
Building Bricks of Integrated Care Pathway for Autism Spectrum Disorder: A Systematic Review
 ,
,
Abstract
:1. Introduction
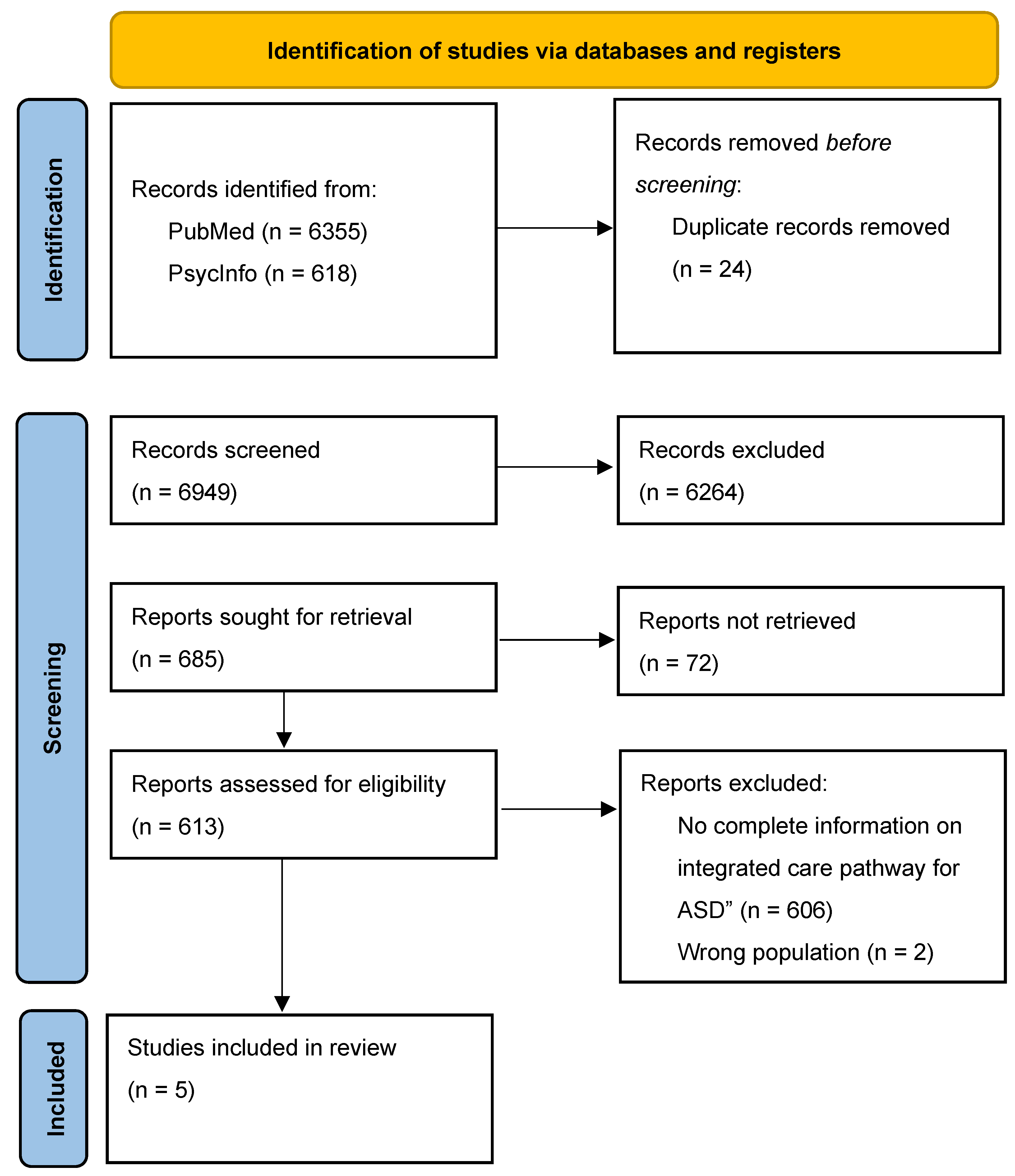
2. Materials and Methods
2.1. International Literature Review
- Description of a structured and stepped multidisciplinary plan of care with timeframes or criteria-based progression from referral to care management and post-diagnosis support.
- Population with a diagnosis of ASD, Asperger Syndrome, Child Development Disorders or Pervasive Developmental Disorder performed using the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) [24], DSM-IV-TR [25], DSM5 [1], International Statistical Classification of Diseases and Related Health Problems-10 [26], or scores above a clinical threshold.
2.2. European Policies and Legislations Search Strategy
3. Results
3.1. International Literature Review
3.1.1. Multidisciplinary Plans of Care from Referral to Post-Diagnosis
3.1.2. Actions Aimed at Improving Healthcare Procedures
Early Recognition, Screening, Diagnosis, and Intervention for Autistic People
Transition from Adolescence to Adulthood
Coordination between Organizations to Facilitate Education and Employment
Health Care Services, Multidisciplinary Approach, and Inpatient Settings
Digital Platforms for the Management of Care Pathways
3.2. European Policies and Legislations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Cawthorpe, D. A 16-Year Cohort Analysis of Autism Spectrum Disorder-Associated Morbidity in a Pediatric Population. Front. Psychiatry 2018, 9, 635. [Google Scholar] [CrossRef]
- Lord, C.; Charman, T.; Havdahl, A.; Carbone, P.; Anagnostou, E.; Boyd, B.; Carr, T.; de Vries, P.J.; Dissanayake, C.; Divan, G.; et al. The Lancet Commission on the Future of Care and Clinical Research in Autism. Lancet 2022, 399, 271–334. [Google Scholar] [CrossRef]
- Howlin, P.; Magiati, I.; Charman, T. Systematic Review of Early Intensive Behavioral Interventions for Children With Autism. Am. J. Intellect. Dev. Disabil. 2009, 114, 23–41. [Google Scholar] [CrossRef]
- Siegel, M.; King, B.H. Autism and Developmental Disorders: Management of Serious Behavioral Disturbance. Child Adolesc. Psychiatr. Clin. N. Am. 2014, 23, xiii–xv. [Google Scholar] [CrossRef]
- Wei, X.; Wagner, M.; Christiano, E.R.A.; Shattuck, P.; Yu, J.W. Special Education Services Received by Students With Autism Spectrum Disorders From Preschool Through High School. J. Spec. Educ. 2014, 48, 167–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orsmond, G.I.; Krauss, M.W.; Seltzer, M.M. Peer Relationships and Social and Recreational Activities Among Adolescents and Adults with Autism. J. Autism Dev. Disord. 2004, 34, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Shattuck, P.T.; Wagner, M.; Narendorf, S.; Sterzing, P.; Hensley, M. Post–High School Service Use Among Young Adults With an Autism Spectrum Disorder. Arch. Pediatr. Adolesc. Med. 2011, 165, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.L.; McPheeters, M.L.; Sathe, N.A.; Dove, D.; Veenstra-VanderWeele, J.; Warren, Z. A Systematic Review of Vocational Interventions for Young Adults With Autism Spectrum Disorders. Pediatrics 2012, 130, 531–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shattuck, P.T.; Roux, A.M.; Hudson, L.E.; Taylor, J.L.; Maenner, M.J.; Trani, J.-F. Services for Adults with an Autism Spectrum Disorder. Can. J. Psychiatry 2012, 57, 284–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penner, M.; Anagnostou, E.; Andoni, L.Y.; Ungar, W.J. Systematic Review of Clinical Guidance Documents for Autism Spectrum Disorder Diagnostic Assessment in Select Regions. Autism 2018, 22, 517–527. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. A Transition from Children’s to Adults’ Services for Young People Using Health or Social Care Services. 2016. Available online: https://www.nice.org.uk/guidance/ng43 (accessed on 4 May 2022).
- Anderson, C.; Butt, C. Young Adults on the Autism Spectrum: The Struggle for Appropriate Services. J. Autism Dev. Disord. 2018, 48, 3912–3925. [Google Scholar] [CrossRef] [PubMed]
- Bejarano-Martín, Á.; Canal-Bedia, R.; Magán-Maganto, M.; Fernández-Álvarez, C.; Cilleros-Martín, M.V.; Sánchez-Gómez, M.C.; García-Primo, P.; Rose-Sweeney, M.; Boilson, A.; Linertová, R.; et al. Early Detection, Diagnosis and Intervention Services for Young Children with Autism Spectrum Disorder in the European Union (ASDEU): Family and Professional Perspectives. J. Autism Dev. Disord. 2020, 50, 3380–3394. [Google Scholar] [CrossRef]
- Crane, L.; Batty, R.; Adeyinka, H.; Goddard, L.; Henry, L.A.; Hill, E.L. Autism Diagnosis in the United Kingdom: Perspectives of Autistic Adults, Parents and Professionals. J. Autism Dev. Disord. 2018, 48, 3761–3772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurt, L.; Langley, K.; North, K.; Southern, A.; Copeland, L.; Gillard, J.; Williams, S. Understanding and Improving the Care Pathway for Children with Autism. IJHCQA 2019, 32, 208–223. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Goddard, L.; Hill, E.L.; Henry, L.A.; Crane, L. Experiences of Receiving a Diagnosis of Autism Spectrum Disorder: A Survey of Adults in the United Kingdom. J. Autism Dev. Disord. 2014, 44, 3033–3044. [Google Scholar] [CrossRef]
- Lewis, L.F. A Mixed Methods Study of Barriers to Formal Diagnosis of Autism Spectrum Disorder in Adults. J. Autism Dev. Disord. 2017, 47, 2410–2424. [Google Scholar] [CrossRef]
- Micai, M.; Ciaramella, A.; Salvitti, T.; Fulceri, F.; Fatta, L.M.; Poustka, L.; Diehm, R.; Iskrov, G.; Stefanov, R.; Guillon, Q.; et al. Autistic Adult Health and Professional Perceptions of It: Evidence From the ASDEU Project. Front. Psychiatry 2021, 12, 614102. [Google Scholar] [CrossRef]
- Micai, M.; Ciaramella, A.; Salvitti, T.; Fulceri, F.; Fatta, L.M.; Poustka, L.; Diehm, R.; Iskrov, G.; Stefanov, R.; Guillon, Q.; et al. Intervention Services for Autistic Adults: An ASDEU Study of Autistic Adults, Carers, and Professionals’ Experiences. J. Autism Dev. Disord. 2022, 52, 1623–1639. [Google Scholar] [CrossRef]
- Scattoni, M.L.; Micai, M.; Ciaramella, A.; Salvitti, T.; Fulceri, F.; Fatta, L.M.; Poustka, L.; Diehm, R.; Iskrov, G.; Stefanov, R.; et al. Real-World Experiences in Autistic Adult Diagnostic Services and Post-Diagnostic Support and Alignment with Services Guidelines: Results from the ASDEU Study. J. Autism Dev. Disord. 2021, 51, 4129–4146. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, DSM-IV, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, DSM-IV-TR, 4th ed.; text revised; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. Available online: https://apps.who.int/iris/handle/10665/37958 (accessed on 22 March 2023).
- Green, J.; Leadbitter, K.; Ainsworth, J.; Bucci, S. An Integrated Early Care Pathway for Autism. Lancet Child Adolesc. Health 2022, 6, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Liu, J.; Chien, T.; Batalden, M.; Hirsh, D.A. A Systematic Network of Autism Primary Care Services (SYNAPSE): A Model of Coproduction for the Management of Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 1847–1853. [Google Scholar] [CrossRef] [PubMed]
- Fueyo, M.; Caldwell, T.; Mattern, S.B.; Zahid, J.; Foley, T. The Health Home: A Service Delivery Model for Autism and Intellectual Disability. Psychiatr. Serv. 2015, 66, 1135–1137. [Google Scholar] [CrossRef]
- Rutherford, M.; Burns, M.; Gray, D.; Bremner, L.; Clegg, S.; Russell, L.; Smith, C.; O’Hare, A. Improving Efficiency and Quality of the Children’s ASD Diagnostic Pathway: Lessons Learned from Practice. J. Autism Dev. Disord. 2018, 48, 1579–1595. [Google Scholar] [CrossRef] [Green Version]
- Rutherford, M.; Forsyth, K.; McKenzie, K.; McClure, I.; Murray, A.; McCartney, D.; Irvine, L.; O’Hare, A. Implementation of a Practice Development Model to Reduce the Wait for Autism Spectrum Diagnosis in Adults. J. Autism Dev. Disord. 2018, 48, 2677–2691. [Google Scholar] [CrossRef] [Green Version]
- Rutherford, M.; McKenzie, K.; Forsyth, K.; McCartney, D.; O’Hare, A.; McClure, I.; Irvine, L. Why Are They Waiting? Exploring Professional Perspectives and Developing Solutions to Delayed Diagnosis of Autism Spectrum Disorder in Adults and Children. Res. Autism Spectr. Disord. 2016, 31, 53–65. [Google Scholar] [CrossRef]
- Melton, J.; Forsyth, K.; Freeth, D. A Practice Development Programme to Promote the Use of the Model of Human Occupation: Contexts, Influential Mechanisms and Levels of Engagement Amongst Occupational Therapists. Br. J. Occup. Ther. 2010, 73, 549–558. [Google Scholar] [CrossRef]
- Levy, S.E.; Wolfe, A.; Coury, D.; Duby, J.; Farmer, J.; Schor, E.; Van Cleave, J.; Warren, Z. Screening Tools for Autism Spectrum Disorder in Primary Care: A Systematic Evidence Review. Pediatrics 2020, 145, S47–S59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNally Keehn, R.; Ciccarelli, M.; Szczepaniak, D.; Tomlin, A.; Lock, T.; Swigonski, N. A Statewide Tiered System for Screening and Diagnosis of Autism Spectrum Disorder. Pediatrics 2020, 146, e20193876. [Google Scholar] [CrossRef] [PubMed]
- Crowley, N.; O’Connell, H.; Gervin, M. Autistic Spectrum Disorder without Intellectual Impairment in Adult Mental Health Services—Fostering New Perspectives and Enhancing Existing Services. Ir. J. Psychol. Med. 2022, 39, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Ibañez, L.V.; Stoep, A.V.; Myers, K.; Zhou, C.; Dorsey, S.; Steinman, K.J.; Stone, W.L. Promoting Early Autism Detection and Intervention in Underserved Communities: Study Protocol for a Pragmatic Trial Using a Stepped-Wedge Design. BMC Psychiatry 2019, 19, 169. [Google Scholar] [CrossRef] [Green Version]
- Rotholz, D.A.; Kinsman, A.M.; Lacy, K.K.; Charles, J. Improving Early Identification and Intervention for Children at Risk for Autism Spectrum Disorder. Pediatrics 2017, 139, e20161061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams-Arya, P.; Anixt, J.; Kuan, L.; Johnson, H.; Kent, B.; Bing, N.; Ehrhardt, J.; Manning-Courtney, P. Improving Access to Diagnostic Assessments for Autism Spectrum Disorder Using an Arena Model. J. Dev. Behav. Pediatr. 2019, 40, 161–169. [Google Scholar] [CrossRef]
- McAllister, J.W.; Keehn, R.M.; Rodgers, R.; Lock, T.M. Care Coordination Using a Shared Plan of Care Approach: From Model to Practice. J. Pediatr. Nurs. 2018, 43, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Shepley, C.; Shepley, S.B.; Allday, R.A.; Tyner-Wilson, M.; Larrow, D. Rationale, Development, and Description of a Brief Family-Centered Service Provision Model for Addressing Children’s Severe Behavior. Dev. Neurorehabilit. 2021, 24, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Brede, J.; Cage, E.; Trott, J.; Palmer, L.; Smith, A.; Serpell, L.; Mandy, W.; Russell, A. “We Have to Try to Find a Way, a Clinical Bridge”—Autistic Adults’ Experience of Accessing and Receiving Support for Mental Health Difficulties: A Systematic Review and Thematic Meta-Synthesis. Clin. Psychol. Rev. 2022, 93, 102131. [Google Scholar] [CrossRef]
- Nathenson, R.A.; Zablotsky, B. The Transition to the Adult Health Care System Among Youths With Autism Spectrum Disorder. Psychiatr. Serv. 2017, 68, 735–738. [Google Scholar] [CrossRef] [Green Version]
- Cleverley, K.; Rowland, E.; Bennett, K.; Jeffs, L.; Gore, D. Identifying core components and indicators of successful transitions from child to adult mental health services: A scoping review. Eur. Child Adolesc. Psychiatry 2020, 29, 107–121. [Google Scholar] [CrossRef] [Green Version]
- Davidson, S.; Cappelli, M. We’ve Got Growing UP to Do: Policy and Practice in Youth Mental Health Transitions; Canadian Electronic Library: Ottawa, ON, Canada, 2011; Available online: https://canadacommons.ca/artifacts/1205298/weve-got-growing-up-to-do/1758407/ (accessed on 22 March 2023).
- Mental Health Commission of Canada. Mental Health Matters, Annual Report 2014–2015; Mental Health Commission of Canada: Ottawa, ON, Canada, 2015. [Google Scholar]
- Tunesi, S.; Bosio, M.; Russo, A.G. Do Autistic Patients Change Healthcare Services Utilisation through the Transition Age? An Italian Longitudinal Retrospective Study. BMJ Open 2019, 9, e030844. [Google Scholar] [CrossRef] [Green Version]
- Laghi, F.; Trimarco, B. Individual Planning Starts at School. Tools and Practices Promoting Autonomy and Supporting Transition to Work for Adolescents with Autism Spectrum Disorder. Ann. Dell’istituto Super. Sanità 2020, 56, 222–229. [Google Scholar] [CrossRef]
- Hatfield, M.; Murray, N.; Ciccarelli, M.; Falkmer, T.; Falkmer, M. Pilot of the BOOST-ATM: An Online Transition Planning Program for Adolescents with Autism. Aust. Occup. Ther. J. 2017, 64, 448–456. [Google Scholar] [CrossRef] [PubMed]
- White, S.W.; Smith, I.C.; Miyazaki, Y.; Conner, C.M.; Elias, R.; Capriola-Hall, N.N. Improving Transition to Adulthood for Students with Autism: A Randomized Controlled Trial of STEPS. J. Clin. Child Adolesc. Psychol. 2021, 50, 187–201. [Google Scholar] [CrossRef]
- Jonsson, U.; Coco, C.; Fridell, A.; Brown, S.; Berggren, S.; Hirvikoski, T.; Bölte, S. Proof of Concept: The TRANSITION Program for Young Adults with Autism Spectrum Disorder and/or Attention Deficit Hyperactivity Disorder. Scand. J. Occup. Ther. 2021, 28, 78–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Accardo, A.L.; Kuder, S.J.; Woodruff, J. Accommodations and support services preferred by college students with autism spectrum disorder. Autism 2019, 23, 574–583. [Google Scholar] [CrossRef]
- Sung, C.; Connor, A.; Chen, J.; Lin, C.C.; Kuo, H.J.; Chun, J. Development, feasibility, and preliminary efficacy of an employment-related social skills intervention for young adults with high-functioning autism. Autism 2019, 23, 1542–1553. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.; Falkmer, M.; Falkmer, T.; Girdler, S. Evaluating the Effectiveness of an Autism-Specific Workplace Tool for Employers: A Randomised Controlled Trial. J. Autism Dev. Disord. 2018, 48, 3377–3392. [Google Scholar] [CrossRef] [Green Version]
- Kuriakose, S.; Filton, B.; Marr, M.; Okparaeke, E.; Cervantes, P.; Siegel, M.; Horwitz, S.; Havens, J. Does an Autism Spectrum Disorder Care Pathway Improve Care for Children and Adolescents with ASD in Inpatient Psychiatric Units? J. Autism Dev. Disord. 2018, 48, 4082–4089. [Google Scholar] [CrossRef]
- Thom, R.P.; McDougle, C.J.; Hazen, E.P. Challenges in the Medical Care of Patients With Autism Spectrum Disorder: The Role of the Consultation-Liaison Psychiatrist. Psychosomatics 2019, 60, 435–443. [Google Scholar] [CrossRef]
- Samet, D.; Luterman, S. See-Hear-Feel-Speak: A Protocol for Improving Outcomes in Emergency Department Interactions With Patients With Autism Spectrum Disorder. Pediatr. Emerg. Care 2019, 35, 157–159. [Google Scholar] [CrossRef]
- Austin, J.; Manning-Courtney, P.; Johnson, M.L.; Weber, R.; Johnson, H.; Murray, D.; Ratliff-Schaub, K.; Tadlock, A.M.; Murray, M. Improving Access to Care at Autism Treatment Centers: A System Analysis Approach. Pediatrics 2016, 137, S149–S157. [Google Scholar] [CrossRef] [Green Version]
- Iannuzzi, D.; Kopecky, K.; Broder-Fingert, S.; Connors, S.L. Addressing the Needs of Individuals with Autism: Role of Hospital-Based Social Workers in Implementation of a Patient-Centered Care Plan. Health Soc. Work 2015, 40, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Fenning, R.M.; Steinberg-Epstein, R.; Butter, E.M.; Chan, J.; McKinnon-Bermingham, K.; Hammersmith, K.J.; Moffitt, J.; Shui, A.M.; Parker, R.A.; Coury, D.L.; et al. Access to Dental Visits and Correlates of Preventive Dental Care in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 3739–3747. [Google Scholar] [CrossRef] [PubMed]
- Mangione, F.; Bdeoui, F.; Monnier-Da Costa, A.; Dursun, E. Autistic Patients: A Retrospective Study on Their Dental Needs and the Behavioural Approach. Clin. Oral Investig. 2020, 24, 1677–1685. [Google Scholar] [CrossRef] [PubMed]
- Stein Duker, L.I.; Floríndez, L.I.; Como, D.H.; Tran, C.F.; Henwood, B.F.; Polido, J.C.; Cermak, S.A. Strategies for Success: A Qualitative Study of Caregiver and Dentist Approaches to Improving Oral Care for Children with Autism. Pediatr. Dent. 2019, 41, 4E–12E. [Google Scholar] [PubMed]
- Haydon, C.; Doherty, M.; Davidson, I.A. Autism: Making Reasonable Adjustments in Healthcare. Br. J. Hosp. Med. 2021, 82, 1–11. [Google Scholar] [CrossRef]
- Downs, S.M.; Bauer, N.S.; Saha, C.; Ofner, S.; Carroll, A.E. Effect of a Computer-Based Decision Support Intervention on Autism Spectrum Disorder Screening in Pediatric Primary Care Clinics: A Cluster Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e1917676. [Google Scholar] [CrossRef] [Green Version]
- Schrader, E.; Delehanty, A.D.; Casler, A.; Petrie, E.; Rivera, A.; Harrison, K.; Paterniti, T.; Sebastiany, L.; Nottke, C.; Sohl, K.; et al. Integrating a New Online Autism Screening Tool in Primary Care to Lower the Age of Referral. Clin. Pediatr. 2020, 59, 305–309. [Google Scholar] [CrossRef]
- Nicolaidis, C.; Raymaker, D.; McDonald, K.; Kapp, S.; Weiner, M.; Ashkenazy, E.; Gerrity, M.; Kripke, C.; Platt, L.; Baggs, A. The Development and Evaluation of an Online Healthcare Toolkit for Autistic Adults and Their Primary Care Providers. J. Gen. Intern. Med. 2016, 31, 1180–1189. [Google Scholar] [CrossRef] [Green Version]
- Dreiling, N.G.; Cook, M.L.; Lamarche, E.; Klinger, L.G. Mental Health Project ECHO Autism: Increasing Access to Community Mental Health Services for Autistic Individuals. Autism 2022, 26, 434–445. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Autism Spectrum Disorder in Adults: Diagnosis and Management. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554918/ (accessed on 22 March 2023).
- Featherstone, C.; Sharpe, R.A.; Axford, N.; Asthana, S.; Husk, K. Health and Wellbeing Outcomes and Social Prescribing Pathways in Community-based Support for Autistic Adults: A Systematic Mapping Review of Reviews. Health Soc. Care Comm. 2022, 30, e621–e635. [Google Scholar] [CrossRef] [PubMed]
- Rotter, T.; Kinsman, L.; James, E.L.; Machotta, A.; Gothe, H.; Willis, J.; Snow, P.; Kugler, J. Clinical Pathways: Effects on Professional Practice, Patient Outcomes, Length of Stay and Hospital Costs. Cochrane Database Syst. Rev. 2010, 3, CD006632. [Google Scholar] [CrossRef] [PubMed]
- Lawal, A.K.; Rotter, T.; Kinsman, L.; Machotta, A.; Ronellenfitsch, U.; Scott, S.D.; Goodridge, D.; Plishka, C.; Groot, G. What Is a Clinical Pathway? Refinement of an Operational Definition to Identify Clinical Pathway Studies for a Cochrane Systematic Review. BMC Med. 2016, 14, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, B.C.K.; Pak, A.W.P. Multidisciplinarity, Interdisciplinarity and Transdisciplinarity in Health Research, Services, Education and Policy: 1. Definitions, Objectives, and Evidence of Effectiveness. Clin. Investig. Med. 2006, 29, 351–364. [Google Scholar]
- Hyman, S.L.; Levy, S.E.; Myers, S.M.; Council On Children with Disabilities, Section on Developmental and Behavioral Pediatrics; Kuo, D.Z.; Apkon, S.; Davidson, L.F.; Ellerbeck, K.A.; Foster, J.E.A.; Noritz, G.H.; et al. Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Disabled Children and Young People up to 25 with Severe Complex Needs: Integrated Service Delivery and Organisation across Health, Social Care and Education. 2022. Available online: https://www.nice.org.uk/guidance/ng213 (accessed on 9 March 2022).
- Oakley, B.; Tillmann, J.; Ruigrok, A.; Baranger, A.; Takow, C.; Charman, T.; Jones, E.; Cusack, J.; Doherty, M.; Violland, P.; et al. COVID-19 Health and Social Care Access for Autistic People: European Policy Review. BMJ Open 2021, 11, e045341. [Google Scholar] [CrossRef]
- Sutherland, R.; Trembath, D.; Roberts, J. Telehealth and Autism: A Systematic Search and Review of the Literature. Int. J. Speech-Lang. Pathol. 2018, 20, 324–336. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Domain | Search Strategy |
|---|---|
| Population | Autistic Disorder [Mesh] OR Autism Spectrum Disorder [MeSH] OR Child Development Disorders, Pervasive [MeSH] OR Asperger Syndrome [MeSH] OR “pervasive developmental disorder” |
| Intervention | “Integrated carepathways” OR “Integrated care pathway” OR “Care coordination” OR “Care coordinator” OR “Care coordinators” OR “Care management” OR “Care maps” OR “Care map” OR “Care model” OR “Care models” OR “Care paths” OR “Care path” OR “Care pathways” OR “Care pathway” OR “Case management” OR “Case management plans” OR “Case management plan” OR Case manager [MeSH] OR Outcome and Process Assessment OR Outcome and Process Assessment (Health Care) OR “Clinical care pathways” OR “Clinical care pathway” OR Continuity of patient care [MeSH] OR Critical pathways [MeSH] OR “Empowerment” OR Delivery of Health Care, Integrated [MeSH] OR Health Services [MeSH] OR “Health care organization” OR “Health care services” OR “Health care service” OR “Lean approach” OR “Lean approaches” OR “Lean management” OR “Patient care” OR Patient care management [MeSH] OR “Patient centred model” OR “Patient centered model” OR “Patient centred models” OR “Patient centered models” OR “Patient-care” OR “Patient-centered care” OR “Patient-centred care” OR “Social care organization” OR “Social care services” OR “Social care service” OR “Care Transitions” OR Transition, Care OR Transitions, Care OR Transition of Care OR Health Care Transition OR Care Transition, Health OR Care Transitions, Health OR Health Care Transitions OR Transition, Health Care OR Transitions, Health Care OR Transitional care [MeSH] OR Management Service Organizations [MeSH] OR “Diagnostic-therapeutic-assistance pathway” OR “Employment” OR Employment, Supported [Mesh] OR Residence Characteristics [MeSH] OR “Housing” OR Continuing Care Retirement Centers OR Life Care Centers, Retirement OR “Residential housing” OR “Supported living” OR “Transitional models” OR “Supported residence” OR “Supported residences” OR Group home [MeSH] OR Residential Facilities [MeSH] OR Intermediate Care Facilities [MeSH]) |
| Studies | Plans of Care from Referral to Post-Diagnosis |
|---|---|
| Green 2022 [27] | Implementation of the integrated and proactive care pathway through
|
| Kong 2020 [28] | Networks of ASD-trained primary care providers:
|
| Fueyo 2015 [29] | Specialty behavioral health professionals:
|
| Rutherford 2018 [30] | Implementation of actions for children with ASD in key areas:
|
| Rutherford 2018 [31] | Implementation of actions for adults with ASD through
|
| Phases | Service/Pattern | Coordination | Facilitation | Training | Note | |
|---|---|---|---|---|---|---|
| [27] | Pre diagnosis: identify neurodivergent development and pre-diagnosis care. Around diagnosis: support family understanding and adjustment. Post diagnosis: family focused intervention. Long term support: family or carer management/CM. | CM. Step-up and step-down care during transition points or to react to co-occurring conditions. | CM sustains family self-care, resilience. CM: interface between family support and multi-agency collaborative care (health, social care, education). | Digital health technologies. Digital care navigators. | Effective intervention. ASD monitoring with (HV protocols and education assessments). | Large datasets; learning health system. Co-production in service design. Collaborative care. |
| [28] | ASD early detection. Comprehensive evaluation package. Management of psychiatric and medical co-occurring conditions. Comprehensive functional evaluation and care. | ASD-trained PCPs: coordinate care linked with ASD specialist networks, standardized AP co-developed by individuals, families, providers. | Collaboration with special education, community, adult transitions. Bidirectional collaboration with services in community and medical system. | Accessible workforce training connecting/outreach and IT platform. | ASD-specific PCPs training. Evidence-based care and protocols. | Co-production of care. Organizing care, family/multidisciplinary/interprofessional discussions. |
| [29] | Diagnostic evaluation by multidisciplinary team; case conceptualization and initial care plan. Periodic reassessment; clinical monitoring. Comprehensive care. | Regional comprehensive treatment center; ASD team in behavioral health setting. HM integration with PC/GM services. | HM team works closely with school districts, vocational training agencies, adult transition services, sheltered workshops. | Electronic health records. Monitoring survey instruments. | Highly trained life-care managers. Life-care manual. | Patients, families, and team work collaboratively. HM. |
| [30] | AP implementation for identification, referral for specialist assessment; diagnostic assessment; post diagnostic support; quality; adherence to CG. | CP/CSLPT assessment; CAHMS, Choice and Partnership Appointment or CAHMS caseworker assessment; Specialist assessment. | - | - | Training according to levels of skill required by staff. | AP from [32] and guidelines * |
| [31] | AP implementation for identification, diagnostic process, nonattendance rates inappropriate referrals, efficient working and communication, effectiveness of care pathways. | Health Services with mixed ASD service history. | - | - | Training according to needs in service. | Specific local targets and action plan based on [32] and guidelines * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulceri, F.; Gila, L.; Caruso, A.; Micai, M.; Romano, G.; Scattoni, M.L. Building Bricks of Integrated Care Pathway for Autism Spectrum Disorder: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 6222. https://doi.org/10.3390/ijms24076222
Fulceri F, Gila L, Caruso A, Micai M, Romano G, Scattoni ML. Building Bricks of Integrated Care Pathway for Autism Spectrum Disorder: A Systematic Review. International Journal of Molecular Sciences. 2023; 24(7):6222. https://doi.org/10.3390/ijms24076222
Chicago/Turabian StyleFulceri, Francesca, Letizia Gila, Angela Caruso, Martina Micai, Giovanna Romano, and Maria Luisa Scattoni. 2023. "Building Bricks of Integrated Care Pathway for Autism Spectrum Disorder: A Systematic Review" International Journal of Molecular Sciences 24, no. 7: 6222. https://doi.org/10.3390/ijms24076222