
Matrix Metalloproteinase 8 Expression in a Tumour Predicts a Favourable Prognosis in Pancreatic Ductal Adenocarcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Immunohistochemical Staining of MMP-8 in Cancer Cells, Number of Tumour-Associated MMP-8-Positive PMNs and Plasma CRP Levels
2.2. Association of MMP-8 Expression, Tumour-Associated MMP-8-Positive PMNs and Plasma CRP Level with Clinicopathological Characteristics
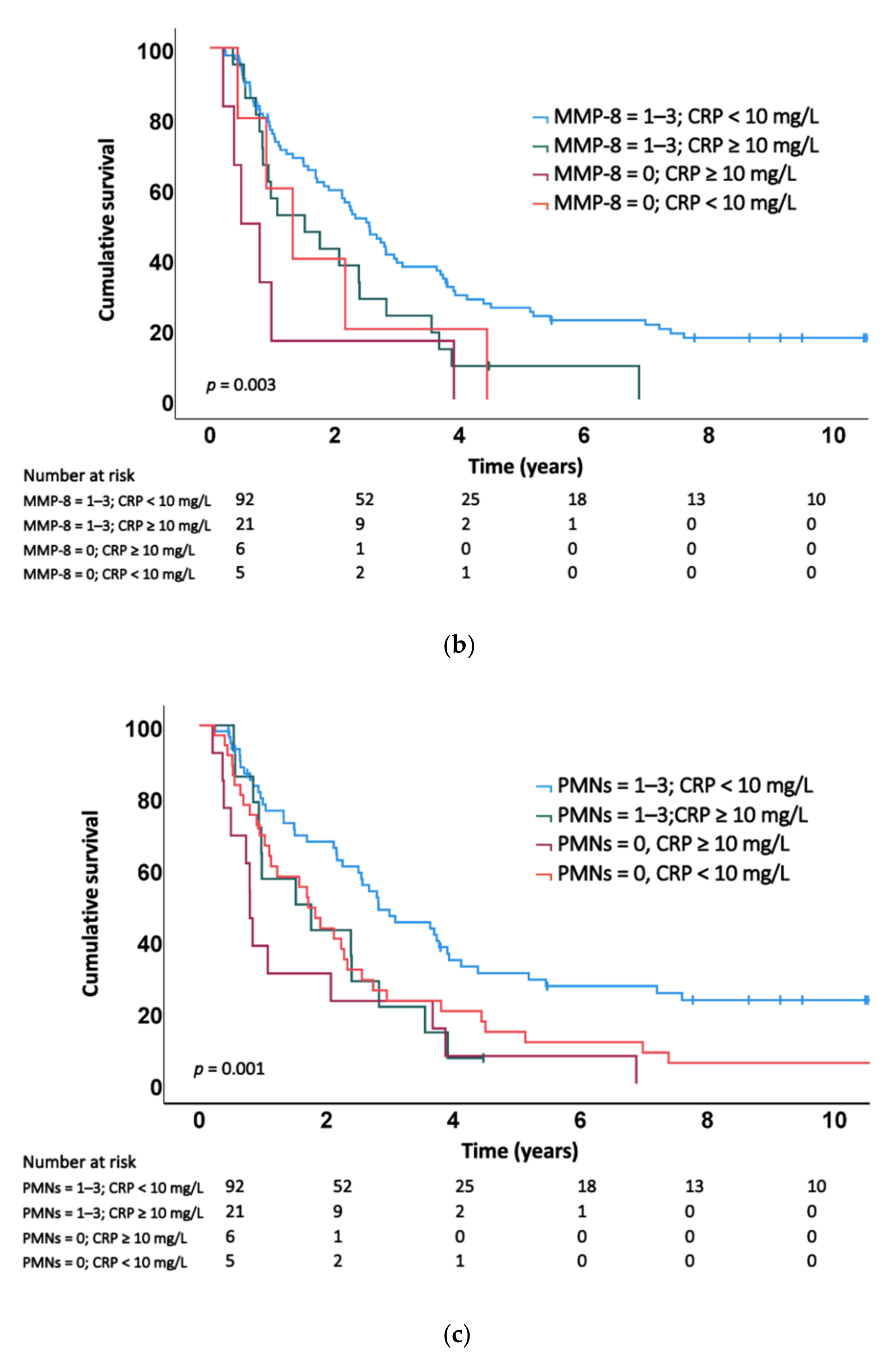
2.3. Association of MMP-8 Expression, Tumour-Associated MMP-8-Positive PMNs and the Plasma CRP Level with Survival
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Preparation of Tumour Tissue Microarrays, Immunohistochemistry and the Measurement of the Plasma C-Reactive Protein Level
4.3. Evaluation of Stainings
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Cancer Research UK. Pancreatic Cancer Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/pancreatic-cancer#heading-Two (accessed on 3 June 2020).
- World Health Organization. Cancer Today. 2018. Available online: https://gco.iarc.fr/today/online-analysis-table?v=2018&mode=cancer&mode_population=continents&population=900&populations=900&key=a (accessed on 2 June 2020).
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [PubMed]
- Seppänen, H.; Juuti, A.; Mustonen, H.; Haapamäki, C.; Nordling, S.; Carpelan-Holmström, M.; Sirén, J.; Luettges, J.; Haglund, C.; Kiviluoto, T. The Results of Pancreatic Resections and Long-Term Survival for Pancreatic Ductal Adenocarcinoma: A Single-Institution Experience. Scand. J. Surg. 2017, 106, 54–61. [Google Scholar] [PubMed] [Green Version]
- Ying, H.; Dey, P.; Yao, W.; Kimmelman, A.C.; Draetta, G.F.; Maitra, A.; DePinho, R.A. Genetics and biology of pancreatic ductal adenocarcinoma. Genes Dev. 2016, 30, 355–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laheru, D.; Jaffee, E.M. Immunotherapy for pancreatic cancer—Science driving clinical progress. Nat. Rev. Cancer 2005, 5, 459–467. [Google Scholar] [CrossRef]
- Malemud, C.J. Matrix metalloproteinases (MMPs) in health and disease: An overview. Front. Biosci. 2006, 11, 1696–1701. [Google Scholar] [CrossRef] [PubMed]
- Cui, N.; Hu, M.; Khalil, R.A. Biochemical and Biological Attributes of Matrix Metalloproteinases. Prog. Mol. Biol. Transl. Sci. 2017, 147, 1–73. [Google Scholar] [PubMed] [Green Version]
- Egeblad, M.; Werb, Z. New functions for the matrix metalloproteinases in cancer progression. Nat. Rev. Cancer 2002, 2, 161–174. [Google Scholar] [CrossRef]
- Curran, S.; Murray, G.I. Matrix metalloproteinases in tumour invasion and metastasis. J. Pathol. 1999, 189, 300–308. [Google Scholar]
- Hanemaaijer, R.; Sorsa, T.; Konttinen, Y.T.; Ding, Y.; Sutinen, M.; Visser, H.; van Hinsbergh, V.W.M.; Helaakoski, T.; Kainulainen, T.; Rönkä, H.; et al. Matrix metalloproteinase-8 is expressed in rheumatoid synovial fibroblasts and endothelial cells. Regulation by tumor necrosis factor-alpha and doxycycline. J. Biol. Chem. 1997, 272, 31504–31509. [Google Scholar] [CrossRef] [Green Version]
- Herman, M.P.; Sukhova, G.K.; Libby, P.; Gerdes, N.; Tang, N.; Horton, D.B.; Kilbride, M.; Breitbart, R.E.; Chun, M.; Schönbeck, U. Expression of neutrophil collagenase (matrix metalloproteinase-8) in human atheroma: A novel collagenolytic pathway suggested by transcriptional profiling. Circulation 2001, 104, 1899–1904. [Google Scholar] [CrossRef] [Green Version]
- Juurikka, K.; Butler, G.S.; Salo, T.; Nyberg, P.; Åström, P. The Role of MMP8 in Cancer: A Systematic Review. Int. J. Mol. Sci. 2019, 20, 4506. [Google Scholar] [CrossRef] [Green Version]
- Moilanen, M.; Pirilä, E.; Grénman, R.; Sorsa, T.; Salo, T. Expression and regulation of collagenase-2 (MMP-8) in head and neck squamous cell carcinomas. J. Pathol. 2002, 197, 72–81. [Google Scholar] [CrossRef]
- Stadlmann, S.; Pollheimer, J.; Moser, P.L.; Raggi, A.; Amberger, A.; Margreiter, R.; Offner, F.; Mikuz, G.; Dirnhofer, S.; Moch, H. Cytokine-regulated expression of collagenase-2 (MMP-8) is involved in the progression of ovarian cancer. Eur. J. Cancer 2003, 39, 2499–2505. [Google Scholar] [CrossRef]
- Sirniö, P.; Tuomisto, A.; Tervahartiala, T.; Sorsa, T.; Klintrup, K.; Karhu, T.; Herzig, K.-H.; Mäkelä, J.; Karttunen, T.J.; Salo, T.; et al. High-serum MMP-8 levels are associated with decreased survival and systemic inflammation in colorectal cancer. Br. J. Cancer 2018, 119, 213–219. [Google Scholar] [CrossRef]
- Böckelman, C.; Beilmann-Lehtonen, I.; Kaprio, T.; Koskensalo, S.; Tervahartiala, T.; Mustonen, H.; Stenman, U.-H.; Sorsa, T.; Haglund, C. Serum MMP-8 and TIMP-1 predict prognosis in colorectal cancer. BMC Cancer 2018, 18, 679. [Google Scholar] [CrossRef]
- Laitinen, A.; Hagström, J.; Mustonen, H.; Kokkola, A.; Tervahartiala, T.; Sorsa, T.; Böckelman, C.; Haglund, C. Serum MMP-8 and TIMP-1 as prognostic biomarkers in gastric cancer. Tumour. Biol. 2018, 40, 1010428318799266. [Google Scholar] [CrossRef] [Green Version]
- Oberg, H.H.; Wesch, D.; Kalyan, S.; Kabelitz, D. Regulatory Interactions Between Neutrophils, Tumor Cells and T Cells. Front. Immunol. 2019, 10, 1690. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhang, W.; Yuan, X.; Fu, M.; Qian, H.; Xu, W. Neutrophils in cancer development and progression: Roles, mechanisms, and implications (Review). Int. J. Oncol. 2016, 49, 857–867. [Google Scholar] [CrossRef] [Green Version]
- Van Lint, P.; Libert, C. Matrix metalloproteinase-8: Cleavage can be decisive. Cytokine Growth Factor Rev. 2006, 17, 217–223. [Google Scholar] [CrossRef]
- Balbín, M.; Fueyo, A.; Tester, A.M.; Pendás, A.M.; Pitiot, A.S.; Astudillo, A.; Overall, C.M.; Shapiro, S.D.; López-Otín, C. Loss of collagenase-2 confers increased skin tumor susceptibility to male mice. Nat. Genet. 2003, 35, 252–257. [Google Scholar] [CrossRef]
- Landskron, G.; De la Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic inflammation and cytokines in the tumor microenvironment. J. Immunol. Res. 2014, 2014, 149185. [Google Scholar] [CrossRef] [Green Version]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef]
- Salmiheimo, A.; Mustonen, H.; Stenman, U.H.; Puolakkainen, P.; Kemppainen, E.; Seppänen, H.; Haglund, C. Systemic Inflammatory Response and Elevated Tumour Markers Predict Worse Survival in Resectable Pancreatic Ductal Adenocarcinoma. PLoS ONE 2016, 11, e0163064. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Fernández, A.; Fueyo, A.; Folgueras, A.R.; Garabaya, C.; Pennington, C.J.; Pilgrim, S.; Edwards, D.R.; Holliday, D.L.; Jones, J.L.; Span, P.N.; et al. Matrix metalloproteinase-8 functions as a metastasis suppressor through modulation of tumor cell adhesion and invasion. Cancer Res. 2008, 68, 2755–2763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Fernández, A.; Inada, M.; Balbín, M.; Fueyo, A.; Pitiot, A.S.; Astudillo, A.; Hirose, K.; Hirata, M.; Shapiro, S.D.; Noel, A.; et al. Increased inflammation delays wound healing in mice deficient in collagenase-2 (MMP-8). FASEB J. 2007, 21, 2580–2591. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.H.; Dean, R.A.; Roberts, C.R.; Overall, C.M. Matrix metalloproteinase processing of CXCL11/I-TAC results in loss of chemoattractant activity and altered glycosaminoglycan binding. J. Biol. Chem. 2008, 283, 19389–19399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, D.R.; Huttenlocher, A. Neutrophils in the Tumor Microenvironment. Trends Immunol. 2016, 37, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.J.; Hu, Z.G.; Shi, W.X.; Deng, T.; He, S.Q.; Yuan, S.G. Prognostic significance of neutrophil to lymphocyte ratio in pancreatic cancer: A meta-analysis. World J. Gastroenterol. 2015, 21, 2807–2815. [Google Scholar] [CrossRef]
- Padoan, A.; Plebani, M.; Basso, D. Inflammation and Pancreatic Cancer: Focus on Metabolism, Cytokines, and Immunity. Int. J. Mol. Sci. 2019, 20, 676. [Google Scholar] [CrossRef] [Green Version]
- Caruso, R.A.; Bellocco, R.; Pagano, M.; Bertoli, G.; Rigoli, L.; Inferrera, C. Prognostic value of intratumoral neutrophils in advanced gastric carcinoma in a high-risk area in northern Italy. Mod. Pathol. 2002, 15, 831–837. [Google Scholar] [CrossRef]
- Gunnarsson, U.; Strigård, K.; Edin, S.; Gkekas, I.; Mustonen, H.; Kaprio, T.; Böckelman, C.; Hagström, J.; Palmqvist, R.; Haglund, C. Association between local immune cell infiltration, mismatch repair status and systemic inflammatory response in colorectal cancer. J. Transl. Med. 2020, 18, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Reid, M.D.; Basturk, O.; Thirabanjasak, D.; Hruban, R.H.; Klimstra, D.S.; Bagci, P.; Altinel, D.; Adsay, V. Tumor-infiltrating neutrophils in pancreatic neoplasia. Mod. Pathol. 2011, 24, 1612–1619. [Google Scholar] [CrossRef]
- Hu, D.; Ansari, D.; Pawłowski, K.; Zhou, Q.; Sasor, A.; Welinder, C.; Kristl, T.; Bauden, M.; Rezeli, M.; Jiang, Y.; et al. Proteomic analyses identify prognostic biomarkers for pancreatic ductal adenocarcinoma. Oncotarget 2018, 9, 9789–9807. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.E.; Humphreys, M.J.; Campbell, F.; Neoptolemos, J.P.; Boyd, M.T. Comprehensive analysis of matrix metalloproteinase and tissue inhibitor expression in pancreatic cancer: Increased expression of matrix metalloproteinase-7 predicts poor survival. Clin. Cancer Res. 2004, 10, 2832–2845. [Google Scholar] [CrossRef] [Green Version]
- Lempinen, M.; Lyytinen, I.; Nordin, A.; Tervahartiala, T.; Mäkisalo, H.; Sorsa, T.; Isoniemi, H. Prognostic value of serum MMP-8, -9 and TIMP-1 in patients with hepatocellular carcinoma. Ann. Med. 2013, 45, 482–487. [Google Scholar] [CrossRef]
- Wang, Y.; Fang, T.; Huang, L.; Wang, H.; Zhang, L.; Wang, Z.; Cui, Y. Neutrophils infiltrating pancreatic ductal adenocarcinoma indicate higher malignancy and worse prognosis. Biochem. Biophys. Res. Commun. 2018, 501, 313–319. [Google Scholar] [CrossRef]
- Edin, S.; Kaprio, T.; Hagström, J.; Larsson, P.; Mustonen, H.; Böckelman, C.; Strigård, K.; Gunnarsson, U.; Haglund, C.; Palmqvist, R. The Prognostic Importance of CD20+ B lymphocytes in Colorectal Cancer and the Relation to Other Immune Cell subsets. Sci. Rep. 2019, 9, 19997–19998. [Google Scholar] [CrossRef]
- Tao, L.; Zhang, L.; Peng, Y.; Tao, M.; Li, G.; Xiu, D.; Yuan, C.; Ma, C.; Jiang, B. Preoperative neutrophil-to-lymphocyte ratio and tumor-related factors to predict lymph node metastasis in patients with pancreatic ductal adenocarcinoma (PDAC). Oncotarget 2016, 7, 74314–74324. [Google Scholar] [CrossRef] [Green Version]
- Abe, H.; Morikawa, T.; Saito, R.; Yamashita, H.; Seto, Y.; Fukayama, M. In Epstein-Barr virus-associated gastric carcinoma a high density of CD66b-positive tumor-associated neutrophils is associated with intestinal-type histology and low frequency of lymph node metastasis. Virchows Arch. 2016, 468, 539–548. [Google Scholar] [CrossRef]
- Allin, K.H.; Nordestgaard, B.G. Elevated C-reactive protein in the diagnosis, prognosis, and cause of cancer. Crit. Rev. Clin. Lab. Sci. 2011, 48, 155–170. [Google Scholar] [CrossRef]
- Saukkonen, K.; Hagström, J.; Mustonen, H.; Juuti, A.; Nordling, S.; Fermér, C.; Seppänen, H.; Haglund, C. Podocalyxin Is a Marker of Poor Prognosis in Pancreatic Ductal Adenocarcinoma. PLoS ONE 2015, 10, e0129012. [Google Scholar] [CrossRef] [Green Version]
- Prikk, K.; Maisi, P.; Pirilä, E.; Reintam, M.A.; Salo, T.; Sorsa, T.; Sepper, R. Airway obstruction correlates with collagenase-2 (MMP-8) expression and activation in bronchial asthma. Lab. Investig. 2002, 82, 1535–1545. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Cell MMP-8 | p Value | PMNs | p Value | CRP Levels | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Negative (0) | Positive (1–3) | Negative (0) | Positive (1–3) | Low (<10 mg/L) | High (≥10 mg/L) | ||||
| n (%) | 12 (8.5) | 129 (86.5) | 59 (41.8) | 82 (58.2) | 97 (78.2) | 27 (21.8) | |||
| Age, in years | 0.208 | 0.135 | 0.107 | ||||||
| <65 | 5 (7.2) | 64 (92.8) | 29 (42.0) | 40 (58.0) | 50 (82.0) | 11 (18.0) | |||
| ≥65 | 7 (9.7) | 65 (90.3) | 30 (41.7) | 42 (58.3) | 47 (74.6) | 16 (25.4) | |||
| Sex | 0.168 | 0.001 | 0.170 | ||||||
| Male | 8 (10.4) | 69 (89.6) | 41 (53.2) | 36 (46.8) | 55 (77.5) | 16 (22.5) | |||
| Female | 4 (6.3) | 60 (93.8) | 18 (28.1) | 46 (71.9) | 42 (79.2) | 11 (20.8) | |||
| T1 | 1 (7.1) | 13 (92.9) | 0.171 | 2 (14.3) | 12 (85.7) | 0.036 | 12 (100.0) | 0 (0.0) | |
| T2 | 7 (7.6) | 85 (92.4) | 41 (44.6) | 51 (55.4) | 63 (78.8) | 17 (21.2) | |||
| T3 | 4 (11.4) | 31 (88.6) | 16 (45.7) | 19 (54.3) | 22 (68.8) | 10 (31.2) | |||
| N0 | 4 (9.8) | 37 (90.2) | 0.163 | 10 (24.4) | 31 (75.6) | 0.003 | 28 (84.8) | 5 (15.2) | |
| N1 | 5 (7.5) | 62 (92.5) | 31 (46.3) | 36 (53.7) | 43 (72.9) | 16 (27.1) | |||
| N2 | 3 (9.1) | 30 (90.9) | 18 (54.5) | 15 (45.5) | 26 (81.3) | 6 (18.7) | |||
| Grade | 0.094 | 0.113 | |||||||
| 1 | 0 (0.0) | 15 (100.0) | 6 (40.0) | 9 (60.0) | 9 (75.0) | 3 (25.0) | |||
| 2 | 8 (8.9) | 82 (91.9) | 37 (41.1) | 53 (58.9) | 61 (76.3) | 19 (23.7) | |||
| 3 | 3 (13.0) | 20 (87.0) | 11 (47.8) | 12 (52.2) | 17 (81.0) | 4 (19.0) | |||
| Perineural invasion | 0.249 | 0.088 | |||||||
| No | 4 (9.1) | 40 (90.9) | 16 (36.4) | 28 (63.6) | |||||
| Yes | 8 (8.7) | 84 (91.3) | 42 (45.7) | 50 (54.3) | |||||
| Perivascular invasion | 0.266 | 0.010 | |||||||
| No | 9 (9.0) | 91 (91.0) | 37 (37.0) | 63 (63.0) | |||||
| Yes | 3 (8.1) | 34 (91.9) | 22 (59.5) | 15 (40.5) | |||||
| ASA score | 0.190 | 0.102 | |||||||
| 1 | 0 (0.0) | 3 (100.0) | 0 (0.0) | 3 (100.0) | 2 (66.7) | 1 (33.3) | |||
| 2 | 5 (12.2) | 36 (87.8) | 18 (43.9) | 23 (56.1) | 33 (84.6) | 6 (15.4) | |||
| 3 | 5 (9.8) | 46 (90.2) | 23 (45.1) | 28 (54.9) | 31 (68.9) | 14 (31.1) | |||
| 4 | 1 (20.0) | 4 (80.0) | 2 (40.0) | 3 (60.0) | 3 (75.0) | 1 (25.0) | |||
| CRP | 0.011 | 0.102 | |||||||
| <10 mg/L | 5 (5.2) | 92 (94.8) | 36 (37.1) | 61 (62.9) | |||||
| ≥10 mg/L | 6 (22.2) | 21 (77.8) | 13 (48.1) | 14 (51.9) | |||||
| Hazard Ratio | 95% CI | p Value | |
|---|---|---|---|
| Age | 1.16 | 0.81–1.66 | 0.420 |
| Sex | 0.87 | 0.60–1.24 | 0.431 |
| T1 | 1 (reference) | ||
| T2 | 1.16 | 0.63–2.13 | 0.641 |
| T3 | 1.52 | 0.78–2.97 | 0.223 |
| N0 | 1 (reference) | ||
| N1 | 1.47 | 0.95–2.28 | 0.084 |
| N2 | 2.62 | 1.59–4.33 | <0.001 |
| Grade | |||
| 1 | 1 (reference) | 0.486 | |
| 2 | 0.90 | 0.52–1.57 | 0.707 |
| 3 | 1.21 | 0.62–2.38 | 0.573 |
| Perivascular invasion | 1.71 | 1.14–2.55 | 0.009 |
| Perineural invasion | 1.06 | 0.72–1.55 | 0.773 |
| Adjuvant therapy | 0.88 | 0.62–1.26 | 0.485 |
| Tumour size | 1.32 | 0.92–1.89 | 0.132 |
| CA19-9 (kU/l, log10) | 1.28 | 1.08–1.53 | 0.006 |
| CRP ≥ 10 vs. <10 mg/L | 1.93 | 1.23–3.03 | 0.005 |
| MMP-8 = 1–3 vs. 0 | 0.43 | 0.24–0.79 | 0.006 |
| PMNs = 1–3 vs. 0 | 0.53 | 0.37–0.76 | 0.001 |
| MMP-8 = 1–3, CRP < 10 mg/L | 1 (reference) | 0.005 | |
| MMP-8 = 0, CRP < 10 mg/L | 1.98 | 0.80–4.94 | 0.141 |
| MMP-8 = 1–3, CRP ≥ 10 mg/L | 1.78 | 1.07–2.94 | 0.025 |
| MMP-8 = 0, CRP ≥ 10 mg/L | 3.45 | 1.49–8.01 | 0.004 |
| PMNs = 1–3, CRP < 10 mg/L | 1 (reference) | 0.001 | |
| PMNs = 0, CRP < 10 mg/L | 1.86 | 1.19–2.93 | 0.007 |
| PMNs = 1,2,3, CRP ≥ 10 mg/L | 2.06 | 1.10–3.87 | 0.025 |
| PMNs = 0, CRP ≥ 10 mg/L | 2.99 | 1.60–5.59 | 0.001 |
| Hazard Ratio | 95% CI | p Value | |
|---|---|---|---|
| Age | 1.43 | 0.93–2.20 | 0.101 |
| Sex | 1.05 | 0.67–1.66 | 0.829 |
| T1 | 1 (reference) | 0.317 | |
| T2 | 0.61 | 0.29–1.30 | 0.203 |
| T3 | 0.52 | 0.22–1.22 | 0.132 |
| N0 | 1 (reference) | 0.001 | |
| N1 | 1.96 | 1.09–3.53 | 0.025 |
| N2 | 4.00 | 1.98–8.10 | <0.001 |
| Perivascular invasion | 1.63 | 1.02–2.61 | 0.043 |
| Adjuvant therapy | 0.62 | 0.40–0.97 | 0.038 |
| CA19-9 (kU/l, log10) | 1.26 | 1.00–1.58 | 0.047 |
| CRP ≥ 10 vs. <10 mg/L | 2.25 | 1.34–3.76 | 0.002 |
| MMP-8 = 1–3 vs. 0 | 0.33 | 0.16–0.68 | 0.003 |
| PMNS = 1–3 vs. 0 | 0.75 | 0.48–1.16 | 0.196 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaasinen, M.; Hagström, J.; Mustonen, H.; Sorsa, T.; Sund, M.; Haglund, C.; Seppänen, H. Matrix Metalloproteinase 8 Expression in a Tumour Predicts a Favourable Prognosis in Pancreatic Ductal Adenocarcinoma. Int. J. Mol. Sci. 2022, 23, 3314. https://doi.org/10.3390/ijms23063314
Kaasinen M, Hagström J, Mustonen H, Sorsa T, Sund M, Haglund C, Seppänen H. Matrix Metalloproteinase 8 Expression in a Tumour Predicts a Favourable Prognosis in Pancreatic Ductal Adenocarcinoma. International Journal of Molecular Sciences. 2022; 23(6):3314. https://doi.org/10.3390/ijms23063314
Chicago/Turabian StyleKaasinen, Mirjami, Jaana Hagström, Harri Mustonen, Timo Sorsa, Malin Sund, Caj Haglund, and Hanna Seppänen. 2022. "Matrix Metalloproteinase 8 Expression in a Tumour Predicts a Favourable Prognosis in Pancreatic Ductal Adenocarcinoma" International Journal of Molecular Sciences 23, no. 6: 3314. https://doi.org/10.3390/ijms23063314