Abstract
In recent years, there has been growing interest in understanding the potential role of microbiota dysbiosis or alterations in the composition and function of human microbiota in the development of chronic rhinosinusitis with nasal polyposis (CRSwNP). This systematic review evaluated the literature on CRSwNP and host microbiota for the last ten years, including mainly nasal bacteria, viruses, and fungi, following the PRISMA guidelines and using the major scientific publication databases. Seventy original papers, mainly from Asia and Europe, met the inclusion criteria, providing a comprehensive overview of the microbiota composition in CRSwNP patients and its implications for inflammatory processes in nasal polyps. This review also explores the potential impact of microbiota-modulating therapies for the CRSwNP treatment. Despite variability in study populations and methodologies, findings suggest that fluctuations in specific taxa abundance and reduced bacterial diversity can be accepted as critical factors influencing the onset or severity of CRSwNP. These microbiota alterations appear to be implicated in triggering cell-mediated immune responses, cytokine cascade changes, and defects in the epithelial barrier. Although further human studies are required, microbiota-modulating strategies could become integral to future combined CRSwNP treatments, complementing current therapies that mainly target inflammatory mediators and potentially improving patient outcomes.
1. Introduction
Chronic respiratory diseases (CRDs) are persistent and non-communicable diseases affecting the upper and lower airways that cause significant morbidity and mortality [1]. Chronic rhinosinusitis (CRS) is characterized by an inflammatory disorder involving the nose, paranasal sinuses, and upper airways, persisting for at least 12 weeks despite appropriate medical therapy. This debilitating disease affects 5–12% of the general population and common symptoms, which might be similar to acute cases, include anterior or posterior nasal discharge/congestion, facial pain or pressure, impairment of smell or anosmia, difficulty breathing through the nose, headache, fatigue, and cough [2,3]. Anatomical changes of the nose and paranasal sinuses contribute to the presence and recurrence of CRS symptoms. Imaging studies have shown a significant reduction in the size of the maxillary, sphenoid, and frontal sinuses, along with near-total opacification of these areas and the ethmoid air cells. There is also a rarefaction of the ethmoid bony septae, as well as the ostiomeatal units, and sphenoethmoidal recesses, and frontal outflow tracts are compromised due to thickened mucosa and retained secretions [4,5,6,7].
The CRS incidence has increased, leading to subsequent socio-economic impacts on healthcare systems and economies [8]. In the United States, handling CRS is projected to cost between USD 11 billion and USD 13 billion annually, equating to USD 2609 per patient per year. Meanwhile, CRS contributes to a direct healthcare spending increase of EUR 2500 per patient per year in Europe. Beyond direct expenses, indirect costs stemming from absenteeism and reduced workplace productivity are substantial, with CRS ranking among the top 10 most expensive health conditions for United States employers, surpassing USD 20 billion annually [9].
Although with significant limitations, CRS has traditionally been classified into two phenotypes based on diagnosis with nasal endoscopy and inflammatory biomarkers: CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP) [2,10]. CRSwNP is typically characterized by nasal congestion and/or congestion and loss of smell and taste, while CRSsNP is mainly associated with rhinorrhea and facial pain or pressure [2,11]. Based on endotype dominance, CRSwNP is predominantly related to type 2 inflammatory response in the general adult population in Western countries. It is characterized by activation and recruitment of T-helper type-2 (Th2) cells, e.g., eosinophils and mast cells, as well as increased levels of Th2 inflammatory interleukins (ILs), e.g., IL-4, IL-5, and IL-13, and immunoglobulin E (IgE). In contrast, CRSsNP, which is more prevalent than CRSwNP [9,11], has been associated with non-eosinophilic/non-type-2 inflammation involving a mixture of type-1 and type-3 inflammatory response mediated by Th1 and Th17 cells, respectively [9,12,13,14]. Since type-2 inflammation is involved in the pathogenesis of several comorbidities, the prevalence of asthma, and/or nonsteroidal anti-inflammatory drug-exacerbated respiratory disease (NSAID-ERD) or aspirin-exacerbated respiratory disease (AERD) in patients with CRSwNP is higher than those with CRSsNP [15,16,17]. Consequently, CRSwNP patients often show more severe clinical symptoms, reduced quality of life (QOL), greater healthcare resource utilization, and direct and indirect costs, thus making this phenotype more clinically relevant [15,18,19,20].
The prevalence of CRSwNP in the general population has been estimated to range from 1 to 3%, although it varies across diverse regions of the world [16,17,21]. About the diagnosis, CRSwNP is confirmed by computed tomography scans and nasal endoscopic visualization of nasal polyps with specific scoring systems such as the Lund–Mackay score [22,23]. Nasal polyps or fleshy swellings result from soft tissue growth in the lining of the nose and paranasal sinuses, probably due to chronic inflammation of unknown causes [21]. They usually manifest as bilateral lesions, being more frequent in males (3.2–3.7%) than females (2.0–3.3%) and for the age group ranging from 60 to 69 years [19,21,24]. Besides male sex and aging, the other most commonly reported risk factors for developing CRSwNP include diseases associated with a worse respiratory function, such as asthma, eosinophilia, allergy, smoking, obesity, or variations and polymorphisms in genes related to immune response, structural proteins, or tissue remodeling [9,21,25,26,27,28]. The presence of microbiota dysbiosis or alterations in the composition, function, and local distribution of host microbiota also implies an increased risk for nasal polyps [29].
The human microbiota is defined as a community of microorganisms, including mainly a wide variety of bacterial species, as well as archaea (primitive single-celled organisms), eukarya, and viruses that live in and on the mucosal surfaces of the gut and skin, as well as the respiratory and genital tract [30]. Host–microbial community interactions have been determined to play a crucial role in developing and maintaining several vital functions, such as regulation of the immune system, protection against pathogens, digestion of food, biotransformation of foreign substances, or production of vitamins, among others [31,32,33]. However, older age; host genetic susceptibility; environmental factors; infections; and changes in antibiotic use, diet, or lifestyle can lead the transition from host–microbiota symbiosis to dysbiosis, contributing to the pathogenesis of a variety of inflammatory and autoimmune diseases, including CRS [29,34,35].
Accumulating data suggest that CRSwNP immunopathogenesis can be partially explained by alterations in the host microbiota, such as reductions in bacterial diversity with an increase in pathogenic bacteria that induce inflammatory reactions (e.g., Staphylococcus aureus or Pseudomona aeruginosa) and a loss of beneficial bacteria with potential immune protective properties (Lactobacillus, Dolosigranulum, and Citrobacter species). The formation of nasal biofilms, referring to microbial communities that adhere to a surface or biological tissue and are embedded in a matrix of self-produced extracellular polymeric substances, can also be relevant [36]. The presence of defects in the nasal mechanical or physical barrier with inappropriate immune response can also be a critical factor [29,37,38,39]. In this context, an enhancement of the permeability due to environmental and intrinsic factors of the nasal physical barrier, which consists of airway mucus, epithelial cells with cilia, adhesion molecules, or apical junctional complexes (tight and adherens junctions, desmosomes, and hemidesmosomes), as well as endogenous antimicrobial substances [37,40], was previously associated with CRSwNP [37,41,42,43]. A vulnerable epithelial barrier to pathogens and allergens/foreign material contributes toward activating an intense local Th2 response of the adaptive immune system with an accumulation of inflammatory cells, which triggers a remodeling of nasal mucosal tissue pattern consisting of decreased collagen and increased fibrin. This dynamic inflammatory process leading to polyp formation is described under the immune barrier hypothesis [29,37,39,42,44].
Considering the potential role of the host microbiota in CRSwNP and the estimation that up to 40% of CRSwNP patients cannot achieve an acceptable level of disease control despite adequate endoscopic sinus surgery (ESS), corticosteroid treatment, and up to two short courses of systemic corticosteroids in the last year (difficult-to-treat patients according to the European Position Paper on CRS (EPOS) guideline) [9,15], modulation of the nasal and gut microbiota emerges is a promising therapeutic strategy worth exploring. Besides ESS and oral and intranasal corticosteroids, the mainstays of treatment for patients with CRSwNP involve other medical management/medication, including antibiotics and antifungals, antihistamines, and monoclonal antibodies targeting interleukins, such as IL-4, IL-5, and IL-13, or IgE (benralizumab, dupilumab, mepolizumab, and omalizumab), among others with varying efficacy [9,21,43,45,46].
To take a deep look into the complex role of the human microbiota in the pathogenesis of CRSwNP, we conducted a systematic literature review of the last decade, focusing on the nasal and gut bacterial microbiota. The microbiome was also considered, which refers to the microorganisms and their genomes occupying a reasonably well-defined habitat and microbial structural elements, metabolites, and environmental conditions [47]. The results of this systematic review are organized into three main sections, which provide a concise and precise examination of the most recent publications focused on the composition of nasal and gut microbiota in CRSwNP patients and point out the critical microbial species associated with nasal polyps (“Microbiota Composition in CRSwNP”), on the potential mechanism underlying microbial dysbiosis and inflammatory processes in nasal polyps (“Relationship between Microbial Dysbiosis and Inflammation in CRSwNP”), and on the evaluation of promising therapeutic strategies involving the modulation of the bacterial microbiota for the CRSwNP treatment (“Effect of CRSwNP Treatment on the Modulation of the Microbiota”). The review includes both adult and children studies and excludes literature reviews.
2. Materials and Methods
2.1. Study Design and Search Strategy
It is worth noting that the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [48] and the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) recommendations [49] were taken into account to carry out this systematic review. PICO (Population, Intervention, Control, and Outcome) criteria [50] were defined as follows: P = CRSwNP, intervention = host microbiota or dysbiosis contributing to the CRSwNP pathogenesis; C = disease control or healthy subjects, placebo, or standard-care groups, or comparisons before or after the implementation of microbiota-related interventions; and O = outcomes related to the impact of microbiota on CRSwNP, such as changes in symptom severity, recurrence rates, quality of life, histological findings, or other clinically relevant measures.
The literature search was carried out between January and February 2024 in Medline (PubMed), Wiley (Cochrane Library), Embase, and Scopus online databases using a combination of terms related to “Chronic rhinosinusitis with nasal polyps” or “nasal polyps” and “microbiota” or “microbiome” or “dysbiosis”. The selected terminology was chosen considering MeSH and Emtree terms from Medline and Embase, respectively, incorporating input from experienced specialists in the field and reviewing relevant literature. Available government and professional organization websites were also manually reviewed, and a references list of included articles was used to avoid missing any relevant studies. Supplementary Table S1 provides details of the search strategies.
2.2. Selection Criteria
All original articles and meta-analyses indexed from 2014 to February 2024 focused on the evaluation of the microbiota in CRSwNP were identified as eligible studies using the following inclusion criteria: (1) original study or meta-analysis written in English; (2) studies including human subjects, both children and adults; (3) patients with CRSwNP or nasal polyps; and (4) studies describing key microbial species, dysbiosis, or microbiota changes in associations with disease onset, severity, prevalence, or treatment. In contrast, the exclusion criteria were (1) animal, in vitro or in silico studies; (2) review articles, case reports, expert-opinion articles, commentaries, or letters; (3) conference abstract published after 1 January 2023; (4) articles mainly focused on other diseases, such as antrochoanal polyps; and (5) articles whose full-text version was not available to us.
2.3. Review Process and Data Extraction
Three review authors carried out the initial screening of abstracts and titles retrieved from each study, using the open-access Rayyan software [51]. The consideration of each study for full review was based on the PICO previously described, when it was possible. Subsequently, at least two reviewers independently screened the full-text articles selected. Any disagreements during screenings were resolved by consensus or a third independent reviewer.
Data reported in the selected articles were collected using a standardized data-extraction template in Microsoft Excel, allowing us to plot the information for each of this review’s previously described main sections. The following information was extracted: information about the article (name of the first author, years of publication, and title) and the study (study type, objective, population/country in which the study was carried out, and sample size), patient demographics (age, sex, and other diseases associated/comorbidities), details of microbiota-related interventions (type/format), quantitative, and/or qualitative results and conclusions.
A risk of bias (RoB) assessment was carried out to establish the degree of certainty and quality of the randomized controlled studies, which included using version 2 of the Cochrane risk-of-bias tool (RoB 2) [52]. In detail, studies were classified as “High, Moderate, and Low RoB”. As in previous studies, the Newcastle–Ottawa Scale (NOS) tool for cohort and case–control studies [52,53] and an adapted form of NOS for cross-sectional [54] were used to assess the validity of the findings of non-randomized studies. The scales assess aspects related to study quality concerning selection (four points for cohort and case–control studies or five points for cross-sectional studies) and comparability (two points) of study groups, as well as assessment of outcomes or ascertainment of exposure (three points) [53]. NOS scores were again classified as “High” (zero-to-three NOS points for cohort and case–control studies and zero-to-four points for cross-sectional studies), “Moderate” (four-to-six or five-to-seven points), and “Low” (seven-to-nine or eight-to-ten points) RoB. It is worth noting that a lower score was assigned to any study that referred to too-small sample size (less than ten CRSwNP patients), was without appropriate controls, or did not clearly describe the methodology used.
3. Results
3.1. Search Results
Before the beginning of this systemic review, the review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO, study ID: CRD42024509276).
The initial database search using synonymous terms of CRSwNP, nasal polyps, microbiota, microbiome, and dysbiosis yielded 464 references that initially met the inclusion criteria previously described. After identifying and excluding duplicates, 300 references were selected for title and abstract review, and, subsequently, 111 references were selected for a full-text review. As a result, a total of 70 eligible studies (65 articles published and 5 included after manual searching) that met the inclusion criteria were finally included in this review. Figure 1 summarizes the results of each screening stage and the selection of studies presented as a PRISMA flow diagram.
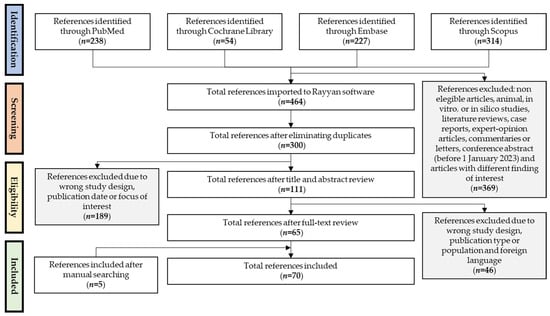
Figure 1.
A flow diagram shows the screening and selection process of the studies through the different stages of the present systematic review. n: number of references/studies included or excluded.
Out of 70 studies included in this systematic review (Supplementary Data S1), 68 (97.4%) focused on the identification of the microbiota composition of CRSwNP subjects, 21 (30.0%) on the study of the relationship between microbial dysbiosis and inflammation in CRSwNP, and 9 (12.9%) on the evaluation of the effect of different CRSwNP treatment on the microbiota. Note that the studies have a publication range from 2014 to 2024, with 60 studies published relatively recently, between 2019 and 2024 (60.0%). The most significant number of studies was from Asia (24, 34.3%, mainly from China), and to a lesser extent from Europe (14, 20.0%), Oceania (13, 18.6%, mainly from New Zealand), and North America (13, 18.6%, mainly from the USA). Only one study included was a multicenter international cohort study across nine countries [55].
The studies collected data from more than 7450 subjects, of whom approximately 4000 were CRSwNP patients ranging in age from 13 to 88 years. Forty-nine studies (70%) were relatively small (initial sample size less than 100 subjects), and only ten studies showed results from more than 100 CRSwNP patients (14.3%). Considering the studies that reported the gender data, men (2665 subjects of whom 2103 were patients with CRSwNP) were more abundant than women (1451 subjects, 927 patients with CRSwNP). Disease-control (non-CRS) and/or healthy subjects were also included in 41 studies (58.6%), and CRSsNP patients in 39 studies (55.7%). Seven studies distinguished CRSwNP patients as eosinophilic (ECRSwNP) and non-eosinophilic (NECRSwNP) based on the infiltration of eosinophils in inflamed tissues (proportion of eosinophils more than ten percent and less than ten percent of inflammatory cells, respectively) [56,57,58,59,60,61,62,63]. Comorbidities, such as atopy, allergy, allergic rhinitis, aspirin sensitivity, acetylsalicylic acid sensitivity, AERD, and asthma—the most commonly reported—were also included in 49 studies (70%). A total of 26 studies (37.1%) reported that all subjects or a majority of them had not taken antibiotics and/or corticosteroids—two of the most commonly used drugs for CRSwNP [21]—at least the month before the analysis.
Regarding the study design, most of them (64, 91.4%) were identified as non-randomized studies of frequency (cohort or cross-sectional designs) or exposure (cohort and case–control studies), with only 6 (8.6%) being randomized controlled trials. In detail, 52 (74.3%) cross-sectional, 10 (14.3%) cohort, and 2 (2.9%) case–control studies were included in this review. Considering the prospective studies (one randomized controlled trial and nine cohort studies) that reported the follow-up time, the average follow-up was 10.4 months, with the shortest and longest follow-up time of two weeks and five years, respectively.
As previously described, the current version of the RoB 2 was used to performed a RoB assessment for randomized controlled trials and NOS tools to assess the validity of the findings of non-randomized controlled studies. The main concern regarding the RoB assessment referred to a well-defined selection of CRSwNP patients, a justified and satisfactory sample size, appropriate controls, or healthy subjects, or the description of the methodology selected to achieve the intended results. Considering that the RoB 2 tool showed that one (16.7%) randomized controlled trial was classified as “Low RoB” and four (66.7%) and “Some concerns”, mainly referred to the randomization process and deviations from intended interventions. One study (16.7%) accomplished the criteria for “Low RoB” because there were deviations from the intended intervention which arose because of the experimental context and some concerns about the randomization process (Figure 2a and Supplementary Data S2). By using NOS questionnaires, 44 of 64 (68.8%) non-randomized controlled studies included were considered “High quality”, whereas 17 (26.6%) and three (4.7%) met the criteria of “Moderate and Low quality”, respectively (Figure 2b and Supplementary Data S3). Of note, 27 (42.2%) studies did not include disease (non-CRS) or healthy control subjects, 2 (3.1%) had no reference to the number of CRSwNP patients included, and 7 (10.9%) referred to less than ten CRSwNP patients. All of them described the methodology used. Overall, the assessment of outcomes or ascertainment of exposure was the better-scored category.
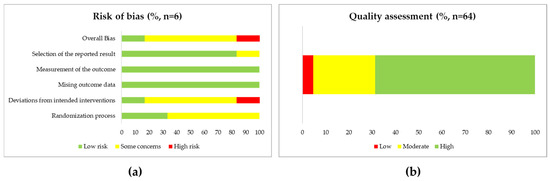
Figure 2.
(a) Bar graph showing results of risk of bias (RoB) assessment obtained for the randomized controlled trials (n = 6) included in this review, using version 2 of the Cochrane risk-of-bias tool (RoB 2) [52]. (b) Bar graph showing results of quality assessment obtained for the non-randomized controlled studies (n = 64) included in this review, using the Newcastle–Ottawa Scale (NOS) tool [53,54].
3.2. Study Analysis
3.2.1. Microbiota Composition in CRSwNP
Table 1 summarizes the most relevant information extracted from the studies included in this systematic review and focuses on the microbiota composition analysis in CRSwNP patients. Out of 66 studies, 61 (92.4%), 9 (13.6%), and 3 (4.5%) studies reported data about the bacterial, fungal, and viral composition from nasal samples, respectively, mainly taken from middle meatus (41, 62.1%). Only one study also focused on the gut microbiota from fecal samples [61]. Of note, two articles showed the same results of nasal microbiota composition obtained for the same CRSwNP patients [64,65].
The microbiota composition analyses were carried out using both molecular techniques (47, 71.2%), based mainly on marker-gene sequencing analysis with clustering of the sequencing reads into operational taxonomic units (OTUs) at a fixed similarity threshold (>97%), as well as standard microbiological techniques (40.9%), such as bacterial culture, typical colony morphology analysis, Gram staining, or biochemical test, among others.
Regarding the results for bacteria, it is worth noting that six out of seven studies with culture-positive patient data showed that the positive-culture rate was relatively high in CRSwNP patients (over 63.0%) [38,57,58,66,67,68,69]. The three studies focused on the characterizing of bacterial biofilm on the nasal mucosa in CRSwNP patients also showed a prevalence of over 44.2% [70,71,72]. Overall, the bacterial composition of the core microbiota found was dominated by the phylum Firmicutes, highlighting the bacterial genera Staphylococcus and Streptococcus, followed by Proteobacteria, with the genera Haemophylus and Enterobacter; and Actinobacteria, with Corynebacterium and Propionibacterium (Cultibacterium). The most frequently identified bacterial species were Staphylococcus aureus, coagulase-negative staphylococci (CoNS) or Staphylococcus epidermidis, Streptococcus pneumoniae, Escherichia coli, Pseudomona aeruginosa, Enterobacter aerogenes, Klebsiella neumoniae, and Propionibacterium acne (Cultibacterium acne) (Figure 3).
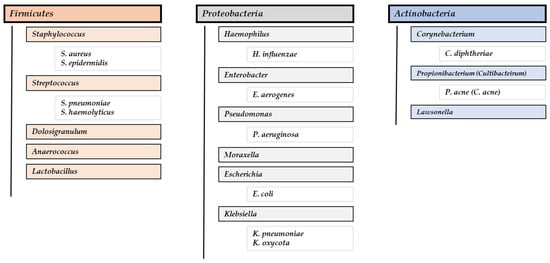
Figure 3.
Dominant bacterial phyla, genera, and species found in CRSwNP patients.
In the case of the results for fungal microbiota, different studies showed low isolation or identification of fungi [38,72,73,74,75]. All fungi reported were from the phyla Basidiomycota or Ascomycota, highlighting the following fungal genera: Aspergillus, Malassezia, and Candida [73,74,76,77,78,79]. About the few results obtained for the virus [80,81,82], note that human herpesvirus 6 (HHV-6), Epstein–Barr virus (EBV), cytomegalovirus (CMV), and Herpes simplex virus type 1 (HSV-1) showed the highest prevalence in 21 CRSwNP patients [80]. Significantly elevated IgG and IgA antibodies to influenza A virus (H3N2 and H1N1) and rhinovirus were also identified in CRSwNP patients [82].
Out of 24 studies that compared the results obtained in CRSwNP patients with those in disease control patients (non-CRS) or healthy subjects, 6 studies reported the lack of significant differences in the bacterial species or the number of different isolates obtained [73,83]; the total bacterial load [24]; both the alpha diversity (intra-community diversity mainly assessing through Chao1 index, focused on total species richness, and the Shannon index, assessing evenness in addition to richness) and beta diversity (intersample variability) [84]; the mycobiome composition [75]; or the whole microbiome identified [85]. The results shown in the rest of these studies are controversial regarding data interpretation. However, the most common differences reported were related to a decrease in alpha diversity [24,60,61,75,86,87,88,89], along with an underabundance of the bacterial genera Corynebacterium [55,64,65,86,88,90] and Dolosigranulum [64,65,84,86], as well as an overabundance of different bacteria of the phylum Proteobacteria, such as Haemophylus, Moraxella, or Pseudomonas [24,38,40,88,89,91]. Differences between both groups in the abundance or prevalence of specific Firmicutes species were also found [24,40,55,60,89,90]. The only study that compared the fungal microbiota of sinus mucosa between CRSwNP patients and control subjects obtained a significantly greater abundance of Alternaria and Ranularia and a significantly lower abundance of Cutaneotrichosporon in CRSwNP patients than in controls [75].
The studies evaluating the sinus microbiota of ECRSwNP and NECRSwNP patients showed differences in bacterial composition mainly at the genus level [59,60,61,62,63,86]. Remarkably, a higher abundance of Moraxella was found in the ECRSwNP group [60,61,63]. Likewise, prospective cohort studies through the post-operative follow-up of CRSwNP patients for one or five years showed no significant differences in microbial diversity between patients with recurrence or non-recurrence of nasal polyps (NPs). However, a notable variation in the abundance of specific bacterial genera was also observed [64,92].
Finally, significant differences in the nasal microbiota composition at different sample types but not at sample sites have been reported [90,93,94]. Gender-specific differences were also found in CRSwNP patients who used intranasal corticosteroid spray, obtaining a significantly higher abundance of Corynebacterium in men than in females [95]. Three studies showed that the bacterial spectrum changed after functional endoscopic sinus surgery (FESS) [38,79,96], and specific bacterial genera were significantly correlated with the disease severity measured using the Lund–Mackay score in computed tomography (CT) scans [65,86,94]. There was controversy about the relationship between the microbiota and clinical characteristics of CRSwNP patients, such as asthma, allergy, and sensitivity to drugs [24,38,97,98].

Table 1.
Summary of the main findings of the included studies focused on the microbiota composition analysis in CRSwNP patients.
Table 1.
Summary of the main findings of the included studies focused on the microbiota composition analysis in CRSwNP patients.
| Ref. | Study Type | Objective | Sample Size | Country | Age (Average) | Sex (n with CRSwNP) | Other Disease (n with CRSwNP) | Sample Type | Methodology | Results/Conclusion | Observ. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [73] | CSS | To compare the predominant bacteriological profiles in the middle meatus of Chinese CRSwNP and CRSsNP patients and DC subjects. | 537 (285 completed the study) CRSwNP: 165 CRSsNP: 76 DC: 44 | China | 18–80 CRSwNP: 18–78 (45.2) | M: 185 (109 with CRSwNP) F: 100 (56) | AS: 14 (13 with CRSwNP) AL: 11 (10) AsS: 1 (1) | MMSS collected during ESS | SMT | The most common bacteria were Coagulase-negative staphylococci (CoNS), Streptococcus, Corynebacterium spp., Staphylococcus aureus, and Haemophilus influenzae. No significant differences in the species or the number of different bacterial isolates between CRSwNP and DC. Very few fungi were isolated: one case each of Penicillium notatum, Verticillium, Aspergillus, and Schizophyllum. | No antibiotics or corticosteroids in the previous two weeks |
| [80] | CS | To evaluate human herpesviruses (HHV) 1–6 and community-acquired respiratory viruses (CARVS) prevalence in CRSwNP patients undergoing FESS | 35 CRSwNP: 35 | Italy | CRSwNP: 23–77 (50.3) | M: (25) F: (10) | AS: (8) AL: (15) | Bioptic samples of NP collected during FESS | MT (PCR and qPCR) | 60% of patients (21/35) were positive for at least one virus in at least one specimen studied. The highest prevalence was found for herpesviruses 6 (HHV-6), Epstein–Barr virus (EBV), cytomegalovirus (CMV), and Herpes simplex virus type 1 (HSV-1). | NA |
| [96] | RCT | To evaluate the efficacy of long-term antibiotic therapy to prevent recurrence of NP | 66 CRSwNP: 66 (55 completed the study) | Russia | 18–77 (48.7) | M: 36 F: 30 | AS: 35 AT: 19 AERD: 27 | MMSS pre-FESS and post-FESS | SMT (system Microscan walk away 40) | The most common bacteria were S. aureus, Streptococcus haemolyticus, Escherichia coli, Pseudomonas aeruginosa, and Enterobacter aerogenes. The bacterial spectrum changed significantly after surgery. | No corticosteroids |
| [66] | CS | To evaluate the association between bacterial infection and surgical outcomes following FEES | 71 CRSwNP: 71 | Republic of Korea | NA | M: 42 F: 29 | * Patients with a history of asthma were excluded | Maxillary sinus samples after MM antrostomy | SMT | Most of the patients (55/71, 77.5%) showed positive culture results. The most common bacteria were S. epidermidis, Propionibacterium acne, Corynebacterium, and E. aerogenes. The “normal flora group” (S. epidermidis and Corynebacterium) had the worst prognosis of postoperation, while the “culture-negative group” had the best prognosis. | NA |
| [99] | CSS | To compare the diversity of nasal microbiota and their secreted extracellular vesicles between CRSwNP patients and DCs | 11 CRSwNP: 5 CRSsNP: 3 DC: 3 | Republic of Korea | 19–67 (43.1) CRSwNP: 23–67, (45.6) | M: 8 (4) F: 3 (1) | AT: 3 (1) | Nasal lavage fluid samples during ESS | MT (sequencing, OTUs) | The major bacterial genera were Pseudomonas, Haemophilus, Staphylococcus, Moraxella, Enterobacter, and Fusobacterium *. | No antibiotics or corticosteroids in the previous month |
| [100] | CSS | To determine whether smoking affects CT score, bacterial diversity of the upper airways, and distribution of inflammatory cells in nasal mucosa in CRS patients | 64 CRSwNP: 20 CRSsNP: 17 DC: 27 | Slovakia | CRSwNP: 22–76 (49.6) | NA | Patients with a history of asthma, atopy, and aspirin intolerance were excluded | MMSS | SMT | The most common bacteria were CoNS, S. aureus, and Corynebacterium species. | No antibiotics in the previous month |
| [70] | RCT | To compare the efficacy of topical nasal corticosteroids either as monotherapy or combined in eradicating the biofilm of NP | 44 CRSwNP: 44 (34 completed the study) | Turkey | NA | M: 26 F: 18 | NA | NP | Scanning electron microscopic (SEM) examination | In the initial baseline SEM examination, biofilm prevalence was 68.0% (23/34). | No antibiotics and/or corticosteroids in the previous month |
| [81] | CSS | To determine the presence of respiratory viruses in the paranasal sinuses of CRSwNP and CRSsNP patients compared to DCs | 35 CRSwNP: 13 CRSsNP: 8 DC: 14 | USA | CRSwNP: (55.3) | M: 19 (9) F: 16 (4) | AS: 15 (11) AR: 19 (11) AERD: 2 (2) | MMSS | MT (RT-PCR) | The presence of viruses (Coronavirus) was detected in only 7.7% of patients (1/13). None of the controls had a positive screen. | NA |
| [71] | CCS | To determine the presence of bacterial biofilm on the sinus mucosa of CRSwNP and CRSsNP patients and DCs | 100 CRwNP: 18 ACP: 12 CRSsNP: 20 DC: 50 | India | NA | NA | NA | Nasal–sinus tissue sample | SMT | Bacterial biofilm was detected in 66.7% of patients (12/18). | NA |
| [97] | CSS | To determine whether Gram-negative bacterial carriage impacted disease evolution and inflammatory profile in CRSwNP patients | 337 CRSwNP: 337 | Canada | NA (approx. 50) | NA | AS: aprox. 200 AL: 215 ASA: 101 (self-reported) | MMSS | SMT | The most common bacteria were CoNS, S. aureus, and C. diphtheriae. P. aeruginosa carriage was associated with a higher self-reported incidence of asthma. | NA |
| [95] | CSS | To evaluate the impact of saline irrigation and topical corticosteroids on the post-surgical sinonasal microbiota of CRSwNP patients and DCs | 42 CRSwNP: 14 DC: 28 | USA | 22–77 CRSwNP: 27–65 (52.0) | M: 15 (3) F: 27 (11) | NA | Nasal cavity and maxillary swab samples | MT (sequencing, 16S RNA gene sequences) | The most abundant bacteria were Propionibacterium, Corynebacterium, S. aureus, S. epidermis, and Staphylococcus pasteuri. A higher proportional abundance of Corynebacterium, Serratia, and Finegoldia was found in men than in women who used intranasal steroid spray. | No antibiotics or corticosteroids in the previous two months |
| [101] | CSS | To determine the association between smoking history and sinonasal microbiome alterations in both CRS patients and DCs | 101 CRSwNP: 22 CRSsNP: 48 DC: 31 | USA | >18 | M: 59 F: 42 | AS: 31 AR 60 | MMSS collected during ESS | MT (PCR and sequencing, OTUs) | The most abundant genera were Staphylococcus, Corynebacterium, Carnobacteriaceae, and Streptococcus. Smoking had a stronger effect on the microbiota at the phylum level (Bacteroides, Firmicutes, and Proteobacteria). Cigarette-smoking history was associated with less bacterial diversity, with a significant decrease in the phylum Firmicutes and an increase in the genera Carnobacteriaceae. | No systemic corticosteroids for at least one month |
| [76] | CSS | To determine the presence of specific fungal microbial species in CRS patients and DCss | 28 CRSwNP: 15 Allergic fungal rhinosinusitis: 3 Fungus ball: 3 DC: 7 | USA | CRSwNP: (49.0) | M: 17 (9) F: 11 (6) | AS: 12 (10) AsS: 4 (4) | Ethmoid and maxillary sinus brush samples | MT (qPCR) | Malassezia spp., M. restricta, and M. globosa were identified in ten, seven, and four CRSwNP patients, respectively. | NA |
| [67] | CSS | To define the bacteriology of CRSwNP and CRSsNP patients and DCs | 163 CRSwNP: 60 CRSsNP: 50 DC: 26 HC: 27 | Israel | CRSwNP: (51.2) | M: (37) F: (23) | NA | MMSS pre-FESS | SMT | Positive cultures (52/60) mainly for pathogenic bacteria (47/60) were found in most of the patients (86.7% and 78.3%, respectively). A higher rate of Gram-negative bacteria isolates than Gram-positive bacteria was found. The pathogenic bacteria most frequently isolated were S. aureus, Citrobacter diversus, Proteus mirabilis, Enterobacter, Pseudomonas, Klebsiella oxytoca, S. pneumoniae, and Klebsiella pneumoniae. | No antibiotics in the previous month |
| [68] | CSS | To define the bacteriology of CRSwNP and “sinonasal complication of dental disease or treatment” (SCDDT) patients | 44 CRSwNP: 16 SCDDT: 28 | Italy | CRSwNP: (49,4) | M: 26 (13) F: 18 (3) | NA | Endosinusal pus and biopsies from nasal polyps and fungus balls collected during surgery | SMT and MT (sequencing, 16S RNA gene sequences) | 56.3% of patients (9/16) did not show microbial growth. S. aureus and other staphylococci, Peptostreptococcus spp., E. coli, and Bacteroides spp., were identified. | NA |
| [93] | CSS | To compare the nasal microbiota in regard to health state, anatomical region, and sampling strategy | 79 CRSwNP: 15 CRSsNP: 27 DC: 37 | Germany | 18–79 CRSwNP: 20–77 (52.0) | M: 50 (13) F: 29 (2) | AS: 6 (4) AR: 23 (5) AsS: 3 (3) | Swab samples at four different regions along the nasal passage (anterior and posterior vestibules and inferior meatus and MM) and tissue biopsies | MT (sequencing, 16S RNA gene sequences) | No significant differences in global bacterial profiles at the sampling sites. Significant differences between the bacterial assemblages and diversity measured for different sample types (tissue biopsies and swabs). | No antibiotics at the time of sampling |
| [102] | CSS | To determine the association between the sino-nasal microbiota and toll-like receptor (TLR) activation in DCs and CRS patients | 36 CRSwNP: 11 CRSsNP: 9 CRS/CF: 6 DC: 10 | New Zealand | 18–84 (43.9) CRSwNP: 18–71 (41.1) | M: 14 (7) F: 22 (4) | AS: 2 (8) AsS: 2 (0) | Nasal lavage and sino-nasal mucus samples collected during ESS | MT (qPCR and sequencing, OTUs) | Pseudomonas, Haemophilus, Enterobacter, and Staphylococcus were the dominating genera. | No antibiotics and prednisone |
| [103] | CSS | To determine the association of distinct pathogenic sinus microbiota with specific innate and adaptive immune responses and the relative risk of NP | 76 (69 completed the study) CRSwNP: 32 CRSsNP: 27 DC: 10 | USA | 18–88 (46.6) CRSwNP: 19–88 (48.4) | M: 40 (21) F: 29 (11) | AS: 18 (12) CF: 9 (7) | Sinus brushing samples collected during ESS | MT (qPCR and sequencing, OTUs) | Most of the patients clustered into a subgroup typically dominated by Corynebacteriaceae | Most of patients (30/32, 93.8%) had taken pre-operative antibiotics (<3 months) |
| [90] | CSS | To compare the microbiota of the MM and inferior meatus in HCs, AR, and CRS patients and characterize intra- and inter-subject and inter-group differences | 65 (48 for mapping intrasubject microbiota diversity and composition) CRSwNP: 18 CRSsNP: 15 AR: 11 HC: 4 | USA | NA * | NA * | NA | MM and inferior meatus swab samples | MT (sequencing, OTUs) | No differences in phylogenetic diversity or Shannon diversity between MM and inferior meatus-associated microbiota. No differences in beta diversity across all subjects. Taxa enriched included Staphylococcus and Alloiococcus, as well as low-abundance Corynebacterium, Haemophilus, Prevotella, and Porphyromonas compared to HC. | No antibiotics and/or corticosteroids in the previous month |
| [74] | CSS | To analyze and quantify the sinonasal mycobiome in HC and CRS patients in an attempt to better elucidate its role in sinus disease | 90 CRSwNP: 31 CRSsNP: 32 DC: 27 | Australia | NA | NA | AS and AL | MMSS intra-operatively collected | SMT and MT (sequencing, OTUs) | Fungi were detected in 12.9% of patients (4/31) (Aspergillus, Fusarium, and without fungus identified). | NA |
| [104] | CSS | To study the association between inflammatory cells and signaling markers of CRS endotypes and the sinonasal bacterial community patterns | 110 CRSwNP: 46 CRSsNP: 46 CRS/CF: 7 DC: 17 | New Zealand (Most of the patients were European (31/38)) | 18–84 CRSwNP: 18–71 (48.0) | M: 55 (25) F: 55 (14) | AS: 48 (28) AsS: 14 (40) AERD: 11 (11) | Tissue biopsies collected from the bulla ethmoidal | MT (qPCR and sequencing, OTUs) | Patients were grouped in subject clusters mainly associated with Staphylococcus, Corynebacterium, Streptococcus, and Propionibacterium. | Most of the patients (35/39, 89.7%) had not taken pre-operative antibiotics and corticosteroids (<3 months) |
| [105] | RCT | To describe the effect of oral antibiotics and corticosteroids on the bacterial microbiome within the paranasal mucus in CRS patients | 26 CRSwNP: 13 CRSsNP: 13 | New Zealand | 22–67 (48.9) CRSwNP: 29–64 (49.5) | M: 13 (7) F: 13 (6) | NA | MMSS | MT (qPCR and sequencing, OTUs) | Bacterial communities were typically dominated by Corynebacterium and Staphylococcus and at lower abundance by Streptococcus, Dolosigranulum, Haemophilus, and Moraxella. | No antibiotics and systemic corticosteroids in the previous month |
| [106] | CCS | To detect bacteria in culture-negative cases of CRS using 16S rRNA gene PCR and sequencing | 20 CRSwNP: 15 CRSsNP: 5 | India | NA | NA | NA | Discharge from the sinus and mucosal biopsies from the MM region collected during FESS | SMT and MT (qPCR and sequencing) | Two patients with a history of a previous sinus surgery yielded Staphylococcus spp. by qPCR (2/15, 13.3%). MRSA was isolated from one of them. | Cases with a history of a previous sinus surgery also had history of prior treatment with corticosteroids |
| [38] | CCS | To compare the microbiological features in middle meatus samples from CRSwNP and CRSsNP patients and DCs | 251 CRSwNP: 136 CRSsNP: 66 DC: 49 | China | CRSwNP: (45.4) | M: 154 (89) F: 96 (47) | AS: 41 (37) AR: 85 (61) | MMSS pre-ESS | SMT | Most patients (120/136, 88.4%) showed a positive culture result. The most abundant bacteria were CoNS, Corynebacterium, and S. epidermidis. The isolate rate of fungi was very low (3.7%). The strains were mainly Gram-positive aerobic and facultative anaerobic bacteria (69.8%). Patients with asthma showed a significantly lower isolation rate of Corynebacterium and P. aeruginosa. Patients with a history of ESS exhibited a significantly lower isolation rate of CoNS, and a significantly higher isolation rate of P. aeruginosa. A relatively high proportion of Citrobacter was observed compared with DCs. The isolation rate of S. aureus in the subgroup of patients with an increased percentage of eosinophils (>5%) in peripheral blood was higher than that in the subgroup with a standard percentage of eosinophils. | No antibiotics and glucocorticoids at least one month before surgery |
| [72] | CS | To investigate the relevance of the bitter-taste receptor TAS2R38 genetic variants in the susceptibility to bacterial infections associated with in vivo biofilm formation in CRSwNP patients | 100 CRSwNP: 100 | Italy | CRSwNP: (53.0) | M: (68) F: (32) | NA | Sinonasal mucosa samples pre-FESS | SMT and confocal laser scanning microscopy assay | 63.0% of patients (63/100) showed positive culture result. The most common bacteria were S. epidermidis, S. aureus, and Enterobacteriaceae (Klebsiella spp., Citrobacter koseri, and Serratia marcescens). Only in one sample was found a mixed microbiota composed of Candida albicans with S. aureus. 19 of 43 samples (44.2%) were biofilm-positive. Biofilms were associated with Klebsiella, Citrobacter, Haemophilus, Kocuria, S. aureus, and S. epidermidis. | No antibiotics or corticosteroids in the previous month |
| [85] | CSS | To evaluate the bacterial community composition on the distinct types of CRS compared to healthy bacterial communities | 18 CRSwNP: 5 CRSsNP: 5 CRS with unilateral purulent maxillary: 5 DC: 3 | Germany | 13–>70 CRSwNP: 13–29 | M: 8 F: 10 | NA | MMSS and tissue samples collected during ESS | SMT and MT (sequencing, OTUs) | Enterobacteria, Staphylococci, coryneform bacteria, Propionibacteria, Viridans streptococci, and Haemophilus were identified. The most common bacteria were S. epidermidis, P. acnes, and Corynebacterium spp. No significant differences were found in the microbiome between patients and DCs. | All patients had eosinophilia (>5%). No antibiotics in the previous month |
| [24] | CSS | To compare the bacterial communities of HCs with CRSwNP patients with (CRSwNP+A)/without (CRSwNP-A) comorbid asthma | 58 CRSwNP: 41 (CRSwNP+A: 20 CRSwNP-A: 21) HC *: 17 | Belgium | CRSwNP+A: 45.8 CRSwNP-A: 47.5 | M: 31 (22) F: 27 (19) | AS: (20) AT: (20) AaS: (7) | MMSS and tissue samples collected during ESS | MT (sequencing, OTUs) | HCs and CRSwNP patients had about the same total bacterial load, but the bacterial diversity and evenness were significantly lower in the CRSwNP group, especially the CRSwNP-A group (both evenness and Shannon’s diversity), compared with HCs. The phylum Proteobacteria and genus Haemophilus (H. influenzae) were more abundant than in HCs. In contrast, Staphylococcus xylosus and Bifidobacterium longum were less prevalent and abundant than in the HCs. The most abundant species in CRSwNP-A was S. aureus, and E. coli was found in high amounts in CRSwNP+A. | No antibiotics or systematic corticosteroids in the previous three months * |
| [77] | CSS | To characterize the sinonasal fungal communities (mycobiota) in CRS patients and DCs via the fungal ITS2 marker amplicon sequencing | 144 CRSwNP: 49 CRSsNP: 50 CRS/CF: 7 DC: 38 | New Zealand (Most of the patients were European (111/144, 77.1%)) | 18–84 CRSwNP: 18–71 (50.0) | M: 72 (29) F: 72 (19) | AS: 58 (35) AsS: 18 (15) | MMSS collected during ESS | MT (sequencing, ZOTUs) | At the phylum level, Basidiomycota and Ascomycota showed the highest RA. The most abundant fungi were Malassezia, followed by Davidiella. | Most of the patients had not taken antibiotics (41/49, 83.7%) and corticosteroids (44/49, 89.8%) in the previous month |
| [107] | RCT | To investigate the safety and preliminary efficacy of Manuka honey (MH) with augmented methylglyoxal (MGO) rinses in recalcitrant CRS | 25 CRSwNP: 20 (10 with useful information) CRSsNP: 5 | New Zealand | 27–86 CRSwNP: 49–69 | M: 14 F: 11 | AS: 10 AR: 12 AsS: 2 | Sinonasal swab samples post-EES | SMT | The most common and abundant bacteria were S. aureus and Pseudomonas. | NA |
| [108] | CSS | To describe the sinus microbiota of acute exacerbations in CRSwNP, CRSsNP, and allergic fungal rhinosinusitis (AFRS) patients | 143 CRSwNP: 55 CRSsNP: 65 AFRS: 14 | USA | (52.7) CRSwNP: (53.2) | M: 75 (33) F: 59 (22) | AS: 56 (38) AL: 66 (33) AsS: 9 (7) | Aspiration samples of purulent secretions from within the MM or previously opened sinus | MT (sequencing, OTUs) | The most common bacteria were Staphylococcus spp. (S. aureus and S. epidermidis), Pseudomonas spp., Haemophilus spp. Enterobacter spp., and Corynebacterium spp. Staphylococcus spp., Pseudomonas spp., and Streptococcus spp. showed the most RA. An average of 3 taxa per specimen isolated showed a low level of diversity in acute exacerbation CRSwNP | Some patients (no data) had taken antibiotics and corticosteroids |
| [69] | CS | To demonstrate differential expression of trefoil family factor (TFF) protein genes in CRSwNP patients and the impact of bacterial colonization on their expression. | 54 CRSwNP: 29 DC: 25 | Croatia | 21–69 CRSwNP: 26–69 (53.4) | M: 30 (16) F: 24 (13) | AERD: (3) | Nasal and sinus swab samples collected during FESS | SMT | Most of the patients (23/29, 79.3%) showed positive culture results, of which 15 had isolated pathogenic bacteria and 8 nonpathogenic bacteria (S. epidermidis). * Pathogenic bacteria isolated: S. aureus, E. coli, Group B S. haemolyticus, Morganella morganii, Enterobacter spp., Serratia marcescens, P. mirabilis, Enterobacter freundii, and K. oxytoca. | Patients had taken corticosteroids in the previous three weeks and some cases had also taken antibiotics (no data) |
| [109] | CCS | To identify a microbiome profile in CRSwNP and CRSsNP patients | 20 CRSwNP: 10 CRSsNP: 10 | Indonesia | 18–>50 | M: 9 F: 11 | NA | Nasal tissue sample collected during FESS | MT (sequencing, OTUs) | The most common bacteria (phyla) were Proteobacteria, Firmicutes, Cyanobacteria, Fusobacteria, Actinobacteria, and Bacteoidetes. | NA |
| [57] | CS | To identify trends in bacteria isolated and their antibiotic resistance from Korean adults with CRS | 510 CRSwNP: 376 (ECRSwNP: 36 NECRSwNP: 22) CRSsNP: 134 | Korea | >18 | NA | AS: (33) AT: (51) | Purulent discharge in the maxillary and ethmoid sinuses samples collected during ESS | SMT | 73.9% of patients (278/376) showed positive culture results. The most common bacteria were CoNS (S. epidermidis), Streptococcus spp., Corynebacterium, Propionibacterium spp., Haemophilus spp., S. aureus, and Klebsiella spp. S. epidermidis, Corynebacterium spp., and Enterobacter spp. were significantly associated with ECRSwNP, and Haemophilus spp., Klebsiella spp., and P. aeruginosa with NECRSwNP. | No antibiotics or systemic corticosteroids for at least the previous month |
| [110] | CSS | To stratify CRS patients based on their microbial community compositions using a probabilistic modeling approach and the traditional phenotypic approach | 31 CRSwNP: 8 CRSsNP: 8 CRS/CF: 7 DC: 8 | New Zealand | >18 | NA | NA | Ethmoidal sinus biopsy specimens collected during FESS | MT (sequencing, OTUs) | Staphylococcus, Streptococcus, Propionibacterium, and Corynebacterium were prevalent in a majority but at low RA. In CRSwNP, Moraxella and Stenotrophomonas were dominant but showed less Streptococcus and Veillonella than DC. | No antibiotics or systemic corticosteroids in the previous month |
| [111] | CSS | To identify reactive allergens of IgE antibodies produced locally in NPs | 51 ECRSwNP: 46 (4 finally included) DC: 15 | Japan | ECRSwNP: 39–77 (53.3) | M: (2) F: (2) | AS: (3) | Swab and NP samples | SMT | Moraxella catarrhalis, Corynebacterium spp., and S. aureus were identified. | NA |
| [86] | CSS | To characterize the differences in microbiome profiles between CRSwNP patients and DCs | 86 CRSwNP: 59 DC: 27 | China | CRSwNP: (46.4) | M: 53 (35) F: 33 (24) | AS: 12 (11) AR: 16 (14) | MMSS collected during FESS | MT (sequencing, OTUs) | The predominant bacterial phyla were Firmicutes, Proteobacteria, Actinobacteria, Bacteroidetes, and Fusobacteria. The predominant bacterial genera were Lactobacillus, Corynebacterium, Staphylococcus, Streptococcus, Erysipelotrichales, Escherichia–Shigella, Haemophilus, Enterobacter, Propionibacterium, and Pseudomonas. CRSwNP had a lower nasal microbiome richness than DC. The RA of Actinobacteria (predominantly Corynebacterium), and Dolosigranulum was significantly lower in CRSwNP than in DC. Lactobacillus, Escherichia–Shigella, Turicibacter, Clostridium, Enterococcus, and Romboutsia were positively correlated with the severity of CRSwNP (Lund–Mackay CT score). Smoking status, asthma, or allergic rhinitis did not change the microbiome distribution. | No antibiotics and corticosteroids in the previous month |
| [112] | CSS | To compare bacterial community composition and absolute abundances of S. aureus and S. epidermidis between CRS patients and DCs | 54 CRSwNP: 18 CRSsNP: 22 DC: 14 | New Zealand (Most of the patients were European (44/54, 81.5%)) | CRSwNP: (53.2) | M: 31 F: 23 | AS: 14 (10) | MMSS | MT (qPCR and sequencing, OTUs) | The most common bacteria were Corynebacterium, Haemophilus, Staphylococcus, and Dolosigranulum. CRSwNP had a significantly higher overall bacterial load than DCs. | Most of the patients had taken antibiotics and corticosteroids in the previous year |
| [58] | CSS | To investigate the expression of lipopolysaccharide (LPS) and its relationship with glucocorticoid receptors (GRs) in CRSwNP | 162 CRSwNP: 112 (ECRSwNP: 49 NECRSwNP: 63) | China | CRSwNP: 13–71 (ECRSwNP: 19–65 (46.0) NECRSwNP: 13–71 (44.0)) | M: 91 (65, ECRSwNP: 28, NECRSwNP: 37) F: 71 (47, ECRSwNP: 21, NECRSwNP: 26) | AS: (8, ECRSwNP: 5, NECRSwNP: 3) AT: (5, ECRSwNP: 4, NECRSwNP: 1) | Swab samples and specimens pre-ESS | SMT | 82.1% of patients (82.1%) showed positive culture. The positive rate of bacterial culture of different groups was not different. The main bacterial strains were S. epidermidis, CoNS, E. coli, S. pneumoniae, and K. pneumoniae. | No corticosteroids in the previous two weeks |
| [113] | CS | To verify if topical administration of Lactobacillus lactis W136 to the nasal and sinus cavities would be safe for CRS patients refractory to medical and surgical treatment | 27 (24 completed the study) CRSwNP: 17 CRSsNP: 7 | USA | (54.9) | M: 11 F: 13 | AS: 18 AL: 5 | Nasal swab and brushing samples pre-ESS and post-ESS | SMT and MT (sequencing, OTUs) | Conventional culture: Oropharyngeal flora, CoNS, S. aureus, and P. aeruginosa were the most common bacteria. | No antibiotics and corticosteroids in the previous month |
| [87] | CSS | To investigate the prevalence, diversity, and abundance of archaea in the human sinuses and any associations with disease state | 60 CRSwNP: 16 CRSsNP: 15 DC: 9 HC: 20 | New Zealand (Most of the subjects were European (44/60, 73.3%)) | CRSwNP: (52.8) | M: 37 (14) F: 23 (2) | AS: 19 (6) | MMSS collected during ESS | MT (sequencing, ASVs; and digital PCR) | Phyla Euryarchaeota and Thaumarchaeota were detected. The most abundant bacteria were Corynebacterium, Staphylococcus, Moraxella, Lawsonella, and Haemophilus. CRSwNP subjects showed significantly decreased alpha diversity than HCs. | Most of the patients (13/16, 81.3%) had not taken antibiotics in the previous month |
| [114] | CSS | To establish associations among medication usage, the sinus microbiota, and patients’ clinical outcomes | 236 CRSwNP: 79 CRSsNP: 77 DC: 45 HC: 35 | New Zealand (Most of the subjects were European (191/236, 80.9%)) | 18–82 CRSwNP: 18–75 (46.0) | M: 100 (26) F: 136 (53) | AS: 78 (72) | MMSS and tissue samples intra-operatively collected | MT (sequencing, ASVs) | The most common bacteria were Corynebacterium and Staphylococcus The number of observed ASVs was significantly lower when compared to HCs. | Most of the patients (67/78, 85.9%) had not taken antibiotics in the previous month. |
| [115] | CSS | To analyze the bacterial flora of the nose and paranasal sinuses in CRS patients who underwent ESS over 65 years of age compared to a younger group of patients (<40 years) | 529 (269 completed the study) CRSwNP: 150 CRSsNP: 119 | Poland | >18 | M: 147 F: 122 | AS, AL, and AERD | MMSS collected during ESS | SMT | The most common bacteria was S. aureus. There were no statistically significant differences between the occurrence of a particular type of bacteria and the presence of NP in both age groups. | No antibiotics and systemic corticosteroids in the previous month |
| [59] | CSS | To investigate whether the sinus microbiota in CRSwNP is associated with eosinophilic inflammation | 37 CRSwNP: 31 (ECRSwNP: 21 NECRSwNP: 10) DC: 6 | Republic of Korea | ECRSwNP: (50.6) NECRSwNP: (37.3) | NA | AT: (13, ECRSwNP: 10, NECRSwNP: 3) AS: (8, ECRSwNP: 8) * Patients with AERD were excluded | MMSS | MT (sequencing, OTUs) | The most common bacteria were Firmicutes (mainly Staphylococci), Actinobacteria (mainly Corynebacterium, Bifidobacterium, and Propionibacterium species), and Proteobacteria (mainly Moraxella, Pseudomonas, Enterobacter and Aggregatibacter). ECRSwNP: RA of Anaerococcus, Tepidimonas, and Mesorhizobium were significantly decreased and Lachnoclostridium increased compared to those in DCs. ECRSwNP patients had higher asthma incidence and clinical severity scores. NECRSwNP: RA of Lachnospiraceae was increased compared with that in DCs. Deinococcus, Sphingomonas, and Lactobacillus were positively correlated with serum extracellular vesicles (EVs). | No antibiotics and systemic corticosteroids for at least the previous month |
| [55] | CSS | To characterize the normal microbiome, assess for any geographical or clinical influences, and identify any changes associated with CRS within and across geographical sites | 532 (410 reached the final stage of analysis) CRSwNP: 172 CRSsNP: 99 DC: 139 | Australia New Zealand Thailand India Brazil Chile The Netherlands Canada USA | 20–75 | NA | AS and AsS | MMSS collected during ESS | MT (sequencing, ASVs) | The most abundant bacteria were Corynebacterium, Staphylococcus, Streptococcus, Haemophilus, and Moraxella. Corynebacterium was significantly reduced and Streptococcus increased compared to DCs. | Clinicians were free to treat patients |
| [98] | CSS | To compare the bacterial flora in CRSwNP and CRSsNP patients and investigate a possible link between the type of bacterial flora and the coexistence | 470 (458 completed the study) CRSwNP: 245 CRSNsNP: 213 | Poland | M: (50.6) W: (49.8) | M: 248 F: 222 | AS: 104 (83) AL: 87 (52) AsS and other non-steroidal anti-inflammatory drugs: 53 (44) | MMSS collected during ESS | SMT | Gram-negative intestinal bacilli Enterobacteriaceae, CoNS and streptococci, and S. aureus were the most common bacteria. No statistically significant relationship was found between bacterial flora and the presence of asthma, hypersensitivity to drugs, or allergy. No statistical significance between the occurrence of a particular flora and the multiplicity of operations. | No antibiotics in the previous month |
| [88] | CSS | To characterize the microbiome dysbiosis in AERD patients | 37 AERD: 17 HC: 17 | USA | NA | NA | AERD: (17) | Inferior turbinate swab samples | MT (sequencing, OTUs) | AERD subjects showed reduced bacterial diversity (fewer species per sample and lower Shannon Diversity indexes). Moraxella, Corynebacterium, Pseudomonas, Staphylococcus, Sphingomonas, Streptococcus, Propionibacterium, and Eikenella showed the highest RA. Overabundance of Eikenella corrodens, M. catarrhalis, and Pseudomonas (Proteobacteria phylum) and underabundance of Corynebacterium in AERD patients compared to HCs. | No recent use of antibiotics and corticosteroids |
| [89] | CSS | To analyze the effects of antibiotics on the nasal microbiome and secreted proteome in CRS patients | 99 CRSwNP: 40 CRSsNP: 30 DC: 29 | Republic of Korea | CRSwNP: (48.8) | M: 67 (27) W 32 (13) | AS: 4 (2) AT 31 (13) AR: 33 (8) | Nasal secretion samples from MM | MT (sequencing, OTUs) | Corynebacterium (Actinobacteria), Staphylococcaceae (Firmicutes), Streptococcaceae (Firmicutes), Burkholderiaceae (Proteobacteria), Lachnospiraceae (Firmicutes), Veillonellaceae (Firmicutes), Propionibacteriaceae (Actinobacteria), and Moraxellacea (Proteobacteria) showed the highest level of RA. Shannon and Simpson indexes were significantly decreased across CRSwNP to DCs. The sinonasal microbiota of the CRSwNP showed significantly decreased bacterial diversity. Firmicutes and Bacteroidetes (Prevotellaceae) were significantly decreased compared to DCs. Cyanobacteria, Staphylococcaceae, Propionibacteriaceae, and Moraxellaceae were significantly increased compared to DCs. In the NABX (subjects who had not taken antibiotics three months before sampling) group, the Shannon and Simpson indexes were significantly decreased compared to DCs. Shannon and Simpson indexes were significantly lower in the ABX group than in the NABX group. Streptococcaceae, Lachnospiraceae, and Neisseriaceae were significantly decreased in the ABX group compared to the levels in the NABX group. | Some patients (24/40, 60%) had not taken antibiotics in the previous three months |
| [60] | CSS | To evaluate the bacterial community composition on distinct types of CRSwNP patients (ECRSwNP and NECRSwNP) | 73 CRSwNP: 34 (ECRSwNP: 16 NECRSwNP: 18) HC *: 39 | China | ECRsWNP: (48.3) NECRSwNP: (28.5) | M: 36 (18, ECRSwNP: 11, NECRSwNP: 7) F: 37 (16, ECRSwNP: 5, NECRSwNP: 11) | AS: (2, ECRSwNP: 2) * Patients with AERD were excluded | MMSS collected during FESS | MT (sequencing, OTUs) | The most common bacteria were Firmicutes, Actinobacteria, Proteobacteria, and Bacteroidetes. The most abundant genera were Staphylococcus, Corynebacterium, and Dolosigranulum. The diversity of sinus microbiota (Chao1 and Shannon indexes) was significantly lower in the CRSwNP than in DC. ECRSwNP: Firmicutes, Actinobacteria, and Proteobacteria. Staphylococcus, Corynebacterium, and Moraxella. NECRSwNP: Firmicutes, Actinobacteria and Bacteroidetes. Staphylococcus, Dolosigranulum, and Corynebacterium. Staphylococcus was significantly lower in the ECRSwNP compared to HC. The Shannon index significantly decreased only in the NECRSwNP, but not in the ECRSwNP, compared to HCs. Staphylococcus (S. aureus) abundance was the lowest in the ECRSwNP. The abundance of S. aureus was the highest in the NECRSwNP. The abundance of Moraxella was significantly decreased in the NECRSwNP compared with that in the ECRSwNP. The abundance of Haemophilus was significantly increased in the NECRSwNP compared to HC. | No antibiotics or corticosteroids in the previous month |
| [64] | CS | To explore nasal microbial diversity effects on the pathogenesis and prognosis of CRSwNP | 147 CRSwNP: 77 (NP recurrent: 12, NP non-recurrent: 65) CRSsNP: 36 DC: 34 | China | CRSwNP: (46.4) (NP recurrent: (48.6), NP non-recurrent: (49.7)) | M: 86 (43, NP recurrent: 5, NP non-recurrent: 36) F: 61 (34, NP recurrent: 7, NP non-recurrent: 29) | AS: 14 (11, NP recurrent: 3, NP non-recurrent: 8) AR: 22 (14, NP recurrent: 4, NP non-recurrent: 10) | MMSS collected during ESS and MM secretions after 1-year post-ESS | MT (sequencing, OTUs) | The most abundant bacteria were Lactobacillus, Corynebacterium, Staphylococcus, Streptococcus, Escherichia–Shigella, Enterobacter, Haemophilus, Moraxella, and Propionibacterium. The RA of Actinobacteria (Corynebacterium), Chlamydia, and Dolosigranulum was significantly lower than that in DCs. Lactobacillus, Escherichia–Shigella, Turicibacter, Clostridium, Enterococcus, and Romboutsia were positively correlated with the severity of CRSwNP (Lund–Mackay CT score). Smoking status, asthma, or allergic rhinitis did not change the microbiome distribution. Faecalibaculum had a significant negative correlation with the TNSS of patients with CRSwNP. The abundance of Actinobacteria after surgery was significantly higher than before in the NP non-recurrent group, while there was no significant change in nasal flora in the NP recurrent group. | No antibiotics or corticosteroids in the previous month |
| [94] | CSS | To assess the microbial composition in CRS patients, comparing different sampling methods and disease subtypes | 22 CRSwNP: 8 CRSsNP: 6 DC: 8 | Republic of Korea | 21–76 CRSwNP: (48) | M: 12 (3) F: 10 (5) | AS: 2 (2) AT: 6 (1) | MMSS, tissue biopsied from the uncinate process (UT) and NP tissue collected during ESS | MT (sequencing, 16S rRNA) | Bacteroidetes, Firmicutes, Proteobacteria, Actinobacteria, and Fusobacteria were the dominant phyla. The Shannon index was significantly decreased in NP compared to UT. Firmicutes was remarkably reduced in NP, whereas Proteobacteria was more abundant in NP than in UT. Sphingomonas and Sediminibacterium were enriched in the NP, while Ralstonia was reduced in NP. Prevotella was significantly and inversely correlated with disease severity. | No antibiotics and systemic corticosteroids in the previous month |
| [61] | CSS | To investigate the changes in the clinical, histopathological, and hematological properties and the gut and airway microbiota in CRSwNP endotypes | 58 CRSwNP: 46 (ECRSwNP: 32 NECRSwNP: 14) HC: 12 | Sudan | CRSwNP: (34.7) (ECRSwNP: 34.8 NECRSwNP: (34.7)) | M: 26 (20, ECRSwNP: 13, NECRSwNP: 7) F: 32 (26, ECRSwNP: 19, NECRSwNP: 7) | AS: (4, ECRSwNP:4) AL: (1, ECRSwNP: 1) | MMSS (17) and fecal samples (10) | MT (sequencing, OTUs) | In the airway: Reduced alpha diversity in comparison to HCs. Moraxella, Parvimonas, and Porphyromonas increased more in the ECRSwNP than in the NECRSwNP. These bacteria were positively correlated with CT scores and severe disease. Prevotella 9, Succinivibrio, Lawsonella, and Exiguobacterium significantly decreased in ECRSwNP. These bacteria were negatively associated with CT scores and endoscopic score eosinophil percentage. In the gut microbiome: Actinobacteria phylum and its major genus (Bifidobacteria) were remarkably reduced in CRSwNP, mainly in ECRSwNP. Bifidobacterium and Barnesiell were negatively associated with CT score and endoscopic score. The abundance of Enterobacterales; Enterobacteriaceae; and several genera, such as Enterobacter, increased in NECRSwNP. | No antibiotics or systemic corticosteroids in the previous month |
| [78] | CS | To undertake a comprehensive multi-omics assessment of NP tissue transcriptome, proteome, and associated bacterial and fungal microbiome in CRSwNP patients | 3 CRSwNP: 3 | New Zealand (all patients were of European ancestry) | CRSwNP: 46–59 | M: (3) F: (0) | AS: (1) | NP tissue | MT (sequencing, ZOTUs) | The most abundant bacterial genera were Staphylococcus, Corynebacterium, Dolosigranulum, Anaerococcus, and Propionibacterium. The most abundant fungal genera were Malassezia; Candida; Rhodotorula; and unclassified members of Malasseziales, Dothideomycetes, Mycosphaerellaceae, and Phaeophaeriacea. | No antibiotics and corticosteroids in the previous month |
| [65] | CS | To explore the effects of nasal microbial diversity and inflammatory types on the prognosis of NPs | 77 and DC CRSwNP: 77 (NP recurrent: 12, NP non-recurrent: 62) | China | CRSwNP: (NP recurrent (48.6), NP non-recurrent (49.7)) | M: (34, NP recurrent: 5, NP non-recurrent: 29) F: (43, NP recurrent: 7, NP non-recurrent: 36) | AS: (11, NP recurrent: 3, NP non-recurrent: 8) AR: (14, NP recurrent: 4 and NP non-recurrent: 10) | MMSS and NP tissue and MM secretions after 1-year post-ESS | MT (sequencing, OTUs) | The most abundant bacteria were Firmicutes, Proteobacteria, Actinobacteria, Bacteroidetes, Fusobacteria, and Spirochaetae. Actinobacteria, Corynebacterium, and Dolosigranulum were significantly lower than in DCs. There was no significant difference in nasal microbiome richness between NP recurrent and non-recurrent groups. At the genus level, the dominant bacteria were Lactobacillus, Staphylococcus, Streptococcus, and Bacteroides. Faecalibaculum was negatively correlated with the overall nasal symptoms. The RA of Actinomycetes and Corynebacterium was significantly higher, and Staphylococci was significantly lower, in the NP non-recurrent group than in the NP recurrent group. | No antibiotics and corticosteroids in the previous month |
| [116] | CSS | To identify and characterize prophages present in S. aureus from patients suffering from CRS, concerning CRS disease phenotype and severity | 67 CRSwNP: 30 CRSsNP: 28 DC: 9 | Australia | NA | NA | NA | Samples collected during ESS | SMT * | S. aureus clinical isolates were obtained (in silico: intact prophages encoding human immune evasion cluster genes and more frequent in patients with more severe disease). | NA |
| [79] | CS | To analyze the alteration in the sinonasal microbiome in CRSwNP and CRSsNP patients after FESS | 35 CRSwNP: 20 CRSsNP: 15 | India | 12–76 (40.0) | M: 19 F: 16 | NA | MMSS pre-FESS and post-FESS | SMT | Pre-FESS cultures: MRSA predominantly, followed by S. aureus, Pseudomonas, E. coli, and Aspergillus. Post-FESS culture: S. aureus and E. coli. | Postoperatively patients were prescribed antibiotics |
| [117] | CSS | To investigate the potential role of Pantoea dispersa in rhinosinusitis | 390 (274 completed the study) | Taiwan | 20–99 (53.6) | M: 156 F: 118 | AS: 8 AR: 75 | Nasal swab samples | SMT | Seven CRSwNP patients had culture growth of P. dispersa. | NA |
| [40] | CSS | To examine the bacterial communities of the sphenoidal sinus in Iranian patients with and without CRS | 36 CRSwNP: 18 DC: 18 | Iran | CRSwNP: 30–63 (42.7) | M: 18 (9) F: 18 (8) | AS: 6 | Sphenoidal sinus surface mucosa swab samples collected during FESS | MT (qPCR) | The most common bacteria were Actinobacteria (Corynebacterium) and Staphylococcus spp. S. pneumoniae and H. influenza were not detected in any of the samples. S. haemolyticus and P. aeruginosa were significantly more prevalent than DCs. | No antibiotics in the previous month |
| [92] | CS | To determine whether altered nasal microbiota constituents could be used as biomarkers to predict CRSwNP recurrence | 85 (60 with complete clinical information for the establishment of a predictive model of CRSwNP recurrence) CRSwNP: 85 (NP recurrent: 39, NP non-recurrent: 46) | China | CRSwNP: 18–73 (46.4) (NP recurrent: (46.2), NP non-recurrent (46.5) | M: (64, recurrent: 28, non-recurrent: 36) F: (21, NP recurrent: 11, NP non-recurrent: 10) | AS: (17, NP recurrent: 15, NP non-recurrent: 2) | MMSS collected during ESS * | MT (sequencing, OTUs) | There was no significant difference in community diversity (OTUs, Shannon diversity index, and Chao richness), but both groups (recurrence and non-recurrence) showed distinct composition. Genera from the Proteobacteria and Firmicutes phyla were the major taxa that differed in abundance between both groups. Campylobacter, Bdellovibrio, and Aggregatibacter were more abundant than in the recurrence group. Actinobacillus, Gemella, and Moraxella were more abundant in non-recurrence. Shewanella and Preptostreptococcus exhibited a decrease in abundance, and Friedmanniella, Curvibacter, and Pseudoxanthomonas were more abundant in recurrence than non-recurrence. Porphyromonas, Bacteroides, Moryella, Aggregatibacter, Butyrivibrio, Shewanella, Pseudoxanthomonas, Friedmanniella, Limnobacter, and Curvibacter were the most important taxa discriminating recurrence from non-recurrence specimens. | No antibiotics or corticosteroids in the previous month |
| [118] | CSS | To explore the difference between sinus bacteriology in CRSwNP and CRSsNP patients and to analyze the differences in culture results from swabs taken from the MM versus the ethmoid sinus | 448 CRSwNP: 160 CRSsNP: 288 | Jordan | (40.0) CRSwNP: (39.7) | M: (96) F: (64) | NA | Ethmoid sinus and MMSS collected during FESS | SMT | The most common bacteria were MRSA, followed by CoNS and S. aureus. | No antibiotics or corticosteroids before surgery |
| [119] | CSS | To investigate the changes in microbiota and cytokines levels in CRSwNP and CRSsNP patients. | 36 CRSwNP: 12 CRSsNP: 10 DC: 15 | China | CRSwNP: (47.3) | M: 24 (9) F: (13/3) | NA | Secretions collected from the middle nasal canal, maxillary sinus, and ethmoid sinus intra-operatively collected | MT (sequencing, OTUs) | The most common bacteria were Staphylococcus, Corynebacterium, Porphyromonas, Serratia, Pseudomonas, Fusobacterium, Carnobacterium, Dolosigranulim, Cultibacterium (formerly Propionibacterium acnes), and Lawsonella. Beta diversity was significantly different between CRSwNP and DC. The abundance of C. propinquum and Carnobacterium maltaromaticum in CRSwNP differed from that in DC. Lawsonella, Moraxella, Corynebacterium, Carnobacterium, and Hafnia–Obesumbacterium were different at the genus level. | No corticosteroids in the previous month |
| [82] | CSS | To examine evidence of microbial exposure in subjects by probing serum samples of CRS patients and controls for seroreactivity to microbial protein-directed IgG and IgA | 118 CRS: 39 DC: 79 | USA | NA | NA | NA | Serum samples | MT (CRS-focused Nucleic Acid Programmable Protein Array (NAPPA)) | CRSwNP patients showed elevated sero-reactivity against S. aureus. Influenza A virus (H1N1 and H3N2) and rhinovirus B14 were identified. | No antibiotics and corticosteroids in the previous month |
| [91] | CSS | To demonstrate the role of bacteria in the pathogenesis of fungal ball (FB) versus CRSwNP and investigate the differences in microbiome profiles through a comparative analysis of microbial community diversity | 42 CRSwNP: 10 FB: 49 DC: 4 | China | CRSwNP: (41.3) | M: 15 (7) F: 28 (3)) | NA | MM and superior meatus swab samples | MT (sequencing, OTUs) | The major abundant phyla were Firmicutes, Proteobacteria, Bacteroidetes, and Actinobacteria. The abundance of TM7 (Saccharimonadia), Chloroflexi, and Bacteroidete significantly differed between the CRSwNP and DC groups. The RA of Ruminococcacea from the phylum of clostridia and Comamonadaceae from the phylum of Burkholderiales was significantly higher, while that of Lactobacillus, Bacteroides S24-7, and Desulfovibrio was significantly lower than DC. The RA of Haemophilus was increased in CRSwNP. | No antibiotics in the previous month |
| [62] | CSS | To compare the nasal bacteriology between ECRSwNP and nECRSwNP patients | CRSwNP: 295 | Taiwan | CRSwNP: 20–84 (46.1) | M: (205) F: (90) | AS: (14, ECRSwNP: 9, NECRSwNP: 5) AR: (124, ECRSwNP: 70, NECRSwNP: 54) AsS: (1, NECRSwNP: 1) | MMSS pre-FESS | SMT | The most common bacteria were S. aureus and CoNS. Culture rates were similar between ECRSwNP and nECRSwNP. Gram-negative aerobes (mainly H. influenzae and C. koseri) were significantly more isolated from the NECRSwNP than the ECRSwNP. | No antibiotics in the previous week |
| [84] | CSS | To evaluate the microbial composition in the context of the inflammatory environment in patients suffering from CRSwNP, AERD, and CRSsNP | 80 CRSwNP: 20 CRSsNP: 20 AERD: 20 DC: 20 | Austria | CRSwNP: (49.4) AERD: (46.8)) | M: 50 (CRSwNP: 16, AERD: 12) F: 30 (CRSwNP: 4, AERD: 8) | AS: 42 (CRSwNP: 16, AERD: 20) AL: 32 (CRSwNP: 8, AERD: 8) | Anterior naris swab samples and MMSS | MT (sequencing, ASV) | Corynebacteria and staphylococci showed the highest RA in both CRSwNP and AERD. No alpha and beta diversity difference was observed between the DC, the CRSwNP, and the AERD groups. Dolosigranulum was less prevalent, and Lawsonella was more prevalent in patients with NP than in DCs. A higher RA of staphylococci in the MM in AERD patients compared to CRSwNP was observed, as well as of Lawsonella in patients suffering from CRSwNP in MM and anterior naris compared to DC. | No corticosteroids in the previous two weeks |
| [63] | CSS | To characterize nasal dysbiosis in a cohort of ECRSwNP patients and compare their nasal microbiomes with those of HCs | 88 ECRSwNP: 34 Patients without CRSwNP: 10 HC: 44 | China | 18–79 ECRSwNP: 18–67 (43.8) | M: 69 (30) F: 19 (4) | AS: 7 AT: 7 | MM brush samples | MT (sequencing, ASVs, and OTUs) | ECRSwNP had higher bacterial alpha diversity (Shannon and Chao1 indexes, intra-individual bacterial diversity). The most dominant phyla were Actinobacteria and Firmicutes. ECRSwNP was defined by increased RA of Sphingomonas, Moraxellaceae, Bacteroides, Bifidobacterium, Ruminococcus, and Faecalibacterium, as well as by decreased abundances of Ralstonia, Propionibacterium, and Propionibacter. Sphingomonas was more abundant in ECRSwNP than in HCs. Parabacteroides, Akkermansia, Devosia, Sutterella, and Desulfovibrio positively correlated with the SNOT-20 score. The abundances of Dyella, Gordonia, and Moraxella were positively correlated with LM (Lund–Mackay) CT scores, whereas the abundances of Gemmiger, Faecalibacterium, Anaeroplasma, Sutterella, Blautia, Geobacillus, Bifidobacterium, Sphingomonas, Dorea, Roseburia, and Ruminococcus negatively correlated with LM CT scores. | No antibiotics and corticosteroids in the previous week |
| [83] | RCT | To assess the longitudinal effect of corticosteroid therapy on sinus microbiota in CRSwNP patients | 44 CRSwNP: 29 DC: 15 | Canada | NA | M: 25 (14) W 18 (14) | AS: 18 (18) AsS: 11 (11) | MMSS | SMT and MT (microbiotyping using MALDI-TOF-MS) | The most prevalent organisms were Staphylococcus and Corynebacterium. The difference in the number of isolated organisms and the difference between Gram-positive and Gram-negative isolates were not statistically significant between HCs and CRSwNP patients. | No antibiotics and/or corticosteroids for at least the previous month |
| [120] | CSS | To evaluate the nasal microbiome, NP inflammation mediators, and inflammatory cell infiltration in CRSwNP patients | 77 CRSwNP: 77 | China | CRSwNP: 46.4 | M: (34) F: (43) | AS: (11) AL: (14) | MMSS collected during ESS | MT (sequencing, OTUs) | The most common genus was Enterobacter. | No antibiotics and corticosteroids for at least the previous month |
| [75] | CSS | To investigate the fungal and bacterial microbiome of sinus mucosa in CRSwNP and CRSsNP patients versus HC | 92 CRSwNP: 31 CRSsNP: 31 HC: 30 | USA | (50.0) | M: 47 F: 45 | AS: 32 (20) | Ethmoid tissue and skull base collected during ESS | MT (sequencing, ASVs) | Two patients (2/31, 6.5%) had positive fungal cultures. The mycobiome composition was not significantly different between HC and CRSwNP. Saccharomycetales and Cutaneotrichosporon were lower among CRSwNP, and Alternaria species were higher among CRSwNP. Beta diversity at the ASV and the genus level differed significantly between CRSwNP and HC. CRSwNP had a significantly greater abundance of Alternaria and Ramularia and a significantly lower abundance of Cutaneotrichosporon than HC. CRSwNP had significantly lower alpha diversity compared with HC. | NA |
RCT, randomized controlled trial; CCS, case–control study; CS, cohort study; CSS, cross-sectional study; NP, nasal polyp; CRSwNP, chronic rhinosinusitis with nasal polyps; ECRSwNP, eosinophilic CRSwNP; NECRSwNP, non-eosinophilic CRSwNP; CRSsNP, chronic rhinosinusitis without nasal polyps; ACP, antrochoanal polyps; DC, disease control patient; HC, healthy control subject; M, men with CRSwNP; F, females with CRSwNP; AS, subjects with asthma; AT, subjects with atopia; AL, subjects with allergy; AR, subjects with allergic rhinitis; AsS, subjects with aspirin sensitivity; ASA, subjects with acetylsalicylic acid sensitivity; AERD, subjects with aspirin-exacerbated respiratory disease; CF, cystic fibrosis; MM, middle meatus; MMSS, MM Swab samples; ESS, endoscopic sinus surgery; FESS, functional ESS; SMT, microbial identification using standard microbiological techniques; MT, microbial identification using molecular techniques; OTU, operational taxonomic unit; ZOTU, zero-radius out; ASV, amplicon sequence variant; PCR, polymerase chain reaction; qPCR, quantitative polymerase chain reaction; RT-PCR, reverse-transcriptase PCR; RA, relative abundance; MRSA, methicillin-resistant Staphylococcus aureus; CT, computed tomography; SNOT: Sinonasal Outcome Test; TNSS, total nasal symptom scores; NA, not applicable. *: Information not fully confirmed.
3.2.2. Relationship between Microbial Dysbiosis and Inflammation in CRSwNP
The most relevant information extracted from the 21 studies that reported results about the relationship between nasal microbiota and inflammation in CRSwNP patients is summarized in Table 2. Information about each study about the study type, objective, sample size, population/country, age, sex, and other comorbidities of the patients included, as well as sample type and methodology used or other observations, is detailed in Table 1, with the only exception of two studies [121,122] (Supplementary Data S1). The methodology employed to identify or measure included molecular techniques such as polymerase chain reaction (PCR) assays, immunoassays, histological analysis, or cytometry, among other techniques.
Studies mainly focused on the bacterial microbiota, including only one ex vivo study with information on nasal fungi and viruses and no study on viruses. In detail, enzyme-linked immunosorbent assay (ELISA) showed that Aspergillus niger stimulation increased the pro-inflammatory cytokines tumor necrosis factor-alpha (TNF-α), granulocyte-macrophage colony-stimulating factor (GM-CSF), and IL-6. In contrast, Cladosporium sphaerospermum, Alternaria alternata, and Penicillium notatum stimulation reduced TNF-α and IL-6 but induced under a dose-dependent remodeling of transforming growth factor beta 1 (TGF-β1) and basic fibroblast growth factor (bFGF) [121].
Among the most remarkable bacterial results, Gram-negative bacteria were associated with an increase in blood eosinophils and serum IgE levels, just as CRSwNP patients with activity of toll-like receptors (TLRs) [73,97,102]. The peripheral blood levels of the Gram-negative bacterial product lipopolysaccharide (LPS) were also positively correlated with the expression of the glucocorticoid receptor-beta (GR-β) involved in inflammation modulation [58]. Bacterial biofilm was more frequently found in samples from subjects with non-functional taste receptor 2 member 38 (TAS2R38), a protein associated with the innate bacterial defense mechanism of the human upper airway [72]. Associations between specific bacterial groups of the core microbiota of CRSwNP patients and inflammation patterns were also reported. Thus, bacteria taxa commonly found in CRSwNP patients, including Corynebacterium or Staphylococcus, were associated with peroxisome proliferator-activated receptor gamma (PPAR-y) and retinoic acid-inducible gene I (RIG-I) signaling pathways involved in the eosinophil activation [103], as well as elevated levels of multiple inflammatory cells and cytokines [104]. A higher concentration of bacteria of the Enterobacteriaceae family was found in patients with IL-5-positive NPs [64,120] and associated with higher levels of IL-8 [122]. At the genus level, Enterobacter was positively correlated with neutrophils in NP [120]. Several studies also showed a positive correlation between Bacteroides and tissue eosinophils count [63,120], and Moraxella was associated with an increase in T and B lymphocytes and macrophages [110], just as negatively correlated with blood eosinophils [120]. The relative abundance of Anaerococcus was negatively correlated with IL-5 levels in tissues and IL-5-producing innate lymphoid cells (ILC2) [59], although this genus was also negatively associated with tissue proteins and positively correlated with collagen proteins (COL6A3 and COL1A2) in other studies [78]. Streptococcus positively correlated with immunoglobulin proteins (immunoglobulin kappa constant, IGKC; and immunoglobulin heavy constant gamma 1, IGHG1) [78]. At the species level, it is notable that Corynebacterium accolens was negatively correlated with eosinophilic cationic protein (ECP) [24] and Eotaxin-3 [84], while CRSwNP patients with S. epidermidis isolated showed an upregulation of trefoil family factor peptide 3 (TFF3), involved in the preservation of epithelial surface integrity, in middle nasal turbinate and NPs [69].
Table 2.
Summary of the main findings of the included studies focused on the study of the relationship between microbial dysbiosis and inflammation in CRSwNP. Sample type and methodology employed to identify or measure the microbiota and the different types of cells or factors involved in regulating the immune response.
Table 2.
Summary of the main findings of the included studies focused on the study of the relationship between microbial dysbiosis and inflammation in CRSwNP. Sample type and methodology employed to identify or measure the microbiota and the different types of cells or factors involved in regulating the immune response.
| Ref. | Sample Type | Methodology | Results/Conclusion |
|---|---|---|---|
| [73] | MMSS + blood samples | SMT + NA | More Gram-negative aerobic and facultative anaerobic bacteria in the normal subgroup than in the subgroup with increased blood eosinophils. |
| [100] | MMSS + tissue samples from the uncinated processor posterior part of the inferior nasal turbinate | SMT + histological analysis (hematoxylin and eosin staining) | Differences in the distribution of neutrophils and macrophages in nasal mucosa were significant between smokers with pathogenic bacteria and non-smokers without pathogenic bacteria. |
| [97] | MMSS + blood samples | SMT + standard hospital protocol to determine serum biomarkers | CRSwNP patients colonized with Gram-negative bacteria have a similar inflammation pattern to those colonized with only Gram-positive bacteria. Higher serum IgE levels were associated with non-Pseudomonas Gram-negative bacteria. |
| [121] (Ex vivo) | NP tissues | ELISA and nasal polyp explant tissue stimulation model | Aspergillus niger stimulation increased pro-inflammatory cytokines tumor necrosis alpha (TNF-α), granulocyte-macrophage colony-stimulating factor (GM-CSF), and interleukin- (IL-6), while having little effect on the remodeling cytokines basic fibroblast growth factor (bFGF) and transforming growth factor beta 1 (TGF-b1). Cladosporium sphaerospermum, Alternaria alternata, and Penicillium notatum stimulation reduced pro-inflammatory cytokines TNF-α and IL-6 but induced a dose-dependent increase in remodeling cytokines bFGF and TGF-b1. |
| [102] (Ex vivo) | Nasal lavage and sino-nasal mucus samples | MT + transfected human embryonic kidney (HEK293) cells | Two patients only showed toll-like receptor 4 (TLR4) activation correlated positively with TNF and with a more elevated bacterial abundance but lower bacterial diversity than non-activated samples. The microbiota of samples with TLR activity was mainly composed of Gram-negative bacteria (Gammaproteobacteria, including the genera Haemophilus or Moraxella). Samples without TLR activity showed microorganisms commonly implicated in CRSwNP (Staphylococcus, Corynebacterium, or Moraxella). |
| [103] | Sinus brushing samples | MT + qRT-PCR | Most of the CRSwNP patients cluster into a subgroup typically dominated by Corynebacterium. Most of the CRSwNP patients cluster into a subgroup associated with peroxisome proliferator-activated receptor gamma (PPAR-y) and retinoic acid-inducible gene I (RIG-I) signaling pathways and a significant increase in IL-5. |
| [104] | Tissue biopsies collected from the bulla ethmoidalis | MT + Cytometric Bead Array (CBA) and transfected human embryonic kidney (HEK293) cells | CRSwNP patients were grouped in subject clusters associated with Staphylococcus, Corynebacterium, Streptococcus, and Propionibacterium. IL-8, cluster of differentiation (CD68)-positive macrophages, eosinophils, neutrophils, plasma cells, and IL-5 were significantly elevated in CRSwNP patients. |
| [72] | Sinonasal mucosa samples + saliva or venous blood | SMT and confocal laser scanning microscopy assay + qRT-PCR and genotyping | Bacterial biofilms were more frequently found in samples from subjects with nonfunctional taste receptor 2 member 38 (TAS2R38). |
| [24] | MMSS + nasal tissue samples | MT + UniCAP systems | IgE and IL-5 were negatively correlated with Geobacter anodireducens/sulfurreducens and Pelomonas puraquae. IL-5 was negatively correlated with Corynebacterium macginleyi and eosinophil cationic protein (ECP) with Corynebacterium accolens, Corynebacterium macginleyi, and S. pneumoniae. ECP and IL-5 were positively correlated with E. coli (CRSwNP+AS patients). Specific IgE to staphylococcal enterotoxins (SE-IgE) was significantly more frequent in CRSwNP with asthma and correlated with disease severity. |
| [69] | Nasal and sinus swab samples + tissue samples | SMT + qPCR and immunochemistry | Patients with normal flora (S. epidermidis) showed a significant seven-fold upregulation of the trefoil factor 3 (TFF3) gene in middle nasal turbinate and nasal samples compared to the same tissue specimen from patients with sterile swabs. |
| [110] | Ethmoidal sinus biopsy specimens | MT + histological analysis | CRSwNP were dominated by Moraxella and Stenotrophomonas but had less Streptococcus and Veillonella than DCs. T and B lymphocytes and macrophages were significantly elevated in the CRSwNP cohort compared to DCs. |
| [58] | Swab samples and specimens pre-ESS + blood samples | SMT + limulus amoebocyte lysate (LAL) assay, immunohistochemistry, and immunofluorescence | An abundant lipopolysaccharide (LPS) was found in the peripheral blood, especially for NECRSwNP patients. LPS levels were positively correlated with glucocorticoid receptor-beta (GR-β) expression in CRSwNP. Neutrophils and macrophages were the principal inflammatory cells containing LPS. |
| [59] | MMSS + NP tissues | MT + flow cytometry and ELISA | The RA of Lachnoclostridium showed a positive correlation with IL-5-producing innate lymphoid cells (ILC2s) and IL-5 levels. In contrast, the RA of Anaerococcus showed a negative correlation with IL-5-producing ILC2 and IL-5 levels in tissues. |
| [122] | Middle nasal passage swab samples + blood serum and nasal lavage fluid | SMT + enzyme immunoassay | The level of cytokines in the nasal lavage fluid (IL-8) and blood serum (IL-1β) was correlated with the total number of microorganisms and the concentration of Enterobacteriaceae and Staphylococci. |
| [64] | MMSS and MM secretions + NP tissues | MT + immunoassay | Enterobacter in patients with the IL-5-positive NP group was higher than that of the IL-5-negative NP group. |
| [78] | NP tissues | MT + transcriptome (RNA sequencing) and proteome analysis | Corynebacterium and Anaerococcus were negatively associated with tissue structural proteins (vimentin (VIM) and histoneHIST1H4A), actin beta (ACTB), and glyceraldehyde 3 phosphate dehydrogenase (GAPDH). Anaerococcus positively correlated with collagen proteins COL6A3 and COL1A2. Streptococcus positively correlated with immunoglobulin kappa constant (IGKC) and immunoglobulin heavy constant gamma 1 (IGHG1). |
| [65] | MMSS + NP tissues | MT + immunoassays and immunohistochemical staining | The RA of Actinomycetes and Corynebacterium was significantly higher, and Staphylococci was significantly lower in the NP non-recurrent group than in the NP recurrent group. The median expression levels of IFN-γ, IL-8, IL-17A, IL-17E, and IL-18 were significantly higher in the NP recurrent group than in the NP non-recurrent group. |
| [119] | Secretions collected from the middle nasal canal, maxillary sinus, and ethmoid sinus | MT + ELISA | The abundance of Cultibacterium acnes was positively related to IL-2 level, while Staphylococcus caprae negatively correlated with IFN-γ. |
| [84] | Anterior naris and MMSS + nasal-secretion samples | MT + electrochemiluminescence technology | Corynebacteria and Staphylococci were the most abundant taxa in all patient groups. Dolosigranulum was also less prevalent, and Lawsonella was more prevalent in patients with NP than in DCs. AERD patients showed an increased RA of Staphylococcus and a decreased RA of Corynebacterium compared to other patient groups. Elevated levels of type 2 response-associated cytokines IL-5, IL-9, and Eotaxin-3 in patients with NP. Eotaxin, chemokine CCL17, and IL-6 levels were significantly elevated in CRSwNP patients compared to DCs. Staphylococcus and IL-5 showed a moderately strong correlation, while Corynebacterium accolens and Eotaxin-3 were negatively correlated. |
| [63] | MM brush samples + NP | MT + histological analysis | Sphingomonas, Akkermansia, Blautia, Devosia, Desulfovibrio, Parabacteroides, and Bacteroides were positively correlated with absolute tissue eosinophil count. The abundances of Bifidobacterium, Blautia, Desulfovibrio, Gemmiger, and Bacteroides were positively correlated with the percentage of tissue eosinophils. |
| [120] | MMSS + NP tissue samples + blood samples | MT + immunoassays and hematoxylin-and-eosin staining, immunohistochemical staining, and flow cytometry | Enterobacter was significantly higher in the IL-5-positive NP group than in the IL-5-negative NP group. IL-17 and IL-27 were negatively correlated with Enterobacter and Anaerococcus. IL-8 was negatively correlated with Enterobacter and Staphylococcus. IL-18 was positively correlated with Candidatus–Arthromitus and Arthrofilaria and negatively correlated with Haemophilus. IL-27 was positively correlated with Faecalibaculum. Arthrofilaria was positively correlated, and Moraxella and Peptostreptococcus were negatively correlated with blood neutrophil counts. Lactobacillus and Enterobacter were positively correlated with the degree of neutrophil infiltration in NP tissue. Porphyromonas was negatively correlated with tissue neutrophil infiltration. |
NP, nasal polyp; CRSwNP, chronic rhinosinusitis with nasal polyps; ECRSwNP, eosinophilic CRSwNP; NECRSwNP, non-eosinophilic CRSwNP; CRSsNP, chronic rhinosinusitis without nasal polyps; DC, disease control patient; AERD, subjects with aspirin-exacerbated respiratory disease; MM, middle meatus; MMSS, MM swab samples; SMT, microbial identification using standard microbiological techniques; MT, microbial identification using molecular techniques; ELISA, Enzyme-Linked Immunosorbent Assay; PCR, polymerase chain reaction; qPCR, quantitative polymerase chain reaction; qRT-PCR, quantitative reverse-transcriptase PCR; RA, relative abundance; NA, not applicable.
3.2.3. Effect of the Modulation of the Microbiota on the CRSwNP Treatment
According to the PICO criteria, Table 3 summarizes the evidence found in nine studies in the present systematic review of the impact of different treatments on the nasal microbiota in CRSwNP patients. Again, further information for each of the studies included can be found in Table 1 or (Supplementary Data S1). The studies mainly evaluated the effect of mixed medical treatments including antibiotics, such as clarithromycin, doxycycline or amoxicillin–clavulanate; nasal saline irrigation; or oral and systemic corticosteroids, such as mometasone furoate or prednisone [70,83,95,96,105], as well as different alternative to the antibiotics: a natural compound (Manuka honey) [107], a probiotic (Lactococcus lactis W136) [113], and a bacteriophage mixture (Otofag) [122]. Three studies involved placebo control groups [105,107,122], two studies included disease control patients [83,95], and only one did not include placebo control [113]. In the rest of the studies, a group of patients who had not taken the primary evaluation treatment was used for comparison. The duration of the treatments ranged from seven days to six months.
Table 3.
Summary of the main findings from the included studies focused on the evaluation of microbiota modulation in the CRSwNP treatment.
Regarding the main results obtained, a significant decrease in alpha diversity and specific bacteria was observed in CRSwNP patients who had taken antibiotics [83,89]. Adding clarithromycin to mometasone furoate spray was also associated with significantly eradicating biofilm formation [70]. The total number of bacteria significantly decreased after the administration of intranasal gel with bacteriophages [122]. Topical administration of alive L. lactis W126 reduced the abundance of multiple species of Staphylococcus, Peptostreptococcae, and Enterobacialles. It increased the abundance of Dolosigranulum pigrum [113], while Manuka honey reduced the standard semiquantitative bacterial culture rate (mainly about S. aureus) in half of the CRSwNP patients [107]. The rest of the studies reported no significant changes in the nasal microbiota [95,96,105]. Some clinical benefits in the experimental groups were reported in three studies [96,113,122].
4. Discussion
In recent years, the human microbiota has been identified as a contributing factor in the development and maintenance of diverse pathologies and in the modulation of the immune system. This systematic review comprises original studies focused on the characterization of the host microbiota composition and the study of its influence on inflammatory processes in CRSwNP patients. The results of the evaluation of promising strategies aimed to promote changes in microbiota composition to restore a healthier profile were also included. After reviewing the literature published between January 2014 and February 2024, 70 articles that focused mainly on nasal microbiota were finally included. Although compositional or functional alterations in the gut microbiota play a role in upper-airway diseases such as CRSwNP [29,123], only one study focused on the gut microbiota from fecal samples [61]. The fact that nasal microbiota directly interacts with the nasal epithelial barrier, potentially modulating the local immune response and influencing polyp development [77], as well as constituting a potential therapeutic target [92], can explain the almost absence of studies that comprised gut-microbiota results.
All the variables that could potentially impact the final appreciation of the results included in this review were initially considered: study type, sample size, population, country, patient characteristics (age, sex, and comorbidities), type of sample, and methodology used. It is worth noting that most of the studies were identified as cross-sectional, providing data at a single point in time, unlike the longitudinal studies in which the relative impact of host and environmental factors on human microbiota cannot be further clarified. Evidence of the limitations of this kind of study aimed to identify significant microbiota–disease (CRSwNP) links for helpful diagnostic purposes has previously been described, notably when high inter-subject variability is reported [114,124]. Numerous studies showed high inter-patient variability within the CRSwNP cohort and other cohorts evaluated [55,75,77,88,92,94,102,105,114]. The relatively small sample size of most studies (initial sample size less than 100 subjects) may have led to substantial variability between samples [125,126].
In this context, differences in microbiota composition and inflammatory profile can also be explained by geographical factors, including diet; climate; lifestyle habits, such as smoking; antibiotics; corticosteroid-prescribing patterns; or other environmental exposures [55,75,84,104]. By way of example, previous studies have reported a lower isolation rate of S. aureus in patients from China than in Caucasian patients, as well as a different pattern of association for IL-5, nasal polyps, and eosinophilia between European and Chinese patients [4,73]. As mentioned above, the highest number of the studies included were from Asia and Europe. However, in agreement with the results obtained with the only multicenter international cohort study included [55], the composition of the nasal core microbiota appears to be preserved across the countries evaluated. In-depth, the nasal microbiota of CRSwNP patients was primarily composed of the bacterial phyla Firmicutes, followed by Proteobacteria, Actinobacteria, and Bacteroidetes, corresponding to the most predominant microbial communities that colonize the upper respiratory tract [127].
Regarding remarkable patient characteristics, on the one hand, the number of male subjects enrolled was slightly higher than that of females, obtaining an average gender ratio (females/males) of 0.85 for the general population and 0.75 for CRSwNP patients. Only one study reported a gender-specific difference in CRSwNP patients, obtaining a significantly higher abundance of Corynebacterium in men than in females [95]. On the other hand, the age range was relatively large (from 13 to 88 years), although the age means reported were mainly comprised between 40 and 50 years. Changes in the microbial community composition during aging, probably due to the result of immunosenescence [128], can be observed [127,129]. Although the more frequent occurrence of NPs in older patients was confirmed, Leszczyńska et al. [115] found no statistically significant differences between the occurrence of a specific type of bacteria and the presence of NPs in both patients over 65 years of age and younger patients (from 18 to 40 years).
CRSwNP patients showed a high incidence of asthma, among other comorbidities, such as hypersensitivity to drugs or allergy, being, in some cases, significantly higher than other groups evaluated (CRSsNP patients or control subjects) [114]. Despite being crucial factors for the composition of the microbial core [130,131,132], smoking, history of recurrent exacerbations, endoscopic sinus surgery, or even disease severity could not be analyzed because a significant number of studies evaluated did not detail these data. In contrast, the majority of the studies reported antibiotic- and/or corticosteroid-prescribing patterns. The general criterium in the studies was no antibiotic use within one month before sample collection, as one month appears to be enough time to return the microbiota to a steady level [86,133].
Concerning methodology aspects, first, different types of samples from distinct nasal sites were taken at different moments, before, during, or after surgery, with the middle meatus swab samples and tissue biopsies standing out. As previously mentioned, the microbiota analysis may be more influenced by the sampling technique than the anatomical sampling site [90,93,94]. Swabs taken from the middle meatus are the traditional method of sampling because of their ease of collection, and they likely accurately reflect the sinus microbiological profile, as the middle meatus is the drainage area for the anterior ethmoid sinus, the maxillary sinus, and the frontal sinus, as well as the nasal polyps that usually originate from the uncinate process, ethmoid bulla, or middle turbinate [73,74,118]. In the case of the maxillary sinuses, of note, it is involved in heating and humidifying the air, in the development of odontogenic sinusitis, and in different types of regenerative techniques to treat bone atrophies [134]. In contrast, other studies justified the use of tissue specimens because they incorporate bacterial biofilms that grow on the surface and penetrate the mucosal epithelium [94], whereas sampling from the middle meatus may provide inadequate information [132,135]. The risk of possible sample contamination when using swabs in the sampling method has been described [73].
The authors used culture-dependent techniques, focused on traditional direct growth and identification, and culture-independent techniques, focused on sequencing and molecular analyses. Because most of the human microbiota cannot be cultured, it is necessary to use molecular techniques, which can provide more detailed information on microbiota abundance and diversity [40,74,106]. However, these methods for microbiological characterization have limitations, such as the inability to differentiate between viable and non-viable or commensal and inhaled microorganisms, extensive training, and higher costs [83]. In this context, the differences in the bioinformatics analysis could explain the discrepancies observed between the studies based on the sequencing technology (mainly bacterial 16S ribosomal RNA (rRNA) and fungal internal transcribed spacer (ITS) gene sequencing) [114]. Most studies in the present review analyzed sequencing data by clustering sequences into OTUs at over a 97% sequence similarity threshold. Although OTU clustering is standardly accepted for quantifying microbiological diversity [29,136], it can give misleading results, as it is study-specific and, therefore, not comparable between different datasets [114,137]. It was observed that amplicon sequence variants (ASVs), sequence entities that can be comparable across datasets and provide better resolution and accuracy than the OTU method [137], were employed by more recent studies [55,63,75,84,87,114].
4.1. Microbiota Composition in CRSwNP
Although discrepancies were also found, likely due to the limitations described above, the dysbiosis hypothesis as a potential critical explanatory factor of the CRSwNP pathogenesis may be supported by the results of different studies included [55,61,86]. The most predominant microbiota alterations observed in CRSwNP patients compared to controls highlight a trend of lower alpha diversity or level of bacterial diversity within individual samples described with the observed richness (number of bacterial taxa mainly obtained using Chao1 index) and evenness or the relative abundance of those taxa (Shannon or Simpson indexes) [138]. Decreased alpha diversity of the nasal and gut microbiota has been previously associated with the development of inflammatory airway diseases, including asthma or chronic obstructive pulmonary disease (COPD) [139,140,141,142,143,144,145]. Host and environmental factors, such as antibiotics, can directly affect the composition of human microbiota, enhancing the prevalence of this kind of disease [105,140,145,146,147,148]. Nevertheless, the lower diversity mentioned in the present review cannot be explained by the use of antibiotics, as most studies reported that no CRSwNP patients received antibiotics for at least the last month before sampling [24,60,61,75,86,87,88,89].
Enrichment of specific bacteria from the phyla Proteobacteria in CRSwNP patients compared with controls—precisely, bacteria from the genera Haemophilus, Moraxella, and Pseudomonas—was also reported across multiple studies [24,38,40,88,89,91]. Considered opportunistic pathogens [139,149], these bacteria have been related to lower-respiratory disease control with increased exacerbation risk [139,140,150]. On the one hand, Haemophilus and Moraxella, belonging to the class Gammaproteobacteria, can induce epithelial damage and expression of host inflammatory pathways [150,151]. A greater abundance of Moraxella was found in the CRSwNP subgroup characterized by eosinophil-dominant inflammatory cell infiltration in NPs [60,61,63]. On the other hand, a pathogenic role of Pseudomonas and other aerobic and facultative Gram-negative roads has been suggested, as they are infrequently identified from middle meatus from healthy subjects [152]. In this context, it has been described that lipopolysaccharide, the main chemical component of the outer layer of the Gram-negative bacteria cell wall, can induce persistent mucosal inflammation and cause tissue remodeling [153].
In contrast, a decrease in the abundance of Corynebacterium and Dolosigranulum was also observed [55,64,65,84,86,88,90]. Both respiratory commensal bacteria include specific species that may play a protective role in the nasal airways, modulating the innate immune response and providing better resistance to bacterial and viral pathogens [24,55,139,154]. An improvement in the levels of respiratory cytokines and immune cell populations critical for host defense against microbial infection associated with specific strains of these bacteria has been shown [154]. Commensal bacteria can also exclude pathogens both passively, by competing for space and nutrients, and actively, by secreting antimicrobial compounds [58].
The results obtained for bacteria from the phyla Firmicutes were controversial [24,40,55,60,89,90]. It is worth noting that, unlike other Staphylococcus species, S. aureus colony formation in the nasal mucosa tissue can be essential in the sustained inflammatory response of CRS [39,155]. Although multiple authors have suggested that alterations of bacterial community may play a more significant role in the development of CRSsNP than CRSwNP [57,85,102,109,156,157], S. aureus is more prevalent in the latter clinical phenotype [39]. The staphylococcal superantigen hypothesis postulates that S. aureus secretes relevant enterotoxins, which induce the local inflammatory response, promoting an increase in cytokines and other inflammatory mediators’ synthesis and eosinophil infiltration in epithelial tissue and inducing an increase in IgE levels [39,63,115,155]. The disruption of intercellular adhesion factors and damage to the epithelial ciliary transport system promoting mucosal barrier defects could also be associated with the colonization of intranasal S. aureus. Barrier dysfunction can contribute to bacterial invasion and biofilm formation, resulting in an intensification of local inflammation and polyp development [39,155].
The limited number of results obtained concerning nasal fungal and viral communities suggests that these microbial taxa are unlikely to play a direct pathogenic etiological role in CRSwNP. Further research focused on differentiating whether the identified nasal mycobiota might be a local functional community or simply reflect inhaled environmental fungal material, which has been previously indicated [77]. In the case of respiratory viruses, viral respiratory infection may play a minor role in symptom exacerbation in CRSwNP than CRSsNP [81]. Despite that, viral and fungal dysbiosis may exacerbate the inflammatory process and, thus, contribute to CRSwNP symptomatology through an indirect/secondary role, influencing the bacterial microbiota, deteriorating the epithelial barrier, or persisting in the mucosal inflammation [75,77,158].
Regarding the controversy found in the influence of the simultaneous presence of relevant comorbidities on the nasal microbiota, it is notable that multiple studies obtained differences in the nasal microbiota of CRSwNP patients with and without asthma [24,38,97], the most common comorbidity reported. An intimate association between the gut and respiratory microbial communities, host immune development, and the pathogenesis and manifestation of asthma has been previously suggested [159]. Likewise, it is remarkable that there is a higher abundance of Moraxella in the CRSwNP subtype, in which tissue eosinophils predominate among inflammatory cells (ECRSwNP) [60,61,63]. A greater risk of NP recurrence, as well as a worse prognosis post-surgery, have been found in patients with tissue eosinophilia [65,158,160]. Evidence suggests that eosinophils contribute to histological tissue remodeling and, thus, NP development by releasing mediators, pro-inflammatory cytokines, and toxic proteins such as ECP [161]. Finally, although different demographics or biological parameters were not found to be statistically significant in causing the recurrence of polyposis in a recent study [162], differences in the abundance of specific bacterial genera between recurrent and non-recurrent groups were reported [64,92].
4.2. Relationship between Microbial Dysbiosis and Inflammation in CRSwNP
The present systematic review also revised possible connections between nasal dysbiosis and inflammation markers. Gram-negative bacteria have been one of the most extensively analyzed mediators for inflammatory reactions. In detail, members of this group of bacteria were positively associated with the activity of transmembrane receptors, such as TLRs, with a prominent role in recognizing pathogens’ components, thus stimulating inflammatory factors’ production and immune cell activity [102]. By way of example, the same author found, in two different studies, a clear correlation between Enterobacter and patients with NPs positive for IL-5, a major cellular inflammatory factor in eosinophil-mediated Th2-type inflammation [64,120]. It has been suggested that this commonly conditional pathogen in the human gut can trigger the release of IL-5 when colonizing the nasal cavity, leading to a cascade activation and eosinophil recruitment, further aggravating the Th2 inflammatory response [120].
Likewise, different Gram-positive bacterial genera, such as Staphylococcus, Lachnoclostridium, or Streptococcus, were positively associated with eosinophilic inflammation, elevated levels of type 2 response-associated cytokines and immunoglobulin proteins [59,78,84,104]. A negative association with tissue structural proteins was also reported, which could be linked to a loss of mucosal epithelial disruption, a predisposition toward eosinophil infiltration, and increased permeability to diverse microorganisms into submucosa [104]. Thus, an epithelial barrier with compromised integrity can expose more TLRs to pathogens, promoting the initiation of the inflammation response [110]. Tissue-related effects of specific common airborne fungal species, mainly inducing and remodeling pro-inflammatory cytokines, have been shown in ex vivo NP tissue [121].
On the other hand, specific bacterial species with a potential protective function were negatively correlated with cytokines and other mediators of the host defense response, as in the case of C. accolens with eotaxin-3 [84] and ECP [24]. The antimicrobial potential of C. accolens against S. aureus and methicillin-resistant S. aureus (MRSA) clinical isolates or S. pneumoniae has also been shown [163,164]. Similarly, a higher expression of peptides involved in preserving epithelial surface integrity was associated with S. epidermidis [69]. This commensal bacterium, found in great abundance in human skin and mucosa, has a well-documented role in the control and inhibition of respiratory tract pathogens through the secretion of antimicrobial compounds or the stimulation of the host immune response [165].
As previously suggested, the lower bacterial diversity commonly found in CRSwNP could also contribute to the host’s innate and adaptive immune response [102]. The presence of bacterial biofilm, with a detection rate reaching over 44% of the cases, can also be implicated as an essential feature of sinonasal infections in CRSwNP, acting as a reservoir of pathogenic bacteria and conferring high resistance to host antimicrobial defense strategies [29,72].
Remarkably, the geographic and ethnic variations in the CRSwNP pathophysiology, with a predominance of eosinophilic inflammation involving mainly Th2 cytokines in European and American patients and a predominance of non-eosinophilic and mixed Th1, Th2, and Th17 cytokines patients from East Asia, could explain the differences in the immune response and cytokine profiles associated with specific bacterial groups [119,120]. Apart from this, it seems clear that the role of the nasal microbiota in the CRSwNP pathophysiology causes an onset of cell-mediated immune responses, changes in the cytokine cascade, and defects in the epithelial barrier. However, other non-microbial and host factors, such as innate immune deficiencies, anatomic abnormalities, genetic predisposition, or the co-occurrence of comorbidities, must be considered as modulators influencing disease establishment and severity, as previously noted [139].
4.3. Effect of the Modulation of the Microbiota on the CRSwNP Treatment
Taking into account the evidence of a relationship between alterations in the microbiota and CRSwNP, different studies have assessed the effect of different treatments and adjuvants commonly employed in CRSwNP therapy, such as antibiotics, corticosteroids, or nasal saline irrigation, as well as other novel alternative strategies, including microbiome-based therapeutics, on the modulation of the dysbiotic nasal microbiota. As previously mentioned [122], the efficacy of these treatments is not primarily dependent on pathogen removal. Instead, their focus is on restoring a healthy microbial balance or eubiosis.
Due to their anti-inflammatory properties, corticosteroids and antibiotics have been recommended as a first-line CRS therapy. In addition to antimicrobial properties, the current literature implies that long-term macrolide and doxycycline treatment can inhibit neutrophilic and eosinophilic inflammation or even reduce polyp size [165]. Considering the results collected in the present review, no significant changes in microbial communities in CRSwNP patients were found before and after nasal saline irrigation or corticosteroid therapies [70,83,95,105]. Different potential benefits in the sinonasal mucosa of both treatment options have been previously proposed, such as the alteration and elimination of antigens, biofilms, and inflammatory mediators, as well as the contribution to a diverse and balanced sinonasal microbiota [166,167].
The combined treatment of clarithromycin with mometasone furoate nasal spray did not cause significant changes in the nasal microbiota in the study carried out by Varvyanskaya and collaborators [96]. In contrast, a significant eradication in biofilm formation was observed in another study, even with a shorter treatment but different initial daily dose [70]. A decrease in the alpha diversity in patients who had taken antibiotics during the three months before sampling compared to those without antibiotic treatment was also reported [89], denoting the importance of considering antibiotic use when evaluating the association between microbiota and a specific disease state. Based on these results and the trend of a lower alpha diversity observed in CRSwNP patients compared to controls, the antibiotics can negatively affect the microbiota and, consequently, the host physiology, increasing the risk of airway inflammation [159].
Even though, the proportion of clarithromycin-resistant strains remained constant throughout the antibiotic therapy in a study previously cited [96], long-term antibiotic treatment, as well as the repeated use of antibiotics in recalcitrant, difficult-to-treat patients, can increase the risk of inducing significant bacterial resistance to this kind of drug. Thus, given the general trend to dispense with antibiotics in situations where there is an apparent lack of infection according to clinical practice guideline recommendations [9,83], the search for novel antimicrobial alternatives to conventional treatments is an increased area of interest. Changes, but non-significant, in the abundance of multiple bacterial species, total number, and culture rate associated with administering this kind of treatment were found in fewer studies [107,113,122], reflecting the need for more research. Regarding probiotics with a therapeutic potential because of their well-known role in decreasing the density of specific microbial pathogens and modulating the immune response [29], it is necessary to note that their use through intranasal irrigation can also become problematic in specific contexts. For example, probiotic strains can represent pathogen agents after surgery, since the anatomical barriers have been removed, or in patients with significant defects in the epithelial barrier with inappropriate immune response [113].
Finally, the fact that treated groups reported improved sinonasal symptoms despite no significant changes in the nasal microbiota supports the hypothesis that these treatments also show non-microbiological mechanisms. Enhancements in the different natural defense mechanisms of the host respiratory tract, including mucociliary clearance, and the reduction in specific inflammatory mediators associated with these treatments likely contribute to their beneficial effects [95].
5. Conclusions
The literature related to human microbiota and CRSwNP from the last ten years was evaluated in the present systematic review. Our primary focus was on the microbiota composition found in CRSwNP patients and the significance of microbiota dysbiosis or alterations in the composition and function of the inflammatory processes in CRSwNP. Studies investigating current and promising therapeutic approaches to manipulate the microbiota in CRSwNP were also included.
As discussed above, the main limitation of this review was related to the absence of uniformity in both the populations studied and the methodologies employed. Nevertheless, the results of the included studies suggest that nasal microbiota dysbiosis can be accepted as a critical factor influencing the onset or severity of CRSwNP. Thus, as has been previously reported for other chronic inflammatory diseases, CRSwNP appears to be a complex interplay, involving innate immune deficiencies, anatomic abnormalities, and genetic predisposition, influenced by the alterations in microbiota composition and diversity.
To sum up, this review provides a valuable understanding of the relationship between nasal microbiota and CRSwNP pathophysiology. Although biological therapies targeting inflammatory mediators, such as the monoclonal antibodies dupilumab, omalizumab, or mepolizumab, have currently been found to be effective in CRSwNP patients, approaches aimed at modulating the host microbiota could become an essential part of combined CRSwNP treatment. Indeed, it is important to remark that further studies into humans are clearly needed to understand the contribution of both nasal and gut microbiota in respiratory diseases as the design of potential therapeutic options based on microbiota modulation.
6. Future Directions
A high abundance of several pathogen-related taxa and low microbial diversity, associated with changes in the host’s innate and adaptive immune response and defects in the epithelial barrier, seem characteristic of CRSwNP patients. However, the specific bacterial taxa changes and the associated immune response and cytokine profiles were not always consistent across studies. These observations allow for speculation on the future directions for microbiological diagnosis and treatment of CRSwNP. It seems conceivable that future research focused on the geographic and ethnic variations in host microbiota could provide insights into the influence of environmental and intrinsic factors on CRSwNP, thereby identifying commonly relevant microbial targets and region-specific considerations. In this context, further longitudinal studies that provide an overview of microbiota changes over time would help to clarify whether dysbiosis is a cause or effect of the disease and identify key microbial taxa preceding CRSwNP onset. Future studies should also investigate the roles of nasal viruses and fungi and gut microbiota, providing a more comprehensive view of the CRSwNP aetiology. Advanced omics technologies, such as metagenomics, transcriptomics, or metabolomics, could elucidate how gut microbiota influences nasal health and the mechanistic underlying microbiota, immune response, and barrier integrity.
Finally, the identification of specific microbiota profiles as potential diagnostic biomarkers could lead to non-invasive methods for the early detection and monitoring of CRSwNP. Well-designed clinical trials with extensive CRSwNP patient recruitment could enable researchers to develop appropriate and personalized microbiota-modulating strategies adapted to specific microbiota profiles, enhancing treatment efficacy and minimizing adverse effects.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/ijms25158223/s1.
Author Contributions
M.G.-G., A.G.-S., M.E., I.D. and C.S. designed and performed the systematic review, analyzed and validated the data, and co-wrote the original draft; M.G.-G., E.M.-J. and N.M. performed bioinformatics analyses; A.G.-S., M.G.-M., J.P.-P., M.E., M.I.-G., I.D. and C.S. supervised the review, revising it critically, and gave the final approval of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the projects PI23/00446 and PI20/00268, funded by Carlos III Health Institute (ISCIII) and co-funded by the European Union; RD21/0002/0054 and PMP22/00124, funded by ISCIII and the European Union’s NextGeneration EU, Mecanismo para la Recuperación y la Resiliencia (MRR); IMP/00009, funded by ISCIII and European Regional Development Fund “A way to make Europe”; and by the Grant PID2021-125117OB-I00 funded by MCIN/AEI/10.13039/501100011033 and by ERDF “A way of making Europe”. MG-G is a recipient of a Sara Borrell postdoctoral fellowship from the ISCIII (CD23/00185), co-funded by the European Social Fund. EM-J is a recipient of a predoctoral grant PFIS, funded by ISCIII through the project “FI-21/00048” and co-funded by the European Union. NM is a recipient of a contract financed by “Programa Investigo” funded by the European Union’s NextGenerationEU, Recovery and Resilience Facility (RRF) (2022 C23.I01.P03.S0020–0000205).
Conflicts of Interest
A.G.-S. has received payment for lectures from Leti. M.E. has received payment for lectures from SANOFI in the last three years. M.G.-M. has received payment for lectures from Astra-Zeneca, GSK, and Sanofi. I.D. has received payment for lectures, including service on speaker’s bureaus from Allergy Therapeutics, Astra-Zeneca, Chiesi, Diater, GSK, Leti, Novartis, and Sanofi; for a consultancy from Allergy Therapeutics, ALK-Abello, Astra-Zeneca, GSK, Merck, MSD, Novartis, and Sanofi; and grants for Thermofisher Diagnostics. The rest of the authors declare no conflict of interest. The funders had no role in the study’s design, in the collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
| AERD | aspirin-exacerbated respiratory disease |
| ASV | amplicon sequence variant |
| bFGF | casic fibroblast growth factor |
| CMV | cytomegalovirus |
| CoNS | coagulase-negative staphylococci |
| COPD | chronic obstructive pulmonary disease |
| CRD | chronic respiratory disease |
| CRS | chronic rhinosinusitis |
| CRSsNP | chronic respiratory disease without nasal polyps |
| CRSwNP | chronic respiratory disease with nasal polyps |
| CT | computed tomography |
| EBV | Epstein–Barr virus |
| ECP | eosinophilic cationic protein |
| ECRSwNP | eosinophilic chronic respiratory disease with nasal polyps |
| ELISA | enzyme-linked immunosorbent assay |
| EPOS | European Position Paper on chronic rhinosinusitis |
| ESS | endoscopic sinus surgery |
| FESS | functional endoscopic sinus surgery |
| GM-CSF | granulocyte-macrophage colony-stimulating factor |
| GR | glucocorticoid receptor |
| GRADE | Grading of Recommendations, Assessment, Development, and Evaluations |
| HHV-6 | human herpesvirus 6 |
| HSV-1 | herpes simplex virus type 1 |
| IgE | immunoglobulin E |
| IGHG1 | immunoglobulin heavy constant gamma 1 |
| IGKC | ommunoglobulin kappa constant |
| IL | interleukin |
| ILC | innate lymphoid cells |
| ITS | internal transcribed spacer |
| LPS | lipopolysaccharide |
| MRSA | methicillin-resistant Staphylococcus aureus |
| NECRSwNP | non-eosinophilic chronic respiratory disease with nasal polyps |
| NOS | Newcastle–Ottawa Scale |
| NP | nasal polyp |
| NSAID-ERD | nonsteroidal anti-inflammatory drug-exacerbated respiratory disease |
| OTU | operational taxonomic unit |
| PCR | polymerase chain reaction |
| PICO | Population, Intervention, Control, and Outcome |
| PPAR | peroxisome proliferator-activated receptor |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| QOL | quality of life |
| RIG-I | retinoic acid-inducible gene I |
| RoB | risk of bias |
| RoB 2 | version 2 of the Cochrane risk-of-bias tool |
| rRNA | ribosomal ribonucleic acid |
| TAS2R38 | taste receptor 2 member 38 |
| TFF3 | trefoil family factor peptide 3 |
| Th2 | T-helper type 2 |
| TLR | Toll-like receptors |
| TNF | tumor necrosis factor |
References
- GBD 2019 Chronic Respiratory Diseases Collaborators. Global Burden of Chronic Respiratory Diseases and Risk Factors, 1990–2019: An Update from the Global Burden of Disease Study 2019. EClinicalMedicine 2023, 59, 101936. [Google Scholar] [CrossRef]
- Bachert, C.; Marple, B.; Schlosser, R.J.; Hopkins, C.; Schleimer, R.P.; Lambrecht, B.N.; Bröker, B.M.; Laidlaw, T.; Song, W.-J. Adult Chronic Rhinosinusitis. Nat. Rev. Dis. Prim. 2020, 6, 86. [Google Scholar] [CrossRef] [PubMed]
- de Loos, D.D.; Lourijsen, E.S.; Wildeman, M.A.M.; Freling, N.J.M.; Wolvers, M.D.J.; Reitsma, S.; Fokkens, W.J. Prevalence of Chronic Rhinosinusitis in the General Population Based on Sinus Radiology and Symptomatology. J. Allergy Clin. Immunol. 2019, 143, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Zhang, N.; Holtappels, G.; De Lobel, L.; van Cauwenberge, P.; Liu, S.; Lin, P.; Bousquet, J.; Van Steen, K. Presence of IL-5 Protein and IgE Antibodies to Staphylococcal Enterotoxins in Nasal Polyps Is Associated with Comorbid Asthma. J. Allergy Clin. Immunol. 2010, 126, 962–968.e6. [Google Scholar] [CrossRef] [PubMed]
- Farina, D.; Ravanelli, M.; Borghesi, A.; Maroldi, R. Flying through Congested Airspaces: Imaging of Chronic Rhinosinusitis. Insights Imaging 2010, 1, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Ting, F.; Hopkins, C. Outcome Measures in Chronic Rhinosinusitis. Curr. Otorhinolaryngol. Rep. 2018, 6, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Abdulrashid, N.A.; Ali, O.I.; Elsharkawy, M.A. Effect of Photobiomodulation Therapy on Headache, and Fatigue in Patients with Chronic Rhinosinusitis: A Randomized Controlled Study. Lasers Med. Sci. 2024, 39, 62. [Google Scholar] [CrossRef] [PubMed]
- Wahid, N.W.; Smith, R.; Clark, A.; Salam, M.; Philpott, C.M. The Socioeconomic Cost of Chronic Rhinosinusitis Study. Rhinology 2020, 58, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef]
- Grayson, J.W.; Cavada, M.; Harvey, R.J. Clinically Relevant Phenotypes in Chronic Rhinosinusitis. J. Otolaryngol. Head Neck Surg. 2019, 48, 23. [Google Scholar] [CrossRef]
- Cho, S.H.; Kim, D.W.; Gevaert, P. Chronic Rhinosinusitis without Nasal Polyps. J. Allergy Clin. Immunol. Pract. 2016, 4, 575. [Google Scholar] [CrossRef] [PubMed]
- Snidvongs, K.; Sangubol, M.; Poachanukoon, O. Pediatric Versus Adult Chronic Rhinosinusitis. Curr. Allergy Asthma Rep. 2020, 20, 29. [Google Scholar] [CrossRef]
- Bartosik, T.J.; Liu, D.T.; Campion, N.J.; Villazala-Merino, S.; Janik, S.; Dahm, V.; Mueller, C.A.; Vyskocil, E.; Stanek, V.; Quint, T.; et al. Differences in Men and Women Suffering from CRSwNP and AERD in Quality of Life. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Ahern, S.; Cervin, A. Inflammation and Endotyping in Chronic Rhinosinusitis—A Paradigm Shift. Medicina 2019, 55, 95. [Google Scholar] [CrossRef]
- Cui, Y.; Wang, K.; Shi, J.; Sun, Y. Endotyping Difficult-to-Treat Chronic Rhinosinusitis with Nasal Polyps by Structured Histopathology. Int. Arch. Allergy Immunol. 2023, 184, 1036–1046. [Google Scholar] [CrossRef]
- Vizuete, J.A.C.; Sastre, J.; Bernal, A.D.C.; Picado, C.; Moragón, E.M.; García, J.M.I.; Serrano, C.C.; Gutiérrez, F.J.Á.; Miret, J.M. Asthma, Rhinitis, and Nasal Polyp Multimorbidities. Arch. Bronconeumol. 2019, 55, 146–155. [Google Scholar] [CrossRef]
- Khan, A.; Vandeplas, G.; Huynh, T.M.T.; Joish, V.N.; Mannent, L.; Tomassen, P.; Van Zele, T.; Cardell, L.O.; Arebro, J.; Olze, H.; et al. The Global Allergy and Asthma European Network (GALEN) Rhinosinusitis Cohort: A Large European Cross-Sectional Study of Chronic Rhinosinusitis Patients with and without Nasal Polyps. Rhinology 2019, 57, 32–42. [Google Scholar] [CrossRef]
- Chen, S.; Zhou, A.; Emmanuel, B.; Garcia, D.; Rosta, E. Systematic Literature Review of Humanistic and Economic Burdens of Chronic Rhinosinusitis with Nasal Polyposis. Curr. Med. Res. Opin. 2020, 36, 1913–1926. [Google Scholar] [CrossRef]
- Stevens, W.W.; Schleimer, R.P.; Kern, R.C. Chronic Rhinosinusitis with Nasal Polyps. J. Allergy Clin. Immunol. Pract. 2016, 4, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Alobid, I.; Antón, E.; Armengot, M.; Chao, J.; Colás, C.; del Cuvillo, A.; Dávila, I.; Dordal, M.T.; Escobar, C.; Fernández-Parra, B.; et al. SEAIC-SEORL. Consensus Document on Nasal Polyposis. POLINA Project. J. Investig. Allergol. Clin. Immunol. 2011, 21 (Suppl. 1), 1–58. [Google Scholar]
- Chen, S.; Zhou, A.; Emmanuel, B.; Thomas, K.; Guiang, H. Systematic Literature Review of the Epidemiology and Clinical Burden of Chronic Rhinosinusitis with Nasal Polyposis. Curr. Med. Res. Opin. 2020, 36, 1897–1911. [Google Scholar] [CrossRef] [PubMed]
- Al-Ahmad, M.; Alsaleh, S.; Al-Reefy, H.; Al Abduwani, J.; Nasr, I.; Al Abri, R.; Alamadi, A.M.H.; Fraihat, A.A.; Alterki, A.; Abuzakouk, M.; et al. Expert Opinion on Biological Treatment of Chronic Rhinosinusitis with Nasal Polyps in the Gulf Region. J. Asthma Allergy 2022, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sudiro, M.; Kuntara, A.; Waldi, D. Correlation of Lund-Mackay Score on Computed Tomography Scan and Nasoendoscopic Score in Chronic Rhinosinusitis. Acta Inform. Medica AIM J. Soc. Med. Inform. Bosnia Herzeg. Cas. Drus. Za Med. Inform. BiH 2023, 31, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Chalermwatanachai, T.; Vilchez-Vargas, R.; Holtappels, G.; Lacoere, T.; Jáuregui, R.; Kerckhof, F.M.; Pieper, D.H.; Van De Wiele, T.; Vaneechoutte, M.; Van Zele, T.; et al. Chronic Rhinosinusitis with Nasal Polyps Is Characterized by Dysbacteriosis of the Nasal Microbiota. Sci. Rep. 2018, 8, 7926. [Google Scholar] [CrossRef] [PubMed]
- Lal, D.; Brar, T.; Ramkumar, S.P.; Li, J.; Kato, A.; Zhang, L. Genetics and Epigenetics of Chronic Rhinosinusitis. J. Allergy Clin. Immunol. 2023, 151, 848–868. [Google Scholar] [CrossRef] [PubMed]
- Heredero-Jung, D.H.; Elena-Pérez, S.; García-Sánchez, A.; Estravís, M.; Isidoro-García, M.; Sanz, C.; Dávila, I. Interleukin 5 Receptor Subunit Alpha Expression as a Potential Biomarker in Patients with Nasal Polyposis. Biomedicines 2023, 11, 1966. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.J.; Garcia-Sanchez, A.; Estravis, M.; Gil-Melcón, M.; Isidoro-Garcia, M.; Sanz, C.; Davila, I. Genetics and Epigenetics of Nasal Polyposis: A Systematic Review. J. Investig. Allergol. Clin. Immunol. 2021, 31, 196–211. [Google Scholar] [CrossRef]
- Pérez-Pazos, J.; García-Sánchez, A.; Estravís, M.; Moreno-Jimenez, E.; Morgado, N.; Gómez-García, M.; Ramos-González, J.; Gil-Melcón, M.; Martín-García, C.; Muñoz-Bellido, F.; et al. Beyond T2-Asthma Biomarkers: Risk Stratification for NSAID-Exacerbated Respiratory Disease. ERJ Open Res. 2024, 10, 00909–02023. [Google Scholar] [CrossRef]
- Huntley, K.S.; Raber, J.; Fine, L.; Bernstein, J.A. Influence of the Microbiome on Chronic Rhinosinusitis With and Without Polyps: An Evolving Discussion. Front. Allergy 2021, 2, 737086. [Google Scholar] [CrossRef]
- Hou, K.; Wu, Z.X.; Chen, X.Y.; Wang, J.Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in Health and Diseases. Signal Transduct. Target. Ther. 2022, 7, 135. [Google Scholar] [CrossRef]
- Khaledi, M.; Poureslamfar, B.; Alsaab, H.O.; Tafaghodi, S.; Hjazi, A.; Singh, R.; Alawadi, A.H.; Alsaalamy, A.; Qasim, Q.A.; Sameni, F. The Role of Gut Microbiota in Human Metabolism and Inflammatory Diseases: A Focus on Elderly Individuals. Ann. Microbiol. 2024, 74, 1. [Google Scholar] [CrossRef]
- Riccio, P.; Rossano, R. The Human Gut Microbiota Is Neither an Organ nor a Commensal. FEBS Lett. 2020, 594, 3262–3271. [Google Scholar] [CrossRef] [PubMed]
- Hillman, E.T.; Lu, H.; Yao, T.; Nakatsu, C.H. Microbial Ecology along the Gastrointestinal Tract. Microbes Environ. 2017, 32, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Malard, F.; Dore, J.; Gaugler, B.; Mohty, M. Introduction to Host Microbiome Symbiosis in Health and Disease. Mucosal Immunol. 2021, 14, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.; Liwinski, T.; Elinav, E. Interaction between Microbiota and Immunity in Health and Disease. Cell Res. 2020, 30, 492–506. [Google Scholar] [CrossRef] [PubMed]
- Gelardi, M.; Giancaspro, R.; Cassano, M. Biofilm in Sino-Nasal Infectious Diseases: The Role Nasal Cytology in the Diagnostic Work up and Therapeutic Implications. Eur. Arch. Oto-Rhino-Laryngol. 2023, 280, 1523–1528. [Google Scholar] [CrossRef] [PubMed]
- Lam, K.; Schleimer, R.; Kern, R.C. The Etiology and Pathogenesis of Chronic Rhinosinusitis: A Review of Current Hypotheses. Curr. Allergy Asthma Rep. 2015, 15, 41. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.Z.; Li, Y.C.; Wang, X.D.; Lu, X.X.; Hu, C.H.; He, S.; Liu, X. The Microbiology of Chronic Rhinosinusitis with and without Nasal Polyps. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 1439–1447. [Google Scholar] [CrossRef]
- Huang, J.; Xu, Y. Autoimmunity: A New Focus on Nasal Polyps. Int. J. Mol. Sci. 2023, 24, 8444. [Google Scholar] [CrossRef]
- Chegini, Z.; Shariati, A.; Asghari, A.; Rajaeih, S.; Ghorbani, M.; Jalessi, M.; Mirshekar, M.; Razavi, S. Molecular Analysis of Dominant Paranasal Sinus Bacteria in Patients with and without Chronic Rhinosinusitis. Arch. Microbiol. 2022, 204, 327. [Google Scholar] [CrossRef] [PubMed]
- Soyka, M.B.; Wawrzyniak, P.; Eiwegger, T.; Holzmann, D.; Treis, A.; Wanke, K.; Kast, J.I.; Akdis, C.A. Defective Epithelial Barrier in Chronic Rhinosinusitis: The Regulation of Tight Junctions by IFN-γ and IL-4. J. Allergy Clin. Immunol. 2012, 130, 1087–1096.e10. [Google Scholar] [CrossRef] [PubMed]
- Pothoven, K.L.; Norton, J.E.; Hulse, K.E.; Suh, L.A.; Carter, R.G.; Rocci, E.; Harris, K.E.; Shintani-Smith, S.; Conley, D.B.; Chandra, R.K.; et al. Oncostatin M Promotes Mucosal Epithelial Barrier Dysfunction, and Its Expression Is Increased in Patients with Eosinophilic Mucosal Disease. J. Allergy Clin. Immunol. 2015, 136, 737–746.e4. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Alessandrini, L.; Marioni, G. Structured Histopathology for Endotyping and Planning Rational Treatment in Chronic Rhinosinusitis. Am. J. Otolaryngol. Head Neck Med. Surg. 2021, 42, 102795. [Google Scholar] [CrossRef] [PubMed]
- Goulioumis, A.K.; Kourelis, K.; Gkorpa, M.; Danielides, V. Pathogenesis of Nasal Polyposis: Current Trends. Indian J. Otolaryngol. Head Neck Surg. 2023, 75, 733–741. [Google Scholar] [CrossRef]
- Estravís, M.; Pérez-Pazos, J.; Moreno-Jimenez, E.; Triviño, J.C.; García-Sánchez, A.; Gómez-García, M.; Morgado, N.; Ramos-González, J.; Gil-Melcón, M.; Martín-García, C.; et al. Transcriptomics Reveals New Regulatory Mechanisms Involved in Benralizumab Response. Allergy Eur. J. Allergy Clin. Immunol. 2023, 78, 3023–3026. [Google Scholar] [CrossRef]
- Estravís, M.; Pérez-Pazos, J.; Martin, M.J.; Ramos-González, J.; Gil-Melcón, M.; Martín-García, C.; García-Sánchez, A.; Sanz, C.; Dávila, I. Quantitative and Qualitative Methods of Evaluating Response to Biologics in Severe Asthma Patients: Results from a Real-World Study. J. Allergy Clin. Immunol. Pract. 2023, 11, 949–951.e2. [Google Scholar] [CrossRef] [PubMed]
- Berg, G.; Rybakova, D.; Fischer, D.; Cernava, T.; Vergès, M.C.C.; Charles, T.; Chen, X.; Cocolin, L.; Eversole, K.; Corral, G.H.; et al. Microbiome Definition Re-Visited: Old Concepts and New Challenges. Microbiome 2020, 8, 103. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; Agostoni, P.; Barros, H.; et al. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef]
- Paramasivan, S.; Bassiouni, A.; Shiffer, A.; Dillon, M.R.; Cope, E.K.; Cooksley, C.; Ramezanpour, M.; Moraitis, S.; Ali, M.J.; Bleier, B.; et al. The International Sinonasal Microbiome Study: A Multicentre, Multinational Characterization of Sinonasal Bacterial Ecology. Allergy Eur. J. Allergy Clin. Immunol. 2020, 75, 2033–2045. [Google Scholar] [CrossRef]
- Cao, P.P.; Bin Li, H.; Wang, B.F.; Bin Wang, S.; You, X.J.; Cui, Y.H.; Wang, D.Y.; Desrosiers, M.; Liu, Z. Distinct Immunopathologic Characteristics of Various Types of Chronic Rhinosinusitis in Adult Chinese. J. Allergy Clin. Immunol. 2009, 124, 478–484.e2. [Google Scholar] [CrossRef]
- Kim, D.; Assiri, A.M.; Kim, J.H. Recent Trends in Bacteriology of Adult Patients with Chronic Rhinosinusitis. J. Clin. Med. 2019, 8, 1889. [Google Scholar] [CrossRef]
- Bin Wang, S.; Chen, S.M.; Zhu, K.S.; Zhou, B.; Chen, L.; Zou, X.Y. Increased Lipopolysaccharide Content Is Positively Correlated with Glucocorticoid Receptor-Beta Expression in Chronic Rhinosinusitis with Nasal Polyps. Immunity, Inflamm. Dis. 2020, 8, 605–614. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, S.H.; Lim, J.Y.; Kim, D.; Jeong, I.S.; Lee, D.K.; Jang, Y.J. Association between the Sinus Microbiota with Eosinophilic Inflammation and Prognosis in Chronic Rhinosinusitis with Nasal Polyps. Exp. Mol. Med. 2020, 52, 978–987. [Google Scholar] [CrossRef]
- Feng, T.; Miao, P.; Liu, B.; Liu, Y.; Bao, X.; Xu, J.; Ren, N.; Li, Y.; Shi, J.; Cao, W.; et al. Sinus Microbiota in Patients With Eosinophilic and Non-Eosinophilic Chronic Rhinosinusitis With Nasal Polyps. Front. Cell. Infect. Microbiol. 2021, 11, 672355. [Google Scholar] [CrossRef]
- Abbas, E.E.; Li, C.; Xie, A.; Lu, S.; Tang, L.; Liu, Y.; Elfadil, A.; Wen, S. Distinct Clinical Pathology and Microbiota in Chronic Rhinosinusitis With Nasal Polyps Endotypes. Laryngoscope 2021, 131, E34–E44. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.S.; Liang, K.L. Comparison of Bacteriology Between Eosinophilic and Noneosinophilic Chronic Rhinosinusitis With Nasal Polyps. Otolaryngol. Head Neck Surg. 2023, 168, 1545–1550. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Xie, R.; Xiong, X.; Hu, Z.; Mao, X.; Wang, X.; Zhang, J.; Sun, P.; Yue, Z.; Wang, W.; et al. Alterations of Nasal Microbiome in Eosinophilic Chronic Rhinosinusitis. J. Allergy Clin. Immunol. 2023, 151, 1286–1295.e2. [Google Scholar] [CrossRef]
- Gan, W.; Zhang, H.; Yang, F.; Liu, S.; Liu, F.; Meng, J. The Influence of Nasal Bacterial Microbiome Diversity on the Pathogenesis and Prognosis of Chronic Rhinosinusitis Patients with Polyps. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1075–1088. [Google Scholar] [CrossRef]
- Gan, W.; Zhang, H.; Yang, F.; Liu, S.; Liu, F.; Meng, J. The Influence of Nasal Microbiome Diversity and Inflammatory Patterns on the Prognosis of Nasal Polyps. Sci. Rep. 2021, 11, 6364. [Google Scholar] [CrossRef]
- Lee, C.W.; Lee, B.J.; Yoo, S.H.; Yi, J.S. Relationship between Positive Bacterial Culture in Maxillary Sinus and Surgical Outcomes in Chronic Rhinosinusitis with Nasal Polyps. Auris Nasus Larynx 2014, 41, 446–449. [Google Scholar] [CrossRef] [PubMed]
- Stern, S.; Hadar, T.; Nachalon, Y.; Ben-Zvi, H.; Soudry, E.; Yaniv, E. Bacteriology of the Middle Meatus in Chronic Rhinosinusitis with and without Polyposis. ORL 2016, 78, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Saibene, A.M.; Vassena, C.; Pipolo, C.; Trimboli, M.; De Vecchi, E.; Felisati, G.; Drago, L. Odontogenic and Rhinogenic Chronic Sinusitis: A Modern Microbiological Comparison. Int. Forum Allergy Rhinol. 2016, 6, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Mihalj, M.; Bujak, M.; Butković, J.; Zubčić, Ž.; Levak, M.T.; Čes, J.; Kopić, V.; Lončar, M.B.; Mihalj, H. Differential Expression of TFF1 and TFF3 in Patients Suffering from Chronic Rhinosinusitis with Nasal Polyposis. Int. J. Mol. Sci. 2019, 20, 5461. [Google Scholar] [CrossRef]
- Korkmaz, H.; Ocal, B.; Tatar, E.C.; Tatar, I.; Ozdek, A.; Saylam, G.; Celik, H.H. Biofilms in Chronic Rhinosinusitis with Polyps: Is Eradication Possible? Eur. Arch. Otorhinolaryngol. 2014, 271, 2695–2702. [Google Scholar] [CrossRef]
- Singh, P.; Mehta, R.; Agarwal, S.; Mishra, P. Bacterial Biofilm on the Sinus Mucosa of Healthy Subjects and Patients with Chronic Rhinosinusitis (with or without Nasal Polyposis). J. Laryngol. Otol. 2015, 129, 46–49. [Google Scholar] [CrossRef]
- Cantone, E.; Negri, R.; Roscetto, E.; Grassia, R.; Catania, M.R.; Capasso, P.; Maffei, M.; Soriano, A.A.; Leone, C.A.; Iengo, M.; et al. In Vivo Biofilm Formation, Gram-Negative Infections and TAS2R38 Polymorphisms in CRSw NP Patients. Laryngoscope 2018, 128, E339–E345. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Lu, X.; Bo, M.; Qing, H.; Wang, X.; Zhang, L. The Microbiology of Chronic Rhinosinusitis with and without Nasal Polyps. Acta Otolaryngol. 2014, 134, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.C.; Bassiouni, A.; Tanjararak, K.; Vreugde, S.; Wormald, P.J.; Psaltis, A.J. Role of Fungi in Chronic Rhinosinusitis through ITS Sequencing. Laryngoscope 2018, 128, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.T.; Simpson, C.A.; Yang, H.H.; Suh, J.D.; Wang, M.B.; Lagishetty, V.; Liang, F.; Jacobs, J.P. Fungal and Bacterial Microbiome in Sinus Mucosa of Patients with and without Chronic Rhinosinusitis. Laryngoscope 2024, 134, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Gelber, J.T.; Cope, E.K.; Goldberg, A.N.; Pletcher, S.D. Evaluation of Malassezia and Common Fungal Pathogens in Subtypes of Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2016, 6, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Hoggard, M.; Zoing, M.; Biswas, K.; Taylor, M.W.; Douglas, R.G. The Sinonasal Mycobiota in Chronic Rhinosinusitis and Control Patients. Rhinology 2019, 57, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Hoggard, M.; Jacob, B.; Wheeler, D.; Zoing, M.; Chang, K.; Biswas, K.; Middleditch, M.; Douglas, R.G.; Taylor, M.W. Multiomic Analysis Identifies Natural Intrapatient Temporal Variability and Changes in Response to Systemic Corticosteroid Therapy in Chronic Rhinosinusitis. Immunity, Inflamm. Dis. 2021, 9, 90–107. [Google Scholar] [CrossRef]
- Babu, H.; Sharma, R.; Sharma, V.K.; Goyal, R.; Rana, A.K. Does FESS Alter the Sinonasal Microbiome. Egypt. J. Ear Nose Throat Allied Sci. 2022, 23, 1–6. [Google Scholar] [CrossRef]
- Costa, C.; Garzaro, M.; Boggio, V.; Sidoti, F.; Simeone, S.; Raimondo, L.; Cavallo, G.P.; Pecorari, G.; Cavallo, R. Detection of Herpesviruses 1–6 and Community-Acquired Respiratory Viruses in Patients with Chronic Rhinosinusitis with Nasal Polyposis. Intervirology 2014, 57, 101–105. [Google Scholar] [CrossRef]
- Rowan, N.R.; Lee, S.; Sahu, N.; Kanaan, A.; Cox, S.; Phillips, C.D.; Wang, E.W. The Role of Viruses in the Clinical Presentation of Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2015, 29, e197–e200. [Google Scholar] [CrossRef] [PubMed]
- Lal, D.; Song, L.; Brar, T.; Cope, E.K.; Keim, P.; Williams, S.; Chung, Y.; Murugan, V.; LaBaer, J.; Magee, D.M. Antibody Responses to the Host Microbiome in Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2023, 13, 1503–1510. [Google Scholar] [CrossRef]
- Alammar, Y.; Rousseau, S.; Desrosiers, M.; Tewfik, M.A. The Effect of Corticosteroids on Sinus Microbiota in Chronic Rhinosinusitis Patients with Nasal Polyposis. Am. J. Rhinol. Allergy 2023, 37, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Bartosik, T.J.; Campion, N.J.; Freisl, K.; Liu, D.T.; Gangl, K.; Stanek, V.; Tu, A.; Pjevac, P.; Hausmann, B.; Eckl-Dorna, J.; et al. The Nasal Microbiome in Patients Suffering from Non-Steroidal Anti-Inflammatory Drugs-Exacerbated Respiratory Disease in Absence of Corticosteroids. Front. Immunol. 2023, 14, 1112345. [Google Scholar] [CrossRef] [PubMed]
- Koeller, K.; Herlemann, D.P.R.; Schuldt, T.; Ovari, A.; Guder, E.; Podbielski, A.; Kreikemeyer, B.; Olzowy, B. Microbiome and Culture Based Analysis of Chronic Rhinosinusitis Compared to Healthy Sinus Mucosa. Front. Microbiol. 2018, 9, 643. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.; Yang, F.; Tang, Y.; Zhou, D.; Qing, D.; Hu, J.; Liu, S.; Liu, F.; Meng, J. The Difference in Nasal Bacterial Microbiome Diversity between Chronic Rhinosinusitis Patients with Polyps and a Control Population. Int. Forum Allergy Rhinol. 2019, 9, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Wagner Mackenzie, B.; West, A.G.; Waite, D.W.; Lux, C.A.; Douglas, R.G.; Taylor, M.W.; Biswas, K. A Novel Description of the Human Sinus Archaeome During Health and Chronic Rhinosinusitis. Front. Cell. Infect. Microbiol. 2020, 10, 398. [Google Scholar] [CrossRef] [PubMed]
- Cook, K.A.; Domissy, A.; Simon, R.A.; White, A.A.; Modena, B.D. Dysbiosis in Aspirin-Exacerbated Respiratory Disease. Int. Forum Allergy Rhinol. 2021, 11, 1116–1120. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Han, D.; Mo, J.H.; Kim, Y.M.; Kim, D.W.; Choi, H.G.; Park, J.W.; Shin, H.W. Antibiotic-Dependent Relationships between the Nasal Microbiome and Secreted Proteome in Nasal Polyps. Allergy Asthma Immunol. Res. 2021, 13, 589–608. [Google Scholar] [CrossRef]
- Lal, D.; Keim, P.; Delisle, J.; Barker, B.; Rank, M.A.; Chia, N.; Schupp, J.M.; Gillece, J.D.; Cope, E.K. Mapping and Comparing Bacterial Microbiota in the Sinonasal Cavity of Healthy, Allergic Rhinitis, and Chronic Rhinosinusitis Subjects. Int. Forum Allergy Rhinol. 2017, 7, 561–569. [Google Scholar] [CrossRef]
- Shi, P.; Wei, H.; Liu, X.; Dong, S.; He, S.; Zeng, Y.; Yang, T.; Liu, C.; Li, Y. The Nasal Bacteria Microbiome Comparison Among Fungal Ball Sinusitis, Chronic Sinusitis with Polyps. Indian J. Microbiol. 2023, 63, 120–128. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, J.; Hao, Y.; Wang, B.; Wang, Y.; Liu, Q.; Zhao, J.; Li, Y.; Wang, P.; Wang, X.; et al. Predicting the Recurrence of Chronic Rhinosinusitis with Nasal Polyps Using Nasal Microbiota. Allergy Eur. J. Allergy Clin. Immunol. 2022, 77, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Wos-Oxley, M.L.; Chaves-Moreno, D.; Jáuregui, R.; Oxley, A.P.A.; Kaspar, U.; Plumeier, I.; Kahl, S.; Rudack, C.; Becker, K.; Pieper, D.H. Exploring the Bacterial Assemblages along the Human Nasal Passage. Environ. Microbiol. 2016, 18, 2259–2271. [Google Scholar] [CrossRef]
- Cho, S.W.; Kim, D.Y.; Choi, S.; Won, S.; Kang, H.R.; Yi, H. Microbiome Profiling of Uncinate Tissue and Nasal Polyps in Patients with Chronic Rhinosinusitis Using Swab and Tissue Biopsy. PLoS ONE 2021, 16, e0249688. [Google Scholar] [CrossRef]
- Liu, C.M.; Kohanski, M.A.; Mendiola, M.; Soldanova, K.; Dwan, M.G.; Lester, R.; Nordstrom, L.; Price, L.B.; Lane, A.P. Impact of Saline Irrigation and Topical Corticosteroids on the Postsurgical Sinonasal Microbiota. Int. Forum Allergy Rhinol. 2015, 5, 185–190. [Google Scholar] [CrossRef]
- Varvyanskaya, A.; Lopatin, A. Efficacy of Long-Term Low-Dose Macrolide Therapy in Preventing Early Recurrence of Nasal Polyps after Endoscopic Sinus Surgery. Int. Forum Allergy Rhinol. 2014, 4, 533–541. [Google Scholar] [CrossRef]
- Tabet, P.; Endam, L.M.; Boisvert, P.; Boulet, L.P.; Desrosiers, M. Gram-Negative Bacterial Carriage in Chronic Rhinosinusitis with Nasal Polyposis Is Not Associated with More Severe Inflammation. Int. Forum Allergy Rhinol. 2015, 5, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Stryjewska-Makuch, G.; Janik, M.A.; Klamińska-Cebula, H.; Kolebacz, B.; Ścierski, W.; Lisowska, G. Bacteriological Analysis of Selected Phenotypes of Chronic Rhinosinusitis with Co-Existing Asthma, Allergy and Hypersensitivity to Non-Steroidal Anti-Inflammatory Drugs. Postep. Dermatologii i Alergol. 2021, 38, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.B.; Hong, S.W.; Kim, D.K.; Jeon, S.G.; Kim, K.R.; Cho, S.H.; Gho, Y.S.; Jee, Y.K.; Kim, Y.K. Decreased Diversity of Nasal Microbiota and Their Secreted Extracellular Vesicles in Patients with Chronic Rhinosinusitis Based on a Metagenomic Analysis. Allergy Eur. J. Allergy Clin. Immunol. 2014, 69, 517–526. [Google Scholar] [CrossRef]
- Uhliarova, B.; Adamkov, M.; Svec, M.; Calkovska, A. The Effect of Smoking on CT Score, Bacterial Colonization and Distribution of Inflammatory Cells in the Upper Airways of Patients with Chronic Rhinosinusitis. Inhal. Toxicol. 2014, 26, 419–425. [Google Scholar] [CrossRef]
- Ramakrishnan, V.R.; Frank, D.N. Impact of Cigarette Smoking on the Middle Meatus Microbiome in Health and Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2015, 5, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Biswas, K.; Chang, A.; Hoggard, M.; Radcliff, F.J.; Jiang, Y.; Taylor, M.W.; Darveau, R.; Douglas, R.G. Toll-like Receptor Activation by Sino-Nasal Mucus in Chronic Rhinosinusitis. Rhinology 2017, 55, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Cope, E.K.; Goldberg, A.N.; Pletcher, S.D.; Lynch, S.V. Compositionally and Functionally Distinct Sinus Microbiota in Chronic Rhinosinusitis Patients Have Immunological and Clinically Divergent Consequences. Microbiome 2017, 5, 53. [Google Scholar] [CrossRef] [PubMed]
- Hoggard, M.; Waldvogel-Thurlow, S.; Zoing, M.; Chang, K.; Radcliff, F.J.; Mackenzie, B.W.; Biswas, K.; Douglas, R.G.; Taylor, M.W. Inflammatory Endotypes and Microbial Associations in Chronic Rhinosinusitis. Front. Immunol. 2018, 9, 2065. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Hoggard, M.; Zoing, M.; Jiang, Y.; Biswas, K.; Taylor, M.W.; Douglas, R.G. The Effect of Medical Treatments on the Bacterial Microbiome in Patients with Chronic Rhinosinusitis: A Pilot Study. Int. Forum Allergy Rhinol. 2018, 8, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Karunasagar, A.; Jalastagi, R.; Naik, A.; Rai, P. Detection of Bacteria by 16S RRNA PCR and Sequencing in Culture-Negative Chronic Rhinosinusitis. Laryngoscope 2018, 128, 2223–2225. [Google Scholar] [CrossRef] [PubMed]
- Ooi, M.L.; Jothin, A.; Bennett, C.; Ooi, E.H.; Vreugde, S.; Psaltis, A.J.; Wormald, P.J. Manuka Honey Sinus Irrigations in Recalcitrant Chronic Rhinosinusitis: Phase 1 Randomized, Single-Blinded, Placebo-Controlled Trial. Int. Forum Allergy Rhinol. 2019, 9, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Vandelaar, L.J.; Hanson, B.; Marino, M.; Yao, W.C.; Luong, A.U.; Arias, C.A.; Ramakrishnan, V.; Citardi, M.J. Analysis of Sinonasal Microbiota in Exacerbations of Chronic Rhinosinusitis Subgroups. OTO Open 2019, 3, 2473974X19875100. [Google Scholar] [CrossRef] [PubMed]
- Zakiah, A.M.; Perkasa, M.F.; Utami, A.D.; Djamin, R.; Bahar, B.; Hamid, F.; Punagi, A.Q. Microbiome Profile in Chronic Rhinosinusitis with and without Polyps of Makassar, Indonesia. Otorhinolaryngol. Clin. 2019, 11, 55–63. [Google Scholar] [CrossRef]
- Biswas, K.; Cavubati, R.; Gunaratna, S.; Hoggard, M.; Waldvogel-Thurlow, S.; Hong, J.; Chang, K.; Wagner Mackenzie, B.; Taylor, M.W.; Douglas, R.G. Comparison of Subtyping Approaches and the Underlying Drivers of Microbial Signatures for Chronic Rhinosinusitis. mSphere 2019, 4, e00679-18. [Google Scholar] [CrossRef]
- Takeda, K.; Sakakibara, S.; Yamashita, K.; Motooka, D.; Nakamura, S.; El Hussien, M.A.; Katayama, J.; Maeda, Y.; Nakata, M.; Hamada, S.; et al. Allergic Conversion of Protective Mucosal Immunity against Nasal Bacteria in Patients with Chronic Rhinosinusitis with Nasal Polyposis. J. Allergy Clin. Immunol. 2019, 143, 1163–1175.e15. [Google Scholar] [CrossRef] [PubMed]
- Wagner Mackenzie, B.; Baker, J.; Douglas, R.G.; Taylor, M.W.; Biswas, K. Detection and Quantification of Staphylococcus in Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2019, 9, 1462–1469. [Google Scholar] [CrossRef]
- Endam, L.M.; Alromaih, S.; Gonzalez, E.; Madrenas, J.; Cousineau, B.; Renteria, A.E.; Desrosiers, M. Intranasal Application of Lactococcus Lactis W136 Is Safe in Chronic Rhinosinusitis Patients With Previous Sinus Surgery. Front. Cell. Infect. Microbiol. 2020, 10, 440. [Google Scholar] [CrossRef]
- Lux, C.A.; Wagner Mackenzie, B.; Johnston, J.; Zoing, M.; Biswas, K.; Taylor, M.W.; Douglas, R.G. Antibiotic Treatment for Chronic Rhinosinusitis: Prescription Patterns and Associations With Patient Outcome and the Sinus Microbiota. Front. Microbiol. 2020, 11, 595555. [Google Scholar] [CrossRef] [PubMed]
- Leszczyńska, J.; Stryjewska-Makuch, G.; Ścierski, W.; Lisowska, G. Bacterial Flora of the Nose and Paranasal Sinuses among Patients over 65 Years Old with Chronic Rhinosinusitis Who Underwent Endoscopic Sinus Surgery. Clin. Interv. Aging 2020, 15, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Nepal, R.; Houtak, G.; Shaghayegh, G.; Bouras, G.; Shearwin, K.; Psaltis, A.J.; Wormald, P.; Vreugde, S. Prophages Encoding Human Immune Evasion Cluster Genes Are Enriched in Staphylococcus Aureus Isolated from Chronic Rhinosinusitis Patients with Nasal Polyps. Microb. Genom. 2021, 7, 000726. [Google Scholar] [CrossRef]
- Su, Y.W.; Huang, W.H.; Yeh, C.F. Pantoea Dispersa Rhinosinusitis: Clinical Aspects of a Rare Sinonasal Pathogen. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 4389–4395. [Google Scholar] [CrossRef]
- Odat, H.; Al-Ashqar, R.; Al-Ali, R.A.; Al-Qudah, M. The Bacteriology of Middle Meatus and Ethmoid Sinuses in Chronic Rhinosinusitis: Epidemiological Analysis and Surgical Impact. Int. Tinnitus J. 2022, 26, 110–114. [Google Scholar] [CrossRef]
- Zhu, Z.S.; Lan, J.; Wei, R.; Xu, Y.; Hong, Y.; Bao, W.; He, G. Microbiome and Th Cytokines Association in Chronic Rhinosinusitis with or without Nasal Polyp. Laryngoscope Investig. Otolaryngol. 2023, 8, 335–345. [Google Scholar] [CrossRef]
- Gan, W.; Xiang, Y.; Wei, B.; Liu, S.; Liu, F. The Inflammatory Microenvironment of Nasal Polyps in Patients with Chronic Rhinosinusitis and the Relationship of This Microenvironment with the Nasal Microbiome. Asian J. Surg. 2024, 47, 124–133. [Google Scholar] [CrossRef]
- Sproson, E.L.; Thomas, K.M.; Lau, L.C.; Harries, P.G.; Howarth, P.H.; Salib, R.J. Common Airborne Fungi Induce Species-Specific Effects on Upper Airway Inflammatory and Remodelling Responses. Rhinology 2016, 54, 51–55. [Google Scholar] [CrossRef]
- Dobretsov, K.G.; Kolenchukova, O.; Sipkin, A.; Bellussi, L.M.; Ciprandi, G.; Passali, D. A Randomized, Double-Blind, Placebo- -Controlled Study to Investigate the Use of Bacteriophages in Patients with Chronic Rhinosinusitis with Nasal Polyps. Otolaryngol. Pol. 2021, 75, 33–37. [Google Scholar] [CrossRef]
- Ancona, G.; Alagna, L.; Alteri, C.; Palomba, E.; Tonizzo, A.; Pastena, A.; Muscatello, A.; Gori, A.; Bandera, A. Gut and Airway Microbiota Dysbiosis and Their Role in COVID-19 and Long-COVID. Front. Immunol. 2023, 14, 1080043. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.S.B.; Raes, J.; Bork, P. The Human Gut Microbiome: From Association to Modulation. Cell 2018, 172, 1198–1215. [Google Scholar] [CrossRef] [PubMed]
- Ferdous, T.; Jiang, L.; Dinu, I.; Groizeleau, J.; Kozyrskyj, A.L.; Greenwood, C.M.T.; Arrieta, M.C. The Rise to Power of the Microbiome: Power and Sample Size Calculation for Microbiome Studies. Mucosal Immunol. 2022, 15, 1060–1070. [Google Scholar] [CrossRef] [PubMed]
- Kers, J.G.; Saccenti, E. The Power of Microbiome Studies: Some Considerations on Which Alpha and Beta Metrics to Use and How to Report Results. Front. Microbiol. 2022, 12, 796025. [Google Scholar] [CrossRef] [PubMed]
- Kumpitsch, C.; Koskinen, K.; Schöpf, V.; Moissl-Eichinger, C. The Microbiome of the Upper Respiratory Tract in Health and Disease. BMC Biol. 2019, 17, 87. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liang, Q.; Ren, Y.; Guo, C.; Ge, X.; Wang, L.; Cheng, Q.; Luo, P.; Zhang, Y.; Han, X. Immunosenescence: Molecular Mechanisms and Diseases. Signal Transduct. Target. Ther. 2023, 8, 200. [Google Scholar] [CrossRef] [PubMed]
- Whelan, F.J.; Verschoor, C.P.; Stearns, J.C.; Rossi, L.; Luinstra, K.; Loeb, M.; Smieja, M.; Johnstone, J.; Surette, M.G.; Bowdish, D.M.E. The Loss of Topography in the Microbial Communities of the Upper Respiratory Tract in the Elderly. Ann. Am. Thorac. Soc. 2014, 11, 513–521. [Google Scholar] [CrossRef]
- Jain, R.; Hoggard, M.; Biswas, K.; Zoing, M.; Jiang, Y.; Douglas, R. Changes in the Bacterial Microbiome of Patients with Chronic Rhinosinusitis after Endoscopic Sinus Surgery. Int. Forum Allergy Rhinol. 2017, 7, 7–15. [Google Scholar] [CrossRef]
- Shah, S.J.; Hawn, V.S.; Zhu, N.; Fang, C.H.; Gao, Q.; Akbar, N.A.; Abuzeid, W.M. Postoperative Infection Rate and Associated Factors Following Endoscopic Sinus Surgery. Ann. Otol. Rhinol. Laryngol. 2022, 131, 5–11. [Google Scholar] [CrossRef]
- Szaleniec, J.; Bezshapkin, V.; Krawczyk, A.; Kopera, K.; Zapała, B.; Gosiewski, T.; Kosciolek, T. Determinants of the Microbiome Spatial Variability in Chronic Rhinosinusitis. Rhinology 2024, 62, 119–126. [Google Scholar] [CrossRef]
- Antonopoulos, D.A.; Huse, S.M.; Morrison, H.G.; Schmidt, T.M.; Sogin, M.L.; Young, V.B. Reproducible Community Dynamics of the Gastrointestinal Microbiota Following Antibiotic Perturbation. Infect. Immun. 2009, 77, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Gerardi, D.; Santostasi, N.; Torge, D.; Rinaldi, F.; Bernardi, S.; Bianchi, S.; Piattelli, M.; Varvara, G. Regenerative Potential of Platelet—Rich Fibrin in Maxillary Sinus Floor Lift Techniques: A Systematic Review. J. Biol. Regul. Homeost. Agents 2023, 37, 2357–2369. [Google Scholar] [CrossRef]
- Szaleniec, J.; Gibała, A.; Hartwich, P.; Hydzik-Sobocińska, K.; Konior, M.; Gosiewski, T.; Szaleniec, M. Challenging the Gold Standard: Methods of Sampling for Microbial Culture in Patients with Chronic Rhinosinusitis. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 4795–4803. [Google Scholar] [CrossRef]
- Lee, J.T.; Frank, D.N.; Ramakrishnan, V. Microbiome of the Paranasal Sinuses: Update and Literature Review. Am. J. Rhinol. Allergy 2016, 30, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Callahan, B.J.; McMurdie, P.J.; Holmes, S.P. Exact Sequence Variants Should Replace Operational Taxonomic Units in Marker-Gene Data Analysis. ISME J. 2017, 11, 2639–2643. [Google Scholar] [CrossRef]
- Walters, K.E.; Martiny, J.B.H. Alpha-, Beta-, and Gamma-Diversity of Bacteria Varies across Habitats. PLoS ONE 2020, 15, e0233872. [Google Scholar] [CrossRef]
- Copeland, E.; Leonard, K.; Carney, R.; Kong, J.; Forer, M.; Naidoo, Y.; Oliver, B.G.G.; Seymour, J.R.; Woodcock, S.; Burke, C.M.; et al. Chronic Rhinosinusitis: Potential Role of Microbial Dysbiosis and Recommendations for Sampling Sites. Front. Cell. Infect. Microbiol. 2018, 8, 57. [Google Scholar] [CrossRef]
- Hufnagl, K.; Pali-Schöll, I.; Roth-Walter, F.; Jensen-Jarolim, E. Dysbiosis of the Gut and Lung Microbiome Has a Role in Asthma. Semin. Immunopathol. 2020, 42, 75–93. [Google Scholar] [CrossRef]
- Garcia-Nuñez, M.; Millares, L.; Pomares, X.; Ferrari, R.; Pérez-Brocal, V.; Gallego, M.; Espasa, M.; Moya, A.; Monsó, E. Severity-Related Changes of Bronchial Microbiome in Chronic Obstructive Pulmonary Disease. J. Clin. Microbiol. 2014, 52, 4217–4223. [Google Scholar] [CrossRef] [PubMed]
- Ege, M.J.; Mayer, M.; Normand, A.-C.; Genuneit, J.; Cookson, W.O.; Phil, D.; Braun-Fahrländer, C.; Heederik, D.; Piarrroux, R.; von Mutius, E. Exposure to Environmental Microorganisms and Childhood Asthma. N. Engl. J. Med. 2011, 364, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.J.; Jithpratuck, W.; Wasylik, K.; Sriaroon, P.; Dishaw, L.J. Associations of Microbial Diversity with Age and Other Clinical Variables among Pediatric Chronic Rhinosinusitis (CRS) Patients. Microorganisms 2023, 11, 422. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, T.R.; Jakobsson, H.E.; Andersson, A.F.; Björkstén, B.; Engstrand, L.; Jenmalm, M.C. Low Gut Microbiota Diversity in Early Infancy Precedes Asthma at School Age. Clin. Exp. Allergy 2014, 44, 842–850. [Google Scholar] [CrossRef]
- Man, W.H.; De Steenhuijsen Piters, W.A.A.; Bogaert, D. The Microbiota of the Respiratory Tract: Gatekeeper to Respiratory Health. Nat. Rev. Microbiol. 2017, 15, 259–270. [Google Scholar] [CrossRef]
- Slattery, J.; Macfabe, D.F.; Frye, R.E. The Significance of the Enteric Microbiome on the Development of Childhood Disease: A Review of Prebiotic and Probiotic Therapies in Disorders of Childhood. Clin. Med. Insights Pediatr. 2016, 10, CMPed.S38338. [Google Scholar] [CrossRef]
- Mulder, B.; Pouwels, K.B.; Schuiling-Veninga, C.C.M.; Bos, H.J.; de Vries, T.W.; Jick, S.S.; Hak, E. Antibiotic Use during Pregnancy and Asthma in Preschool Children: The Influence of Confounding. Clin. Exp. Allergy 2016, 46, 1214–1226. [Google Scholar] [CrossRef] [PubMed]
- Maxfield, A.Z.; Korkmaz, H.; Gregorio, L.L.; Busaba, N.Y.; Gray, S.T.; Holbrook, E.H.; Guo, R.; Bleier, B.S. General Antibiotic Exposure Is Associated with Increased Risk of Developing Chronic Rhinosinusitis. Laryngoscope 2017, 127, 296–302. [Google Scholar] [CrossRef]
- Konovalovas, A.; Armalytė, J.; Klimkaitė, L.; Liveikis, T.; Jonaitytė, B.; Danila, E.; Bironaitė, D.; Mieliauskaitė, D.; Bagdonas, E.; Aldonytė, R. Human Nasal Microbiota Shifts in Healthy and Chronic Respiratory Disease Conditions. BMC Microbiol. 2024, 24, 150. [Google Scholar] [CrossRef]
- Mccauley, K.; Durack, J.; Valladares, R.; Douglas, W.; Lin, D.L.; Calatroni, A.; Lebeau, P.K.; Hoang, T. Distinct nasal airway bacterial microbiotas differentially relate to exacerbation in pediatric patients with asthma. J. Allergy Clin. Immunol. 2019, 144, 1187–1197. [Google Scholar] [CrossRef]
- Wang, Z.; Maschera, B.; Lea, S.; Kolsum, U.; Michalovich, D.; Van Horn, S.; Traini, C.; Brown, J.R.; Hessel, E.M.; Singh, D. Airway Host-Microbiome Interactions in Chronic Obstructive Pulmonary Disease. Respir. Res. 2019, 20, 113. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. Microbiology of Chronic Rhinosinusitis. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Song, B.; Zheng, H.; Han, S.; Tang, L.; Yang, X.; Chu, P.; Wang, P.; Lu, J.; Ge, W.; Ni, X. Detection of Nasal Microbiota in Pediatric Patients with Antrochoanal Polyps by TLDA. Int. J. Pediatr. Otorhinolaryngol. 2020, 130, 109811. [Google Scholar] [CrossRef] [PubMed]
- Moyano, R.O.; Tonetti, F.R.; Tomokiyo, M.; Kanmani, P.; Vizoso-Pinto, M.G.; Kim, H.; Quilodrán-Vega, S.; Melnikov, V.; Alvarez, S.; Takahashi, H.; et al. The Ability of Respiratory Commensal Bacteria to Beneficially Modulate the Lung Innate Immune Response Is a Strain Dependent Characteristic. Microorganisms 2020, 8, 727. [Google Scholar] [CrossRef]
- Fujieda, S.; Imoto, Y.; Kato, Y.; Ninomiya, T.; Tokunaga, T.; Tsutsumiuchi, T.; Yoshida, K.; Kidoguchi, M.; Takabayashi, T. Eosinophilic Chronic Rhinosinusitis. Allergol. Int. 2019, 68, 403–412. [Google Scholar] [CrossRef]
- Stryjewska-Makuch, G.; Janik, M.A.; Lisowska, G.; Kolebacz, B. Bacteriological Analysis of Isolated Chronic Sinusitis without Polyps. Postep. Dermatol. Alergol. 2018, 35, 375–380. [Google Scholar] [CrossRef]
- Yaniv, D.; Stern, D.; Vainer, I.; Ben Zvi, H.; Yahav, D.; Soudry, E. The Bacteriology of Recurrent Acute Exacerbations of Chronic Rhinosinusitis: A Longitudinal Analysis. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 3051–3057. [Google Scholar] [CrossRef]
- Jeican, I.I.; Gheban, D.; Barbu-Tudoran, L.; Inișca, P.; Albu, C.; Ilieș, M.; Albu, S.; Vică, M.L.; Matei, H.V.; Tripon, S.; et al. Respiratory Nasal Mucosa in Chronic Rhinosinusitis with Nasal Polyps versus COVID-19: Histopathology, Electron Microscopy Analysis and Assessing of Tissue Interleukin-33. J. Clin. Med. 2021, 10, 4110. [Google Scholar] [CrossRef]
- Ver Heul, A.; Planer, J.; Kau, A.L. The Human Microbiota and Asthma. Clin. Rev. Allergy Immunol. 2019, 57, 350–363. [Google Scholar] [CrossRef]
- Brescia, G.; Contro, G.; Giacomelli, L.; Barion, U.; Frigo, A.C.; Marioni, G. Blood Eosinophilic and Basophilic Trends in Recurring and Non-Recurring Eosinophilic Rhinosinusitis with Nasal Polyps. Am. J. Rhinol. Allergy 2021, 35, 296–301. [Google Scholar] [CrossRef]
- Tosun, F.; Arslan, H.H.; Karslioglu, Y.; Deveci, M.S.; Durmaz, A. Relationship between Postoperative Recurrence Rate and Eosinophil Density of Nasal Polyps. Ann. Otol. Rhinol. Laryngol. 2010, 119, 455–459. [Google Scholar] [CrossRef]
- Cavaliere, C.; Masieri, S.; Begvarfaj, E.; Loperfido, A.; Baroncelli, S.; Cascone, F.; Ciofalo, A. Long-Term Perspectives on Chronic Rhinosinusitis with Nasal Polyps: Evaluating Recurrence Rates after Functional Endoscopic Sinus Surgery in the Biologics Era—A 5-Year Follow-Up Study. J. Pers. Med. 2024, 14, 297. [Google Scholar] [CrossRef] [PubMed]
- Bomar, L.; Brugger, S.D.; Yost, B.H.; Davies, S.S.; Lemon, K.P. Corynebacterium Accolens Releases Antipneumococcal Free Fatty Acids from Human Nostril and Skin Surface Triacylglycerols. MBio 2016, 7, e01725-15. [Google Scholar] [CrossRef] [PubMed]
- Menberu, M.A.; Liu, S.; Cooksley, C.; Hayes, A.J.; Psaltis, A.J.; Wormald, P.J.; Vreugde, S. Corynebacterium Accolens Has Antimicrobial Activity against Staphylococcus Aureus and Methicillin-Resistant s. Aureus Pathogens Isolated from the Sinonasal Niche of Chronic Rhinosinusitis Patients. Pathogens 2021, 10, 207. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Peña, S.; Rodríguez-Martínez, S.; Cancino-Diaz, M.E.; Cancino-Diaz, J.C. Staphylococcus Epidermidis Controls Opportunistic Pathogens in the Nose, Could It Help to Regulate SARS-CoV-2 (COVID-19) Infection? Life 2022, 12, 341. [Google Scholar] [CrossRef] [PubMed]
- Loperfido, A.; Cavaliere, C.; Begvarfaj, E.; Ciofalo, A.; D’Erme, G.; De Vincentiis, M.; Greco, A.; Millarelli, S.; Bellocchi, G.; Masieri, S. The Impact of Antibiotics and Steroids on the Nasal Microbiome in Patients with Chronic Rhinosinusitis: A Systematic Review According to PICO Criteria. J. Pers. Med. 2023, 13, 1583. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.C.; Adappa, N.D.; Cohen, N.A. Use of Topical Nasal Therapies in the Management of Chronic Rhinosinusitis. Laryngoscope 2013, 123, 2347–2359. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).