
Use of Ultra-Translucent Monolithic Zirconia as Esthetic Dental Restorative Material: A Narrative Review

1
Department of Prosthetic Dental Sciences, College of Dentistry, King Saud University, Riyadh 11545, Saudi Arabia
2
Prosthodontics Department, College of Dentistry, University of Hail, Hail P.O. Box 2440, Saudi Arabia
*
Author to whom correspondence should be addressed.
Ceramics 2024, 7(1), 264-275; https://doi.org/10.3390/ceramics7010017
Submission received: 18 January 2024
/
Revised: 19 February 2024
/
Accepted: 21 February 2024
/
Published: 23 February 2024
Abstract
:It has been observed in recent years that zirconia (Zr) is being increasingly used for a wide range of clinical applications. There are several reasons for this, but the most significant one is its excellent mechanical properties, specifically its transformation toughening properties compared to other dental ceramics and its improved natural appearance when compared to ceramometal restorations. As a result of the advancement of chairside milling and developments in rapid-sintering technology, the fabrication of dental restorations has become more computerized, time-saving, and accurate over the past few decades. However, a main disadvantage of conventional Zr restorations is that they lack the translucency of glass–ceramics, although they are extremely strong. Recently, by increasing the yttrium %, changing the grain size, and reducing the impurities, the ultra-translucent monolithic zirconia “5-mol%-yttria-stabilized tetragonal zirconia polycrystals” has been introduced, with successful attempts to make translucent Zr an aesthetically attractive option for minimally invasive veneer restorations. It is important to note that veneer restorations do not possess the mechanical retentive features of the tooth preparations and rely primarily on bonding to resin cement. This presents a great challenge for the inert Zr since it does not bond chemically with resin cement, unlike glass–ceramic materials that establish chemical adhesion with resin cement, favoring their use for indirect veneer restorations. Taking this into account, this article aims to review the progressive development of ultra-translucent monolithic Zr materials as they are available today and, in the future, represents a concerted drive toward maximum translucency and strength, which renders them a viable treatment option for esthetic veneer restorations.
1. Introduction
More and more zirconia (Zr) is being created for various dental therapeutic uses. This is due to its superior natural appearance over ceramometal restorations and its superior mechanical qualities, which are connected to transformation toughening compared to other dental ceramics [1]. Furthermore, the creation of dental restorations is becoming more automated, accurate, and time-efficient because of the development of chairside milling and its connection to cutting-edge rapid-sintering technology [2].
The first Zr used in dentistry as “white metal” was “3-mol% yttria tetragonal Zr polycrystalline” (3Y-TZP), which was used in conventional restorations. They are used with ceramic veneering and as framework cores [3]. Conventional Zr restorations lack the translucency of glass–ceramics despite their considerable strength. Traditionally, powder-firing porcelain onto a zirconia core has been the method used to overcome this aesthetic shortcoming [4]. However, using this method exposes the restoration to chipping and delamination. To reduce this susceptibility, several strategies have been used, including separately milling the veneer and the framework before combining them with resin cement or fusion firing. However, covering the Zr core with ceramic veneer would result in a thicker restoration overall, which would require the removal of more tooth structure and consequently weaken the abutment tooth. Monolithic Zr was presented as a solution to these challenges in an effort to resolve them [5].
According to Zhang and Lawn, concentrated efforts were directed toward monolithic Zr restorations aiming to improve their aesthetic and durability requirements, simplify their production, and minimize the need for material thickness [6]. To improve Zr’s translucency and optical characteristics, the majority of these efforts concentrated on changing the crystal’s size and aligning the reflective indices of crystalline and matrix phases [7,8]. Additionally, increasing the yttrium content, adjusting the grain size, and lowering the contaminants were effective ways to achieve success. As a result, translucent Zr has been advertised as an attractive treatment modality for minimally invasive veneer restorations [9]. However, veneer restorations rely mostly on resin cement bonding because they lack the mechanical retentive characteristics of tooth preparation. Nevertheless, in contrast to silica-based glass ceramics, the composition and physical properties of high-strength ceramic materials, such as those based on zirconium oxide (ZrO2) and aluminum oxide (Al2O3), vary greatly, necessitating alternative bonding techniques to create an adhesive bond that is robust, long-lasting, and durable [7,8,9].
To give general dentists a thorough understanding of the material, this review attempts to integrate the literature on the developments in composition, physical properties, translucency, preparation designs, and bonding characteristics that render these materials a viable option for the use of esthetic veneer restoration.
2. Search Strategy
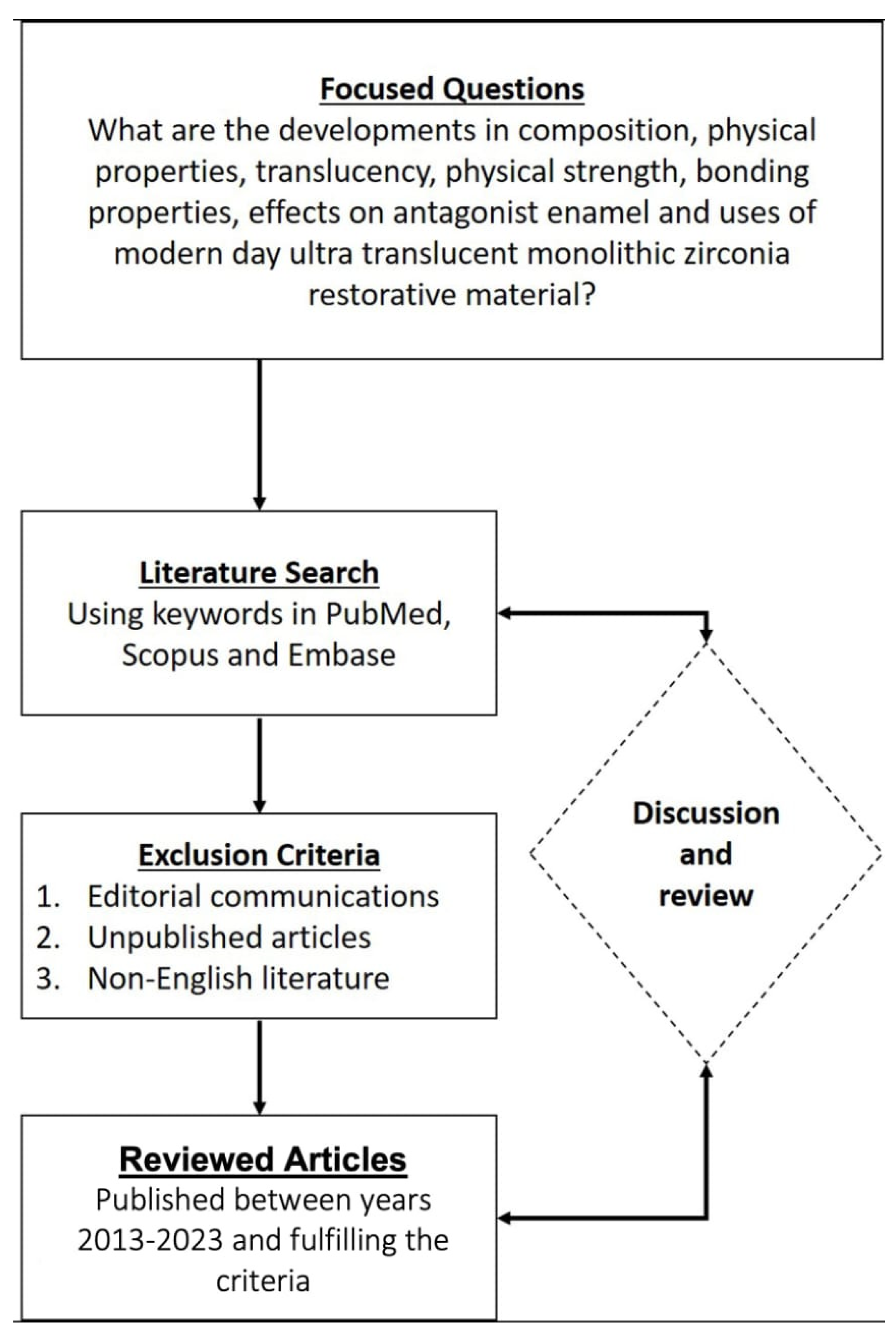
To address the focused questions, a literature search was carried out to identify suitable articles that have reported on the progressive development of ultra-translucent monolithic Zr as it is available today and in the future, representing a concerted drive toward maximum translucency and strength.
Well-known scientific databases like PubMed, Scopus, Elsevier, and Embase were searched to find pertinent English-language literature published between 2000 and 2023. The terms “Zirconia”, “Dental ceramics, “Veneers”, “Lithium disilicate”, “Ceramics”, “Monolithic Zirconia”, “Translucent Zirconia”, “Zirconia Crowns”, “All Ceramic Crowns”, “Esthetic Crowns”, “Bonding of Zirconia”, “Strength of Zirconia”, “Esthetic Veneers”, “Zirconia Wear”, “Zirconia Preparation”, and “Zirconia Restorations” were utilized in various combinations. The flow chart below schematically depicts the literature search and study selection procedure (Figure 1).
3. Development and Associated Physical Properties
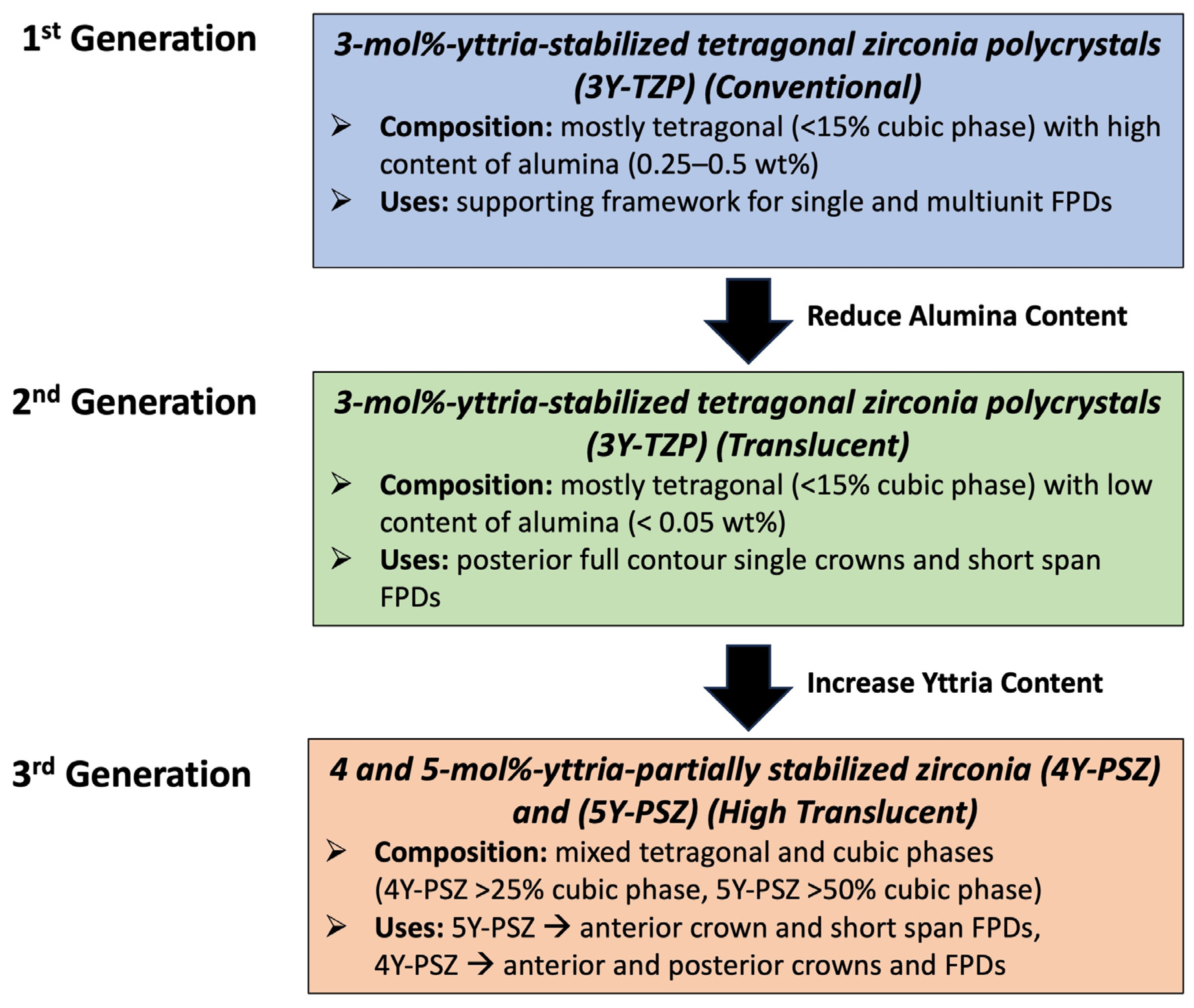
Zr, as a dental restorative material, has undergone many advancements and modifications over time (Figure 2). Compared to other ceramic substances, the 3Y-TZP, which is the first generation of dental Zr, was more durable because it incorporated a small quantity of alumina (Al2O3) sintering benefit [8]. However, this form of Zr had limited translucency because of the non-cubic Zr phases, which led to light scattering from pores, grain boundaries, and other inclusions, resulting in high opacity and poor optical appearance [6,7,8,9,10,11,12,13,14]. Accordingly, it was mostly utilized as a supporting framework for fixed dental prostheses (FDPs) for posterior teeth due to its strong flexural strength and biocompatibility [8,9,10,11].
In 2013, an improved version of the 3Y-TZP materials was released (Figure 2). This was achieved via sintering at a higher temperature to eliminate porosity and by drastically reducing the amount of alumina addition [15]. There was also more light transmission since the alumina grains were positioned at the edges of the Zr grains [15]. Because of such modification, this generation of Zr has improved aesthetic qualities, but its application was restricted to the posterior area.
The next stage in the development of monolithic Zr required the inclusion of transparent phases in the final product to increase its translucency. Zr’s translucency was further improved by raising the yttria (Y2O3) content to 5 mol%-yttria-partially stabilized zirconia (5Y-PSZ) [16]. Cubic Zr is the vernacular name for this Zr, which is described as having a cubic-tetragonal microstructure [14,15,16]. Approximately 50% of the material is cubic. Light traveling through the restorations travels through fewer edges and porosities because cubic crystals are larger than tetragonal crystals. As a result, it appears more translucent. However, mechanical qualities like flexural strength and fracture toughness suffer when the cubic crystal concentration rises. Therefore, its use is limited to single tooth restorations in the anterior region and fixed partial denture prostheses (FPDs) with up to three units and one pontic between two crowns in the premolar region [6,12,13,14,15,16]. The prescription range for monolithic Zr restorations is being expanded by a range of improvements aimed at optimizing the material qualities. In 2017, modifications to the third generation of Zr were performed through a reduction in yttria concentration to 4 mol% (4Y-PSZ) to increase the mechanical qualities compared to 5Y-PSZ from the third generation [6,12,13,14,15,16].
Monolithic Zr restorations are constructed using “CAD/CAM technology” (Computer-aided design and computer-aided manufacturing). Utilizing a single monolithic zirconium oxide ceramic ingot or black, sintering and cutting are carried out via computer numerical control [17,18]. The manufactured crowns exhibit superior flexural strength and fracture toughness in contrast to ceramic crowns based on silica (Table 1). Monolithic Zr ceramic restorations have an advantage over other all-ceramic restorations because of their mechanical qualities, which allow them to withstand stronger chewing with a lower risk of chipping (Table 1) [19]. In addition, monolithic Zr crown restorations require less tooth structure trimming than all ceramic crown restorations, preserving more natural tooth structure [20]. While conventional Zr has an elastic modulus of 215 GPa and a flexural strength of >1100 GPa (Table 1), the strength of translucent Zr is determined to be only half that of conventional Zr, with variations occurring based on the manufacturer [9]. However, translucent Zr has been discovered to have better fracture resistance than lithium disilicate and other porcelain-veneered restorations, in addition to its flexural strength [9,21,22,23,24,25,26].
Translucent monolithic Zr undergoes slow aging, sometimes referred to as low-temperature deterioration (LTD) over time [27,28]. This begins at the surface of the material and gradually works its way down to change the substance’s overall characteristics. LTD will result in a 20–40% reduction in fracture load by making the surface area rougher, causing microcracks to form, and lowering the mechanical characteristics of the material. This will happen regardless of the surface treatment applied [29]. Several variables affect Zr’s capacity to tolerate LTD, including the amount of yttria, grain size, cubic phase content, the concentration of Al2O3 and SiO3, and the degree of residual stress. According to research, the level of Al2O3 should be kept at least 0.15 weight percent (with an acceptable range of 0.15–0.25 weight percent) to prevent the aging process [30]. Reducing the alumina content to increase translucency, however, runs the risk of increasing the material’s vulnerability to LTD. The literature reports that the monoclinic phase tends to rise following the LTD phase, potentially resulting in reduced fracture resistance in translucent Zr crowns [31,32,33].
Although raising the amount of Y2O3 to enhance the optical features has been associated with a drop in mechanical properties of translucent monolithic Zr, Elsayed et al. have demonstrated that the fracture strength of translucent monolithic Zr 5Y-PSZ with higher Y2O3 was still high when comparing it with 3Y-TZP and 4Y-PSZ molar crowns [34]. On the other hand, 8 mol% monolithic Zr specimens were discovered to be considerably more prone to strength loss following mechanical cycling, particularly when thermal cycling was added to mechanical cycling [35]. Moreover, following thermal cycling in water, unglazed monolithic crowns showed the least strength. In contrast to these results, Bergamo et al. also state that the combined effects of mechanical and thermal aging do not considerably reduce the fracture loads associated with the restoration of monolithic zirconia crowns [36].
4. Progress in Color Properties and Enhanced Translucency
To establish a natural appearance with desirable translucency, the composition and microstructure of zirconia have been modified. Like conventional Zr, translucent Zr also contains yttria. However, translucent Zr has a greater yttria content, ranging from 4% mol to 8% mol. As a result, at room temperature, PSZ has both tetragonal and cubic phases [37]. A portion of the tetragonal phase changes into a cubic phase as the yttria content rises, rendering the phase optically isotropic. Translucency is increased, and light scattering at the grain boundaries is decreased as a result [20,21]. The restoration’s flexural strength and toughness were impaired by this increase in translucency. Zhang et al. claim that this is because an increase in yttria content would prevent the cubic Zr from undergoing a stress-induced transformation, which would have caused the strength compromise [30].
In recent years, various manufacturers have developed Zr’s composition to become a polychromatic multilayer, with the ultimate goal being to reproduce the shade gradient seen in natural teeth, in which the incisal portion of the veneer represents the most translucent area, increasing in chroma and opacity as it moves down to the gingival portion of the veneer [38]. Initially, pre-shade layers of the same Zr composition were produced as polychromatic multilayer uniform Zr. It has been stated that only pigment composition varies among the different layers of this uniform multilayer zirconia material, resulting in different shades but showing similar translucency [38]. Thereafter, ultra-translucent Zr with different microstructures among the layers were introduced, in which TZP and PSZ layers with various compositions and properties were present, giving the polychromatic multilayer hybrid composition of Zr [39]. Depending on the Yttrium content and chemical composition, the layers appear as variable formulations; therefore, their physical properties in a material may be different [39]. Various manufacturers state that the developments in different grades of ultra-translucent Zr have rendered monolithic translucent Zr a viable treatment option for the restoration of anterior teeth through indirect veneer restorations [3,38].
The total translucency is also significantly influenced by scattering, material compositions, and microstructures [21,22,23]. Alumina plays a role in light-scattering within zirconia due to variations in refractive index, reducing the translucency of zirconia; therefore, in new translucent generations, alumina content has been reduced [23].
According to Lambert’s law, light is transmitted more when the thickness is generally decreased since there is less absorption [40]. Zr restorations that are only 0.5 mm thick may exhibit translucent to a degree comparable to lithium disilicate ceramics that are at least 1 mm thick and are considered to be extremely translucent [8]. The monolithic Zr ceramics exhibit distinct optical characteristics that vary depending on the brand [41]. An in vitro investigation was conducted to assess the shade of translucent zirconia laminate veneers with variable thicknesses over teeth of different hues. The color imaging spectrophotometer indicates that thinner veneer restorations typically display higher values, suggesting that thinner veneer restorations may produce better color matching [42].
High translucency has been associated with thinner translucent zirconia, specifically those measuring around 0.3 mm [43]. It is crucial to consider the ultimate appearance of restorations employing translucent Zr, which lets light pass through by evaluating the shade of the cement or composite–resin luting agent. For the greatest results, it is therefore advised to utilize try-in pastes to confirm the expected appearance and select a cement shade that complements the shade of the abutment tooth [44].
Several studies have documented the influence of some factors on the color and optical properties of translucent monolithic Zr [19,39]. However, little is known about how aging or low temperatures affect the translucency of a new generation of translucent Zr ceramics. In a study, Subasi et al. looked at the effect of material and thickness (0.5, 0.7, and 1.0 mm) on the color. During thermocycling in coffee solution, the color stability and relative translucency parameters (RTP) of monolithic Zr ceramics were evaluated [45]. In the groups with varying thicknesses, material and thickness interacted highly significantly, but there was also a statistically significant difference between them. Kim et al. reported that hydrothermal aging increased the translucency of monolithic Zr [46].
5. Veneer Preparation Design, Marginal Fit, and Adaptation
According to several manufacturers, the thickness of their translucent monolithic Zr dental restorative material can be as thin as 0.3 mm, falling between 0.3 and 0.7 mm. More retentive preparation designs and data about the thickness of translucent monolithic Zr are nevertheless needed and should be included in the literature [47,48]. A careful and accurate reduction of tooth tissue is necessary to get effective results with aesthetic veneers. Ensuring the lifespan and natural appearance of the veneers requires careful and suitable execution of this process. The location and function of the tooth will determine how best to prepare it for monolithic Zr restorations, but as a general rule of thumb, anterior teeth should have wall thicknesses of at least 0.3 mm and between 1.0 and 1.5 mm; incisal depth cut with a continuous circumferential chamfer at the gingival edge that is at least 0.3 mm to facilitate accurate milling of the pre-sintered Zr [49,50].
The veneer preparation design lacks retentive features, creating a great challenge for monolithic Zr veneer restorations. It is significant to remember that a variety of factors influence the retention of monolithic Zr restorations. Lepe et al. discovered in a study that Zr restorations can be adequately retained in a clinical context with a tooth preparation that has an optimum taper and axial length [51]. In another study employing a minimally invasive vertical preparation procedure, Zr and Zr reinforced lithium silicate restorations fabricated through CAD/CAM techniques were bonded with dual-polymerizing luting resin over a three-year follow-up period. Both ceramic materials produced good aesthetic results supported healthy and stable soft tissues and did not present any mechanical complications [52,53].
The marginal adaption of monolithic translucent Zr laminates is influenced by both the sintering process and the design of tooth preparation. A variety of marginal designs, including modified vertical with reverse shoulder, deep chamfer, and vertical, can influence the failure modes and fracture strengths of monolithic Zr veneer restorations [54]. According to Abdulazeez et al., the vertical marginal design had the lowest fracture load, and the chamfer, succeeding the modified vertical, had the highest fracture load [54]. The average fracture strengths of the monolithic Zr restorations across all groups exceeded the premolar region’s maximal occlusal forces. The fracture strength was improved by the vertical preparation adjustment, which included placing a reverse shoulder at the buccal surface, to the point that the difference between the chamfer group and the control group was not statistically significant [55,56]. Fracture resistance will also be impacted by the marginal thicknesses of zirconia veneer restorations. The reduction in fracture resistance was statistically significant when the marginal width was lowered below 0.8 mm, even if it was not statistically significant up to 0.8 mm, per a study looking at the marginal thickness [57]. In another in-vitro study on the fracture resistance of zirconia crowns made using CAD/CAM with different marginal thickness abutments, it was demonstrated that when marginal thickness decreased, the fracture load value decreased [58]. Saker and Ozcan, on the other hand, have shown that the sintering process and tooth preparation design have an impact on the marginal adaptation of monolithic transparent Zr [59]. Regardless of the tooth preparation design utilized, the sintering process has a major impact on the translucent Zr restorations’ resistance to breakage [60]. According to Jurado et al., chair-side milled Zr-reinforced lithium silicate veneers’ fracture resistance was significantly impacted by the designs used for incisal preparation [61]. In contrast to incisal shoulder preparation or no preparation at all, the incisal palatal chamfer incisal preparation design resulted in much greater fracture resistance of monolithic Zr-reinforced lithium silicate laminate veneers. Additionally, this study discovered that adhesive fractures occurred primarily in the incisal palatal shoulder and chamfer [62].
The marginal gap of two thicknesses of monolithic Zr restorations (0.5 and 1 mm) was evaluated in a study by Mohaghegh in 2020, and the results showed no statistically significant difference between the two groups [49]. The layered Zr crowns, on the other hand, had a marginal gap that was noticeably larger than the monolithic Zr veneers. Thus, they proposed that Zr with a thickness of 0.5 mm can be employed for aesthetic purposes without risking the marginal fit of the restoration [49,62]. Studies have also shown that the butt joint veneer preparation design was significantly better than the palatal chamfer design in terms of marginal fit [63]. A recent case report demonstrated successful treatment after one year of follow-up with ultrathin zirconia veneer restorations on the anterior teeth with veneers ranging in thickness from 0.3 to 0.6 mm [43]. Case series reports of two patients who had received zirconia veneer restorations (0.6 mm thick) on anterior teeth have also documented patients’ satisfaction with the cosmetic results of their treatment. The backdrop teeth did not have any stains; therefore, it was not difficult to match the final hue, even though these reports found that translucent zirconia restorations produced outstanding esthetic outcomes [46].
Veneer resistance and retention are directly correlated with internal fit. Greater misfit values raise the possibility of fracture under stresses and reduce retention. An even distribution of cement space within the crown prevents loss of retention and possible fracture and is essential for appropriate force dissipation under occlusal stresses [63,64,65,66]. Different studies have reported that the mean axial and occlusal gap values ranged from 57 to 105 µm, while mean marginal gap values were reported by Paul et al. to be 77 µm [64]. Studies now appear to concur that any misfit at the veneer margin should be less than 120 µm. Some argue that when CAD-CAM technology is used, this restriction should not be more than 100 µm [67]. The ultra-translucent monolithic zirconia veneers have clinically acceptable marginal and internal fit. The manufacturing technique or the different thicknesses of monolithic zirconia veneers do not significantly affect the marginal and internal fit [67]
6. Bonding Properties with Adhesive Cements
Since veneer preparations lack retentive features, retention of laminate veneer restorations depends mainly on bonding with adhesive cement. Adequate retention, enhanced marginal adaptation, reduced micro-leakage, and increased fracture resistance of the restored tooth and the restoration are all benefits of a robust, long-lasting resin cement bond [68]. Modern all-ceramic systems and adhesive bonding techniques provide a multitude of extremely aesthetic treatment alternatives. When certain instructions are followed, including conditioning using hydrofluoric acid (4–10%) followed by silanization, bonding to conventional silica-based ceramics is a predictable process that produces long-lasting effects [69,70]. On the other hand, treatment with zirconia veneers presents a major challenge due to inferior adherence properties to resin cement. This is one of the reasons glass–ceramic materials have been widely chosen for indirect veneer restorations, as they form a chemical link with the resin cement, in contrast to Zr restorations, which are chemically inert [69,70]. For this reason, various surface preparations have been suggested to alter the surface of zirconia and enhance adhesion to resin cement [71,72,73,74]. These techniques include airborne-particle abrasion (APA), tribo-chemical silica airborne-particle abrasion (TBS), laser irradiation, plasma spraying, Zr ceramic powder coating, low-fusion porcelain application, hot chemical etching solutions, and selective infiltration etching (SIE) [74].
The application of surface preparation techniques improves mechanical and chemical bonding. Zr resin bonding can be strengthened and prolonged using primers and resin cement based on “phosphate ester monomers” or “10-Methacryloyloxydecyl Dihydrogen Phosphate (MDP)” monomers as surface pretreatments [74]. Because these monomers may establish strong chemical bonds with the metal oxides in Zr, they are very helpful. Furthermore, well-known studies have shown that 10-MDP-containing resin luting agents and airborne-particle abrasion are efficient ways to achieve long-term, durable Zr resin bonding [75]. According to research by Blatz et al., the APC Zr Bonding Concept is a useful technique for creating strong, durable resin bindings to Zr [76]. The three primary processes of zirconia cementation are referred to as the APC Zirconia Bonding Concept; Step A: Alumina or silica-coated alumina particles are air-particle abraded; Step P: MDP or phosphate-monomer-based primer is applied to the air-abraded surfaces; Step C: Dual- or self-cured composite resin cement is applied [76]. The material can be efficiently strengthened by air-abrading the bonding surface of Zr with a sandblaster utilizing small alumina particles (50 μm) or silica-coated alumina particles at low pressure. The bonding ability would then be increased by putting Zr primer, such as MDP, onto the Zr bonding surface, which would naturally be effective in bonding with metal oxides. It is essential to use dual- or self-cure resin cement to ensure sufficient polymerization [69,70,71,72,73,74,75,76]. However, it is worth noting that when using a 0.5 mm thin monolithic Zr veneer material, it is necessary to increase the resin composite’s curing time by about 40% over what it would be if the Zr ceramics were not used. However, the curing period must be doubled if the thickness of the Zr ceramic material is increased to 1 mm [77]. A case series of up to five years of follow-up has demonstrated a survival rate of 100% of ultra-translucent Zr veneers luted with adhesive resin cement following airborne particle abrasion and silica coating. There were no obvious failures such as debonding, veneer fracture, or secondary caries [78].
7. Effect on Antagonist Teeth
The strongest ceramic material used in restorative materials is Zr [79]. However, it is important to realize that a material’s hardness does not always indicate that it would cause greater abrasion on the opposing tooth’s enamel surface [80]. Conversely, a number of tests revealed that in contrast to glass ceramics with a greater degree of surface roughness, translucent monolithic Zr has less wear effect on the opposing enamel because of its smooth polished surface [81]. The antagonist’s natural dentition becomes more abrasive and has a rougher surface when the glass–ceramics microstructure disappears and reveals the crystalline phase. It is important to remember that translucent monolithic Zr can seriously erode the enamel of the opposing teeth. However, this only happens if it has been subjected to sandblasting or glazing or if the polishing process was insufficiently carried out [82]. It is, therefore, essential to ensure that proper polishing and treatment methods are employed when using translucent monolithic Zr to prevent any damage to the opposing teeth’s enamel [83].
According to prior in vitro studies, translucent monolithic Zr may be used as a safe antagonist to human enamel despite its hardness [84]. The hardest materials should theoretically be able to wear antagonist teeth the most; however, there are other elements that affect a material’s wear capacity, such as surface roughness. In vitro studies by Preis et al. and Amer et al. discovered that polishing significantly reduced the surface roughness of monolithic Zr and that, in contrast to human enamel, the material’s surface roughness does not alter after three-body wear [85,86]. Even though these tests are rapid, simple, and inexpensive, they are not able to replicate the oral environment accurately. A few clinical research have looked into how antagonist enamel or ceramic/metal ceramic crown restorations degrade over time when combined with monolithic zirconia crown restorations. Esquivel-Upshaw et al. concluded that polished monolithic zirconia was just as wear-resistant as enamel coatings and metal–ceramics based on a randomized controlled study with a one-year observation period. Zr restorations yield nearly the same outcomes as other dental repair options [86].
When studied for up to a year, translucent monolithic Zr crowns produced less wear of the opposing enamel than the known wear values of normal teeth [87]. Enamel against monolithic Zr crowns showed less wear after a year of wear monitoring than common ceramic materials such as lithium disilicate and feldspathic porcelain; furthermore, the enamel wear against Zr (16.3 μm) was significantly less than that against metal–ceramic crowns [88,89,90]. After a year of follow-up, the authors observed wear of 69.20 μm in the premolar region and 179.70 μm in the molar region. This may be the result of the surface roughness of Zr, which, in contrast to feldspathic porcelain, does not change significantly following three-body wear against human enamel. When different clinical criteria were examined, monolithic Zr crowns demonstrated outstanding overall clinical survival over a one-year period [91,92].
8. Summary
Because of its exceptional optical and physical qualities, the ultra-translucent monolithic zirconia (Zr), a dental restorative material largely made of zirconium oxide, is emerging as a favored choice for the aesthetic zone. It has been demonstrated that this material’s strong mechanical properties and ability to yield superior aesthetic outcomes make it a great choice for indirect aesthetic veneer restorations. This is made possible by meticulously organizing, incorporating, and executing the essential ideas and methods necessary for these Zr-based aesthetic restorations to be successful in providing a visually stunning and structurally solid final result. Modern ultra-translucent monolithic Zr restorations are strong, do not have to be very thick, and take up less tooth structure. Prior to using resin luting agents with these restorations in a predictable manner, the bonding surface of the restorations must be roughened using grit blasting to enhance mechanical interlocking and chemical conditioning. To ensure durable microstructures of the ultra-translucent monolithic Zr in an environment that closely mimics oral circumstances, more research is needed to elucidate their wear behavior, mechanical performance, durability, stress distribution, and survival. This is a challenging technique designed to improve the aesthetics of fine-grain microstructures without sacrificing their inherent strength. Published data demonstrated promising results and satisfactory aesthetics for the use of translucent monolithic zirconia veneers. However, limited clinical studies documenting their survival were found in the literature. Therefore, long-term clinical studies are mandatory to confirm this type of treatment.
Author Contributions
Conceptualization, G.A., A.H.A.-S. and S.A.; methodology, G.A., A.H.A.-S. and S.A.; validation, G.A.; investigation, A.H.A.-S. and S.A.; resources, A.H.A.-S. and S.A.; data curation, A.H.A.-S. and S.A.; writing—original draft preparation, G.A., A.H.A.-S. and S.A.; writing—review and editing, G.A.; visualization, G.A; supervision, G.A.; project administration, G.A.; funding acquisition, G.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hjerppe, J.; Özcan, M. Zirconia: More and more translucent. Curr. Oral Health Rep. 2023, 10, 203–211. [Google Scholar] [CrossRef]
- Prithviraj, D.R.; Bhalla, H.K.; Vashisht, R.; Sounderraj, K.; Prithvi, S. Revolutionizing restorative dentistry: An overview. J. Indian Prosthodont. Soc. 2014, 14, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Kongkiatkamon, S.; Rokaya, D.; Kengtanyakich, S.; Peampring, C. Current classification of zirconia in dentistry: An updated review. PeerJ 2023, 11, e15669. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Reveron, H.; Spies, B.C.; Van Meerbeek, B.; Chevalier, J. Trade-off between fracture resistance and translucency of zirconia and lithium-disilicate glass ceramics for monolithic restorations. Acta Biomater. 2019, 91, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Subash, M.; Vijitha, D.; Deb, S.; Satish, A.; Mahendirakumar, N. Evaluation of shear bond strength between zirconia core and ceramic veneers fabricated by pressing and layering techniques: In vitro study. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. S2), S612–S615. [Google Scholar] [PubMed]
- Zhang, Y.; Lawn, B.R. Novel zirconia materials in dentistry. J. Dent. Res. 2018, 97, 140–147. [Google Scholar] [CrossRef]
- Khattar, A.; Alsaif, M.H.; Alghafli, J.A.; Alshaikh, A.A.; Alsalem, A.M.; Almindil, I.A.; Alsalman, A.M.; Alboori, A.J.; Al-Ajwad, A.M.; Almuhanna, H.M.; et al. Influence of ZrO2 nanoparticle addition on the optical properties of denture base materials fabricated using additive technologies. Nanomaterials 2022, 12, 4190. [Google Scholar] [CrossRef]
- Alqutaibi, A.Y.; Ghulam, O.; Krsoum, M.; Binmahmoud, S.; Taher, H.; Elmalky, W.; Zafar, M.S. Revolution of current dental zirconia: A comprehensive review. Molecules 2022, 27, 1699. [Google Scholar] [CrossRef]
- Bajraktarova-Valjakova, E.; Korunoska-Stevkovska, V.; Kapusevska, B.; Gigovski, N.; Bajraktarova-Misevska, C.; Grozdanov, A. Contemporary dental ceramic materials, A review: Chemical composition, physical and mechanical properties, indications for use. Maced. J. Med. Sci. 2018, 6, 1742–1755. [Google Scholar] [CrossRef]
- Song, X.; Ding, Y.; Zhang, J.; Jiang, C.; Liu, Z.; Lin, C.; Zheng, W.; Zeng, Y. Thermophysical and mechanical properties of cubic, tetragonal and monoclinic ZrO2. J. Mater. Res. Technol. 2023, 23, 648–655. [Google Scholar] [CrossRef]
- Zhang, Y. Making yttria-stabilized tetragonal zirconia translucent. Dent. Mater. 2014, 30, 1195–1203. [Google Scholar] [CrossRef]
- Arellano Moncayo, A.M.; Peñate, L.; Arregui, M.; Giner-Tarrida, L.; Cedeño, R. State of the art of different zirconia materials and their indications according to evidence-based clinical performance: A narrative review. Dent. J. 2023, 11, 18. [Google Scholar] [CrossRef]
- Camposilvan, E.; Leone, R.; Gremillard, L.; Sorrentino, R.; Zarone, F.; Ferrari, M.; Chevalier, J. Aging resistance, mechanical properties and translucency of different yttria-stabilized zirconia ceramics for monolithic dental crown applications. Dent. Mater. 2018, 34, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Stawarczyk, B.; Keul, C.; Eichberger, M.; Figge, D.; Edelhoff, D.; Lümkemann, N. Three generations of zirconia: From veneered to monolithic. Part I. Quintessence Int. 2017, 48, 369–380. [Google Scholar]
- Stawarczyk, B.; Keul, C.; Eichberger, M.; Figge, D.; Edelhoff, D.; Lümkemann, N. Three generations of zirconia: From veneered to monolithic. Part II. Quintessence Int. 2017, 48, 441–450. [Google Scholar] [PubMed]
- Ban, S. Classification and properties of dental zirconia as implant fixtures and superstructures. Materials 2021, 14, 4879. [Google Scholar] [CrossRef]
- Leitão, C.I.; de Oliveira Fernandes, G.V.; Azevedo, L.P.; Araújo, F.M.; Donato, H.; Correia, A.R. Clinical performance of monolithic CAD/CAM tooth-supported zirconia restorations: Systematic review and meta-analysis. J. Prosthod. Res. 2022, 66, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 134. [Google Scholar] [CrossRef]
- Kontonasaki, E.; Rigos, A.E.; Ilia, C.; Istantsos, T. Monolithic zirconia: An update to current knowledge. optical properties, wear, and clinical performance. Dent. J. 2019, 7, 90. [Google Scholar] [CrossRef]
- Kaur, D.P.; Raj, S.; Bhandari, M. Chapter 2—Recent advances in structural ceramics. In Advanced Ceramics for Versatile Interdisciplinary Applications; Singh, S., Kumar, P., Mondal, D.P., Eds.; Elsevier Series on Advanced Ceramic Materials; Elsevier: Amsterdam, The Netherlands, 2022; pp. 15–39. [Google Scholar]
- Harada, K.; Raigrodski, A.J.; Chung, K.H.; Flinn, B.D.; Dogan, S.; Mancl, L.A. A comparative evaluation of the translucency of zirconias and lithium disilicate for monolithic restorations. J. Prosthet. Dent. 2016, 116, 257–263. [Google Scholar] [CrossRef]
- Singh, S.P.; Sontakke, A.D. Transparent glass ceramics. Crystals 2021, 11, 156. [Google Scholar] [CrossRef]
- Kim, H.K. Optical and mechanical properties of highly translucent dental zirconia. Materials 2020, 13, 3395. [Google Scholar] [CrossRef] [PubMed]
- Kontonasaki, E.; Giasimakopoulos, P.; Rigos, A.E. Strength and aging resistance of monolithic zirconia: An update to current knowledge. Jpn. Dent. Sci. Rev. 2020, 56, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Kui, A.; Manziuc, M.; Petruțiu, A.; Buduru, S.; Labuneț, A.; Negucioiu, M.; Chisnoiu, A. translucent zirconia in fixed prosthodontics—An integrative overview. Biomedicines 2023, 11, 3116. [Google Scholar] [CrossRef] [PubMed]
- Abad-Coronel, C.; Paladines, Á.; Ulloa, A.L.; Paltán, C.A.; Fajardo, J.I. Comparative fracture resistance analysis of translucent monolithic zirconia dioxide milled in a cad/cam system. Ceramics 2023, 6, 1179–1190. [Google Scholar] [CrossRef]
- de Araújo-Júnior, E.N.; Bergamo, E.T.; Bastos, T.M.; Jalkh, E.B.; Lopes, A.C.; Monteiro, K.N.; Cesar, P.F.; Tognolo, F.C.; Migliati, R.; Tanaka, R.; et al. Ultra-translucent zirconia processing and aging effect on microstructural, optical, and mechanical properties. Dent. Mater. 2022, 38, 587–600. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.K.; Venturini, A.B.; Silvestri, T.; Dapieve, K.S.; Montagner, A.F.; Soares, F.Z.; Valandro, L.F. Low-temperature degradation of Y-TZP ceramics: A systematic review and meta-analysis. J. Mech. Behav. Biomed. Mater. 2016, 55, 151–163. [Google Scholar] [CrossRef]
- Ramesh, S.; Lee, K.S.; Tan, C.Y. A review on the hydrothermal ageing behaviour of Y-TZP ceramics. Ceram. Int. 2018, 44, 20620–20634. [Google Scholar] [CrossRef]
- Zhang, F.; Vanmeensel, K.; Inokoshi, M.; Batuk, M.; Hadermann, J.; Van Meerbeek, B.; Naert, I.; Vleugels, J. Critical influence of alumina content on the low temperature degradation of 2–3 mol% yttria-stabilized TZP for dental restorations. J. Eur. Ceram. Soc. 2015, 35, 741–750. [Google Scholar] [CrossRef]
- Jia-Mahasap, W.; Jitwirachot, K.; Holloway, J.A.; Rangsri, W.; Rungsiyakull, P. Wear of various restorative materials against 5Y-ZP zirconia. J Prosthet. Dent. 2022, 128, 814.e1–814.e10. [Google Scholar] [CrossRef]
- Arya, N.R.; Gupta, R.; Weber, D.D.S.; Kurt, K. Zirconia Biomaterials. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493144/ (accessed on 14 August 2023).
- El-Ghany, O.; Sherief, A. Zirconia based ceramics, some clinical and biological aspects: Review. Future Dent. J. 2016, 2, 55–64. [Google Scholar] [CrossRef]
- Elsayed, A.; Meyer, G.; Wille, S.; Kern, M. Influence of the yttrium content on the fracture strength of monolithic zirconia crowns after artificial aging. Quintessence Int. 2019, 50, 344–348. [Google Scholar] [PubMed]
- Almohammed, S.N.; Alshorman, B.; Abu-Naba’a, L.A. Mechanical properties of five esthetic ceramic materials used for monolithic restorations: A comparative in vitro study. Ceramics 2023, 6, 1031–1049. [Google Scholar] [CrossRef]
- Bergamo, E.T.; da Silva, W.J.; Cesar, P.F.; Del Bel Cury, A.A. Fracture load and phase transformation of monolithic zirconia crowns submitted to different aging protocols. Oper. Dent. 2016, 41, E118–E130. [Google Scholar] [CrossRef] [PubMed]
- Ban, S. Chemical durability of high translucent dental zirconia. Dent. Mater. J. 2020, 39, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Kolakarnprasert, N.; Kaizer, M.R.; Kim, D.K.; Zhang, Y. New multi-layered zirconias: Composition, microstructure and translucency. Dent. Mater. 2019, 35, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Toma, F.R.; Porojan, S.D.; Vasiliu, R.D.; Porojan, L. The effect of polishing, glazing, and aging on optical characteristics of multi-layered dental zirconia with different degrees of translucency. J. Funct. Biomater. 2023, 14, 68. [Google Scholar] [CrossRef] [PubMed]
- Oshina, I.; Spigulis, J. Beer-Lambert law for optical tissue diagnostics: Current state of the art and the main limitations. J. Biomed. Opt. 2021, 26, 100901. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Y.; Agingu, C.; Tsoi, J.K.H.; Yu, H. Effects of aging on the color and translucency of monolithic translucent y-tzp ceramics: A systematic review and meta-analysis of in vitro studies. BioMed Res. Int. 2021, 2021, 8875023. [Google Scholar] [CrossRef]
- Mekled, S.; Elwazeer, S.; Jurado, C.A.; White, J.; Faddoul, F.; Afrashtehfar, K.I.; Fischer, N.G. Ultra-translucent zirconia laminate veneers: The influence of restoration thickness and stump tooth-shade. Materials 2023, 16, 3030. [Google Scholar] [CrossRef]
- Souza, R.; Barbosa, F.; Araújo, G.; Miyashita, E.; Bottino, M.A.; Melo, R.; Zhang, Y. ultrathin monolithic zirconia veneers: Reality or future? Report of a clinical case and one-year follow-up. Oper. Dent. 2018, 43, 3–11. [Google Scholar] [CrossRef]
- Alrabeah, G.; Alamro, N.; Alghamdi, A.; Almslam, A.; Azaaqi, M. Influences of luting cement shade on the color of various translucent monolithic zirconia and lithium disilicate ceramics for veneer restorations. J. Adv. Prosthodont. 2023, 15, 238–247. [Google Scholar] [CrossRef]
- Subaşı, M.G.; Alp, G.; Johnston, W.M.; Yilmaz, B. Effects of fabrication and shading technique on the color and translucency of new-generation translucent zirconia after coffee thermocycling. J. Prosthet. Dent. 2018, 120, 603–608. [Google Scholar] [CrossRef]
- Kim, H.K.; Kim, S.H. Effect of hydrothermal aging on the optical properties of precolored dental monolithic zirconia ceramics. J. Prosthet. Dent. 2019, 121, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Bang, H.J.; Choi, N.H.; Park, E.J. Translucency and masking ability of translucent zirconia; comparison with conventional zirconia and lithium disilicate. J. Adv. Prosthodont. 2022, 14, 324–333. [Google Scholar] [CrossRef]
- Alshali, S.A.; Kazim, S.A.; Nageeb, R.; Almarshoud, H.S. Comparative evaluation of the translucency of monolithic zirconia. J. Contemp. Dent. Pract. 2020, 21, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Mohaghegh, M.; Firouzmandi, M.; Ansarifard, E.; Ramazani, L. Marginal fit of full contour monolithic zirconia in different thicknesses and layered zirconia crowns. J. Int. Soc. Prev. Community Dent. 2020, 10, 652–658. [Google Scholar] [PubMed]
- Lepe, X.; Streiff, K.R.; Johnson, G.H. Long-term retention of zirconia crowns cemented with current automixed cements. J. Prosthet. Dent. 2021, 125, 788–794. [Google Scholar] [CrossRef]
- Shokry, M.; Al-Zordk, W.; Ghazy, M. Retention strength of monolithic zirconia crowns cemented with different primer-cement systems. BMC Oral Health 2022, 22, 187. [Google Scholar] [CrossRef]
- Emerson, J.S.; Johnson, G.H.; Kronström, M.H. Comparison of retention of monolithic zirconia crowns with alumina airborne-particle abraded and nonabraded intaglio using three different cements: A clinical simulation. J. Prosthet. Dent. 2023, 131, 100.e1–100.e5. [Google Scholar] [CrossRef]
- Kusaba, K.; Komine, F.; Honda, J.; Kubochi, K.; Matsumura, H. Effect of preparation design on marginal and internal adaptation of translucent zirconia laminate veneers. Eur. J. Oral Sci. 2018, 126, 507–511. [Google Scholar] [CrossRef]
- Abdulazeez, M.I.; Majeed, M.A. Fracture strength of monolithic zirconia crowns with modified vertical preparation: A comparative in vitro study. Eur. J. Dent. 2022, 16, 209–214. [Google Scholar] [CrossRef]
- Kim, S.H.; Yeo, M.Y.; Choi, S.Y.; Park, E.J. Fracture resistance of monolithic zirconia crowns depending on different marginal thicknesses. Materials 2022, 15, 4861. [Google Scholar] [CrossRef] [PubMed]
- Tekin, Y.H.; Hayran, Y. Fracture resistance and marginal fit of the zirconia crowns with varied occlusal thickness. J. Adv. Prosthodont. 2020, 12, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Habib, S.R.; Al Ajmi, M.G.; Al Dhafyan, M.; Jomah, A.; Abualsaud, H.; Almashali, M. Effect of margin designs on the marginal adaptation of zirconia copings. Acta Stomatol. Croat. 2017, 51, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Abushanan, A.; Sharanesha, R.B.; Aljuaid, B.; Alfaifi, T.; Aldurayhim, A. Fracture resistance of primary zirconia crowns: An in vitro study. Children 2022, 9, 77. [Google Scholar] [CrossRef] [PubMed]
- Saker, S.; Özcan, M. Marginal discrepancy and load to fracture of monolithic zirconia laminate veneers: The effect of preparation design and sintering protocol. Dent. Mater. J. 2021, 40, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Catramby, M.F.; do Vale, A.L.; Dos Santos, H.E.S.; Elias, C.N. Effect of sintering process on microstructure, 4-point flexural strength, and grain size of yttria-stabilized tetragonal zirconia polycrystal for use in monolithic dental restorations. J. Prosthet. Dent. 2021, 125, e1–e824. [Google Scholar] [CrossRef]
- Jurado, C.A.; Sadid-Zadeh, R.; Watanabe, H.; Robbins, C.E.; Afrashtehfar, K.I.; Fischer, N.G.; Lee, D.J. Effect of incisal preparation design on the fracture strength of monolithic zirconia-reinforced lithium silicate laminate veneers. J. Prosthodont. 2023. [Google Scholar] [CrossRef]
- Chai, S.; Bennani, V.; Aarts, J.; Lyons, K. Incisal preparation design for ceramic veneers. J. Am. Dent. Assoc. 2018, 149, 25–37. [Google Scholar] [CrossRef]
- Baig, M.R.; Qasim, S.S.; Baskaradoss, J.K. Marginal and internal fit of porcelain laminate veneers: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 131, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Paul, N.; Raghavendra Swamy, K.N.; Dhakshaini, M.R.; Sowmya, S.; Ravi, M.B. Marginal and internal fit evaluation of conventional metal-ceramic versus zirconia CAD/CAM crowns. J. Clin. Exp. Dent. 2020, 12, e31–e37. [Google Scholar] [CrossRef] [PubMed]
- Alrabeah, G.; Binhassan, F.; Al Khaldi, S.; Al Saleh, A.; Al Habeeb, K.; Anwar, S.; Habib, S.R. Effect of self-adhesive resin cement film thickness on the shear bond strength of lithium disilicate ceramic–cement–tooth triplex. Inorganics 2023, 12, 14. [Google Scholar] [CrossRef]
- Çin, V.; İzgi, A.D.; Kale, E.; Yilmaz, B. Marginal and internal fit of monolithic zirconia crowns fabricated by using two different cad-cam workflows: An in vitro study. Prosthesis 2023, 5, 35–47. [Google Scholar] [CrossRef]
- Vág, J.; Nagy, Z.; Bocklet, C.; Kiss, T.; Nagy, Á.; Simon, B.; Mikolicz, Á.; Renne, W. Marginal and internal fit of full ceramic crowns milled using CADCAM systems on cadaver full arch scans. BMC Oral Health 2020, 20, 189. [Google Scholar] [CrossRef]
- Aldakheel, M.; Aldosary, K.; Alnafissah, S.; Alaamer, R.; Alqahtani, A.; Almuhtab, N. Deep margin elevation: Current concepts and clinical considerations: A review. Medicina 2022, 58, 1482. [Google Scholar] [CrossRef]
- Heboyan, A.; Vardanyan, A.; Karobari, M.I.; Marya, A.; Avagyan, T.; Tebyaniyan, H.; Mustafa, M.; Rokaya, D.; Avetisyan, A. Dental luting cements: An updated comprehensive review. Molecules 2023, 28, 1619. [Google Scholar] [CrossRef]
- Homsy, F. Self-adhesive cements and all ceramic crowns: A review. Int. J. Dent. 2014, 2, 65–73. [Google Scholar] [CrossRef]
- Colombo, M.; Gallo, S.; Padovan, S.; Chiesa, M.; Poggio, C.; Scribante, A. Influence of different surface pretreatments on shear bond strength of an adhesive resin cement to various zirconia ceramics. Materials 2020, 13, 652. [Google Scholar] [CrossRef]
- Gołasz, P.; Kołkowska, A.; Zieliński, R.; Simka, W. Zirconium surface treatment via chemical etching. Materials 2023, 16, 7404. [Google Scholar] [CrossRef]
- Scaminaci Russo, D.; Cinelli, F.; Sarti, C.; Giachetti, L. Adhesion to zirconia: A systematic review of current conditioning methods and bonding materials. Dent. J. 2019, 7, 74. [Google Scholar] [CrossRef]
- Comino-Garayoa, R.; Peláez, J.; Tobar, C.; Rodríguez, V.; Suárez, M.J. Adhesion to zirconia: A systematic review of surface pretreatments and resin cements. Materials 2021, 14, 2751. [Google Scholar] [CrossRef]
- Alrabeah, G.; Alomar, S.; Almutairi, A.; Alali, H.; ArRejaie, A. Analysis of the effect of thermocycling on bonding cements to zirconia. Saudi Dent. J. 2023, 35, 734–740. [Google Scholar] [CrossRef]
- Blatz, M.B.; Conejo, J. cementation and bonding of zirconia restorations. Compend. Contin. Educ. Dent. 2018, 39 (Suppl. S4), 9–13. [Google Scholar]
- Fathy, H.; Hamama, H.H.; El-Wassefy, N.; Mahmoud, S.H. Clinical performance of resin-matrix ceramic partial coverage restorations: A systematic review. Clin. Oral Investig. 2022, 26, 3807–3822. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.R.; Araújo, G.D.; Moura, D.M.; Araújo, L.D.; Gurgel, B.D.; Melo, R.M.; Bottino, M.A.; Özcan, M.; Zhang, Y.; Souza, R.O. Clinical Performance of Minimally Invasive Monolithic Ultratranslucent Zirconia Veneers: A Case Series up to Five Years of Follow-up. Oper. Dent. 2023, 48, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.Y.; Pang, R.; Yang, J.; Fan, D.; Cai, H.; Jiang, H.B.; Han, J.; Lee, E.S.; Sun, Y. Overview of several typical ceramic materials for restorative dentistry. BioMed Res. Int. 2022, 2022, 8451445. [Google Scholar] [CrossRef]
- Daou, E.E. The zirconia ceramic: Strengths and weaknesses. Open Dent. J. 2014, 8, 33–42. [Google Scholar] [CrossRef]
- Dikicier, S.; Korkmaz, C.; Atay, A. Surface roughness and characteristics of CAD/CAM zirconia and glass ceramics after combined treatment procedures. BMC Oral Health 2022, 22, 524. [Google Scholar] [CrossRef] [PubMed]
- Jitwirachot, K.; Rungsiyakull, P.; Holloway, J.A.; Jia-Mahasap, W. Wear Behavior of Different Generations of Zirconia: Present Literature. Int. J. Dent. 2022, 2022, 9341616. [Google Scholar] [CrossRef]
- Preis, V.; Weiser, F.; Handel, G.; Rosentritt, M. Wear performance of monolithic dental ceramics with different surface treatments. Quintessence Int. 2013, 44, 393–405. [Google Scholar] [PubMed]
- Rosentritt, M.; Preis, V.; Behr, M.; Strasser, T. Fatigue and wear behaviour of zirconia materials. J. Mech. Behav. Biomed. Mater. 2020, 110, 103970. [Google Scholar] [CrossRef] [PubMed]
- Preis, V.; Grumser, K.; Schneider-Feyrer, S.; Behr, M.; Rosentritt, M. Cycle-dependent in vitro wear performance of dental ceramics after clinical surface treatments. J. Mech. Behav. Biomed. Mater. 2016, 53, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Amer, J.Y.; Rayyan, M.M. Effect of different surface treatments and bonding modalities on the shear bond strength between metallic orthodontic brackets andglazed monolithic zirconia crowns. J. Orthod. Sci. 2018, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Esquivel-Upshaw, J.F.; Kim, M.J.; Hsu, S.M.; Abdulhameed, N.; Jenkins, R.; Neal, D.; Ren, F.; Clark, A.E. Randomized clinical study of wear of enamel antagonists against polished monolithic zirconia crowns. J. Dent. 2018, 68, 19–27. [Google Scholar] [CrossRef]
- Soleimani, F.; Jalali, H.; Mostafavi, A.S.; Zeighami, S.; Memarian, M. Retention, and clinical performance of zirconia crowns: A comprehensive review. Int. J. Dent. 2020, 2020, 8846534. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Choi, J.W.; Jeong, C.M.; Huh, J.B.; Lee, S.H.; Lee, H.; Yun, M.J. Evaluating the wear of resin teeth by different opposing restorative materials. Materials 2019, 12, 3684. [Google Scholar] [CrossRef]
- Solá-Ruíz, M.F.; Baima-Moscardó, A.; Selva-Otaolaurruchi, E.; Montiel-Company, J.M.; Agustín-Panadero, R.; Fons-Badal, C.; Fernández-Estevan, L. Wear in antagonist teeth produced by monolithic zirconia crowns: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 997. [Google Scholar] [CrossRef]
- Mundhe, K.; Jain, V.; Pruthi, G.; Shah, N. Clinical study to evaluate the wear of natural enamel antagonist to zirconia and metal ceramic crowns. J. Prosthet. Dent. 2015, 114, 358–363. [Google Scholar] [CrossRef]
- Pathan, M.S.; Kheur, M.G.; Patankar, A.H.; Kheur, S.M. Assessment of antagonist enamel wear and clinical performance of full-contour monolithic zirconia crowns: One-year results of a prospective study. J. Prosthodont. 2019, 28, e411–e416. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the literature search and study selection process.
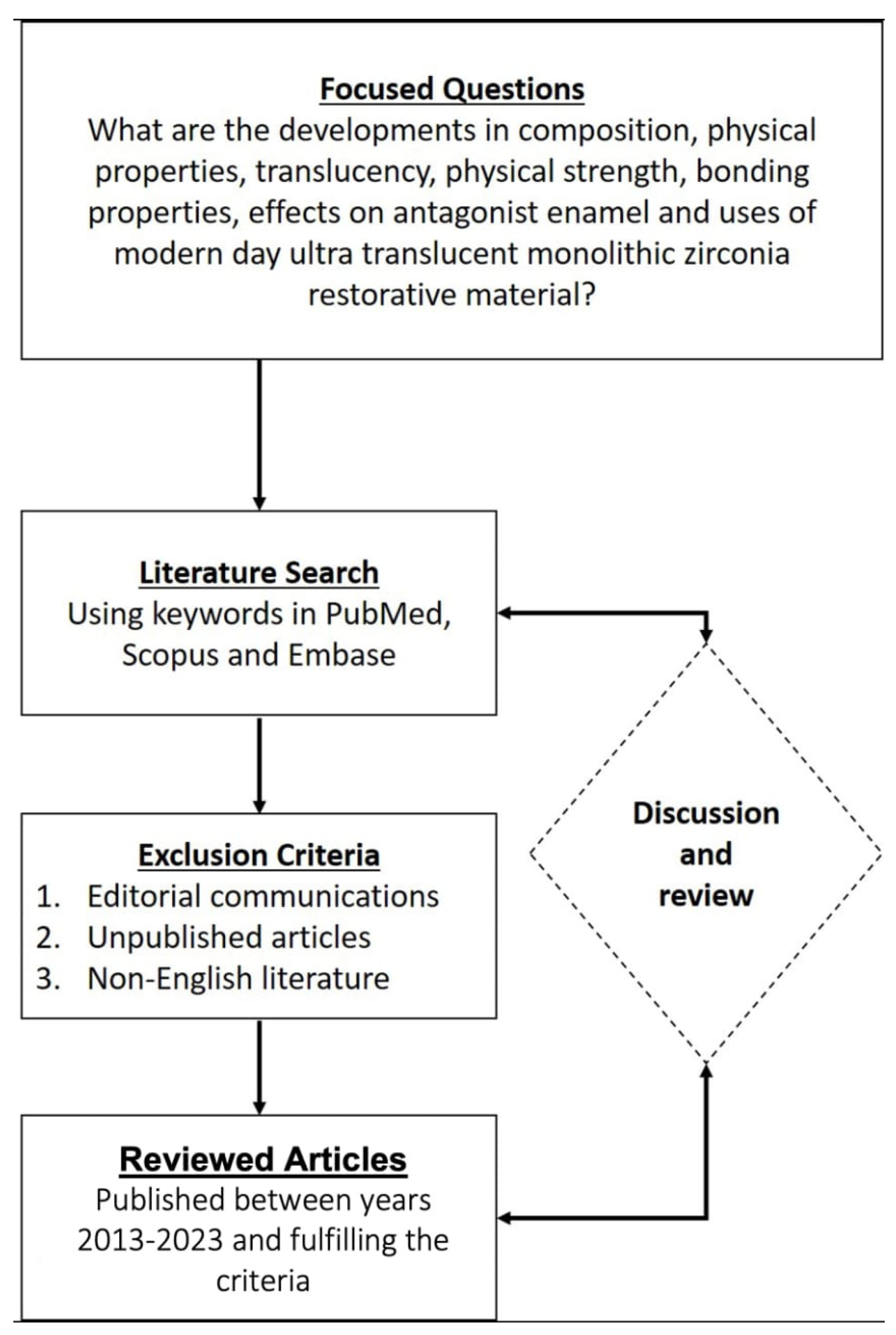
Figure 2.
Schematic diagram of evolution and generations of yttria-stabilized dental zirconia.

{kind=link}
{kind=link}
Table 1.
Physical properties of three commercial brands of zirconia representative of the three dental zirconia generations compared to silica-based ceramic.
Table 1.
Physical properties of three commercial brands of zirconia representative of the three dental zirconia generations compared to silica-based ceramic.
| First Generation Lava Frame * (3M ESPE) | Second Generation Cercon ht * Dentsply Sirona | Third Generation Cercon xt * Dentsply Sirona | Lithium Disilicate IPS Emax CAD (LT) * Ivoclar Vivadent | |
|---|---|---|---|---|
| Flexural Strength (MPa) | >1100 | 1200 | 750 | 400 |
| Coefficient of Thermal Expansion (CTE) | 10.5 μm/m·K (25–500 °C) | 10.5 μm/m·K (25–500 °C) | 10.1 μm/m·K (25–500 °C) | 10.5 μm/m·K (100–500 °C) |
| Modulus of Elasticity (GPa) | 210 | 210 | 210 | 95 |
| Fracture Toughness (Mpa.m0.5) | 3.5–4.5 | 3.5–4.5 | 2.7–3.5 | 2.75 |
| Translucency ** | --- | 41% | 49% | 40.32% *** |
* Data published by representative manufacturers, ** transmittance of light as a percentage, *** obtained from literature source [21] for LT: low translucency Emax CAD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Alrabeah, G.; Al-Sowygh, A.H.; Almarshedy, S. Use of Ultra-Translucent Monolithic Zirconia as Esthetic Dental Restorative Material: A Narrative Review. Ceramics 2024, 7, 264-275. https://doi.org/10.3390/ceramics7010017
AMA Style
Alrabeah G, Al-Sowygh AH, Almarshedy S. Use of Ultra-Translucent Monolithic Zirconia as Esthetic Dental Restorative Material: A Narrative Review. Ceramics. 2024; 7(1):264-275. https://doi.org/10.3390/ceramics7010017
Chicago/Turabian StyleAlrabeah, Ghada, Abdulrahman H. Al-Sowygh, and Samaher Almarshedy. 2024. "Use of Ultra-Translucent Monolithic Zirconia as Esthetic Dental Restorative Material: A Narrative Review" Ceramics 7, no. 1: 264-275. https://doi.org/10.3390/ceramics7010017