
The Resolution of Obstructive Sleep Apnea in a Patient with Goiter after Total Thyroidectomy: A Case Report

 , , ,
, , ,
Abstract
:1. Introduction
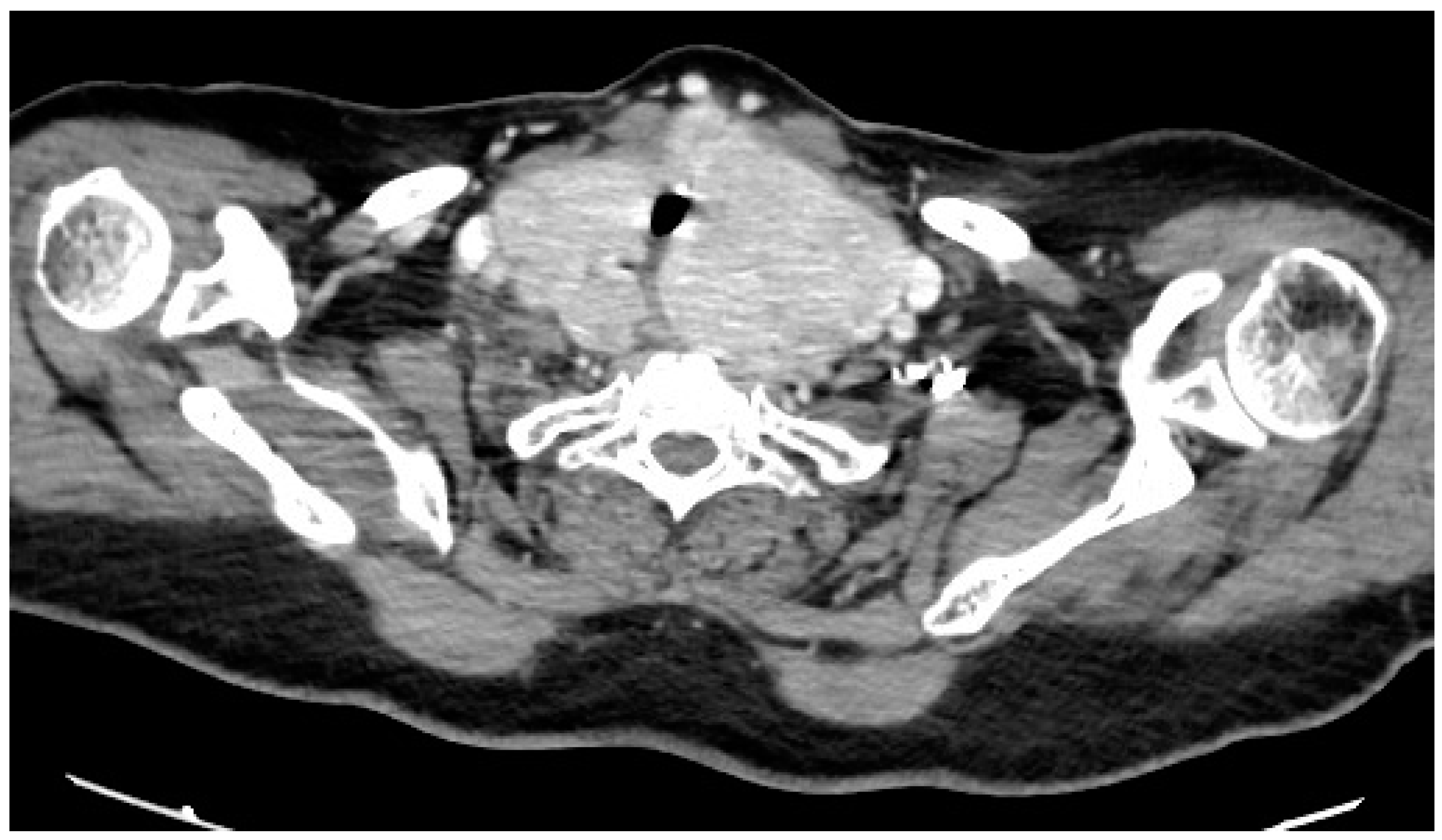
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hirani, R.; Smiley, A. A Scoping Review of Sleep Apnea: Where Do We Stand? Life 2023, 13, 387. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Bonitati, A. Obstructive Sleep Apnea Syndrome—A Review for Primary Care Physicians and Pulmonologists. Rhode Isl. Med. J. 2021, 104, 10–13. [Google Scholar]
- Chang, J.L.; Goldberg, A.N.; Alt, J.A.; Mohammed, A.; Ashbrook, L.; Auckley, D.; Ayappa, I.; Bakhtiar, H.; Barrera, J.E.; Bartley, B.L.; et al. International Consensus Statement on Obstructive Sleep Apnea. Int. Forum Allergy Rhinol. 2023, 13, 1061–1482. [Google Scholar] [CrossRef] [PubMed]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Molnar, V.; Lakner, Z.; Molnar, A.; Tarnoki, D.L.; Tarnoki, A.D.; Kunos, L.; Jokkel, Z.; Tamas, L. The Predictive Role of the Upper-Airway Adipose Tissue in the Pathogenesis of Obstructive Sleep Apnoea. Life 2022, 12, 1543. [Google Scholar] [CrossRef] [PubMed]
- Deegan, P.C.; McNamara, V.M.; Morgan, W.E. Goitre: A cause of obstructive sleep apnoea in euthyroid patients. Eur. Respir. J. 1997, 10, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, T.; Leong, A.C.; Pang, L.; Chevretton, E.; Jeannon, J.P.; Simo, R. Multinodular thyroid goitre causing obstructive sleep apnoea syndrome. J. Laryngol. Otol. 2012, 126, 190–195. [Google Scholar] [CrossRef]
- Reiher, A.E.; Mazeh, H.; Schaefer, S.; Chen, H.; Sippel, R.S. Thyroidectomy decreases snoring and sleep apnea symptoms. Thyroid 2012, 22, 1160–1164. [Google Scholar] [CrossRef]
- Masarwy, R.; Kampel, L.; Ungar, O.J.; Warshavsky, A.; Horowitz, G.; Rosenzweig, E.; Tauman, R.; Muhanna, N. The impact of thyroidectomy on obstructive sleep apnea: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2022, 279, 5801–5811. [Google Scholar] [CrossRef]
- Yuan, J.; Qi, S.; Zhang, X.; Lai, H.; Li, X.; Xiaoheng, C.; Li, Z.; Yao, S.; Ding, Z. Local symptoms of Hashimoto’s thyroiditis: A systematic review. Front. Endocrinol. 2022, 13, 1076793. [Google Scholar] [CrossRef]
- Tunc, M.; Sazak, H.; Karlilar, B.; Ulus, F.; Tastepe, I. Coexistence of Obstructive Sleep Apnea and Superior Vena Cava Syndromes Due to Substernal Goitre in a Patient With Respiratory Failure: A Case Report. Iran. Red Crescent Med. J. 2015, 17, e18342. [Google Scholar] [CrossRef] [PubMed]
- Haddad, L.; Haddad, F.L.; Bittencourt, L.; Gregorio, L.C.; Tufik, S.; Abrahao, M. Clinical and polysomnographic findings of patients with large goiters: Polysomnographic findings of large goiters. Sleep Breath 2013, 17, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.; Furtado, R.; Ramani, A.; Mitta, N.; Kudchadkar, S.; Falari, S. A rare instance of retrosternal goitre presenting with obstructive sleep apnoea in a middle-aged person. Int. J. Surg. Case Rep. 2013, 4, 1064–1066. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Bourahla, K.; Petiau, C.; Velten, M.; Volkmar, P.P.; Rodier, J.F. Role of thyroid surgery in the obstructive sleep apnea syndrome. World J. Surg. 2014, 38, 1990–1994. [Google Scholar] [CrossRef] [PubMed]
- Haddad, L.; Martinho Haddad, F.L.; Bittencourt, L.; Gregorio, L.C.; Tufik, S.; Abrahao, M. Impact of thyroidectomy on the control of obstructive sleep apnea syndrome in patients with large goiters. Sleep Breath 2014, 18, 825–828. [Google Scholar] [CrossRef] [PubMed]
- Agrama, M.T. Thyroidectomy for goiter relieves obstructive sleep apnea: Results of 8 cases. Ear Nose Throat J. 2011, 90, 315–317. [Google Scholar] [CrossRef] [PubMed]
- De Felice, A.; Fuschillo, S.; Martucci, M.; De Angelis, E.; Balzano, G. Euthyroid goitre and sleep apnea. Monaldi Arch. Chest Dis. 2006, 65, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Charciunaite, K.; Gauronskaite, R.; Slekyte, G.; Danila, E.; Zablockis, R. Evaluation of Obstructive Sleep Apnea Phenotypes Treatment Effectiveness. Medicina 2021, 57, 335. [Google Scholar] [CrossRef]
- Fernandez-Sanjuan, P.; Alcaraz, M.; Bosco, G.; Perez-Martin, N.; Morato, M.; Lugo, R.; Arrieta, J.J.; Sanabria, J.; Rios-Lago, M.; Plaza, G. Modifications in Upper Airway Collapsibility during Sleep Endoscopy with a Mandibular Positioner: Study in Snorers and Obstructive Sleep Apnea Patients. J. Clin. Med. 2024, 13, 1184. [Google Scholar] [CrossRef]
- De Vito, A.; Olszewska, E.; Kotecha, B.; Thuler, E.; Casale, M.; Cammaroto, G.; Vicini, C.; Vanderveken, O.M. A Critical Analysis of Pharyngeal Patterns of Collapse in Obstructive Sleep Apnea: Beyond the Endoscopic Classification Systems. J. Clin. Med. 2023, 13, 165. [Google Scholar] [CrossRef]
- Carrasco-Llatas, M.; Matarredona-Quiles, S.; De Vito, A.; Chong, K.B.; Vicini, C. Drug-Induced Sleep Endoscopy: Technique, Indications, Tips and Pitfalls. Healthcare 2019, 7, 93. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Before Thyroidectomy | After Thyroidectomy |
|---|---|---|
| Evaluation period | 22 h 30–05 h 30 | 23 h 00–07 h 00 |
| AHI, e/h | 32 (severe OSA: AHI ≥ 30) | 3 |
| AI, e/h | 2 | 0 |
| HI, e/h | 30 | 3 |
| ODI, e/h | 31 | 4 |
| Mean SpO2, % | 95 | 95 |
| T90, % | 0.4 | 0 |
| SI, e/h | 65 | 35 |
| Right side, %ST | 25 | 42 |
| Left side, %ST | 67 | 55 |
| Supine, %ST | 4 | 2 |
| Prone, %ST | 0 | 0 |
| Standing, %ST | 4 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouahchi, Y.; Mejbri, M.; Mediouni, A.; Hedhli, A.; Ouahchi, I.; El Euch, M.; Toujani, S.; Dhahri, B. The Resolution of Obstructive Sleep Apnea in a Patient with Goiter after Total Thyroidectomy: A Case Report. Reports 2024, 7, 29. https://doi.org/10.3390/reports7020029
Ouahchi Y, Mejbri M, Mediouni A, Hedhli A, Ouahchi I, El Euch M, Toujani S, Dhahri B. The Resolution of Obstructive Sleep Apnea in a Patient with Goiter after Total Thyroidectomy: A Case Report. Reports. 2024; 7(2):29. https://doi.org/10.3390/reports7020029
Chicago/Turabian StyleOuahchi, Yacine, Maha Mejbri, Azza Mediouni, Abir Hedhli, Ines Ouahchi, Mounira El Euch, Sonia Toujani, and Besma Dhahri. 2024. "The Resolution of Obstructive Sleep Apnea in a Patient with Goiter after Total Thyroidectomy: A Case Report" Reports 7, no. 2: 29. https://doi.org/10.3390/reports7020029