
Revascularization of Non-Vital, Immature, Permanent Teeth with Two Bioceramic Cements: A Randomized Controlled Trial


1
Department of Endodontic and Operative Dentistry, Faculty of Dentistry, Damascus University, Damascus 0100, Syria
2
Department of Endodontic and Operative Dentistry, Faculty of Dentistry, International University for Science and Technology, Damascus 0100, Syria
3
Department of Periodontology, Faculty of Dentistry, Al Wadi International Private University, Homs 77, Syria
4
Department of Biomaterials and Bioengineering, INSERM UMR_S 1121, Strasbourg University, 67000 Strasbourg, France
5
Department of Endodontics and Conservative Dentistry, Faculty of Dental Medicine, Strasbourg University, 67000 Strasbourg, France
*
Author to whom correspondence should be addressed.
Ceramics 2024, 7(1), 86-100; https://doi.org/10.3390/ceramics7010007
Submission received: 16 November 2023
/
Revised: 17 January 2024
/
Accepted: 23 January 2024
/
Published: 25 January 2024
Abstract
:The aim of this study was to clinically and radiographically assess the effects of two bioceramic cements as coronal plug materials for the revascularization of non-vital, immature, permanent teeth with apical periodontitis. Twenty non-vital, immature, permanent, anterior teeth with apical periodontitis were included in this study. Samples were randomly divided into two groups based on the coronal plug materials used; group I (GI): Well Root PT (Vericom, Gangwon-do, Korea) and group II (GII): MTA Biorep (Itena Clinical, Paris, France) (n = 10). Follow-up was conducted clinically and radiographically for up to 12 months to evaluate the changes in root dimensions and resolution of the periapical disease and investigate the degree of success. Data were statistically analyzed using ANOVA tests and Mann–Whitney U tests at a 0.05 significance level. At 12 months, none of the patients in either test group had clinical signs/symptoms. There was a slight increase in root length (4.4% in GI and 3.4% in GII) and a slight increase in dentin wall thickness (10.2% in GI and 9.9% in GII) with no statistically significant (p > 0.05) differences. Whilst there was a significant decrease in lesion dimension in all patients after 12 moths of treatment (93% in GI and 91% in GII), there were no statistically significant differences between the two study groups (p > 0.05). Regarding the degree of success, all cases (100%) achieved the primary goal (the elimination of symptoms and the evidence of bony healing), while 60% in GI and 40% in GII achieved the secondary goal (increased root wall thickness and/or increased root length). No statistically significant difference was found between groups (p > 0.05). Both bioceramic cements showed satisfactory clinical and radiographic findings. Premixed calcium aluminosilicate and tricalcium silicate cements could be used as coronal plug materials in revascularization procedures. Bioceramic cements can be considered promising coronal plug materials for the revascularization of immature, permanent teeth with necrotic pulps and apical periodontitis due to their physicochemical and biological properties.
1. Introduction
Traumatic injuries are frequently seen in the anterior teeth of young children. Since the root development is completed two years after the tooth erupts into the oral cavity, one of the most common complications seen in traumatized teeth is incomplete root development. When the vitality of the pulp is lost before the completion of dentin deposition, it results in the development of a root with weak dentinal walls, increasing the probability of fracture [1]. Permanent immature teeth with necrotic pulp and periapical disease present a real challenge for endodontists, as the root canal space in these teeth is difficult to prepare and disinfect using endodontic files with standard protocols. Another difficulty could be encountered during root canal filling due to lack of apical barrier in the open apex [2,3].
Various treatment modalities have been described to treat the immature teeth, such as non-vital pulp therapy with calcium hydroxide or apexification with mineral trioxide aggregate (MTA) [4]. Although these techniques demonstrated successful results in the healing of apical pathosis and achieving apical closure, they have specific drawbacks, such as the persistence of thin and short root walls, as the hard tissue barrier only forms at the apical region, without additional root development [5].
As an alternative to conventional methods, regenerative endodontics has gained significant interest in the field of endodontics [6], which emphasizes the replacement of damaged structures such as dentine, dentin-pulp complex cells, and root structures [7]. An optimal coronal seal is recommended in this treatment, as it ensures a coronal barrier to prevent reinfection by coronal bacteria, which is considered one of the major causes of treatment failure [8]. Different biocompatible materials were recommended for the regenerative procedures.
Calcium silicate-based cements (CSCs) are commonly used in endodontic treatments, including pulpal regeneration and hard tissue repair [9,10]. Physicochemical interactions in the local environment, sealing ability, and biocompatibility are the main factors that explain the popularity of CSCs for use as materials in these clinical situations [11].
MTA was initially introduced as a calcium phosphate-based cement, but this material was recognized as a hydraulic calcium silicate cement in 2005 [12]. MTA was considered the recommended material for regenerative procedures to be applied over a blood clot, as it gives an excellent seal [13]. The application of MTA was technically challenging, and the material was displaced apically during condensation processes [14,15]. In addition to the extended setting time observed in many MTA brands, tooth discoloration was also observed after treatment [1]. Several modifications were performed in the chemical composition of this material to ameliorate its properties. MTA Biorep (Itena Clinical, Paris, France) contains calcium tungstate as the radiopaque element to avoid the negative effects of bismuth oxide [16], which was used in old versions. Moreover, the liquid of this product contains organic plasticizer, which could play an important role in the handling of this material [17]. This material demonstrated good chemical, physicochemical, and antibacterial properties [17].
Premixed CSCs were introduced in 2007 in both formulations, sealer and putty [18]. These formulations could avoid the errors which could be produced during mixing [17]. Several studies noted that any change or error in the powder liquid ratio during mixing could affect the setting time and physicochemical properties of these materials [17]. Recently, Well Root PT (Vericom, Gangwon-do, Republic of Korea), a novel premixed bioceramic material, was introduced in the dental market and its physicochemical, antibacterial, and mechanical properties were investigated [17,19]. Until now, there has been no clinical study that used this new material in a revascularization procedure. Moreover, the active element in this material is calcium aluminosilicate, whilst in MTA Biorep, the active element is tricalcium silicate. In addition, the present randomized controlled trial of the revascularization of non-vital, immature, permanent teeth with apical periodontitis is the first clinical study which clinically compares both bioceramic materials.
Therefore, the aim of the present study was to evaluate the effect of tricalcium silicate-based cement (MTA Biorep) and premixed calcium aluminosilicate-based cement (Well Root PT) on the clinical and radiographical success of the revascularization of non-vital, immature teeth with apical periodontitis at a follow-up one year later. The null hypothesis was that there would be no difference between the materials on the clinical and radiographical success of the revascularization procedure.
2. Materials and Methods
The protocol was approved by the Ethics Committee of Damascus University in Syria (n° MD-160124-179). The study was also registered to the ISRCTN Registry with ID: ISRCTN69846868 (https://www.isrctn.com/ISRCTN69846868, accessed on 1 November 2023). This study was designed as a randomized, controlled, parallel-group, and double-blinded (patients and assessor) clinical trial with an allocation ratio of 1:1, and the study adhered to the ethical values of the Helsinki Declaration.
2.1. Sample Size Calculation
The sample size was calculated using GPower 3.1 software (The G*Power Team, University of Düsseldorf, Düsseldorf, Germany). According to the means and standards deviations of Aly et al. [1], a total sample size of 18 cases (9 for each group) was estimated at an effect size of 1.71, a power of 0.95, and with a significance level of 0.05.
2.2. Study Design
From July 2020 to March 2022, consecutive patients referred for endodontic treatment to the Faculty of Dentistry, Damascus University, Damascus, Syria, were screened for enrollment. After comprehensive clinical and radiological examinations, a total of 20 teeth from 15 patients aged 9–25 years with non-vital, immature, permanent, anterior teeth with apical periodontitis were enrolled in the study.
The study was conducted in the Department of Endodontics, Faculty of Dentistry, Damascus University, Damascus, Syria. The study was designed in accordance with the CONSORT Statement 2010 guidelines to ensure quality and transparency. A blinded researcher conducted the randomization, while a different researcher performed the treatment. The patient was blinded to the assigned treatment group, and another researcher, blinded to the groups, conducted the data analysis. A total of 20 teeth were included in the present study according to the following inclusion and exclusion criteria:
Inclusion criteria: non-vital, permanent, anterior teeth with an open apex and apical periodontitis, that are single-rooted, with no post and core are needed for the final restoration of the tooth, and patients without any systemic diseases that could interfere with the normal healing process.
Exclusion criteria: teeth with vital pulp or complete root formation, teeth with previous endodontic treatment, patients allergic to the medications and antibiotics necessary to complete the treatment, and uncooperative patients.
After a comprehensive explanation of the treatment procedure, benefits, and possible complications, written informed consent was obtained from the patient or his parent.
2.3. Allocation & Randomization
Allocation in the study was carried out in a randomized manner with a 1:1 ratio using the sealed envelope method, where patients were assigned to two groups according to the coronal plug materials (n = 10). Group I (GI) involved sealing teeth with Well Root PT (Vericom, Gangwon-do, Republic of Korea), while Group II (GII) involved sealing teeth with MTA Biorep (Itena Clinical, Paris, France).
Sequence generation:
The simple randomization process involved using a computer-generated random sequence at www.randomizer.org (1 July 2020) to ensure a random and equitable distribution of participants, thereby enhancing internal validity and reducing selection bias.
Allocation concealment mechanism:
The sealed envelope method employed for allocation was implemented by enclosing twenty papers numbered from 1 to 20 within non transparent envelopes. Each patient, prior to treatment, selected an envelope, and the patient’s assigned group was determined by the number inside the chosen envelope.
2.4. Clinical Procedures
All procedures were performed by a single operator, Alaa Shaker, a PhD student in the Department of Endodontics at Damascus University, following the protocol recommended by the American Association of Endodontists [20]. Patients in both groups received the same treatment protocol, with the only variation being the application of the coronal plug material.
Before the treatment, a medical history and clinical symptoms were collected, and a preoperative examination was performed. A preoperative radiographic assessment with a standardized paralleling technique was performed using an intraoral digital X-ray sensor (Vatech Ez sensor, Gyeonggi-do, Republic of Korea). After pulp testing using PULP SPRAY (Cerkamed, Stalowa Wola, Poland) (ethyl chloride spray), local anesthesia was administered and teeth were isolated with a rubber dam. A conventional access cavity was prepared using a high-speed bur (Dentsply Maillefer, Tulsa, OK, USA) (Figure 1a), the working length was determined radiographically 1 mm short of the open apex and the canal was gently irrigated with 1.5% Sodium Hypochlorite (NaOCl) (20 mL/canal, 5 min), followed by saline (20 mL/canal, 5 min) at 1 mm before the working length. After drying the canal with paper points, triple antibiotic paste (TAP), prepared by mixing ciprofloxacin, metronidazole and minocycline powder with polyethylene glycol and propylene glycol at a concentration of 5 mg/mL, was applied. It was delivered into the root canal using a syringe to the level slightly under the cementoenamel junction (CEJ). The access cavity was closed with dry cotton and a 3–4 mm layer of 1DERFUL™ TEMPORARY FILLING (SKY DENT, New York, NY, USA) and the patient was released for a two-week period.
The treatment response was evaluated after two weeks. If the clinical signs/symptoms persisted, the first appointment’s treatment procedures were repeated. If symptoms were resolved, local anesthesia was administered using mepivacaine 3% without a vasoconstrictor, and the teeth were isolated with a rubber dam. Copious, gentle irrigation was applied with 20 mL of 17% ethylene diamine tetraacetic acid (EDTA) to remove the antibiotic paste, then the canal was dried with sterile paper points. Bleeding was induced by rotating a pre-curved K-file size #30 into the root canal at 2 mm past the apical foramen (Figure 1b). A dry cotton pellet was placed at a level that allows for 3–4 mm of restorative material and left in place for 10 min to allow the formation of a blood clot (Figure 1c). HEMOSPONGE Dental SL (Goodwill Lifesciences, Gujarat, India) was placed over the blood clot in order to minimize the apical displacement of the coronal plug material. GI and GII were applied following the manufacturer’s instructions (Table 1). Both cements were placed over the clot carefully (Figure 1d), a wet sterile cotton pellet was placed over both materials, and the access cavity was sealed temporarily with 1DERFUL™ TEMPORARY FILLING (SKY DENT, New York, NY, USA).
The following day, the temporary filling and the cotton pellet were replaced with a layer of glass ionomer cement (Ketac™ Molar, 3M ESPE, Germany) and composite resin (Filtek™ Z250, 3M ESPE, St. Paul, MN, USA), and a postoperative radiograph was taken using a standardized paralleling technique using an intraoral digital X-ray sensor and sensor holder (Vatech Ez sensor, Gyeonggi-do, Republic of Korea).
2.5. Evaluation of Treatment Outcomes
Main outcome:
- ▪
- The degree of success: assessed using the American Association of Endodontists’ criterion.
Secondary outcomes:
- ▪
- Pain on percussion: identified by gently tapping the tooth with a dental instrument.
- ▪
- Pain on biting: identified by asking the patient directly about its presence or absence.
- ▪
- Soft tissue swelling: identified through a visual examination.
- ▪
- Sinus tract: identified through a visual examination.
- ▪
- Mobility: identified by applying pressure using the tips of two metal instruments.
- ▪
- Pulp sensitivity: identified using Ethyl Chloride spray.
- ▪
- Change in root length: calculated radiographically using Image J software (version 1.54d).
- ▪
- Change in root thickness: calculated radiographically using Image J software.
- ▪
- Change in the periapical lesion area: calculated radiographically using Image J software.
The clinical and radiographic variables were registered at baseline and at 12 months after treatment. The images were transferred to the Image J software (National Institutes of Health, USA), mathematically corrected using the TurboReg plug-in (Biomedical Imaging Group, Swiss Federal Institute of Technology, Lausanne, Switzerland), and the measurements were performed by another researcher who was blind to the group being studied to avoid bias. A measurement scale in Image J software was set by comparing a known clinical dimension with its radiographic counterpart, calculating the scale as the number of pixels measured per millimeter length. This calibration process allowed for the measurement of root dimension changes on a millimeter scale.
The root lengths were measured as a straight line from the CEJ to the radiographic apex of the tooth (Figure 2a). The root length was measured pre- and post-operatively, the difference in length was calculated, and then the percentage of increase in length was calculated [21].
The root thickness and pulp width were measured at the same fixed level in three levels of the tooth (coronal, middle, apical) (Figure 2b). Root dentine thickness in each level was measured by subtracting the pulp space from the entire root thickness at the same fixed level, and then the measurements were averaged to obtain the total root dentine thickness as follows: (coronal root thickness − coronal pulp width) + (middle root thickness − middle pulp width) + (apical root thickness − apical pulp width)/3 [22].
Pre- and post-operative measurements were performed. The difference in thickness was calculated and the percentage increase in root dentine thickness was calculated.
The contour of the periapical radiolucency suggestive of periapical lesions were outlined with the cursor and the values obtained were automatically converted to square millimeters (mm2) [23] (Figure 2c).
The area of the periapical lesion was measured pre- and post-operatively, the difference in the area was calculated, then the percentage of change in the area was calculated.
The degree of success of the treatment was assessed using the American Association of Endodontists’ criterion, and the failure criterion was added as follows:
Score 0 (Failure): persistent clinical signs and symptoms and/or increased size of the periradicular lesion or internal/external resorption.
Score 1 (Primary goal): the elimination of symptoms and the evidence of bony healing.
Score 2 (Secondary goal): increased root wall thickness and/or increased root length.
Score 3 (Tertiary goal): positive response to vitality testing.
2.6. Statistical Analysis
Quantitative data (root length, root thickness, and the area of the periapical lesion) were collected, represented as mean and standard deviation (SD) values, and analyzed for significant differences using an ANOVA test. Qualitative data (the degree of success) were presented as frequencies and percentages, and the Mann–Whitney U test was utilized to evaluate significant differences in qualitative data. Statistical analysis was performed using S.P.S.S. version 19 (SPSS Inc., Chicago, IL, USA). The level of significance was set at p ≤ 0.05.
3. Results
A total of 20 non-vital, immature, permanent, anterior teeth with apical periodontitis in 15 patients (8 females and 7 males) were included in this study. The patients ranged in age from 9 to 25 with an average age of 14.7 years. The baseline demographic and clinical characteristics are detailed in (Table 2). No significant differences in study variables, such as sex, average age, tooth type, or cause of necrosis, were identified between the two groups (all p > 0.05). All cases were evaluated clinically and radiographically at 12 months and none of the patients were lost in the follow-up visit. The flow of the patients through the study is depicted as a flowchart in (Figure 3).
At 12 months of treatment, none of the patients in the two tested groups had pain on biting or percussion, swelling, abscess, sinus tract or pathological tooth mobility.
Radiographically, cases in GI showed a slightly greater change in root length (4.4%) and root thickness (10.2%) at the follow-up one year later. However, these differences were not statistically significant (p = 0.544 and p = 0.075, respectively). In contrast, lesion dimension was found to be significantly smaller after 1 year of follow-up (p < 0.001) (Table 3, Figure 4). The decrease in lesion dimension after 1 year of follow-up was 93%.
Radiographically, cases in GII showed a slightly greater change in root length (3.4%) and dentin wall thickness (9.9%) before and after 1 year of follow-up. However, these differences were not statistically significant (p = 0.068 and p = 0.244, respectively). In contrast, lesion dimension was found to be significantly smaller after 1 year of follow-up (p < 0.001) (Table 4, Figure 5). The decrease in lesion dimension after 1 year of follow-up was 91%.
After 1 year of follow-up, no statistically significant differences were found between the mean values of GI and GII among the changes in root length, root thickness, and lesion dimension (p > 0.05) (Figure 6).
4. Discussion
Ensuring a coronal seal is an essential aspect in pulp revascularization, typically achieved with biocompatible material such as MTA, which is favored by 85% of clinical studies [1,24]. However, long setting time, crown discoloration, and poor handling characteristics are some of MTA’s disadvantages [25], which necessitate the search for MTA’s replacement. Premixed bioceramic cement is considered an ideal substitute to MTA as it has excellent biocompatibility, sealing ability, and antibacterial activity [26]. Therefore, the clinical and radiographic evaluation of premixed bioceramic cement in the coronal seal in pulp revascularization of non-vital, immature teeth is important.
In the present study, no instrumentation procedures were performed because mechanical preparation may further weaken the fragile and thin dentin walls, and there is no mechanical instrumentation recommended in the most recent guidelines of AAE for revascularization procedures [27].
NaOCl solution was used for irrigation at a low concentration (1.5%), because it significantly reduces the stem cell survival in higher concentrations [28,29].
Triple antibiotic paste was applied as a medication due to its established effectiveness in disinfecting necrotic root canals [27,30], and used at a concentration of 5 mg/mL to avoid damage of stem cells from the apical papilla (SCAPs) [20].
At the second visit, the anesthesia was given without a vasoconstrictor to minimize the possibility of inadequate intra-canal bleeding [27]. After that, 17% EDTA solution was applied to the superficial dentin layer as a method of conditioning, due to its demineralizing effect with the release of growth factors and elimination of the smear layer [31]. The bleeding was induced into the root canal to create a cross-linked fibrin meshwork that serves as a biological scaffold containing essential growth factors for supporting endogenous stem cell migration, proliferation, and differentiation. In addition, mechanical irritation of the periapical tissues also stimulates the influx of different types of mesenchymal stem cells (MSCs) into the canal space, which can restore the physiological structure and function of the pulp dentin complex [32,33].
The effectiveness of revascularization has been demonstrated only in teeth with disinfected root canals. Therefore, obtaining a bacteria-tight coronal seal was deemed necessary to prevent bacterial infiltration into the pulp space before initiating the revascularization process [34]. Moreover, the coronal plug material is required to be bioactive, biocompatible, noncytotoxic, and antimicrobial since it is in direct contact with the blood clot [7]. Premixed bioceramic cement has the necessary assets for this procedure due to its excellent biocompatibility and sealing ability, and could overcome various disadvantages of MTA [26]. Unlike MTA, it is a premixed material, which offers several advantages including greater uniformity and the ability to inject only the required amount, thus reducing material waste [35,36]. Moreover, premixed bioceramic cement is a fast-setting product, it is used clinically in the form of a capsule and is known for its excellent antibacterial properties [17,37].
There is no clinical study in the literature which has used this new material (Well-Root PT) in a revascularization procedure. Moreover, the new calcium aluminosilicate was rarely clinically studied. One recent clinical work, Joo et al., studied the success rates of pulpotomy using Well-Root PT compared to ProRoot MTA and reported similarly high success rates (82% for Well-Root PT and 92% for ProRoot MTA) with no significant differences between the two materials [11].
In the present study, no signs of swelling, abscess, sinus tract or pathological tooth mobility were observed during the clinical examination. Teeth were not sensitive to percussion and palpation, possibly due to the bactericidal efficacy of TAP [38]. These results are in accordance with Gibbs et al., who observed clinical success in all 20 treated teeth in their study at the follow-up 12 months after revascularization [39].
There was a slight increase in root length (4.4% in group I and 3.4% in group II) and a slight increase in dentin wall thickness (10.25% in group I and 9.9% in group II) after 1 year of follow-up (p > 0.05). This slight, non-significant increase may be due to the need for a longer follow-up period, as the AAE suggested a follow-up period ranging between 6 and 12 months to follow the resolution of apical radiolucency and 12–24 months to follow the increase in root wall width and root length [20].
There were no statistically significant differences regarding the changes in root length and dentin wall thickness between the two groups (p > 0.05), which can be explained by the fact that calcium aluminosilicate cement and tricalcium silicate-based cement have similar osteogenic/dentinogenic properties [40]. In addition, various in vitro studies have demonstrated that Well Root PT has similar or superior physical and chemical properties compared to MTA; this product also ensures better handling than powder-liquid materials [11]. Moreover, several physicochemical and biological properties are identical in both materials [17]. These results were comparable to Aly et al., who reported that the use of MTA resulted in increased root length (5.02 (±1.65) %) over 12 months of follow-up [1]. In accordance with the result of the present study, Saoud et al. reported that there was a 5% average increase in root length and a 21% average increase in root thickness at 12 months when using MTA [39]. Moreover, Wikström et al. showed an increase in root length (11%) and in root width (30%) when using MTA or premixed bioceramic putty (calcium silicate-based) in revascularization [41]. The higher increase percentages could be related to the longer follow-up period (24 months) compared the follow-up period of the present work (12 months).
In terms of changes in lesion dimension, there was a highly statistically significant decrease in lesion dimension for all the cases. The percentage of decrease in the lesion dimension after 1 year of follow-up was 93% in group I and 91% in group II. There was no statistically significant difference in the percentage of decrease in lesion dimension between the two groups (p > 0.05). This may be due to the effective coronal seal attained by both materials and the standardized disinfection procedures [1]. These findings agreed with many previous studies which used MTA and premixed bioceramic putty (calcium silicate-based) as coronal sealing materials in revascularization procedures in immature teeth and reported significant resolution of apical lesions [41,42,43,44,45,46,47].
The American Association of Endodontists’ criterion was used in the present study, in which the degree of success of RET is measured by the possibility of achieving the primary goal (the elimination of symptoms and the evidence of bony healing), the secondary goal (increased root wall thickness and/or increased root length), and the tertiary goal (positive response to vitality testing). In the present study, there was no statistically significant difference in the degree of success between groups. Therefore, the null hypothesis must be accepted (p > 0.05). All cases achieved primary success (100%) in both groups. The regenerative endodontic treatment resulted in the absence of clinical symptoms and resolution of the periapical lesion in all clinical cases. However, the secondary success rate was 60% in GI and 40% in GII. In contrast, there were no cases of failure during the follow-up period (12 months) in either group. Among both groups, no case achieved tertiary success within this clinical study after 12 months of follow-up. Failure to respond to the pulp vitality test does not necessarily indicate a lack or absence of vitality, because a number of cases had a negative test result despite the presence of radiographic evidence of root development, which indicates the presence of vital tissue within the canal space [48]. In addition, it is difficult to evaluate the response to vitality tests due to the presence of a multi-layered coronal seal over the scaffold used.
The use of both materials resulted in a similar degree of success which could be explained by the fact that premixed calcium aluminosilicate cement, such as MTA, has high biocompatibility and success rates and is capable of achieving coronal and apical seals. Furthermore, Song et al. reported that the use of premixed bioceramic putty showed clinically acceptable chemomechanical properties and favorable mineralization processes [49]. Bukhari et al. indicated that the use of premixed bioceramic putty (based on tricalcium silicate) and MTA resulted in apical healing with root maturation in 75% of teeth when used in RET in immature teeth with pulp necrosis [47]. Also, the present study was in agreement with the study by Cymerman et al., who used premixed bioceramic putty in RET, and reported that all periapical lesions were resolved, and all teeth showed partial to complete apical closure at the follow-up visit [46]. Also, these findings are in agreement with Peng et al., who reported a success rate of 93% when MTA was used [50]. Until now, the level of evidence for the use of premixed bioceramics other than MTA in RET is low, as it is generally seen in in vitro studies and case reports [51,52].
The limitations of the present study were as follows. Patients with the included criteria are not as readily available. Moreover, the study’s follow-up period of 12 months may be relatively short for assessing the full range of regenerative outcomes. An extended follow-up period would provide valuable insights into the long-term success and stability of pulp revascularization. While statistical significance was not observed for differences between the two materials in the findings of this study, another study with a larger sample size could show different results. This limited sample size is one of the limitations of this study, and a study with a larger sample size should be conducted to achieve more accurate results, thus enhancing the external validity of the findings. In addition, a longer follow-up period should be investigated to evaluate coronal discoloration and obliteration in the root canal. Within the limitations of the present study, revascularization of immature teeth with necrotic pulps and apical periodontitis using different coronal plug materials was successful in accomplishing satisfactory clinical and radiographic findings, making it an acceptable option while taking into consideration the necessity for further clinical studies with larger sample sizes and longer recall periods to assess the risk, success, and the benefits of these materials. In addition, histological studies should further investigate the actual contents of the pulp space after revascularization procedures using these materials.
5. Conclusions
Both bioceramic cements showed satisfactory clinical and radiographical success when used in the revascularization procedure. Premixed calcium aluminosilicate and tricalcium silicate-based cements can be considered promising coronal plug materials in the revascularization of immature, permanent teeth with necrotic pulps and apical periodontitis due to their physicochemical and biological properties.
Author Contributions
Conceptualization, A.S. and M.S.R.; methodology, A.S.; software, M.A.; validation, N.K.; formal analysis, A.S.; writing—original draft preparation, A.S., M.A. and M.S.R.; writing—review and editing, N.K.; supervision, M.A.; project administration, M.S.R.; funding acquisition, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The protocol was approved by the Ethics Committee of Damascus University in Syria (n° MD-160124-179).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available from the first and the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Aly, M.M.; Taha, S.E.E.D.; El Sayed, M.A.; Youssef, R.; Omar, H.M. Clinical and radiographic evaluation of Biodentine and Mineral Trioxide Aggregate in revascularization of non-vital immature permanent anterior teeth (randomized clinical study). Int. J. Paediatr. Dent. 2019, 29, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Chueh, L.-H.; Ho, Y.-C.; Kuo, T.-C.; Lai, W.-H.; Chen, Y.-H.M.; Chiang, C.-P. Regenerative endodontic treatment for necrotic immature permanent teeth. J. Endod. 2009, 35, 160–164. [Google Scholar] [CrossRef]
- Trope, M. Treatment of the immature tooth with a non–vital pulp and apical periodontitis. Dent. Clin. 2010, 54, 313–324. [Google Scholar] [CrossRef]
- Wigler, R.; Kaufman, A.Y.; Lin, S.; Steinbock, N.; Hazan-Molina, H.; Torneck, C.D. Revascularization: A treatment for permanent teeth with necrotic pulp and incomplete root development. J. Endod. 2013, 39, 319–326. [Google Scholar] [CrossRef]
- Shin, S.; Albert, J.; Mortman, R. One step pulp revascularization treatment of an immature permanent tooth with chronic apical abscess: A case report. Int. Endod. J. 2009, 42, 1118–1126. [Google Scholar] [CrossRef]
- Smith, A.J.; Cooper, P.R. Regenerative endodontics: Burning questions. J. Endod. 2017, 43, S1–S6. [Google Scholar] [CrossRef]
- Hameed, M.H.; Gul, M.; Ghafoor, R.; Badar, S.B. Management of immature necrotic permanent teeth with regenerative endodontic procedures-a review of literature. J. Pak. Med. Assoc. 2019, 69, 1514–1520. [Google Scholar] [CrossRef]
- Garcia-Godoy, F.; Murray, P.E. Recommendations for using regenerative endodontic procedures in permanent immature traumatized teeth. Dent. Traumatol. 2012, 28, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Dawood, A.E.; Parashos, P.; Wong, R.H.; Reynolds, E.C.; Manton, D.J. Calcium silicate-based cements: Composition, properties, and clinical applications. J. Investig. Clin. Dent. 2017, 8, e12195. [Google Scholar] [CrossRef] [PubMed]
- Bossù, M.; Iaculli, F.; Di Giorgio, G.; Salucci, A.; Polimeni, A.; Di Carlo, S. Different pulp dressing materials for the pulpotomy of primary teeth: A systematic review of the literature. J. Clin. Med. 2020, 9, 838. [Google Scholar] [CrossRef]
- Joo, Y.; Lee, T.; Jeong, S.J.; Lee, J.-H.; Song, J.S.; Kang, C.-M. A randomized controlled clinical trial of premixed calcium silicate-based cements for pulpotomy in primary molars. J. Dent. 2023, 137, 104684. [Google Scholar] [CrossRef]
- Camilleri, J. Classification of hydraulic cements used in dentistry. Front. Dent. Med. 2020, 1, 9. [Google Scholar] [CrossRef]
- Faizuddin, U.; Solomon, R.V.; Mattapathi, J.; Guniganti, S.S. Revitalization of traumatized immature tooth with platelet-rich fibrin. Contemp. Clin. Dent. 2015, 6, 574–576. [Google Scholar]
- Timmerman, A.; Parashos, P. Delayed root development by displaced mineral trioxide aggregate after regenerative endodontics: A case report. J. Endod. 2017, 43, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Llaquet, M.; Mercadé, M.; Plotino, G. Regenerative endodontic procedures: A review of the literature and a case report of an immature central incisor. G. Ital. Endod. 2017, 31, 65–72. [Google Scholar] [CrossRef]
- Kharouf, N.; Zghal, J.; Addiego, F.; Gabelout, M.; Jmal, H.; Haikel, Y.; Bahlouli, N.; Ball, V. Tannic acid speeds up the setting of mineral trioxide aggregate cements and improves its surface and bulk properties. J. Colloid Interface Sci. 2021, 589, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Ashi, T.; Mancino, D.; Hardan, L.; Bourgi, R.; Zghal, J.; Macaluso, V.; Al-Ashkar, S.; Alkhouri, S.; Haikel, Y.; Kharouf, N. Physicochemical and antibacterial properties of bioactive retrograde filling materials. Bioengineering 2022, 9, 624. [Google Scholar] [CrossRef] [PubMed]
- Debelian, G.; Trope, M. The use of premixed bioceramic materials in endodontics. G. Ital. Endod. 2016, 30, 70–80. [Google Scholar] [CrossRef]
- Ashi, T.; Richert, R.; Mancino, D.; Jmal, H.; Alkhouri, S.; Addiego, F.; Kharouf, N.; Haïkel, Y. Do the Mechanical Properties of Calcium-Silicate-Based Cements Influence the Stress Distribution of Different Retrograde Cavity Preparations? Materials 2023, 16, 3111. [Google Scholar] [CrossRef] [PubMed]
- AAE. AAE Clinical Considerations for a Regenerative Procedure. Available online: https://www.aae.org/specialty/wp-content/uploads/sites/2/2021/08/ClinicalConsiderationsApprovedByREC062921.pdf (accessed on 1 February 2020).
- Jiang, X.; Liu, H.; Peng, C. Clinical and radiographic assessment of the efficacy of a collagen membrane in regenerative endodontics: A randomized, controlled clinical trial. J. Endod. 2017, 43, 1465–1471. [Google Scholar] [CrossRef]
- Ulusoy, A.T.; Turedi, I.; Cimen, M.; Cehreli, Z.C. Evaluation of blood clot, platelet-rich plasma, platelet-rich fibrin, and platelet pellet as scaffolds in regenerative endodontic treatment: A prospective randomized trial. J. Endod. 2019, 45, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Ordinola-Zapata, R.; Bramante, C.M.; Duarte, M.H.; Fernandes, L.M.R.; Camargo, E.J.; De Moraes, I.G.; Bernardineli, N.; Vivan, R.R.; Capelozza, A.L.A.; Garcia, R.B. The influence of cone-beam computed tomography and periapical radiographic evaluation on the assessment of periapical bone destruction in dog’s teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Kontakiotis, E.G.; Filippatos, C.G.; Tzanetakis, G.N.; Agrafioti, A. Regenerative endodontic therapy: A data analysis of clinical protocols. J. Endod. 2015, 41, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review—Part III: Clinical applications, drawbacks, and mechanism of action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.-J.; Kim, Y.-J.; Vu, H.T.; Park, J.-H.; Shin, S.-J.; Dashnyam, K.; Knowles, J.C.; Lee, H.-H.; Jun, S.-K.; Han, M.-R. Physicochemical, Biological, and Antibacterial Properties of Four Bioactive Calcium Silicate-Based Cements. Pharmaceutics 2023, 15, 1701. [Google Scholar] [CrossRef]
- Wei, X.; Yang, M.; Yue, L.; Huang, D.; Zhou, X.; Wang, X.; Zhang, Q.; Qiu, L.; Huang, Z.; Wang, H. Expert consensus on regenerative endodontic procedures. Int. J. Oral Sci. 2022, 14, 55. [Google Scholar] [CrossRef]
- Trevino, E.G.; Patwardhan, A.N.; Henry, M.A.; Perry, G.; Dybdal-Hargreaves, N.; Hargreaves, K.M.; Diogenes, A. Effect of irrigants on the survival of human stem cells of the apical papilla in a platelet-rich plasma scaffold in human root tips. J. Endod. 2011, 37, 1109–1115. [Google Scholar] [CrossRef]
- Martin, D.E.; De Almeida, J.F.A.; Henry, M.A.; Khaing, Z.Z.; Schmidt, C.E.; Teixeira, F.B.; Diogenes, A. Concentration-dependent effect of sodium hypochlorite on stem cells of apical papilla survival and differentiation. J. Endod. 2014, 40, 51–55. [Google Scholar] [CrossRef]
- Wang, H.-J.; Chen, Y.-H.M.; Chen, K.-L. Conservative treatment of immature teeth with apical periodontitis using triple antibiotic paste disinfection. J. Dent. Sci. 2016, 11, 196–201. [Google Scholar] [CrossRef]
- Subbiya, A.; Saatwika, L.; Tamilselvi, R. Regenerative endodontics on necrotic mature permanent teeth—A review. Eur. J. Mol. Clin. Med. 2020, 7, 2121–2127. [Google Scholar]
- Lin, L.; Huang, G.T.J.; Sigurdsson, A.; Kahler, B. Clinical cell-based versus cell-free regenerative endodontics: Clarification of concept and term. Int. Endod. J. 2021, 54, 887–901. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Lu, J.; Jiang, Q.; Haapasalo, M.; Qian, J.; Tay, F.R.; Shen, Y. Biomaterial scaffolds for clinical procedures in endodontic regeneration. Bioact. Mater. 2022, 12, 257–277. [Google Scholar] [CrossRef] [PubMed]
- Dudeja, P.G.; Grover, S.; Srivastava, D.; Dudeja, K.K.; Sharma, V. Pulp revascularization-it’s your future whether you know it or not? J. Clin. Diagn. Res. JCDR 2015, 9, ZR01. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, S.; Watanabe, S.; Okiji, T. Effects of heating on the physical properties of premixed calcium silicate-based root canal sealers. J. Oral Sci. 2021, 63, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Motwani, N.; Ikhar, A.; Nikhade, P.; Chandak, M.; Rathi, S.; Dugar, M.; Rajnekar, R. Premixed bioceramics: A novel pulp capping agent. J. Conserv. Dent. JCD 2021, 24, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Choi, N.; Kim, S. Color Change in Tooth Induced by Various Calcium Silicate-Based Pulp-Capping Materials. J. Korean Acad. Pediatr. Dent. 2021, 48, 280–290. [Google Scholar] [CrossRef]
- do Couto, A.M.; Espaladori, M.C.; Leite, A.P.P.; Martins, C.C.; de Aguiar, M.C.F.; Abreu, L.G. A systematic review of pulp revascularization using a triple antibiotic paste. Pediatr. Dent. 2019, 41, 341–353. [Google Scholar] [PubMed]
- Saoud, T.M.A.; Zaazou, A.; Nabil, A.; Moussa, S.; Lin, L.M.; Gibbs, J.L. Clinical and radiographic outcomes of traumatized immature permanent necrotic teeth after revascularization/revitalization therapy. J. Endod. 2014, 40, 1946–1952. [Google Scholar] [CrossRef]
- Eid, A.A.; Niu, L.-N.; Primus, C.M.; Opperman, L.A.; Pashley, D.H.; Watanabe, I.; Tay, F.R. In vitro osteogenic/dentinogenic potential of an experimental calcium aluminosilicate cement. J. Endod. 2013, 39, 1161–1166. [Google Scholar] [CrossRef]
- Wikström, A.; Brundin, M.; Romani Vestman, N.; Rakhimova, O.; Tsilingaridis, G. Endodontic pulp revitalization in traumatized necrotic immature permanent incisors: Early failures and long-term outcomes—A longitudinal cohort study. Int. Endod. J. 2022, 55, 630–645. [Google Scholar] [CrossRef]
- Al-Tammami, M.F.; Al-Nazhan, S.A. Retreatment of failed regenerative endodontic of orthodontically treated immature permanent maxillary central incisor: A case report. Restor. Dent. Endod. 2017, 42, 65–71. [Google Scholar] [CrossRef]
- Carmen, L.; Asunción, M.; Beatriz, S.; Rosa, Y.-V. Revascularization in immature permanent teeth with necrotic pulp and apical pathology: Case series. Case Rep. Dent. 2017, 2017, 3540159. [Google Scholar] [CrossRef]
- Žižka, R.; Šedý, J.; Voborná, I. Retreatment of failed revascularization/revitalization of immature permanent tooth—A case report. J. Clin. Exp. Dent. 2018, 10, e185–e188. [Google Scholar]
- Ajram, J.; Khalil, I.; Gergi, R.; Zogheib, C. Management of an immature necrotic permanent molar with apical periodontitis treated by regenerative endodontic protocol using calcium hydroxide and MM-MTA: A case report with two years follow up. Dent. J. 2019, 7, 1. [Google Scholar] [CrossRef]
- Cymerman, J.J.; Nosrat, A. Regenerative endodontic treatment as a biologically based approach for non-surgical retreatment of immature teeth. J. Endod. 2020, 46, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Kohli, M.R.; Setzer, F.; Karabucak, B. Outcome of revascularization procedure: A retrospective case series. J. Endod. 2016, 42, 1752–1759. [Google Scholar] [CrossRef]
- Staffoli, S.; Plotino, G.; Nunez Torrijos, B.G.; Grande, N.M.; Bossù, M.; Gambarini, G.; Polimeni, A. Regenerative endodontic procedures using contemporary endodontic materials. Materials 2019, 12, 908. [Google Scholar] [CrossRef]
- Song, M.; Lee, S.-M.; Bang, J.-Y.; Kim, R.H.; Kwak, S.W.; Kim, H.-C. Chemomechanical Properties and Biocompatibility of Various Premixed Putty-type Bioactive Ceramic Cements. J. Endod. 2023, 49, 1713–1721. [Google Scholar] [CrossRef]
- Peng, C.; Yang, Y.; Zhao, Y.; Liu, H.; Xu, Z.; Zhao, D.; Qin, M. Long-term treatment outcomes in immature permanent teeth by revascularisation using MTA and GIC as canal-sealing materials: A retrospective study. Int. J. Paediatr. Dent. 2017, 27, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Adnan, S.; Ullah, R. Top-cited articles in regenerative endodontics: A bibliometric analysis. J. Endod. 2018, 44, 1650–1664. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Xu, X. Bioceramics in endodontics: Updates and future perspectives. Bioengineering 2023, 10, 354. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Intrabuccal images: (a) access cavity; (b) bleeding by rotating a pre-curved K-file; (c) blood clot formation; (d) bioceramic application.
Figure 1.
Intrabuccal images: (a) access cavity; (b) bleeding by rotating a pre-curved K-file; (c) blood clot formation; (d) bioceramic application.

Figure 2.
Digital measurements using image J software: (a) root length; (b) root dentin thickness; (c) the area of the apical lesion.
Figure 2.
Digital measurements using image J software: (a) root length; (b) root dentin thickness; (c) the area of the apical lesion.

Figure 3.
The CONSORT flowchart showing the flow of patients through the study.

Figure 4.
Comparison of GI (BC Putty) before and after one year of follow-up. An increase in root length and root thickness values and a decrease in lesion dimension values were observed. (* p < 0.05).
Figure 4.
Comparison of GI (BC Putty) before and after one year of follow-up. An increase in root length and root thickness values and a decrease in lesion dimension values were observed. (* p < 0.05).

Figure 5.
Comparison of GII (MTA) before and after one year of follow-up. An increase in root length and root thickness values and a decrease in lesion dimension values were observed. (* p < 0.05).
Figure 5.
Comparison of GII (MTA) before and after one year of follow-up. An increase in root length and root thickness values and a decrease in lesion dimension values were observed. (* p < 0.05).

Figure 6.
Comparison between GI (BC Putty) and GII (MTA) after 1 year of follow-up regarding the increase in root length and root thickness values and the decrease in lesion dimension values.
Figure 6.
Comparison between GI (BC Putty) and GII (MTA) after 1 year of follow-up regarding the increase in root length and root thickness values and the decrease in lesion dimension values.

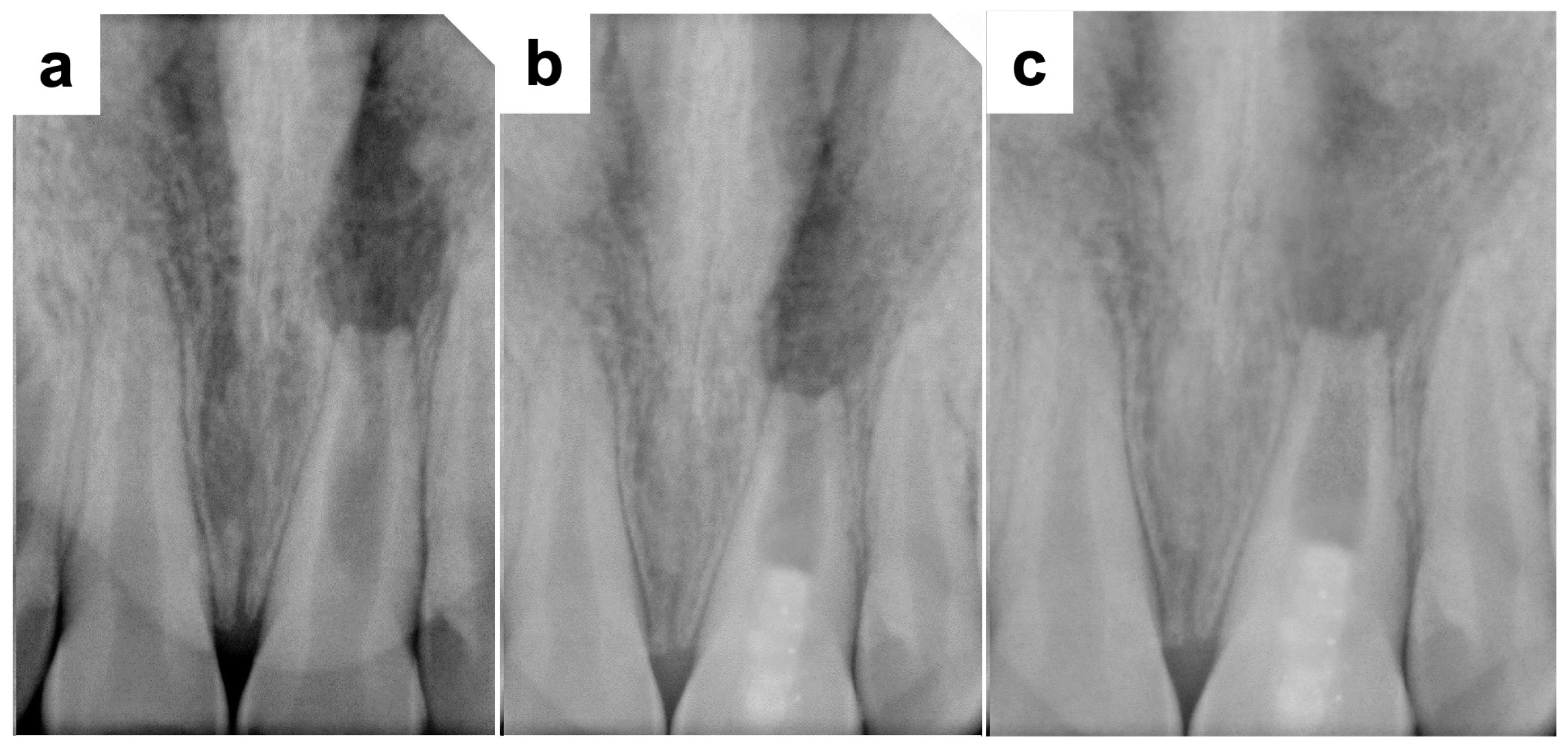
Figure 7.
A primary success case from GI. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with BC Putty. (c) A radiograph at the 12-month follow-up showed the resolution of the apical lesion without root development after revascularization.
Figure 7.
A primary success case from GI. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with BC Putty. (c) A radiograph at the 12-month follow-up showed the resolution of the apical lesion without root development after revascularization.

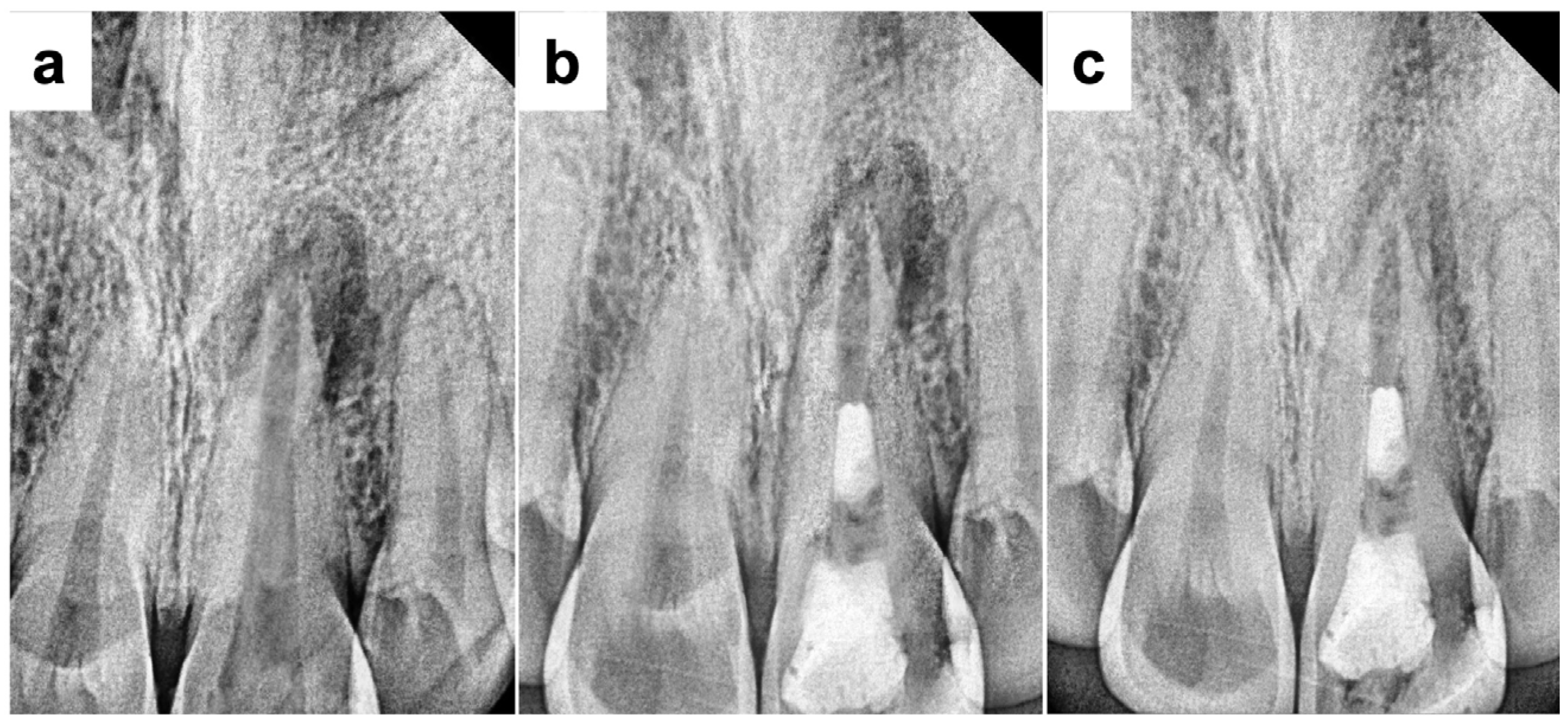
Figure 8.
A primary success case from GII. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with MTA. (c) A radiograph at the 12-month follow-up showed the resolution of the apical lesion without root development after revascularization.
Figure 8.
A primary success case from GII. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with MTA. (c) A radiograph at the 12-month follow-up showed the resolution of the apical lesion without root development after revascularization.

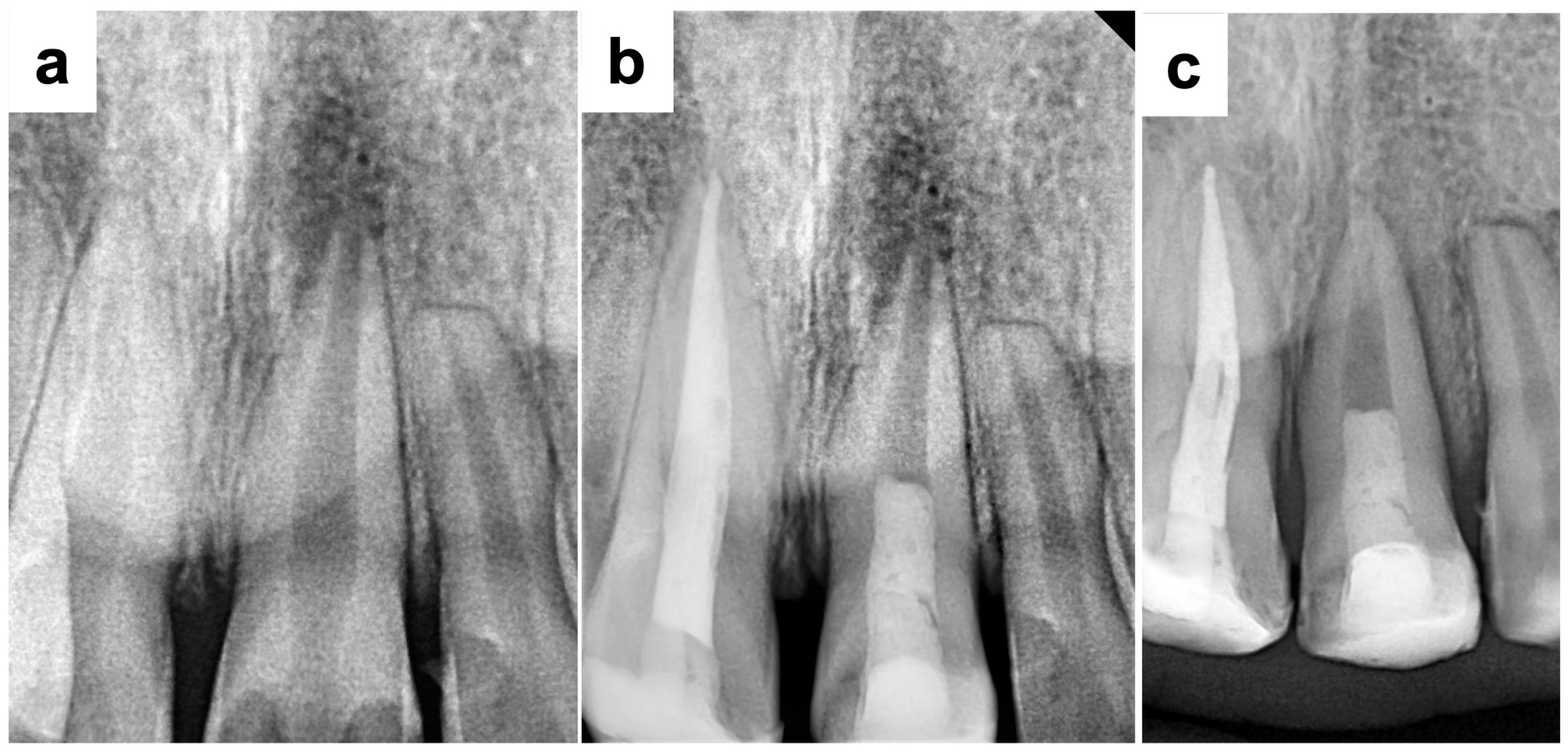
Figure 9.
A secondary success case from GI. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with BC Putty. (c) A radiograph at the 12-month follow-up showed increased thickening of the canal walls and apical closure after revascularization.
Figure 9.
A secondary success case from GI. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with BC Putty. (c) A radiograph at the 12-month follow-up showed increased thickening of the canal walls and apical closure after revascularization.

Figure 10.
A secondary success case from GII. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with MTA. (c) A radiograph at the 12-month follow-up showed increased thickening of the canal walls and apical closure after revascularization.
Figure 10.
A secondary success case from GII. (a) Preoperative radiograph showed an upper left central incisor with an open apex and periapical radiolucency. (b) Immediate postoperative radiograph showed a coronal root canal filling with MTA. (c) A radiograph at the 12-month follow-up showed increased thickening of the canal walls and apical closure after revascularization.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Chemical composition, manufacturer, and mixing procedures of both tested materials.
| Materials | Manufacturer | Mixing | Composition |
|---|---|---|---|
| Well Root PT | Vericom, Gangwon-do, Republic of Korea | Premixed | Calcium aluminosilicate, Zirconium oxide, Thickening agent |
| MTA Biorep | Itena Clinical, Paris, France | 4 drops + 1 capsule | Powder: Tricalcium silicate, Dicalcium silicate, Tricalcium aluminate, Calcium oxide, Calcium tungstate Liquid: Water and Plasticizer |
Table 2.
The baseline demographic and clinical characteristics of the participating patients.
| Group I (n = 10) n (%) | Group II (n = 10) n (%) | |
|---|---|---|
| Sex | ||
| Male | 6 (60.0) | 5 (50.0) |
| Female | 4 (40.0) | 5 (50.0) |
| Age (y) | 15.7 ± 6.5 | 13.7 ± 4.4 |
| Tooth type | ||
| 11 | 4 (40.0) | 3 (30.0) |
| 12 | 0 (0.0) | 1 (10.0) |
| 21 | 4 (40.0) | 5 (50.0) |
| 22 | 2 (20.0) | 1 (10.0) |
| Cause of necrosis | ||
| Trauma | 10 (100) | 10 (100) |
Table 3.
Comparing root length, root thickness, and lesion dimension values in GI (BC Putty) before and after one year of follow-up.
Table 3.
Comparing root length, root thickness, and lesion dimension values in GI (BC Putty) before and after one year of follow-up.
| Variable | Before | After 1y | The Mean of Change (%) | p-Value |
|---|---|---|---|---|
| Root length (mm) | 20.04 (±3.8) | 20.93 (±3.93) | +4.4 | 0.544 |
| Root thickness (mm) | 3.6 (±0.51) | 3.97 (±0.6) | +10.2 | 0.075 |
| lesion dimension (mm2) | 31.02 (±10.94) | 2.15 (±2.04) | −93 | <0.001 |
Table 4.
Comparing root length, root thickness, and lesion dimension values in GII (MTA) before and after one year of follow-up.
Table 4.
Comparing root length, root thickness, and lesion dimension values in GII (MTA) before and after one year of follow-up.
| Variable | Before | After 1y | The Mean of Change (%) | p-Value |
|---|---|---|---|---|
| Root length (mm) | 17.9 (±2.64) | 18.53 (±3) | +3.4 | 0.068 |
| Root thickness (mm) | 2.64 (±0.35) | 2.9 (±0.95) | +9.9 | 0.244 |
| lesion dimension (mm2) | 25.03 (±12.93) | 2 (±1.53) | −91 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shaker, A.; Rekab, M.S.; Alharissy, M.; Kharouf, N. Revascularization of Non-Vital, Immature, Permanent Teeth with Two Bioceramic Cements: A Randomized Controlled Trial. Ceramics 2024, 7, 86-100. https://doi.org/10.3390/ceramics7010007
AMA Style
Shaker A, Rekab MS, Alharissy M, Kharouf N. Revascularization of Non-Vital, Immature, Permanent Teeth with Two Bioceramic Cements: A Randomized Controlled Trial. Ceramics. 2024; 7(1):86-100. https://doi.org/10.3390/ceramics7010007
Chicago/Turabian StyleShaker, Alaa, Mohamed Salem Rekab, Mohammad Alharissy, and Naji Kharouf. 2024. "Revascularization of Non-Vital, Immature, Permanent Teeth with Two Bioceramic Cements: A Randomized Controlled Trial" Ceramics 7, no. 1: 86-100. https://doi.org/10.3390/ceramics7010007