; Sun, L.; Ma, W.; Fan, X.; Wen, W.; Lei, W. Validity study of a multi-scaled fusion network using single-lead electrocardiogram signals for obstructive sleep apnea diagnosis. J. Clin. Sleep Med. 2023, 19, 1017–1025. [Google Scholar] [CrossRef]
- Jothi, E.S.J.; Anitha, J.; Priyadharshini, J.; Hemanth, D.J. Deep Learning Based Obstructive Sleep Apnea Detection for e-health Applications. In International Conference on Electronic Governance with Emerging Technologies; Springer: Cham, Switzerland, 2022; pp. 1–11. [Google Scholar]
- Rathore, K.S.; Sricharan, V.; Preejith, S.; Sivaprakasam, M. MRNet—A Deep Learning Based Multitasking Model for Respiration Rate Estimation in Practical Settings. In Proceedings of the 2022 IEEE 10th International Conference on Serious Games and Applications for Health(SeGAH), Sydney, Australia, 10–12 August 2022; pp. 1–6. [Google Scholar]
- Kumar, A.K.; Ritam, M.; Han, L.; Guo, S.; Chandra, R. Deep learning for predicting respiratory rate from biosignals. Comput. Biol. Med. 2022, 144, 105338. [Google Scholar] [CrossRef]
- Liu, J.; Xu, H.; Wang, J.; Peng, X.; He, C. Non-invasive diagnosis of fetal arrhythmia based on multi-domain feature and hierarchical extreme learning machine. Biomed. Signal Process. Control 2023, 79, 104191. [Google Scholar] [CrossRef]
- Al-Saadany, D.; Attallah, O.; Elzaafarany, K.; Nasser, A.A.A. A Machine Learning Framework for Fetal Arrhythmia Detection via Single ECG Electrode. In International Conference on Computational Science; Springer: Cham, Switzerland, 2022; pp. 546–553. [Google Scholar]
- Baghel, N.; Burget, R.; Dutta, M.K. 1D-FHRNet: Automatic Diagnosis of Fetal Acidosis from Fetal Heart Rate Signals. Biomed. Signal Process. Control 2021, 71, 102794. [Google Scholar] [CrossRef]
- Nakatani, S.; Yamamoto, K.; Ohtsuki, T. Fetal Arrhythmia Detection based on Deep Learning using Fetal ECG Signals. In Proceedings of the GLOBECOM 2022—2022 IEEE Global Communications Conference, Rio de Janeiro, Brazil, 4–8 December 2022; pp. 2266–2271. [Google Scholar]
- Long, W.; Wang, X. BPNet: A multi-modal fusion neural network for blood pressure estimation using ECG and PPG. Biomed. Signal Process. Control 2023, 86, 105287. [Google Scholar] [CrossRef]
- Mamun, M.M.R.K.; Alouani, A. Using Photoplethysmography & ECG Towards a Non-Invasive Cuff less Blood Pressure Measurement Technique. In Proceedings of the 2019 IEEE Canadian Conference of Electrical and Computer Engineering (CCECE), Edmonton, AB, Canada, 5–8 May 2019; pp. 1–4. [Google Scholar]
- Bose S, S.N. Dual-Stage Learning Approach towards Continuous Cuffless Blood Pressure Monitoring; Innovations in Information and Communication Technology Series; IJAICT India Publications: Waterloo, ON, Canada, 2020; pp. 369–372. [Google Scholar] [CrossRef]
- Mamun, M.M.R.K.; Sherif, A. Advancement in the Cuffless and Noninvasive Measurement of Blood Pressure: A Review of the Literature and Open Challenges. Bioengineering 2022, 10, 27. [Google Scholar] [CrossRef]
- Mamun, M.M.R.K. Cuff-less blood pressure measurement based on hybrid feature selection algorithm and multi-penalty regularized regression technique. Biomed. Phys. Eng. Express 2021, 7, 065030. [Google Scholar] [CrossRef]
- Attia, Z.I.; Harmon, D.M.; Behr, E.R.; Friedman, P.A. Application of artificial intelligence to the electrocardiogram. Eur. Heart J. 2021, 42, 4717–4730. [Google Scholar] [CrossRef]
- Weil, E.L.; Noseworthy, P.A.; Lopez, C.L.; Rabinstein, A.A.; Friedman, P.A.; Attia, Z.I.; Yao, X.; Siontis, K.C.; Kremers, W.K.; Christopoulos, G.; et al. Artificial Intelligence–Enabled Electrocardiogram for Atrial Fibrillation Identifies Cognitive Decline Risk and Cerebral Infarcts. Mayo Clin. Proc. 2022, 97, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Park, S.; Kwon, S.-H.; Cho, K.-H.; Lee, H. AI-Based Stroke Disease Prediction System Using ECG and PPG Bio-Signals. IEEE Access 2022, 10, 43623–43638. [Google Scholar] [CrossRef]
- Chau, T.; Lin, C.-S.; Shang, H.-S.; Fang, W.-H.; Lee, D.-J.; Lee, C.-C.; Tsai, S.-H.; Wang, C.-H.; Lin, S.-H. Point-of-care artificial intelligence-enabled ECG for dyskalemia: A retrospective cohort analysis for accuracy and outcome prediction. NPJ Digit. Med. 2022, 5, 8. [Google Scholar] [CrossRef]
- Dash, D.P.; Kolekar, M.H.; Chakraborty, C.; Khosravi, M.R. Review of Machine and Deep Learning Techniques in Epileptic Seizure Detection using Physiological Signals and Sentiment Analysis. ACM Trans. Asian Low-Resour. Lang. Inf. Process. 2022. [Google Scholar] [CrossRef]
- Chen, S.; Zheng, R.; Wang, T.; Jiang, T.; Gao, F.; Wang, D.; Cao, J. Deterministic Learning-Based WEST Syndrome Analysis and Seizure Detection on ECG. IEEE Trans. Circuits Syst. II Express Briefs 2022, 69, 4603–4607. [Google Scholar] [CrossRef]
- McInnis, R.P.; Ayub, M.A.; Jing, J.; Halford, J.J.; Mateen, F.J.; Westover, M.B. Epilepsy diagnosis using a clinical decision tool and artificially intelligent electroencephalography. Epilepsy Behav. 2023, 141, 109135. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The article selection process for the literature review.

Figure 2.
An example of an ECG wave with waves and segments highlighted [51] CC by 4.0.
Figure 2.
An example of an ECG wave with waves and segments highlighted [51] CC by 4.0.

Figure 3.
An example of an ECG wave with and without baseband wander [51] CC by 4.0.
Figure 3.
An example of an ECG wave with and without baseband wander [51] CC by 4.0.

Figure 4.
Machine learning framework using ECG data.

Figure 5.
Future research directions.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Current literature survey on using ECG with AI for diagnosis.
| Reference | Year | Aspects (First: ECG Is the Primary Signal, Second: AI Is the Focus Technology; Third: Sufficient Discussion on Challenges and Future Directions | Summary | Limitations |
|---|---|---|---|---|
| [21] | 2019 | 1 and 2 | Focus:
| Lacks:
|
| [22] | 2020 | 1 and 3 | Focus:
| Lacks:
|
| [23] | 2020 | 1, partial 2 and 3 | Focus:
| Lacks:
|
| [24] | 2020 | 1 and partial 2 | Focus:
| Lacks:
|
| [25] | 2021 | 1, partial 2 and patial 3 | Focus:
| Lacks:
|
| [26] | 2021 | 1, 2 and 3 | Focus:
| Lacks:
|
| [27] | 2021 | 1, partial 2 and 3 | Focus:
| Lacks:
|
| [28] | 2022 | 1, partial 2 and 3 | Focus:
| Lacks:
|
| [29] | 2022 | 1, partial 2 and 3 | Focus:
| Lacks:
|
| [30] | 2022 | 1 and 2 | Focus:
| Lacks:
|
| [31] | 2022 | 1, partial 2 and 3 | Focus:
| Lacks:
|
| [32] | 2022 | 1, partial 2 and partial 3 | Focus:
| Lacks:
|
| [33] | 2023 | 1 and 2 | Focus:
| Lacks:
|
| [34] | 2023 | 1, partial 2 and 3 | Focus:
| Lacks:
|
Table 2.
Use of machine learning and ECG data for heart disease diagnosis.
| Ref. | Year | Heart Disease | Algorithm | Summary | Limitations |
|---|---|---|---|---|---|
| [65] | 2023 | Bundle branch block, cardiomyopathy, Dysrhythmia, and myocardial infarction | Support vector machine | Assessing HOG-SVM for precise 15-lead ECG heartbeat disease classification. | Requires a large dataset of ECG signals to train the machine learning models. It is not always accurate, especially for rare or complex arrhythmias. |
| [66] | 2023 | Arrhythmia | Random forest classification, support vector machines | The study highlights the importance of ML in precisely detecting aberrant heartbeats. 98.26% and 100% accuracy are reached across a variety of datasets. | The study used a small dataset of ECG signals, which may not represent the wider population. The study did not consider the impact of noise and artifacts on the ECG signals. |
| [67] | 2023 | Cardiovascular infirmity | Decision tree, Naïve Bayes, KNN, SVM | With an F-measure of 0.95 and an accuracy rate of 95.5%, ML predicts cardiac disease. In comparison to current models, the integration of characteristics and ensembles enhances the prediction of coronary disease. | Small data: 300 patients A few features: Age, gender, blood pressure. |
| [68] | 2023 | General heart condition | Logistic regression, KNN, SVM, DT, RF, GB | Grid search CV innovation: improved accuracy. The results of the experiments found the most influential factors for predicting heart disease. | Small dataset: The study used a small dataset of 296 patients. Not generalizable: The results may not be generalizable to other datasets or populations. |
| [69] | 2022 | AF | Support vector machine | Atrial fibrillation was detected utilizing a hybrid technique with a Dual Support Vector Machine as the primary strategy. | Noisy data: The study did not consider the impact of noise and artifacts on the ECG signals. Single lead: The study only used a single lead ECG recording, which may not be enough to classify atrial fibrillation accurately. |
| [70] | 2022 | Premature ventricular contraction | Support vector machine, K nearest neighbor | 22 ECG recordings were provided via the MIT/BIH arrhythmia database. Q-factor wavelet generated sub-bands while reducing noise. ANOVA for feature extraction and a variety of ML methods for evaluation. | Noisy data: The study did not consider the impact of noise and artifacts on the ECG signals. Single algorithm: The study only evaluated the performance of a single algorithm, KNN. |
| [71] | 2022 | Arrhythmia | Gradient boosting | ECGs from 18,612 CA success patients were examined. Four classification schemes are created and compared by ML models. IVA origin prediction has a high 98.24% accuracy, outperforming previous studies and human experts. | Single type: The study only considered a single type of idiopathic ventricular arrhythmia. Real-world: The study was not conducted in a real-world clinical setting. |
| [72] | 2022 | AF | Support vector machine | P-wave characteristics that indicate postoperative atrial fibrillation are the focus of this study. | Single-lead ECG: The study used a single-lead ECG, which may not be as sensitive as a 12-lead ECG. Retrospective data: The data were collected retrospectively, which may introduce bias. |
| [73] | 2021 | Ventricular arrhythmia | Support vector machine | The suggested deep learning approach for diagnosing VA makes use of Cubic SVM. 97.6% accuracy is achieved on the MIT-BIH dataset. | Requires ECG signal preprocessing: The proposed method requires ECG signal preprocessing, which can be time-consuming and error-prone. Not generalizable to all arrhythmias: The method was only evaluated on a small number of arrhythmias, so it is unclear how generalizable it is to other arrhythmias. |
| [74] | 2021 | Amyloid builds up in organs | KNN | This research aims to create an AI-powered tool to recognize cardiac amyloidosis by analyzing a conventional 12-lead electrocardiogram. | Unclear generalizability: How the results would generalize to other populations or settings is unclear. Need for validation: The model needs to be validated in a more extensive and more diverse population before it can be used in clinical practice. |
| [75] | 2021 | CVD | ML | Simulation modeling is used in the work to diagnose ECG disorders automatically. Includes waveform localization, denoising, and ML-based disease identification and feature extraction. | Noisy data: The study did not consider the impact of noise and artifacts on the ECG signals. Single model: The study only used a single machine learning model, which may not be generalizable to other datasets or conditions. |
| [76] | 2021 | Arrhythmia | Support vector machine | ECG descriptors of several types (LBP, wavelet, HOS, morphological) were extracted. MRFO-SVM hybrid for feature selection and classification (MRFO + SVM). Performance enhanced using MIT-BIH Arrhythmia database training. | Limited features: The study only considered a limited number of features, such as the QRS complex and the ST segment. Not interpretable: The model is not interpretable, making it difficult to understand why it makes its predictions. |
| [77] | 2020 | Arrhythmia | Support vector machine | A method for arrhythmia identification using ECG readings is introduced. Uses average energy, zero-crossing values, feature extraction, and SVM classification during preprocessing. Evaluated using the QT, normal sinus rhythm, and MIT-BIH arrhythmia databases. | Limited features: The study only considered two features, average energy and zero-crossing, which may not be sufficient to detect all types of arrhythmias accurately. Noisy data: The study did not consider the impact of noise and artifacts on the ECG recordings, which could affect the accuracy of the detection algorithm. |
| [78] | 2020 | Arrhythmia | KNN | The study developed a computer-aided diagnostic system that automatically classifies and diagnoses seven types of cardiac arrhythmias by analyzing ECG signals. | Limited features: The study only considered a limited number of features, such as heart rate and rhythm. Noisy data: The study did not consider the impact of noise and artifacts on the ECG signals. |
| [79] | 2020 | Arrhythmia | Support vector machine | ECG data are used in the study to assess heart abnormalities that cause arrhythmias. After filtering and segmenting, the R-R interval, BPM, P wave, and QRS peak are extracted. SVM classifier validates the technique’s efficacy with 91% accuracy, improved precision, recall, and F1 score. | Noisy data: The study did not consider the impact of noise and artifacts on the ECG signals. Single classifier: The study only used a single machine learning classifier, which may not be the best approach for all arrhythmias. |
| [80] | 2020 | Myocardial Infarction | RF, SVM, KNN, and NN | The study proposes a new ECG-based MI detection method. Features that were extracted using PCA, statistics, entropy, and data augmentation. In terms of accuracy, sensitivity, specificity, and F1, random forests perform better than SVM, BPNN, and KNN. | Single lead: The study only used a single lead of the ECG signal, which may not be sufficient to detect myocardial infarction accurately. Noisy data: The study did not consider the impact of noise and artifacts on the ECG signals. |
| [81] | 2020 | CVD | Support vector machine | ECG fragment alignment and PCA classification method are introduced. ECG waveform analysis using the MIMIC III dataset is used for AF diagnosis in ICU patients. | Small dataset: The study used a small dataset of 200 patients, which may not represent the wider population. Limited features: The study only considered a limited number of features, such as ECG signals and medical records. |
| [82] | 2019 | AF. | Support vector machine, KNN. | The research described a technique for identifying AF in ICU patients by analyzing the ECG waveform data from the MIMIC III dataset. | The study only evaluated the algorithm’s performance on a single type of AF, so its performance may not be as good for other types of AF. The study did not consider the patient medical history or other clinical factors, which could also affect the diagnosis of AF. |
| [83] | 2019 | AF. | IRBF-RVM, SVM, KNN, Naïve Bayes, AdaBoost, RF | Research suggests using a 12-lead ECG to diagnose AF using the IRBF-RVM model. As diagnostic characteristics, RR intervals are employed. AF classification of 98.16% on ECG Channel II. | Not generalizable: The study was conducted on a single dataset and may not be generalizable to other populations. Sensitive to noise: The model is sensitive to noise in the ECG signals. |
| [84] | 2019 | AF | RF, KNN, SVM | Through comparison research, the study seeks to recommend the best AF classifier for coronary heartbeat detection. | Lack of diversity: The dataset was not diverse, consisting of only young, healthy patients. Noisy data: The ECG signals in the dataset were noisy, which could have affected the accuracy of the classifiers. |
Table 3.
Use of deep learning and ECG data for heart disease diagnosis.
| Reference | Year | Heart Disease | Deep Learning Algorithm | Summary |
|---|---|---|---|---|
| [87] | 2023 | General heart disease | CNN | The suggested system uses the ANOVA-F test as a feature selection technique to organize data efficiently. Using a Convolutional Neural Network Model, it classifies patient data, determines the severity of cardiac illnesses, and swiftly notifies clinicians. Accurate input data from ECG sensors and IoT devices are used. |
| [88] | 2023 | Arrhythmia | Generative Adversarial Network (GAN) | A hierarchical deep learning framework called MadeGAN is presented in this research for the interpretation of ECG signals. MadeGAN combines a Memory-Augmented Deep AutoEncoder with GAN to identify multi-class arrhythmias and anomaly detection. Experimental findings utilizing the MIT-BIH arrhythmia database show that the suggested model performs better than current approaches. |
| [89] | 2023 | Heart failure | ECG-AI model based on deep learning | The effectiveness of ECG-AI in predicting heart failure has been verified using real-world data; ECG-AI could potentially play a crucial role in accurately identifying patients. |
| [90] | 2023 | Arrhythmia | Bi-directional LSTM, CNN, intra LSTM | This study suggests the MTGBi-LSTM approach for categorizing arrhythmias to solve the overfitting issue in CNN. It uses multitask learning and global/intra-LSTM techniques to improve feature selection and avoid local optimum. The MTGBi-LSTM model outperforms the current AFibNet, achieving a 96.48% accuracy and a 97.73% sensitivity on the MIT-BIH dataset. |
| [91] | 2023 | Left/right BBB | CNN | This work emphasizes the usage of a feature picture. It provides a global feature extraction approach for categorizing multi-periodic heartbeats. Empirical Mode Decomposition (EMD) creates the feature picture, successfully depicting the "heartbeat condition." This feature picture is then used by a two-dimensional Convolutional Neural Network (CNN) to classify the patient’s heartbeat status accurately. The efficiency of the suggested technique is demonstrated by the experimental findings, which also indicate how well it can identify and analyze heartbeats. |
| [92] | 2023 | Myocardial infarction | EfficientNetV2B2-based transfer learning model | A new method for automatic detection of myocardial infarction (MI) using 12-lead ECG trace images is introduced in the article through an edge domain-based deep representation learning (DRL) approach. |
| [93] | 2023 | Ventricular arrhythmia | CNN | This study trained a 5-layer 1D convolutional neural network (CNN) using a selected dataset of 46,595 ECG recordings. The model outperformed comparable models in the literature when tested using cross-validation, held-out data, and an external dataset. Using brief, single-lead ECG data, the computationally effective CNN correctly diagnosed ventricular arrhythmia (VA), demonstrating the possibility for accelerated and enhanced patient treatment using MCT monitor data. |
| [94] | 2023 | Myocardial Infraction | DenseNet | Image augmentation techniques are applied to detect Normal, Abnormal Heartbeat and Myocardial infarction (MI) to balance the ECG image dataset classes. |
| [95] | 2023 | Arrhythmia | Conditional generative adversarial network | An accurate ECG is produced using the contactless cardiac monitoring device, RF-ECG, employing ultra-wideband signals. In addition to mapping mechanical-to-electrical cardiac activity, complementary restoration techniques restore pulse signal fluctuation. Results from experiments support its usefulness in identifying heart problems. |
| [96] | 2023 | Abnormal heart rate type | Temporal convolutional network | The paper proposes a novel ML architecture using temporal convolution networks (TCN) for classifying five heart diseases based on ECG signals. |
| [97] | 2023 | Arrhythmia | LSTM and RNN | An LSTM and RNN cascaded model for categorizing ECG signal abnormalities is presented in this study. The suggested model yields a 93.46% sensitivity, an 84.36% specificity, and an 89.9% accuracy. The comparison findings show that LSTM with RNN successfully analyzes ECG signals and is ideal for real-time produced data sequences like ECG. |
| [98] | 2023 | Arrhythmia | MLP | The DL algorithms for locating the earliest systolic activation sites were trained using a library of simulated paced beats and post-infarct VTs. The platform successfully localized VTs from implanted device intracardiac EGMs (mean LE = 13.10 2.36 mm) and surface ECGs (mean LE = 9.61 2.61 mm). Clinical VT localization was in line with the targets for ablation. |
| [99] | 2023 | Abnormal beat classification | DNN | This work suggests a personalized deep learning method for identifying ECG beats. Preprocessing employs EMD to break down beats into intrinsic mode functions (IMFs) and segment the signal based on R-peaks. A deep learning-based bespoke model is used to recognize beats utilizing certain IMFs. The method accurately detects ECG beats by removing important data using convolutional layers with various steps. |
| [100] | 2023 | Abnormal heart rate type | AlexNet, CNN, LSTMs, and ResNet50V2 | The article introduces a practical and reliable approach for determining the average heart rate by analyzing the reflected light on the skin. |
| [101] | 2022 | LVH | LSTM and CNN | Using a 12-lead ECG, a CNN-LSTM DL model was created to identify left ventricular hypertrophy (LVH). One thousand eight hundred sixty-three patients’ echocardiogram and ECG data were examined, and the model was developed and evaluated using various patient subgroups according to gender and relative wall thickness. |
| [102] | 2022 | Arrhythmia | CNN, LSTM, autoencoder | Utilizing a network layer design based on LSTM, the team optimized an autoencoder structure that increases the precision of arrhythmia classification when used alongside their ECG preprocessing process. |
| [103] | 2021 | AF | CNN and LSTM | Using ECG signals and deep learning-based techniques in the time-frequency domain to identify AF and differentiate between terminating and non-terminating AF episodes. |
| [104] | 2021 | Premature ventricular contraction | G.R.U., CNN | In order to enhance the recognition of PVC signals, the paper presents a modified gated recurrent unit model that integrates a scale parameter into the current bidirectional GRU model. |
| [105] | 2021 | Arrhythmia | LSTM and CNN | The article aimed to develop a wearable application that uses signal preprocessing and a deep learning model comprising 1-D CNN and LSTM. |
Table 4.
Use of machine learning and deep learning using ECG data for other health conditions.
| Ref. | Year | Health Problem | Algorithm | Vital Parameter | Summary |
|---|---|---|---|---|---|
| [117] | 2023 | Obstructive sleep apnea (OSA) | CNN-transformer | Single channel ECG | From single-channel ECG data, OSA was identified using a CNN-Transformer architecture. The model consists of two components: a Transformer for global context modeling and a CNN for feature learning. The approach obtained an 88.2% accuracy and a 0.95 AUC for segment classification, while for recording classification, it reached a 100% accuracy and a 4.33 MAE. |
| [118] | 2023 | Obstructive sleep apnea | 1D CNN-LSTM | ECG signal | The initial model, which used a modified Alexnet architecture with a long short-term memory layer added, had an accuracy rate of 90.87%. The accuracy of the second model, ApneaNet, was 90.13% while using fewer processing resources. Both models showed promising results and the real-time ability to identify sleep apnea. |
| [119] | 2023 | Obstructive sleep apnea | Deep Belief Networks (DBN) | ECG signal and ECG-derived respiration | The technique used two types of Deep Belief Network (DBN) structures with Restricted Boltzmann Machines (RBM). The suggested method outperformed previous SLA detection techniques, achieving an accuracy of 89.11% for per-segment detection and 97.17% for per-recording detection. |
| [120] | 2023 | Obstructive sleep apnea | Multi-scaled fusion network | Single channel ECG | On an FAH-ECG dataset, a squeeze-and-excitation and multiscale fusion network (SE-MSCNN) algorithm demonstrated strong agreement with manual scoring and attained an accuracy of 86.6%. The SE-MSCNN may make creating wearable technology for effective obstructive sleep apnea screening easier. |
| [121] | 2023 | Obstructive sleep apnea | CNN and LSTM | ECG and PPG | 200 ECG and PPG signals were recorded for the investigation using publicly accessible apnea databases. The DC-LSTM network attained a 98.2% accuracy rate, a 97.4% sensitivity rate, a 97.5% specificity rate, and a 0.92 Kappa coefficient. These outcomes are equivalent to those of fully automated algorithms, making it appropriate for OSA e-health monitoring carried out at home. |
| [122] | 2022 | Respiration rate | Deep learning | ECG, PPG, and accelerometer | The study proposes a new multitasking deep learning network that simultaneously forecasts respiratory rate and waveform, which ultimately helps reduce error rates across different activities. |
| [123] | 2022 | Respiration rate | CNN-LSTM | ECG, PPG, and EMG | The models were assessed using two window sizes—32 s and 64 s—based on mean absolute error (MAE). The 64 s timeframe produced more accurate forecasts, according to the results. Bi-LSTM with Bahdanau attention outperformed the other models in terms of how well it handled the bio-signals, especially when it came to sEMG-based data (MAE of 0.51 0.03) and PPG/ECG-based data (MAE of 0.24 0.03). |
| [124] | 2023 | Fetal arrhythmia | Hierarchical extreme learning machine | Fetal ECG | This study introduces a multi-domain feature extraction approach to predict fetal arrhythmia accurately. The technique entails utilizing neighborhood component analysis (NCA) to screen sensitive data and a stacked ELM-SAE network for high-level fusion features. |
| [125] | 2022 | Fetal arrhythmia | Machine learning algorithm | Abdomen ECG | The framework uses approaches for noise reduction and pulls out important characteristics from various domains. The boosted decision tree classifier, one of four machine learning classifiers, achieves the maximum accuracy of 93.12%. |
| [126] | 2022 | Fetal heart rate | 1D-CNN | Fetal ECG | Fetal acidosis is correctly identified from FHR signals by a diagnostic method that uses a 1D-CNN model. With signal preprocessing, accuracy rises to 99.09% on a large dataset. Real-time use is made possible by integration with inexpensive electrical components. |
| [127] | 2022 | Fetal arrhythmia | Deep learning | Fetal ECG | A deep learning model divides segmented signals into standard and arrhythmic categories. The approach provides improved accuracy compared to traditional methods by concentrating on labeled segments, which lessens the influence of heartbeat detection findings. |
| [128] | 2023 | Blood pressure | Box–Cox transformation | ECG and PPG | The paper introduces the Box–Cox transformation technique to rectify label distribution and an end-to-end model called “BPNet” with a cross-modal fusion module capable of accurately capturing the relationship between multi-level ECG and PPG features. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Khan Mamun, M.M.R.; Elfouly, T. AI-Enabled Electrocardiogram Analysis for Disease Diagnosis. Appl. Syst. Innov. 2023, 6, 95. https://doi.org/10.3390/asi6050095
AMA Style
Khan Mamun MMR, Elfouly T. AI-Enabled Electrocardiogram Analysis for Disease Diagnosis. Applied System Innovation. 2023; 6(5):95. https://doi.org/10.3390/asi6050095
Chicago/Turabian StyleKhan Mamun, Mohammad Mahbubur Rahman, and Tarek Elfouly. 2023. "AI-Enabled Electrocardiogram Analysis for Disease Diagnosis" Applied System Innovation 6, no. 5: 95. https://doi.org/10.3390/asi6050095