

Role of Advanced Glycation End Products as New Biomarkers in Systemic Lupus Erythematosus

 , , , , ,
, , , , ,  ,
,  ,
,
Abstract
:1. Background
2. Results
2.1. Characteristics of Patients and Controls
2.2. Comparison of AGEs in SLE Patients vs. Healthy Controls
2.3. Characteristics of SLE Patients According to AGEs Levels: Bivariate Analysis
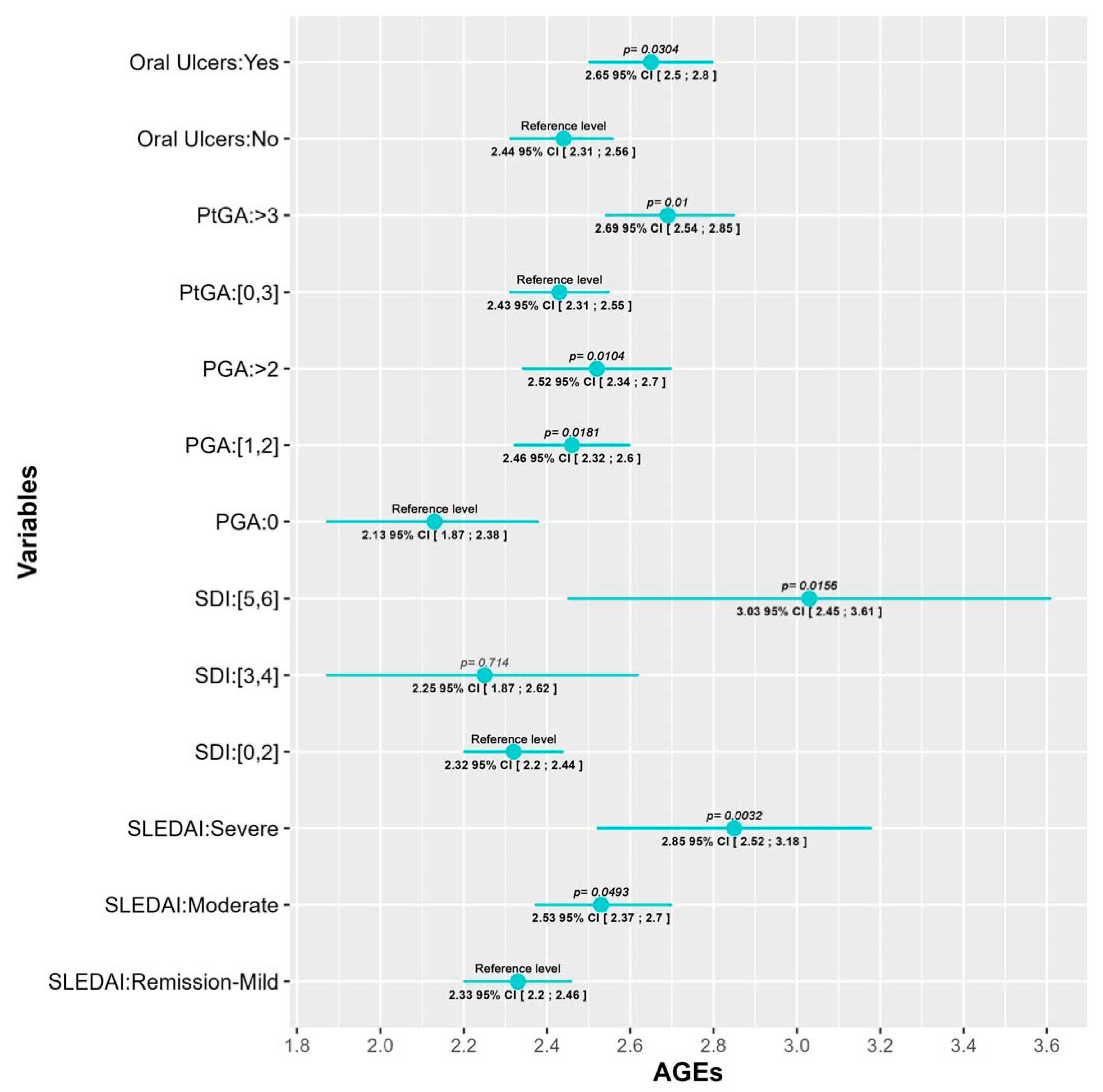
2.4. Correlations between AGEs and SLE Characteristics: Multivariate Analysis
3. Discussion
4. Methodology
4.1. Subjects
4.2. Healthy Controls
4.3. Assessment of AGES Accumulation
4.4. Statistical Methods
4.4.1. Comparison of Accumulated AGEs between Patients and Controls
4.4.2. Relation between Characteristics of SLE and Accumulated AGEs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AGEs | Advanced glycation end-products |
| ANA | antinuclear antibodies |
| ANCOVA | analysis of covariance |
| BMI | body mass index |
| CVRF | cardiovascular risk factors |
| HC | healthy controls |
| LDL | low-density lipoproteins |
| PGA | physician global assessment |
| PROs | patient reported outcomes |
| PtGA | patient global assessment |
| RAGE | receptor for advanced glycation end-products |
| SDI | systemic lupus erythematosus damage index |
| SjS | Sjögren syndrome |
| SLE | systemic lupus erythematosus |
| SLEDAI | systemic lupus erythematosus disease activity index |
| SLICC | Systemic Lupus International Collaborating Clinics |
Appendix A
- Cristina Farràs 1, Ferrán Barbé 2, Reinald Pamplona 3, Dídac Mauricio 4,5,6, Elvira Fernández 7, Eva Miquel 1, Marta Ortega 1, Jessica González 2, Jordi de Batlle 2, Silvia Barril 2, Manuel Sánchez-de-la-Torre 2, Manuel Portero-Otín 6, Mariona Jové 6, Marta Hernández 4,8, Ferran Rius 4,8, Josep Franch-Nadal 4,5, Esmeralda Castelblanco 4,5, Pere Godoy 9, Montse Martinez-Alonso 10.
- 1
- Centre d’Atenció Primària Cappont. Gerència Territorial de Lleida, Institut Català de la Salut, Barcelona, Spain. Research Support Unit Lleida, Fundació Institut Universitari per a la recerca a l’Atenció Primària de Salut Jordi Gol i Gorina (IDIAPJGol), Barcelona, Spain.
- 2
- Departament de Medicina Respiratòria, Hospital Universitari Arnau de Vilanova, Grup Recerca Translational Medicina Respiratòria, IRBLleida, Universitat de Lleida, Lleida, CIBER de enfermedades respiratorias (CIBERES), Madrid, Spain.
- 3
- Departament de Medicina Experimental, IRBLleida, Universitat de Lleida, Lleida, Spain.
- 4
- Centro de Investigación Biomédica en Red de Diabetes y Enfermedades Metabólicas Asociadas (CIBERDEM), Instituto de Salud Carlos III (ISCIII), Madrid, Spain.
- 5
- Departament d’Endocrinologia i Nutrició, Hospital de la Santa Creu i Sant Pau, Institut de Recerca Biomèdica Sant Pau (IIB Sant Pau), Barcelona, Spain.
- 6
- Faculty of Medicine, University of Vic & Central University of Vic, Vic, Spain.
- 7
- Grupo de investigación Translacional vascular y Renal, IRBLleida, Red de Investigación Renal (RedInRen. ISCIII), Lleida, Spain.
- 8
- Departament d’Endocrinologia i Nutrició, Hospital Universitari Arnau de Vilanova, Grup de Recerca Obesitat i Metabolisme (ODIM), IRBLleida, Universitat de Lleida, Lleida, Spain.
- 9
- Agència de Salut Pública de Catalunya, Departament de Salut, IRBLleida, Universitat de Lleida, Lleida, Spain, CIBER de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain.
- 10
- Unitat de Bioestadística, IRBLleida, Departament de ciències Mèdiques Bàsiques, Universitat de Lleida, Lleida, Spain.
References
- Rabbani, N.; Thornalley, P.J. Advanced Glycation End Products in the Pathogenesis of Chronic Kidney Disease. Kidney Int. 2018, 93, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Kurien, B.T.; Hensley, K.; Bachmann, M.; Scofield, R.H. Oxidatively Modified Autoantigens in Autoimmune Diseases. Free Radic. Biol. Med. 2006, 41, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Pullerits, R.; Bokarewa, M.; Dahlberg, L.; Tarkowski, A. Decreased Levels of Soluble Receptor for Advanced Glycation End Products in Patients with Rheumatoid Arthritis Indicating Deficient Inflammatory Control. Arthritis Res. Ther. 2005, 7, R817–R824. [Google Scholar] [CrossRef] [PubMed]
- Hudson, B.I.; Lippman, M.E. Targeting RAGE Signaling in Inflammatory Disease. Annu. Rev. Med. 2018, 69, 349–364. [Google Scholar] [CrossRef]
- Sárkány, Z.; Ikonen, T.P.; Ferreira-da-Silva, F.; Saraiva, M.J.; Svergun, D.; Damas, A.M. Solution Structure of the Soluble Receptor for Advanced Glycation End Products (SRAGE). J. Biol. Chem. 2011, 286, 37525–37534. [Google Scholar] [CrossRef]
- Geroldi, D.; Falcone, C.; Emanuele, E. Soluble Receptor for Advanced Glycation End Products: From Disease Marker to Potential Therapeutic Target. Curr. Med. Chem. 2006, 13, 1971–1978. [Google Scholar] [CrossRef] [PubMed]
- Nienhuis, H.L.; De Leeuw, K.; Bijzet, J.; Smit, A.; Schalkwijk, C.G.; Graaff, R.; Kallenberg, C.G.; Bijl, M. Skin Autofluorescence Is Increased in Systemic Lupus Erythematosus but Is Not Reflected by Elevated Plasma Levels of Advanced Glycation Endproducts. Rheumatology 2008, 47, 1554–1558. [Google Scholar] [CrossRef]
- Thorpe, S.R.; Baynes, J.W. Maillard Reaction Products in Tissue Proteins: New Products and New Perspectives. Amino Acids 2003, 25, 275–281. [Google Scholar] [CrossRef]
- Coll, J.-C.; Turcotte, A.-F.; Garceau, É.; Michou, L.; Weisnagel, S.J.; Mac-Way, F.; Morin, S.N.; Rabasa-Lhoret, R.; Gagnon, C. Skin and Serum Advanced Glycation End Products in Adults With Type 1 Diabetes. Can. J. Diabetes 2022, 46, S25. [Google Scholar] [CrossRef]
- Meerwaldt, R.; Graaf, R.; Oomen, P.H.N.; Links, T.P.; Jager, J.J.; Alderson, N.L.; Thorpe, S.R.; Baynes, J.W.; Gans, R.O.B.; Smit, A.J. Simple Non-Invasive Assessment of Advanced Glycation Endproduct Accumulation. Diabetologia 2004, 47, 1324–1330. [Google Scholar] [CrossRef]
- Nowak, A.; Przywara-Chowaniec, B.; Damasiewicz-Bodzek, A.; Blachut, D.; Nowalany-Kozielska, E.; Tyrpień-Golder, K. Advanced Glycation End-Products (Ages) and Their Soluble Receptor (Srage) in Women Suffering from Systemic Lupus Erythematosus (Sle). Cells 2021, 10, 3523. [Google Scholar] [CrossRef] [PubMed]
- Ene, C.D.; Georgescu, S.R.; Tampa, M.; Matei, C.; Mitran, C.I.; Mitran, M.I.; Penescu, M.N.; Nicolae, I. Cellular Response against Oxidative Stress, a Novel Insight into Lupus Nephritis Pathogenesis. J. Pers. Med. 2021, 11, 693. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.Y.; Chen, Y.M.; Lin, C.C.; Hsieh, C.W.; Wu, Y.C.; Hung, W.T.; Chen, H.H.; Lan, J.L. The Potential Role of Advanced Glycation End Products (AGEs) and Soluble Receptors for AGEs (SRAGE) in the Pathogenesis of Adult-Onset Still’s Disease. BMC Musculoskelet. Disord. 2015, 16, 111. [Google Scholar] [CrossRef]
- Nienhuis, H.L.A.; de Leeuw, K.; Bijzet, J.; van Doormaal, J.J.; van Roon, A.M.; Smit, A.J.; Graaff, R.; Kallenberg, C.G.M.; Bijl, M. Small Artery Elasticity Is Decreased in Patients with Systemic Lupus Erythematosus without Increased Intima Media Thickness. Arthritis Res. Ther. 2010, 12, R181. [Google Scholar] [CrossRef]
- De Leeuw, K.; Graaff, R.; de Vries, R.; Dullaart, R.P.; Smit, A.J.; Kallenberg, C.G.; Bijl, M. Accumulation of Advanced Glycation Endproducts in Patients with Systemic Lupus Erythematosus. Rheumatology 2007, 46, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Quyyumi, A.A. Inflamed Joints and Stiff Arteries. Circulation 2006, 114, 1137–1139. [Google Scholar] [CrossRef]
- Makita, Z.; Yanagisawa, K.; Kuwajima, S.; Bucala, R.; Vlassara, H.; Koike, T. The Role of Advanced Glycosylation End-Products in the Pathogenesis of Atherosclerosis. Nephrol. Dial. Transplant. 1996, 11, 31–33. [Google Scholar] [CrossRef]
- Vekic, J.; Vujcic, S.; Bufan, B.; Bojanin, D.; Al-Hashmi, K.; Al-Rasadi, K.; Stoian, A.P.; Zeljkovic, A.; Rizzo, M. The Role of Advanced Glycation End Products on Dyslipidemia. Metabolites 2023, 13, 77. [Google Scholar] [CrossRef]
- De Leeuw, K.; Freire, B.; Smit, A.J.; Bootsma, H.; Kallenberg, C.G.; Bijl, M. Traditional and Non-Traditional Risk Factors Contribute to the Development of Accelerated Atherosclerosis in Patients with Systemic Lupus Erythematosus. Lupus 2006, 15, 675–682. [Google Scholar] [CrossRef]
- Peters, M.J.L.; Symmons, D.P.M.; McCarey, D.; Dijkmans, B.A.C.; Nicola, P.; Kvien, T.K.; McInnes, I.B.; Haentzschel, H.; Gonzalez-Gay, M.A.; Provan, S.; et al. EULAR Evidence-Based Recommendations for Cardiovascular Risk Management in Patients with Rheumatoid Arthritis and Other Forms of Inflammatory Arthritis. Ann. Rheum. Dis. 2010, 69, 325–331. [Google Scholar] [CrossRef]
- Cotton, T.; Fritzler, M.J.; Choi, M.Y.; Zheng, B.; Niaki, O.Z.; Pineau, C.A.; Lukusa, L.; Bernatsky, S. Serologic Phenotypes Distinguish Systemic Lupus Erythematosus Patients Developing Interstitial Lung Disease and/or Myositis. Lupus 2022, 31, 1477–1484. [Google Scholar] [CrossRef]
- Raj, D.S.; Choudhury, D.; Welbourne, T.C. Advanced Glycation End Products: A Nephrologist’s Perspective. Am. J. Kidney Dis. 2000, 35, 365–380. [Google Scholar] [CrossRef]
- Sourris, K.C.; Watson, A.; Jandeleit-Dahm, K. Inhibitors of Advanced Glycation End Product (AGE) Formation and Accumulation. Handb. Exp. Pharmacol. 2021, 264, 395–423. [Google Scholar] [CrossRef]
- Goldberg, T.; Cai, W.; Peppa, M.; Dardaine, V.; Baliga, B.S.; Uribarri, J.; Vlassara, H. Advanced Glycoxidation End Products in Commonly Consumed Foods. J. Am. Diet. Assoc. 2004, 104, 1287–1291. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, A.; Alexander, R.V.; Zack, D.J. A Review of Complement Activation in SLE. Curr. Rheumatol. Rep. 2021, 23, 16. [Google Scholar] [CrossRef] [PubMed]
- Gandino, I.J.; Scolnik, M.; Bertiller, E.; Scaglioni, V.; Catoggio, L.J.; Soriano, E.R. Complement Levels and Risk of Organ Involvement in Patients with Systemic Lupus Erythematosus. Lupus Sci. Med. 2017, 4, e000209. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lin, S.; Yang, S.; Chen, L.; Zheng, X. Diagnostic Value of Serum Complement C3 and C4 Levels in Chinese Patients with Systemic Lupus Erythematosus. Clin. Rheumatol. 2015, 34, 471–477. [Google Scholar] [CrossRef]
- Lee, K.E.; Mun, S.; Kim, S.M.; Shin, W.; Jung, W.; Paek, J.; Lee, J.; Erin, H.; Welsey, H.L.; Han, K.; et al. The Inflammatory Signature in Monocytes of Sjögren’s Syndrome and Systemic Lupus Erythematosus, Revealed by the Integrated Reactome and Drug Target Analysis. Genes Genom. 2022, 44, 1215–1229. [Google Scholar] [CrossRef]
- Stewart, C.; Cha, S.; Caudle, R.M.; Berg, K.; Katz, J. Decreased Levels of Soluble Receptor for Advanced Glycation End Products in Patients with Primary Sjögren’s Syndrome. Rheumatol. Int. 2008, 28, 771–776. [Google Scholar] [CrossRef]
- Katz, J.; Stavropoulos, F.; Bhattacharyya, I.; Stewart, C.; Perez, F.M.; Caudle, R.M. Receptor of Advanced Glycation End Product (RAGE) Expression in the Minor Salivary Glands of Patients with Sjögren’s Syndrome: A Preliminary Study. Scand. J. Rheumatol. 2004, 33, 174–178. [Google Scholar] [CrossRef]
- Kanne, A.M.; Jülich, M.; Mahmutovic, A.; Tröster, I.; Sehnert, B.; Urbonaviciute, V.; Voll, R.E.; Kollert, F. Association of High Mobility Group Box Chromosomal Protein 1 and Receptor for Advanced Glycation End Products Serum Concentrations with Extraglandular Involvement and Disease Activity in Sjögren’s Syndrome. Arthritis Care Res. 2018, 70, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Pisetsky, D.S.; Lipsky, P.E. New Insights into the Role of Antinuclear Antibodies in Systemic Lupus Erythematosus. Nat. Rev. Rheumatol. 2020, 16, 565–579. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C. Updating the American College of Rheumatology Revised Criteria for the Classification of Systemic Lupus Erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.M.; Alarcõn, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and Validation of the Systemic Lupus International Collaborating Clinics Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://Elbusdelasalut.Cat/Professionals/Protocol-Estudi/ (accessed on 5 September 2023).
- Shardlow, A.; McIntyre, N.J.; Kolhe, N.V.; Nellums, L.B.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. The Association of Skin Autofluorescence with Cardiovascular Events and All-Cause Mortality in Persons with Chronic Kidney Disease Stage 3: A Prospective Cohort Study. PLoS Med. 2020, 17, e1003163. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Controls | Cases | p-Value | |
|---|---|---|---|
| N = 189 | N = 62 | ||
| Ethnicity | <0.001 | ||
| Caucasian | 189 (100%) | 46 (74.2%) | |
| Other | 0 (0.00%) | 16 (25.8%) | |
| Age | 56.0 [52.0; 62.0] | 55.0 [51.0; 61.8] | 0.193 |
| Sex: Female | 180 (95.2%) | 58 (93.5%) | 0.748 |
| Hypertension | 73 (38.6%) | 14 (22.6%) | 0.032 |
| Obesity | 61 (32.3%) | 12 (19.4%) | 0.075 |
| Dyslipidemia | 85 (45.0%) | 9 (14.5%) | <0.001 |
| Smoking | 0.054 | ||
| Never | 79 (41.8%) | 24 (38.7%) | |
| Former (>1 year) | 54 (28.6%) | 27 (43.5%) | |
| Active | 56 (29.6%) | 11 (17.7%) | |
| Body mass index | 28.9 (5.98) | 25.6 (4.65) | <0.001 |
| Creatinine | 0.70 [0.61; 0.77] | 0.74 [0.64; 0.90] | 0.006 |
| Uric acid | 4.90 (1.27) | 4.70 (1.62) | 0.365 |
| Cholesterol | 210 (37.5) | 187 (39.5) | <0.001 |
| HDL | 61.9 (14.0) | 65.9 (15.7) | 0.125 |
| LDL | 138 (29.3) | 112 (34.6) | <0.001 |
| Triglycerides | 123 [95.8; 160] | 92.0 [70.0; 159] | 0.003 |
| Antidyslipidemics | 27 (14.3%) | 11 (17.7%) | 0.649 |
| Antihypertensives | 61 (32.3%) | 16 (25.8%) | 0.424 |
| AGEs | 1.98 (0.45) | 2.71 (0.56) | <0.001 |
| AGEs in tertiles | <0.001 | ||
| [1.0, 1.9) | 83 (43.9%) | 3 (4.84%) | |
| [1.9, 2.4) | 74 (39.2%) | 13 (21.0%) | |
| [2.4, 4.2] | 32 (16.9%) | 46 (74.2%) |
| Est. | 2.5% | 97.5% | t Val. | p-Value | |
|---|---|---|---|---|---|
| Intercept | 1.9418 | 1.8450 | 2.0385 | 39.5252 | <0.0001 |
| Group: Cases | 0.7210 | 0.5660 | 0.8759 | 9.1645 | <0.0001 |
| Age (57.5 years) | 0.0168 | 0.0081 | 0.0254 | 3.8359 | 0.0002 |
| Smoking (Yes) | 0.3265 | 0.1945 | 0.4585 | 4.8724 | <0.0001 |
| Creatinine (0.72 mg/dL) | 0.2110 | −0.1763 | 0.5983 | 1.0732 | 0.2843 |
| Dyslipidemia (Yes) | −0.1240 | −0.2544 | 0.0065 | −1.8720 | 0.0624 |
| (Group: Cases) + (Dyslipidemia (Yes)) | 0.1286 | −0.2227 | 0.4799 | 0.7211 | 0.4715 |
| Variables | All | 1st Tertile [1.2, 2.3) | 2nd Tertile [2.3, 2.8) | 3rd Tertile [2.8, 4.6] | p-Val M1 | p-Val M2 |
|---|---|---|---|---|---|---|
| N = 122 | N = 44 | N = 41 | N = 37 | |||
| Age | 50.4 (14.9) | 41.8 (13.8) | 49.9 (12.2) | 61.2 (11.9) | <0.001 | |
| Smoker | 32 (26.2%) | 10 (22.7%) | 11 (26.8%) | 11 (29.7%) | <0.001 | |
| cDisease duration (years) | 0.082 | 0.090 | ||||
| 0–5 | 50 (41.0%) | 19 (43.2%) | 18 (43.9%) | 13 (35.1%) | ||
| 6–10 | 16 (13.1%) | 7 (15.9%) | 6 (14.6%) | 3 (8.11%) | ||
| 11–20 | 33 (27.0%) | 13 (29.5%) | 11 (26.8%) | 9 (24.3%) | ||
| >20 | 23 (18.9%) | 5 (11.4%) | 6 (14.6%) | 12 (32.4%) | ||
| Classificatory Criteria and Other Clinical and Serological Data | ||||||
| Oral ulcers ever | 50 (41.0%) | 13 (29.5%) | 18 (43.9%) | 19 (51.4%) | 0.022 | 0.033 |
| Arthritis ever | 92 (75.4%) | 31 (70.5%) | 32 (78.0%) | 29 (78.4%) | 0.070 | 0.092 |
| Renal disease ever | 8 (6.56%) | 2 (4.55%) | 1 (2.44%) | 5 (13.5%) | 0.067 | 0.054 |
| cNumber of manifestations | 0.032 | 0.069 | ||||
| [3, 7) | 58 (47.5%) | 19 (43.2%) | 21 (51.2%) | 18 (48.6%) | ||
| 7 | 24 (19.7%) | 10 (22.7%) | 8 (19.5%) | 6 (16.2%) | ||
| [8, 12] | 40 (32.8%) | 15 (34.1%) | 12 (29.3%) | 13 (35.1%) | ||
| Disease Activity Indexes | ||||||
| SLEDAI | 4.00 [2.00; 6.00] | 4.00 [0.00; 6.00] | 4.00 [2.00; 6.00] | 6.00 [2.00; 8.00] | 0.016 | 0.041 |
| cSLEDAI | 0.003 | 0.008 | ||||
| Remission/Mild | 71 (58.7%) | 29 (67.4%) | 25 (61.0%) | 17 (45.9%) | ||
| Moderate | 39 (32.2%) | 11 (25.6%) | 14 (34.1%) | 14 (37.8%) | ||
| Severe | 11 (9.09%) | 3 (6.98%) | 2 (4.88%) | 6 (16.2%) | ||
| SDI | 0.00 [0.00; 1.00] | 0.00 [0.00; 1.00] | 0.00 [0.00; 1.00] | 1.00 [0.00; 2.00] | 0.026 | 0.007 |
| cSDI_3 | 0.052 | 0.017 | ||||
| 0–2 | 110 (90.9%) | 41 (95.3%) | 38 (92.7%) | 31 (83.8%) | ||
| 3–4 | 8 (6.61%) | 2 (4.65%) | 2 (4.88%) | 4 (10.8%) | ||
| 5–6 | 3 (2.48%) | 0 (0.00%) | 1 (2.44%) | 2 (5.41%) | ||
| PGA | 2.00 [1.00; 3.00] | 1.50 [1.00; 2.00] | 2.00 [1.00; 3.00] | 2.00 [1.00; 2.00] | 0.083 | 0.051 |
| cPGA | 0.051 | 0.029 | ||||
| <1 | 18 (14.9%) | 7 (16.3%) | 6 (14.6%) | 5 (13.5%) | ||
| 1–2 | 69 (57.0%) | 27 (62.8%) | 19 (46.3%) | 23 (62.2%) | ||
| >2 | 34 (28.1%) | 9 (20.9%) | 16 (39.0%) | 9 (24.3%) | ||
| Patient Reported Outcomes | ||||||
| FACIT | 17.5 [10.0; 27.0] | 14.0 [9.00; 23.0] | 22.0 [13.0; 30.0] | 18.0 [10.0; 28.0] | 0.099 | 0.138 |
| PtGA | 2.75 [1.00; 5.00] | 2.00 [1.00; 3.00] | 3.00 [2.00; 5.00] | 3.00 [1.00; 5.00] | 0.028 | 0.042 |
| cPtGA | 0.112 | 0.121 | ||||
| [0.0, 2.5) | 57 (46.7%) | 26 (59.1%) | 14 (34.1%) | 17 (45.9%) | ||
| [2.5, 4.5) | 28 (23.0%) | 9 (20.5%) | 12 (29.3%) | 7 (18.9%) | ||
| [4.5, 8.0] | 37 (30.3%) | 9 (20.5%) | 15 (36.6%) | 13 (35.1%) | ||
| Serological variables | ||||||
| GPT * | 17.0 [13.0; 22.0] | 16.0 [12.0; 22.5] | 16.0 [13.0; 20.0] | 18.0 [15.0; 23.0] | 0.095 | 0.068 |
| Total cholesterol * | 181 (37.7) | 172 (29.6) | 174 (38.0) | 201 (39.5) | 0.046 | 0.093 |
| cCRP * | 0.058 | 0.053 | ||||
| [0.03, 0.12) | 45 (37.2%) | 24 (55.8%) | 8 (19.5%) | 13 (35.1%) | ||
| [0.12, 0.28) | 36 (29.8%) | 11 (25.6%) | 17 (41.5%) | 8 (21.6%) | ||
| [0.28, 3.92] | 40 (33.1%) | 8 (18.6%) | 16 (39.0%) | 16 (43.2%) | ||
| cIL-6 * | 0.049 | 0.025 | ||||
| [0.63, 1.88) | 36 (33.3%) | 18 (48.6%) | 12 (31.6%) | 6 (18.2%) | ||
| [1.88, 3.33) | 36 (33.3%) | 11 (29.7%) | 14 (36.8%) | 11 (33.3%) | ||
| [3.33, 144.10] | 36 (33.3%) | 8 (21.6%) | 12 (31.6%) | 16 (48.5%) | ||
| ANA+ * | 112 (92.6%) | 43 (100%) | 38 (92.7%) | 31 (83.8%) | 0.027 | 0.036 |
| Anti-Ro60+ * | 45 (37.8%) | 17 (40.5%) | 19 (47.5%) | 9 (24.3%) | 0.183 | 0.164 |
| C4 * | 19.8 (8.23) | 18.5 (7.97) | 18.7 (7.09) | 22.4 (9.23) | 0.025 | 0.017 |
| Leukocyturia * | 0.00 [0.00; 1.00] | 0.00 [0.00; 0.00] | 0.00 [0.00; 1.00] | 1.00 [0.00; 2.00] | 0.004 | 0.001 |
| Hematuria * | 0.00 [0.00; 0.00] | 0.00 [0.00; 0.00] | 0.00 [0.00; 0.00] | 0.00 [0.00; 1.00] | 0.031 | 0.067 |
| cLeukocyturia * | 0.052 | 0.024 | ||||
| 0 | 72 (60.0%) | 33 (78.6%) | 24 (58.5%) | 15 (40.5%) | ||
| 1 | 25 (20.8%) | 6 (14.3%) | 11 (26.8%) | 8 (21.6%) | ||
| [2, 5] | 23 (19.2%) | 3 (7.14%) | 6 (14.6%) | 14 (37.8%) | ||
| Treatments | ||||||
| GC | 30 (24.6%) | 7 (15.9%) | 11 (26.8%) | 12 (32.4%) | 0.004 | <0.001 |
| Current dose of GC | 5.00 [2.50; 10.0] | 7.50 [3.75; 10.0] | 5.00 [2.50; 12.5] | 5.00 [2.50; 6.25] | 0.050 | 0.029 |
| Tacrolimus | 1 (0.82%) | 0 (0.00%) | 0 (0.00%) | 1 (2.70%) | 0.147 | 0.083 |
| cTreatment2 | 0.077 | 0.092 | ||||
| No IS | 66 (54.1%) | 27 (61.4%) | 20 (48.8%) | 19 (51.4%) | ||
| IS | 56 (45.9%) | 17 (38.6%) | 21 (51.2%) | 18 (48.6%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrión-Barberà, I.; Triginer, L.; Tío, L.; Pérez-García, C.; Ribes, A.; Abad, V.; Pros, A.; Bermúdez-López, M.; Castro-Boqué, E.; Lecube, A.; et al. Role of Advanced Glycation End Products as New Biomarkers in Systemic Lupus Erythematosus. Int. J. Mol. Sci. 2024, 25, 3022. https://doi.org/10.3390/ijms25053022
Carrión-Barberà I, Triginer L, Tío L, Pérez-García C, Ribes A, Abad V, Pros A, Bermúdez-López M, Castro-Boqué E, Lecube A, et al. Role of Advanced Glycation End Products as New Biomarkers in Systemic Lupus Erythematosus. International Journal of Molecular Sciences. 2024; 25(5):3022. https://doi.org/10.3390/ijms25053022
Chicago/Turabian StyleCarrión-Barberà, Irene, Laura Triginer, Laura Tío, Carolina Pérez-García, Anna Ribes, Victoria Abad, Ana Pros, Marcelino Bermúdez-López, Eva Castro-Boqué, Albert Lecube, and et al. 2024. "Role of Advanced Glycation End Products as New Biomarkers in Systemic Lupus Erythematosus" International Journal of Molecular Sciences 25, no. 5: 3022. https://doi.org/10.3390/ijms25053022
APA StyleCarrión-Barberà, I., Triginer, L., Tío, L., Pérez-García, C., Ribes, A., Abad, V., Pros, A., Bermúdez-López, M., Castro-Boqué, E., Lecube, A., Valdivielso, J. M., ILERVAS Project Group, Monfort, J., & Salman-Monte, T. C. (2024). Role of Advanced Glycation End Products as New Biomarkers in Systemic Lupus Erythematosus. International Journal of Molecular Sciences, 25(5), 3022. https://doi.org/10.3390/ijms25053022