1. Introduction
The application of mesenchymal stem/stromal cells (MSC) in regenerative medicine has been intensively studied in hundreds of clinical trials as these cells represent a promising source of multipotent adult stem and progenitor cells for cell therapy and tissue engineering [
1,
2]. However, excessive MSC heterogeneity hampers profound cell characterization [
3,
4,
5,
6,
7]. Several safety concerns related to MSC transplantation still remain because of the potential risk of immune reactions and cancer development [
8]. Furthermore, poor engraftment and insufficient viability of transplanted cells restrict their therapeutic efficacy [
9,
10,
11,
12].
Therapeutic effects of MSC are generally mediated by various secreted cytokines, growth factors, extracellular matrix proteins and factors involved in matrix remodeling as well as different types of extracellular vesicles [
13,
14,
15,
16,
17]. MSC-CM that contains cell-secreted products has demonstrated therapeutic benefit for the treatment of ischemic diseases such as myocardial infarction, stroke and acute and chronic hindlimb ischemia, neurodegenerative diseases, spinal cord injury, alopecia, acute and chronic wounds, acute liver injury/failure, lung injury, periodontal tissues injury, male infertility, soft tissue and bone defects [
18,
19,
20,
21,
22,
23]. There are several clinical trials including the use of MSC-CM for hair follicle regeneration [
24], fractional carbon dioxide resurfacing wound healing [
25] as well as for inflammatory arthritis [
26], and multiple sclerosis [
27]. MSC-secreted extracellular vesicles that carry regulatory noncoding RNAs were also used as therapeutic agents to stimulate tissue regeneration [
28,
29,
30,
31,
32]. Thus, MSC secretome is suggested as a novel cell-free medicinal product that can recapitulate the beneficial effects of MSC and has various advantages in overcoming the limitations and risks associated with cell-based therapy [
33,
34].
However, significant variability of approaches to MSC-CM bioprocessing has a serious impact on experimental outcomes [
34,
35]. Particularly, the need for disease-specific identity and potency testing due to undefined mechanisms of action of MSC secretome makes development of this class of biopharmaceuticals more complicated, expensive and precarious [
1,
34,
36]. Additionally, the composition of MSC-CM is significantly influenced by donor variability and tissue of MSC origin [
37,
38] and it should be considered during MSC-CM bioprocessing. In this study, we analyzed how several manufacturing features such as duration of cell conditioning or selection of particular growth medium might influence the composition of human adipose-derived MSC-CM as well as its biological activity in several potency assays routinely used for the development of cell-based therapy products. We then performed regression analysis to estimate power to predict biological activity of MSC-CM samples despite high donor variability and complex composition of MSC-CM.
3. Discussion
According to the current concepts, MSC could orchestrate tissue development, maintenance and repair, mostly by producing multiple secretory factors [
45,
46,
47,
48,
49,
50,
51]. Therefore, the application of MSC-CM might be an effective strategy for regenerative medicine. To date, several MSC-derived conditioned media were tested on various diseases and many of them showed positive results [
22]. An additional benefit is that MSC-CM might be an off-the-shelf material that could be used to treat patients promptly without MSC isolation and subsequent culture. However, despite the clear benefits of using MSC-CM for regenerative medicine, several issues must be addressed before its successful clinical application. Among them, one of the most important is a lack of common recommendations or standards for bioprocessing and quality control of MSC secretome-based therapeutics [
52]. In this study, we suggested universal approaches that might help to overcome these issues and, finally, optimize the development of MSC-CM based products in general.
To develop the MSC-CM bioprocessing protocol we selected two growth media for MSC conditioning: DMEM due to its wide application in the manufacturing of MSC-based cell products, including the clinical trials [
53] and NutriStem as one of the specific media with great potential to support growth and functional properties of undifferentiated human MSC. Both media were chemically defined, available as GMP-grade media and appropriate for cell manufacturing. It is critical to note that we used only basic media for MSC conditioning without adding the specific nutrimental supplements, because of their high risk influence on the biosafety of a final product and serious challenges for further clinical translation [
54]. We showed that both media supported appropriate viability of MSC during the long-term conditioning in supplement-free conditions.
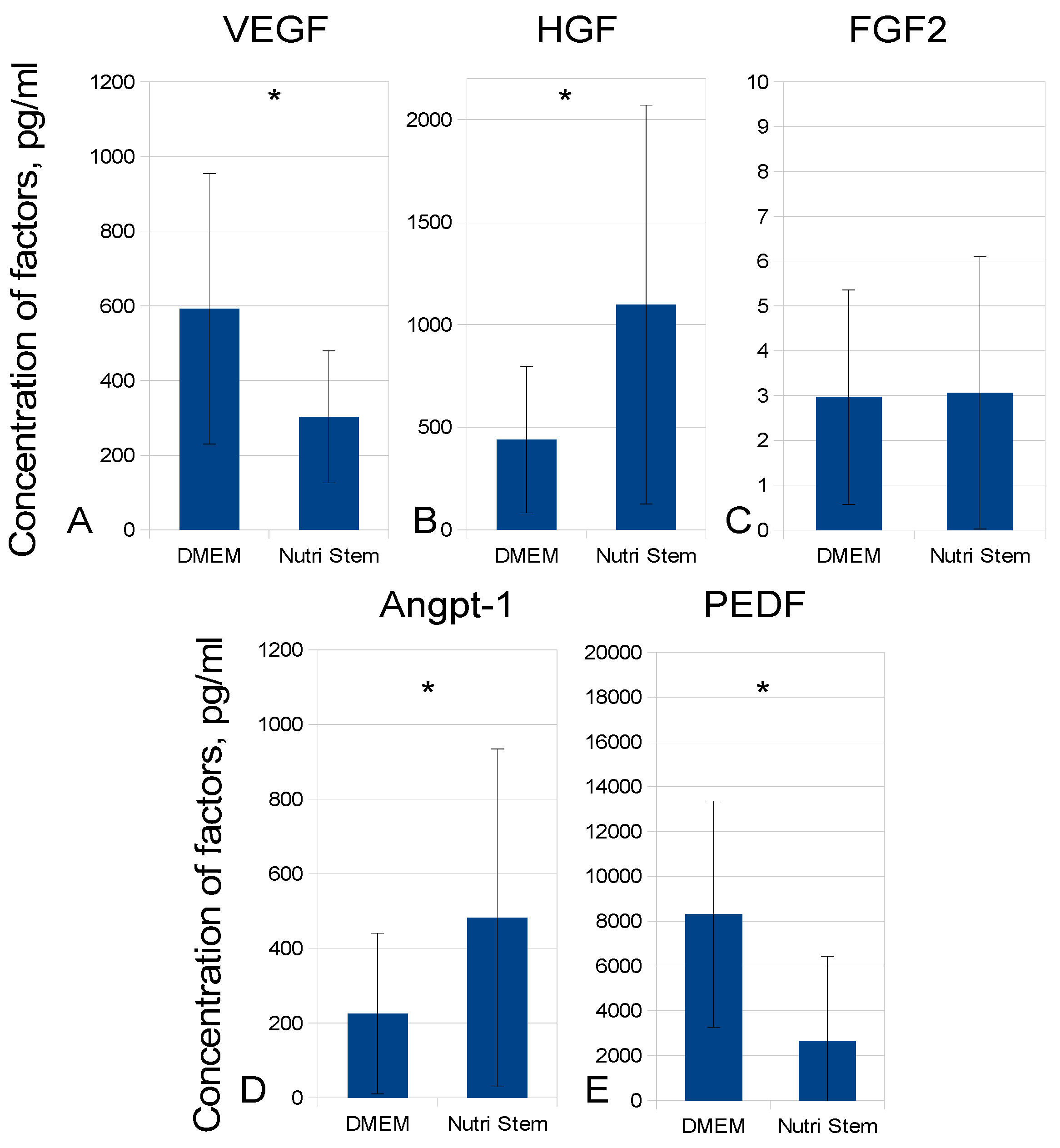
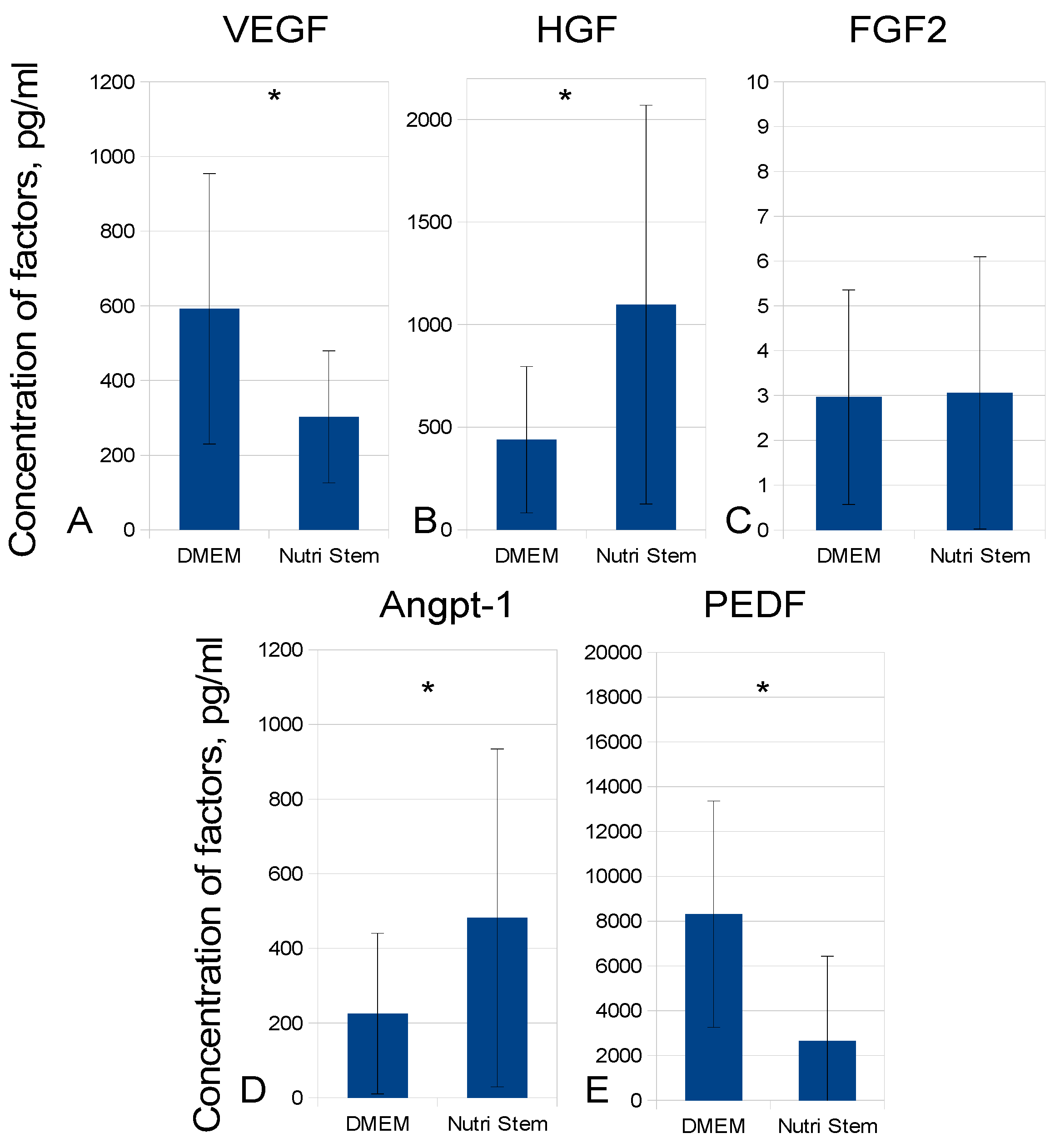
Due to complex composition of MSC-CM, it was necessary to focus on components that would reflect its regenerative potency for a specific condition. In our study, we selected several factors crucial for MSC secretome-mediated tissue regeneration, which was also confirmed by our previous data [
42,
43,
44]. VEGF, an important pro-angiogenic and neurotrophic factor [
43], is produced by MSC and served as one of the main mediators in MSC interaction with endothelial cells. Particularly, VEGF expression by MSC was associated with the stimulation of angiogenesis and endothelial cell proliferation in both small and large animal studies [
55], and blocking of VEGF in MSC-CM resulted in significant reduction in its ability to stimulate angiogenesis [
42,
44]. On the contrary, PEDF, another factor highly represented in MSC secretome [
56], has anti-angiogenic effects; the ratio of VEGF/PEDF produced by MSC may indicate the ability of the cells to stimulate angiogenesis [
57]. MSC also secretes HGF, a factor with angiogenic, anti-apoptotic and immune modulating activity shown to be critical in several in vitro and in vivo therapeutic effects of MSC [
43,
58]. FGF2, a strong mitogenic and pro-migratory factor for fibroblasts, has the potential to promote angiogenesis and to increase survival and proliferation of stem cells in vivo [
59,
60].
Obviously, the panel of factors evaluated in MSC-CM may vary depending on potential therapeutic mechanisms for a specific disease. Particularly, in several injury models, either a complex of growth factors from MSC-CM as well as other bioactive components of MSC secretome (i.e., extracellular vesicles) might confer the principal potency for restoration [
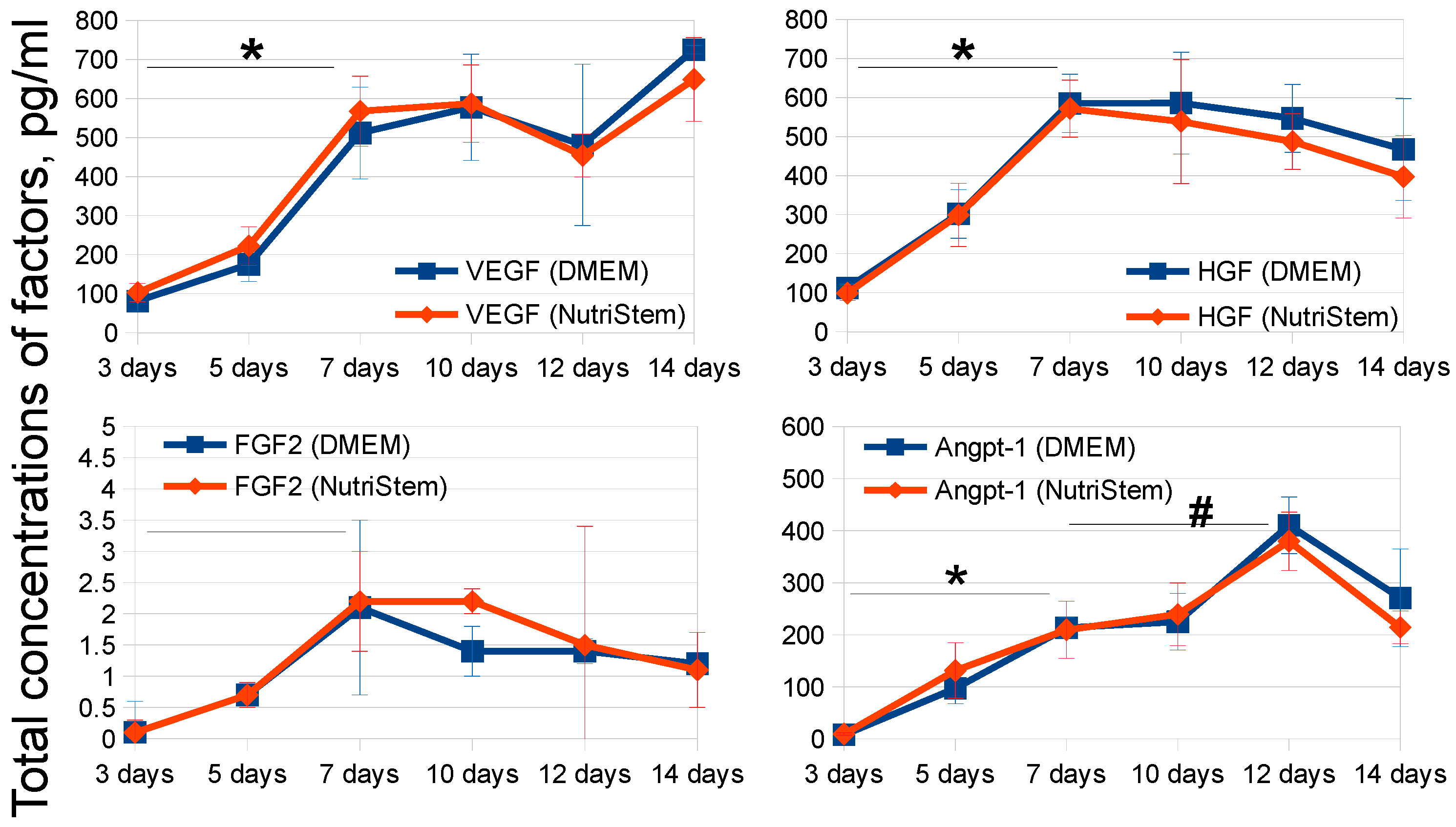
61]. The components of MSC-CM also might differ by their accumulation dynamics in cell growth medium, so we considered the peak concentrations of several factors to improve the performance of the bioprocessing protocol. Importantly, it was demonstrated that the type of a cell growth medium affected secretory potential of MSC, which was in accordance with literature data [
62,
63].
To optimize specific biological activity testing of MSC-CM, we suggested to perform regression analysis. Based on initial results of the testing on biological models, this approach can help to select MSC-CM factors, which concentrations are closely associated with the specific biological activity of MSC-CM. This might make possible to predict specific activity using precise instrumental analysis, thus bypassing expensive and laborious biological assays. Accordingly, the estimation of the concentrations of irrelevant MSC-CM factors might be omitted.
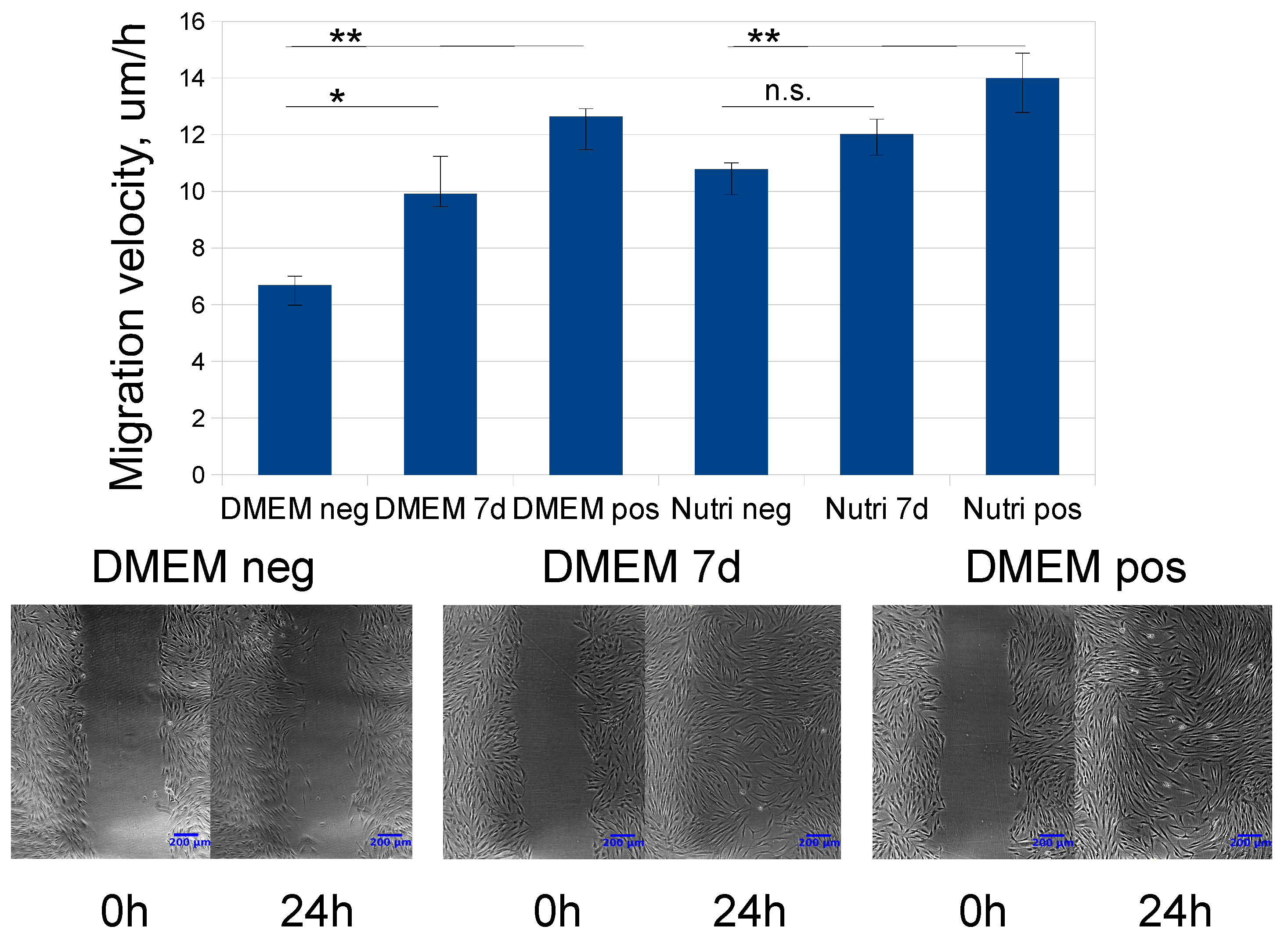
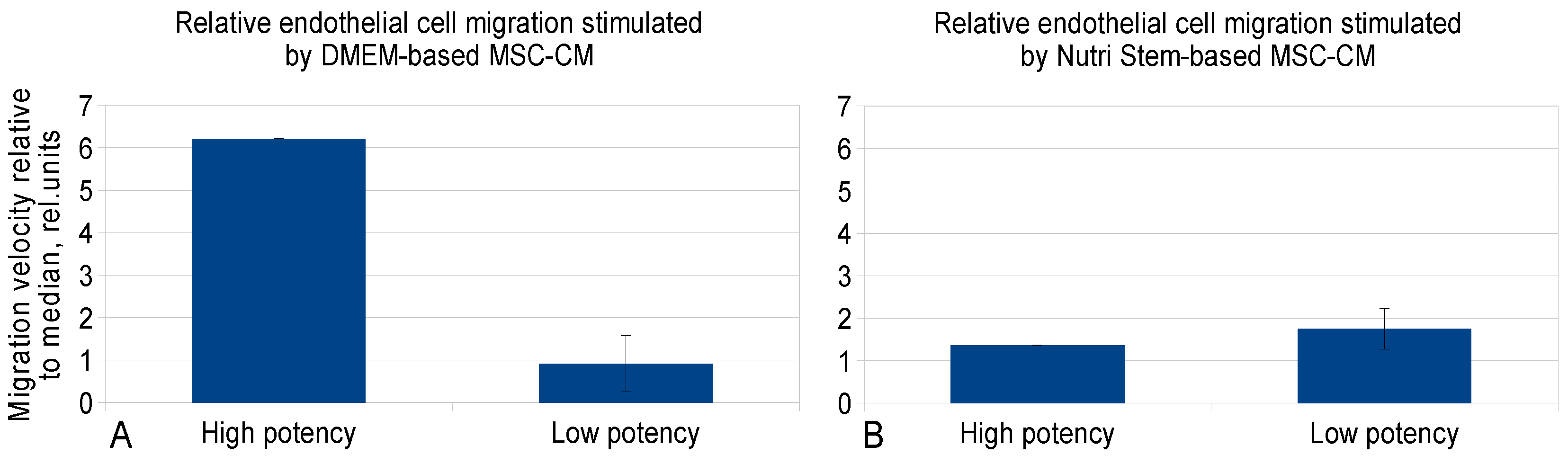
In this study, we demonstrated that FGF2 concentration in MSC-CM was associated with DMEM-based CM-stimulated endothelial cell migration velocity. Importantly, these results were concordant with the mechanisms of action of this factor [
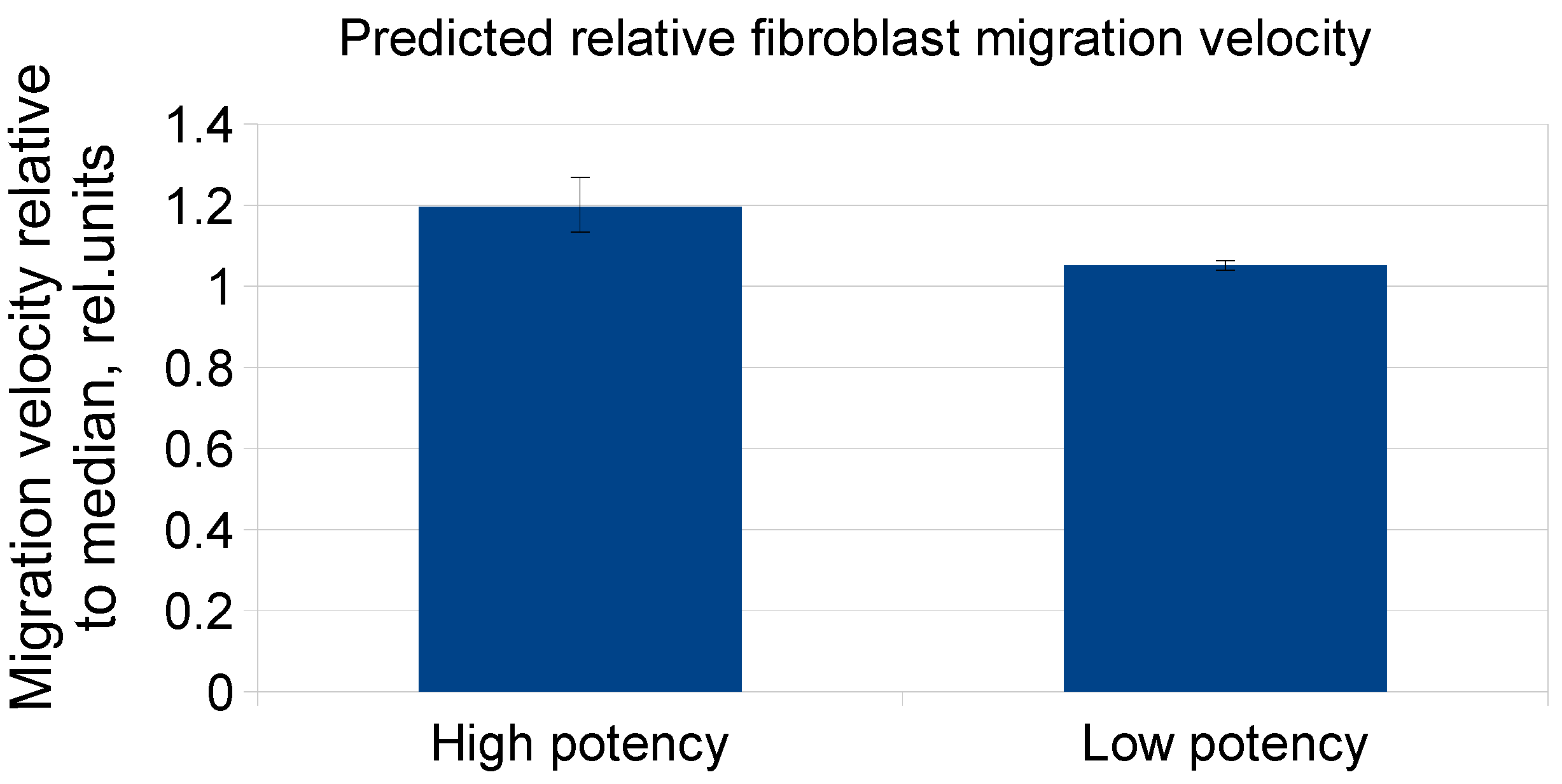
60]. However, the similar results were not obtained for NutriStem-based MSC-CM samples possibly due to direct substantial influence of the basal medium on the potency. Unexpectedly, it was also demonstrated that Angpt-1 concentration in MSC-CM was inversely associated with CM-stimulated fibroblast migration velocity independently of the type of cell culture medium. Indeed, it did not fit with the well-established superior pro-migratory potential of FGF2 [
59]. Nevertheless, these results might be interpreted as evidence that Angpt-1 concentrations predicted activity to stimulate fibroblast migration for the set composed of DMEM and NutriStem MSC-CM samples, even despite lack of established biological associations. Use of such an approach allows to make MSC-CM bioprocessing protocols more flexible in relation to the choice of raw materials.
Noteworthy, regression analysis used in this study has several limitations. It is impossible to consider all the interactions of soluble factors in MSC-CM. Furthermore, the analyzed components of MSC-CM could have synergistic or antagonist effects on each other which might distort their real impact on biological activity of MSC-CM, but couldn’t be revealed by mathematical modeling. Nevertheless, use of the regression analysis might be rational. We interpreted the release of factors as endpoints that might vary due to donor-associated heterogeneity or influence of other MSC-CM components. The obtained results would reflect associations of factor concentrations with specific biological activity of a sample considering its variability but possibly irrelevant to its biological function.
Taken together, our results have demonstrated the applicability of the approaches to MSC-CM bioprocessing and quality control optimization. Despite hurdles associated with the development of MSC secretome-based products, we tried to circumvent the high variability between donors and indicate a practical way to the choice of relevant quality control criteria. We suggest that these approaches might be adapted for other cell types and their secretomes promising for application in regenerative medicine.
4. Materials and Methods
4.1. Patients
Thirty patients were included in the study. They underwent surgery because of general surgical pathology, kidney and bladder revision. Exclusion criteria included any patient aged less than 18 years and more than 70 years, autoimmune pathologies, cancer (even in the past history), acute or chronic inflammatory disease, type 2 diabetes mellitus, acute myocardial infarction in the previous six months, long-term hormone or antibiotics therapy, hematological disorders, stroke or craniocerebral injury in the previous 12 months, polyvalent allergy and pregnancy. The clinical features of the patient cohort are presented in
Table S1. All procedures performed with tissue samples from patients were in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Lomonosov Moscow State University (IRB00010587), protocol #4 (2018). Each donor participated in the study, signed an informed written consent form for harvesting and using adipose tissue samples as well as for handling clinical data for research purposes.
4.2. Isolation of Adipose-Derived MSC
Subcutaneous adipose tissue samples (0.5–5 mL) harvested during surgery were homogenized and digested in collagenase I (200 U/mL, Worthington Biochemical) and dispase (40 U/mL, Sigma, St. Louis, MO, USA) solutions under agitation for 30–40 min at 37 °C. Then tissue was centrifuged at 200 g for 10 min; supernatant was discarded. Erythrocytes were removed from the MSC pellet by a brief hypoosmotic shock. Then, cell suspension was filtered through a sieve (BD Falcon Cell Strainer, 100 um, Franklin Lakes, NJ, USA) and centrifuged at 200 g for 10 min. The final pellet was resuspended in culture medium. The cells were cultured in standard conditions (5% CO2; 37 °C) in Advance Stem Cell Basal Medium (ASCBM, HyClone, Marlborough, MA, USA) with 10% of Advance Stem Cell Growth Supplement (HyClone), and 100 U/mL penicillin/streptomycin (HyClone). Unattached cells were washed off 24 h after isolation, and then, medium was changed every 3 to 4 days. The yield of cells was 4–7 × 104 of attached cells per ml of tissue. Cells were passaged at 70% confluency using HyQTase solution (HyClone).
4.3. Collection of MSC conditioned medium
MSC at 4–5th passages were seeded with a density of 3 × 103 cells/cm2 on uncoated culture plastic (Corning) and were cultured to 70–80% confluence in 100 mm culture dishes. Then MSC were washed thoroughly 3 times using 10 mL of HBSS without Ca2+ and Mg2+, and replenished with MSC NutriStem XF Basal Medium (Nutristem, Biological Industries, Beit-Haemek, Israel) or DMEM with low glucose (DMEM-LG, HyClone). Cells were cultured in standard conditions (5% CO2; 37 °C) for different time periods. Then, conditioned media samples were collected, centrifuged at 3000 rpm for 10 min at 4 °C to remove cell debris, then frozen in aliquots at −70 °C. 36 MSC-CM samples were manufactured (n = 21 for DMEM-LG, n = 15 for NutriStem).
4.4. Analysis of Cell Viability
The quantity and viability of MSC were assessed at the end of the experiment by staining with trypan blue solution. Cell viability was interpreted as the ability of viable cells to eject the trypan blue stain. The amount of viable (bright) and dead (blue) cells was evaluated using the automated cell counter Countess (Invitrogen, Carlsbad, CA, USA). Cell viability was determined as a ratio of viable cells to the total cell amount. To estimate cell viability during long-term conditioning, the cells were grown in separate dishes and were analyzed in certain time points independently.
4.5. MSCs Immunophenotyping and Differentiation Assays
To confirm that MSC were multipotent mesenchymal stromal cells we analyzed their immunophenotype according to the published criteria [
39]. Cells were stained with anti- CD73, CD90, CD105, CD14, CD20, CD34, CD45 antibodies and appropriate isotype control antibodies (MSC Phenotyping Kit, Miltenyi Biotec, Bergisch Gladbach, Germany) and analyzed using flow cytometry.
The potential of MSC for osteogenic and adipogenic differentiation was tested using standard techniques in vitro. Briefly, osteogenic differentiation was induced by plating 6 × 104 MSC on a 24-well plate and incubated in an Advance Stem Cell Osteogenic Medium (HyClone) containing 10% Advance Stem Cell Supplement and 100 U/mL penicillin/streptomycin for 21 days. Differentiation efficiency was analyzed using Alizarin Red S staining for calcium accumulation. Adipogenic differentiation was induced by the incubation of MSC in Advance Stem Cell Adipogenic Medium (HyClone) containing 10% Advance Stem Cell Supplement and 100 U/mL penicillin/streptomycin for 18 days. Cells accumulated intracellular lipids were analyzed using Oil-Red-O staining.
4.6. Analysis of Concentrations of Growth Factors in MSC-Conditioned Medium by ELISA
The concentrations of VEGF, HGF, FGF2, Angpt-1 and PEDF in MSC-CM samples were analyzed using ELISA (R&D Systems) according to the manufacturer’s instructions. Factor concentrations were determined in conditioned medium collected from independent cell culture plates. The cells isolated were seeded on cell culture dishes. Then, the medium was collected, centrifuged and frozen. The total release of factors was calculated based on the analysis of secretome samples at every time point.
4.7. Migration of Fibroblasts in the Scratch Assay
Scratch assay is a specific test with an artificial wound scrapped mechanically in a confluent cell monolayer. Fibroblasts activated by an empty plastic area move from the edge to the center of the wound up to wound closure. Several factors like FBS or other factors, contained in MSC-CM, might have an influence on cell motility. Human skin fibroblasts were grown to confluent in 24-well plates in DMEM-LG containing 10% of the FBS. Then, fibroblasts were deprived in DMEM with 0% FBS for 24 h. Cell monolayers were scratched with a 1 mL pipette tip and briefly rinsed. Then, the sample of MSC-CM or DMEM-LG supplemented with 10% FBS as a positive control or serum-free DMEM-LG as a negative control were added. Following this, culture plates were transferred onto the microscopic stage of a motorized Nikon Ti inverted microscope (Nikon, Japan) equipped with the 5x objective, on-stage culture box, temperature controller set to 37 °C and continuous carbogen administration unit. The time-lapse series was continuously acquired every 15 min over 24 h using a cooled CCD camera (Nikon, Tokyo, Japan) and the “Mark and Find” application in NIS Elements (Nikon, Japan) to achieve simultaneous image acquisition in all 24 wells of the plate. This frequency ensured that in each series two successive displacements of a cell were resolved and all cell divisions were captured to be excluded from the analysis later on. The time series were analyzed by manual tracking of all cells on the edge of the experimental wounds and their velocity was measured in two randomly chosen positions of the wounded areas using free ImageJ software, Madison, WI, USA. Routinely, 50 cells were tracked for each data point.
4.8. Endothelial Cell Migration Analysis in the xCELLigence RTCA DP System
To analyze endothelial cell migration using the CIM-Plate 16, human endothelial cells EA.hy926 were cultured in DMEM with high glucose supplemented with 10% FBS; cells were deprived in serum-free DMEM for 6 to 8 h prior to the experiment and seeded 30 × 104 cells in 50 uL of serum-free DMEM per well into the upper chambers of the CIM-Plate 16. Samples of MSC-CM (160 uL per well) were placed into the lower chambers. DMEM supplemented with 10% FBS was used as a positive control and serum-free DMEM served as a negative control. Then CIM-Plate 16 was placed in the RTCA DP Instrument (Roche, Basel, Switzerland) equilibrated in a CO2 incubator. Endothelial cell migration was continuously monitored using the RTCA DP Instrument. MSC-CM provided a strong chemoattractant signal, which induced the directional migration of endothelial cells through the micropores of the CIM-Plate 16. Migrating cells were detected by the electronic sensing microelectrodes, producing changes in the measured Cell Index values. Time-dependent cell migration was monitored over 4 h. All experiments were performed in duplicates. The RTCA Software 1.2 was used to calculate Cell Index values for MSC-CM-mediated endothelial cell migration.
4.9. Regression Analysis
The samples were randomized to training and validation groups prior to analysis (2:1 for fibroblast migration and initial endothelial cell migration, 1.5:1 for cell growth medium-specific endothelial cell migration). Growth factor concentrations in MSC-CM samples were standardized prior to regression model building. We used the Python StatsModels library and the Logit model, to perform regression analysis. For fibroblast scratch assay we categorized our data into two groups according to their specific activity: The first group consisted of samples with below median activity (n = 18), the second group included samples with equal to or above median activity (n = 18). For endothelial cell migration we split our data into two groups similarly: The first group consisted of 20 samples, the second included 11 more potent samples. We selected factor concentrations as well as the type of cell culture medium as independent variables.
4.10. Statistical Analysis
Statistical analysis was performed using RStudio. The normality was tested using the Shapiro–Wilk test. Normally distributed data were compared using a Student’s t-test; data that were not normally distributed were compared using the Mann–Whitney U-test or the Kruskal–Wallis test. Multiple comparisons were made using the Kruskall–Wallis test with subsequent application of Dunn criteria. Correlations were calculated using the Hmisc R package. Statistical significance was defined as p-value <0.05.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}