
BDNF and Cognitive Function in Chilean Schizophrenic Patients

 ,
,
Abstract
1. Introduction
2. Results
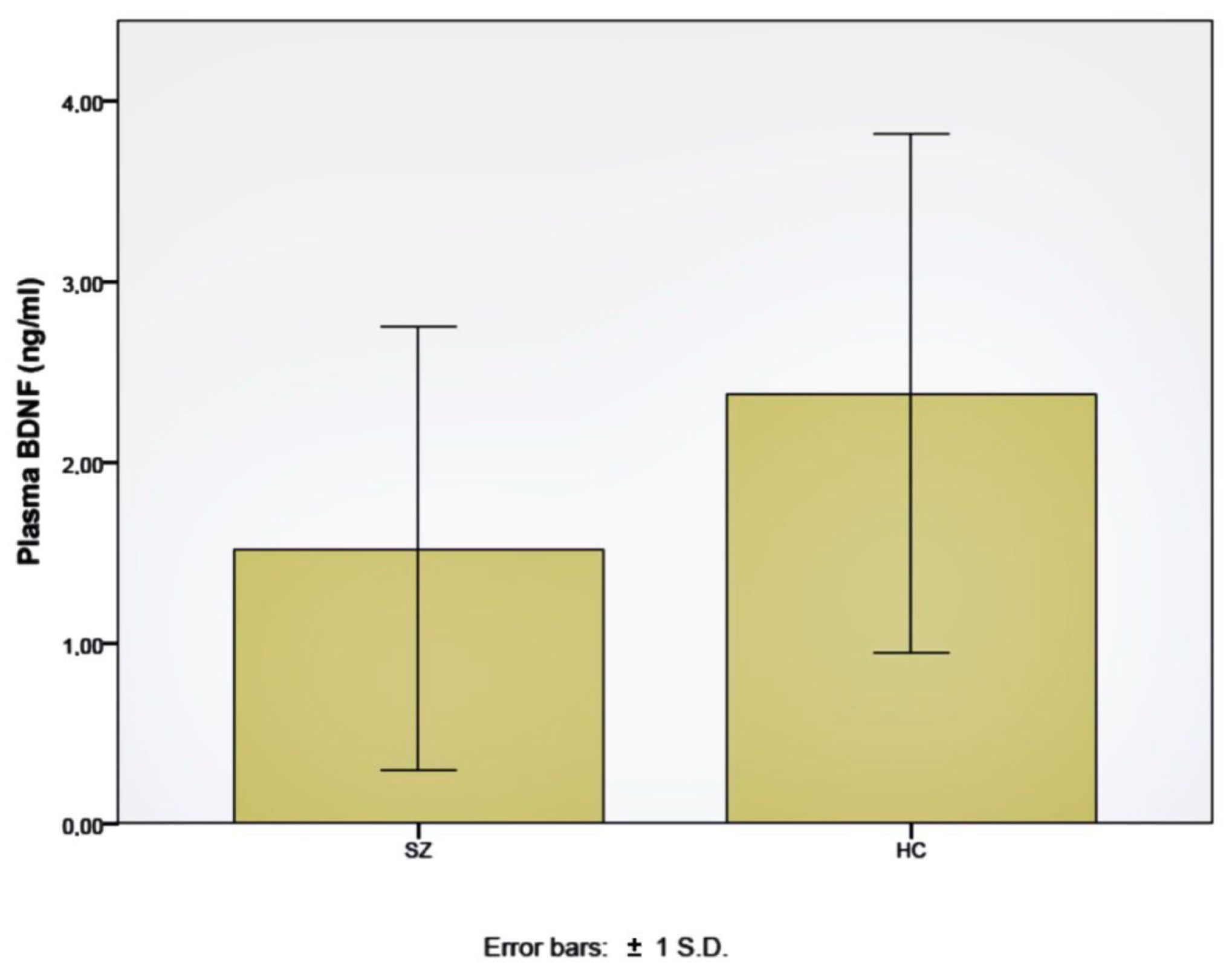
2.1. BDNF Plasma Levels
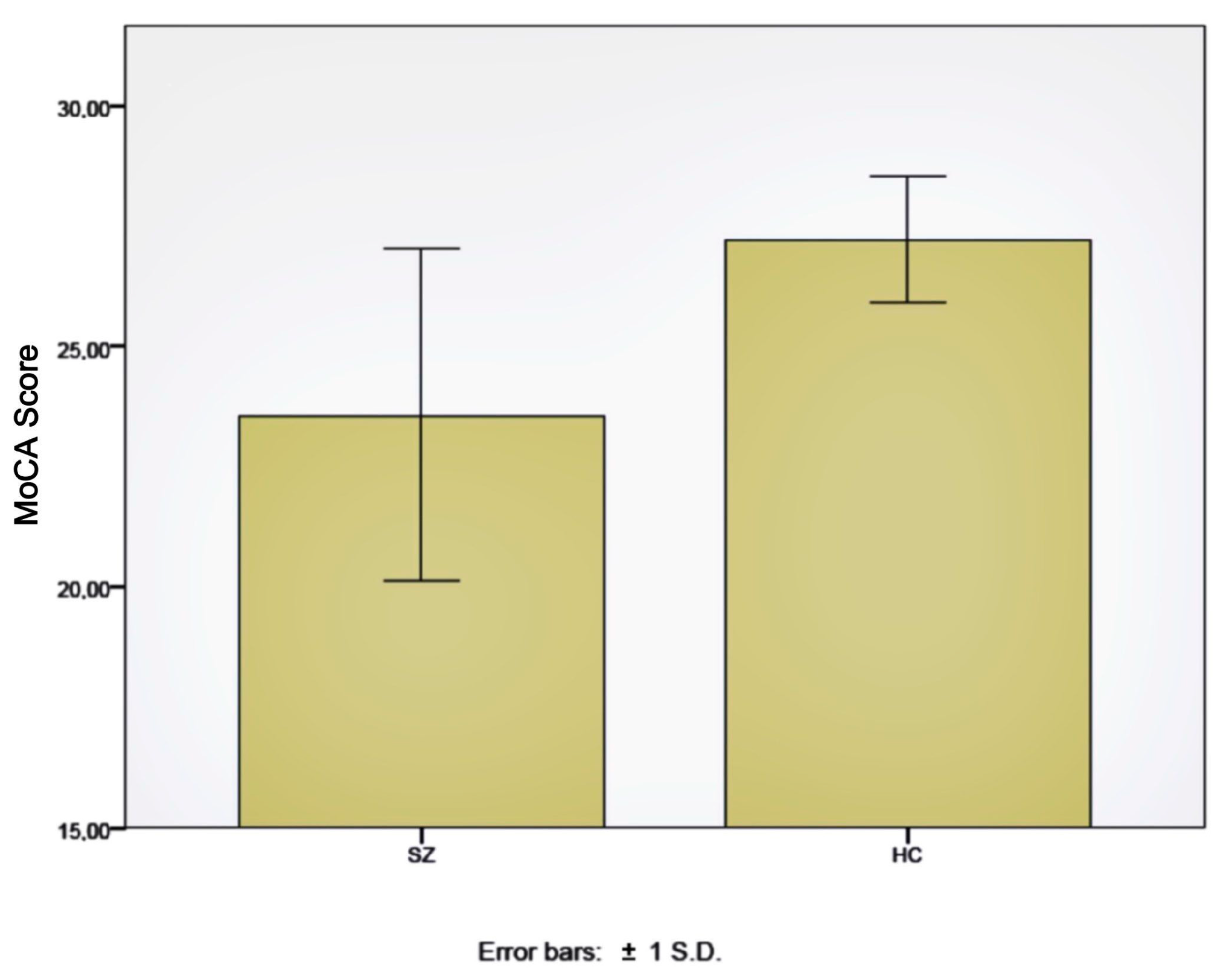
2.2. Cognitive Assessments
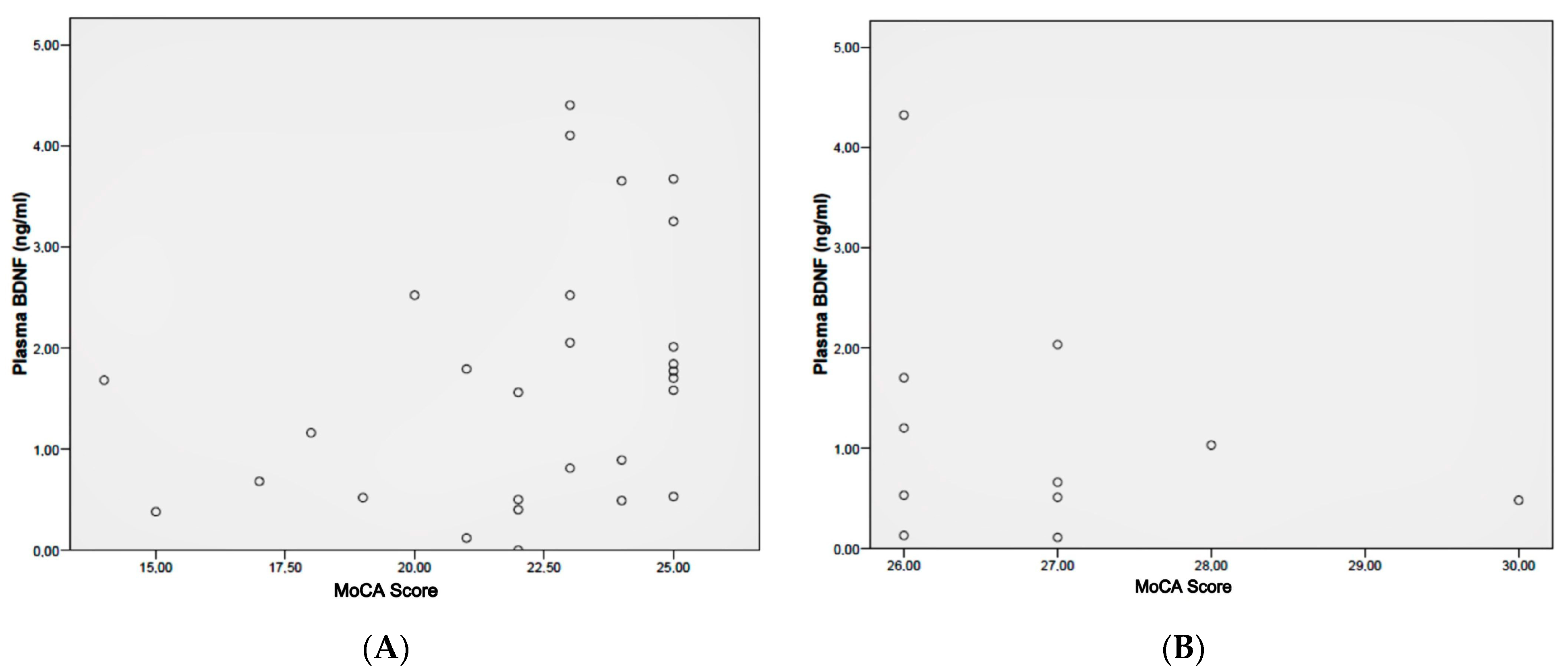
2.3. Correlation between BDNF Levels and Cognitive Assessments
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Clinical and Cognitive Assessments
4.3. BDNF Levels Measurements
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Owen, M.J.; Sawa, A.; Mortensen, P.B. Schizophrenia. Lancet 2016, 388, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Kahn, R.S.; Sommer, I.E.; Murray, R.M.; Meyer-Lindenberg, A.; Weinberger, D.R.; Cannon, T.D.; O’Donovan, M.; Correll, C.U.; Kane, J.M.; van Os, J.; et al. Schizophrenia. Nat. Rev. Dis. Prim. 2015, 1, 15067. [Google Scholar] [CrossRef]
- Schaefer, J.; Giangrande, E.; Weinberger, D.R.; Dickinson, D. The global cognitive impairment in schizophrenia: Consistent over decades and around the world. Schizophr. Res. 2013, 150, 42–50. [Google Scholar] [CrossRef]
- Green, M.F. What are the functional consequences of neurocognitive deficits in schizophrenia? Am. J. Psychiatry 1996, 153, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.S.; Almasy, L.; Gur, R.C.; Prasad, K.; Roalf, D.R.; Gur, R.E.; Nimgaonkar, V.L.; Pogue-Geile, M.F. Cognition and community functioning in schizophrenia: The nature of the relationship. J. Abnorm. Psychol. 2018, 127, 216–227. [Google Scholar] [CrossRef] [PubMed]
- McCleery, A.; Nuechterlein, K.H. Cognitive impairment in psychotic illness: Prevalence, profile of impairment, developmental course, and treatment considerations. Dialogues Clin. Neurosci. 2019, 21, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Czepielewski, L.S.; Alliende, L.M.; Castañeda, C.P.; Castro, M.; Guinjoan, S.M.; Massuda, R.; Berberian, A.A.; Fonseca, A.O.; Gadelha, A.; Bressan, R.; et al. Effects of socioeconomic status in cognition of people with schizophrenia: Results from a Latin American collaboration network with 1175 subjects. Psychol. Med. 2022, 52, 2177–2188. [Google Scholar] [CrossRef]
- Nieto, R.; Kukuljan, M.; Silva, H. BDNF and schizophrenia: From neurodevelopment to neuronal plasticity, learning, and memory. Front. Psychiatry 2013, 4, 45. [Google Scholar] [CrossRef]
- Penadés, R.; Garcia-Rizo, C.; Bioque, M.; González-Rodríguez, A.; Cabrera, B.; Mezquida, G.; Bernardo, M. The search for new biomarkers for cognition in schizophrenia. Schizophr. Res. Cogn. 2015, 2, 172–178. [Google Scholar] [CrossRef]
- Nieto, R.R.; Carrasco, A.; Corral, S.; Castillo, R.; Gaspar, P.A.; Bustamante, M.L.; Silva, H. BDNF as a Biomarker of Cognition in Schizophrenia/Psychosis: An Updated Review. Front. Psychiatry 2021, 12, 662407. [Google Scholar] [CrossRef]
- Vicario-Abejón, C.; Owens, D.; McKay, R.; Segal, M. Role of neurotrophins in central synapse formation and stabilization. Nat. Rev. Neurosci. 2002, 3, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Poo, M. Neurotrophins as synaptic modulators. Nat. Rev. Neurosci. 2001, 2, 24–32. [Google Scholar] [CrossRef]
- Chao, M. Neurotrophins and their receptors: A convergence point for many signaling pathways. Nat. Rev. Neurosci. 2003, 4, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Aicardi, G.; Argilli, E.; Cappello, S.; Santi, S.; Riccio, M.; Thoenen, H.; Canossa, M. Induction of long-term potentiation and depression is reflected by corresponding changes in secretion of endogenous brain-derived neurotrophic factor. Proc. Natl. Acad. Sci. USA 2004, 101, 15788–15792. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Silva, A. The molecular and cellular biology of enhanced cognition. Nat. Rev. Neurosci. 2009, 10, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Gorski, J.A.; Balogh, S.A.; Wehner, J.M.; Jones, K.R. Learning deficits in forebrain-restricted brain-derived neurotrophic factor mutant mice. Neuroscience 2003, 121, 341–354. [Google Scholar] [CrossRef]
- Lu, B.; Pang, P.; Woo, N. The yin and yang of neurotrophin action. Nat. Rev. Neurosci. 2005, 6, 603–614. [Google Scholar] [CrossRef]
- Ross, C.; Margolis, R.; Reading, S.; Plenikov, M.; Coyle, J. Neurobiology of schizophrenia. Neuron 2006, 52, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Buckley, P.; Mahadik, S.; Pillai, A.; Terry, A. Neurotrophins and schizophrenia. Schizophr. Res. 2007, 94, 1–11. [Google Scholar] [CrossRef]
- Favalli, G.; Li, J.; Belmonte-de-Abreu, P.; Wong, A.H.; Daskalakis, Z.J. The role of BDNF in the pathophysiology and treatment of schizophrenia. J. Psychiatr. Res. 2012, 46, 1–11. [Google Scholar] [CrossRef]
- Green, M.J.; Matheson, S.L.; Shepherd, A.; Weickert, C.S.; Carr, V.J. Brain-derived neurotrophic factor levels in schizophrenia: A systematic review with meta-analysis. Mol. Psychiatry 2011, 16, 960–972. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Liang, J.; Chen, D.C.; Xiu, M.H.; De Yang, F.; Kosten, T.A.; Kosten, T.R. Low BDNF is associated with cognitive impairment in chronic patients with schizophrenia. Psychopharmacology 2012, 222, 277–284. [Google Scholar] [CrossRef] [PubMed]
- De Azua, S.; Matute, C.; Stertz, L.; Mosquera, F.; Palomino, A.; De la Rosa, I.; Barbeito, S.; Vega, P.; Kapczinski, F.; González-Pinto, A. Plasma brain-derived neurotrophic factor levels learning capacity and cognition in patients with first episode psychosis. BMC Psychiatry 2013, 13, 27. [Google Scholar] [CrossRef]
- Asevedo, E.; Gadelha, A.; Noto, C.; Mansur, R.B.; Zugman, A.; Belangero, S.I.; Berberian, A.A.; Scarpato, B.S.; Leclerc, E.; Teixeira, A.L.; et al. Impact of peripheral levels of chemokines, BDNF and oxidative markers on cognition in individuals with schizophrenia. J. Psychiatr. Res. 2013, 47, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Niitsu, T.; Shirayama, Y.; Matsuzawa, D.; Hasegawa, T.; Kanahara, N.; Hashimoto, T.; Shiraishi, T.; Shiina, A.; Fukami, G.; Fujisaki, M.; et al. Associations of serum brainderived neurotrophic factor with cognitive impairments and negative symptoms in schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 1836–1840. [Google Scholar] [CrossRef]
- Ahmed, A.O.; Mantini, A.M.; Fridberg, D.J.; Buckley, P.F. Brain-derived neurotrophic factor (BDNF) and neurocognitive deficits in people with schizophrenia: A meta-analysis. Psychiatry Res. 2015, 226, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bora, E. Peripheral inflammatory and neurotrophic biomarkers of cognitive impairment in schizophrenia: A meta-analysis. Psychol. Med. 2019, 49, 1971–1979. [Google Scholar] [CrossRef]
- Pan, W.; Banks, W.A.; Fasold, M.B.; Bluth, J.; Kastin, A.J. Transport of brain-derived neurotrophic factor across the blood-brain barrier. Neuropharmacology 1998, 37, 1553–1561. [Google Scholar] [CrossRef]
- Pillai, A.; Kale, A.; Joshi, S.; Naphade, N.; Raju, M.S.V.K.; Nasrallah, H.; Mahadik, S.P. Decreased BDNF levels in CSF of drug-naive first-episode psychotic subjects: Correlation with plasma BDNF and psychopathology. Int. J. Neuropsychopharmacol. 2010, 13, 535–539. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Durany, N.; Thome, J. Neurotrophic factors and the pathophysiology of schizophrenic psychoses. Eur. Psychiatry 2004, 19, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Shoval, H.; Weizman, A. The possible role of neurotrophins in the pathogenesis and therapy of schizophrenia. Eur. Neuropsychopharmacol. 2005, 15, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.O.; Kramer, S.; Hofman, N.; Flynn, J.; Hansen, M.; Martin, V.; Pillai, A.; Buckley, P.F. A Meta-Analysis of Brain-Derived Neurotrophic Factor Effects on Brain Volume in Schizophrenia: Genotype and Serum Levels. Neuropsychobiology 2021, 80, 411–424. [Google Scholar] [CrossRef]
- Korte, M.; Griesbeck, O.; Gravel, C.; Carroll, P.; Staiger, V.; Thoenen, H.; Bonhoeffer, T. Virus-mediated gene transfer into hippocampal CA1 region restores long-term potentiation in brain-derived neurotrophic factor mutant mice. Proc. Natl. Acad. Sci. USA 1996, 93, 12547–12552. [Google Scholar] [CrossRef] [PubMed]
- Rizos, E.; Papathanasiou, M.; Michalopoulou, P.; Mazioti, A.; Douzenis, A.; Kastania, A.; Nikolaidou, P.; Laskos, E.; Vasilopoulou, K.; Lykouras, L. Association of serum BDNF levels with hippocampal volumes in first psychotic episode drug-naïve schizophrenic patients. Schizophr. Res. 2011, 129, 201–204. [Google Scholar] [CrossRef]
- Green, M.F.; Nuechterlein, K.H. The MATRICS initiative: Developing a consensus cognitive battery for clinical trials. Schizophr. Res. 2004, 72, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Haddad, C.; Salameh, P.; Sacre, H.; Clément, J.-P.; Calvet, B. The use of the Montreal Cognitive Assessment (MoCA) screening tool to evaluate cognitive deficits in Lebanese in-patients with schizophrenia. Asian J. Psychiatr. 2022, 70, 103029. [Google Scholar] [CrossRef]
- Elfving, B.; Plougmann, P.H.; Wegener, G. Detection of brain-derived neurotrophic factor (BDNF) in rat blood and brain preparations using ELISA: Pitfalls and solutions. J. Neurosci. Methods 2010, 187, 73–77. [Google Scholar] [CrossRef]
- Biagianti, B.; Castellaro, G.A.; Brambilla, P. Predictors of response to cognitive remediation in patients with major psychotic disorders: A narrative review. J. Affect. Disord. 2021, 281, 264–270. [Google Scholar] [CrossRef]
- Di Carlo, P.; Punzi, G.; Ursini, G. Brain-derived neurotrophic factor and schizophrenia. Psychiatr. Genet. 2019, 29, 200–210. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Schizophrenia | Healthy Subjects | |
|---|---|---|
| n | 40 | 14 |
| Gender (M/F) | 34/6 | 10/4 |
| Age | 22.7 (±4.7) | 23.8 (±3.5) |
| Years of education | 12.4 (±2.2) | 15.9 (±2.1) |
| Age of onset | 20.1 (±3.2) | - |
| Years since onset | 2.7 (±3.2) | - |
| Ever hospitalized | 19/40 (47.5%) | - |
| SGA treatment | 37 (92.5%) | - |
| Antidepressants | 9 (22.5%) | - |
| PANSS score | 70.04 (±31.5) | - |
| BDI score | 11.45 (±10.3) | - |
| CGI score | 2.84 (±1.2) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nieto, R.R.; Silva, H.; Armijo, A.; Nachar, R.; González, A.; Castañeda, C.P.; Montes, C.; Kukuljan, M. BDNF and Cognitive Function in Chilean Schizophrenic Patients. Int. J. Mol. Sci. 2023, 24, 10569. https://doi.org/10.3390/ijms241310569
Nieto RR, Silva H, Armijo A, Nachar R, González A, Castañeda CP, Montes C, Kukuljan M. BDNF and Cognitive Function in Chilean Schizophrenic Patients. International Journal of Molecular Sciences. 2023; 24(13):10569. https://doi.org/10.3390/ijms241310569
Chicago/Turabian StyleNieto, Rodrigo R., Hernán Silva, Alejandra Armijo, Rubén Nachar, Alfonso González, Carmen Paz Castañeda, Cristián Montes, and Manuel Kukuljan. 2023. "BDNF and Cognitive Function in Chilean Schizophrenic Patients" International Journal of Molecular Sciences 24, no. 13: 10569. https://doi.org/10.3390/ijms241310569
APA StyleNieto, R. R., Silva, H., Armijo, A., Nachar, R., González, A., Castañeda, C. P., Montes, C., & Kukuljan, M. (2023). BDNF and Cognitive Function in Chilean Schizophrenic Patients. International Journal of Molecular Sciences, 24(13), 10569. https://doi.org/10.3390/ijms241310569