
Hierarchical Biomaterial Scaffolds for Periodontal Tissue Engineering: Recent Progress and Current Challenges


Abstract
:1. Introduction
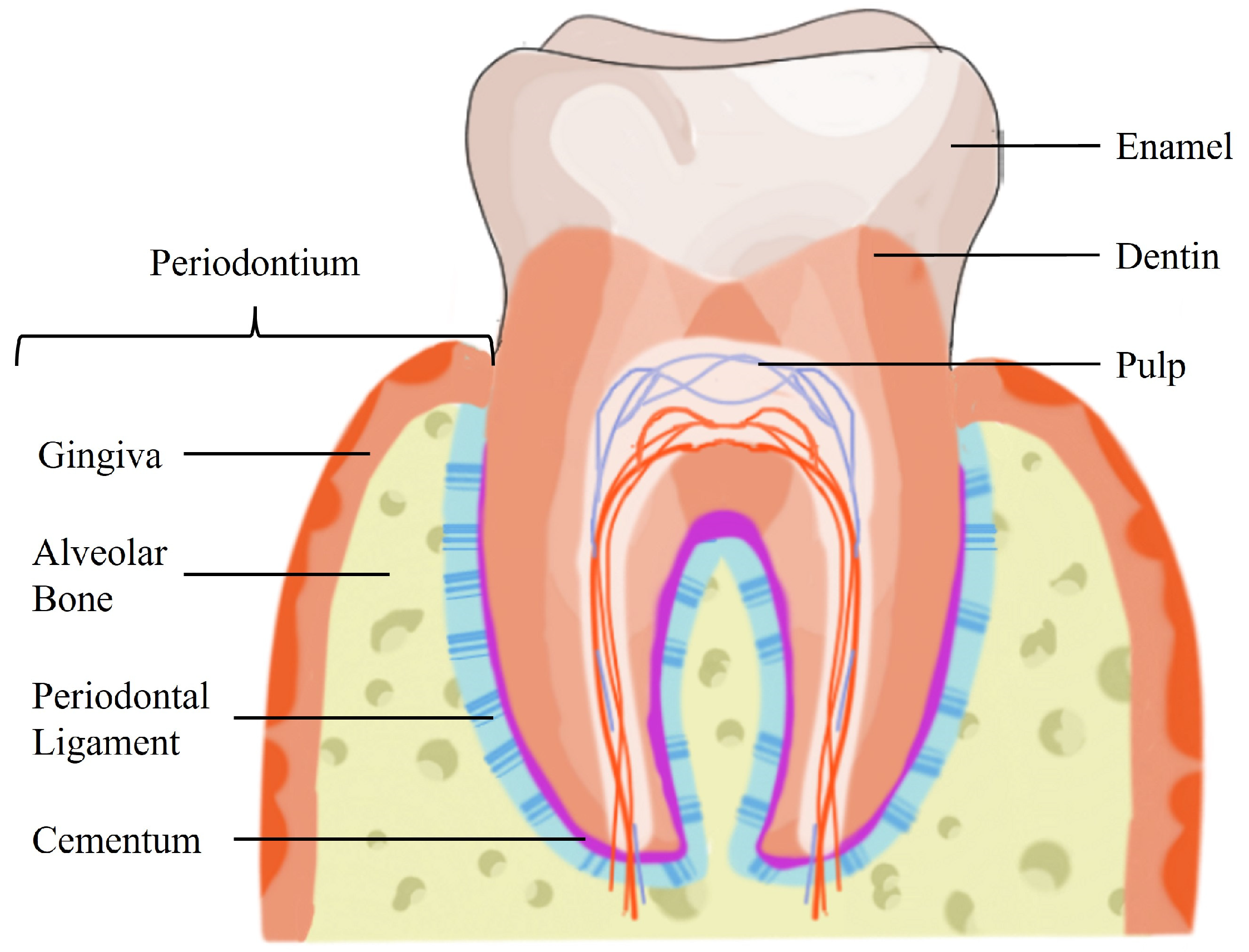
2. Periodontium Hierarchical Structure
3. Limitations of the Current Therapeutic Strategies for Periodontal Regeneration
4. Periodontal Tissue Engineering
5. Hierarchical Scaffolds for Periodontal Tissue Engineering
6. Current Challenges and Future Directions
7. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALP | alkaline phosphatase |
| BMP | bone morphogenetic protein |
| BSA | bovine serum albumin |
| BSP | bone sialoprotein |
| CAD | computer-aided design |
| CaO | calcium oxide |
| CAP | cementum attachment protein |
| CGF | concentrated growth factor |
| CMP1 | cementum protein 1 |
| COL I | type I collagen |
| CTGF | connective tissue growth factor |
| CTS | chitosan |
| DFSCs | dental follicle stem cells |
| ECM | extracellular matrix |
| EMD | enamel matrix derivative |
| FDM | fused deposition modeling |
| FGF | fibroblast growth factor |
| FSP | fibroblast surface protein |
| GCs | gingival cells |
| GelMA | gelatin methacrylate |
| GTR | guided tissue regeneration |
| HAp | hydroxyapatite |
| IMC | intrafibrillar mineralized collagen |
| MgO | magnesium oxide |
| MW | molecular weight |
| NaOH | sodium hydroxide |
| nBGC | nano-bioactive glass ceramic |
| nCSi | nonstoichiometric wollastonite |
| NPs | nanoparticles |
| OC | osteocalcin |
| OPG | osteoprotegerin |
| OPN | osteopontin |
| PCL | polycaprolactone |
| PDGF | platelet-derived growth factors |
| PDL | periodontal ligament |
| PDLCs | periodontal ligament cells |
| PDLSCs | periodontal ligament stromal cells |
| PDMS | polydimethylsiloxane |
| PEG | polyethylene glycol |
| PLA | polylactic acid |
| PLAP1 | periodontal ligament associated protein 1 |
| PLGA | polylactic-co-glycolic acid |
| POSTN | periostin |
| PRP | platelet-rich plasma |
| rBMSCs | rat bone marrow mesenchymal stem/stromal cells |
| rhCMP1 | recombinant human cementum protein 1 |
| RUNX2 | Runt-related transcription factor 2 |
| Si-HPMC | silanized hydroxypropyl methylcellulose |
| Smad3 | Mothers against decapentaplegic homolog 3 |
| Sr | strontium |
| TCP | tricalcium phosphate |
| TE | tissue engineering |
| TGF-β1 | transforming growth factor-β1 |
References
- Nanci, A.; Bosshardt, D.D. Structure of Periodontal Tissues in Health and Disease. Periodontology 2000 2006, 40, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal Diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M.; Seymour, R.A.; Heasman, P.A. Current Concepts in Periodontal Pathogenesis. Dent. Update 2004, 31, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Fu, H.; Li, R.; Li, H.; Wang, S.; Li, B.; Sun, J. A New Direction in Periodontitis Treatment: Biomaterial-Mediated Macrophage Immunotherapy. J. Nanobiotechnol. 2024, 22, 359. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal Diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Leira, Y.; Proença, L.; Chambrone, L.; Mendes, J.J. Economic Burden of Periodontitis in the United States and Europe: An Updated Estimation. J. Periodontol. 2022, 93, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.X.; Zhong, Y.J.; Dong, Q.Q.; Wong, H.M.; Wen, Y.F. Global, Regional, and National Burden of Severe Periodontitis, 1990–2019: An Analysis of the Global Burden of Disease Study 2019. J. Clin. Periodontol. 2021, 48, 1165–1188. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Sculean, A. Current Status of Regenerative Periodontal Treatment. Curr. Oral Health Rep. 2017, 4, 34–43. [Google Scholar] [CrossRef]
- Ivanovski, S. Periodontal Regeneration. Aust. Dent. J. 2009, 54, S118–S128. [Google Scholar] [CrossRef] [PubMed]
- Sufaru, I.-G.; Macovei, G.; Stoleriu, S.; Martu, M.-A.; Luchian, I.; Kappenberg-Nitescu, D.-C.; Solomon, S.M. 3D Printed and Bioprinted Membranes and Scaffolds for the Periodontal Tissue Regeneration: A Narrative Review. Membranes 2022, 12, 902. [Google Scholar] [CrossRef]
- Santos, M.S.; Carvalho, M.S.; Silva, J.C. Recent Advances on Electrospun Nanofibers for Periodontal Regeneration. Nanomaterials 2023, 13, 1307. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.S.; dos Santos, A.B.; Carvalho, M.S. New Insights in Hydrogels for Periodontal Regeneration. J. Funct. Biomater. 2023, 14, 545. [Google Scholar] [CrossRef]
- Fehrenbach, M.J.; Popowics, T. Illustrated Dental Embryology, Histology, and Anatomy; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Cho, M.-I.; Garant, P.R. Development and General Structure of the Periodontium. Periodontology 2000 2000, 24, 9–27. [Google Scholar] [CrossRef]
- Carvalho, M.S.; Cabral, J.M.S.; da Silva, C.L.; Vashishth, D. Bone Matrix Non-Collagenous Proteins in Tissue Engineering: Creating New Bone by Mimicking the Extracellular Matrix. Polymers 2021, 13, 1095. [Google Scholar] [CrossRef]
- Bosshardt, D.D. Are Cementoblasts a Subpopulation of Osteoblasts or a Unique Phenotype? J. Dent. Res. 2005, 84, 390–406. [Google Scholar] [CrossRef] [PubMed]
- de Jong, T.; Bakker, A.D.; Everts, V.; Smit, T.H. The Intricate Anatomy of the Periodontal Ligament and Its Development: Lessons for Periodontal Regeneration. J. Periodontal. Res. 2017, 52, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Andrei, M.; Dinischiotu, A.; Didilescu, A.C.; Ionita, D.; Demetrescu, I. Periodontal Materials and Cell Biology for Guided Tissue and Bone Regeneration. Ann. Anat. Anat. Anz. 2018, 216, 164–169. [Google Scholar] [CrossRef]
- Zhu, L.; Zhou, C.; Chen, S.; Huang, D.; Jiang, Y.; Lan, Y.; Zou, S.; Li, Y. Osteoporosis and Alveolar Bone Health in Periodontitis Niche: A Predisposing Factors-Centered Review. Cells 2022, 11, 3380. [Google Scholar] [CrossRef]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef]
- Nazir, M.A. Prevalence of Periodontal Disease, Its Association with Systemic Diseases and Prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Angelov, N.; Soldatos, N.; Ioannidou, E.; Carter, T.C.; Shimpi, N.; Applegate, J.; Kookal, K.K.; Parsegian, K. A Retrospective Analysis of the Role of Age and Sex in Outcomes of Non-Surgical Periodontal Therapy at a Single Academic Dental Center. Sci. Rep. 2024, 14, 9504. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.Y.; Li, X.; Wang, J.; He, X.T.; Sun, H.H.; Chen, F.M. Concise Review: Periodontal Tissue Regeneration Using Stem Cells: Strategies and Translational Considerations. Stem Cells Transl. Med. 2019, 8, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef] [PubMed]
- Ciszyński, M.; Dominiak, S.; Dominiak, M.; Gedrange, T.; Hadzik, J. Allogenic Bone Graft in Dentistry: A Review of Current Trends and Developments. Int. J. Mol. Sci. 2023, 24, 16598. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, S.; Bernardi, S.; Mattei, A.; Cristiano, L.; Mancini, L.; Torge, D.; Varvara, G.; Macchiarelli, G.; Marchetti, E. Morphological and Biological Evaluations of Human Periodontal Ligament Fibroblasts in Contact with Different Bovine Bone Grafts Treated with Low-Temperature Deproteinisation Protocol. Int. J. Mol. Sci. 2022, 23, 5273. [Google Scholar] [CrossRef] [PubMed]
- Solakoglu, Ö.; Götz, W.; von Baehr, V.; Heydecke, G.; Pantel, K.; Schwarzenbach, H. Characterization of Immunologically Detectable T-Cell Sensitization, Immunohistochemical Detection of pro-Inflammatory Cytokines, and Clinical Parameters of Patients after Allogeneic Intraoral Bone Grafting Procedures: A Prospective Randomized Controlled Clinical Trial in Humans. BMC Oral Health 2022, 22, 592. [Google Scholar] [CrossRef]
- Moraschini, V.; de Almeida, D.C.F.; Calasans-Maia, M.D.; Kischinhevsky, I.C.C.; Louro, R.S.; Granjeiro, J.M. Immunological Response of Allogeneic Bone Grafting: A Systematic Review of Prospective Studies. J. Oral Pathol. Med. 2020, 49, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Bannister, S.R.; Powell, C.A. Foreign Body Reaction to Anorganic Bovine Bone and Autogenous Bone With Platelet-Rich Plasma in Guided Bone Regeneration. J. Periodontol. 2008, 79, 1116–1120. [Google Scholar] [CrossRef] [PubMed]
- Scolozzi, P.; Perez, A.; Verdeja, R.; Courvoisier, D.S.; Lombardi, T. Association between Maxillary Sinus Fungus Ball and Sinus Bone Grafting with Deproteinized Bovine Bone Substitutes: A Case-Control Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, e143–e147. [Google Scholar] [CrossRef]
- Fernandez de Grado, G.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.-M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone Substitutes: A Review of Their Characteristics, Clinical Use, and Perspectives for Large Bone Defects Management. J. Tissue Eng. 2018, 9, 204173141877681. [Google Scholar] [CrossRef]
- Fraser, D.; Caton, J.; Benoit, D.S.W. Periodontal Wound Healing and Regeneration: Insights for Engineering New Therapeutic Approaches. Front. Dent. Med. 2022, 3, 815810. [Google Scholar] [CrossRef]
- Woo, H.N.; Cho, Y.J.; Tarafder, S.; Lee, C.H. The Recent Advances in Scaffolds for Integrated Periodontal Regeneration. Bioact. Mater. 2021, 6, 3328–3342. [Google Scholar] [CrossRef] [PubMed]
- Ramseier, C.A.; Rasperini, G.; Batia, S.; Giannobile, W.v. Advanced Reconstructive Technologies for Periodontal Tissue Repair. Periodontology 2000 2012, 59, 185–202. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Fan, L.; Alkildani, S.; Liu, L.; Emmert, S.; Najman, S.; Rimashevskiy, D.; Schnettler, R.; Jung, O.; Xiong, X.; et al. Barrier Membranes for Guided Bone Regeneration (GBR): A Focus on Recent Advances in Collagen Membranes. Int. J. Mol. Sci. 2022, 23, 14987. [Google Scholar] [CrossRef]
- Liang, Y.; Luan, X.; Liu, X. Recent Advances in Periodontal Regeneration: A Biomaterial Perspective. Bioact. Mater. 2020, 5, 297–308. [Google Scholar] [CrossRef]
- Soldatos, N.K.; Stylianou, P.; Koidou, V.P.; Angelov, N.; Yukna, R.; Romanos, G.E. Limitations and Options Using Resorbable versus Nonresorbable Membranes for Successful Guided Bone Regeneration. Quintessence Int. 2017, 48, 131–147. [Google Scholar] [CrossRef]
- Park, C.H.; Kim, K.H.; Lee, Y.M.; Seol, Y.J. Advanced Engineering Strategies for Periodontal Complex Regeneration. Materials 2016, 9, 57. [Google Scholar] [CrossRef]
- Christgau, M.; Bader, N.; Schmalz, G.; Hiller, K.-A.; Wenzel, A. Postoperative exposure of bioresorbable GTR membranes: Effect on healing results. Clin. Oral Investig. 1997, 1, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wang, S.; Shi, B.; Wang, Y.; Chen, Y.; Wang, X.; Lee, E.-S.; Jiang, H.-B. Advances in Modification Methods Based on Biodegradable Membranes in Guided Bone/Tissue Regeneration: A Review. Polymers 2022, 14, 871. [Google Scholar] [CrossRef]
- Hassan, S.U.; Bilal, B.; Nazir, M.S.; Naqvi, S.A.R.; Ali, Z.; Nadeem, S.; Muhammad, N.; Palvasha, B.A.; Mohyuddin, A. Recent progress in materials development and biological properties of GTR membranes for periodontal regeneration. Chem. Biol. Drug Des. 2021, 98, 1007–1024. [Google Scholar] [CrossRef]
- Wang, H.H.; Sarmast, N.D.; Shadmehr, E.; Angelov, N.; Shabahang, S.; Torabinejad, M. Application of Enamel Matrix Derivative (Emdogain) in Endodontic Therapy: A Comprehensive Literature Review. J. Endod. 2018, 44, 1066–1079. [Google Scholar] [CrossRef]
- de Ry, S.P.; Roccuzzo, A.; Lang, N.P.; Sculean, A.; Salvi, G.E. Long-Term Clinical Outcomes of Periodontal Regeneration with Enamel Matrix Derivative: A Retrospective Cohort Study with a Mean Follow-up of 10 Years. J. Periodontol. 2021, 93, 548–559. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.; Papanikolaou, N.; Coulthard, P.; Worthington, H. Enamel Matrix Derivative (Emdogain®) for Periodontal Tissue Regeneration in Intrabony Defects. Aust. Dent. J. 2010, 55, 101–104. [Google Scholar] [CrossRef]
- Gulameabasse, S.; Gindraux, F.; Catros, S.; Fricain, J.; Fenelon, M. Chorion and Amnion/Chorion Membranes in Oral and Periodontal Surgery: A Systematic Review. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 1216–1229. [Google Scholar] [CrossRef]
- Miron, R.J. Optimized Bone Grafting. Periodontology 2000 2024, 94, 143–160. [Google Scholar] [CrossRef]
- Vaquette, C.; Pilipchuk, S.P.; Bartold, P.M.; Hutmacher, D.W.; Giannobile, W.V.; Ivanovski, S. Tissue Engineered Constructs for Periodontal Regeneration: Current Status and Future Perspectives. Adv. Healthc. Mater. 2018, 7, e1800457. [Google Scholar] [CrossRef]
- Galli, M.; Yao, Y.; Giannobile, W.V.; Wang, H.-L. Current and Future Trends in Periodontal Tissue Engineering and Bone Regeneration. Plast. Aesthet. Res. 2021, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Keshvardoostchokami, M.; Majidi, S.S.; Huo, P.; Ramachandran, R.; Chen, M.; Liu, B. Electrospun Nanofibers of Natural and Synthetic Polymers as Artificial Extracellular Matrix for Tissue Engineering. Nanomaterials 2021, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Chen, X.; Bai, S.; Li, B.; Liu, H.; Wu, G.; Liu, S. Fabrication of Gelatin Methacrylate/Nanohydroxyapatite Microgel Arrays for Periodontal Tissue Regeneration. Int. J. Nanomed. 2016, 11, 4707–4718. [Google Scholar] [CrossRef]
- Tanongpitchayes, K.; Randorn, C.; Lamkhao, S.; Chokethawai, K.; Rujijanagul, G.; Na Lampang, K.; Somrup, L.; Boonyapakorn, C.; Thongkorn, K. Effectiveness of a Nanohydroxyapatite-Based Hydrogel on Alveolar Bone Regeneration in Post-Extraction Sockets of Dogs with Naturally Occurring Periodontitis. Vet. Sci. 2022, 9, 7. [Google Scholar] [CrossRef]
- Dieterle, M.P.; Steinberg, T.; Tomakidi, P.; Nohava, J.; Vach, K.; Schulz, S.D.; Hellwig, E.; Proksch, S. Novel In Situ-Cross-Linked Electrospun Gelatin/Hydroxyapatite Nonwoven Scaffolds Prove Suitable for Periodontal Tissue Engineering. Pharmaceutics 2022, 14, 1286. [Google Scholar] [CrossRef] [PubMed]
- Abdelrasoul, M.; El-Fattah, A.A.; Kotry, G.; Ramadan, O.; Essawy, M.; Kamaldin, J.; Kandil, S. Regeneration of critical-sized grade II furcation using a novel injectable melatonin-loaded scaffold. Oral Dis. 2023, 29, 3583–3598. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Zhang, X.; Meng, S.; Dai, X.; Han, B.; Deng, X. Enhanced Critical Size Defect Repair in Rabbit Mandible by Electrospun Gelatin/β-TCP Composite Nanofibrous Membranes. J. Nanomater. 2015, 2015, 396916. [Google Scholar] [CrossRef]
- Al-allaq, A.A.; Kashan, J.S. A Review: In Vivo Studies of Bioceramics as Bone Substitute Materials. Nano Sel. 2023, 4, 123–144. [Google Scholar] [CrossRef]
- Tan, J.; Zhang, M.; Hai, Z.; Wu, C.; Lin, J.; Kuang, W.; Tang, H.; Huang, Y.; Chen, X.; Liang, G. Sustained Release of Two Bioactive Factors from Supramolecular Hydrogel Promotes Periodontal Bone Regeneration. ACS Nano 2019, 13, 5616–5622. [Google Scholar] [CrossRef] [PubMed]
- Divband, B.; Aghazadeh, M.; Al-qaim, Z.H.; Samiei, M.; Hussein, F.H.; Shaabani, A.; Shahi, S.; Sedghi, R. Bioactive Chitosan Biguanidine-Based Injectable Hydrogels as a Novel BMP-2 and VEGF Carrier for Osteogenesis of Dental Pulp Stem Cells. Carbohydr. Polym. 2021, 273, 118589. [Google Scholar] [CrossRef] [PubMed]
- Zang, S.; Mu, R.; Chen, F.; Wei, X.; Zhu, L.; Han, B.; Yu, H.; Bi, B.; Chen, B.; Wang, Q.; et al. Injectable Chitosan/β-Glycerophosphate Hydrogels with Sustained Release of BMP-7 and Ornidazole in Periodontal Wound Healing of Class III Furcation Defects. Mater. Sci. Eng. C 2019, 99, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Liu, Y.; Miao, L.; Wang, Y.; Ren, S.; Yang, X.; Hu, Y.; Sun, W. Controlled Release of Recombinant Human Cementum Protein 1 from Electrospun Multiphasic Scaffold for Cementum Regeneration. Int. J. Nanomed. 2016, 11, 3145–3158. [Google Scholar] [CrossRef]
- Sato, Y.; Kikuchi, M.; Ohata, N.; Tamura, M.; Kuboki, Y. Enhanced Cementum Formation in Experimentally Induced Cementum Defects of the Root Surface with the Application of Recombinant Basic Fibroblast Growth Factor in Collagen Gel In Vivo. J. Periodontol. 2004, 75, 243–248. [Google Scholar] [CrossRef]
- Jiang, L.; Ding, Z.; Xia, S.; Liu, Y.; Lei, S.; Zhong, M.; Chen, X. Poly Lactic-Co-Glycolic Acid Scaffold Loaded with Plasmid DNA Encoding Fibroblast Growth Factor-2 Promotes Periodontal Ligament Regeneration of Replanted Teeth. J. Periodontal Res. 2020, 55, 488–495. [Google Scholar] [CrossRef]
- Galarraga-Vinueza, M.E.; Barootchi, S.; Nevins, M.L.; Nevins, M.; Miron, R.J.; Tavelli, L. Twenty-five Years of Recombinant Human Growth Factors RhPDGF-BB and RhBMP-2 in Oral Hard and Soft Tissue Regeneration. Periodontology 2000 2024, 94, 483–509. [Google Scholar] [CrossRef] [PubMed]
- Ammar, M.M.; Waly, G.H.; Saniour, S.H.; Moussa, T.A. Growth Factor Release and Enhanced Encapsulated Periodontal Stem Cells Viability by Freeze-Dried Platelet Concentrate Loaded Thermo-Sensitive Hydrogel for Periodontal Regeneration. Saudi Dent. J. 2018, 30, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Iviglia, G.; Kargozar, S.; Baino, F. Biomaterials, Current Strategies, and Novel Nano-Technological Approaches for Periodontal Regeneration. J. Funct. Biomater. 2019, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.Y.; Ning, Y.; Huang, X. Advanced Technologies in Periodontal Tissue Regeneration Based on Stem Cells: Current Status and Future Perspectives. J. Dent. Sci. 2021, 16, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Deng, J.; Yu, L.; Wang, Y.; Zhang, W.; Han, X.; Camargo, P.H.C.; Wang, J.; Liu, Y. Investigating the Repair of Alveolar Bone Defects by Gelatin Methacrylate Hydrogels-Encapsulated Human Periodontal Ligament Stem Cells. J. Mater. Sci. Mater. Med. 2019, 31, 3. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Ji, Y.; Zhong, T.; Wan, W.; Yang, Q.; Li, A.; Zhang, X.; Lin, M. Bioprinting-Based PDLSC-ECM Screening for in Vivo Repair of Alveolar Bone Defect Using Cell-Laden, Injectable and Photocrosslinkable Hydrogels. ACS Biomater. Sci. Eng. 2017, 3, 3534–3545. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Bertl, K.; Spineli, L.M.; Sculean, A.; Cortellini, P.; Tonetti, M. Medium- and Long-Term Clinical Benefits of Periodontal Regenerative/Reconstructive Procedures in Intrabony Defects: Systematic Review and Network Meta-Analysis of Randomized Controlled Clinical Studies. J. Clin. Periodontol. 2021, 48, 410–430. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Ruan, J.; Weir, M.D.; Ren, K.; Schneider, A.; Wang, P.; Oates, T.W.; Chang, X.; Xu, H.H.K. Periodontal Bone-Ligament-Cementum Regeneration via Scaffolds and Stem Cells. Cells 2019, 8, 537. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, M.N.; Sowmya, S.; Deepthi, S.; Bumgardener, J.D.; Jayakumar, R. Bilayered Construct for Simultaneous Regeneration of Alveolar Bone and Periodontal Ligament. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 761–770. [Google Scholar] [CrossRef]
- Khadre, A.; Raif, E.L.; Junaid, S.; Goudouri, O.M.; Refaat, W.; Ramadan, A.; Boccaccini, A.R.; El-Gendy, R. A Bilayered Tissue Engineered in Vitro Model simulating the Tooth Periodontium. Eur. Cells Mater. 2021, 41, 232–245. [Google Scholar] [CrossRef]
- Wei, Y.; Wang, Z.; Han, J.; Jiang, X.; Lei, L.; Yang, X.; Sun, W.; Gou, Z.; Chen, L. Modularized Bioceramic Scaffold/Hydrogel Membrane Hierarchical Architecture Beneficial for Periodontal Tissue Regeneration in Dogs. Biomater. Res. 2022, 26, 68. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zou, Q.; Wang, C.; Lin, M.; Li, Y.; Zhang, R.; Li, Y. Electrospinning and 3D Printed Hybrid Bi-Layer Scaffold for Guided Bone Regeneration. Mater. Des. 2021, 210, 110047. [Google Scholar] [CrossRef]
- Yu, M.; Luo, D.; Qiao, J.; Guo, J.; He, D.; Jin, S.; Tang, L.; Wang, Y.; Shi, X.; Mao, J.; et al. A Hierarchical Bilayer Architecture for Complex Tissue Regeneration. Bioact. Mater. 2022, 10, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Pilipchuk, S.P.; Monje, A.; Jiao, Y.; Hao, J.; Kruger, L.; Flanagan, C.L.; Hollister, S.J.; Giannobile, W.V. Integration of 3D Printed and Micropatterned Polycaprolactone Scaffolds for Guidance of Oriented Collagenous Tissue Formation In Vivo. Adv. Healthc. Mater. 2016, 5, 676–687. [Google Scholar] [CrossRef] [PubMed]
- Vaquette, C.; Fan, W.; Xiao, Y.; Hamlet, S.; Hutmacher, D.W.; Ivanovski, S. A Biphasic Scaffold Design Combined with Cell Sheet Technology for Simultaneous Regeneration of Alveolar Bone/Periodontal Ligament Complex. Biomaterials 2012, 33, 5560–5573. [Google Scholar] [CrossRef]
- Costa, P.F.; Vaquette, C.; Zhang, Q.; Reis, R.L.; Ivanovski, S.; Hutmacher, D.W. Advanced Tissue Engineering Scaffold Design for Regeneration of the Complex Hierarchical Periodontal Structure. J. Clin. Periodontol. 2014, 41, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Vaquette, C.; Saifzadeh, S.; Farag, A.; Hutmacher, D.W.; Ivanovski, S. Periodontal Tissue Engineering with a Multiphasic Construct and Cell Sheets. J. Dent. Res. 2019, 98, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Farag, A.; Abdal-hay, A.; Han, P.; Ivanovski, S. Fabrication of 3D Melt Electrowritting Multiphasic Scaffold with Bioactive and Osteoconductivite Functionalities for Periodontal Regeneration. Ceram. Int. 2023, 49, 8015–8021. [Google Scholar] [CrossRef]
- Jiang, W.; Li, L.; Zhang, D.; Huang, S.; Jing, Z.; Wu, Y.; Zhao, Z.; Zhao, L.; Zhou, S. Incorporation of Aligned PCL-PEG Nanofibers into Porous Chitosan Scaffolds Improved the Orientation of Collagen Fibers in Regenerated Periodontium. Acta Biomater. 2015, 25, 240–252. [Google Scholar] [CrossRef]
- Yang, M.; Gao, X.; Shen, Z.; Shi, X.; Lin, Z. Gelatin-Assisted Conglutination of Aligned Polycaprolactone Nanofilms into a Multilayered Fibre-Guiding Scaffold for Periodontal Ligament Regeneration. RSC Adv. 2019, 9, 507–518. [Google Scholar] [CrossRef]
- Yao, Y.; Raymond, J.E.; Kauffmann, F.; Maekawa, S.; Sugai, J.V.; Lahann, J.; Giannobile, W.V. Multicompartmental Scaffolds for Coordinated Periodontal Tissue Engineering. J. Dent. Res. 2022, 101, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Varoni, E.M.; Vijayakumar, S.; Canciani, E.; Cochis, A.; Nardo, L.D.; Lodi, G.; Rimondini, L.; Cerruti, M. Chitosan-Based Trilayer Scaffold for Multitissue Periodontal Regeneration. J. Dent. Res. 2018, 97, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Porta, M.; Tonda-Turo, C.; Pierantozzi, D.; Ciardelli, G.; Mancuso, E. Towards 3D Multi-Layer Scaffolds for Periodontal Tissue Engineering Applications: Addressing Manufacturing and Architectural Challenges. Polymers 2020, 12, 2233. [Google Scholar] [CrossRef] [PubMed]
- Sowmya, S.; Mony, U.; Jayachandran, P.; Reshma, S.; Kumar, R.A.; Arzate, H.; Nair, S.V.; Jayakumar, R. Tri-Layered Nanocomposite Hydrogel Scaffold for the Concurrent Regeneration of Cementum, Periodontal Ligament, and Alveolar Bone. Adv. Healthc. Mater. 2017, 6, 1601251. [Google Scholar] [CrossRef] [PubMed]
- Hua, W.; Xiang, J.; Wu, Y.; Yang, W.; Zhao, L. Growth Factor-Encapsulated Triphasic Scaffolds of Electrospun Polylactic Acid–Polycaprolactone (PLA–PCL) Nanofibrous Mats Combined with a Directionally Freeze-Dried Chitosan Hydrogel for Periodontal Tissue Regeneration. Mater. Adv. 2023, 4, 4798–4811. [Google Scholar] [CrossRef]
- Woodruff, M.A.; Hutmacher, D.W. The Return of a Forgotten Polymer—Polycaprolactone in the 21st Century. Prog. Polym. Sci. 2010, 35, 1217–1256. [Google Scholar] [CrossRef]
- Zhang, Y.; Dou, X.; Zhang, L.; Wang, H.; Zhang, T.; Bai, R.; Sun, Q.; Wang, X.; Yu, T.; Wu, D.; et al. Facile Fabrication of a Biocompatible Composite Gel with Sustained Release of Aspirin for Bone Regeneration. Bioact. Mater. 2022, 11, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Babo, P.S.; Cai, X.; Plachokova, A.S.; Reis, R.L.; Jansen, J.; Gomes, M.E.; Walboomers, X.F. Evaluation of a Platelet Lysate Bilayered System for Periodontal Regeneration in a Rat Intrabony Three-wall Periodontal Defect. J. Tissue Eng. Regen. Med. 2018, 12, e1277–e1288. [Google Scholar] [CrossRef] [PubMed]
- Castilho, M.; de Ruijter, M.; Beirne, S.; Villette, C.C.; Ito, K.; Wallace, G.G.; Malda, J. Multitechnology Biofabrication: A New Approach for the Manufacturing of Functional Tissue Structures? Trends Biotechnol. 2020, 38, 1316–1328. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Kang, M.S.; Eltohamy, M.; Kim, T.-H.; Kim, H.-W. Dynamic Mechanical and Nanofibrous Topological Combinatory Cues Designed for Periodontal Ligament Engineering. PLoS ONE 2016, 11, e0149967. [Google Scholar] [CrossRef]
- Roato, I.; Masante, B.; Putame, G.; Massai, D.; Mussano, F. Challenges of Periodontal Tissue Engineering: Increasing Biomimicry through 3D Printing and Controlled Dynamic Environment. Nanomaterials 2022, 12, 3878. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Composition and Fabrication | Main Results | Year, [Ref] |
|---|---|---|
| CTS/calcium sulfate hydrogel prepared via NaOH neutralization (for alveolar bone regeneration). PCL electrospun membrane (for PDL regeneration). | In vitro: Osteogenic differentiation of human DFSCs on the hydrogel showed maximum ALP activity on day seven. Fibroblastic differentiation of human DFSCs on the membrane confirmed by the expression of PLAP1 and COL I proteins. | 2016, [70] |
| Scaffold composed of Silica, CaO, and MgO, fabricated via a sol–gel technique combined with foam replica method and coated with gelatin and genipin (for alveolar bone regeneration). Bio-Gide® collagen membrane (for PDL regeneration) | In vitro: Human PDLCs cultured on a sol–gel scaffold showed increased gene expression of COL I and OPG compared to cells cultured on well plates and on the Bio-Gide® membrane. Cell viability and growth were maintained in both individual layers and in the bilayered construct. | 2021, [71] |
| nCSi scaffold fabricated via digital light processing (for alveolar bone regeneration). GelMA/Si-HPMC barrier membrane produced via photo-crosslinked hydrogel injection. A barrier membrane was placed on top of the nCSi scaffold (for PDL regeneration) | In vitro: Mouse mandible-derived osteoblasts cultured with hydrogel solution showed higher migration to the scratch area, increased ALP expression, and calcium deposition. In vivo: Scaffolds were implanted in the dog’s one-wall intrabony periodontal defects. Biphasic scaffolds showed significantly more newly formed bone volume and higher trabecular number than the nCSi scaffold. Scaffolds were fully biodegraded at 8 weeks. Scaffolds paired WITH a barrier membrane resulted in a longer distance to the junctional epithelium and more newly formed PDL. | 2022, [72] |
| PCL/gelatin scaffold with HAp NPs (PGH) fabricated via extrusion printing (for alveolar bone regeneration). PCL/gelatin electrospun membrane with heparin (for PDL regeneration). | In vitro: PGH scaffold showed enhanced proliferation of rBMSCs compared to pure PCL scaffolds. HAp NPs resulted in increased gene expressions of RUNX2, COL I, and BMP-2 in rBMSCs. Heparin increased L929 fibroblast viability and proliferation. In vivo: Scaffolds were implanted in the rabbit osteochondral defect model. The biphasic scaffold showed more newly formed bone compared to the PGH scaffold only. | 2021, [73] |
| Intrafibrillar mineralized collagen (IMC) scaffold fabricated via self-assembly (for alveolar bone regeneration). The CGF/collagen mixture was coated on microstamping models produced via photolithography, to obtain parallel-aligned arrays (for PDL regeneration). CGF arrays were imprinted on the IMC scaffold, and the biphasic construct was lyophilized. | In vitro: Human PDLCs cultured on IMC scaffold showed RUNX2 and OPN upregulated gene expressions and decreased expression of Elastin. Parallel CGF arrays resulted in increased gene expressions of POSTN and Elastin and decreased expressions of RUNX2 and OPN. In vivo: Scaffolds were implanted in rat periodontal defect and also subcutaneously in rats. The biphasic scaffold showed significantly more newly formed bone volume and thickness, as well as TGF-β1 and Smad3 expressions compared to the monophasic CGF scaffold and a non-hierarchical control composed of CGF and deproteinized bovine bone mineral. Subcutaneous implantation demonstrated that BMP-2+ and COL I+ cells were more abundant in the biphasic scaffold. | 2022, [74] |
| PCL and HAp scaffold fabricated via selective laser sintering and seeded with BMP7 expressing GCs (for alveolar bone regeneration). PCL films fabricated through spin coating onto PDMS micropatterned via soft lithography and seeded with PDLCs (for PDL regeneration). | In vitro: Patterned films promoted PDLC elongation along the grooves. Nonpatterned films showed randomly oriented cells. In vivo: Scaffolds were press-fitted with a dentin chip and then subcutaneously implanted in rats. Scaffolds with micropatterned films showed increased tissue alignment, with enhanced oriented collagen fiber thickness, cell alignment, and nuclear elongation perpendicular to the dentin segment. | 2016, [75] |
| PCL scaffold with β-TCP fabricated using fused deposition modeling and seeded with osteoblasts (for alveolar bone regeneration). PCL membrane produced via solution electrospinning and with 3 PDL cell sheets superimposed (for PDL regeneration). | In vitro: The bone compartment promoted the growth of osteoblasts and was highly filled with cells after 21 days. In vivo: Scaffolds were assembled on top of a dentin slice and then subcutaneously implanted in rats. Scaffolds seeded with osteoblasts showed more intense ALP staining and higher bone density. Scaffolds combined with cell sheets demonstrated better attachment to the dentin surface and deposition of cementum-like tissue. | 2012, [76] |
| PCL scaffold with β-TCP fabricated using fused deposition modeling, coated with calcium phosphate, and seeded with osteoblasts (for alveolar bone regeneration). PCL membrane produced via melt electrospinning and with 3 PDL cell sheets superimposed (for PDL regeneration). | In vitro: Calcium phosphate coating significantly increased ALP activity and enhanced the mineralization of osteoblasts. In vivo: Scaffolds were assembled on top of a dentin slice and then subcutaneously implanted in rats. Calcium phosphate-coated scaffolds showed significantly more bone formation. Blood vessels penetrated the biphasic scaffold. Cell sheets facilitated attachment and oblique orientation of the tissue to the dentin block. | 2014, [77] |
| PCL scaffold produced via melt electrospinning (for alveolar bone regeneration). PCL membrane is produced via solution electrospinning and combined with a cell sheet of PDLCs, GCs, or BMSCs (for PDL regeneration). | In vivo: Scaffolds with PDLC or BMSC cell sheets showed increased cementum coverage between weeks 5 and 10 after implantation in sheep periodontal defect. Scaffolds with GC cell sheets resulted in inferior periodontal regeneration compared to the other groups. All scaffolds promoted new cementum and bone formation, and oblique PDL fiber insertion. | 2019, [78] |
| PCL scaffold produced via melt electrowriting, coated with calcium phosphate (for alveolar bone regeneration) and with a PDL cell sheet superimposed (for PDL regeneration). | In vitro: Calcium phosphate coating stimulated the synthesis of bone matrix by osteoblasts. Scaffolds retained functional extracellular matrix after decellularization. | 2023, [79] |
| Composition and Fabrication | Main Results | Year, [Ref] |
|---|---|---|
| Multilayered CTS scaffold with embedded PCL/PEG-aligned electrospun fibers for PDL regeneration. Electrospinning and stacking of 30 layers of fibrous mats in CTS solution, followed by genipin crosslinking and lyophilization. | In vitro: Aligned fibers promoted oriented arrangement and elongation of rBMSCs, increased cell viability, and periodontal ligament-related gene expression (POSTN and COL I) compared to non-aligned fibers. In vivo: Scaffolds were implanted in rat periodontal fenestration defect followed by filling of the alveolar defect with bone graft Bio-Oss®. Scaffolds with aligned fibers showed higher expression of POSTN, higher collagen I/III ratio, and formation of oriented PDL-like fibers in the regenerated periodontium. | 2015, [80] |
| Multilayered gelatin scaffold with embedded PCL-aligned electrospun fibers for PDL regeneration. Electrospinning and stacking of 20 layers of fibrous mats in gelatin solution, followed by genipin crosslinking and lyophilization. | In vitro: PDLSCs elongated along the alignment direction of the aligned PCL fibers. In vivo: Scaffolds were implanted in rat periodontal fenestration defect. Scaffolds with aligned fibers showed higher expression of POSTN and formation of newly oriented PDL fibers with angulation similar to natural PDL. | 2019, [81] |
| Tricompartmental PCL scaffold with 50 layers produced via melt electrowriting for alveolar bone and PDL regeneration: Compartment with 10 layers, 250 µm filament spacing, and 90° layer-to-layer rotation for alveolar bone regeneration. Compartment with 30 layers, 500 µm filament spacing, and 90° layer-to-layer rotation as a transition region between bone and PDL compartments. Compartment with 10 layers, 500 µm filament spacing, and 0° layer-to-layer rotation for PDL regeneration. | In vitro: Bone compartment promoted the attachment and growth of murine pre-osteoblast cells compared to monolithic scaffold consisting of only transition region. PDL compartment facilitated the alignment of PDLCs and the orientation and formation of collagen-enriched fibers (COL I). Human calvarial osteoblasts and PDLCs were seeded in the respective compartments of the tri-compartmental scaffold, which promoted cellular and calcium distributions. The bone compartment showed increased calcium deposition compared to the PDL compartment. The transition region presented cell penetration and ligamentous insertions. | 2022, [82] |
| Tricompartmental scaffold for alveolar bone, PDL, and gingiva interface regeneration: Medium MW CTS scaffold produced via genipin-induced gelation and seeded with osteoblasts for alveolar bone regeneration. Low MW CTS scaffold produced via genipin-induced gelation and seeded with GCs for the gingival interface. Medium MW CTS micro-channeled scaffold produced via electrochemical deposition and seeded with PDLCs for PDL regeneration. | In vitro: Cells seeded in their respective compartment showed similar viability and ALP activity compared to the control polystyrene surfaces. In vivo: Scaffolds were assembled on top of a dentin slice and then subcutaneously implanted in rats. Scaffolds showed high biocompatibility, tissue ingrowth, and vascularization. Cell-laden scaffolds resulted in the formation of a thin layer of mineralized tissue at the dentin interface. | 2018, [83] |
| Tricompartmental PCL scaffold with 14 layers fabricated via melt extrusion for alveolar bone, PDL, and cementum regeneration: Compartment with 6 layers and high Sr-doped nano HAp (Sr-nHAp) content (20% w/w) for alveolar bone regeneration. Compartment with 3 layers, 20% w/w Sr-nHAp, and reduced strand distance for PDL regeneration. Compartment with 5 layers and low Sr-doped HAp content (10% w/w) for cementum regeneration. | In vitro: Scaffolds sustained the proliferation of osteosarcoma U2OS cells. Scaffolds with and without Sr-nHAp content showed increased ALP activity up to day 21 and decreased thereafter. Scaffolds with Sr-nHAp content showed greater mineralization than PCL scaffolds. | 2020, [84] |
| Trilayered scaffold for alveolar bone, PDL, and cementum regeneration: Chitin/PLGA hydrogel with nBGC and PRP for alveolar bone regeneration. Chitin/PLGA hydrogel with rhFGF2 for PDL regeneration. Chitin/PLGA hydrogel with nBGC and rhCMP1 for cementum regeneration. The trilayered scaffold was assembled and lyophilized. | In vitro: Human DFSCs cultured in each hydrogel layer showed similar protein expression to hydrogels without additives in induction media. The presence of the additives CMP1, PRP, and FGF-2 resulted in improved cementogenic (CMP1, BSP), osteogenic (RUNX2, OC), and fibrogenic (FSP, PLAP1) differentiation, respectively. In vivo: Scaffolds were implanted in rabbit maxillary periodontal defects. Defects treated with trilayered scaffold containing additives showed complete closure and healing, formation of new cementum, fibrous PDL, and alveolar bone with well-defined bony trabeculae. | 2017, [85] |
| Tricompartmental scaffold for alveolar bone, PDL, and cementum regeneration: The compartment was composed of 4 layers of PLA/PCL electrospun fibers with BMP-2-loaded CTS-BSA NPs, stacked in CTS/genipin solution (for alveolar bone regeneration). The compartment was produced using CTS/genipin solution with CTGF-loaded CTS-BSA NPs, poured on top of the bone compartment followed by crosslinking of both compartments (for PDL regeneration). The compartment was composed of 2 layers of PLA/PCL electrospun fibers with rhCMP1-loaded CTS-BSA NPs, stacked in CTS/genipin solution, followed by crosslinking and superimposition on the PDL compartment (for cementum regeneration). Triphasic scaffolds were then crosslinked and lyophilized. | In vitro: Triphasic scaffold promoted the proliferation of human PDLCs compared to porous CTS blank scaffolds. PDLCs cultured on the bone compartment showed significant upregulation of osteogenic genes (RUNX2, ALP, and POSTN). The PDL compartment led to a significant increase in the expression of the Scleraxis gene and also of POSTN, although less upregulated than in the bone compartment. When cultured in the cementum compartment, PDLCs showed upregulation of CAP and CMP1 genes. In vivo: Scaffolds were implanted in rat periodontal defect. Triphasic scaffold with growth factors showed significantly higher newly formed bone volume and angulation of newly formed PDL fibers similar to natural PDL, in comparison to triphasic scaffold without growth factors and monophasic CTS blank scaffold. Deposition of cementum-like tissue around the root surface was observed. | 2023, [86] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, M.S.; Silva, J.C.; Carvalho, M.S. Hierarchical Biomaterial Scaffolds for Periodontal Tissue Engineering: Recent Progress and Current Challenges. Int. J. Mol. Sci. 2024, 25, 8562. https://doi.org/10.3390/ijms25168562
Santos MS, Silva JC, Carvalho MS. Hierarchical Biomaterial Scaffolds for Periodontal Tissue Engineering: Recent Progress and Current Challenges. International Journal of Molecular Sciences. 2024; 25(16):8562. https://doi.org/10.3390/ijms25168562
Chicago/Turabian StyleSantos, Mafalda S., João C. Silva, and Marta S. Carvalho. 2024. "Hierarchical Biomaterial Scaffolds for Periodontal Tissue Engineering: Recent Progress and Current Challenges" International Journal of Molecular Sciences 25, no. 16: 8562. https://doi.org/10.3390/ijms25168562