

The Prognostic and Predictive Utility of CDX2 in Colorectal Cancer
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Study Population
2.2. Association of CDX2 Staining with Clinicopathological Features
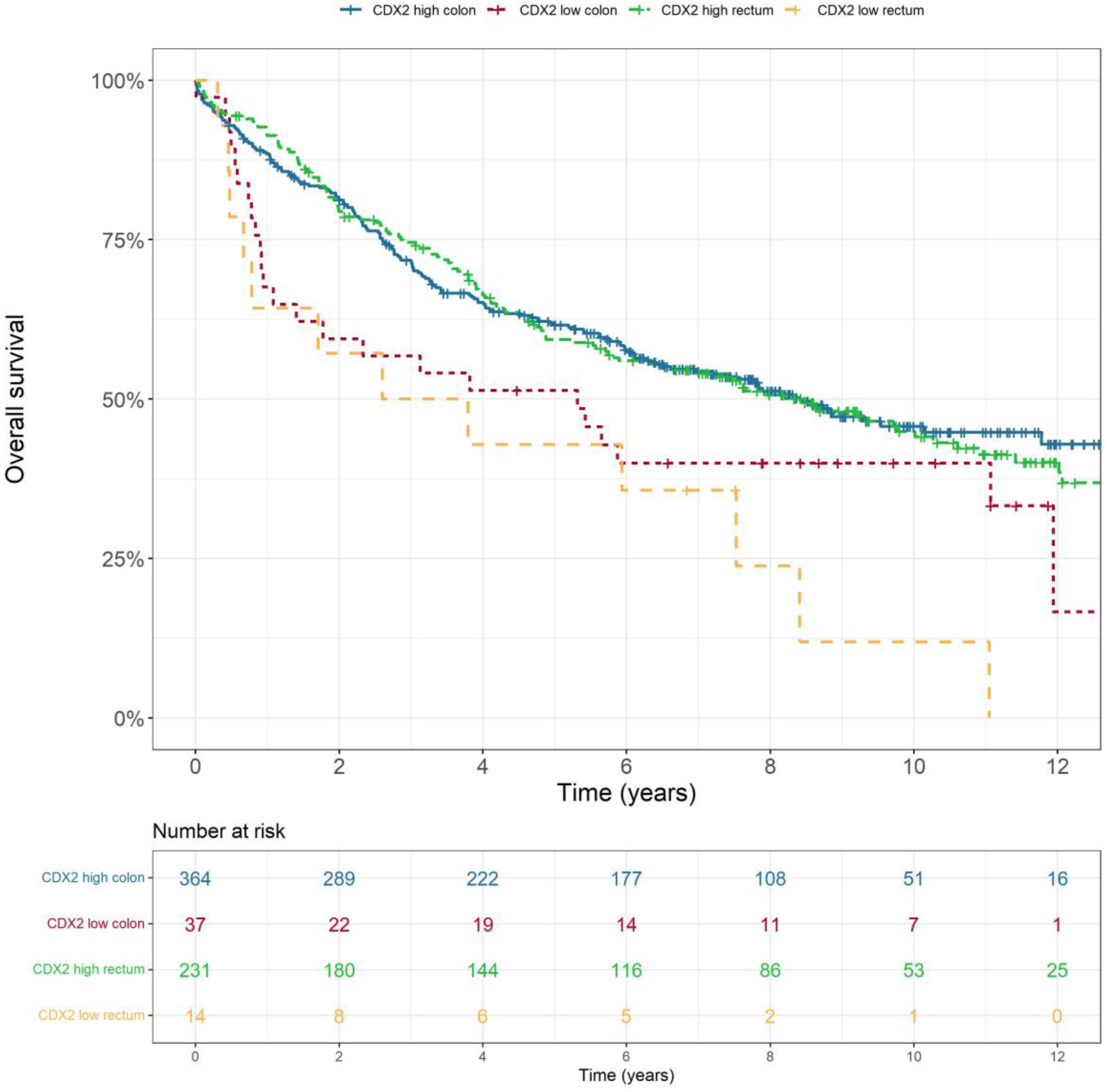
2.3. Low CDX2 Expression Correlates with Poorer Prognosis
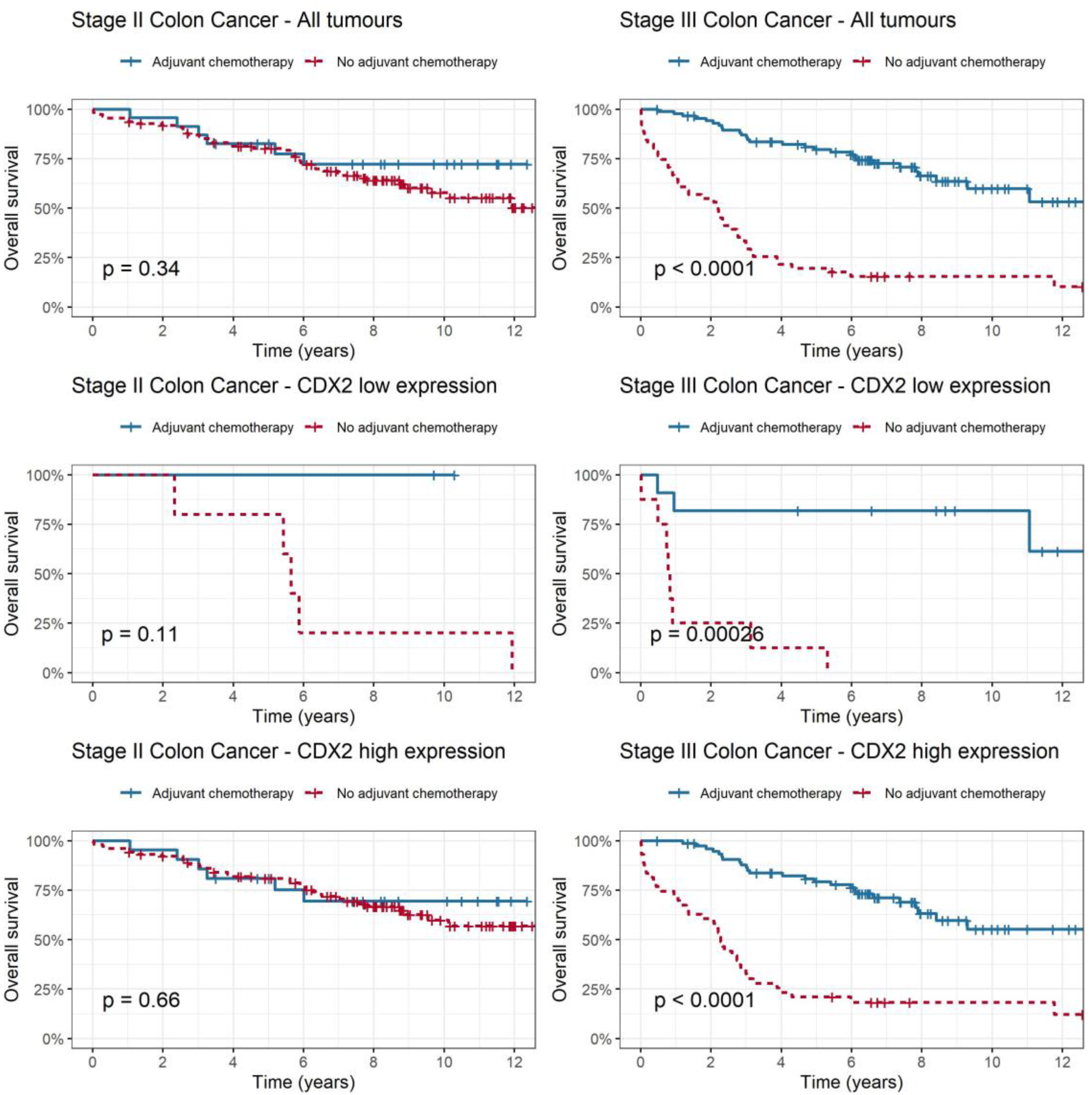
2.4. CDX2 as a Predictive Biomarker for Adjuvant Chemotherapy Benefit in Stage II and III Colon Cancer
2.5. CDX2 as a Predictive Biomarker in Rectal Cancer
3. Discussion
4. Materials and Methods
4.1. Patients and Surgical Specimens
4.2. Tissue Microarrays and Immunohistochemical Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Cancer Data in Australia. 2022. Available online: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia (accessed on 20 August 2022).
- Indicators NCC. Cancer Incidence. 2022. Available online: https://ncci.canceraustralia.gov.au/diagnosis/cancer-incidence/cancer-incidence (accessed on 20 August 2022).
- Cancer Net A. Colorectal Cancer: Statistics. 2023. Available online: https://www.cancer.net/cancer-types/colorectal-cancer/statistics (accessed on 20 August 2022).
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Rebuzzi, S.E.; Pesola, G.; Martelli, V.; Sobrero, A.F. Adjuvant Chemotherapy for Stage II Colon Cancer. Cancers 2020, 12, 2584. [Google Scholar] [CrossRef] [PubMed]
- Koncina, E.; Haan, S.; Rauh, S.; Letellier, E. Prognostic and predictive molecular biomarkers for colorectal cancer: Updates and challenges. Cancers 2020, 12, 319. [Google Scholar] [CrossRef] [PubMed]
- Alves Martins, B.A.; de Bulhões, G.F.; Cavalcanti, I.N.; Martins, M.M.; de Oliveira, P.G.; Martins, A.M.A. Biomarkers in Colorectal Cancer: The Role of Translational Proteomics Research. Front. Oncol. 2019, 9, 1284. [Google Scholar] [CrossRef] [PubMed]
- Asgari-Karchekani, S.; Karimian, M.; Mazoochi, T.; Taheri, M.A.; Khamehchian, T. CDX2 Protein Expression in Colorectal Cancer and ItsCorrelation with Clinical and Pathological Characteristics, Prognosis, and Survival Rate of Patients. J. Gastrointest. Cancer 2019, 51, 844–849. [Google Scholar] [CrossRef]
- Badia-Ramentol, J.; Gimeno-Valiente, F.; Durendez, E.; Martinez-Ciarpaglini, C.; Linares, J.; Iglesias, M.; Cervantes, A.; Calon, A.; Tarazona, N. The prognostic potential of CDX2 in colorectal cancer: Harmonizing biology and clinical practice. Cancer Treat. Rev. 2023, 121, 102643. [Google Scholar] [CrossRef]
- James, R.; Erler, T.; Kazenwadel, J. Structure of the murine homeobox gene cdx-2. Expression in embryonic and adult intestinal epithelium. J. Biol. Chem. 1994, 269, 15229–15237. [Google Scholar] [CrossRef] [PubMed]
- Coskun, M.; Troelsen, J.T.; Nielsen, O.H. The role of CDX2 in intestinal homeostasis and inflammation. Biochim. Biophys. Acta 2011, 1812, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Gao, N.; White, P.; Kaestner, K.H. Establishment of intestinal identity and epithelial-mesenchymal signaling by Cdx2. Dev. Cell 2009, 16, 588–599. [Google Scholar] [CrossRef]
- Mondaca, S.; Walch, H.; Nandakumar, S.; Chatila, W.K.; Schultz, N.; Yaeger, R. Specific Mutations in APC, but Not Alterations in DNA Damage Response, Associate with Outcomes of Patients with Metastatic Colorectal Cancer. Gastroenterology 2020, 159, 1975–1978.e4. [Google Scholar] [CrossRef]
- Bai, Y.Q.; Miyake, S.; Iwai, T.; Yuasa, Y. CDX2, a homeobox transcription factor, upregulates transcription of the p21/WAF1/CIP1 gene. Oncogene 2003, 22, 7942–7949. [Google Scholar] [CrossRef]
- Moskaluk, C.A.; Zhang, H.; Powell, S.M.; Cerilli, L.A.; Hampton, G.M.; Frierson, H.F., Jr. Cdx2 protein expression in normal and malignant human tissues: An immunohistochemical survey using tissue microarrays. Mod. Pathol. 2003, 16, 913–919. [Google Scholar] [CrossRef]
- Werling, R.W.; Yaziji, H.; Bacchi, C.E.; Gown, A.M. CDX2, a highly sensitive and specific marker of adenocarcinomas of intestinal origin: An immunohistochemical survey of 476 primary and metastatic carcinomas. Am. J. Surg. Pathol. 2003, 27, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, G.; Barni, S.; Turati, L.; Ghidini, M.; Pezzica, E.; Passalacqua, R.; Petrelli, F. Association of CDX2 Expression With Survival in Early Colorectal Cancer: A Systematic Review and Meta-analysis. Clin. Color. Cancer 2018, 17, 97–103. [Google Scholar] [CrossRef]
- Baba, Y.; Nosho, K.; Shima, K.; Freed, E.; Irahara, N.; Philips, J.; Meyerhardt, J.A.; Hornick, J.L.; Shivdasani, R.A.; Fuchs, C.S.; et al. Relationship of CDX2 loss with molecular features and prognosis in colorectal cancer. Clin. Cancer Res. 2009, 15, 4665–4673. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.Y.; Jones, J.C.; Briggler, A.M.; Hubbard, J.M.; Kipp, B.R.; Sargent, D.J.; Dixon, J.G.; Grothey, A. Lack of Caudal-Type Homeobox Transcription Factor 2 Expression as a Prognostic Biomarker in Metastatic Colorectal Cancer. Clin. Color. Cancer 2017, 16, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Dalerba, P.; Sahoo, D.; Paik, S.; Guo, X.; Yothers, G.; Song, N.; Wilcox-Fogel, N.; Forgó, E.; Rajendran, P.S.; Miranda, S.P.; et al. CDX2 as a Prognostic Biomarker in Stage II and Stage III Colon Cancer. New Engl. J. Med. 2016, 374, 211–222. [Google Scholar] [CrossRef]
- Ballman, K.V. Biomarker: Predictive or Prognostic? J. Clin. Oncol. 2015, 33, 3968–3971. [Google Scholar] [CrossRef]
- Statisticsc ABo. Sydney South West 2021 Census All Persons QuickStats. Available online: https://abs.gov.au/census/find-census-data/quickstats/2021/127 (accessed on 20 August 2022).
- Bae, J.M.; Lee, T.H.; Cho, N.-Y.Y.; Kim, T.-Y.Y.; Kang, G.H.; Mo Bae, J.; Hun Lee, T.; Cho, N.-Y.Y.; Kim, T.-Y.Y.; Hoon Kang Jeong Mo Bae, G.; et al. Loss of CDX2 expression is associated with poor prognosis in colorectal cancer patients. World J. Gastroenterol. 2014, 21, 1457–1467. [Google Scholar] [CrossRef]
- André, T.; de Gramont, A.; Vernerey, D.; Chibaudel, B.; Bonnetain, F.; Tijeras-Raballand, A.; Scriva, A.; Hickish, T.; Tabernero, J.; Van Laethem, J.L.; et al. Adjuvant Fluorouracil, Leucovorin, and Oxaliplatin in Stage II to III Colon Cancer: Updated 10-Year Survival and Outcomes According to BRAF Mutation and Mismatch Repair Status of the MOSAIC Study. J. Clin. Oncol. 2015, 33, 4176–4187. [Google Scholar] [CrossRef]
- Varghese, A. Chemotherapy for Stage II Colon Cancer. Clin. Colon. Rectal Surg. 2015, 28, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Bruun, J.; Sveen, A.; Barros, R.; Eide, P.W.; Eilertsen, I.; Kolberg, M.; Pellinen, T.; David, L.; Svindland, A.; Kallioniemi, O.; et al. Prognostic, predictive, and pharmacogenomic assessments of CDX2 refine stratification of colorectal cancer. Mol. Oncol. 2018, 12, 1639–1655. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Jiang, T.; Xiao, L.; Yang, S.; Liu, Q.; Gao, Y.; Chen, G.; Xiao, W. Total Neoadjuvant Therapy (TNT) versus Standard Neoadjuvant Chemoradiotherapy for Locally Advanced Rectal Cancer: A Systematic Review and Meta-Analysis. Oncologist 2021, 26, e1555–e1566. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, G.; Canepa, J.; Simonetti, C.; Solo de Zaldívar, L.; Marcelain, K.; González-Montero, J. Consensus molecular subtypes of colorectal cancer in clinical practice: A translational approach. World J. Clin. Oncol. 2021, 12, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Pilati, C.; Taieb, J.; Balogoun, R.; Marisa, L.; De Reyniè, A.; Laurent, P. CDX2 prognostic value in stage II/III resected colon cancer is related to CMS classification. Ann. Oncol. 2017, 28, 1032–1035. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Li, S.; Xu, Z.; Guo, J.; Li, X.; Wu, Y.; Zheng, J.; Sun, X. CDX2 inhibits epithelial-mesenchymal transition in colorectal cancer by modulation of Snail expression and beta-catenin stabilisation via transactivation of PTEN expression. Br. J. Cancer 2021, 124, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yao, Q.; Zhang, L.; Mo, S.; Cai, S.; Huang, D.; Peng, J. IHC-Based Consensus Molecular Subtypes as A Prognostic and Predictive Biomarker for Adjuvant Chemotherapy in Patients with Stage II Colorectal Cancer. Oncologist 2020, 25, e1968–e1979. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Zhu, Y.; Shen, W.; Ding, W.; Wu, T.; Guo, Y.; Chen, X.; Zhou, M.; Chen, Y.; Cui, L.; et al. Combination of CDX2 expression and T stage improves prognostic prediction of colorectal cancer. J. Int. Med. Res. 2019, 47, 1829–1842. [Google Scholar] [CrossRef] [PubMed]
- Hestetun, K.E.; Aasebø, K.; Rosenlund, N.B.; Müller, Y.; Dahl, O.; Myklebust, M.P. Mismatch repair phenotype determines the implications of tumor grade and CDX2 expression in stage II–III colon cancer. Mod. Pathol. 2020, 34, 161–170. [Google Scholar] [CrossRef]
- Hansen, T.F.; Kjaer-Frifeldt, S.; Eriksen, A.C.; Lindebjerg, J.; Jensen, L.H.; Sørensen, F.B.; Jakobsen, A. Prognostic impact of CDX2 in stage II colon cancer: Results from two nationwide cohorts. Br. J. Cancer 2018, 119, 1367–1373. [Google Scholar] [CrossRef]
- Loughrey, M.B.; Webster, F.; Arends, M.J.; Brown, I.; Burgart, L.J.; Cunningham, C.; Flejou, J.F.; Kakar, S.; Kirsch, R.; Kojima, M.; et al. Dataset for Pathology Reporting of Colorectal Cancer: Recommendations From the International Collaboration on Cancer Reporting (ICCR). Ann. Surg. 2022, 275, e549–e561. [Google Scholar] [CrossRef] [PubMed]
- Saad, R.S.; Ghorab, Z.; Khalifa, M.A.; Xu, M. CDX2 as a marker for intestinal differentiation: Its utility and limitations. World J. Gastrointest. Surg. 2011, 3, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Rajesh, N.; Dubashi, B.; Maroju, N.K.; Ganesan, P.; Matta, K.K.; Charles, I.; Kayal, S. Pattern of expression of CDX2 in colorectal cancer and its role in prognosis. J. Cancer Res. Ther. 2022, 18, S420–S427. [Google Scholar] [CrossRef] [PubMed]
- Ben-Aharon, I.; Goshen-Lago, T.; Sternschuss, M.; Morgenstern, S.; Geva, R.; Beny, A.; Dror, Y.; Steiner, M.; Hubert, A.; Idelevich, E.; et al. Sidedness Matters: Surrogate Biomarkers Prognosticate Colorectal Cancer upon Anatomic Location. Oncologist 2019, 24, e696–e701. [Google Scholar] [CrossRef]
- Delgado, A.; Guddati, A.K. Clinical endpoints in oncology—A primer. Am. J. Cancer Res. 2021, 11, 1121–1131. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Class | Total (n = 668) | Percentage (%) | ||
|---|---|---|---|---|---|
| Sex | Male | 392 | 58.7 | ||
| Female | 276 | 41.3 | |||
| CDX2 expression | High (5) | 595 | 89.1 | ||
| Low (1–4) | 51 | 7.6 | |||
| Missing | 22 | 3.3 | |||
| Ethnicity | Caucasian | 577 | 86.4 | ||
| Asian | 76 | 11.4 | |||
| Pacific Islander | 8 | 1.2 | |||
| African | 3 | 0.4 | |||
| Aboriginal/Torres Strait Islander | 4 | 0.6 | |||
| Mean age at diagnosis | 68.6 (23–96) | ||||
| Age at diagnosis | ≤70 years | 340 | 50.9 | ||
| >70 years | 328 | 49.1 | |||
| Cancer stage | Colon | Rectum | Total | ||
| I | 77 | 39 | 116 | 17.4 | |
| II | 133 | 74 | 207 | 31.0 | |
| III | 138 | 112 | 250 | 37.4 | |
| IV | 58 | 37 | 95 | 14.2 | |
| Pathology | Adenocarcinoma | 657 | 98.4 | ||
| Mucinous | 9 | 1.3 | |||
| Signet ring | 2 | 0.3 | |||
| Cancer side | Right | 217 | 32.5 | ||
| Left | 451 | 67.5 | |||
| Colon vs. rectum | Colon | 406 | 60.8 | ||
| Rectum | 262 | 39.2 | |||
| Tumour differentiation | Poor | 98 | 14.7 | ||
| Good/moderate | 570 | 85.3 | |||
| Lymphovascular or perineural invasion | Absent | 438 | 65.8 | ||
| Present | 228 | 34.2 | |||
| Colon | |||||
| Stage II adjuvant chemotherapy | No | 109 | 82.6 | ||
| Yes | 23 | 17.4 | |||
| Stage III adjuvant chemotherapy | None | 51 | 37.5 | ||
| Single agent | 36 | 26.5 | |||
| Doublet | 49 | 36.0 | |||
| Stage IV palliative chemotherapy | No | 20 | 34.5 | ||
| Yes | 38 | 65.5 | |||
| Rectum | |||||
| Neoadjuvant therapy | No | 200 | 76.3 | ||
| Yes | 62 | 23.7 | |||
| Adjuvant chemotherapy | No | 123 | 54.2 | ||
| Yes | 104 | 45.8 | |||
| Variable | Class | CDX2 Expression | ||
|---|---|---|---|---|
| High, n = 595 (%) | Low, n = 51 (%) | p-Value | ||
| Sex | Male | 356 (94.4) | 21 (5.6) | 0.012 |
| Female | 239 (88.8) | 30 (11.2) | ||
| Ethnicity | Caucasian | 511 (91.9) | 45 (8.1) | 0.373 |
| Asian | 71 (94.7) | 4 (5.3) | ||
| Pacific Islander | 7 (87.5) | 1 (12.5) | ||
| African | 3 (100.0) | 0 (0.0) | ||
| Aboriginal/Torres Strait Islander | 3 (75.0) | 1 (25.1) | ||
| Age at diagnosis | ≤70 years | 288 (92.3) | 24 (7.7) | 0.885 |
| >70 years | 307 (91.9) | 27 (8.1) | ||
| Cancer stage | I | 110 (96.5) | 4 (3.5) | 0.015 |
| II | 189 (95.0) | 10 (5.0) | ||
| III | 216 (89.3) | 26 (10.7) | ||
| IV | 80 (87.9) | 11 (12.1) | ||
| Pathology | Adenocarcinoma | 587 (92.2) | 50 (7.8) | 0.525 |
| Mucinous | 7 (87.5) | 1 (12.5) | ||
| Signet ring | 1 (100.0) | 0 (0.0) | ||
| Cancer side | Right | 189 (88.3) | 25 (11.7) | 0.019 |
| Left | 406 (94.0) | 26 (6.0) | ||
| Colon vs. rectum | Colon | 364 (90.8) | 37 (9.2) | 0.132 |
| Rectum | 231 (94.3) | 14 (5.7) | ||
| Tumour differentiation | Poor | 74 (77.1) | 22 (22.9) | <0.001 |
| Good / moderate | 521 (94.7) | 29 (5.3) | ||
| Lymphovascular or perineural invasion | Absent | 399 (94.5) | 23 (5.5) | 0.002 |
| Present | 194 (87.4) | 28 (12.6) | ||
| Colon stage II | Received adjuvant chemotherapy | 21 (91.3) | 2 (8.7) | 0.607 |
| Did not receive adjuvant chemotherapy | 102 (95.3) | 5 (4.7) | ||
| Colon stage III | Received adjuvant chemotherapy | 76 (87.4) | 11 (12.6) | 0.618 |
| Did not receive adjuvant chemotherapy | 43 (84.3) | 8 (15.7) | ||
| Subgroup | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| All patients (n = 668) | ||||
| CDX2-negative | 0.584 (0.413–0.825) | 0.002 | 0.602 (0.421–0.86) | 0.005 |
| Tumour stage | ||||
| Stage I vs. stage IV | 0.117 (0.080–0.172) | <0.001 | 0.118 (0.08–0.173) | <0.001 |
| Stage II vs. stage IV | 0.125 (0.091–0.172) | <0.001 | 0.123 (0.089–0.17) | <0.001 |
| Stage III vs. stage IV | 0.182 (0.136–0.244) | <0.001 | 0.175 (0.13–0.235) | <0.001 |
| Male vs. female sex | 0.947 (0.763–1.177) | 0.624 | 0.906 (0.726–1.131) | 0.384 |
| Right vs. left | 1.119 (0.891–1.404) | 0.332 | 1.116 (0.841–1.482) | 0.447 |
| Colon vs. rectum | 0.963 (0.775–1.198) | 0.736 | 0.937 (0.715–1.228) | 0.637 |
| Percentage of Deeply Stained Nuclei (%) | Score |
|---|---|
| Less than 5 | 1 |
| 5–24 | 2 |
| 25–49 | 3 |
| 50–74 | 4 |
| 75–100 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, W.Y.; Chua, W.; Wilkinson, K.; Epitakaduwa, C.; Mandaliya, H.; Descallar, J.; Roberts, T.L.; Becker, T.M.; Ng, W.; Lee, C.S.; et al. The Prognostic and Predictive Utility of CDX2 in Colorectal Cancer. Int. J. Mol. Sci. 2024, 25, 8673. https://doi.org/10.3390/ijms25168673
Chan WY, Chua W, Wilkinson K, Epitakaduwa C, Mandaliya H, Descallar J, Roberts TL, Becker TM, Ng W, Lee CS, et al. The Prognostic and Predictive Utility of CDX2 in Colorectal Cancer. International Journal of Molecular Sciences. 2024; 25(16):8673. https://doi.org/10.3390/ijms25168673
Chicago/Turabian StyleChan, Wei Yen, Wei Chua, Kate Wilkinson, Chandika Epitakaduwa, Hiren Mandaliya, Joseph Descallar, Tara Laurine Roberts, Therese Maria Becker, Weng Ng, Cheok Soon Lee, and et al. 2024. "The Prognostic and Predictive Utility of CDX2 in Colorectal Cancer" International Journal of Molecular Sciences 25, no. 16: 8673. https://doi.org/10.3390/ijms25168673