

Elevated Midkine Serum Levels Are Associated with Long-Term Survival in Critically Ill Patients

 , , , , ,
, , , , ,  ,
,  ,
,
Abstract
:1. Introduction
2. Results
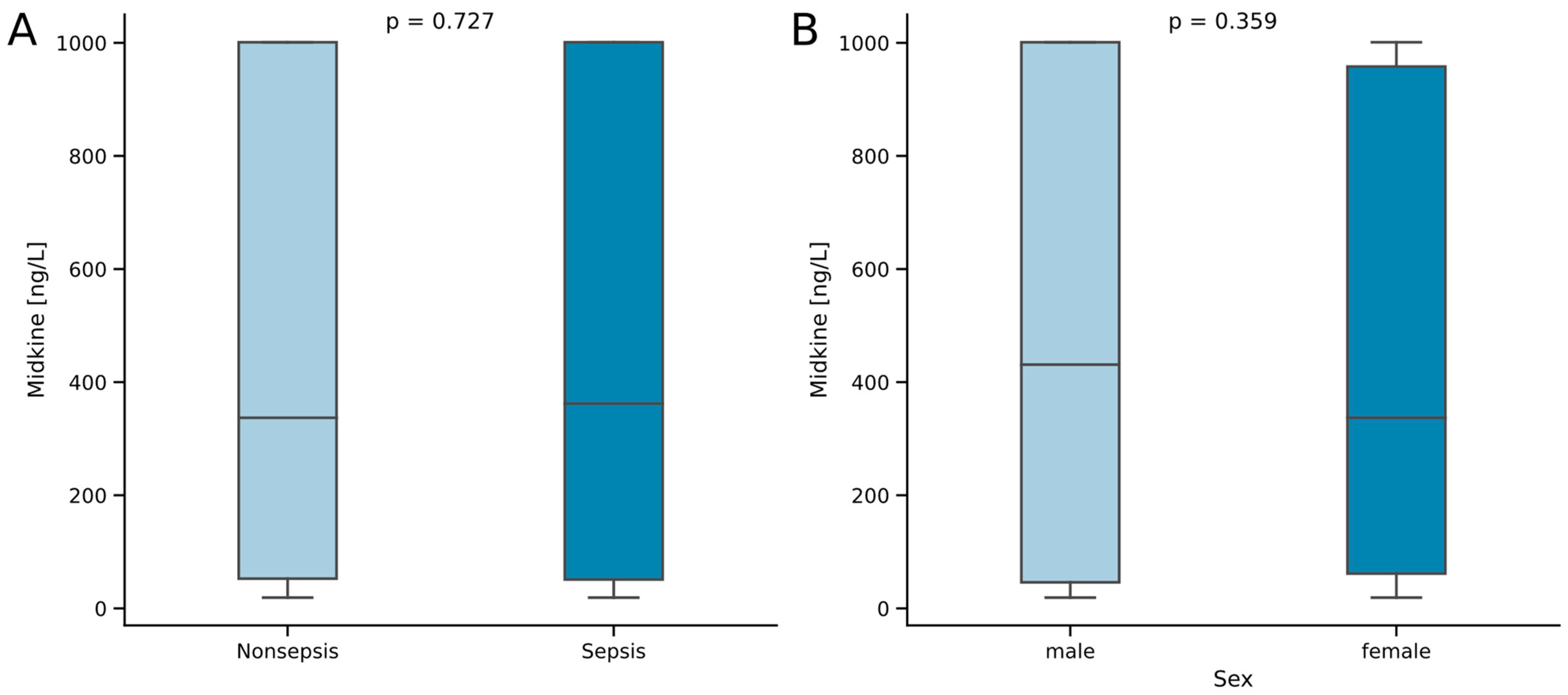
2.1. Midkine Serum Concentrations Do Not Differ between Critically Ill Patients with and without Sepsis
2.2. Midkine Serum Levels Are Not Associated with Disease Etiology in Critically Ill Patients
2.3. Midkine Correlates with Clinically Established Biomarkers of Bacterial Inflammation, Kidney Function, Coagulation Function and Insulin Metabolism
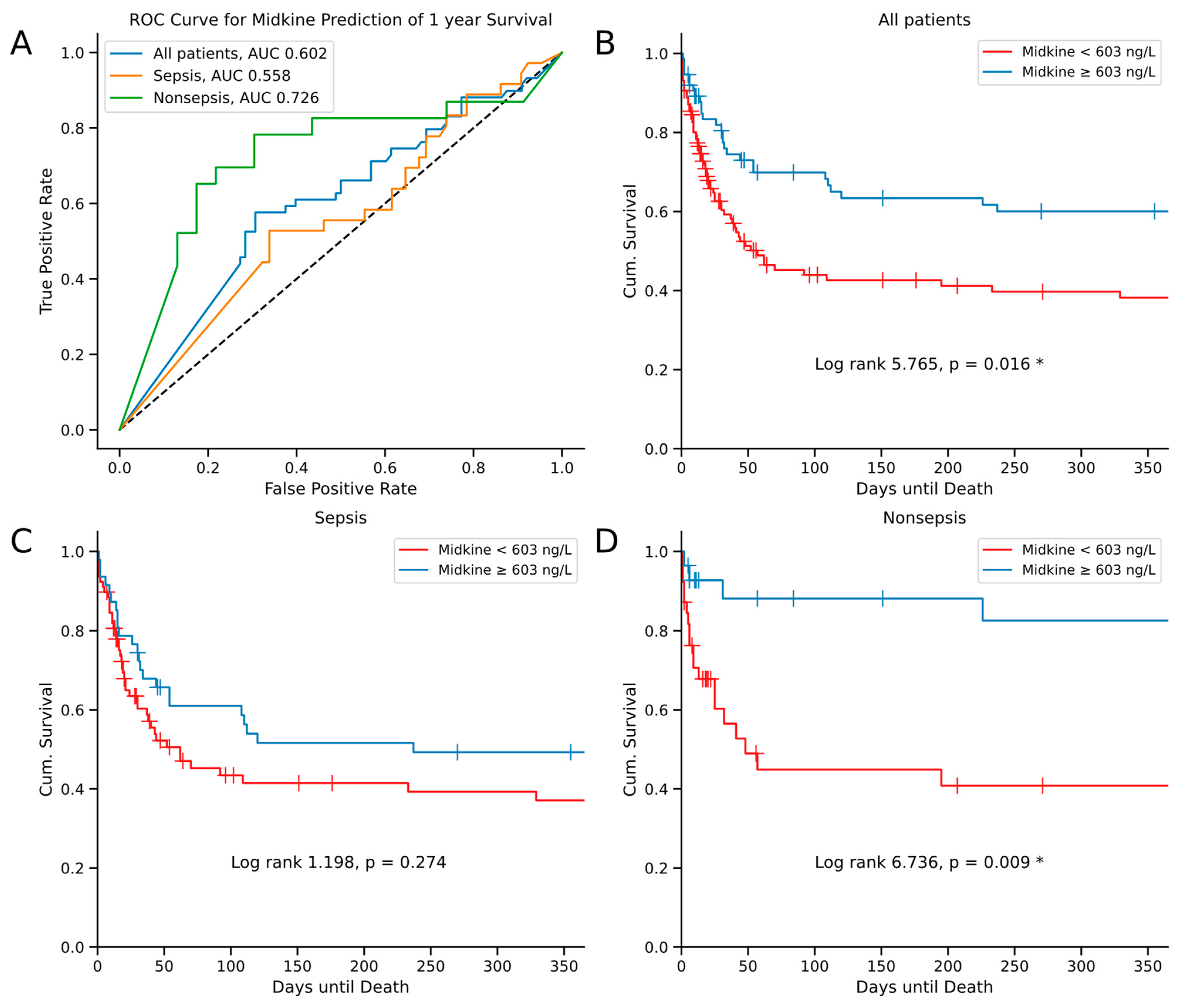
2.4. Midkine Predicts Long-Term Survival in Critically Ill Patients
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Midkine (Mdk) Measurements
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fleischmann-Struzek, C.; Mellhammar, L.; Rose, N.; Cassini, A.; Rudd, K.E.; Schlattmann, P.; Allegranzi, B.; Reinhart, K. Incidence and mortality of hospital- and ICU-treated sepsis: Results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1552–1562. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Boomer, J.S.; Green, J.M.; Hotchkiss, R.S. The changing immune system in sepsis: Is individualized immuno-modulatory therapy the answer? Virulence 2014, 5, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.; Coakley, J.D.; Martin-Loeches, I. Defects in innate and adaptive immunity in patients with sepsis and health care associated infection. Ann. Transl. Med. 2017, 5, 447. [Google Scholar] [CrossRef] [PubMed]
- Kadomatsu, K.; Tomomura, M.; Muramatsu, T. cDNA cloning and sequencing of a new gene intensely expressed in early differentiation stages of embryonal carcinoma cells and in mid-gestation period of mouse embryogenesis. Biochem. Biophys. Res. Commun. 1988, 151, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Winkler, C.; Yao, S. The midkine family of growth factors: Diverse roles in nervous system formation and maintenance. Br. J. Pharmacol. 2014, 171, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Muramatsu, T. Midkine and pleiotrophin: Two related proteins involved in development, survival, inflammation and tumorigenesis. J. Biochem. 2002, 132, 359–371. [Google Scholar] [CrossRef]
- Muramatsu, T. Structure and function of midkine as the basis of its pharmacological effects. Br. J. Pharmacol. 2014, 171, 814–826. [Google Scholar] [CrossRef]
- Jones, D.R. Measuring midkine: The utility of midkine as a biomarker in cancer and other diseases. Br. J. Pharmacol. 2014, 171, 2925–2939. [Google Scholar] [CrossRef]
- Tsutsui, J.; Kadomatsu, K.; Matsubara, S.; Nakagawara, A.; Hamanoue, M.; Takao, S.; Shimazu, H.; Ohi, Y.; Muramatsu, T. A new family of heparin-binding growth/differentiation factors: Increased midkine expression in Wilms’ tumor and other human carcinomas. Cancer Res. 1993, 53, 1281–1285. [Google Scholar] [PubMed]
- Cohen, S.; Shoshana, O.Y.; Zelman-Toister, E.; Maharshak, N.; Binsky-Ehrenreich, I.; Gordin, M.; Hazan-Halevy, I.; Herishanu, Y.; Shvidel, L.; Haran, M.; et al. The cytokine midkine and its receptor RPTPzeta regulate B cell survival in a pathway induced by CD74. J. Immunol. 2012, 188, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Hovanessian, A.G. Midkine, a cytokine that inhibits HIV infection by binding to the cell surface expressed nucleolin. Cell Res. 2006, 16, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Inazumi, T.; Tajima, S.; Nishikawa, T.; Kadomatsu, K.; Muramatsu, H.; Muramatsu, T. Expression of the retinoid-inducible polypeptide, midkine, in human epidermal keratinocytes. Arch. Dermatol. Res. 1997, 289, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Kerzerho, J.; Adotevi, O.; Castelli, F.A.; Dosset, M.; Bernardeau, K.; Szely, N.; Lang, F.; Tartour, E.; Maillere, B. The angiogenic growth factor and biomarker midkine is a tumor-shared antigen. J. Immunol. 2010, 185, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Suh, H.N.; Lee, Y.J.; Seo, B.N.; Ha, J.W.; Han, H.J. Midkine prevented hypoxic injury of mouse embryonic stem cells through activation of Akt and HIF-1alpha via low-density lipoprotein receptor-related protein-1. J. Cell Physiol. 2012, 227, 1731–1739. [Google Scholar] [CrossRef]
- Nordin, S.L.; Jovic, S.; Kurut, A.; Andersson, C.; Gela, A.; Bjartell, A.; Morgelin, M.; Olin, A.I.; Lund, M.; Egesten, A. High expression of midkine in the airways of patients with cystic fibrosis. Am. J. Respir. Cell Mol. Biol. 2013, 49, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Miyashiro, I.; Kaname, T.; Shin, E.; Wakasugi, E.; Monden, T.; Takatsuka, Y.; Kikkawa, N.; Muramatsu, T.; Monden, M.; Akiyama, T. Midkine expression in human breast cancers: Expression of truncated form. Breast Cancer Res. Treat. 1997, 43, 1–6. [Google Scholar] [CrossRef]
- Huang, Y.; Cao, G.; Wang, H.; Wang, Q.; Hou, Y. The expression and location of midkine in gastric carcinomas of Chinese patients. Cell Mol. Immunol. 2007, 4, 135–140. [Google Scholar]
- Muramatsu, H.; Shirahama, H.; Yonezawa, S.; Maruta, H.; Muramatsu, T. Midkine, a retinoic acid-inducible growth/differentiation factor: Immunochemical evidence for the function and distribution. Dev. Biol. 1993, 159, 392–402. [Google Scholar] [CrossRef]
- Filippou, P.S.; Karagiannis, G.S.; Constantinidou, A. Midkine (MDK) growth factor: A key player in cancer progression and a promising therapeutic target. Oncogene 2020, 39, 2040–2054. [Google Scholar] [CrossRef] [PubMed]
- Horiba, M.; Kadomatsu, K.; Yasui, K.; Lee, J.K.; Takenaka, H.; Sumida, A.; Kamiya, K.; Chen, S.; Sakuma, S.; Muramatsu, T.; et al. Midkine plays a protective role against cardiac ischemia/reperfusion injury through a reduction of apoptotic reaction. Circulation 2006, 114, 1713–1720. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Goto, M.; Tsutsui, J.; Ozawa, M.; Sato, E.; Osame, M.; Muramatsu, T. Midkine is present in the early stage of cerebral infarct. Brain Res. Dev. Brain Res. 1995, 85, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Sato, W.; Kadomatsu, K.; Yuzawa, Y.; Muramatsu, H.; Hotta, N.; Matsuo, S.; Muramatsu, T. Midkine is involved in neutrophil infiltration into the tubulointerstitium in ischemic renal injury. J. Immunol. 2001, 167, 3463–3469. [Google Scholar] [CrossRef] [PubMed]
- Horiba, M.; Kadomatsu, K.; Nakamura, E.; Muramatsu, H.; Ikematsu, S.; Sakuma, S.; Hayashi, K.; Yuzawa, Y.; Matsuo, S.; Kuzuya, M.; et al. Neointima formation in a restenosis model is suppressed in midkine-deficient mice. J. Clin. Investig. 2000, 105, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Kawai, H.; Sato, W.; Yuzawa, Y.; Kosugi, T.; Matsuo, S.; Takei, Y.; Kadomatsu, K.; Muramatsu, T. Lack of the growth factor midkine enhances survival against cisplatin-induced renal damage. Am. J. Pathol. 2004, 165, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Kosugi, T.; Sato, W. Midkine and the kidney: Health and diseases. Nephrol. Dial. Transplant. 2012, 27, 16–21. [Google Scholar] [CrossRef]
- Kato, K.; Kosugi, T.; Sato, W.; Arata-Kawai, H.; Ozaki, T.; Tsuboi, N.; Ito, I.; Tawada, H.; Yuzawa, Y.; Matsuo, S.; et al. Growth factor Midkine is involved in the pathogenesis of renal injury induced by protein overload containing endotoxin. Clin. Exp. Nephrol. 2011, 15, 346–354. [Google Scholar] [CrossRef]
- Kosugi, T.; Yuzawa, Y.; Sato, W.; Arata-Kawai, H.; Suzuki, N.; Kato, N.; Matsuo, S.; Kadomatsu, K. Midkine is involved in tubulointerstitial inflammation associated with diabetic nephropathy. Lab. Investig. 2007, 87, 903–913. [Google Scholar] [CrossRef]
- Salaru, D.L.; Mertens, P.R.; Bartsch, P. Loss of heparin-binding protein prevents necrotizing glomerulonephritis: First clues hint at plasminogen activator inhibitor-1. Int. Urol. Nephrol. 2013, 45, 1483–1487. [Google Scholar] [CrossRef]
- Sonobe, Y.; Li, H.; Jin, S.; Kishida, S.; Kadomatsu, K.; Takeuchi, H.; Mizuno, T.; Suzumura, A. Midkine inhibits inducible regulatory T cell differentiation by suppressing the development of tolerogenic dendritic cells. J. Immunol. 2012, 188, 2602–2611. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Neubauer, K.; Matusiewicz, M. Circulating midkine in Crohn’s disease: Clinical implications. Inflamm. Bowel Dis. 2010, 16, 208–215. [Google Scholar] [CrossRef]
- Takada, T.; Toriyama, K.; Muramatsu, H.; Song, X.J.; Torii, S.; Muramatsu, T. Midkine, a retinoic acid-inducible heparin-binding cytokine in inflammatory responses: Chemotactic activity to neutrophils and association with inflammatory synovitis. J. Biochem. 1997, 122, 453–458. [Google Scholar] [CrossRef]
- Liu, X.; Mashour, G.A.; Webster, H.F.; Kurtz, A. Basic FGF and FGF receptor 1 are expressed in microglia during experimental autoimmune encephalomyelitis: Temporally distinct expression of midkine and pleiotrophin. Glia 1998, 24, 390–397. [Google Scholar] [CrossRef]
- Wang, J.; Takeuchi, H.; Sonobe, Y.; Jin, S.; Mizuno, T.; Miyakawa, S.; Fujiwara, M.; Nakamura, Y.; Kato, T.; Muramatsu, H.; et al. Inhibition of midkine alleviates experimental autoimmune encephalomyelitis through the expansion of regulatory T cell population. Proc. Natl. Acad. Sci. USA 2008, 105, 3915–3920. [Google Scholar] [CrossRef]
- Maruyama, K.; Muramatsu, H.; Ishiguro, N.; Muramatsu, T. Midkine, a heparin-binding growth factor, is fundamentally involved in the pathogenesis of rheumatoid arthritis. Arthritis Rheum. 2004, 50, 1420–1429. [Google Scholar] [CrossRef]
- Kadomatsu, K.; Kishida, S.; Tsubota, S. The heparin-binding growth factor midkine: The biological activities and candidate receptors. J. Biochem. 2013, 153, 511–521. [Google Scholar] [CrossRef]
- Sanino, G.; Bosco, M.; Terrazzano, G. Physiology of Midkine and Its Potential Pathophysiological Role in COVID-19. Front. Physiol. 2020, 11, 616552. [Google Scholar] [CrossRef]
- Weckbach, L.T.; Grabmaier, U.; Uhl, A.; Gess, S.; Boehm, F.; Zehrer, A.; Pick, R.; Salvermoser, M.; Czermak, T.; Pircher, J.; et al. Midkine drives cardiac inflammation by promoting neutrophil trafficking and NETosis in myocarditis. J. Exp. Med. 2019, 216, 350–368. [Google Scholar] [CrossRef]
- Muramatsu, T. Midkine: A promising molecule for drug development to treat diseases of the central nervous system. Curr. Pharm. Des. 2011, 17, 410–423. [Google Scholar] [CrossRef]
- Svensson, S.L.; Pasupuleti, M.; Walse, B.; Malmsten, M.; Morgelin, M.; Sjogren, C.; Olin, A.I.; Collin, M.; Schmidtchen, A.; Palmer, R.; et al. Midkine and pleiotrophin have bactericidal properties: Preserved antibacterial activity in a family of heparin-binding growth factors during evolution. J. Biol. Chem. 2010, 285, 16105–16115. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Mierzchala, M.; Neubauer, K.; Durek, G.; Gamian, A. Midkine, a multifunctional cytokine, in patients with severe sepsis and septic shock: A pilot study. Shock 2011, 35, 471–477. [Google Scholar] [CrossRef]
- Chang, W.; Peng, F.; Sun, Q.; Meng, S.S.; Qiu, H.B.; Xu, J.Y. Plasma Midkine Is Associated With 28-Day Mortality and Organ Function in Sepsis. J. Intensive Care Med. 2020, 35, 1290–1296. [Google Scholar] [CrossRef]
- Xu, J.Y.; Chang, W.; Sun, Q.; Peng, F.; Yang, Y. Pulmonary midkine inhibition ameliorates sepsis induced lung injury. J. Transl. Med. 2021, 19, 91. [Google Scholar] [CrossRef]
- Sugito, S.; Hall, S.; Al-Omary, M.S.; De Malmanche, T.; Robertson, G.; Collins, N.; Boyle, A. Heparin Administration, but Not Myocardial Ischemia or Necrosis, Leads to Midkine Elevation. J. Cardiovasc. Transl. Res. 2020, 13, 741–743. [Google Scholar] [CrossRef]
- Yazihan, N. Midkine in inflammatory and toxic conditions. Curr. Drug Deliv. 2013, 10, 54–57. [Google Scholar] [CrossRef]
- Kadomatsu, K.; Bencsik, P.; Gorbe, A.; Csonka, C.; Sakamoto, K.; Kishida, S.; Ferdinandy, P. Therapeutic potential of midkine in cardiovascular disease. Br. J. Pharmacol. 2014, 171, 936–944. [Google Scholar] [CrossRef]
- Cohen, S.; Shachar, I. Midkine as a regulator of B cell survival in health and disease. Br. J. Pharmacol. 2014, 171, 888–895. [Google Scholar] [CrossRef]
- Hohlstein, P.; Brozat, J.F.; Schuler, J.; Abu Jhaisha, S.; Pollmanns, M.R.; Bundgens, L.; Wirtz, T.H.; Yagmur, E.; Hamesch, K.; Weiskirchen, R.; et al. Secreted Frizzled Related Protein 5 (SFRP5) Serum Levels Are Decreased in Critical Illness and Sepsis and Are Associated with Short-Term Mortality. Biomedicines 2023, 11, 313. [Google Scholar] [CrossRef]
- Yagmur, E.; Abu Jhaisha, S.; Buendgens, L.; Sapundzhieva, N.; Brozat, J.F.; Hohlstein, P.; Pollmanns, M.R.; Koek, G.H.; Weiskirchen, R.; Trautwein, C.; et al. Clusterin Plasma Concentrations Are Decreased in Sepsis and Inversely Correlated with Established Markers of Inflammation. Diagnostics 2022, 12, 3010. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Harris, C.R.; Millman, K.J.; van der Walt, S.J.; Gommers, R.; Virtanen, P.; Cournapeau, D.; Wieser, E.; Taylor, J.; Berg, S.; Smith, N.J.; et al. Array programming with NumPy. Nature 2020, 585, 357–362. [Google Scholar] [CrossRef] [PubMed]
- McKinney, W. Data Structures for Statistical Computing in Python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010. [Google Scholar]
- Hunter, J.D. Matplotlib: A 2D Graphics Environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Waskom, M.; Botvinnik, O.; O’Kane, D.; Hobson, P.; Lukauskas, S.; Gemperline, D.C.; Augspurger, T.; Halchenko, Y.; Cole, J.B.; Warmenhoven, J.; et al. Mwaskom/Seaborn: v0.8.1 (September 2017); Zenodo: Genève, Switzerland, 2017. [Google Scholar]
- Vallat, R. Pingouin: Statistics in Python. J. Open Source Softw. 2018, 3, 1026. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Müller, A.; Nothman, J.; Louppe, G.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Davidson-Pilon, C. lifelines: Survival analysis in Python. J. Open Source Softw. 2019, 4, 1317. [Google Scholar] [CrossRef]
- Kluyver, T.; Ragan-Kelley, B.; Pérez, F.; Granger, B.; Bussonnier, M.; Frederic, J.; Kelley, K.; Hamrick, J.; Grout, J.; Corlay, S.; et al. Jupyter Notebooks—A publishing format for reproducible computational workflows. In Proceedings of the 20th International Conference on Electronic Publishing: Players, Agents and Agendas, Göttingen, Germany, 7–9 June 2016; pp. 87–90. [Google Scholar]
- Van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2009. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients | Sepsis | Nonsepsis | p-Value |
|---|---|---|---|---|
| Number n | 192 | 125 | 67 | |
| Sex (male/female) n | 113/79 | 78/47 | 35/32 | 0.226 |
| Age (years) | 64.5 (18–89) | 65 (21–89) | 63 (18–87) | 0.663 |
| APACHE II score | 17 (2–40) | 18 (3–40) | 16 (2–37) | 0.039 * |
| SOFA score | 10 (0–18) | 11 (3–17) | 7 (0–18) | 0.006 * |
| Charlson Comorbidity index | 4 (0–16) | 4 (0–16) | 4 (0–13) | 0.297 |
| Mechanical ventilation n (%) | 130 (68.0) | 92 (73.6) | 38 (57.5) | 0.036 * |
| Vasopressor demand n (%) | 115 (62.2) | 84 (70.0) | 31 (47.7) | 0.005 * |
| ICU days n | 8 (1–137) | 10 (1–137) | 6 (2–44) | <0.001 * |
| Death in ICU n (%) | 52 (27.1) | 38 (30.4) | 14 (20.9) | 0.214 |
| 30-day mortality n (%) | 57 (34.5) | 41 (36.3) | 16 (30.8) | 0.606 |
| 1-year mortality n (%) | 88 (59.9) | 65 (64.4) | 23 (50.0) | 0.142 |
| Midkine (ng/mL) | 358 (19–1000) | 362 (19–1000) | 337 (19–1000) | 0.727 |
| Parameters | r | p-Value |
|---|---|---|
| Demographics | ||
| Age | 0.005 | 0.943 |
| Body mass index | 0.044 | 0.550 |
| Blood count and markers of inflammation | ||
| Leukocytes | 0.005 | 0.945 |
| Hemoglobin | 0.077 | 0.290 |
| Platelets | −0.024 | 0.747 |
| C-reactive Protein | 0.084 | 0.249 |
| Procalcitonin | 0.263 | 0.001 * |
| Interleukin 6 | 0.035 | 0.670 |
| Interleukin 10 | 0.054 | 0.594 |
| Electrolytes and renal system | ||
| Sodium | −0.066 | 0.362 |
| Potassium | 0.058 | 0.428 |
| Urea | 0.103 | 0.156 |
| Uric acid | 0.190 | 0.018 * |
| Creatinine | 0.197 | 0.006 * |
| Cystatin C | 0.231 | 0.010 * |
| Hepato-pancreatico-biliary system and coagulation | ||
| Protein, total | −0.020 | 0.803 |
| Albumin | −0.085 | 0.339 |
| INR | −0.058 | 0.432 |
| aPTT | 0.330 | <0.001 * |
| Bilirubin, total | 0.013 | 0.862 |
| γGT | 0.127 | 0.082 |
| AST | 0.256 | 0.001 * |
| ALT | 0.154 | 0.034 * |
| Lipase | 0.103 | 0.211 |
| Cardiopulmonary system | ||
| NTproBNP | 0.131 | 0.212 |
| Norepinephrine demand at day 1 (µg/day) | 0.055 | 0.456 |
| Horovitz quotient (PaO2/FiO2) | −0.047 | 0.710 |
| Ventilatory FiO2 demand | 0.079 | 0.527 |
| Net fluid balance day 1 | −0.021 | 0.776 |
| Net fluid balance day 3 | −0.062 | 0.450 |
| Metabolism | ||
| Glucose | 0.027 | 0.712 |
| HbA1c | 0.059 | 0.582 |
| Insulin | 0.229 | 0.031 * |
| C-Peptide | 0.254 | 0.016 * |
| HOMA IR | 0.161 | 0.133 |
| Cholesterol | 0.039 | 0.633 |
| HDL-cholesterol | −0.128 | 0.237 |
| LDL-cholesterol | −0.010 | 0.928 |
| Triglycerides | 0.084 | 0.303 |
| Disease severity parameters | ||
| Days on ICU | 0.046 | 0.526 |
| SOFA day 1 | −0.037 | 0.749 |
| SOFA day 3 | −0.059 | 0.668 |
| APACHE-II day 1 | 0.009 | 0.909 |
| APACHE-II day 3 | −0.104 | 0.420 |
| Etiology of (Non)Septic Critical Illness | Sepsis n = 125, n (%) | Nonsepsis n = 67, n (%) | Midkine (ng/L) | p |
|---|---|---|---|---|
| Pulmonary | 69 (55.2) | 425 (19–1000) | 0.481 | |
| Abdominal | 19 (15.2) | 105 (19–1000) | ||
| Urogenital | 10 (8) | 270 (22–1000) | ||
| Other | 27 (21.6) | 431 (19–1000) | ||
| Cardiocirculatory disorder | 13 (19.4) | 365 (19–1000) | 0.772 | |
| Respiratory failure | 10 (14.9) | 300 (19–1000) | ||
| Advanced liver disease | 13 (19.4) | 337 (19–1000) | ||
| Other | 31 (46.3) | 240 (19–1000) |
| Comorbidity | Midkine Concentration in ng/L, Median (Range) | p |
|---|---|---|
| Diabetes (n = 50) | 209 (19–1000) | 0.182 |
| Liver disease (n = 20) | 225 (19–1000) | 0.735 |
| Coronary artery disease (n = 63) | 379 (19–1000) | 0.617 |
| Hypertension (n = 75) | 462 (19–1000) | 0.162 |
| Chronic alcohol abuse (n = 25) | 337 (19–1000) | 0.543 |
| Chronic obstructive lung disease (n = 25) | 425 (19–1000) | 0.939 |
| Active malignancy (n = 23) | 151 (19–1000) | 0.302 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hohlstein, P.; Abu Jhaisha, S.; Yagmur, E.; Wawer, D.; Pollmanns, M.R.; Adams, J.K.; Wirtz, T.H.; Brozat, J.F.; Bündgens, L.; Hamesch, K.; et al. Elevated Midkine Serum Levels Are Associated with Long-Term Survival in Critically Ill Patients. Int. J. Mol. Sci. 2024, 25, 454. https://doi.org/10.3390/ijms25010454
Hohlstein P, Abu Jhaisha S, Yagmur E, Wawer D, Pollmanns MR, Adams JK, Wirtz TH, Brozat JF, Bündgens L, Hamesch K, et al. Elevated Midkine Serum Levels Are Associated with Long-Term Survival in Critically Ill Patients. International Journal of Molecular Sciences. 2024; 25(1):454. https://doi.org/10.3390/ijms25010454
Chicago/Turabian StyleHohlstein, Philipp, Samira Abu Jhaisha, Eray Yagmur, Dennis Wawer, Maike R. Pollmanns, Jule K. Adams, Theresa H. Wirtz, Jonathan F. Brozat, Lukas Bündgens, Karim Hamesch, and et al. 2024. "Elevated Midkine Serum Levels Are Associated with Long-Term Survival in Critically Ill Patients" International Journal of Molecular Sciences 25, no. 1: 454. https://doi.org/10.3390/ijms25010454
APA StyleHohlstein, P., Abu Jhaisha, S., Yagmur, E., Wawer, D., Pollmanns, M. R., Adams, J. K., Wirtz, T. H., Brozat, J. F., Bündgens, L., Hamesch, K., Weiskirchen, R., Tacke, F., Trautwein, C., & Koch, A. (2024). Elevated Midkine Serum Levels Are Associated with Long-Term Survival in Critically Ill Patients. International Journal of Molecular Sciences, 25(1), 454. https://doi.org/10.3390/ijms25010454