
Citrate Dialysate with and without Magnesium Supplementation in Hemodiafiltration: A Comparative Study Versus Acetate
 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Results
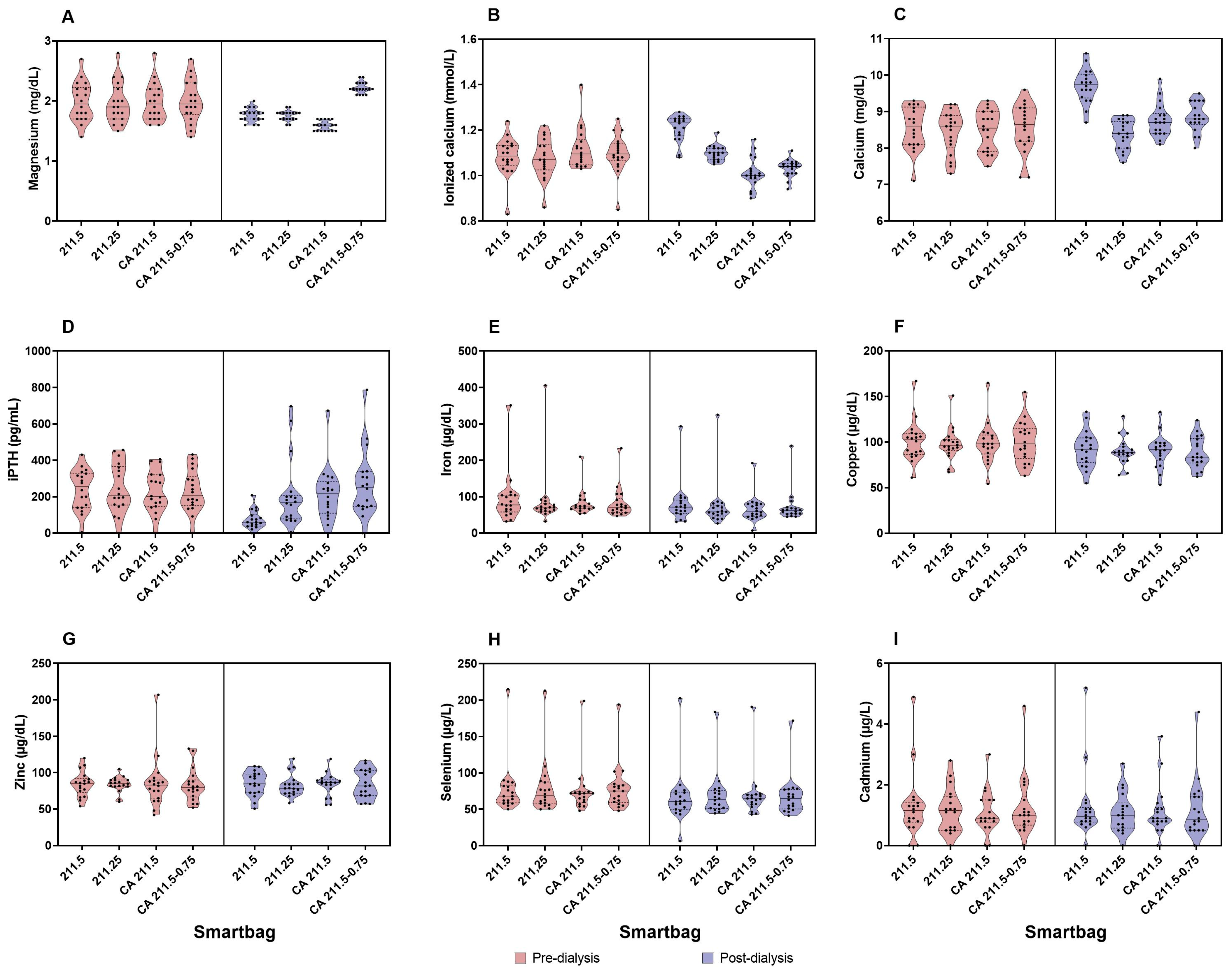
2.1. Calcium and CKD-MBD Biomarkers
2.2. Magnesium
2.3. Cadmium, Selenium, Copper, Zinc, and Iron
3. Discussion
4. Materials and Methods
4.1. Setting
4.2. Materials
- (a)
- Week 1: SmartBag 211.5, week 2: SmartBag 211.25, week 3: SmartBag CA 211.5, week 4: SmartBag CA 211.5-0.75
- (b)
- Week 1: SmartBag 211.25, week 2: SmartBag CA 211.5, week 3: SmartBag CA 211.5-0.75, week 4: SmartBag 211.5.
- (c)
- Week 1: SmartBag CA 211.5, week 2: SmartBag CA 211.5-0.75, week 3: SmartBag 211.5, week 4: SmartBag 211.25.
- (d)
- Week 1: SmartBag CA 211.5-0.75, week 2: SmartBag 211.5, week 3: SmartBag 211.25, week 4: SmartBag CA 211.5.
4.3. Variables
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sarnak, M.J.; Amann, K.; Bangalore, S.; Cavalcante, J.L.; Charytan, D.M.; Craig, J.C.; Gill, J.S.; Hlatky, M.A.; Jardine, A.G.; Landmesser, U.; et al. Chronic Kidney Disease and Coronary Artery Disease: JACC State-of-the-Art Review. J. Am. Coll Cardiol. 2019, 74, 1823–1838. [Google Scholar] [CrossRef] [PubMed]
- Blankestijn, P.J.; Bots, M.L. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. Reply. N. Engl. J. Med. 2023, 389, e42. [Google Scholar] [CrossRef] [PubMed]
- Maduell, F.; Moreso, F.; Pons, M.; Ramos, R.; Mora-Macià, J.; Carreras, J.; Soler, J.; Torres, F.; Campistol, J.M.; Martinez-Castelao, A. High-Efficiency Postdilution Online Hemodiafiltration Reduces All-Cause Mortality in Hemodialysis Patients. J. Am. Soc. Nephrol. 2013, 24, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Daimon, S.; Dan, K.; Kawano, M. Comparison of Acetate-Free Citrate Hemodialysis and Bicarbonate Hemodialysis Regarding the Effect of Intra-Dialysis Hypotension and Post-Dialysis Malaise. Ther. Apher. Dial. 2011, 15, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Pizzarelli, F.; Cerrai, T.; Dattolo, P.; Ferro, G. On-Line Haemodiafiltration with and without Acetate. Nephrol. Dial. Transplant. 2006, 21, 1648–1651. [Google Scholar] [CrossRef] [PubMed]
- Kuragano, T.; Kida, A.; Furuta, M.; Yahiro, M.; Kitamura, R.; Otaki, Y.; Nonoguchi, H.; Matsumoto, A.; Nakanishi, T. Effects of Acetate-Free Citrate-Containing Dialysate on Metabolic Acidosis, Anemia, and Malnutrition in Hemodialysis Patients. Artif. Organs. 2012, 36, 282–290. [Google Scholar] [CrossRef]
- Todeschini, M.; Macconi, D.; Fernández, N.G.; Ghilardi, M.; Anabaya, A.; Binda, E.; Morigi, M.; Cattaneo, D.; Perticucci, E.; Remuzzi, G.; et al. Effect of Acetate-Free Biofiltration and Bicarbonate Hemodialysis on Neutrophil Activation. Am. J. Kidney Dis. 2002, 40, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Vida, C.; Carracedo, J.; de Sequera, P.; Bodega, G.; Pérez, R.; Alique, M.; Ramírez, R. Increasing the Magnesium Concentration in Various Dialysate Solutions Differentially Modulates Oxidative Stress in a Human Monocyte Cell Line. Antioxidants 2020, 9, 319. [Google Scholar] [CrossRef] [PubMed]
- Noris, M.; Todeschini, M.; Casiraghi, F.; Roccatello, D.; Martina, G.; Minetti, L.; Imberti, B.; Gaspari, F.; Atti, M.; Remuzzi, G. Effect of Acetate, Bicarbonate Dialysis, and Acetate-Free Biofiltration on Nitric Oxide Synthesis: Implications for Dialysis Hypotension. Am. J. Kidney Dis. 1998, 32, 115–124. [Google Scholar] [CrossRef]
- Broseta, J.J.; López-Romero, L.C.; Cerveró, A.; Devesa-Such, R.; Soldevila, A.; Bea-Granell, S.; Sánchez-Pérez, P.; Hernández-Jaras, J. Improvements in Inflammation and Calcium Balance of Citrate versus Acetate as Dialysate Buffer in Maintenance Hemodialysis: A Unicentric, Cross-Over, Prospective Study. Blood Purif. 2021, 50, 914–920. [Google Scholar] [CrossRef]
- Azpiazu, D.; González-Parra, E.; Ortiz, A.; Egido, J.; Villa-Bellosta, R. Impact of Post-Dialysis Calcium Level on Ex Vivo Rat Aortic Wall Calcification. PLoS ONE 2017, 12, e0183730. [Google Scholar] [CrossRef] [PubMed]
- Pérez-García, R.; Ramírez Chamond, R.; de Sequera Ortiz, P.; Albalate, M.; Puerta Carretero, M.; Ortega, M.; Ruiz Caro, M.C.; Alcazar Arroyo, R. Citrate Dialysate Does Not Induce Oxidative Stress or Inflammation in Vitro as Compared to Acetate Dialysate. Nefrologia 2017, 37, 630–637. [Google Scholar] [CrossRef]
- Jung, S.W.; Kim, D.R.; Cho, K.S.; Seo, J.W.; Moon, H.; Park, E.J.; Kim, J.S.; Lee, T.W.; Ihm, C.G.; Jeong, D.W.; et al. Effects of Dialysate Acidification With Citrate Versus Acetate on Cell Damage, Uremic Toxin Levels, and Inflammation in Patients Receiving Maintenance Hemodialysis. Am. J. Kidney Dis. 2019, 73, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, K.; Tomo, T.; Kadota, J.I. Acetate-Free Blood Purification Can Impact Improved Nutritional Status in Hemodialysis Patients. J. Artif. Organs. 2011, 14, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Quinaux, T.; Pongas, M.; Guissard, É.; Ait-Djafer, Z.; Camoin-Schweitzer, M.C.; Ranchin, B.; Vrillon, I. Comparison between Citrate and Acetate Dialysate in Chronic Online Hemodiafiltration: A Short-Term Prospective Study in Pediatric Settings. Nephrol. Ther. 2020, 16, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Molina Nuñez, M.; De Alarcón, R.; Roca, S.; Álvarez, G.; Ros, M.S.; Jimeno, C.; Bucalo, L.; Villegas, I.; García, M.Á. Citrate versus Acetate-Based Dialysate in on-Line Haemodiafiltration. A Prospective Cross-over Study. Blood Purif. 2015, 39, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Grundström, G.; Christensson, A.; Alquist, M.; Nilsson, L.G.; Segelmark, M. Replacement of Acetate with Citrate in Dialysis Fluid: A Randomized Clinical Trial of Short Term Safety and Fluid Biocompatibility. BMC Nephrol. 2013, 14, 216. [Google Scholar] [CrossRef]
- Leung, K.C.W.; Tai, D.J.; Ravani, P.; Quinn, R.R.; Scott-Douglas, N.; MacRae, J.M. Citrate vs. Acetate Dialysate on Intradialytic Heparin Dose: A Double Blind Randomized Crossover Study. Hemodial. Int. 2016, 20, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Villa-Bellosta, R.; Hernández-Martínez, E.; Mérida-Herrero, E.; González-Parra, E. Impact of Acetate- or Citrate-Acidified Bicarbonate Dialysate on Ex Vivo Aorta Wall Calcification. Sci. Rep. 2019, 9, 11374. [Google Scholar] [CrossRef]
- Petitclerc, T.; Diab, R.; Le Roy, F.; Mercadal, L.; Hmida, J. Acetate-Free Hemodialysis: What Does It Mean? Nephrol. Ther. 2011, 7, 92–98. [Google Scholar] [CrossRef]
- Barmore, W.; Bajwa, T.; Burns, B. Biochemistry, Clotting Factors. [Updated 2023 Feb 24]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507850/ (accessed on 2 February 2024).
- Ishimura, E.; Okuno, S.; Yamakawa, T.; Inaba, M.; Nishizawa, Y. Serum Magnesium Concentration Is a Significant Predictor of Mortality in Maintenance Hemodialysis Patients. Magnes. Res. 2007, 20, 237–244. [Google Scholar] [CrossRef]
- Shimohata, H.; Yamashita, M.; Ohgi, K.; Tsujimoto, R.; Maruyama, H.; Takayasu, M.; Hirayama, K.; Kobayashi, M. The Relationship between Serum Magnesium Levels and Mortality in Non-Diabetic Hemodialysis Patients: A 10-Year Follow-up Study. Hemodial. Int. 2019, 23, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Pérez-García, R.; Jaldo, M.T.; Puerta, M.; Ortega, M.; Corchete, E.; de Sequera, P.; Martin-Navarro, J.A.; Albalate, M.; Alcázar, R. Hypomagnesemia in Hemodialysis Is Associated with Increased Mortality Risk: Its Relationship with Dialysis Fluid. Nefrología 2020, 40, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia Is a Significant Predictor of Cardiovascular and Non-Cardiovascular Mortality in Patients Undergoing Hemodialysis. Kidney Int. 2014, 85, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Dellepiane, S.; Medica, D.; Guarena, C.; Musso, T.; Quercia, A.D.; Leonardi, G.; Marengo, M.; Migliori, M.; Panichi, V.; Biancone, L.; et al. Citrate Anion Improves Chronic Dialysis Efficacy, Reduces Systemic Inflammation and Prevents Chemerin-Mediated Microvascular Injury. Sci. Rep. 2019, 9, 10622. [Google Scholar] [CrossRef] [PubMed]
- Urena-Torres, P.; Bieber, B.; Guebre-Egziabher, F.; Ossman, R.; Jadoul, M.; Inaba, M.; Robinson, B.M.; Port, F.; Jacquelinet, C.; Combe, C. Citric Acid-Containing Dialysate and Survival Rate in the Dialysis Outcomes and Practice Patterns Study. Kidney360 2021, 2, 666–673. [Google Scholar] [CrossRef]
- Nilsson, A.; Sternby, J.; Gundstrom, G.; Alquist Hegbrant, M. Citrate Dialysis Fluid and Calcium Mass Balance (Abstract). Nephrol. Dial. Transplant. 2013, 28 (Suppl. S1), 207. [Google Scholar]
- Argilés, A.; Mion, C.M. Calcium Balance and Intact PTH Variations during Haemodiafiltration. Nephrol. Dial. Transplant. 1995, 10, 2083–2089. [Google Scholar] [PubMed]
- Panichi, V.; Fiaccadori, E.; Rosati, A.; Fanelli, R.; Bernabini, G.; Scatena, A.; Pizzarelli, F. Post-Dilution on Line Haemodiafiltration with Citrate Dialysate: First Clinical Experience in Chronic Dialysis Patients. Sci. World J. 2013, 1, 703612. [Google Scholar] [CrossRef] [PubMed]
- Dao, M.; Touam, M.; Joly, D.; Mercadal, L. Acetate-Free Bicarbonate Dialysate: Which Acid in the Dialysis Buffer? Nephrol. Ther. 2019, 15 (Suppl. S1), S91–S97. [Google Scholar] [CrossRef]
- Steckiph, D.; Bertucci, A.; Petraulo, M.; Baldini, C.; Calabrese, G.; Gonella, M. Calcium mass balances in on-line hemodiafiltration using citrate-containing acetate-free and regular dialysis concentrates. Abstr. ERA-EDTA Congr. 2013, 7. [Google Scholar]
- Pérez-García, R.; Albalate, M.; Sequera, P.; Ortega, M. El Balance de Calcio Es Menor Con Un Líquido de Diálisis Con Citrato Que Con Acetato. Nefrología 2017, 37, 109–110. [Google Scholar] [CrossRef]
- Ficociello, L.H.; Zhou, M.; Mullon, C.; Anger, M.S.; Kossmann, R.J. Effect of Citrate-Acidified Dialysate on Intact Parathyroid Hormone in Prevalent Hemodialysis Patients: A Matched Retrospective Cohort Study. Int. J. Nephrol. Renovasc. Dis. 2021, 14, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Kuragano, T.; Furuta, M.; Yahiro, M.; Kida, A.; Otaki, Y.; Hasuike, Y.; Matsumoto, A.; Nakanishi, T. Acetate Free Citrate-Containing Dialysate Increase Intact-PTH and BAP Levels in the Patients with Low Intact-PTH. BMC Nephrol. 2013, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.K.; Fleming, L.W. The Effect of Dialysate Magnesium on Plasma and Erythrocyte Magnesium and Potassium Concentrations during Maintenance Haemodialysis. Nephron 1973, 10, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Gonella, M.; Bonaguidi, F.; Buzzigoli, G.; Bartolini, V.; Mariani, G. On the Effect of Magnesium on the PTH Secretion in Uremic Patients on Maintenance Hemodialysis. Nephron 1981, 27, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Zaslow, S.; Oliveira-Paula, G.H.; Chen, W. Magnesium and Vascular Calcification in Chronic Kidney Disease: Current Insights. Int. J. Mol. Sci. 2024, 18, 25–1155. [Google Scholar] [CrossRef]
- Cross, J.; Davenport, A. Does Online Hemodiafiltration Lead to Reduction in Trace Elements and Vitamins? Hemodial. Int. 2011, 15, 509–514. [Google Scholar] [CrossRef]
- Hsu, C.W.; Lin, J.L.; Lin-Tan, D.T.; Yen, T.H.; Huang, W.H.; Ho, T.C.; Huang, Y.L.; Yeh, L.M.; Huang, L.M. Association of Environmental Cadmium Exposure with Inflammation and Malnutrition in Maintenance Haemodialysis Patients. Nephrol. Dial. Transplant. 2009, 24, 1282–1288. [Google Scholar] [CrossRef] [PubMed]
- Kefalas, E.T.; Dakanali, M.; Panagiotidis, P.; Raptopoulou, C.P.; Terzis, A.; Mavromoustakos, T.; Kyrikou, I.; Karligiano, N.; Bino, A.; Salifoglou, A. PH-Specific Aqueous Synthetic Chemistry in the Binary Cadmium(II)-Citrate System. Gaining Insight into Cadmium(II)-Citrate Speciation with Relevance to Cadmium Toxicity. Inorg. Chem. 2005, 44, 4818–4828. [Google Scholar] [CrossRef]
- Rode, S.; Henninot, C.; Vallières, C.; Matlosz, M. Complexation Chemistry in Copper Plating from Citrate Baths. J. Electrochem. Soc. 2004, 151, C405. [Google Scholar] [CrossRef]
- Mattar, G.; Haddarah, A.; Haddad, J.; Pujola, M.; Sepulcre, F. Are Citric Acid-Iron II Complexes True Chelates or Just Physical Mixtures and How to Prove This? Foods 2023, 12, 410. [Google Scholar] [CrossRef] [PubMed]
- Bai, K.; Hong, B.; Hong, Z.; Sun, J.; Wang, C. Selenium Nanoparticles-Loaded Chitosan/Citrate Complex and Its Protection against Oxidative Stress in d-Galactose-Induced Aging Mice. J. Nanobiotechnology 2017, 15, 92. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, C.W. Calcium Balance during Hemodialysis. Semin. Dial. 2008, 21, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Malberti, F.; Ravani, P. The Choice of the Dialysate Calcium Concentration in the Management of Patients on Haemodialysis and Haemodiafiltration. Nephrol. Dial. Transplant. 2003, 18 (Suppl. S7), vii37–vii40. [Google Scholar] [CrossRef]
- Bergström, J.; Wehle, B. No Change in Corrected Β2-Microglobulin Concentration after Cuprophane Haemodialysis. Lancet 1987, 14, 628–629. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Components | SmartBag 211.25 | SmartBag 211.5 | SmartBag CA 211.5 | SmartBag CA 211.5-0.75 |
|---|---|---|---|---|
| Sodium (mmol/L) | 138 | 138 | 138 | 138 |
| Potassium (mmol/L) | 2 | 2 | 2 | 2 |
| Calcium (mmol/mL) | 1.25 | 1.5 | 1.5 | 1.5 |
| Magnesium (mmol/mL) | 0.5 | 0.5 | 0.5 | 0.75 |
| Chloride (mmol/mL) | 108.5 | 109 | 109 | 109.5 |
| Acetate (mmol/L) | 3 | 3 | - | - |
| Citrate (mmol/L) | - | - | 1 | 1 |
| Glucose (g/L) | 1 | 1 | 1 | 1 |
| Bicarbonate (mmol/L) | 32 | 32 | 32 | 32 |
| Osmolarity (mosm/L) | 290.8 | 291.55 | 290 | 290 |
| Variable | SmartBag 211.25 | SmartBag 211.5 | SmartBag CA 211.5 | SmartBag CA 211.5-0.75 | p Value |
|---|---|---|---|---|---|
| Blood flow (mL/min, mean ± SD) | 449 ± 1 | 444 ± 4 | 447 ± 3 | 446 ± 3 | 0.364 |
| Dialysis session (min, mean ± SD) | 284.33 ± 4.31 | 284.5 ± 4.17 | 285.44 ± 4.37 | 285.33 ± 4.08 | 0.152 |
| Total ultrafiltration (L, mean ± SD) | 1.79 ± 0.82 | 1.98 ± 0.7 | 1.97 ± 1.05 | 2.03 ± 0.79 | 0.618 |
| Treated blood volume (L, mean ± SD | 125.13 ± 8 | 126.36 ± 8.16 | 126.26 ± 8.51 | 125.82 ± 9.47 | 0.426 |
| Kt, (n ± SD) | 70.07 ± 6.09 | 70.97 ± 7.19 | 71.64 ± 7.47 | 71.48 ± 6.46 | 0.348 |
| BUN RR (%, mean ± SD) | 84.62 ± 3.08 | 85.23 ± 4 | 85.6 ± 3.04 | 84.79 ± 2.94 | 0.345 |
| Creatinine RR (%, mean ± SD) | 78.05 ± 4.44 | 77.84 ± 4.68 | 78.89 ± 4.23 | 77.9 ± 4.7 | 0.276 |
| Albumin RR (%, mean ± SD) | 8.53 ± 5.84 | 9.54 ± 5.88 | 9.06 ± 6.27 | 10.67 ± 3.88 | 0.228 |
| ΔpH (mean ± SD) | 0.09 ± 0.01 | 0.07 ± 0.02 | 0.07 ± 0.01 | 0.06 ± 0.01 | 0.394 |
| ΔHCO3 (mean ± SD) | 4.89 ± 0.42 | 4.09 ± 0.65 | 4.72 ± 0.45 | 4.58 ± 0.38 | 0.573 |
| ΔTCO2 (mean ± SD) | 4.61 ± 0.47 | 3.78 ± 0.51 | 3.22 ± 0.45 | 3.39 ± 0.36 | 0.051 |
| Replacement volume (L, mean ± SD) | 31.7 ± 4.92 | 31.22 ± 5.8 | 32.05 ± 5.78 | 31.35 ± 5.21 | 0.604 |
| Recirculation (%, mean ± SD) | 17.22 ± 5.7 | 16.56 ± 4.74 | 15.28 ± 4.73 | 15.56 ± 2.85 | 0.187 |
| BVM nadir (kg/m2 mean ± SD) | 90.75 ± 3.47 | 90.55 ± 2.86 | 90.46 ± 4.07 | 90.54 ± 3.51 | 0.988 |
| Pre-dialysis SBP (mmHg, mean ± SD) | 123.7 ± 25.6 | 126.8 ± 27.9 | 120.9 ± 23.5 | 125.9 ± 25.6 | 0.433 |
| Post-dialysis SBP (mmHg, mean ± SD) | 112.1 ± 21.2 | 115.8 ± 16.2 | 106.5 ± 15 | 105.2 ± 13.6 | 0.054 |
| Pre-dialysis DBP (mmHg, mean ± SD) | 60 ± 13.2 | 60 ± 11.3 | 58.3 ± 13.1 | 61.2 ± 11.5 | 0.698 |
| Post-dialysis DBP (mmHg, mean ± SD) | 54.7 ± 10.4 | 56.1 ± 7 | 53.8 ± 10.7 | 53.1 ± 6.8 | 0.54 |
| Variable | SmartBag 211.25 | SmartBag 211.5 | SmartBag CA 211.5 | SmartBag CA 211.5-0.75 | p Value |
|---|---|---|---|---|---|
| Total calcium (mg/dL) | |||||
| Pre-dialysis | 8.44 ± 0.59 | 8.54 ± 0.59 | 8.49 ± 0.56 | 8.55 ± 0.67 | 0.139 |
| Post-dialysis | 8.38 ± 0.4 | 9.71 ± 0.47 | 8.77 ± 0.46 | 8.84 ± 0.41 | <0.001 |
| Variation | −0.07 ± 0.48 | 1.16 ± 0.66 | 0.28 ± 0.51 | 0.29 ± 0.55 | <0.001 |
| Ionized calcium (mmol/L) | |||||
| Pre-dialysis | 1.08 ± 0.09 | 1.08 ± 0.09 | 1.12 ± 0.09 | 1.1 ± 0.09 | 0.114 |
| Post-dialysis | 1.1 ± 0.03 | 1.21 ± 0.06 | 1.01 ± 0.07 | 1.03 ± 0.04 | <0.001 |
| Variation | 0.02 ± 0.08 | 0.13 ± 0.08 | −0.11 ± 0.1 | −0.07 ± 0.09 | <0.001 |
| Parathormone (pg/mL) | |||||
| Pre-dialysis | 244.83 ± 31.83 | 238.44 ± 26.46 | 228.78 ± 27.14 | 229.83 ± 27.21 | 0.785 |
| Post-dialysis | 207.78 ± 44.79 | 74.28 ± 11.93 | 214.28 ± 34.97 | 269.5 ± 43.53 | <0.001 |
| Variation | −37.06 ± 36.96 | −164.17 ± 21.73 | −12.5 ± 26.02 | 39.67 ± 35.55 | <0.001 |
| Phosphorus (mg/dL) | |||||
| Pre-dialysis | 3.86 ± 0.21 | 3.81 ± 0.23 | 3.82 ± 0.21 | 3.85 ± 0.18 | 0.984 |
| Post-dialysis | 1.39 ± 0.06 | 1.53 ± 0.07 | 1.28 ± 0.06 | 1.66 ± 0.33 | 0.424 |
| Variation | −2.47 ± 0.18 | −2.28 ± 2.1 | −2.53 ± 0.18 | −2.19 ± 0.37 | 0.622 |
| Magnesium (mg/dL) | |||||
| Pre-dialysis | 1.97 ± 0.08 | 1.98 ± 0.8 | 1.98 ± 0.08 | 1.99 ± 0.08 | 0.862 |
| Post-dialysis | 1.76 ± 0.02 | 1.77 ± 0.03 | 1.59 ± 0.02 | 2.22 ± 0.02 | <0.001 |
| Variation | −0.21 ± 0.07 | −0.22 ± 0.07 | −0.39 ± 0.07 | 0.23 ± 0.07 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Espinosa, D.; Cuadrado-Payán, E.; Rico, N.; Torra, M.; Fernández, R.M.; Casals, G.; Rodríguez-García, M.; Maduell, F.; Broseta, J.J. Citrate Dialysate with and without Magnesium Supplementation in Hemodiafiltration: A Comparative Study Versus Acetate. Int. J. Mol. Sci. 2024, 25, 8491. https://doi.org/10.3390/ijms25158491
Rodríguez-Espinosa D, Cuadrado-Payán E, Rico N, Torra M, Fernández RM, Casals G, Rodríguez-García M, Maduell F, Broseta JJ. Citrate Dialysate with and without Magnesium Supplementation in Hemodiafiltration: A Comparative Study Versus Acetate. International Journal of Molecular Sciences. 2024; 25(15):8491. https://doi.org/10.3390/ijms25158491
Chicago/Turabian StyleRodríguez-Espinosa, Diana, Elena Cuadrado-Payán, Naira Rico, Mercè Torra, Rosa María Fernández, Gregori Casals, María Rodríguez-García, Francisco Maduell, and José Jesús Broseta. 2024. "Citrate Dialysate with and without Magnesium Supplementation in Hemodiafiltration: A Comparative Study Versus Acetate" International Journal of Molecular Sciences 25, no. 15: 8491. https://doi.org/10.3390/ijms25158491