
Impact of Heated Tobacco Products, E-Cigarettes, and Cigarettes on Inflammation and Endothelial Dysfunction
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
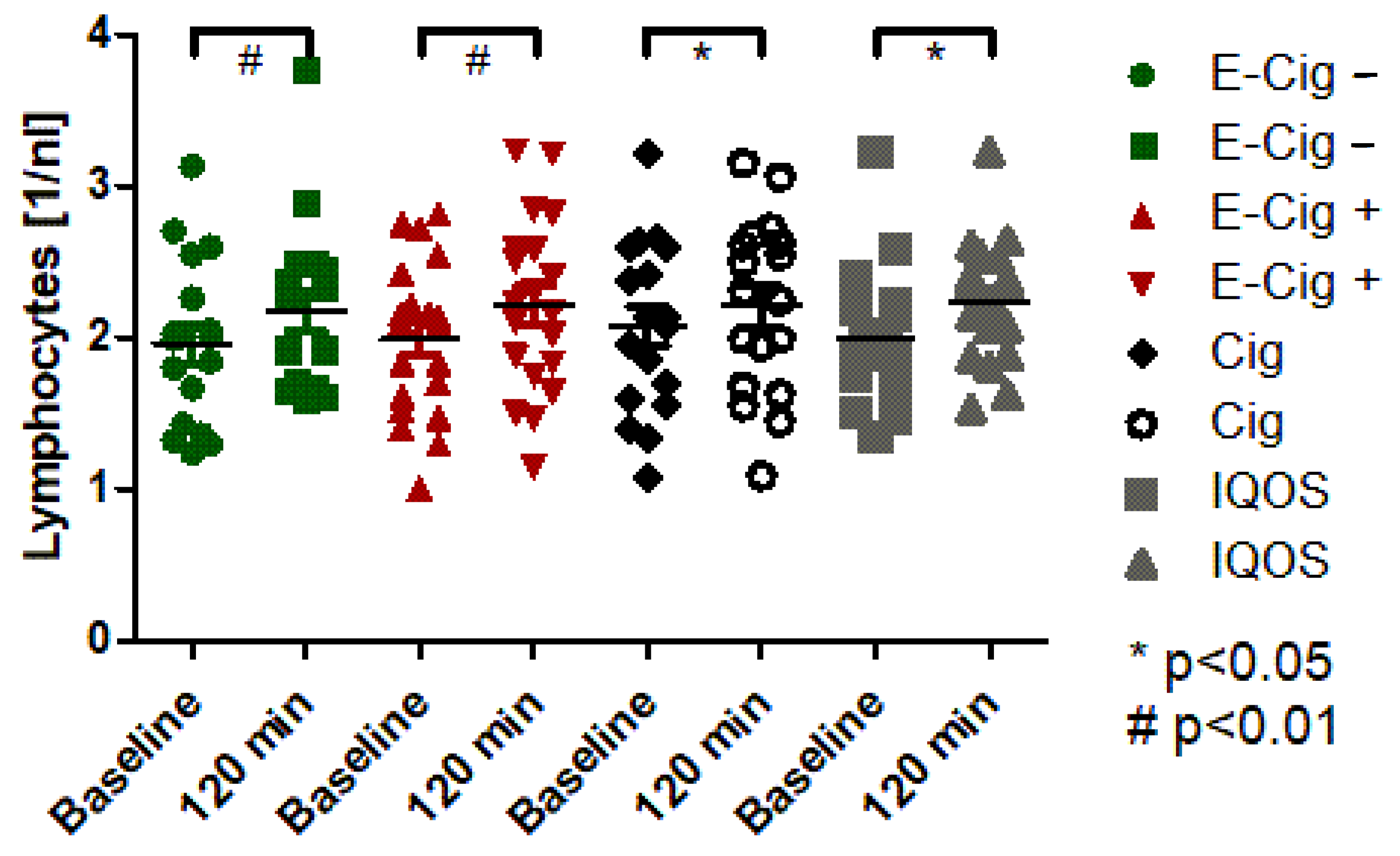
2.2. Cigarette, E-Cigarette, and HTPs Increased Leukocytes and Lymphocytes
2.3. Cigarette, E-Cigarette, and HTPs Increased Inflammation Values
2.4. Inflammation Due to Smoking and Vaping Causes Endothelial Dysfunction
2.5. Clinical Correlation of Inflammation, Endothelial Dysfunction, and Arterial Stiffness
3. Discussion
4. Materials and Methods
4.1. Study Cohort and Design
4.2. Measurement of Inflammation Markers, Endothelial Dysfunction, and Arterial Stiffness
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, W.H.; Ong, S.-G.; Zhou, Y.; Tian, L.; Bae, H.R.; Baker, N.; Whitlatch, A.; Mohammadi, L.; Guo, H.; Nadeau, K.C.; et al. Modeling Cardiovascular Risks of E-Cigarettes with Human Induced Pluripotent Stem Cell-Derived Endothelial Cells. J. Am. Coll. Cardiol. 2019, 73, 2722. [Google Scholar] [CrossRef] [PubMed]
- Gassmann, R.; Kaldewai, D.; Lindemann, F. Jahrbuch Sucht 2009; Neuland Verlagsgesellschaft: Hamm, Germany, 2009. [Google Scholar]
- Lampert, T.; von der Lippe, E.; Müters, S. Prevalence of Smoking in the Adult Population of Germany: Results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 802–808. [Google Scholar] [CrossRef] [PubMed]
- DEBRA Study–Deutsche Befragung zum Rauchverhalten|German Study on Tobacco Use. Available online: https://www.debra-study.info/ (accessed on 22 February 2023).
- The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Available online: https://pubmed.ncbi.nlm.nih.gov/24455788/ (accessed on 22 February 2023).
- Commissioner, O. of the FDA Denies Authorization to Market JUUL Products. Available online: https://www.fda.gov/news-events/press-announcements/fda-denies-authorization-market-juul-products (accessed on 5 May 2023).
- Mallock, N.; Pieper, E.; Hutzler, C.; Henkler-Stephani, F.; Luch, A. Heated Tobacco Products: A Review of Current Knowledge and Initial Assessments. Front. Public Health 2019, 7, 287. [Google Scholar] [CrossRef] [PubMed]
- RKI-GEDA: Gesundheit in Deutschland Aktuell–GEDA 2014/2015-EHIS: Ergebnisse Im Journal of Healh Monitoring. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Studien/Geda/geda2014_einzelbeitraege_inhalt.html (accessed on 22 February 2023).
- Castaldelli-Maia, J.M.; Ventriglio, A.; Bhugra, D. Tobacco Smoking: From “glamour” to “Stigma”. A Comprehensive Review. Psychiatry Clin. Neurosci. 2016, 70, 24–33. [Google Scholar] [CrossRef]
- Neubauer, S.; Welte, R.; Beiche, A.; Koenig, H.-H.; Buesch, K.; Leidl, R. Mortality, Morbidity and Costs Attributable to Smoking in Germany: Update and a 10-Year Comparison. Tob. Control 2006, 15, 464–471. [Google Scholar] [CrossRef]
- Zhu, S.-H.; Sun, J.Y.; Bonnevie, E.; Cummins, S.E.; Gamst, A.; Yin, L.; Lee, M. Four Hundred and Sixty Brands of E-Cigarettes and Counting: Implications for Product Regulation. Tob. Control 2014, 23 (Suppl. 3), iii3–iii9. [Google Scholar] [CrossRef]
- Haustein, K.-O. (Ed.) Tabakabhängigkeit; Springer: Berlin/Heidelberg, Germany, 2008; ISBN 978-3-540-73308-9. [Google Scholar]
- Münzel, T. Endotheliale Dysfunktion: Pathophysiologie, Diagnostik und prognostische Bedeutung. Dtsch. Med. Wochenschr. 2008, 133, 2465–2470. [Google Scholar] [CrossRef]
- Nabavizadeh, P.; Liu, J.; Havel, C.M.; Ibrahim, S.; Derakhshandeh, R.; Iii, P.J.; Springer, M.L. Vascular Endothelial Function Is Impaired by Aerosol from a Single IQOS HeatStick to the Same Extent as by Cigarette Smoke. Tob. Control 2018, 27, 1161–1169. [Google Scholar] [CrossRef]
- Jauss, M.; Sitzer, M.; Stolz, E.; Misselwitz, B.; Rosenow, F. Lack of Increase of Cerebrovascular Events during German World Cup Soccer Games in 2006. J. Neurol. 2009, 256, 863–866. [Google Scholar] [CrossRef]
- van Popele, N.M.; Grobbee, D.E.; Bots, M.L.; Asmar, R.; Topouchian, J.; Reneman, R.S.; Hoeks, A.P.; van der Kuip, D.A.; Hofman, A.; Witteman, J.C. Association between Arterial Stiffness and Atherosclerosis: The Rotterdam Study. Stroke 2001, 32, 454–460. [Google Scholar] [CrossRef]
- Sutton-Tyrrell, K.; Najjar, S.S.; Boudreau, R.M.; Venkitachalam, L.; Kupelian, V.; Simonsick, E.M.; Havlik, R.; Lakatta, E.G.; Spurgeon, H.; Kritchevsky, S.; et al. Elevated Aortic Pulse Wave Velocity, a Marker of Arterial Stiffness, Predicts Cardiovascular Events in Well-Functioning Older Adults. Circulation 2005, 111, 3384–3390. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Wang, N.; Palmisano, J.N.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S. Hemodynamic Correlates of Blood Pressure across the Adult Age Spectrum: Noninvasive Evaluation in the Framingham Heart Study. Circulation 2010, 122, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Baulmann, J.; Nürnberger, J.; Slany, J.; Schmieder, R.; Schmidt-Trucksäss, A.; Baumgart, D.; Cremerius, P.; Hess, O.; Mortensen, K.; Weber, T. Arterielle Gefäßsteifigkeit und Pulswellenanalyse. Dtsch. Med. Wochenschr. 2010, 135, S4–S14. [Google Scholar] [CrossRef]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef] [PubMed]
- DuPont, J.J.; Kenney, R.M.; Patel, A.R.; Jaffe, I.Z. Sex Differences in Mechanisms of Arterial Stiffness. Br. J. Pharmacol. 2019, 176, 4208–4225. [Google Scholar] [CrossRef] [PubMed]
- Higham, A.; Bostock, D.; Booth, G.; Dungwa, J.V.; Singh, D. The Effect of Electronic Cigarette and Tobacco Smoke Exposure on COPD Bronchial Epithelial Cell Inflammatory Responses. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 989–1000. [Google Scholar] [CrossRef]
- Scott, A.; Lugg, S.T.; Aldridge, K.; Lewis, K.E.; Bowden, A.; Mahida, R.Y.; Grudzinska, F.S.; Dosanjh, D.; Parekh, D.; Foronjy, R.; et al. Pro-Inflammatory Effects of e-Cigarette Vapour Condensate on Human Alveolar Macrophages. Thorax 2018, 73, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.C.; Sapey, E.; Thickett, D.R.; Scott, A. Predicting the Pulmonary Effects of Long-Term e-Cigarette Use: Are the Clouds Clearing? Eur. Respir. Rev. 2022, 31, 210121. [Google Scholar] [CrossRef]
- Sawa, M.; Ushiyama, A.; Inaba, Y.; Hattori, K. Increased Oxidative Stress and Effects on Inflammatory Cytokine Secretion by Heated Tobacco Products Aerosol Exposure to Mice. Biochem. Biophys. Res. Commun. 2022, 610, 43–48. [Google Scholar] [CrossRef]
- Ridker, P.M.; MacFadyen, J.G.; Everett, B.M.; Libby, P.; Thuren, T.; Glynn, R.J.; Kastelein, J.; Koenig, W.; Genest, J.; Lorenzatti, A.; et al. Relationship of C-Reactive Protein Reduction to Cardiovascular Event Reduction Following Treatment with Canakinumab: A Secondary Analysis from the CANTOS Randomised Controlled Trial. Lancet 2018, 391. [Google Scholar] [CrossRef]
- Pm, R. From C-Reactive Protein to Interleukin-6 to Interleukin-1: Moving Upstream To Identify Novel Targets for Atheroprotection. Circ. Res. 2016, 118. [Google Scholar] [CrossRef]
- Ouyang, Y.; Virasch, N.; Hao, P.; Aubrey, M.T.; Mukerjee, N.; Bierer, B.E.; Freed, B.M. Suppression of Human IL-1β, IL-2, IFN-γ, and TNF-α Production by Cigarette Smoke Extracts. J. Allergy Clin. Immunol. 2000, 106, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Messner, B.; Bernhard, D. Smoking and Cardiovascular Disease: Mechanisms of Endothelial Dysfunction and Early Atherogenesis. Arter. Thromb. Vasc. Biol. 2014, 34, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, R.; Sciarretta, S.; Violi, F.; Nocella, C.; Loffredo, L.; Perri, L.; Peruzzi, M.; Marullo, A.G.M.; De Falco, E.; Chimenti, I.; et al. Acute Impact of Tobacco vs Electronic Cigarette Smoking on Oxidative Stress and Vascular Function. Chest 2016, 150, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Georgakopoulos, D.; Bull, C.; Thomas, O.; Robinson, J.; Deanfield, J.E. Cigarette Smoking Is Associated with Dose-Related and Potentially Reversible Impairment of Endothelium-Dependent Dilation in Healthy Young Adults. Circulation 1993, 88, 2149–2155. [Google Scholar] [CrossRef]
- Nakamura, K.; Barzi, F.; Lam, T.-H.; Huxley, R.; Feigin, V.L.; Ueshima, H.; Woo, J.; Gu, D.; Ohkubo, T.; Lawes, C.M.M.; et al. Cigarette Smoking, Systolic Blood Pressure, and Cardiovascular Diseases in the Asia-Pacific Region. Stroke 2008, 39, 1694–1702. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Lowe, G.D.O.; Shaper, A.G.; Rumley, A.; Lennon, L.; Whincup, P.H. Associations between Cigarette Smoking, Pipe/Cigar Smoking, and Smoking Cessation, and Haemostatic and Inflammatory Markers for Cardiovascular Disease. Eur. Heart J. 2005, 26, 1765–1773. [Google Scholar] [CrossRef]
- Wassertheurer, S.; Kropf, J.; Weber, T.; van der Giet, M.; Baulmann, J.; Ammer, M.; Hametner, B.; Mayer, C.C.; Eber, B.; Magometschnigg, D. A New Oscillometric Method for Pulse Wave Analysis: Comparison with a Common Tonometric Method. J. Hum. Hypertens. 2010, 24, 498–504. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H.; et al. Expert Consensus Document on Arterial Stiffness: Methodological Issues and Clinical Applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | All (n = 20) | Male (n = 10) | Female (n = 10) | p-Value |
|---|---|---|---|---|
| Age (years) | 21.9 ± 2.6 | 21.5 ± 2.3 | 22.2 ± 2.9 | 0.79 |
| Weight (kg) | 72.3 ± 12.1 | 79.6 ± 11.0 | 64.9 ± 8.3 | 0.0109 |
| Height (m) | 1.76 ± 0.1 | 1.84 ± 0.1 | 1.68 ± 0.1 | 0.0099 |
| BMI (kg/m2) | 23.3 ± 1.9 | 23.5 ± 1.5 | 23.1 ± 2.2 | 0.8132 |
| Waist (m) | 0.795 ± 0.08 | 0.839 ± 0.067 | 0.751 ± 0.068 | 0.0354 |
| Hip (m) | 0.971 ± 0.07 | 0.99 ± 0.058 | 0.951 ± 0.0.8 | 0.5452 |
| Cigarettes per day | 1.9 ± 0.8 | 2.6 ± 0.7 | 1.6 ± 0.4 | 0.3228 |
| Fagerström Test for Nicotine Dependence (points) | 1.1 ± 0.4 | 0.9 ± 0.3 | 0.2 ± 0.1 | 0.1459 |
| Sex | All (n = 20) | Male (n = 10) | Female (n = 10) | p-Value |
|---|---|---|---|---|
| Age (years) | 25.2 ± 0.9 | 25.6 ± 0.4 | 24.7 ± 0.3 | 0.6063 |
| Weight (kg) | 78.2 ± 3.5 | 85.9 ± 1.9 | 68.8 ± 0.8 | 0.0104 |
| Height (m) | 1.76 ± 0.02 | 1.8 ± 0.0 | 1.7 ± 0.0 | 0.0040 |
| BMI (kg/m2) | 25.0 ± 0.8 | 25.9 ± 0.4 | 24.0 ± 0.2 | 0.2180 |
| Waist (m) | 0.821 ± 0.02 | 0.861 ± 0.07 | 0.771 ± 0.07 | 0.0181 |
| Hip (m) | 0.929 ± 0.02 | 0.935 ± 0.1 | 0.92 ± 0.07 | 0.7155 |
| Cigarettes per day | 2.1 ± 0.7 | 2.7 ± 0.1 | 1.2 ± 0.2 | 0.2832 |
| Fagerström Test for Nicotine Dependence (points) | 0.5 ± 0.2 | 0.8 ± 0.1 | 0.1 ± 0.0 | 0.1180 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belkin, S.; Benthien, J.; Axt, P.N.; Mohr, T.; Mortensen, K.; Weckmann, M.; Drömann, D.; Franzen, K.F. Impact of Heated Tobacco Products, E-Cigarettes, and Cigarettes on Inflammation and Endothelial Dysfunction. Int. J. Mol. Sci. 2023, 24, 9432. https://doi.org/10.3390/ijms24119432
Belkin S, Benthien J, Axt PN, Mohr T, Mortensen K, Weckmann M, Drömann D, Franzen KF. Impact of Heated Tobacco Products, E-Cigarettes, and Cigarettes on Inflammation and Endothelial Dysfunction. International Journal of Molecular Sciences. 2023; 24(11):9432. https://doi.org/10.3390/ijms24119432
Chicago/Turabian StyleBelkin, Svenja, Julia Benthien, Paul Niklas Axt, Theresa Mohr, Kai Mortensen, Markus Weckmann, Daniel Drömann, and Klaas Frederik Franzen. 2023. "Impact of Heated Tobacco Products, E-Cigarettes, and Cigarettes on Inflammation and Endothelial Dysfunction" International Journal of Molecular Sciences 24, no. 11: 9432. https://doi.org/10.3390/ijms24119432
APA StyleBelkin, S., Benthien, J., Axt, P. N., Mohr, T., Mortensen, K., Weckmann, M., Drömann, D., & Franzen, K. F. (2023). Impact of Heated Tobacco Products, E-Cigarettes, and Cigarettes on Inflammation and Endothelial Dysfunction. International Journal of Molecular Sciences, 24(11), 9432. https://doi.org/10.3390/ijms24119432