
New Modifiable Risk Factors Influencing Coronary Artery Disease Severity

Abstract
:1. Introduction
2. Syntax Score
3. Inflammation Biomarkers
3.1. C-Reactive Protein (CRP)
3.2. Indicators Involving Neutrophil Levels
3.3. Systemic Immune-Inflammation Index (SII)
3.4. Uric Acid (UA)
3.5. Anti-Inflammatory Therapy as a Secondary Prevention of CAD
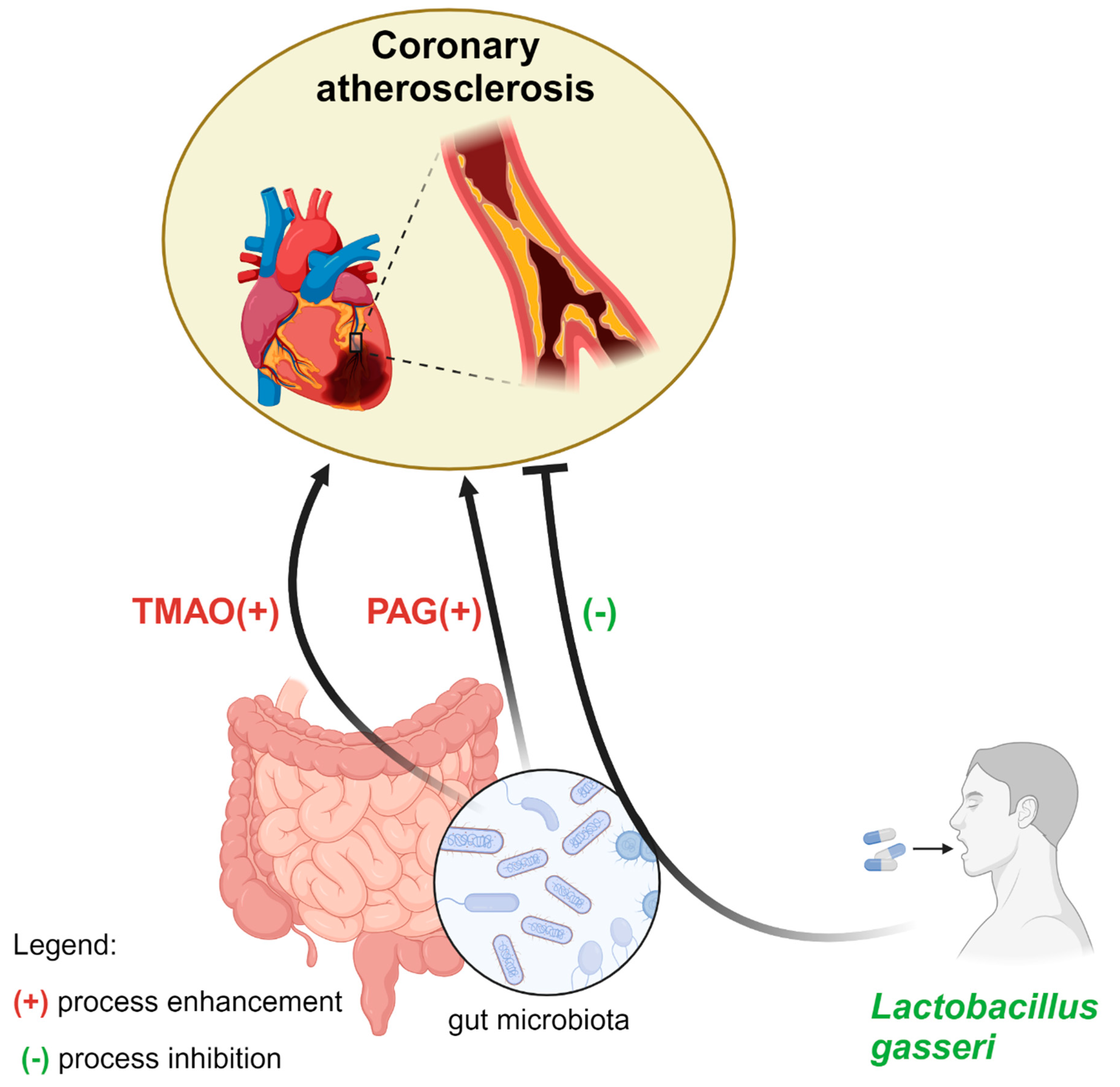
4. Microbiota Alternation
4.1. Lactobacillus
4.2. Trimethylamine N-Oxide (TMAO)
4.3. Phenylacetylglutamine (PAG)
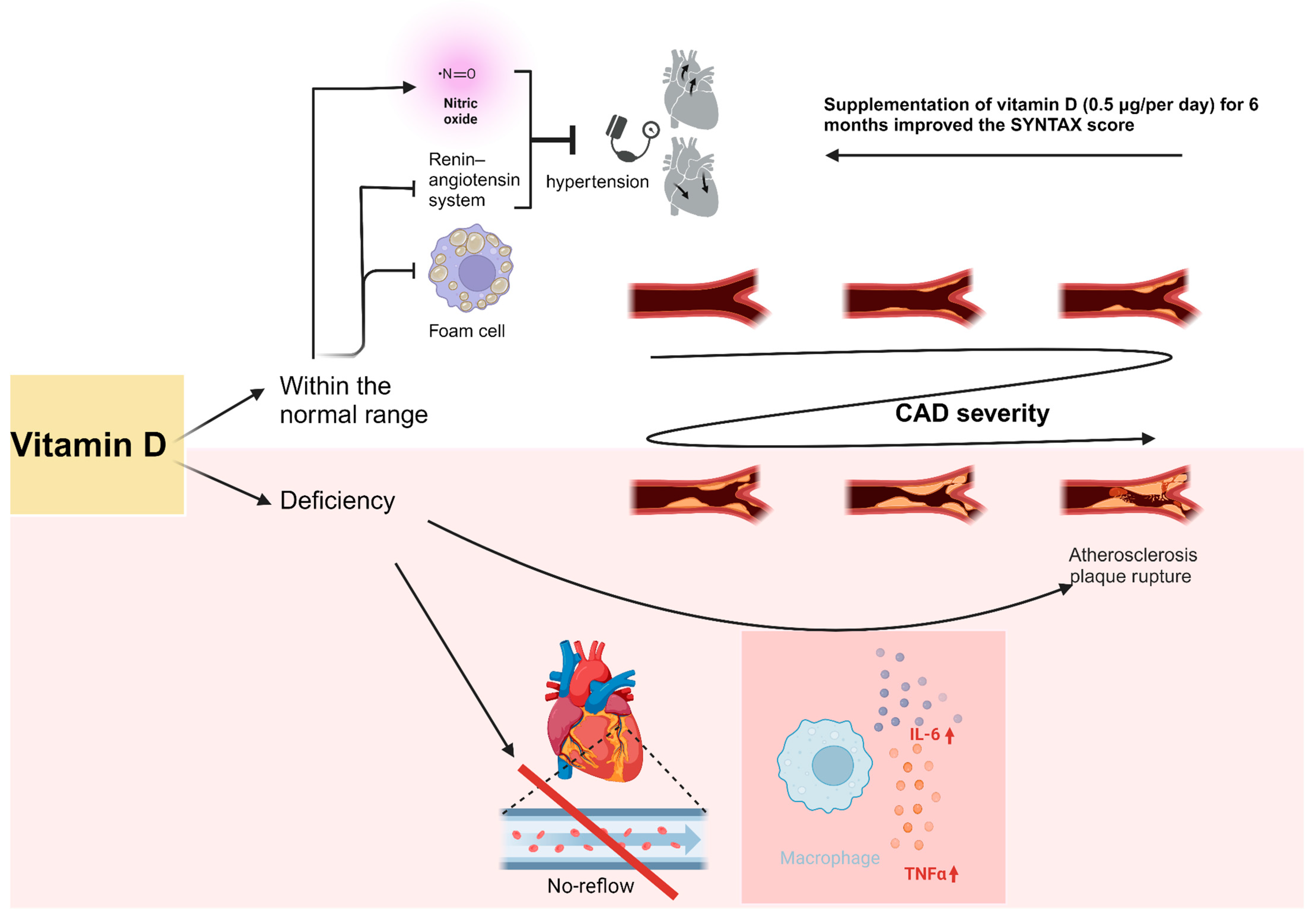
5. Vitamin D
6. Sleep Apnea
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mensah, G.A.; Fuster, V.; Murray, C.J.L.; Roth, G.A. Global Burden of Cardiovascular Diseases and Risks, 1990–2022. J. Am. Coll. Cardiol. 2023, 82, 2350–2473. [Google Scholar] [CrossRef]
- ESC Guidelines on Chronic Coronary Syndromes (Previously titled Stable Coronary Artery Disease). Available online: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Chronic-Coronary-Syndromes (accessed on 18 May 2024).
- Ralapanawa, U.; Sivakanesan, R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J. Epidemiol. Glob. Health 2021, 11, 169–177. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the Epidemiology of Cardiovascular Diseases: A Historical Perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Gerhardt, T.E.; Kwon, E. Risk Factors for Coronary Artery Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: http://www.ncbi.nlm.nih.gov/books/NBK554410/ (accessed on 18 May 2024).
- Özcan, C.; Deleskog, A.; Schjerning Olsen, A.M.; Nordahl Christensen, H.; Lock Hansen, M.; Hilmar Gislason, G. Coronary artery disease severity and long-term cardiovascular risk in patients with myocardial infarction: A Danish nationwide register-based cohort study. Eur. Heart J. Cardiovasc. Pharmacother. 2018, 4, 25–35. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; Verardi, R.; Visconti, M.; Conrotto, F.; Scacciatell, P.; Dziewierz, A.; Stefanini, G.G.; Paradis, J.M.; Omedè, P.; Kodali, S.; et al. Independent impact of extent of coronary artery disease and percutaneous revascularisation on 30-day and one-year mortality after TAVI: A meta-analysis of adjusted observational results. EuroIntervention 2018, 14, e1169–e1177. [Google Scholar] [CrossRef]
- Yang, H.; Zhang, L.; Xu, C.H. Use of the SYNTAX Score II to predict mortality in interventional cardiology: A systematic review and meta-analysis. Medicine 2019, 98, e14043. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, P.J.N.; Falcão, J.L.d.A.A.; Falcão, B.d.A.A.; Rocha, H.A.L. Stent versus Coronary Artery Bypass Surgery in Multi-Vessel and Left Main Coronary Artery Disease: A Meta-Analysis of Randomized Trials with Subgroups Evaluation. Arq. Bras. Cardiol. 2019, 112, 511–523. [Google Scholar] [CrossRef]
- Sianos, G.; Morel, M.A.; Kappetein, A.; Morice, M.C.; Colombo, A.; Dawkins, K.D.; Van Den Brand, M.; Van Dyck, N.; Russell, M.; Serruys, P.W. The SYNTAX Score: An Angiographic Tool Grading the Complexity of Coronary Artery Disease. Eurointervention. Available online: https://eurointervention.pcronline.com/article/the-syntax-score-an-angiographic-tool-grading-the-complexity-of-coronary-artery-disease (accessed on 18 May 2024).
- Cavalcante, R.; Onuma, Y.; Sotomi, Y.; Collet, C.; Thomsen, B.; Rogers, C.; Zeng, Y.; Tenekecioglu, E.; Asano, T.; Miyasaki, Y.; et al. Non-invasive Heart Team assessment of multivessel coronary disease with coronary computed tomography angiography based on SYNTAX score II treatment recommendations: Design and rationale of the randomised SYNTAX III Revolution trial. EuroIntervention 2017, 12, 2001–2008. [Google Scholar] [CrossRef]
- Omidi, N.; Sadeghian, S.; Salarifar, M.; Jalali, A.; Abbasi, S.H.; Yavari, N.; Ghorashi, S.M.; Alidoosti, M.; Poorhosseini, H. Relationship between the Severity of Coronary Artery Disease and Cardiovascular Risk Factors in Acute Coronary Syndrome: Based on Tehran Heart Center’s Data Registry. J. Tehran Heart Cent. 2020, 15, 165–170. [Google Scholar] [CrossRef]
- Dhindsa, D.S.; Sandesara, P.B.; Shapiro, M.D.; Wong, N.D. The evolving understanding and approach to residual cardiovascular risk management. Front. Cardiovasc. Med. 2020, 7, 88. [Google Scholar] [CrossRef]
- Siniawski, D.; Masson, G.; Masson, W.; Barbagelata, L.; Destaville, J.; Lynch, S.; Vitagliano, L.; Parodi, J.B.; Berton, F.; Indavere, A.; et al. Residual cardiovascular risk, use of standard care treatments, and achievement of treatment goals in patients with cardiovascular disease. Int. J. Cardiol. Cardiovasc. Risk Prev. 2023, 18, 200198. [Google Scholar] [CrossRef]
- Ikeno, F.; Brooks, M.M.; Nakagawa, K.; Kim, M.K.; Kaneda, H.; Mitsutake, Y.; Vlachos, H.A.; Schwartz, L.; Frye, R.L.; Kelsey, S.F.; et al. SYNTAX Score and Long-Term Outcomes. J. Am. Coll. Cardiol. 2017, 69, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D. Syntax Score: Reaching Optimal Revascularisation for Complex Coronary Artery Disease. Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-8/Syntax-score-reaching-optimal-revascularisation-for-complex-coronary-artery-di (accessed on 18 May 2024).
- Morice, M.C.; Serruys, P.W.; Kappetein, A.P.; Feldman, T.E.; Ståhle, E.; Colombo, A.; Mack, M.J.; Holmes, D.R.; Choi, J.W.; Ruzyllo, W.; et al. Five-year outcomes in patients with left main disease treated with either percutaneous coronary intervention or coronary artery bypass grafting in the synergy between percutaneous coronary intervention with taxus and cardiac surgery trial. Circulation 2014, 129, 2388–2394. [Google Scholar] [CrossRef] [PubMed]
- Sotomi, Y.; Cavalcante, R.; Van Klaveren, D.; Ahn, J.M.; Lee, C.W.; De Winter, R.J.; Wykrzykowska, J.J.; Onuma, Y.; Steyerberg, E.W.; Park, S.J.; et al. Individual Long-Term Mortality Prediction Following Either Coronary Stenting or Bypass Surgery in Patients With Multivessel and/or Unprotected Left Main Disease: An External Validation of the SYNTAX Score II Model in the 1,480 Patients of the BEST and PRECOMBAT Randomized Controlled Trials. JACC Cardiovasc. Interv. 2016, 9, 1564–1572. [Google Scholar] [CrossRef] [PubMed]
- Farooq, V.; van Klaveren, D.; Steyerberg, E.W.; Meliga, E.; Vergouwe, Y.; Chieffo, A.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.; et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: Development and validation of SYNTAX score II. Lancet 2013, 381, 639–650. [Google Scholar] [CrossRef] [PubMed]
- Farooq, V.; Vergouwe, Y.; Räber, L.; Vranckx, P.; Garcia-Garcia, H.; Diletti, R.; Kappetein, A.P.; Morel, M.A.; De Vries, T.; Swart, M.; et al. Combined anatomical and clinical factors for the long-term risk stratification of patients undergoing percutaneous coronary intervention: The Logistic Clinical SYNTAX score. Eur. Heart J. 2012, 33, 3098–3104. [Google Scholar] [CrossRef] [PubMed]
- Madeira, S.; Raposo, L.; Brito, J.; Rodrigues, R.; Gonçalves, P.; Teles, R.; Gabriel, H.; Machado, F.; Almeida, M.; Mendes, M. Potential Utility of the SYNTAX Score 2 in Patients Undergoing Left Main Angioplasty. Arq. Bras. Cardiol. 2016, 106, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Bertaina, M.; De Filippo, O.; Iannaccone, M.; Colombo, A.; Stone, G.; Serruys, P.; Mancone, M.; Omedè, P.; Conrotto, F.; Pennone, M.; et al. Percutaneous coronary intervention or coronary artery bypass graft in left main coronary artery disease: A comprehensive meta-analysis of adjusted observational studies and randomized controlled trials. J. Cardiovasc. Med. 2018, 19, 554–563. [Google Scholar] [CrossRef]
- D’Ascenzo, F.; De Filippo, O.; Elia, E.; Doronzo, M.P.; Omedè, P.; Montefusco, A.; Pennone, M.; Salizzoni, S.; Conrotto, F.; Gallone, G.; et al. Percutaneous vs. surgical revascularization for patients with unprotected left main stenosis: A meta-analysis of 5-year follow-up randomized controlled trials. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Brener, S.J.; Alapati, V.; Chan, D.; Da-Wariboko, A.; Kaid, Y.; Latyshev, Y.; Moussa, A.; Narayanan, C.A.; O’Laughlin, J.P.; Raizada, A.; et al. The SYNTAX II Score Predicts Mortality at 4 Years in Patients Undergoing Percutaneous Coronary Intervention. J. Invasive Cardiol. 2018, 30, 290–294. [Google Scholar]
- Guedeney, P.; Barthélémy, O.; Zeitouni, M.; Hauguel-Moreau, M.; Hage, G.; Kerneis, M.; Lattuca, B.; Overtchouk, P.; Rouanet, S.; Fuernau, G.; et al. Prognostic Value of SYNTAX Score in Patients With Infarct-Related Cardiogenic Shock: Insights From the CULPRIT-SHOCK Trial. JACC Cardiovasc. Interv. 2020, 13, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Girasis, C.; Garg, S.; Räber, L.; Sarno, G.; Morel, M.A.; Garcia-Garcia, H.M.; Lüscher, T.F.; Serruys, P.W.; Windecker, S. SYNTAX score and Clinical SYNTAX score as predictors of very long-term clinical outcomes in patients undergoing percutaneous coronary interventions: A substudy of SIRolimus-eluting stent compared with pacliTAXel-eluting stent for coronary revascularization (SIRTAX) trial. Eur. Heart J. 2011, 32, 3115–3127. [Google Scholar] [CrossRef]
- Chen, H.Y.; Dina, C.; Small, A.; Shaffer, C.; Levinson, R.; Helgadóttir, A.; Capoulade, R.; Munter, H.M.; Martinsson, A.; Cairns, B.; et al. Dyslipidemia, inflammation, calcification, and adiposity in aortic stenosis: A genome-wide study. Eur. Heart J. 2023, 44, 1927–1939. [Google Scholar] [CrossRef]
- Runjic, F.; Martinovic-Kaliterna, D.; Salamunic, I.; Kristic, I.; Ljubkovic, M.; Marinovic, J. Association of anticardiolipin antibodies, complement and leptin with the severity of coronary artery disease expressed as syntax score. J. Physiol. Pharmacol. 2020, 71, 383–388. [Google Scholar] [CrossRef]
- Lorenzatti, A.; Servato, M.L. Role of anti-inflammatory interventions in coronary artery disease: Understanding the Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS). Eur. Cardiol. 2018, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; HK, S.; Xu, X.F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef]
- Kuppa, A.; Tripathi, H.; Al-Darraji, A.; Tarhuni, W.M.; Abdel-Latif, A. C-Reactive Protein Levels and Risk of Cardiovascular Diseases: A Two-Sample Bidirectional Mendelian Randomization Study. Int. J. Mol. Sci. 2023, 24, 9129. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Harbord, R.M.; Timpson, N.J.; Lowe, G.D.O.; Rumley, A.; Gaunt, T.R.; Baker, I.; Yarnell, J.W.G.; Kivimäki, M.; Kumari, M.; et al. The association of C-reactive protein and CRP genotype with coronary heart disease: Findings from five studies with 4,610 cases amongst 18,637 participants. PLoS ONE 2008, 3, e3011. [Google Scholar] [CrossRef]
- Kaptoge, S.; Di Angelantonio, E.; Lowe, G.; Pepys, M.B.; Thompson, S.G.; Collins, R.; Danesh, J. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: An individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [CrossRef]
- Akboga, M.K.; Inanc, I.H.; Sabanoglu, C.; Akdi, A.; Yakut, I.; Yuksekkaya, B.; Nurkoc, S.; Yalcin, R. Systemic Immune-Inflammation Index and C-Reactive Protein/Albumin Ratio Could Predict Acute Stent Thrombosis and High SYNTAX Score in Acute Coronary Syndrome. Angiology 2023, 74, 693–701. [Google Scholar] [CrossRef]
- Ozdemir, B. Correlation of C-Reactive Protein and Serum Iron Levels with Syntax Score. Arch. Razi Inst. 2020, 75, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Kushner, I.; Broder, M.L.; Karp, D. Control of the acute phase response. Serum C-reactive protein kinetics after acute myocardial infarction. J. Clin. Investig. 1978, 61, 235–242. [Google Scholar] [CrossRef]
- Liu, Y.; Jia, S.D.; Yao, Y.; Tang, X.F.; Xu, N.; Jiang, L.; Gao, Z.; Chen, J.; Yang, Y.J.; Gao, R.L.; et al. Impact of high-sensitivity C-reactive protein on coronary artery disease severity and outcomes in patients undergoing percutaneous coronary intervention. J. Cardiol. 2020, 75, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Thomassen, J.Q.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Frikke-Schmidt, R. Neutrophil counts and cardiovascular disease. Eur. Heart J. 2023, 44, 4953–4964. [Google Scholar] [CrossRef]
- Silvestre-Roig, C.; Braster, Q.; Ortega-Gomez, A.; Soehnlein, O. Neutrophils as regulators of cardiovascular inflammation. Nat. Rev. Cardiol. 2020, 17, 327–340. [Google Scholar] [CrossRef]
- Bedel, C.; Korkut, M.; Aksoy, F.; Kuş, G. Usefulness of Immature Granulocytes to Predict High Coronary SYNTAX Score in Acute Coronary Syndrome; a Cross-sectional Study. Arch. Acad. Emerg. Med. 2020, 8, e73. [Google Scholar]
- Balta, S.; Celik, T.; Mikhailidis, D.P.; Ozturk, C.; Demirkol, S.; Aparci, M.; Iyisoy, A. The Relation Between Atherosclerosis and the Neutrophil–Lymphocyte Ratio. Clin. Appl. Thromb. Hemost. 2016, 22, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Good, E.; Åkerman, L.; Nyström, S.; Jonasson, L.; Ernerudh, J.; de Muinck, E. Changes in natural killer and T lymphocyte phenotypes in response to cardiovascular risk management. Sci. Rep. 2023, 13, 20810. [Google Scholar] [CrossRef]
- Li, X.; Ji, Y.; Kang, J.; Fang, N. Association between blood neutrophil-to-lymphocyte ratio and severity of coronary artery disease evidence from 17 observational studies involving 7017 cases. Medicine 2018, 97, e12432. [Google Scholar] [CrossRef]
- Maleki, M.; Tajlil, A.; Separham, A.; Sohrabi, B.; Pourafkari, L.; Roshanravan, N.; Aslanabadi, N.; Najjarian, F.; Mashayekhi, S.; Ghaffari, S. Association of neutrophil to lymphocyte ratio (NLR) with angiographic SYNTAX score in patients with non-ST-Segment elevation acute coronary syndrome (NSTE-ACS). J. Cardiovasc. Thorac. Res. 2021, 13, 216–221. [Google Scholar] [CrossRef]
- Mohanty, V.; Sharma, S.; Goswami, S.; Kaushik, A.; Choudhary, R.; Yadav, D.; Deora, S.; Singh, K. Association of Novel Hematological Indices with Severity of Coronary Artery Disease using SYNTAX Score in Patients with Acute Coronary Syndrome. Cardiovasc. Hematol. Disord. Drug Targets 2023, 23, 202–211. [Google Scholar] [CrossRef]
- Kahraman, S.; Agus, H.Z.; Avci, Y.; Serbest, N.G.; Guner, A.; Erturk, M. The Neutrophil to Lymphocyte Ratio (NLR) Is Associated With Residual Syntax Score in Patients With ST-Segment Elevation Myocardial Infarction. Angiology 2021, 72, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Zhu, S.; Wang, Y.; Zhao, Y.; Yan, K.; Li, X.; Wang, X.; He, C.; Ding, C.; Chen, Y.; et al. Effect of inflammation on association between cancer and coronary artery disease. BMC Cardiovasc. Disord. 2024, 24, 72. [Google Scholar] [CrossRef]
- Zhu, S.N.; Sun, M.Z.; Wang, Y.H.; Sun, Z.J.; Chen, Y.D.; Hu, S.Y. Association between digestive tract cancer and severity of coronary artery disease. Zhonghua Yi Xue Za Zhi 2023, 103, 3410–3415. [Google Scholar] [CrossRef] [PubMed]
- Kose, N.; Akin, F.; Yildirim, T.; Ergun, G.; Altun, I. The association between the lymphocyte-to-monocyte ratio and coronary artery disease severity in patients with stable coronary artery disease. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 2570–2575. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Tajlil, A.; Separham, A.; Sohrabi, B.; Pourafkari, L.; Roshanravan, N.; Aslanabadi, N.; Ziaee, M.; Mashayekhi, S.; Ghaffari, S. Association between Neutrophil-to-Lymphocyte Ratio and the Systemic Inflammatory Immunologic Index and the Angiographic SYNTAX Score and the TIMI Flow Grade in Acute STEMI: A Cohort Study. J. Tehran Heart Cent. 2021, 16, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Zhang, W.; Li, X.; Chen, Z.; Yang, Y.; Wang, G. Sex Difference in the Association Between Neutrophil to Lymphocyte Ratio and Severity of Coronary Artery Disease. Angiology 2022, 73, 470–477. [Google Scholar] [CrossRef]
- Vural, S.; Muhtaroğlu, A.; Güngör, M. Systemic immune-inflammation index: A new marker in differentiation of different thyroid diseases. Medicine 2023, 102, e34596. [Google Scholar] [CrossRef]
- Massberg, S.; Brand, K.; Grüner, S.; Page, S.; Müller, E.; Müller, I.; Bergmeier, W.; Richter, T.; Lorenz, M.; Konrad, I.; et al. A Critical Role of Platelet Adhesion in the Initiation of Atherosclerotic Lesion Formation. J. Exp. Med. 2002, 196, 887–896. [Google Scholar] [CrossRef]
- Ye, Z.; Hu, T.; Wang, J.; Xiao, R.; Liao, X.; Liu, M.; Sun, Z. Systemic immune-inflammation index as a potential biomarker of cardiovascular diseases: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 933913. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Nie, H.; Bu, G.; Tong, X.; Bai, X. Systemic immune-inflammation index (SII) and the risk of all-cause, cardiovascular, and cardio-cerebrovascular mortality in the general population. Eur. J. Med. Res. 2023, 28, 575. [Google Scholar] [CrossRef] [PubMed]
- Candemir, M.; Kiziltunç, E.; Nurkoç, S.; Şahinarslan, A. Relationship Between Systemic Immune-Inflammation Index (SII) and the Severity of Stable Coronary Artery Disease. Angiology 2021, 72, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Karasu, M.; Karaca, Y.; Yıldırım, E.; Kobat, M.A.; Er, F. Neutrophil-to-albumin ratio: A promising tool for CAD assessment in non-ST elevation AMI. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 11832–11839. [Google Scholar] [CrossRef] [PubMed]
- Mangalesh, S.; Dudani, S.; Mahesh, N.K. Development of a Novel Inflammatory Index to Predict Coronary Artery Disease Severity in Patients With Acute Coronary Syndrome. Angiology 2024, 75, 231–239. [Google Scholar] [CrossRef] [PubMed]
- So, A.; Thorens, B. Uric acid transport and disease. J. Clin. Investig. 2010, 120, 1791–1799. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Cheng, J.D. Uric Acid and Cardiovascular Disease: An Update From Molecular Mechanism to Clinical Perspective. Front. Pharmacol. 2020, 11, 582680. [Google Scholar] [CrossRef] [PubMed]
- Corry, D.B.; Eslami, P.; Yamamoto, K.; Nyby, M.D.; Makino, H.; Tuck, M.L. Uric acid stimulates vascular smooth muscle cell proliferation and oxidative stress via the vascular renin-angiotensin system. J. Hypertens. 2008, 26, 269–275. [Google Scholar] [CrossRef]
- Culleton, B.F.; Larson, M.G.; Kannel, W.B.; Levy, D. Serum uric acid and risk for cardiovascular disease and death: The Framingham Heart Study. Ann. Intern. Med. 1999, 131, 7–13. [Google Scholar] [CrossRef]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef]
- Ekici, B.; Kütük, U.; Alhan, A.; Töre, H.F. The relationship between serum uric acid levels and angiographic severity of coronary heart disease. Kardiol. Pol. 2015, 73, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Çakmak, E.Ö.; Bayam, E.; Çelik, M.; Kahyaoğlu, M.; Eren, K.; Imanov, E.; Karagöz, A.; İzgi, İ.A. Uric Acid-to-Albumin Ratio: A Novel Marker for the Extent of Coronary Artery Disease in Patients with Non-ST-Elevated Myocardial Infarction. Pulse 2021, 8, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Choroszy, M.; Litwinowicz, K.; Bednarz, R.; Roleder, T.; Lerman, A.; Toya, T.; Kamiński, K.; Sawicka-Śmiarowska, E.; Niemira, M.; Sobieszczańska, B. Human Gut Microbiota in Coronary Artery Disease: A Systematic Review and Meta-Analysis. Metabolites 2022, 12, 1165. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Chen, X.; Hu, X.; Niu, H.; Tian, R.; Wang, H.; Pang, H.; Jiang, L.; Qiu, B.; Chen, X.; et al. Alterations in the gut microbiome and metabolism with coronary artery disease severity. Microbiome 2019, 7, 68. [Google Scholar] [CrossRef] [PubMed]
- Hou, K.; Wu, Z.-X.; Chen, X.-Y.; Wang, J.-Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in health and diseases. Signal Transduct. Target. Ther. 2022, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Vetrani, C.; Di Nisio, A.; Paschou, S.A.; Barrea, L.; Muscogiuri, G.; Graziadio, C.; Savastano, S.; Colao, A. From Gut Microbiota through Low-Grade Inflammation to Obesity: Key Players and Potential Targets. Nutrients 2022, 14, 2103. [Google Scholar] [CrossRef] [PubMed]
- Inflammation and Atherosclerosis|Circulation. Available online: https://www.ahajournals.org/doi/10.1161/hc0902.104353 (accessed on 18 May 2024).
- Majumder, S.; Kiritkumar Makwana, R.; Shetty, V.; Mukherjee, S.; Narayan, P. Cardiovascular diseases and the heart–gut cross talk. Indian Hear. J. 2024, 76, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.; Yang, Y.; Wang, Y.; Hu, X.; Wang, Q.; Gao, F.; Sun, S.; Liu, Q.; Li, L.; Liu, J.; et al. Gut microbiota combined with metabolites reveals unique features of acute myocardial infarction patients different from stable coronary artery disease. J. Adv. Res. 2023, 46, 101–112. [Google Scholar] [CrossRef]
- Ottosson, F.; Brunkwall, L.; Smith, E.; Orho-Melander, M.; Nilsson, P.M.; Fernandez, C.; Melander, O. The gut microbiota-related metabolite phenylacetylglutamine associates with increased risk of incident coronary artery disease. J. Hypertens. 2020, 38, 2427–2434. [Google Scholar] [CrossRef]
- Han, Y.; Gong, Z.; Sun, G.; Xu, J.; Qi, C.; Sun, W.; Jiang, H.; Cao, P.; Ju, H. Dysbiosis of Gut Microbiota in Patients With Acute Myocardial Infarction. Front. Microbiol. 2021, 12, 680101. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Mou, X.; Li, J.; Li, M.; Ye, C.; Gao, X.; Liu, X.; Ma, Y.; Xu, Y.; Zhong, Y. Alterations in gut microbiota and host transcriptome of patients with coronary artery disease. BMC Microbiol. 2023, 23, 320. [Google Scholar] [CrossRef] [PubMed]
- An, K.; Jia, Y.; Xie, B.; Gao, J.; Chen, Y.; Yuan, W.; Zhong, J.; Su, P.; Liu, X. Alterations in the gut mycobiome with coronary artery disease severity. eBioMedicine 2024, 103, 105137. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Wang, J.; Zhao, L.-L.; Yao, T.-T.; Chen, Y.; Ma, J.; Zhang, X.; Wang, J.-X.; Wang, Y.; Cui, Z.; et al. Gut Lactobacillus Level Is a Predictive Marker for Coronary Atherosclerotic Lesions Progress and Prognosis in Patients With Acute Coronary Syndrome. Front. Cell Infect. Microbiol. 2021, 11, 687827. [Google Scholar] [CrossRef] [PubMed]
- Ooi, L.G.; Ahmad, R.; Yuen, K.H.; Liong, M.T. Lactobacillus gasseri [corrected] CHO-220 and inulin reduced plasma total cholesterol and low-density lipoprotein cholesterol via alteration of lipid transporters. J. Dairy. Sci. 2010, 93, 5048–5058. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.-T.; Wang, J.; Liang, Y.; Wu, X.-Y.; Li, W.-Q.; Wang, Y.-H.; Jing, A.-R.; Liang, M.-M.; Sun, L.; Dou, J.; et al. The level of serum total bile acid is related to atherosclerotic lesions, prognosis and gut Lactobacillus in acute coronary syndrome patients. Ann. Med. 2023, 55, 2232369. [Google Scholar] [CrossRef] [PubMed]
- Leylabadlo, H.E.; Sanaie, S.; Heravi, F.S.; Ahmadian, Z.; Ghotaslou, R. From role of gut microbiota to microbial-based therapies in type 2-diabetes. Infect. Genet. Evol. 2020, 81, 104268. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Jiao, X.; Ma, Y.; Liu, Y.; Zhang, L.; He, Y.; Chen, Y. Trimethylamine N-oxide induces inflammation and endothelial dysfunction in human umbilical vein endothelial cells via activating ROS-TXNIP-NLRP3 inflammasome. Biochem. Biophys. Res. Commun. 2016, 481, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.E.; Liao, P.D.; Zhao, X.J.; Wang, L. Trimethylamine-N-oxide has prognostic value in coronary heart disease: A meta-analysis and dose-response analysis. BMC Cardiovasc. Disord. 2020, 20, 7. [Google Scholar] [CrossRef]
- Yu, N.; Gu, N.; Wang, Y.; Zhou, B.; Lu, D.; Li, J.; Ma, X.; Zhang, J.; Guo, X. The Association of Plasma Trimethylamine N-Oxide with Coronary Atherosclerotic Burden in Patients with Type 2 Diabetes Among a Chinese North Population. Diabetes Metab. Syndr. Obes. 2022, 15, 69–78. [Google Scholar] [CrossRef]
- Waleed, K.B.; Tse, G.; Lu, Y.-K.; Peng, C.-N.; Tu, H.; Ding, L.-G.; Xia, Y.-L.; Wu, S.-L.; Li, X.-T.; Zhou, H.-Q.; et al. Trimethylamine N-oxide is associated with coronary atherosclerotic burden in non-ST-segment myocardial infarction patients: SZ-NSTEMI prospective cohort study. Rev. Cardiovasc. Med. 2021, 22, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Waleed, K.B.; Lu, Y.; Liu, Q.; Zeng, F.; Tu, H.; Wei, Y.; Xu, S.; Zhang, Z.; Rongfeng, Y.; Fan, A.; et al. Association of trimethylamine N-oxide with coronary atherosclerotic burden in patients with non-ST-segment elevation myocardial infarction. Medicine 2020, 99, e20794. [Google Scholar] [CrossRef] [PubMed]
- Senthong, V.; Li, X.S.; Hudec, T.; Coughlin, J.; Wu, Y.; Levison, B.; Wang, Z.; Hazen, S.L.; Tang, W.H.W. Plasma Trimethylamine N-Oxide, a Gut Microbe-Generated Phosphatidylcholine Metabolite, Is Associated With Atherosclerotic Burden. J. Am. Coll. Cardiol. 2016, 67, 2620–2628. [Google Scholar] [CrossRef] [PubMed]
- Gessner, A.; Di Giuseppe, R.; Koch, M.; Fromm, M.F.; Lieb, W.; Maas, R. Trimethylamine-N-oxide (TMAO) determined by LC-MS/MS: Distribution and correlates in the population-based PopGen cohort. Clin. Chem. Lab. Med. 2020, 58, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Bergeron, N.; Levison, B.S.; Li, X.S.; Chiu, S.; Jia, X.; Koeth, R.A.; Li, L.; Wu, Y.; Tang, W.H.W.; et al. Impact of chronic dietary red meat, white meat, or non-meat protein on trimethylamine N-oxide metabolism and renal excretion in healthy men and women. Eur. Heart J. 2018, 40, 583–594. [Google Scholar] [CrossRef]
- Li, D.Y.; Wang, Z.; Li, X.S.; Hazen, S.L.; Tang, W.W. Relationship between statin use and trimethylamine N-oxide in cardiovascular risk assessment. J. Am. Coll. Cardiol. 2018, 71, A115. [Google Scholar] [CrossRef]
- Awoyemi, A.; Mayerhofer, C.; Felix, A.S.; Hov, J.R.; Moscavitch, S.D.; Lappegård, K.T.; Hovland, A.; Halvorsen, S.; Halvorsen, B.; Gregersen, I.; et al. Rifaximin or Saccharomyces Boulardii in Heart Failure with Reduced Ejection Fraction: Results from the Randomized GutHeart Trial. Available online: https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964(21)00304-2/fulltext (accessed on 12 June 2024).
- Liu, Y.; Liu, S.; Zhao, Z.; Song, X.; Qu, H.; Liu, H. Phenylacetylglutamine is associated with the degree of coronary atherosclerotic severity assessed by coronary computed tomographic angiography in patients with suspected coronary artery disease. Atherosclerosis 2021, 333, 75–82. [Google Scholar] [CrossRef]
- Yu, F.; Feng, X.; Li, X.; Luo, Y.; Wei, M.; Zhao, T.; Xia, J. Gut-Derived Metabolite Phenylacetylglutamine and White Matter Hyperintensities in Patients With Acute Ischemic Stroke. Front. Aging Neurosci. 2021, 13, 675158. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, E.; Sofidis, G.; Papazoglou, A.S.; Deda, O.; Panteris, E.; Moysidis, D.V.; Stalikas, N.; Kartas, A.; Papadopoulos, A.; Stefanopoulos, L.; et al. Correlation of the severity of coronary artery disease with patients’ metabolic profile-rationale, design and baseline patient characteristics of the CorLipid trial. BMC Cardiovasc. Disord. 2021, 21, 79. [Google Scholar] [CrossRef]
- Guo, M.; Cao, X.; Ji, D.; Xiong, H.; Zhang, T.; Wu, Y.; Suo, L.; Pan, M.; Brugger, D.; Chen, Y.; et al. Gut Microbiota and Acylcarnitine Metabolites Connect the Beneficial Association between Estrogen and Lipid Metabolism Disorders in Ovariectomized Mice. Microbiol. Spectr. 2023, 11, e00149-23. [Google Scholar] [CrossRef]
- Hu, T.; Wu, Q.; Yao, Q.; Jiang, K.; Yu, J.; Tang, Q. Short-chain fatty acid metabolism and multiple effects on cardiovascular diseases. Ageing Res. Rev. 2022, 81, 101706. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.L.; Heaver, S.L.; Waters, J.L.; Kim, B.I.; Bretin, A.; Goodman, A.L.; Gewirtz, A.T.; Worgall, T.S.; Ley, R.E. Sphingolipids produced by gut bacteria enter host metabolic pathways impacting ceramide levels. Nat. Commun. 2020, 11, 2471. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Akhthar, T.; Jain, S.K. Coronary artery disease and its association with Vitamin D deficiency. J. Midlife Health 2016, 7, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Wiśniewski, P.; Nessler, J. Witamina D a układ krążenia. Kardiol. Inwazyjna 2016, 11, 62–68. [Google Scholar]
- Bakthavatchalam, R.; Bakthavatchalam, S.; Chandran, I.; Gaur, A.; Natarajaboopathy, R.; Geetha, J.; Reddy, K.S.; Sindhura, G.; Varatharajan, S. Association of Vitamin D with Risk Factors for Coronary Artery Disease. Maedica 2023, 18, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Cerit, L.; Cerit, Z. Vitamin D Deficiency is not Associated with Higher Levels of SYNTAX Score. Braz. J. Cardiovasc. Surg. 2019, 34, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.R.; Qian, Y.A.; Chen, Y.D.; Shi, Y.; Yin, D.W.; Wang, H.; Zhu, P.; Liu, H.W.; Sha, Y. The Effects of Low Vitamin D on Coronary Artery Disease. Heart Lung Circ. 2014, 23, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Baktır, A.O.; Doğan, Y.; Şarlı, B.; Şahin, Ö.; Demirci, E.; Akpek, M.; Özkan, E.; Arınç, H.; Sağlam, H. Relationship between serum 25-hydroxyvitamin D levels and the SYNTAX score in patients with acute coronary syndrome. Anatol. J. Cardiol. 2017, 17, 293–297. [Google Scholar] [CrossRef]
- Şen, Ö.; Şen, S.B.; Topuz, A.N.; Topuz, M. Vitamin D level predicts angiographic no-reflow phenomenon after percutaneous coronary intervention in patients with ST segment elevation myocardial infarction. Biomark. Med. 2021, 15, 1357–1366. [Google Scholar] [CrossRef]
- Şeker, T.; Gür, M.; Kalkan, G.Y.; Kuloğlu, O.; Koyunsever, N.Y.; Şahin, D.Y.; Türkoğlu, C.; Akyol, S.; Elbasan, Z.; Harbalıoğlu, H.; et al. Serum 25-hydroxyvitamin D level and extent and complexity of coronary artery disease. J. Clin. Lab. Anal. 2014, 28, 52–58. [Google Scholar] [CrossRef]
- Wu, Z.; Wang, T.; Zhu, S.; Li, L. Effects of vitamin D supplementation as an adjuvant therapy in coronary artery disease patients*. Scand. Cardiovasc. J. 2016, 50, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Tabaei, S.; Motallebnezhad, M.; Tabaee, S.S. Vitamin D Receptor (VDR) Gene Polymorphisms and Risk of Coronary Artery Disease (CAD): Systematic review and Meta-analysis. Biochem. Genet. 2021, 59, 813–836. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, S.; Djafarian, K.; Alizadeh, H.; Mohseni, R.; Shab-Bidar, S. Common Variants of Vitamin D Receptor Gene Polymorphisms and Susceptibility to Coronary Artery Disease: A Systematic Review and Meta-Analysis. Lifestyle Genom. 2017, 10, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2014, 383, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Ishiwata, S.; Tomita, Y.; Ishiwata, S.; Narui, K.; Daida, H.; Kasai, T. Association between Obstructive Sleep Apnea and SYNTAX Score. J. Clin. Med. 2020, 9, 3314. [Google Scholar] [CrossRef]
- Rivera-Pérez, S.J.; Martinez, D.; Araujo, G.N.; Goncalves, S.C.; Lazzaretti, L.K.; Wainstein, R.V.; Wainstein, M.V.; Ribeiro, J.P. Severity of obstructive sleep apnea and extension of coronary artery disease. Sleep Breath. 2019, 23, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, M.; Shi, J. Influence of obstructive sleep apnoea on coronary artery disease in a Chinese population. J. Int. Med. Res. 2022, 50, 3000605221115389. [Google Scholar] [CrossRef]
- Hein, T.; Loo, G.; Ng, W.-Y.; Tai, B.-C.; Kajiya, T.; Tan, A.; Khoo, S.-M.; Chan, M.; Low, A.F.; Chia, B.-L.; et al. Relationship between apnoea-hypopnoea index and angiographic coronary disease phenotypes in patients presenting with acute myocardial infarction. Acute Card. Care 2013, 15, 26–33. [Google Scholar] [CrossRef]
- Xie, L.; Zhen, P.; Yu, F.; Yu, X.; Qian, H.; Yang, F.; Tong, J. Effects of sleep apnea hypopnea syndromes on cardiovascular events: A systematic review and meta-analysis. Sleep Breath. 2022, 26, 5–15. [Google Scholar] [CrossRef]
- Azarbarzin, A.; Zinchuk, A.; Wellman, A.; Labarca, G.; Vena, D.; Gell, L.; Messineo, L.; White, D.P.; Gottlieb, D.J.; Redline, S.; et al. Cardiovascular Benefit of Continuous Positive Airway Pressure in Adults with Coronary Artery Disease and Obstructive Sleep Apnea without Excessive Sleepiness. Am. J. Respir. Crit. Care Med. 2022, 206, 767–774. [Google Scholar] [CrossRef]
- Lui, M.M.S.; Sau-Man, M. OSA and atherosclerosis. J. Thorac. Dis. 2012, 4, 164–172. [Google Scholar] [CrossRef]
- Alonso-Fernandez, A.; Garcia-Rio, F.; Arias, M.A.; Hernanz, A.; De La Pena, M.; Pierola, J.; Barcelo, A.; Lopez-Collazo, E.; Agusti, A. Effects of CPAP on oxidative stress and nitrate efficiency in sleep apnoea: A randomised trial. Thorax 2009, 64, 581–586. [Google Scholar] [CrossRef] [PubMed]
- De Torres-Alba, F.; Gemma, D.; Armada-Romero, E.; Rey-Blas, J.R.; López-de-Sá, E.; López-Sendon, J.L. Obstructive Sleep Apnea and Coronary Artery Disease: From Pathophysiology to Clinical Implications. Pulm. Med. 2013, 2013, 768064. [Google Scholar] [CrossRef] [PubMed]
- Jehan, S.; Zizi, F.; Pandi-Perumal, S.R.; Wall, S.; Auguste, E.; Myers, A.K.; Jean-Louis, G.; McFarlane, S.I. Obstructive Sleep Apnea and Obesity: Implications for Public Health. Sleep. Med. Disord. 2017, 1, 00019. [Google Scholar] [PubMed]
- Gomes, F.; Telo, D.F.; Souza, H.P.; Nicolau, J.C.; Halpern, A.; Serrano, C.V., Jr. Obesity and coronary artery disease: Role of vascular inflammation. DOAJ (DOAJ Dir. Open Access J.) 2010, 94, 255–256. [Google Scholar] [CrossRef]
- Henning, R.J. Obesity and obesity-induced inflammatory disease contribute to atherosclerosis: A review of the pathophysiology and treatment of obesity. Am. J. Cardiovasc. Dis. 2021, 11, 504–529. [Google Scholar] [PubMed]
- Mitra, A.K.; Bhuiyan, A.R.; Jones, E.A. Association and Risk Factors for Obstructive Sleep Apnea and Cardiovascular Diseases: A Systematic Review. Diseases 2021, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.; O’Mahony, A.M.; McNicholas, W.T.; Ryan, S. Cardiovascular manifestations in obstructive sleep apnea: Current evidence and potential mechanisms. Pol. Arch. Med. Wewnętrznej 2021, 131, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Luyster, F.S.; Kip, K.E.; Aiyer, A.N.; Reis, S.E.; Strollo, P.J. Relation of Obstructive sleep apnea to coronary artery Calcium in Non-Obese versus Obese Men and women aged 45–75 years. Am. J. Cardiol. 2014, 114, 1690–1694. [Google Scholar] [CrossRef]
- Yang, S.; Guo, X.; Liu, W.; Li, Y.; Liu, Y. Alcohol as an independent risk factor for obstructive sleep apnea. Ir. J. Med. Sci. 2021, 191, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Song, R.J.; Nguyen, X.-M.T.; Quaden, R.; Ho, Y.-L.; Justice, A.C.; Gagnon, D.R.; Cho, K.; O’Donnell, C.J.; Concato, J.; Gaziano, J.M.; et al. Alcohol Consumption and Risk of Coronary Artery Disease (from the Million Veteran Program). Am. J. Cardiol. 2018, 121, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A. Effects of alcohol consumption on MI risk—Evidence from INTERHEART. Nat. Rev. Cardiol. 2014, 11, 434. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Smyth, A.; Teo, K.K.; McKee, M.; Rangarajan, S.; Pais, P.; Liu, L.; Anand, S.S.; Yusuf, S. Patterns of alcohol consumption and myocardial infarction risk. Circulation 2014, 130, 390–398. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Risk Factors | Clinical Condition of Risk Factor Significance | Modification | Study Type | |
|---|---|---|---|---|
| Inflammation | CRP [26,27,28,29,30,31,32] | ACS | Canakinumab [29], colchicine [30,31] | RCTs-CANTOS [29], COLCOT [30], LoDoCo2 [31] |
| NLR | ACS [39,40]/ declined [44]/ only in males [46] | |||
| SII | Stable angina and ACS [46,52] | |||
| UAR | NSTEMI | |||
| Microbiota | Lactobacillus abundance | ACS [69,72] | Lactobacillus gasseri supplementation [73] | RCT [73], |
| TMAO | NSTEMI [78], stable angina [79] | Red meat exclusion [90], statins [91], rifaximin [92] | RCT [90], cohort study [91], RCT [92] | |
| Vitamin D | Stable angina [95] | Vitamin D supplementation (0.5 μg/per day) [95] | RCT [95] | |
| Sleep apnea | OSA | CCS | CPAP [102] | RCT [102] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Florek, K.; Kübler, M.; Górka, M.; Kübler, P. New Modifiable Risk Factors Influencing Coronary Artery Disease Severity. Int. J. Mol. Sci. 2024, 25, 7766. https://doi.org/10.3390/ijms25147766
Florek K, Kübler M, Górka M, Kübler P. New Modifiable Risk Factors Influencing Coronary Artery Disease Severity. International Journal of Molecular Sciences. 2024; 25(14):7766. https://doi.org/10.3390/ijms25147766
Chicago/Turabian StyleFlorek, Kamila, Maja Kübler, Magdalena Górka, and Piotr Kübler. 2024. "New Modifiable Risk Factors Influencing Coronary Artery Disease Severity" International Journal of Molecular Sciences 25, no. 14: 7766. https://doi.org/10.3390/ijms25147766