
Early Effects of Modern Radiotherapy for Lung Cancer on Endothelial Damage and Myocardial Fibrosis: A Prospective Single-Center Study

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Results
3. Methods
- Age over 18 years.
- Histopathological diagnosis of lung cancer.
- Future planned treatment with the use of radiochemotherapy or chemotherapy.
- Written consent of the patient to participate in the study.
- Future planned or previous surgical treatment of lung cancer.
- History of potentially cardiotoxic oncological treatment (radiotherapy, chemotherapy, or immunotherapy).
- Severe functional impairment (assessed using the Karnofsky Performance Scale).
- No written consent to participate in the study.
Statistical Analysis
4. Discussion
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koutroumpakis, E.; Deswal, A.; Yusuf, S.W.; Abe, J.-I.; Nead, K.T.; Potter, A.S.; Liao, Z.; Lin, S.H.; Palaskas, N.L. Radiation-Induced Cardiovascular Disease: Mechanisms, Prevention, and Treatment. Curr. Oncol. Rep. 2022, 24, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Wang, H.; Zhang, M.; Ji, R.; Wei, J.; Xin, Y.; Jiang, X. Radiation-induced myocardial fibrosis: Mechanisms underlying its pathogenesis and therapeutic strategies. J. Cell Mol. Med. 2020, 24, 7717–7729. [Google Scholar] [CrossRef] [PubMed]
- Wijerathne, H.; Langston, J.C.; Yang, Q.; Sun, S.; Miyamoto, C.; Kilpatrick, L.E.; Kiani, M.F. Mechanisms of radiation-induced endothelium damage: Emerging models and technologies. Radiother. Oncol. 2021, 158, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Moisander, M.; Skyttä, T.; Kivistö, S.; Huhtala, H.; Nikus, K.; Virtanen, V.; Kellokumpu-Lehtinen, P.L.; Raatikainen, P.; Tuohinen, S. Radiotherapy-induced diffuse myocardial fibrosis in early-stage breast cancer patients—Multimodality imaging study with six-year follow-up. Radiat. Oncol. 2023, 18, 124. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Poulin, F.; Lim, K.D.; Plana, J.C.; Woo, A.; Marwick, T.H. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: A systematic review. J. Am. Coll. Cardiol. 2014, 63 Pt A, 2751–2768. [Google Scholar] [CrossRef]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography. JACC Cardiovasc. Imaging 2019, 11 Pt 1, 260–274. [Google Scholar] [CrossRef]
- Omidi, A.; Weiss, E.; Trankle, C.R.; Rosu-Bubulac, M.; Wilson, J.S. Quantitative assessment of radiotherapy-induced myocardial damage using MRI: A systematic review. Cardiooncology 2023, 9, 24. [Google Scholar] [CrossRef]
- Ma, C.X.; Zhao, X.K.; Li, Y.D. New therapeutic insights into radiation-induced myocardial fibrosis. Ther. Adv. Chronic Dis. 2019, 10, 204062231986838. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 233–271.e14. [Google Scholar] [CrossRef]
- Duane, F.; Aznar, M.C.; Bartlett, F.; Cutter, D.J.; Darby, S.C.; Jagsi, R.; Lorenzen, E.L.; McArdle, O.; McGale, P.; Myerson, S.; et al. A cardiac contouring atlas for radiotherapy. Radiother. Oncol. 2017, 122, 416–422. [Google Scholar] [CrossRef]
- Adams, M.J.; Hardenbergh, P.H.; Constine, L.S.; Lipshultz, S.E. Radiation-associated cardiovascular disease. Crit. Rev. Oncol. Hematol. 2003, 45, 55–75. [Google Scholar] [CrossRef] [PubMed]
- Madan, R.; Benson, R.; Sharma, D.N.; Julka, P.K.; Rath, G.K. Radiation induced heart disease: Pathogenesis, management and review literature. J. Egypt. Natl. Canc Inst. 2015, 27, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Yarnold, J.; Vozenin Brotons, M.C. Pathogenetic mechanisms in radiation fibrosis. Radiother. Oncol. 2010, 97, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Nkomo, V.T.; Badano, L.P.; Bergler-Klein, J.; Bogaert, J.; Davin, L.; Cosyns, B.; Coucke, P.; Dulgheru, R.; Edvardsen, T.; et al. Expert consensus for multi-modality imaging evaluation of cardiovascular complications of radiotherapy in adults: A report from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 721–740. [Google Scholar] [CrossRef] [PubMed]
- Nellessen, U.; Zingel, M.; Hecker, H.; Bahnsen, J.; Borschke, D. Effects of Radiation Therapy on Myocardial Cell Integrity and Pump Function: Which Role for Cardiac Biomarkers? Chemotherapy 2010, 56, 147–152. [Google Scholar] [CrossRef]
- Palumbo, I.; Palumbo, B.; Fravolini, M.L.; Marcantonini, M.; Perrucci, E.; Latini, M.E.; Falcinelli, L.; Sabalich, I.; Tranfaglia, C.; Schillaci, G.; et al. Brain natriuretic peptide as a cardiac marker of transient radiotherapy-related damage in left-sided breast cancer patients: A prospective study. Breast 2016, 25, 45–50. [Google Scholar] [CrossRef]
- Demissei, B.G.; Freedman, G.; Feigenberg, S.J.; Plastaras, J.P.; Maity, A.; Smith, A.M.; McDonald, C.; Sheline, K.; Simone, C.B.; Lin, L.L.; et al. Early Changes in Cardiovascular Biomarkers with Contemporary Thoracic Radiation Therapy for Breast Cancer, Lung Cancer, and Lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 851–860. [Google Scholar] [CrossRef]
- Boulet, J.; Peña, J.; Hulten, E.A.; Neilan, T.G.; Dragomir, A.; Freeman, C.; Lambert, C.; Hijal, T.; Nadeau, L.; Brophy, J.M.; et al. Statin Use and Risk of Vascular Events Among Cancer Patients After Radiotherapy to the Thorax, Head, and Neck. J. Am. Heart Assoc. 2019, 8, e005996. [Google Scholar] [CrossRef] [PubMed]
- Susskind, H.; Hymowitz, M.H.; Lau, Y.H.; Atkins, H.L.; Hurewitz, A.N.; Valentine, E.S.; Meek, A.G.; Zucker, S. Increased plasma levels of matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 in lung and breast cancer are altered during chest radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 1161–1169. [Google Scholar] [CrossRef]
- Çelik, Ö.; Şahin, A.A.; Sarıkaya, S.; Uygur, B. Correlation between serum matrix metalloproteinase and myocardial fibrosis in heart failure patients with reduced ejection fraction: A retrospective analysis. Anatol. J. Cardiol. 2020, 24, 303–308. [Google Scholar]
- Jafarian, A.H.; Kooshki Forooshani, M.; Reisi, H.; Mohamadian Roshan, N. Matrix metalloproteinase-9 (MMP-9) Expression in Non-Small Cell Lung Carcinoma and Its Association with Clinicopathologic Factors. Iran. J. Pathol. 2020, 15, 326–333. [Google Scholar] [CrossRef] [PubMed]
- El-Badrawy, M.K.; Yousef, A.M.; Shaalan, D.; Elsamanoudy, A.Z. Matrix Metalloproteinase-9 Expression in Lung Cancer Patients and Its Relation to Serum MMP-9 Activity, Pathologic Type, and Prognosis. J. Bronchol. Interv. Pulmonol. 2014, 21, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Ogata, Y.; Matono, K.; Sasatomi, T.; Ishibashi, N.; Ohkita, A.; Mizobe, T.; Ogo, S.; Ikeda, S.; Ozasa, H.; Shirouzu, K. The MMP-9 expression determined the efficacy of postoperative adjuvant chemotherapy using oral fluoropyrimidines in stage II or III colorectal cancer. Cancer Chemother. Pharmacol. 2006, 57, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.; Wirtz, R.M.; Pauligk, C.; Steinmetz, K.; Probst, S.; Hartmann, J.T.; Hofheinz, R.; Altmannsberger, H.M.; Petry, C.; Jäger, E. Association of elevated matrix metalloproteinase-9 (MMP-9) mRNA expression levels with resistance to chemotherapy survival in patients with metastatic gastric cancer receiving first-line chemotherapy: Results from the FLO versus FLP gastric cancer phase III trial of the, A.I.O. J. Clin. Oncol. 2008, 26 (Suppl. S15), 4544. [Google Scholar]
- Venkatesulu, B.P.; Mahadevan, L.S.; Aliru, M.L.; Yang, X.; Bodd, M.H.; Singh, P.K.; Yusuf, S.W.; Abe, J.-I.; Krishnan, S. Radiation-Induced Endothelial Vascular Injury. JACC Basic Transl. Sci. 2018, 3, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Sievert, W.; Trott, K.R.; Azimzadeh, O.; Tapio, S.; Zitzelsberger, H.; Multhoff, G. Late proliferating and inflammatory effects on murine microvascular heart and lung endothelial cells after irradiation. Radiother. Oncol. 2015, 117, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Willeit, K.; Pechlaner, R.; Willeit, P.; Skroblin, P.; Paulweber, B.; Schernthaner, C.; Toell, T.; Egger, G.; Weger, S.; Oberhollenzer, M.; et al. Association Between Vascular Cell Adhesion Molecule 1 and Atrial Fibrillation. JAMA Cardiol. 2017, 2, 516–523. [Google Scholar] [CrossRef]
- Aznar, M.C.; Korreman, S.S.; Pedersen, A.N.; Persson, G.F.; Josipovic, M.; Specht, L. Evaluation of dose to cardiac structures during breast irradiation. Br. J. Radiol. 2011, 84, 743–746. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 43) | Study Group (n = 23) | Control Group (n = 20) | p Value |
|---|---|---|---|---|
| Age, years | 64.9 ± 8.1 | 64.4 ± 8.6 | 65.5 ± 7.5 | 0.68 |
| Males, n (%) | 25 (58.1%) | 13 (56.5%) | 12 (60.0%) | 0.82 |
| Comorbidities, n (%): | ||||
| Arterial hypertension | 26 (60.5%) | 14 (60.1%) | 12 (60.0%) | 1.00 |
| Coronary artery disease | 7 (16.3%) | 3 (13.0%) | 4 (20.0%) | 0.69 |
| Heart failure | 6 (13.9%) | 3 (13.0%) | 3 (15.0%) | 0.32 |
| Atrial fibrillation | 14 (32.6%) | 6 (26.1%) | 8 (40.0%) | 0.10 |
| Hypercholesterolemia | 7 (16.3%) | 6 (26.1%) | 1 (5.0%) | 0.52 |
| Diabetes | 1 (2.3%) | 1 (4.3%) | 0 | 0.10 |
| Chronic renal failure | 5 (11.6%) | 2 (8.7%) | 3 (15.0%) | 1.00 |
| Chronic obstructive pulmonary disease | 5 (11.6%) | 2 (8.7%) | 3 (15.0%) | 1.00 |
| Charlson Comorbidity Index, median | 2 (0–6) | 1 (0–3) | 6 (2–7) | 0.029 |
| Smoking history, n (%): | 1.00 | |||
| Current | 12 (27.9%) | 6 (26.1%) | 6 (30%) | |
| Former | 27 (62.8%) | 15 (65.2%) | 12 (60%) | |
| Never | 4 (9.3%) | 2 (8.7%) | 2 (10%) | |
| Number of pack years, n | 37.5 ± 20.2 | 38.5 ± 20.6 | 36.3 ± 20.2 | 0.73 |
| Histological type of lung cancer, n (%): | ||||
| Adenocarcinoma | 20 (46.5%) | 9 (39.1%) | 11 (55.0%) | 0.077 |
| Squamous cell carcinoma | 20 (46.5%) | 14 (60.1%) | 6 (30.0%) | |
| Small cell lung cancer | 2 (4.7%) | 0 | 2 (10.0%) | |
| Carcinoma not otherwise specified | 1 (2.3%) | 0 | 1 (5.0%) | |
| Chemotherapy drugs, n (%): | ||||
| Pemetrexed | 17 (39.5%) | 7 (30.4%) | 10 (50%) | 0.190 |
| Cisplatin | 19 (44.2%) | 13 (56.5%) | 16 (80%) | 0.101 |
| Carboplatin | 15 (34.9%) | 5 (21.7%) | 10 (50%) | 0.052 |
| Paclitaxel | 10 (23.2%) | 5 (21.7%) | 5 (25%) | 0.798 |
| Etoposide | 4 (9.3%) | 3 (13%) | 1 (5%) | 0.367 |
| Vinorelbine | 4 (9.3%) | 2 (8.7%) | 2 (10%) | 0.084 |
| Docetaxel | 2 (4.6%) | 0 | 2 (10%) | 0.120 |
| Radiotherapy characteristics | ||||
| RT duration, days | N/A | 40 (40–40) | N/A | |
| Total RT dose, Gy | 66 (63–66) | |||
| Number of RT fractions | 30 (30–30) | |||
| RT technique: | ||||
| IMRT, n (%) | 14 (60.9%) | |||
| VMAT, n (%) | 9 (39.1%) | |||
| Heart dose, Gy | 9.7 (6.7–13.2) | |||
| Death, n (%): | 9 (20.9%) | 5 (21.7%) | 4 (20%) | 1.00 |
| Variable | All Patients (n = 43) | ||||
|---|---|---|---|---|---|
| Baseline | Immediately after Treatment | p Value | Three Months after Treatment | p Value (vs. Baseline) | |
| BNP [pg/mL] | 66.6 ± 63.8 | 78.6 ± 87.1 | 0.16 | 47.9 ± 38.6 | 0.71 |
| hs-TnI [ng/mL] | 0.003 ± 0.003 | 0.005 ± 0.014 | 0.16 | 0.003 ± 0.004 | 0.5 |
| Creatinine [mg/dL] | 0.80 ± 0.17 | 0.79 ± 0.17 | 0.48 | 0.87 ± 0.25 | 0.041 |
| Total cholesterol [mg/dL] | 171.1 ± 48.3 | 184.4 ± 40.2 | 0.003 | 184.4 ± 40.2 | 0.002 |
| LDL [mg/dL] | 105.6 ± 37.0 | 106.3 ± 41.0 | 0.55 | 109.6 ± 39.4 | 0.3 |
| VCAM-1 [ng/mL] | 805.21 ± 367.68 | 720.98 ± 247.63 | 0.87 | 774.45 ± 278.75 | 0.98 |
| ICAM-1 [ng/mL] | 1271.22 ± 427.28 | 1382.40 ± 492.28 | 0.021 | 1152.93 ± 403.71 | 0.37 |
| MMP-9 [ng/mL] | 259.12 ± 245.90 | 165.67 ± 144.60 | 0.005 | 120.28 ± 74.67 | 0.005 |
| TIMP-1 [ng/mL] | 195.47 ± 181.74 | 203.79 ± 281.45 | 0.41 | 117.77 ± 123.90 | 0.041 |
| Variable | Study group (n = 23) | ||||
| BNP [pg/mL] | 71.1 ± 56.4 | 87.6 ± 94.2 | 0.70 | 52.0 ± 38.7 | 0.20 |
| hs-TnI [ng/mL] | 0.003 ± 0.003 | 0.004 ± 0.004 | 0.17 | 0.004 ± 0.006 | 0.1 |
| Creatinine [mg/dL] | 0.84 ± 0.20 | 0.84 ± 0.20 | 0.28 | 0.93 ± 0.22 | 0.12 |
| Total cholesterol [mg/dL] | 177.3 ± 45.1 | 195.5 ± 60.7 | 0.022 | 189.4 ± 39.4 | 0.025 |
| LDL [mg/dL] | 107.2 ± 39.1 | 119.4 ± 47.5 | 0.048 | 107.6 ± 35.0 | 0.95 |
| VCAM-1 [ng/mL] | 765.17 ± 346.00 | 744.93 ± 304.18 | 0.68 | 768.53 ± 372.08 | 0.73 |
| ICAM-1 [ng/mL] | 1272.75 ± 397.71 | 1506.89 ± 545.72 | 0.008 | 1109.60 ± 369.23 | 0.28 |
| MMP-9 [ng/mL] | 283.88 ± 311.60 | 175.02 ± 176.26 | 0.21 | 131.54 ± 83.60 | 0.13 |
| TIMP-1 [ng/mL] | 203.09 ± 213.47 | 249.49 ± 373.56 | 0.63 | 130.29 ± 164.69 | 0.11 |
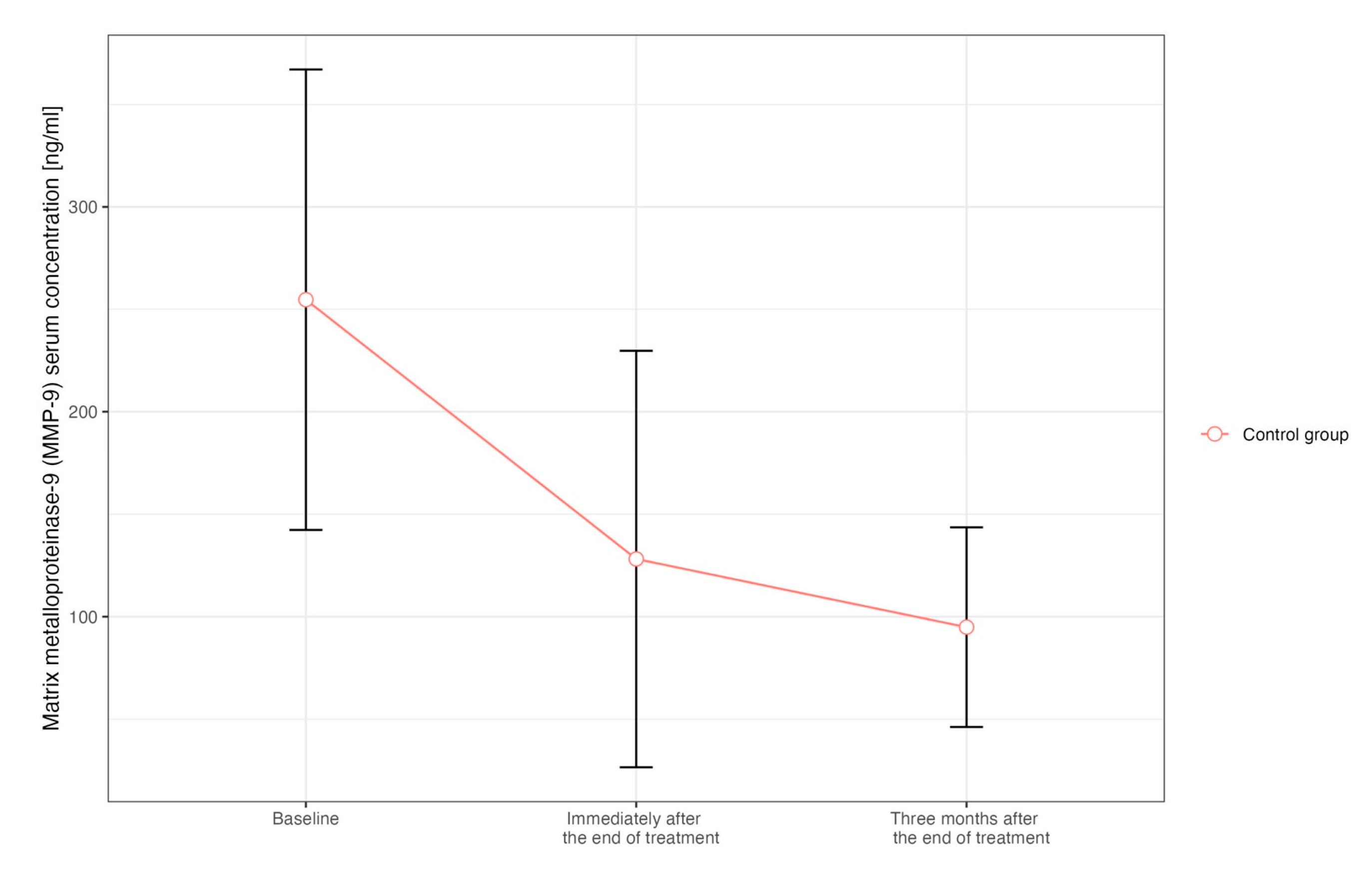
| Variable | Control group (n = 20) | ||||
| BNP [pg/mL] | 61.7 ± 72.3 | 69.1 ± 81.0 | 0.13 | 43.2 ± 39.4 | 0.53 |
| hs-TnI [ng/mL] | 0.003 ± 0.004 | 0.007 ± 0.019 | 0.46 | 0.001 ± 0.001 | 0.18 |
| Creatinine [mg/dL] | 0.75 ± 0.13 | 0.74 ± 0.12 | 0.88 | 0.81 ± 0.28 | 0.16 |
| Total cholesterol [mg/dL] | 164.1 ± 32.6 | 179.7 ± 30.0 | 0.037 | 179.1 ± 41.8 | 0.028 |
| LDL [mg/dL] | 103.7 ± 35.2 | 97.0 ± 26.5 | 0.19 | 111.6 ± 44.6 | 0.22 |
| VCAM-1 [ng/mL] | 851.25 ± 395.03 | 695.624 ± 175.11 | 0.49 | 780.79 ± 134.84 | 0.70 |
| ICAM-1 [ng/mL] | 1269.45 ± 469.49 | 1250.59 ± 403.29 | 0.80 | 1199.36 ± 446.90 | 0.88 |
| MMP-9 [ng/mL] | 230.64 ± 140.16 | 155.77 ± 105.93 | 0.004 | 108.22 ± 64.65 | 0.022 |
| TIMP-1 [ng/mL] | 186.70 ± 139.99 | 155.39 ± 123.63 | 0.47 | 104.34 ± 59.00 | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sławiński, G.; Hawryszko, M.; Lasocka-Koriat, Z.; Romanowska, A.; Myszczyński, K.; Wrona, A.; Ogłoza, A.; Daniłowicz-Szymanowicz, L.; Lewicka, E. Early Effects of Modern Radiotherapy for Lung Cancer on Endothelial Damage and Myocardial Fibrosis: A Prospective Single-Center Study. Int. J. Mol. Sci. 2024, 25, 6705. https://doi.org/10.3390/ijms25126705
Sławiński G, Hawryszko M, Lasocka-Koriat Z, Romanowska A, Myszczyński K, Wrona A, Ogłoza A, Daniłowicz-Szymanowicz L, Lewicka E. Early Effects of Modern Radiotherapy for Lung Cancer on Endothelial Damage and Myocardial Fibrosis: A Prospective Single-Center Study. International Journal of Molecular Sciences. 2024; 25(12):6705. https://doi.org/10.3390/ijms25126705
Chicago/Turabian StyleSławiński, Grzegorz, Maja Hawryszko, Zofia Lasocka-Koriat, Anna Romanowska, Kamil Myszczyński, Anna Wrona, Agata Ogłoza, Ludmiła Daniłowicz-Szymanowicz, and Ewa Lewicka. 2024. "Early Effects of Modern Radiotherapy for Lung Cancer on Endothelial Damage and Myocardial Fibrosis: A Prospective Single-Center Study" International Journal of Molecular Sciences 25, no. 12: 6705. https://doi.org/10.3390/ijms25126705
APA StyleSławiński, G., Hawryszko, M., Lasocka-Koriat, Z., Romanowska, A., Myszczyński, K., Wrona, A., Ogłoza, A., Daniłowicz-Szymanowicz, L., & Lewicka, E. (2024). Early Effects of Modern Radiotherapy for Lung Cancer on Endothelial Damage and Myocardial Fibrosis: A Prospective Single-Center Study. International Journal of Molecular Sciences, 25(12), 6705. https://doi.org/10.3390/ijms25126705