
Borrowing the Features of Biopolymers for Emerging Wound Healing Dressings: A Review

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
- -
- Function in the wound: debridement, antibacterial, occlusive, absorbent, adherence;
- -
- Type of material: hydrocolloid, alginate, collagen;
- -
- Physical form: ointment, film/membranes, foam, gel, spray, composite, particulate systems;
- -
- Type of physical contact with the wound: primary, secondary or island dressings;
- -
- Traditional biomaterial based-dressings or artificial dressings;
- -
- Mechanism of action: passive (protects the wound area with no direct effect on the wound) or interactive (produces an optimum environment at the wound dressing interface).
- -
- Suitable design, with minimal inconvenience to the patient (easy to apply, maintain and store; adaptable to the wound shape; proper elasticity; and high mechanical strength);
- -
- Removes and absorb excessive exudate drainage from the wound;
- -
- Easily sterilized;
- -
- Cost-permissive;
- -
- Induces rapid healing;
- -
- Preserves the body water content and temperature of approximately 37 °C;
- -
- Gas-permeable;
- -
- Ability to release bioactive ingredients when connecting with the wound surface;
- -
- Non-adherent and non-allergenic, biocompatible;
- -
- Easy removal at the end of treatment and/or biodegradable;
- -
- Provides barrier to external contaminants;
- -
- Stimulates growth factors and production of granulation tissue and re-epithelialization;
- -
- Minimizes trauma or maceration to wound edges.
2. Overview of Current Status
3. Methods
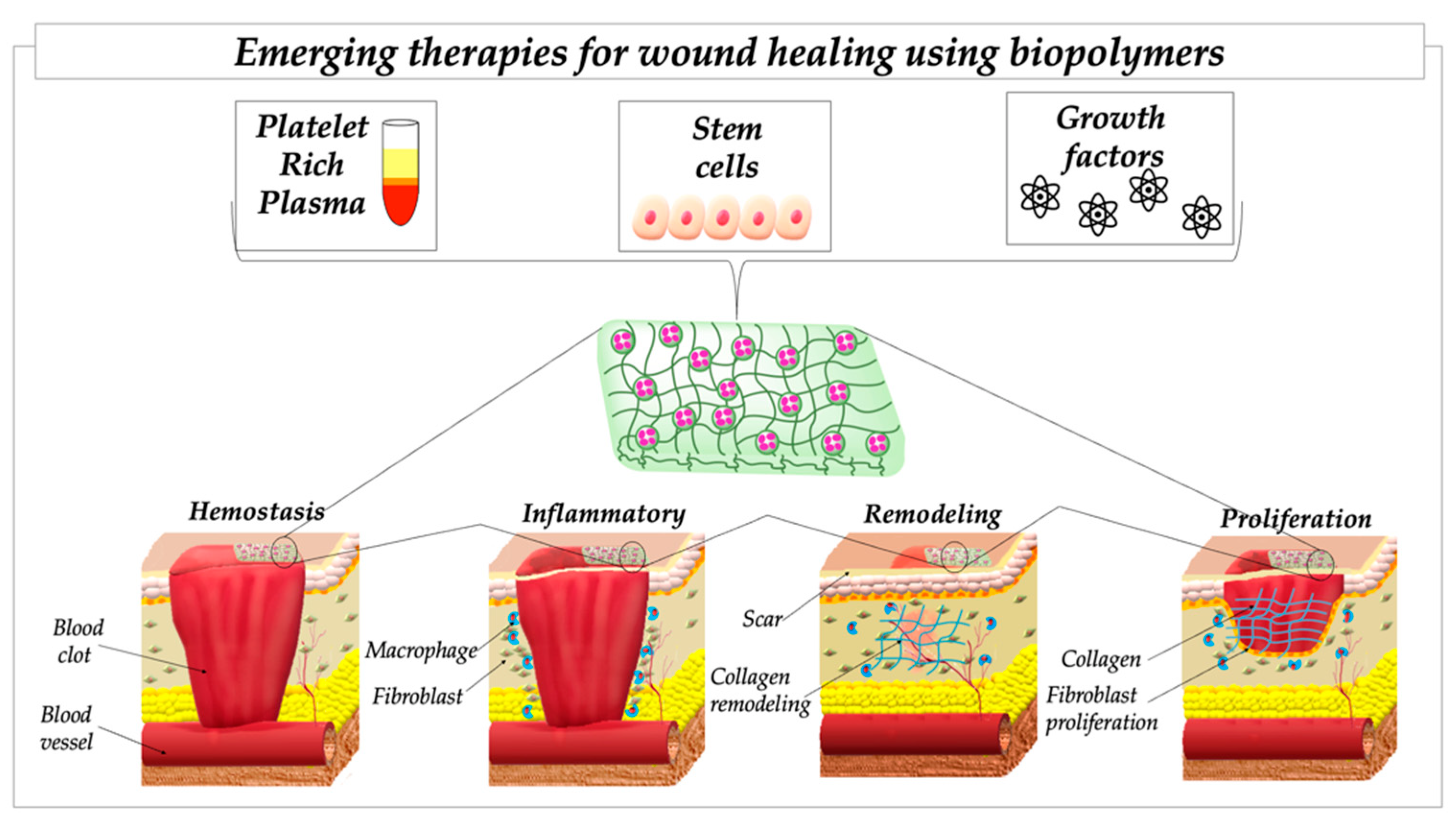
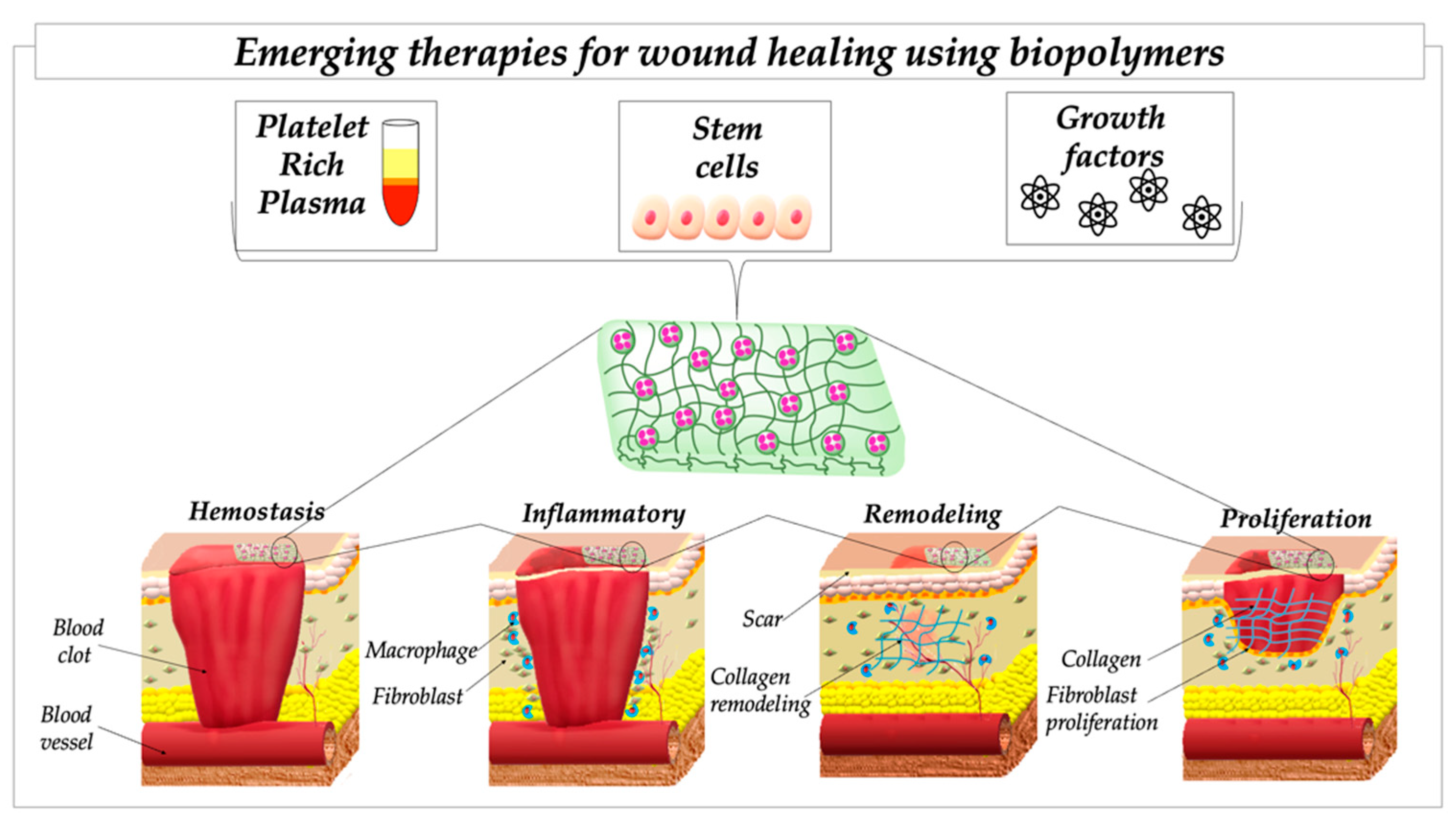
4. Wound-Healing Cascade
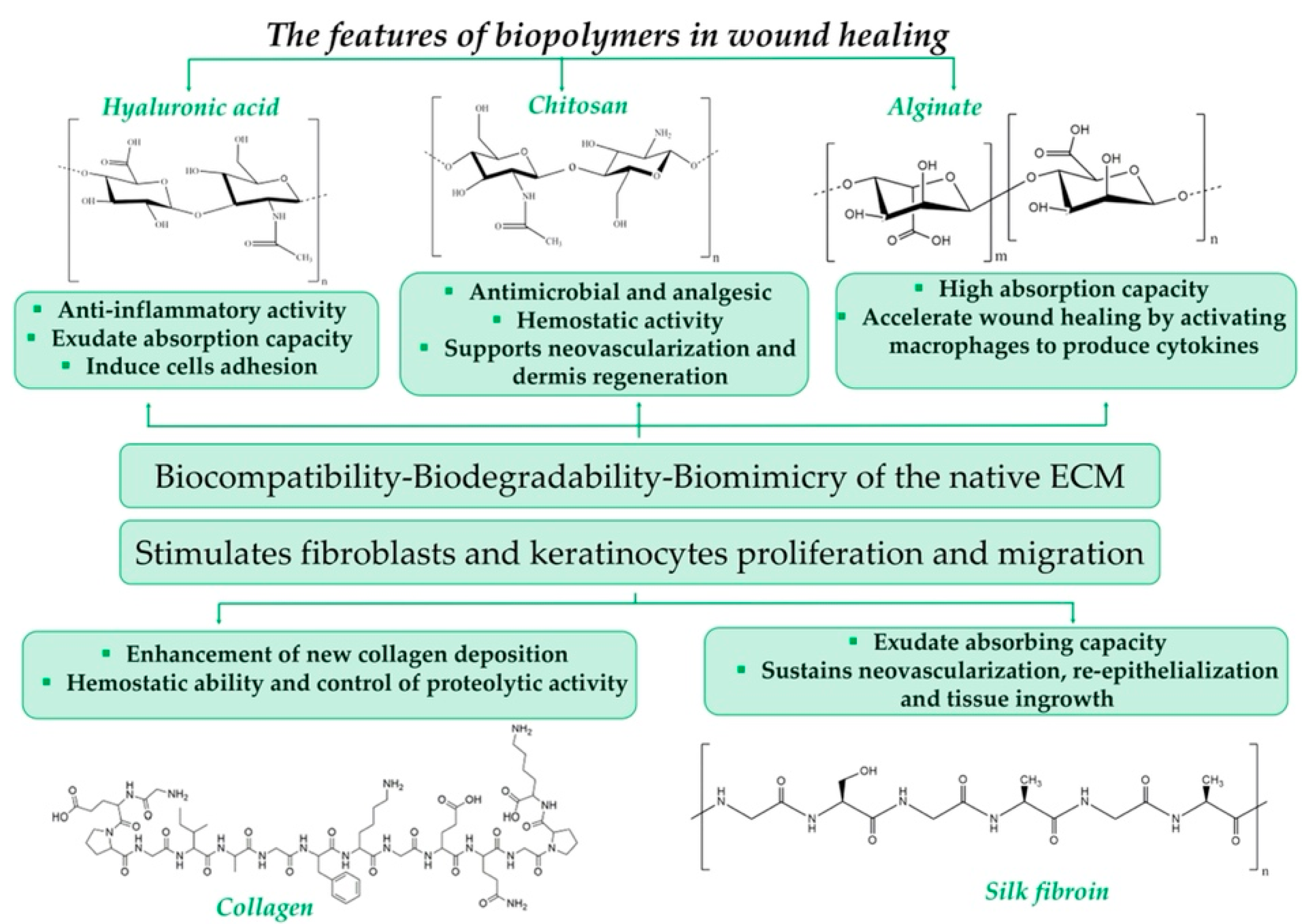
5. Biopolymers as Tuneable Materials
5.1. Chitosan (Cs)
- -
- in haemostasis—by stimulating the aggregation of platelets and erythrocytes and restraining the dissolution of fibrin;
- -
- in inflammation—through its well-known and validated antibacterial properties;
- -
- in proliferation—by promoting the growth of macrophages, fibroblasts and capillaries.
5.2. Hyaluronic Acid (HA)
5.3. Alginate (ALG)
5.4. Silk Fibroin (SF)
5.5. Collagen (Col)
5.6. Combination of Biopolymers
6. Emerging Therapies Using Biopolymers
6.1. Blood Products: Platelet-Rich Plasma
6.2. Therapies Based on Stem Cells
6.3. Growth Factors
7. Conclusions and Future Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Herman, T.F.; Bordoni, B. Wound Classification, 2020th ed.; StatePearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Best Practice Guidelines in Disaster Situation; WHO/EHT/CPR: Geneva, Switzerland, 2005.
- Van Gennip, L.; Haverkamp, F.J.C.; Muhrbeck, M.; Wladis, A.; Tan, E.C.T.H. Using the Red Cross Wound Classification to Predict Treatment Needs in Children with Conflict-Related Limb Injuries: A Retrospective Database Study. World J. Emerg. Surg. 2020, 15, 52. [Google Scholar] [CrossRef] [PubMed]
- Patrulea, V.; Ostafe, V.; Borchard, G.; Jordan, O. Chitosan as a Starting Material for Wound Healing Applications. Eur. J. Pharm. Biopharm. 2015, 97, 417–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boateng, J.S.; Matthews, K.H.; Stevens, H.N.E.; Eccleston, G.M. Wound Healing Dressings and Drug Delivery Systems: A Review. J. Pharm. Sci. 2008, 97, 2892–2923. [Google Scholar] [CrossRef] [PubMed]
- Broussard, K.C.; Powers, J.G. Wound Dressings: Selecting the Most Appropriate Type. Am. J. Clin. Dermatol. 2013, 14, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Adis Medical Writers. Select Appropriate Wound Dressings by Matching the Properties of the Dressing to the Type of Wound. Drugs Ther. Perspect. 2014, 30, 213–217. [Google Scholar] [CrossRef]
- Shi, C.; Wang, C.; Liu, H.; Li, Q.; Li, R.; Zhang, Y.; Liu, Y.; Shao, Y.; Wang, J. Selection of Appropriate Wound Dressing for Various Wounds. Front. Bioeng. Biotechnol. 2020, 8, 182. [Google Scholar] [CrossRef] [Green Version]
- Van Rijswijk, L. Ingredient-Based Wound Dressing Classification: A Paradigm That Is Passe and in Need of Replacement. J. Wound Care 2006, 15, 11–14. [Google Scholar] [CrossRef]
- Solowiej, K.; Mason, V.; Upton, D. Psychological Stress and Pain in Wound Care, Part 3: Management. J. Wound Care 2010, 19, 153–155. [Google Scholar] [CrossRef]
- Landriscina, A.; Rosen, J.; Friedman, A.J. Systematic Approach to Wound Dressings. J. Drugs Dermatol. 2015, 14, 740–744. [Google Scholar]
- Lindholm, C.; Searle, R. Wound Management for the 21st Century: Combining Effectiveness and Efficiency: Wound Management for the 21st Century. Int. Wound J. 2016, 13, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Ghomi, E.R.; Khalili, S.; Khorasani, S.N.; Neisiany, R.E.; Ramakrishna, S. Wound Dressings: Current Advances and Future Directions. J. Appl. Polym. Sci. 2019, 136, 47738. [Google Scholar] [CrossRef] [Green Version]
- Tottoli, E.M.; Dorati, R.; Genta, I.; Chiesa, E.; Pisani, S.; Conti, B. Skin Wound Healing Process and New Emerging Technologies for Skin Wound Care and Regeneration. Pharmaceutics 2020, 12, 735. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, B.; Simmons, J.K.; Stuart, B.; Tung, R.; Zamierowski, D.S.; Mellott, A.J. Enhancing Wound Healing Dressing Development through Interdisciplinary Collaboration. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 1967–1985. [Google Scholar] [CrossRef] [PubMed]
- Mirhaj, M.; Labbaf, S.; Tavakoli, M.; Seifalian, A.M. Emerging Treatment Strategies in Wound Care. Int. Wound J. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Minsart, M.; Van Vlierberghe, S.; Dubruel, P.; Mignon, A. Commercial Wound Dressings for the Treatment of Exuding Wounds: An in-Depth Physico-Chemical Comparative Study. Burn. Trauma 2022, 10, tkac024. [Google Scholar] [CrossRef] [PubMed]
- Baranoski, S. Choosing a Wound Dressing, Part 1. Nursing 2008, 38, 60–61. [Google Scholar] [CrossRef]
- Liu, J.-Y.; Li, Y.; Hu, Y.; Cheng, G.; Ye, E.; Shen, C. Hemostatic Porous Sponges of Cross-Linked Hyaluronic Acid/Cationized Dextran by One Self-Foaming Process. Mater. Sci. Eng. C 2018, 83, 160–168. [Google Scholar] [CrossRef]
- Aderibigbe, B.; Buyana, B. Alginate in Wound Dressings. Pharmaceutics 2018, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Etulain, J. Platelets in Wound Healing and Regenerative Medicine. Platelets 2018, 29, 556–568. [Google Scholar] [CrossRef]
- Popescu, M.N.; Iliescu, M.G.; Beiu, C.; Popa, L.G.; Mihai, M.M.; Berteanu, M.; Ionescu, A.M. Autologous Platelet-Rich Plasma Efficacy in the Field of Regenerative Medicine: Product and Quality Control. BioMed Res. Int. 2021, 2021, 4672959. [Google Scholar] [CrossRef]
- Park, J.; Hwang, S.; Yoon, I.-S. Advanced Growth Factor Delivery Systems in Wound Management and Skin Regeneration. Molecules 2017, 22, 1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandan, K.S.; Sashwati, R.; Gordillo, G. Wound healing, Chapter 13. In Plastic Surgery; Elsevier: Amsterdam, The Netherlands, 2017; Volume 1, ISBN 978-0-323-35694-7. [Google Scholar]
- Mir, M.; Ali, M.N.; Barakullah, A.; Gulzar, A.; Arshad, M.; Fatima, S.; Asad, M. Synthetic Polymeric Biomaterials for Wound Healing: A Review. Prog. Biomater. 2018, 7, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, J.R.; Giacopelli, J.A. A Review of Wound Healing and Wound Dressing Products. J. Foot Ankle Surg. 1997, 36, 2–14. [Google Scholar] [CrossRef]
- Strodtbeck, F. Physiology of Wound Healing. Newborn Infant Nurs. Rev. 2001, 1, 43–52. [Google Scholar] [CrossRef]
- Mast, B.A. The Skin. In Wound Healing: Biochemical and Clinical Aspects; W.B. Saunders Co.: Philadelphia, PA, USA, 1999; ISBN 978-0-7216-2564-5. [Google Scholar]
- Delavary, B.M.; van der Veer, W.M.; van Egmond, M.; Niessen, F.B.; Beelen, R.H.J. Macrophages in Skin Injury and Repair. Immunobiology 2011, 216, 753–762. [Google Scholar] [CrossRef]
- Reinke, J.M.; Sorg, H. Wound Repair and Regeneration. Eur. Surg. Res. 2012, 49, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.; Kämpfer, H.; Wetzler, C.; Stallmeyer, B.; Pfeilschifter, J. Large Induction of the Chemotactic Cytokine RANTES during Cutaneous Wound Repair: A Regulatory Role for Nitric Oxide in Keratinocyte-Derived RANTES Expression. Biochem. J. 2000, 347 Pt 1, 265–273. [Google Scholar] [CrossRef]
- Wilgus, T.A.; Roy, S.; McDaniel, J.C. Neutrophils and Wound Repair: Positive Actions and Negative Reactions. Adv. Wound Care 2013, 2, 379–388. [Google Scholar] [CrossRef] [Green Version]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil Extracellular Traps Kill Bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef]
- Eming, S.A.; Krieg, T.; Davidson, J.M. Inflammation in Wound Repair: Molecular and Cellular Mechanisms. J. Investig. Dermatol. 2007, 127, 514–525. [Google Scholar] [CrossRef] [Green Version]
- Werner, S.; Krieg, T.; Smola, H. Keratinocyte–Fibroblast Interactions in Wound Healing. J. Investig. Dermatol. 2007, 127, 998–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sottile, J. Regulation of Angiogenesis by Extracellular Matrix. Biochim. Biophys. Acta BBA Rev. Cancer 2004, 1654, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Kleinman, H.K.; Martin, G.R.; Lawley, T.J. Role of Laminin and Basement Membrane in the Morphological Differentiation of Human Endothelial Cells into Capillary-like Structures. J. Cell Biol. 1988, 107, 1589–1598. [Google Scholar] [CrossRef]
- Carmeliet, P. Angiogenesis in Life, Disease and Medicine. Nature 2005, 438, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Paquet-Fifield, S.; Schlüter, H.; Li, A.; Aitken, T.; Gangatirkar, P.; Blashki, D.; Koelmeyer, R.; Pouliot, N.; Palatsides, M.; Ellis, S.; et al. A Role for Pericytes as Microenvironmental Regulators of Human Skin Tissue Regeneration. J. Clin. Investig. 2009, 119, 2795–2806. [Google Scholar] [CrossRef] [Green Version]
- Takehara, K. Growth Regulation of Skin Fibroblasts. J. Dermatol. Sci. 2000, 24, S70–S77. [Google Scholar] [CrossRef]
- Pilcher, B.K.; Dumin, J.A.; Sudbeck, B.D.; Krane, S.M.; Welgus, H.G.; Parks, W.C. The Activity of Collagenase-1 Is Required for Keratinocyte Migration on a Type I Collagen Matrix. J. Cell Biol. 1997, 137, 1445–1457. [Google Scholar] [CrossRef]
- Patil, P.P.; Reagan, M.R.; Bohara, R.A. Silk Fibroin and Silk-Based Biomaterial Derivatives for Ideal Wound Dressings. Int. J. Biol. Macromol. 2020, 164, 4613–4627. [Google Scholar] [CrossRef]
- Mogoşanu, G.D.; Grumezescu, A.M. Natural and Synthetic Polymers for Wounds and Burns Dressing. Int. J. Pharm. 2014, 463, 127–136. [Google Scholar] [CrossRef]
- Suarato, G.; Bertorelli, R.; Athanassiou, A. Borrowing from Nature: Biopolymers and Biocomposites as Smart Wound Care Materials. Front. Bioeng. Biotechnol. 2018, 6, 137. [Google Scholar] [CrossRef] [Green Version]
- Clinical Trials, Key Words: Wound Healing, Dressing. Available online: https://clinicaltrials.gov (accessed on 28 December 2021).
- Yang, Y.; Xu, L.; Wang, J.; Meng, Q.; Zhong, S.; Gao, Y.; Cui, X. Recent Advances in Polysaccharide-Based Self-Healing Hydrogels for Biomedical Applications. Carbohydr. Polym. 2022, 283, 119161. [Google Scholar] [CrossRef] [PubMed]
- Moholkar, D.N.; Sadalage, P.S.; Peixoto, D.; Paiva-Santos, A.C.; Pawar, K.D. Recent Advances in Biopolymer-Based Formulations for Wound Healing Applications. Eur. Polym. J. 2021, 160, 110784. [Google Scholar] [CrossRef]
- Gobi, R.; Ravichandiran, P.; Babu, R.S.; Yoo, D.J. Biopolymer and Synthetic Polymer-Based Nanocomposites in Wound Dressing Applications: A Review. Polymers 2021, 13, 1962. [Google Scholar] [CrossRef] [PubMed]
- Nosrati, H.; Khodaei, M.; Alizadeh, Z.; Banitalebi-Dehkordi, M. Cationic, Anionic and Neutral Polysaccharides for Skin Tissue Engineering and Wound Healing Applications. Int. J. Biol. Macromol. 2021, 192, 298–322. [Google Scholar] [CrossRef] [PubMed]
- Raina, N.; Rani, R.; Pahwa, R.; Gupta, M. Biopolymers and Treatment Strategies for Wound Healing: An Insight View. Int. J. Polym. Mater. Polym. Biomater. 2022, 71, 359–375. [Google Scholar] [CrossRef]
- Homaeigohar, S.; Boccaccini, A.R. Antibacterial Biohybrid Nanofibers for Wound Dressings. Acta Biomater. 2020, 107, 25–49. [Google Scholar] [CrossRef] [PubMed]
- Maver, T.; Maver, U.; Pivec, T.; Kurečič, M.; Persin, Z.; Kleinschek, K.S. Polysaccharide Based Wound Care Materials. In Bioactive Polysaccharide Materials for Modern Wound Healing; SpringerBriefs in Molecular Science; Springer International Publishing: Cham, Switzerland, 2018; pp. 9–24. ISBN 978-3-319-89607-6. [Google Scholar]
- Bano, I.; Arshad, M.; Yasin, T.; Ghauri, M.A.; Younus, M. Chitosan: A Potential Biopolymer for Wound Management. Int. J. Biol. Macromol. 2017, 102, 380–383. [Google Scholar] [CrossRef]
- Tang, F.; Lv, L.; Lu, F.; Rong, B.; Li, Z.; Lu, B.; Yu, K.; Liu, J.; Dai, F.; Wu, D.; et al. Preparation and Characterization of N-Chitosan as a Wound Healing Accelerator. Int. J. Biol. Macromol. 2016, 93, 1295–1303. [Google Scholar] [CrossRef]
- Matica, M.A.; Aachmann, F.L.; Tøndervik, A.; Sletta, H.; Ostafe, V. Chitosan as a Wound Dressing Starting Material: Antimicrobial Properties and Mode of Action. Int. J. Mol. Sci. 2019, 20, 5889. [Google Scholar] [CrossRef] [Green Version]
- Feng, P.; Luo, Y.; Ke, C.; Qiu, H.; Wang, W.; Zhu, Y.; Hou, R.; Xu, L.; Wu, S. Chitosan-Based Functional Materials for Skin Wound Repair: Mechanisms and Applications. Front. Bioeng. Biotechnol. 2021, 9, 650598. [Google Scholar] [CrossRef]
- Biranje, S.S.; Madiwale, P.V.; Patankar, K.C.; Chhabra, R.; Bangde, P.; Dandekar, P.; Adivarekar, R.V. Cytotoxicity and Hemostatic Activity of Chitosan/Carrageenan Composite Wound Healing Dressing for Traumatic Hemorrhage. Carbohydr. Polym. 2020, 239, 116106. [Google Scholar] [CrossRef] [PubMed]
- Koumentakou, I.; Terzopoulou, Z.; Michopoulou, A.; Kalafatakis, I.; Theodorakis, K.; Tzetzis, D.; Bikiaris, D. Chitosan Dressings Containing Inorganic Additives and Levofloxacin as Potential Wound Care Products with Enhanced Hemostatic Properties. Int. J. Biol. Macromol. 2020, 162, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Leonhardt, E.E.; Kang, N.; Hamad, M.A.; Wooley, K.L.; Elsabahy, M. Absorbable Hemostatic Hydrogels Comprising Composites of Sacrificial Templates and Honeycomb-like Nanofibrous Mats of Chitosan. Nat. Commun. 2019, 10, 2307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowling, M.B.; Kumar, R.; Keibler, M.A.; Hess, J.R.; Bochicchio, G.V.; Raghavan, S.R. A Self-Assembling Hydrophobically Modified Chitosan Capable of Reversible Hemostatic Action. Biomaterials 2011, 32, 3351–3357. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Tang, Z.; Pan, M.; Wang, Z.; Yang, H.; Liu, H. Chitosan/Kaolin Composite Porous Microspheres with High Hemostatic Efficacy. Carbohydr. Polym. 2017, 177, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Grissom, T.E.; Fang, R. Topical Hemostatic Agents and Dressings in the Prehospital Setting. Curr. Opin. Anaesthesiol. 2015, 28, 210–216. [Google Scholar] [CrossRef]
- Han, W.; Zhou, B.; Yang, K.; Xiong, X.; Luan, S.; Wang, Y.; Xu, Z.; Lei, P.; Luo, Z.; Gao, J.; et al. Biofilm-Inspired Adhesive and Antibacterial Hydrogel with Tough Tissue Integration Performance for Sealing Hemostasis and Wound Healing. Bioact. Mater. 2020, 5, 768–778. [Google Scholar] [CrossRef]
- Movaffagh, J.; Bazzaz, B.S.F.; Yazdi, A.T.; Sajadi-Tabassi, A.; Azizzadeh, M.; Najafi, E.; Amiri, N.; Taghanaki, H.B.; Ebrahimzadeh, M.H.; Moradi, A. Wound Healing and Antimicrobial Effects of Chitosan-Hydrogel/Honey Compounds in a Rat Full-Thickness Wound Model. Wounds Compend. Clin. Res. Pract. 2019, 31, 228–235. [Google Scholar]
- Zhao, X.; Wu, H.; Guo, B.; Dong, R.; Qiu, Y.; Ma, P.X. Antibacterial Anti-Oxidant Electroactive Injectable Hydrogel as Self-Healing Wound Dressing with Hemostasis and Adhesiveness for Cutaneous Wound Healing. Biomaterials 2017, 122, 34–47. [Google Scholar] [CrossRef]
- Zhang, Y.; Guan, J.; Wu, J.; Ding, S.; Yang, J.; Zhang, J.; Dong, A.; Deng, L. N-Alkylated Chitosan/Graphene Oxide Porous Sponge for Rapid and Effective Hemostasis in Emergency Situations. Carbohydr. Polym. 2019, 219, 405–413. [Google Scholar] [CrossRef]
- Zheng, W.; Chen, C.; Zhang, X.; Wen, X.; Xiao, Y.; Li, L.; Xu, Q.; Fu, F.; Diao, H.; Liu, X. Layer-by-Layer Coating of Carboxymethyl Chitosan-Gelatin-Alginate on Cotton Gauze for Hemostasis and Wound Healing. Surf. Coat. Technol. 2021, 406, 126644. [Google Scholar] [CrossRef]
- Wang, H.; Liao, Y.; Wu, A.; Li, B.; Qian, J.; Ding, F. Effect of Sodium Trimetaphosphate on Chitosan-Methylcellulose Composite Films: Physicochemical Properties and Food Packaging Application. Polymers 2019, 11, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Qian, J.; Zhao, C.; Yang, L.; Ding, J.; Guo, H. Preparation and Evaluation of Porous Starch/Chitosan Composite Cross-Linking Hemostatic. Eur. Polym. J. 2019, 118, 17–26. [Google Scholar] [CrossRef]
- Tabriz, A.G.; Douroumis, D.; Boateng, J. 3D printed scaffolds for wound healing and tissue regeneration. In Therapeutic Dressings and Wound Healing Applications; Boateng, J., Ed.; Wiley: Hoboken, NJ, USA, 2020; pp. 385–398. ISBN 978-1-119-43326-2. [Google Scholar]
- Hu, T.; Cui, X.; Zhu, M.; Wu, M.; Tian, Y.; Yao, B.; Song, W.; Niu, Z.; Huang, S.; Fu, X. 3D-Printable Supramolecular Hydrogels with Shear-Thinning Property: Fabricating Strength Tunable Bioink via Dual Crosslinking. Bioact. Mater. 2020, 5, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Lee, J.; Huh, K.M.; Lee, S.H.; Lee, H. Toxicity-Attenuated Glycol Chitosan Adhesive Inspired by Mussel Adhesion Mechanisms. Adv. Healthc. Mater. 2019, 8, 1900275. [Google Scholar] [CrossRef]
- Li, B.; Wang, J.; Gui, Q.; Yang, H. Continuous Production of Uniform Chitosan Beads as Hemostatic Dressings by a Facile Flow Injection Method. J. Mater. Chem. B 2020, 8, 7941–7946. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Yang, X.; Liu, W.; Xi, G.; Wang, M.; Liang, B.; Ma, Z.; Feng, Y.; Chen, H.; Shi, C. Tannic Acid Cross-linked Polysaccharide-Based Multifunctional Hemostatic Microparticles for the Regulation of Rapid Wound Healing. Macromol. Biosci. 2018, 18, 1800209. [Google Scholar] [CrossRef] [PubMed]
- Mohandas, A.; Anisha, B.S.; Chennazhi, K.P.; Jayakumar, R. Chitosan–Hyaluronic Acid/VEGF Loaded Fibrin Nanoparticles Composite Sponges for Enhancing Angiogenesis in Wounds. Colloids Surf. B Biointerfaces 2015, 127, 105–113. [Google Scholar] [CrossRef]
- Saporito, F.; Sandri, G.; Rossi, S.; Bonferoni, M.C.; Riva, F.; Malavasi, L.; Caramella, C.; Ferrari, F. Freeze Dried Chitosan Acetate Dressings with Glycosaminoglycans and Traxenamic Acid. Carbohydr. Polym. 2018, 184, 408–417. [Google Scholar] [CrossRef]
- Wu, Y.; Hu, Y.; Cai, J.; Ma, S.; Wang, X. Coagulation Property of Hyaluronic Acid–Collagen/Chitosan Complex Film. J. Mater. Sci. Mater. Med. 2008, 19, 3621–3629. [Google Scholar] [CrossRef]
- He, Y.; Zhao, W.; Dong, Z.; Ji, Y.; Li, M.; Hao, Y.; Zhang, D.; Yuan, C.; Deng, J.; Zhao, P.; et al. A Biodegradable Antibacterial Alginate/Carboxymethyl Chitosan/Kangfuxin Sponges for Promoting Blood Coagulation and Full-Thickness Wound Healing. Int. J. Biol. Macromol. 2021, 167, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Szymonowicz, M.; Kucharska, M.; Wiśniewska-Wrona, M.; Dobrzyński, M.; Kołodziejczyk, K.; Rybak, Z. The Evaluation of Resorbable Haemostatic Wound Dressings in Contact with Blood in Vitro. Acta Bioeng. Biomech. 2017, 19, 151–165. [Google Scholar] [PubMed]
- Choudhary, A.; Kant, V.; Jangir, B.L.; Joshi, V.G. Quercetin Loaded Chitosan Tripolyphosphate Nanoparticles Accelerated Cutaneous Wound Healing in Wistar Rats. Eur. J. Pharmacol. 2020, 880, 173172. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Zhou, Y.; Ye, M.; An, Y.; Wang, K.; Wu, Q.; Song, L.; Zhang, J.; He, H.; Zhang, Q.; et al. Freeze-Thawing Chitosan/Ions Hydrogel Coated Gauzes Releasing Multiple Metal Ions on Demand for Improved Infected Wound Healing. Adv. Healthc. Mater. 2020, 10, 2001591. [Google Scholar] [CrossRef]
- Moura, L.I.F.; Dias, A.M.A.; Leal, E.C.; Carvalho, L.; de Sousa, H.C.; Carvalho, E. Chitosan-Based Dressings Loaded with Neurotensin—an Efficient Strategy to Improve Early Diabetic Wound Healing. Acta Biomater. 2014, 10, 843–857. [Google Scholar] [CrossRef] [Green Version]
- Graça, M.F.P.; Miguel, S.P.; Cabral, C.S.D.; Correia, I.J. Hyaluronic Acid—Based Wound Dressings: A Review. Carbohydr. Polym. 2020, 241, 116364. [Google Scholar] [CrossRef]
- Litwiniuk, M.; Krejner, A.; Speyrer, M.S.; Gauto, A.R.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration. Wounds Compend. Clin. Res. Pract. 2016, 28, 78–88. [Google Scholar]
- Yang, H.; Song, L.; Zou, Y.; Sun, D.; Wang, L.; Yu, Z.; Guo, J. Role of Hyaluronic Acids and Potential as Regenerative Biomaterials in Wound Healing. ACS Appl. Bio Mater. 2021, 4, 311–324. [Google Scholar] [CrossRef]
- Zhu, J.; Li, F.; Wang, X.; Yu, J.; Wu, D. Hyaluronic Acid and Polyethylene Glycol Hybrid Hydrogel Encapsulating Nanogel with Hemostasis and Sustainable Antibacterial Property for Wound Healing. ACS Appl. Mater. Interfaces 2018, 10, 13304–13316. [Google Scholar] [CrossRef]
- Li, H.; Xue, Y.; Jia, B.; Bai, Y.; Zuo, Y.; Wang, S.; Zhao, Y.; Yang, W.; Tang, H. The Preparation of Hyaluronic Acid Grafted Pullulan Polymers and Their Use in the Formation of Novel Biocompatible Wound Healing Film. Carbohydr. Polym. 2018, 188, 92–100. [Google Scholar] [CrossRef]
- Wang, Z.; Qian, Y.; Li, L.; Pan, L.; Njunge, L.W.; Dong, L.; Yang, L. Evaluation of Emulsion Electrospun Polycaprolactone/Hyaluronan/Epidermal Growth Factor Nanofibrous Scaffolds for Wound Healing. J. Biomater. Appl. 2016, 30, 686–698. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, L.; Hu, J.; Wang, W.; Liu, X. Promote Anti-Inflammatory and Angiogenesis Using a Hyaluronic Acid-Based Hydrogel with MiRNA-Laden Nanoparticles for Chronic Diabetic Wound Treatment. Int. J. Biol. Macromol. 2021, 166, 166–178. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Xu, P.; Yao, Z.; Cui, X.; Lei, X.; Li, L.; Dong, Y.; Zhu, W.; Guo, R.; Cheng, B. A Composite Hydrogel with Co-Delivery of Antimicrobial Peptides and Platelet-Rich Plasma to Enhance Healing of Infected Wounds in Diabetes. Acta Biomater. 2021, 121, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.P.; Santos, T.C.; Rodrigues, D.B.; Pirraco, R.P.; Cerqueira, M.T.; Reis, R.L.; Correlo, V.M.; Marques, A.P. Stem Cell-Containing Hyaluronic Acid-Based Spongy Hydrogels for Integrated Diabetic Wound Healing. J. Investig. Dermatol. 2017, 137, 1541–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes, C.; dos Santos Haupenthal, D.P.; Zaccaron, R.P.; de Bem Silveira, G.; Corrêa, M.E.A.B.; de Roch Casagrande, L.; de Sousa Mariano, S.; de Souza Silva, J.I.; de Andrade, T.A.M.; Feuser, P.E.; et al. Effects of the Association between Photobiomodulation and Hyaluronic Acid Linked Gold Nanoparticles in Wound Healing. ACS Biomater. Sci. Eng. 2020, 6, 5132–5144. [Google Scholar] [CrossRef]
- Liang, J.-I.; Lin, P.-C.; Chen, M.-Y.; Hsieh, T.-H.; Chen, J.-J.J.; Yeh, M.-L. The Effect of Tenocyte/Hyaluronic Acid Therapy on the Early Recovery of Healing Achilles Tendon in Rats. J. Mater. Sci. Mater. Med. 2014, 25, 217–227. [Google Scholar] [CrossRef]
- Barros, S.C.; Martins, J.A.; Marcos, J.C.; Cavaco-Paulo, A. Influence of Secretory Leukocyte Protease Inhibitor-Based Peptides on Elastase Activity and Their Incorporation in Hyaluronic Acid Hydrogels for Chronic Wound Therapy. Biopolymers 2012, 98, 576–590. [Google Scholar] [CrossRef] [Green Version]
- Segal, H.C.; Hunt, B.J.; Gilding, K. The Effects of Alginate and Non-Alginate Wound Dressings on Blood Coagulation and Platelet Activation. J. Biomater. Appl. 1998, 12, 249–257. [Google Scholar] [CrossRef]
- Dhivya, S.; Padma, V.V.; Santhini, E. Wound Dressings—A Review. BioMedicine 2015, 5, 22. [Google Scholar] [CrossRef]
- Varela, P.; Marlinghaus, L.; Sartori, S.; Viebahn, R.; Salber, J.; Ciardelli, G. Response of Human Macrophages to Clinically Applied Wound Dressings Loaded with Silver. Front. Bioeng. Biotechnol. 2020, 8, 124. [Google Scholar] [CrossRef] [Green Version]
- Varaprasad, K.; Jayaramudu, T.; Kanikireddy, V.; Toro, C.; Sadiku, E.R. Alginate-Based Composite Materials for Wound Dressing Application: A Mini Review. Carbohydr. Polym. 2020, 236, 116025. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Xu, K.; Mei, L.; Wu, C.; Liu, J.; Liu, Z.; Wan, L.; Zhong, W. Co-Assembled Supramolecular Hydrogels of Cell Adhesive Peptide and Alginate for Rapid Hemostasis and Efficacious Wound Healing. Soft Matter 2019, 15, 8603–8610. [Google Scholar] [CrossRef] [PubMed]
- Preman, N.K.; Es, S.P.; Prabhu, A.; Shaikh, S.B.; Vipin, C.; Barki, R.R.; Bhandary, Y.P.; Rekha, P.D.; Johnson, R.P. Bioresponsive Supramolecular Hydrogels for Hemostasis, Infection Control and Accelerated Dermal Wound Healing. J. Mater. Chem. B 2020, 8, 8585–8598. [Google Scholar] [CrossRef] [PubMed]
- Tomás, H.; Alves, C.S.; Rodrigues, J. Laponite®: A Key Nanoplatform for Biomedical Applications? Nanomed. Nanotechnol. Biol. Med. 2018, 14, 2407–2420. [Google Scholar] [CrossRef]
- Golafshan, N.; Rezahasani, R.; Esfahani, M.T.; Kharaziha, M.; Khorasani, S.N. Nanohybrid Hydrogels of Laponite: PVA-Alginate as a Potential Wound Healing Material. Carbohydr. Polym. 2017, 176, 392–401. [Google Scholar] [CrossRef]
- Tong, Z.; Chen, Y.; Liu, Y.; Tong, L.; Chu, J.; Xiao, K.; Zhou, Z.; Dong, W.; Chu, X. Preparation, Characterization and Properties of Alginate/Poly(γ-Glutamic Acid) Composite Microparticles. Mar. Drugs 2017, 15, 91. [Google Scholar] [CrossRef] [Green Version]
- Che, C.; Liu, L.; Wang, X.; Zhang, X.; Luan, S.; Yin, J.; Li, X.; Shi, H. Surface-Adaptive and On-Demand Antibacterial Sponge for Synergistic Rapid Hemostasis and Wound Disinfection. ACS Biomater. Sci. Eng. 2020, 6, 1776–1786. [Google Scholar] [CrossRef] [Green Version]
- Ge, F.; Zhu, L.; Yang, L.; Li, W.; Wei, S.; Tao, Y.; Du, G. The Soluble and Particulate Form of Alginates Positively Regulate Immune Response. Iran. J. Immunol. 2018, 15, 228–238. [Google Scholar] [CrossRef]
- Cui, T.; Li, X.; He, S.; Xu, D.; Yin, L.; Huang, X.; Deng, S.; Yue, W.; Zhong, W. Instant Self-Assembly Peptide Hydrogel Encapsulation with Fibrous Alginate by Microfluidics for Infected Wound Healing. ACS Biomater. Sci. Eng. 2020, 6, 5001–5011. [Google Scholar] [CrossRef]
- Hajiali, H.; Summa, M.; Russo, D.; Armirotti, A.; Brunetti, V.; Bertorelli, R.; Athanassiou, A.; Mele, E. Alginate–Lavender Nanofibers with Antibacterial and Anti-Inflammatory Activity to Effectively Promote Burn Healing. J. Mater. Chem. B 2016, 4, 1686–1695. [Google Scholar] [CrossRef] [Green Version]
- Koga, A.Y.; Pereira, A.V.; Lipinski, L.C.; Oliveira, M.R. Evaluation of Wound Healing Effect of Alginate Films Containin g Aloe Vera (Aloe Barbadensis Miller) Gel. J. Biomater. Appl. 2018, 32, 1212–1221. [Google Scholar] [CrossRef] [PubMed]
- Salekdeh, S.S.H.; Daemi, H.; Zare-Gachi, M.; Rajabi, S.; Bazgir, F.; Aghdami, N.; Nourbakhsh, M.S.; Baharvand, H. Assessment of the Efficacy of Tributylammonium Alginate Surface-Modified Polyurethane as an Antibacterial Elastomeric Wound Dressing for Both Noninfected and Infected Full-Thickness Wounds. ACS Appl. Mater. Interfaces 2020, 12, 3393–3406. [Google Scholar] [CrossRef] [PubMed]
- Boddupalli, A.; Bratlie, K.M. Collagen Organization Deposited by Fibroblasts Encapsulated in PH Responsive Methacrylated Alginate Hydrogels. J. Biomed. Mater. Res. A 2018, 106, 2934–2943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neibert, K.; Gopishetty, V.; Grigoryev, A.; Tokarev, I.; Al-Hajaj, N.; Vorstenbosch, J.; Philip, A.; Minko, S.; Maysinger, D. Wound-Healing with Mechanically Robust and Biodegradable Hydrogel Fibers Loaded with Silver Nanoparticles. Adv. Healthc. Mater. 2012, 1, 621–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vepari, C.; Matheson, D.; Drummy, L.; Naik, R.; Kaplan, D.L. Surface Modification of Silk Fibroin with Poly(Ethylene Glycol) for Antiadhesion and Antithrombotic Applications. J. Biomed. Mater. Res. A 2009, 93A, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Liu, J.; Peng, Z.; Liang, M.; Wang, Y.; Wang, X. Gellable Silk Fibroin-Polyethylene Sponge for Hemostasis. Artif. Cells Nanomed. Biotechnol. 2020, 48, 28–36. [Google Scholar] [CrossRef]
- Zheng, H.; Zuo, B. Functional Silk Fibroin Hydrogels: Preparation, Properties and Applications. J. Mater. Chem. B 2021, 9, 1238–1258. [Google Scholar] [CrossRef]
- Kim, S.H.; Hong, H.; Ajiteru, O.; Sultan, T.; Lee, Y.J.; Lee, J.S.; Lee, O.J.; Lee, H.; Park, H.S.; Choi, K.Y.; et al. 3D Bioprinted Silk Fibroin Hydrogels for Tissue Engineering. Nat. Protoc. 2021, 16, 5484–5532. [Google Scholar] [CrossRef]
- Sun, W.; Gregory, D.A.; Tomeh, M.A.; Zhao, X. Silk Fibroin as a Functional Biomaterial for Tissue Engineering. Int. J. Mol. Sci. 2021, 22, 1499. [Google Scholar] [CrossRef]
- Chouhan, D.; Mandal, B.B. Silk Biomaterials in Wound Healing and Skin Regeneration Therapeutics: From Bench to Bedside. Acta Biomater. 2020, 103, 24–51. [Google Scholar] [CrossRef]
- Adalı, T.; Uncu, M. Silk Fibroin as a Non-Thrombogenic Biomaterial. Int. J. Biol. Macromol. 2016, 90, 11–19. [Google Scholar] [CrossRef]
- Sen, S.; Basak, P.; Sinha, B.P.; Maurye, P.; Jaiswal, K.K.; Das, P.; Mandal, T.K. Anti-Inflammatory Effect of Epidermal Growth Factor Conjugated Silk Fibroin Immobilized Polyurethane Ameliorates Diabetic Burn Wound Healing. Int. J. Biol. Macromol. 2020, 143, 1009–1032. [Google Scholar] [CrossRef] [PubMed]
- Chouhan, D.; Janani, G.; Chakraborty, B.; Nandi, S.K.; Mandal, B.B. Functionalized PVA–Silk Blended Nanofibrous Mats Promote Diabetic Wound Healing via Regulation of Extracellular Matrix and Tissue Remodelling. J. Tissue Eng. Regen. Med. 2018, 12, e1559–e1570. [Google Scholar] [CrossRef] [PubMed]
- Arasteh, S.; Khanjani, S.; Golshahi, H.; Mobini, S.; Jahed, M.T.; Heidari-Vala, H.; Edalatkhah, H.; Kazemnejad, S. Efficient Wound Healing Using a Synthetic Nanofibrous Bilayer Skin Substitute in Murine Model. J. Surg. Res. 2020, 245, 31–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gholipourmalekabadi, M.; Seifalian, A.M.; Urbanska, A.M.; Omrani, M.D.; Hardy, J.G.; Madjd, Z.; Hashemi, S.M.; Ghanbarian, H.; Brouki Milan, P.; Mozafari, M.; et al. 3D Protein-Based Bilayer Artificial Skin for the Guided Scarless Healing of Third-Degree Burn Wounds in Vivo. Biomacromolecules 2018, 19, 2409–2422. [Google Scholar] [CrossRef] [Green Version]
- Böhm, S.; Strauß, C.; Stoiber, S.; Kasper, C.; Charwat, V. Impact of Source and Manufacturing of Collagen Matrices on Fibroblast Cell Growth and Platelet Aggregation. Materials 2017, 10, 1086. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.A.; Taylor, N.L.; Jalan, A.A.; Hwang, L.K.; Wang, B.K.; Hartgerink, J.D. A Nanostructured Synthetic Collagen Mimic for Hemostasis. Biomacromolecules 2014, 15, 1484–1490. [Google Scholar] [CrossRef]
- Zheng, C.; Liu, X.; Luo, X.; Zheng, M.; Wang, X.; Dan, W.; Jiang, H. Development of a Novel Bio-Inspired “Cotton-like” Collagen Aggregate/Chitin Based Biomaterial with a Biomimetic 3D Microstructure for Efficient Hemostasis and Tissue Repair. J. Mater. Chem. B 2019, 7, 7338–7350. [Google Scholar] [CrossRef]
- Hsu, F.-Y.; Cheng, Y.-Y.; Tsai, S.-W.; Tsai, W.-B. Fabrication and Evaluation of a Biodegradable Cohesive Plug Based on Reconstituted Collagen/γ-Polyglutamic Acid. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 95B, 29–35. [Google Scholar] [CrossRef]
- Natarajan, J.; Sanapalli, B.K.R.; Bano, M.; Singh, S.K.; Gulati, M.; Karri, V.V.S.R. Nanostructured Lipid Carriers of Pioglitazone Loaded Collagen/Chitosan Composite Scaffold for Diabetic Wound Healing. Adv. Wound Care 2019, 8, 499–513. [Google Scholar] [CrossRef]
- Tort, S.; Demiröz, F.T.; Coşkun Cevher, Ş.; Sarıbaş, S.; Özoğul, C.; Acartürk, F. The Effect of a New Wound Dressing on Wound Healing: Biochemical and Histopathological Evaluation. Burns 2020, 46, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Breder, J.S.C.; Pires, A.L.R.; Azevedo, F.F.; Apolinário, P.P.; Cantaruti, T.; Jiwani, S.I.; Moraes, Â.M.; Consonni, S.R.; Araújo, E.P.; Adams, G.G.; et al. Enhancement of Cellular Activity in Hyperglycemic Mice Dermal Wounds Dressed with Chitosan-Alginate Membranes. Braz. J. Med. Biol. Res. 2020, 53, e8621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caetano, G.F.; Frade, M.A.C.; Andrade, T.A.M.; Leite, M.N.; Bueno, C.Z.; Moraes, Â.M.; Ribeiro-Paes, J.T. Chitosan-Alginate Membranes Accelerate Wound Healing. J. Biomed. Mater. Res. B Appl. Biomater. 2015, 103, 1013–1022. [Google Scholar] [CrossRef]
- Alves, R.; Grimalt, R. A Review of Platelet-Rich Plasma: History, Biology, Mechanism of Action, and Classification. Skin Appendage Disord. 2018, 4, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Everts, P.A.M.; Knape, J.T.A.; Weibrich, G.; Schönberger, J.P.A.M.; Hoffmann, J.; Overdevest, E.P.; Box, H.A.M.; van Zundert, A. Platelet-Rich Plasma and Platelet Gel: A Review. J. Extra. Corpor. Technol. 2006, 38, 174–187. [Google Scholar] [PubMed]
- Andia, I.; Abate, M. Platelet-Rich Plasma: Underlying Biology and Clinical Correlates. Regen. Med. 2013, 8, 645–658. [Google Scholar] [CrossRef]
- Lehn, A. Platelet-rich plasma in tissue engineering. In Biomaterials for Organ and Tissue Regeneration; Elsevier: Amsterdam, The Netherlands, 2020; pp. 477–496. ISBN 978-0-08-102906-0. [Google Scholar]
- Suresh, A.; Balouch, B.; Martha, V.V.; Sataloff, R.T. Laryngeal Applications of Platelet Rich Plasma and Platelet Poor Plasma: A Systematic Review. J. Voice 2021, in press. [CrossRef]
- Andia, I.; Perez-Valle, A.; Del Amo, C.; Maffulli, N. Freeze-Drying of Platelet-Rich Plasma: The Quest for Standardization. Int. J. Mol. Sci. 2020, 21, 6904. [Google Scholar] [CrossRef]
- Magalon, J.; Chateau, A.L.; Bertrand, B.; Louis, M.L.; Silvestre, A.; Giraudo, L.; Veran, J.; Sabatier, F. DEPA Classification: A Proposal for Standardising PRP Use and a Retrospective Application of Available Devices. BMJ Open Sport Exerc. Med. 2016, 2, e000060. [Google Scholar] [CrossRef] [Green Version]
- Harrison, P.; the Subcommittee on Platelet Physiology. The Use of Platelets in Regenerative Medicine and Proposal for a New Classification System: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1895–1900. [Google Scholar] [CrossRef]
- Acebes-Huerta, A.; Arias-Fernández, T.; Bernardo, Á.; Muñoz-Turrillas, M.C.; Fernández-Fuertes, J.; Seghatchian, J.; Gutiérrez, L. Platelet-Derived Bio-Products: Classification Update, Applications, Concerns and New Perspectives. Transfus. Apher. Sci. 2020, 59, 102716. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Stojanovic, P. Platelet Rich Plasma: A Short Overview of Certain Bioactive Components. Open Med. Wars. Pol. 2016, 11, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, R.G.; Santos, G.S.; Alkass, N.; Chiesa, T.L.; Azzini, G.O.; da Fonseca, L.F.; dos Santos, A.F.; Rodrigues, B.L.; Mosaner, T.; Lana, J.F. The Regenerative Mechanisms of Platelet-Rich Plasma: A Review. Cytokine 2021, 144, 155560. [Google Scholar] [CrossRef] [PubMed]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef]
- Samadian, H.; Ehterami, A.; Sarrafzadeh, A.; Khastar, H.; Nikbakht, M.; Rezaei, A.; Chegini, L.; Salehi, M. Sophisticated Polycaprolactone/Gelatin Nanofibrous Nerve Guided Conduit Containing Platelet-Rich Plasma and Citicoline for Peripheral Nerve Regeneration: In Vitro and in Vivo Study. Int. J. Biol. Macromol. 2020, 150, 380–388. [Google Scholar] [CrossRef]
- Chen, L.-C.; Lin, S.-Y.; Sheu, M.-T.; Su, C.-H.; Lin, H.-L.; Hsieh, C.-M. Fabrication and Characterization of Rhizochitosan and Its Incorporation with Platelet Concentrates to Promote Wound Healing. Carbohydr. Polym. 2021, 268, 118239. [Google Scholar] [CrossRef]
- Rossi, S.; Mori, M.; Vigani, B.; Bonferoni, M.C.; Sandri, G.; Riva, F.; Caramella, C.; Ferrari, F. A Novel Dressing for the Combined Delivery of Platelet Lysate and Vancomycin Hydrochloride to Chronic Skin Ulcers: Hyaluronic Acid Particles in Alginate Matrices. Eur. J. Pharm. Sci. 2018, 118, 87–95. [Google Scholar] [CrossRef]
- Horimizu, M.; Kawase, T.; Nakajima, Y.; Okuda, K.; Nagata, M.; Wolff, L.F.; Yoshie, H. An Improved Freeze-Dried PRP-Coated Biodegradable Material Suitable for Connective Tissue Regenerative Therapy. Cryobiology 2013, 66, 223–232. [Google Scholar] [CrossRef]
- Lima, A.C.; Mano, J.F.; Concheiro, A.; Alvarez-Lorenzo, C. Fast and Mild Strategy, Using Superhydrophobic Surfaces, to Produce Collagen/Platelet Lysate Gel Beads for Skin Regeneration. Stem Cell Rev. Rep. 2015, 11, 161–179. [Google Scholar] [CrossRef]
- Nardini, M.; Perteghella, S.; Mastracci, L.; Grillo, F.; Marrubini, G.; Bari, E.; Formica, M.; Gentili, C.; Cancedda, R.; Torre, M.L.; et al. Growth Factors Delivery System for Skin Regeneration: An Advanced Wound Dressing. Pharmaceutics 2020, 12, 120. [Google Scholar] [CrossRef] [Green Version]
- Notodihardjo, S.C.; Morimoto, N.; Kakudo, N.; Mitsui, T.; Le, T.M.; Tabata, Y.; Kusumoto, K. Comparison of the Efficacy of Cryopreserved Human Platelet Lysate and Refrigerated Lyophilized Human Platelet Lysate for Wound Healing. Regen. Ther. 2019, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Notodihardjo, S.C.; Morimoto, N.; Kakudo, N.; Mitsui, T.; Le, T.M.; Tabata, Y.; Kusumoto, K. Efficacy of Gelatin Hydrogel Impregnated with Concentrated Platelet Lysate in Murine Wound Healing. J. Surg. Res. 2019, 234, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Qian, Z.; Liu, B.; Liu, J.; Zhang, L.; Xu, J. In Vitro and in Vivo Evaluation of New PRP Antibacterial Moisturizing Dressings for Infectious Wound Repair. J. Biomater. Sci. Polym. Ed. 2019, 30, 462–485. [Google Scholar] [CrossRef] [PubMed]
- Yassin, G.E.; Dawoud, M.H.S.; Wasfi, R.; Maher, A.; Fayez, A.M. Comparative Lyophilized Platelet-Rich Plasma Wafer and Powder for Wound-Healing Enhancement: Formulation, in vitro and in vivo Studies. Drug Dev. Ind. Pharm. 2019, 45, 1379–1387. [Google Scholar] [CrossRef]
- Goyal, B.; Tewari, S.; Duhan, J.; Sehgal, P.K. Comparative Evaluation of Platelet-Rich Plasma and Guided Tissue Regeneration Membrane in the Healing of Apicomarginal Defects: A Clinical Study. J. Endod. 2011, 37, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Wang, H.; Bai, Y.; Wang, Y.; Tao, L.; Wei, Y.; Fan, Y.; Guo, X.; Liu, H. Improving Chronic Diabetic Wound Healing through an Injectable and Self-Healing Hydrogel with Platelet-Rich Plasma Release. ACS Appl. Mater. Interfaces 2020, 12, 55659–55674. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lin, F.; Zhou, M.; Li, Y.; Li, W.; Shan, G.; Xu, Y.; Xu, J.; Yang, J. Preparation of Biocompatible Wound Dressings with Dual Release of Antibiotic and Platelet-Rich Plasma for Enhancing Infected Wound Healing. J. Biomater. Appl. 2021, 36, 219–236. [Google Scholar] [CrossRef]
- Farjah, M.H.; Farahpour, M.R. Efficacy of Topical Platelet-Rich Plasma and Chitosan Co-Administration on Candida Albicans-Infected Partial Thickness Burn Wound Healing. Burns J. Int. Soc. Burn Inj. 2020, 46, 1889–1895. [Google Scholar] [CrossRef]
- Effect of Platelet Rich Plasma and Keratinocyte Suspensions on Wound Healing (NCT00856934). Available online: https://clinicaltrials.gov/ct2/show/NCT00856934?term=Centre+Hospitalier+Universitaire+Vaudois&cond=PRP&cntry=CH&draw=2&rank=1 (accessed on 30 September 2021).
- Role of Autologous Platelet Rich Plasma in Total Knee Arthroplasty (PRPTKA2012). Available online: https://clinicaltrials.gov/ct2/show/NCT01563380?cond=Role+of+Autologous+Platelet+Rich+Plasma+in+Total+Knee+Arthroplasty&draw=2&rank=1 (accessed on 30 September 2021).
- Aggarwal, A.K.; Shashikanth, V.S.; Marwaha, N. Platelet-Rich Plasma Prevents Blood Loss and Pain and Enhances Early Functional Outcome after Total Knee Arthroplasty: A Prospective Randomised Controlled Study. Int. Orthop. 2014, 38, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Boztug, C.Y.; Karaagac Akyol, T.; Benlice, C.; Koc, M.A.; Erdogan, B.D.; Ozcebe, O.I.; Kuzu, M.A.; Akyol, C. Platelet-Rich Plasma Treatment Improves Postoperative Recovery in Patients with Pilonidal Sinus Disease: A Randomized Controlled Clinical Trial. BMC Surg. 2021, 21, 373. [Google Scholar] [CrossRef]
- Platelet Rich Plasma and Autologous Fat Graft for Diabetic Ulcer (NCT03085550). Available online: https://clinicaltrials.gov/ct2/show/NCT03085550?cond=Platelet+Rich+Plasma+and+Autologous+Fat+Graft+for+Diabetic+Ulcer.&draw=2&rank=1 (accessed on 30 September 2021).
- Smith, O.J.; Leigh, R.; Kanapathy, M.; Macneal, P.; Jell, G.; Hachach-Haram, N.; Mann, H.; Mosahebi, A. Fat Grafting and Platelet-Rich Plasma for the Treatment of Diabetic Foot Ulcers: A Feasibility-Randomised Controlled Trial. Int. Wound J. 2020, 17, 1578–1594. [Google Scholar] [CrossRef] [PubMed]
- Nolan, G.S.; Smith, O.J.; Heavey, S.; Jell, G.; Mosahebi, A. Histological Analysis of Fat Grafting with Platelet-rich Plasma for Diabetic Foot Ulcers—A Randomised Controlled Trial. Int. Wound J. 2022, 19, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Dehkordi, A.N.; Babaheydari, F.M.; Chehelgerdi, M.; Dehkordi, S.R. Skin Tissue Engineering: Wound Healing Based on Stem-Cell-Based Therapeutic Strategies. Stem Cell Res. Ther. 2019, 10, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, K.L.; Goverman, J.; Ma, H.; Fischman, A.; Yu, Y.-M.; Bilodeau, M.; Rad, A.M.; Bonab, A.A.; Tompkins, R.G.; Fagan, S.P. Stem Cells and Burns: Review and Therapeutic Implications. J. Burn Care Res. 2010, 31, 874–881. [Google Scholar] [CrossRef]
- Zakrzewski, W.; Dobrzyński, M.; Szymonowicz, M.; Rybak, Z. Stem Cells: Past, Present, and Future. Stem Cell Res. Ther. 2019, 10, 68. [Google Scholar] [CrossRef]
- Duscher, D.; Barrera, J.; Wong, V.W.; Maan, Z.N.; Whittam, A.J.; Januszyk, M.; Gurtner, G.C. Stem Cells in Wound Healing: The Future of Regenerative Medicine? A Mini-Review. Gerontology 2016, 62, 216–225. [Google Scholar] [CrossRef]
- Kanji, S.; Das, H. Advances of Stem Cell Therapeutics in Cutaneous Wound Healing and Regeneration. Mediat. Inflamm. 2017, 2017, 5217967. [Google Scholar] [CrossRef] [Green Version]
- Langer, R.; Vacanti, J.P. Tissue Engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Swioklo, S.; Connon, C.J. Keeping Cells in Their Place: The Future of Stem Cell Encapsulation. Expert Opin. Biol. Ther. 2016, 16, 1181–1183. [Google Scholar] [CrossRef]
- Kulkarni, P.; Parkale, R.; Khare, S.; Kumar, P.; Arya, N. Cell immobilization strategies for tissue engineering: Recent trends and future perspectives. In Immobilization Strategies; Tripathi, A., Melo, J.S., Eds.; Gels Horizons: From Science to Smart Materials; Springer: Singapore, 2021; pp. 85–139. ISBN 9789811579974. [Google Scholar]
- Wang, S.; Yang, H.; Tang, Z.; Long, G.; Huang, W. Wound Dressing Model of Human Umbilical Cord Mesenchymal Stem Cells-Alginates Complex Promotes Skin Wound Healing by Paracrine Signaling. Stem Cells Int. 2016, 2016, 3269267. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; He, S.; Su, Z.; Yang, Z.; Liang, X.; Wu, Y. Thermosensitive Injectable Chitosan/Collagen/β-Glycerophosphate Composite Hydrogels for Enhancing Wound Healing by Encapsulating Mesenchymal Stem Cell Spheroids. ACS Omega 2020, 5, 21015–21023. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; He, Y.; Zhou, T.; Zhang, P.; Gao, J.; Lu, F. Adipose Extracellular Matrix/Stromal Vascular Fraction Gel Secretes Angiogenic Factors and Enhances Skin Wound Healing in a Murine Model. BioMed Res. Int. 2017, 2017, 3105780. [Google Scholar] [CrossRef] [PubMed]
- Nilforoushzadeh, M.A.; Sisakht, M.M.; Amirkhani, M.A.; Seifalian, A.M.; Banafshe, H.R.; Verdi, J.; Nouradini, M. Engineered Skin Graft with Stromal Vascular Fraction Cells Encapsulated in Fibrin–Collagen Hydrogel: A Clinical Study for Diabetic Wound Healing. J. Tissue Eng. Regen. Med. 2020, 14, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, Z.; Pan, D.; Li, H.; Shen, J. Umbilical Cord-Derived Mesenchymal Stem Cell-Derived Exosomes Combined Pluronic F127 Hydrogel Promote Chronic Diabetic Wound Healing and Complete Skin Regeneration. Int. J. Nanomed. 2020, 15, 5911–5926. [Google Scholar] [CrossRef]
- Palakkara, S.; Maiti, S.K.; Mohan, D.; Shivaraju, S.; Raguvaran, R.; Kalaiselvan, E.; Kumar, N. Healing Potential of Chitosan and Decellularized Intestinal Matrix with Mesenchymal Stem Cells and Growth Factor in Burn Wound in Rat. Wound Med. 2020, 30, 100192. [Google Scholar] [CrossRef]
- Catanzano, O.; Boateng, J. Local Delivery of Growth Factors Using Wound Dressings. In Therapeutic Dressings and Wound Healing Applications; Boateng, J., Ed.; Wiley: Hoboken, NJ, USA, 2020; pp. 291–314. ISBN 978-1-119-43326-2. [Google Scholar]
- Catanzano, O.; Quaglia, F.; Boateng, J.S. Wound Dressings as Growth Factor Delivery Platforms for Chronic Wound Healing. Expert Opin. Drug Deliv. 2021, 18, 737–759. [Google Scholar] [CrossRef]
- Umar, A.K.; Sriwidodo, S.; Maksum, I.P.; Wathoni, N. Film-Forming Spray of Water-Soluble Chitosan Containing Liposome-Coated Human Epidermal Growth Factor for Wound Healing. Molecules 2021, 26, 5326. [Google Scholar] [CrossRef]
- Mariia, K.; Arif, M.; Shi, J.; Song, F.; Chi, Z.; Liu, C. Novel Chitosan-Ulvan Hydrogel Reinforcement by Cellulose Nanocrystals with Epidermal Growth Factor for Enhanced Wound Healing: In Vitro and in Vivo Analysis. Int. J. Biol. Macromol. 2021, 183, 435–446. [Google Scholar] [CrossRef]
- Lin, S.; Pei, L.; Zhang, W.; Shu, G.; Lin, J.; Li, H.; Xu, F.; Tang, H.; Peng, G.; Zhao, L.; et al. Chitosan-Poloxamer-Based Thermosensitive Hydrogels Containing Zinc Gluconate/Recombinant Human Epidermal Growth Factor Benefit for Antibacterial and Wound Healing. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 130, 112450. [Google Scholar] [CrossRef]
- Tsai, H.-C.; Sheng, C.; Chang, L.-S.; Wen, Z.-H.; Ho, C.-Y.; Chen, C.-M. Chitosan-Microencapsulated RhEGF in Promoting Wound Healing. J. Wound Care 2021, 30, IXi. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Z.; Wang, Y.; Wang, Q.; Yao, M.; Zhao, L.; Shi, J.; Guan, F.; Ma, S. PDGF-BB/SA/Dex Injectable Hydrogels Accelerate BMSC-Mediated Functional Full Thickness Skin Wound Repair by Promoting Angiogenesis. J. Mater. Chem. B 2021, 9, 6176–6189. [Google Scholar] [CrossRef] [PubMed]
- Muchová, J.; Hearnden, V.; Michlovská, L.; Vištejnová, L.; Zavaďáková, A.; Šmerková, K.; Kočiová, S.; Adam, V.; Kopel, P.; Vojtová, L. Mutual Influence of Selenium Nanoparticles and FGF2-STAB® on Biocompatible Properties of Collagen/Chitosan 3D Scaffolds: In Vitro and Ex Ovo Evaluation. J. Nanobiotechnol. 2021, 19, 103. [Google Scholar] [CrossRef] [PubMed]
- Caba, B.; Gardikiotis, I.; Topala, I.; Mihaila, I.; Mihai, C.T.; Luca, C.; Pasca, S.; Caba, I.C.; Dimitriu, G.; Huzum, B.; et al. Cold Atmospheric Plasma, Platelet-Rich Plasma, and Nitric Oxide Synthesis Inhibitor: Effects Investigation on an Experimental Model on Rats. Appl. Sci. 2022, 12, 590. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Therapeutic Product | Advantages | Disadvantages | Refs. |
|---|---|---|---|
| Commercial dressings (e.g., Aquacel (carboxymethyl-cellulose), Kaltostat (ALG), Carboflex (ALG), Carbonet (cellulose) [17] |
|
| [8,18] |
| Biopolymer dressings |
|
| [19,20] |
| PRP derivatives |
|
| [21,22] |
| Growth factors |
|
| [23] |
| No. | Biopolymers Used for the Investigated Support | Conditions | Identifier/Status |
|---|---|---|---|
| 1 | Collagen/ type III collagen/ type I calf collagen matrix | Wounds | NCT02314416 Withdrawn 2015 |
| 2 | Diabetic foot ulcers | NCT03010319 Completed 2021 | |
| 3 | Diabetic foot ulcers | NCT01270633 Terminated 2017 (business decision) | |
| 4 | Diabetic foot ulcers | NCT01729286 Terminated | |
| 5 | Localized gingival recessions | NCT02206009 Completed | |
| 6 | Split-thickness skin grafts Wound healing | NCT03334656 Recruiting | |
| 7 | Fibrin | Artificially induced wounds | NCT01253135 Completed 2015 |
| 8 | Silk fibroin | Donor-site wounds | NCT01993030 Completed with results |
| 9 | Late complications from skin graft infection of skin donor site; pain | NCT02091076 Completed 2016 | |
| 10 | Silk sericin | Late complications from skin graft infection of skin donor site; pain | NCT01539980 Completed 2015 |
| 11 | Silk sericin and collagen | Wound healing; wound surgery Donor-site complications | NCT04743375 Recruiting |
| 12 | Cellulose/ carboxymethyl cellulose/ hydroxyethyl cellulose | Venous ulcers | NCT00446823 Completed |
| 13 | Pemphigus Pemphigoid | NCT02365675 Unknown | |
| 14 | Burns | NCT02318056 Withdrawn (reorganization) | |
| 15 | Venous leg ulcers | NCT02921750 Completed 2020 | |
| 16 | Wound healing Patient comfort | NCT00428623 Completed 2007 | |
| 17 | Wound healing Total hip and total knee arthroplasty | NCT01258270 Completed 2013 | |
| 18 | Diabetic foot ulcers | NCT02667327 Terminated | |
| 19 | Chitosan | Postpartum bleeding Vaginal lacerations Cervical lacerations | NCT01373801 Unknown as of 2011 |
| 20 | Tooth extraction | NCT03108365 Completed | |
| 21 | Cesarean wounds Scars; previous cesarean section | NCT04211597 Completed 2019 | |
| 22 | Poly-N-acetyl glucosamine | Venous stasis ulcers Venous insufficiency | Terminated; completed 2013 |
| 23 | Alginate/ calcium alginate | Chronic wounds (>6 weeks) | NCT05009576 Completed 2021 |
| 24 | Impaired wound healing Postoperative deep wound infections | NCT02198066 Completed 2014 | |
| 25 | Pilonidal sinuses | NCT02011802 Completed 2017 | |
| 26 | Hyaluronic acid | Wound healing | NCT03668665 Withdrawn (last update 2019) |
| 27 | Pilonidal cysts | NCT02485860 Recruiting | |
| 28 | Free gingival grafts | NCT04390100 Completed 2020 | |
| 29 | Wound healing Complications | NCT02534415 Completed 2015 | |
| 30 | Oxidized regenerated cellulose and collagen | Venous ulcers Diabetic foot ulcers | NCT02845466 Unknown |
| 31 | Alginate and high-G cellulose | Pilonidal cysts/fistulas | Terminated (due to COVID-19 pandemic) |
| 32 | Carboxymethyl cellulose and sodium alginate | Diabetic foot ulcers Neuropathic diabetic foot ulcers | NCT03700580 Completed 2018 |
| PRP Biopolymer-Based Products | Condition | Ref. |
|---|---|---|
| Polycaprolactone/gelatin filled with citicoline-bearing PRP gel | Autografting approach for peripheral nerve injury (PNI) treatment | [143] |
| Rhizochitosan and PRP | Full-thickness wound model | [144] |
| HA core-shell particles, loaded with PL and coated with calcium alginate, embedded in a VCM-containing alginate matrix | Chronic skin ulcers | [145] |
| Lyophilized Col sponge coated with PRP | Wounds Human periosteal fibroblasts Diabetic mice model | [146] |
| Freeze-dried platelet lysate encapsulated in Col, hASCs encapsulated in collagen plus platelet lysate beads | Wounds; in vitro tests: scratch wound assay, chick chorioallantoic membrane test | [147] |
| ALG/silk sericrin vs. freeze-dried platelet lysate/ALG/silk sericrin vs. alginate/freeze-dried platelet lysate (FD-PL) | Full-thickness chronic wounds in mouse model C57/BL6; granulation tissue, early inflammation, collagen deposition, fibroblast maturation, re-epithelialization, neovascularization | [148] |
| C-hPL, CL-hPL and L-hPL groups plus gelatin Human platelet lysate C-hPL: the cryopreservation hPL group CL-hPL: cryopreservated and lyophilized; L-lyophilized | Full-thickness wounds in male C57bl6J/Jcl mice Histology in mice: wound area, neovascularization, granulation tissue formation | [149] |
| Gelatin hydrogel (GH) sheet impregnated with PRP FD-PL vs. different concentrations of FD-PL | Full-thickness wounds in C57BL6J/Jcl mice; histology: H&E, Azan and anti-CD31 | [150] |
| Cs/SF nanosilver loaded with FD-PRP (freeze-dried) | Wounds in BALBc mice; wound moisture retention and promotion of healing | [151] |
| FD-PRP plus carboxymethyl cellulose (CMC) (wafers) vs. FD-PRP powder | Wounds in a rat wound model | [152] |
| PRP plus a Col sponge (Collacote) | Apicomarginal defects: clinical study | [153] |
| Injectable hydrogel with a composite of chitosan, silk fibroin and PRP | Diabetic skin ulcer: in vitro and in vivo rat model | [154] |
| Carboxymethyl Cs gelatin microspheres loaded with gentamycin sulfate and PRP | Treatment of chronic and infected wounds in a Sprague–Dawley rats model | [155] |
| PRP and Cs dressing | Candida albicans-infected burn wound model in Wistar rats | [156] |
| Oxidized dextran/peptide-modified hyaluronic acid and PRP hydrogel | E. coli-, S. aureus- and P. aeruginosa-infected wounds in diabetic mouse model | [90] |
| Growth Factor Biopolymer-Based Products | Condition | Ref. |
|---|---|---|
| Film-forming spray of water-soluble chitosan containing hEGF-liposomes | Wound in male mice of the Swiss Webster strain | [180] |
| Cs-ulvan hydrogel incorporated in cellulose nanocrystal loaded with epidermal growth factor | Full-thickness skin wound in Balb/c mice | [181] |
| Cs/poloxamer-based thermosensitive hydrogels containing zinc gluconate/recombinant human epidermal growth factor | Scald wound model | [182] |
| Cs and EGF spray | Full-thickness wound in Wistar rat | [183] |
| Injectable hydrogel with sodium ALG, dextran, PDGF-BB and bone marrow-derived mesenchymal stem cells (BMSCs) | Full-thickness excisional wound model in C57BL/6 mice | [184] |
| Three dimensional porous collagen/chitosan scaffolds with selenium nanoparticles and fibroblast growth factor 2 (FGF2-STAB®) | In vitro and ex vivo evaluation | [185] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gardikiotis, I.; Cojocaru, F.-D.; Mihai, C.-T.; Balan, V.; Dodi, G. Borrowing the Features of Biopolymers for Emerging Wound Healing Dressings: A Review. Int. J. Mol. Sci. 2022, 23, 8778. https://doi.org/10.3390/ijms23158778
Gardikiotis I, Cojocaru F-D, Mihai C-T, Balan V, Dodi G. Borrowing the Features of Biopolymers for Emerging Wound Healing Dressings: A Review. International Journal of Molecular Sciences. 2022; 23(15):8778. https://doi.org/10.3390/ijms23158778
Chicago/Turabian StyleGardikiotis, Ioannis, Florina-Daniela Cojocaru, Cosmin-Teodor Mihai, Vera Balan, and Gianina Dodi. 2022. "Borrowing the Features of Biopolymers for Emerging Wound Healing Dressings: A Review" International Journal of Molecular Sciences 23, no. 15: 8778. https://doi.org/10.3390/ijms23158778
APA StyleGardikiotis, I., Cojocaru, F. -D., Mihai, C. -T., Balan, V., & Dodi, G. (2022). Borrowing the Features of Biopolymers for Emerging Wound Healing Dressings: A Review. International Journal of Molecular Sciences, 23(15), 8778. https://doi.org/10.3390/ijms23158778