
A Biodegradable Tissue Adhesive for Post-Extraction Alveolar Bone Regeneration under Ongoing Anticoagulation—A Microstructural Volumetric Analysis in a Rodent Model

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Ethics Statement
4.2. Experimental Animals
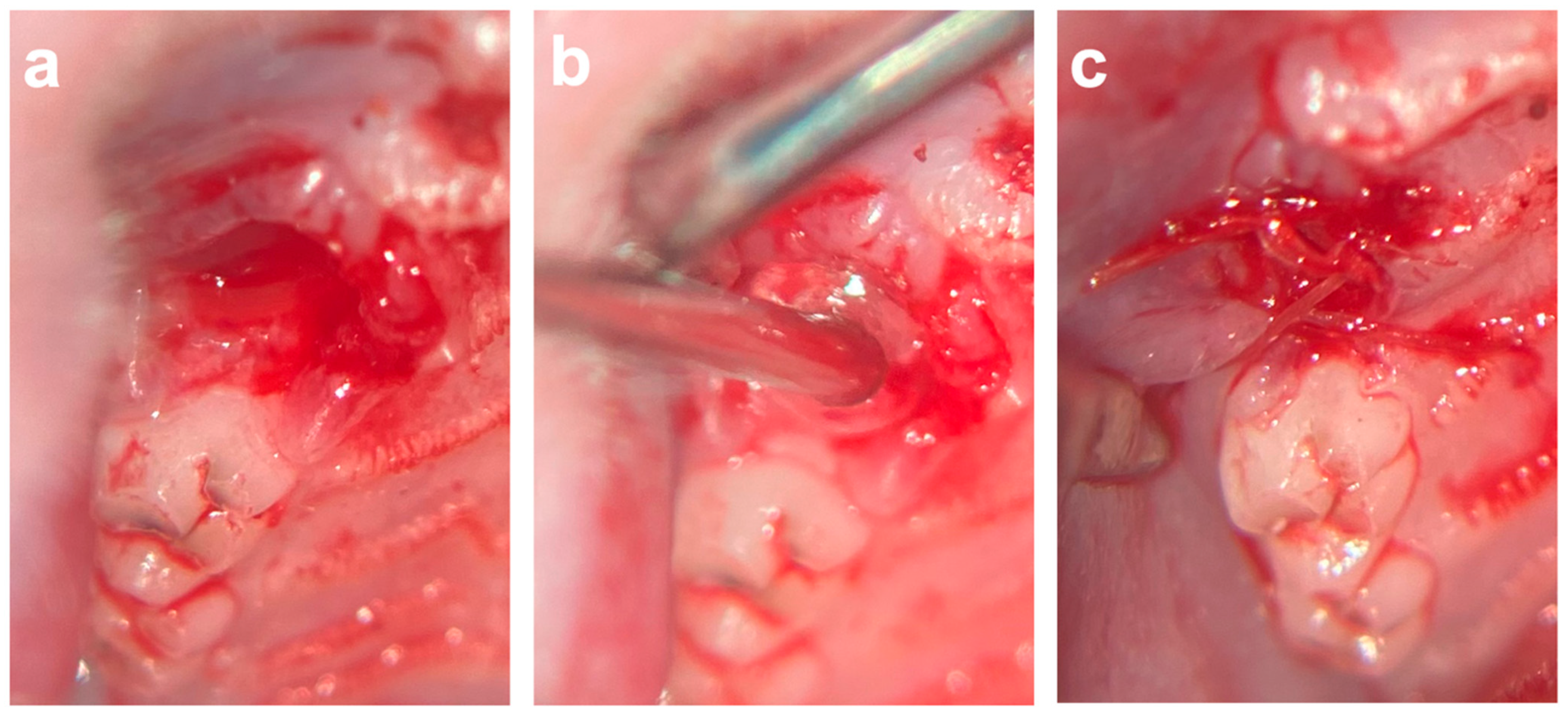
4.3. Surgical Procedures
4.4. Micro-Computed Tomography (µCT) Analysis
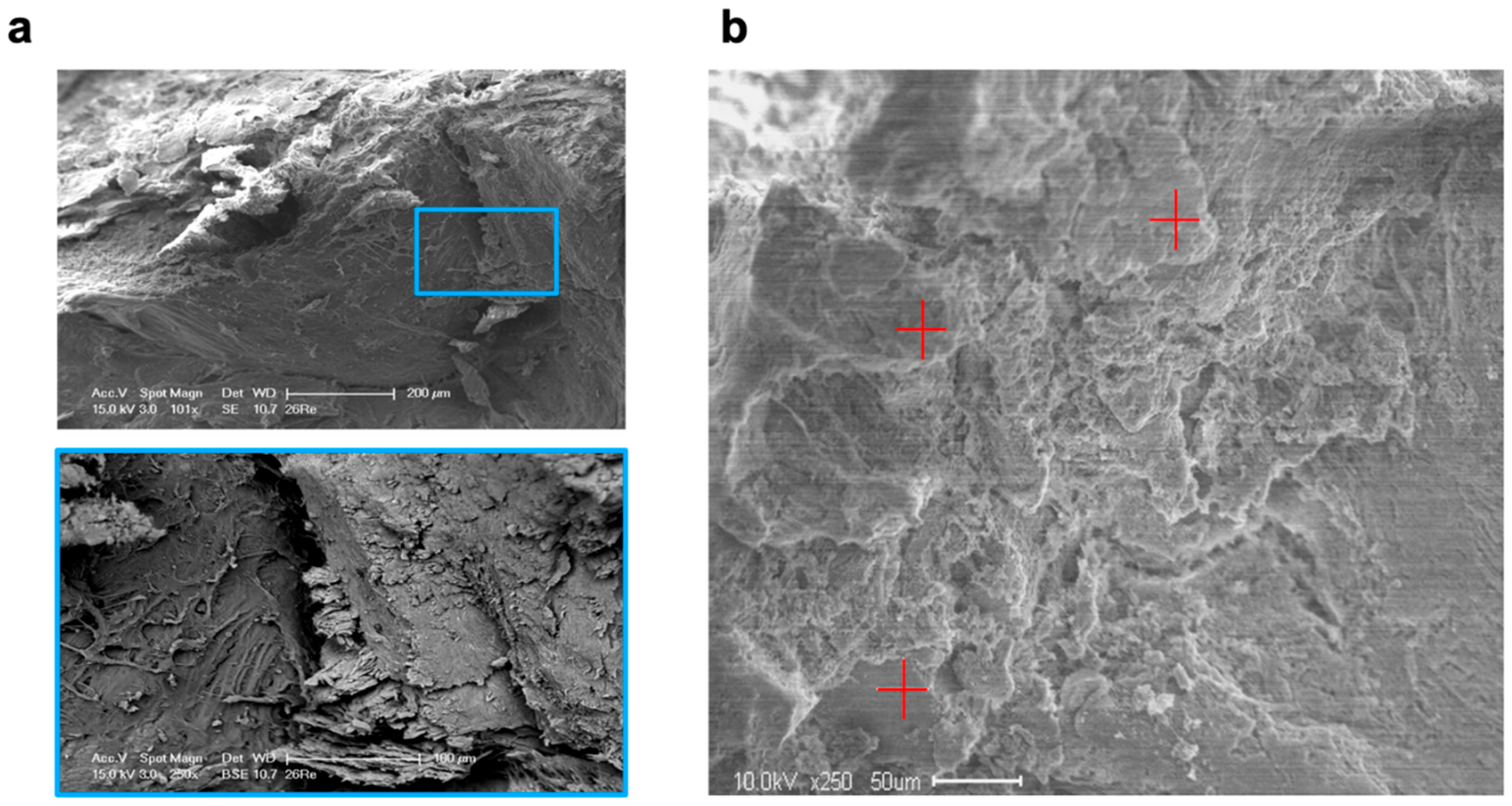
4.5. Scanning Electron Microscopy (SEM) and Energy-Dispersive X-ray Spectroscopy (EDX) Analysis
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMD | Bone mineral density |
| BV/TV | Bone volume fraction |
| C | Carbon |
| Ca | Calcium |
| COSP | Collagen sponge |
| d | Days |
| EDX | Energy-dispersive X-ray spectroscopy |
| µCT | Micro-computed tomography |
| P | Phosphate |
| SEM | Scanning electron microscopy |
| T | Time of radiological imaging |
| Tb.Sp | Trabecular separation |
| Tb.Th | Trabecular thickness |
References
- Gu, J.T.; Jiao, K.; Li, J.; Yan, J.F.; Wang, K.Y.; Wang, F.; Liu, Y.; Tay, F.R.; Chen, J.H.; Niu, L.N. Polyphosphate-crosslinked collagen scaffolds for hemostasis and alveolar bone regeneration after tooth extraction. Bioact. Mater. 2022, 15, 68–81. [Google Scholar] [CrossRef]
- Dang, H.; Chen, W.; Chen, L.; Huo, X.; Wang, F. TPPU inhibits inflammation-induced excessive autophagy to restore the osteogenic differentiation potential of stem cells and improves alveolar ridge preservation. Sci. Rep. 2023, 13, 1574. [Google Scholar] [CrossRef]
- Araujo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontol. 2000 2015, 68, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Khanal, N.; Acharya, N.; Rokaya, D.; Hasan, M.R.; Saito, T. Are Physics Forceps Less Traumatic than Conventional Forceps for Tooth Extraction? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Dent. J. 2022, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Wang, S.; He, Q.; Li, D.; Xin, L.; Xu, C.; Zhu, X.; Mei, L.; Cannon, R.D.; Ji, P.; et al. A Mechanically Reinforced Super Bone Glue Makes a Leap in Hard Tissue Strong Adhesion and Augmented Bone Regeneration. Adv. Sci. 2023, 10, e2206450. [Google Scholar] [CrossRef] [PubMed]
- Pippi, R.; Santoro, M.; Cafolla, A. The effectiveness of a new method using an extra-alveolar hemostatic agent after dental extractions in older patients on oral anticoagulation treatment: An intrapatient study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Kumbargere Nagraj, S.; Prashanti, E.; Aggarwal, H.; Lingappa, A.; Muthu, M.S.; Kiran Kumar Krishanappa, S.; Hassan, H. Interventions for treating post-extraction bleeding. Cochrane Database Syst. Rev. 2018, 3, CD011930. [Google Scholar] [CrossRef] [PubMed]
- Daigo, Y.; Daigo, E.; Fukuoka, H.; Fukuoka, N.; Ishikawa, M.; Takahashi, K. Wound Healing and Cell Dynamics Including Mesenchymal and Dental Pulp Stem Cells Induced by Photobiomodulation Therapy: An Example of Socket-Preserving Effects after Tooth Extraction in Rats and a Literature Review. Int. J. Mol. Sci. 2020, 21, 6850. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Alsabeeha, N.H.; Payne, A.G.; Ali, S.; Faggion, C.M.J.; Esposito, M. Interventions for replacing missing teeth: Alveolar ridge preservation techniques for dental implant site development. Cochrane Database Syst. Rev. 2021, 4, CD010176. [Google Scholar] [CrossRef]
- Yin, S.; Zhang, W.; Tang, Y.; Yang, G.; Wu, X.; Lin, S.; Liu, X.; Cao, H.; Jiang, X. Preservation of alveolar ridge height through mechanical memory: A novel dental implant design. Bioact. Mater. 2021, 6, 75–83. [Google Scholar] [CrossRef]
- Zhang, W.; Yu, M.; Cao, Y.; Zhuang, Z.; Zhang, K.; Chen, D.; Liu, W.; Yin, J. An anti-bacterial porous shape memory self-adaptive stiffened polymer for alveolar bone regeneration after tooth extraction. Bioact. Mater. 2023, 21, 450–463. [Google Scholar] [CrossRef] [PubMed]
- Berton, F.; Costantinides, F.; Stacchi, C.; Corradini, A.; Di Lenarda, A.; Di Lenarda, R. Is L-PRF an effective hemostatic agent in single tooth extractions? A cohort study on VKA and DOAC patients. Clin. Oral Investig. 2023, 27, 2865–2874. [Google Scholar] [CrossRef] [PubMed]
- Poxleitner, P.; Steybe, D.; Kroneberg, P.; Ermer, M.A.; Yalcin-Ulker, G.M.; Schmelzeisen, R.; Voss, P.J. Tooth extractions in patients under antiresorptive therapy for osteoporosis: Primary closure of the extraction socket with a mucoperiosteal flap versus application of platelet-rich fibrin for the prevention of antiresorptive agent-related osteonecrosis of the jaw. J. Craniomaxillofac. Surg. 2020, 48, 444–451. [Google Scholar]
- Heitzer, M.; Winnand, P.; Bock, A.; Ooms, M.; Katz, M.S.; Kniha, K.; Grottke, O.; Holzle, F.; Modabber, A. Evaluation of the Hemostatic Effect of an Innovative Tissue Adhesive during Extraction Therapy under Rivaroxaban in a Rodent Model. J. Funct. Biomater. 2023, 14, 333. [Google Scholar] [CrossRef]
- Kalsi, A.S.; Kalsi, J.S.; Bassi, S. Alveolar ridge preservation: Why, when and how. Br. Dent. J. 2019, 227, 264–274. [Google Scholar] [CrossRef]
- Kang, H.-J.; Park, S.-S.; Saleh, T.; Ahn, K.-M.; Lee, B.-T. In vitro and in vivo evaluation of Ca/P-hyaluronic acid/gelatin based novel dental plugs for one-step socket preservation. Mater. Des. 2020, 194, 108891. [Google Scholar] [CrossRef]
- Dudek, D.; Marchionni, S.; Gabriele, M.; Iurlaro, A.; Helewski, K.; Toti, P.; Gelpi, F.; Bertossi, D.; Barone, A. Bleeding Rate After Tooth Extraction in Patients Under Oral Anticoagulant Therapy. J. Craniofac. Surg. 2016, 27, 1228–1233. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Saito, T. Novel Bioactive Adhesive Monomer CMET Promotes Odontogenic Differentiation and Dentin Regeneration. Int. J. Mol. Sci. 2021, 22, 12728. [Google Scholar] [CrossRef] [PubMed]
- Malysa, A.; Wezgowiec, J.; Grzebieluch, W.; Danel, D.P.; Wieckiewicz, M. Effect of Thermocycling on the Bond Strength of Self-Adhesive Resin Cements Used for Luting CAD/CAM Ceramics to Human Dentin. Int. J. Mol. Sci. 2022, 23, 745. [Google Scholar] [CrossRef]
- Schulten, L.; Spillner, J.; Kanzler, S.; Teubner, A.; Jockenhoevel, S.; Apel, C. A polyurethane-based surgical adhesive for sealing blood vessel anastomoses-A feasibility study in pigs. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 1922–1931. [Google Scholar] [CrossRef]
- Fukushima, K.; Tanaka, H.; Kadaba Srinivasan, P.; Pawlowsky, K.; Kogel, B.; Uemoto, S.; Ku, Y.; Tolba, R.H. Hemostatic Efficacy and Safety of the Novel Medical Adhesive, MAR VIVO-107, in a Rabbit Liver Resection Model. Eur. Surg. Res. 2018, 59, 48–57. [Google Scholar] [CrossRef]
- Nevins, M.; Mendoza-Azpur, G.; De Angelis, N.; Kim, D.M. The Biocompatibility of Cyanoacrylate Tissue Adhesive in Conjunction with a Collagen Membrane for Providing Soft and Hard Tissue Regeneration in Extraction Socket Preservation Procedures. Int. J. Periodontics Restor. Dent. 2018, 38, s37–s42. [Google Scholar] [CrossRef]
- Maia, G.V.; Sousa, C.W.; de Lima, J.C.R.; Vecchio, J.L.; de Barros Silva, P.G.; de Souza Carvalho, A.C.G. Cyanoacrylate glue in socket repair: A comparative study. Br. J. Oral. Maxillofac. Surg. 2022, 60, 145–151. [Google Scholar] [CrossRef]
- Niu, Q.; He, J.; Wu, M.; Liu, J.; Lu, X.; Zhang, L.; Jin, Z. Transplantation of bone marrow mesenchymal stem cells and fibrin glue into extraction socket in maxilla promoted bone regeneration in osteoporosis rat. Life Sci. 2022, 290, 119480. [Google Scholar] [CrossRef]
- Gao, S.Y.; Lin, R.B.; Huang, S.H.; Liang, Y.J.; Li, X.; Zhang, S.E.; Ouyang, D.Q.; Li, K.; Zheng, G.S.; Liao, G.Q. PDGF-BB exhibited therapeutic effects on rat model of bisphosphonate-related osteonecrosis of the jaw by enhancing angiogenesis and osteogenesis. Bone 2021, 144, 115117. [Google Scholar] [CrossRef] [PubMed]
- Bremer, L.; Hagemeister, K.; Moss, M.; Ernst, L.; Tolba, R.H.; Jockenhoevel, S.; Apel, C. Long-Term Degradation Assessment of a Polyurethane-Based Surgical Adhesive-Assessment and Critical Consideration of Preclinical In Vitro and In Vivo Testing. J. Funct. Biomater. 2023, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Hulsart-Billstrom, G.; Dawson, J.I.; Hofmann, S.; Muller, R.; Stoddart, M.J.; Alini, M.; Redl, H.; El Haj, A.; Brown, R.; Salih, V.; et al. A surprisingly poor correlation between in vitro and in vivo testing of biomaterials for bone regeneration: Results of a multicentre analysis. Eur. Cell Mater. 2016, 31, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Kniha, K.; Bock, A.; Peters, F.; Magnuska, Z.A.; Gremse, F.; Mohlhenrich, S.C.; Holzle, F.; Modabber, A. Microstructural volumetric analysis of the jaw following dental implantation under systemic bisphosphonate delivery: An in vivo and ex vivo rat study. J. Periodontol. 2021, 92, 66–75. [Google Scholar] [CrossRef]
- Hatt, L.P.; Thompson, K.; Helms, J.A.; Stoddart, M.J.; Armiento, A.R. Clinically relevant preclinical animal models for testing novel cranio-maxillofacial bone 3D-printed biomaterials. Clin. Transl. Med. 2022, 12, e690. [Google Scholar] [CrossRef]
- Sculean, A.; Stavropoulos, A.; Bosshardt, D.D. Self-regenerative capacity of intra-oral bone defects. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 70–81. [Google Scholar] [CrossRef]
- Yang, Y.; Su, S.; Liu, S.; Liu, W.; Yang, Q.; Tian, L.; Tan, Z.; Fan, L.; Yu, B.; Wang, J.; et al. Triple-functional bone adhesive with enhanced internal fixation, bacteriostasis and osteoinductive properties for open fracture repair. Bioact. Mater. 2023, 25, 273–290. [Google Scholar] [CrossRef] [PubMed]
- Mohlhenrich, S.C.; Kniha, K.; Heitzer, M.; Magnuska, Z.; Hermanns-Sachweh, B.; Gremse, F.; Chhatwani, S.; Holzle, F.; Modabber, A.; Danesh, G. Correlations between radiological and histological findings of bone remodelling and root resorption in a rodent cleft model. Head. Face Med. 2022, 18, 33. [Google Scholar] [CrossRef]
- Muller, R.; Van Campenhout, H.; Van Damme, B.; Van Der Perre, G.; Dequeker, J.; Hildebrand, T.; Ruegsegger, P. Morphometric analysis of human bone biopsies: A quantitative structural comparison of histological sections and micro-computed tomography. Bone 1998, 23, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Kniha, K.; Buhl, E.M.; Al-Sibai, F.; Mohlhenrich, S.C.; Bock, A.; Heitzer, M.; Holzle, F.; Modabber, A. Results of thermal osteonecrosis for implant removal on electron microscopy, implant stability, and radiographic parameters—A rat study. Head. Face Med. 2023, 19, 4. [Google Scholar] [CrossRef] [PubMed]
- Kourkoumelis, N.; Balatsoukas, I.; Tzaphlidou, M. Ca/P concentration ratio at different sites of normal and osteoporotic rabbit bones evaluated by Auger and energy dispersive X-ray spectroscopy. J. Biol. Phys. 2012, 38, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. PLoS Biol. 2020, 18, e3000410. [Google Scholar]
- Gremse, F.; Stark, M.; Ehling, J.; Menzel, J.R.; Lammers, T.; Kiessling, F. Imalytics Preclinical: Interactive Analysis of Biomedical Volume Data. Theranostics 2016, 6, 328–341. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 5 Days (n = 29) | 10 Days (n = 31) | 90 Days (n = 29) | ||||
|---|---|---|---|---|---|---|
| Parameter | COSP | VIVO | COSP | VIVO | COSP | VIVO |
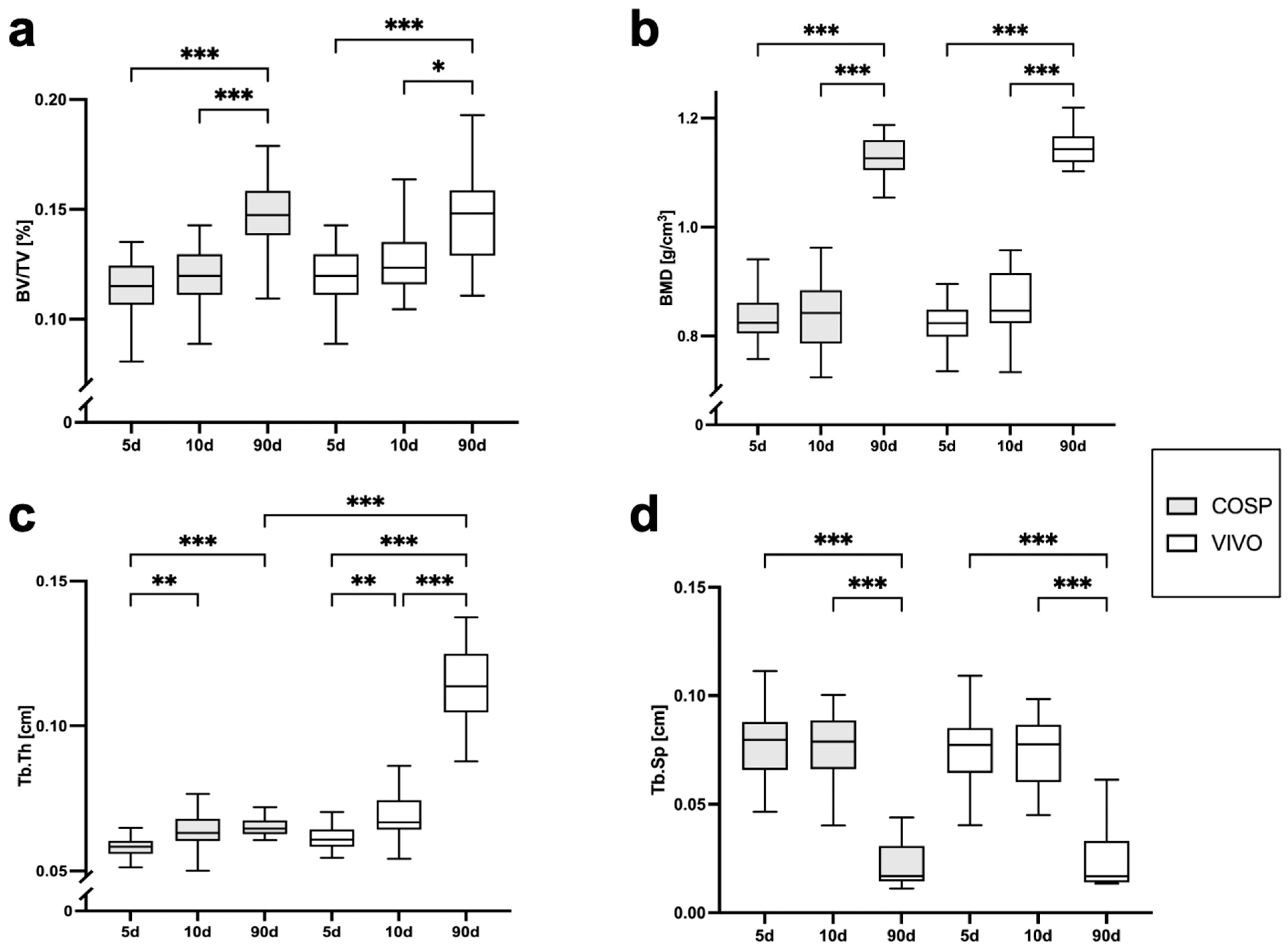
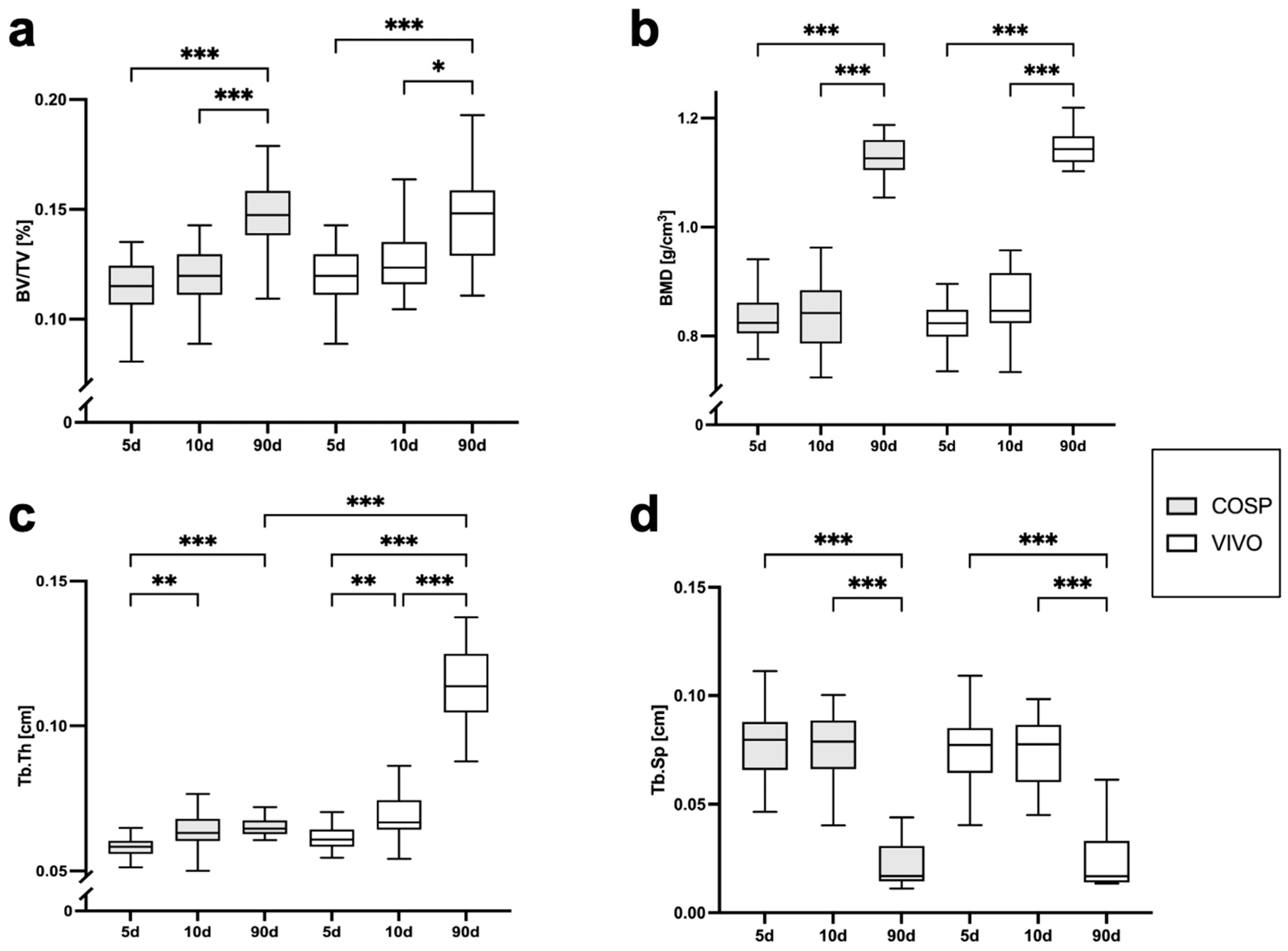
| BV/TV [%] | 0.113 ± 0.016 | 0.12 ± 0.129 | 0.120 ± 0.013 | 0.127 ± 0.015 | 0.148 ± 0.017 | 0.146 ± 0.02 |
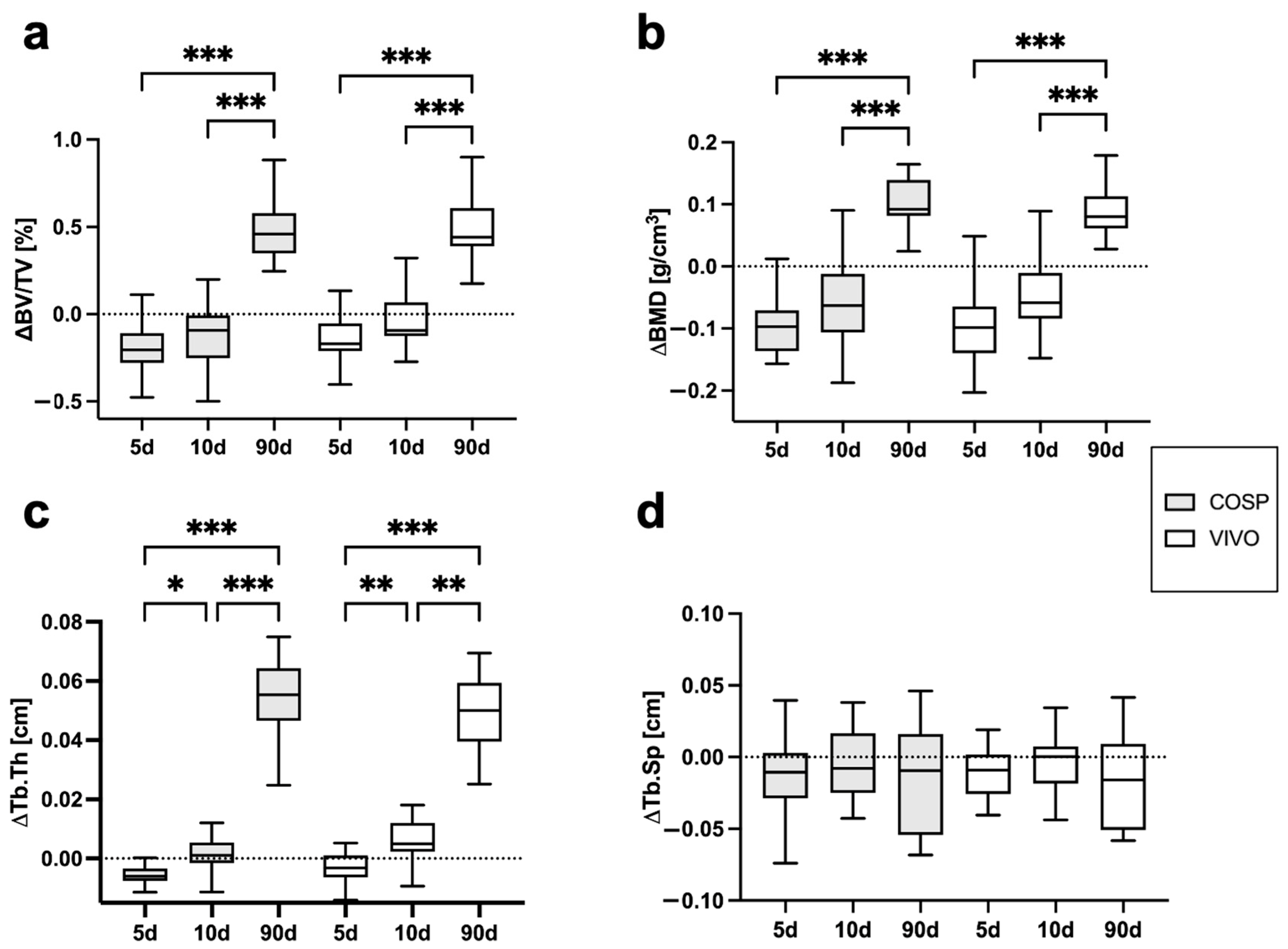
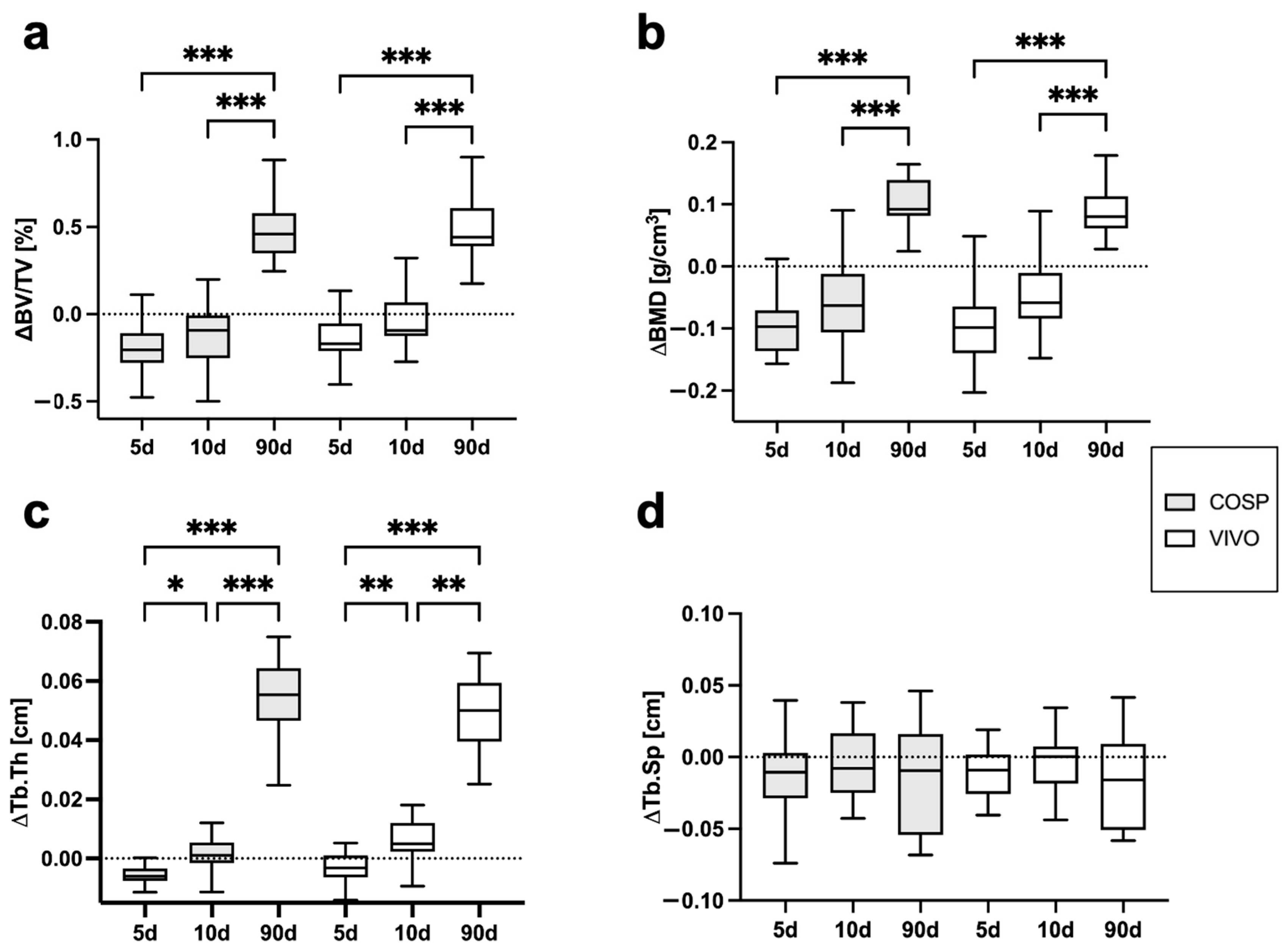
| ΔBV/TV [%] | −0.207 ± 0.155 | −0.144 ± 0.129 | −0.112 ± 0.178 | −0.04 ± 0.144 | 0.463 ± 0.293 | 0.479 ± 0.201 |
| BMD [g/cm3] | 0.836 ± 0.051 | 0.831 ± 0.063 | 0.814 ± 0.16 | 0.861 ± 0.06 | 1.129 ± 0.04 | 1.143 ± 0.035 |
| ΔBMD [g/cm3] | −0.097 ± 0.064 | −0.098 ± 0.075 | −0.061 ± 0.064 | −0.049 ± 0.061 | 0.108 ± 0.049 | 0.093 ± 0.041 |
| Tb.Th [cm] | 0.058 ± 0.033 | 0.062 ± 0.004 | 0.064 ± 0.005 | 0.069 ± 0.007 | 0.065 ± 0.004 | 0.113 ± 0.015 |
| ΔTb.Th [cm] | −0.006 ± 0.034 | −0.003 ± 0.005 | 0.001 ± 0.005 | 0.006 ± 0.007 | 0.053 ± 0.016 | 0.048 ± 0.015 |
| Tb.Sp [cm] | 0.075 ± 0.022 | 0.074 ± 0.018 | 0.075 ± 0.017 | 0.075 ± 0.019 | 0.025 ± 0.016 | 0.026 ± 0.017 |
| ΔTb.Sp [cm] | −0.015 ± 0.033 | −0.015 ± 0.032 | −0.004 ± 0.024 | −0.003 ± 0.026 | −0.015 ± 0.037 | −0.017 ± 0.032 |
| 5 Days | 10 Days | 90 Days | |||||
|---|---|---|---|---|---|---|---|
| Parameter | COSP | VIVO | COSP | VIVO | COSP | VIVO | p Value |
| Weight (%) | |||||||
| Calcium | 4.59 ± 7.14 | 1.81 ± 2.72 | 10.36 ± 11.61 | 8.46 ± 6.58 | 20.21 ± 6.13 | 20.77 ± 15.9 | NS |
| Carbon | 13.45 ± 6.84 | 32.16 ± 19.95 | 13.97 ± 5.91 | 36.75 ± 19.73 | 35.24 ± 12.53 | 43.66 ± 8.52 | NS |
| Oxygen | 6.90 ± 4.00 | 5.72 ± 3.98 | 6.95 ± 6.83 | 12.58 ± 5.37 | 16.66 ± 5.75 | 17.15 ± 9.72 | NS |
| Sodium | 0.68 ± 0.47 | 0.78 ± 0.40 | 1.22 ± 0.46 | 1.95 ± 0.69 | 1.19 ± 0.66 | 0.96 ± 0.59 | NS |
| Phosphate | 4.40 ± 3.92 | 3.64 ± 1.86 | 8.04 ± 6.47 | 6.05 ± 3.97 | 12.62 ± 2.63 | 15.01 ± 6.09 | NS |
| Sulphur | 0.79 ± 0.68 | 0.32 ± 0.27 | 0.41 ± 0.42 | 0.20 ± 0.19 | 0.05 ± 0.11 | 0.28 ± 0.38 | NS |
| Ratios | |||||||
| Ca/C | 0.34 | 0.06 | 0.74 | 0.23 | 0.57 | 0.48 | |
| Ca/P | 1.04 | 0.5 | 1.29 | 1.4 | 1.6 | 1.38 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heitzer, M.; Winnand, P.; Ooms, M.; Magnuska, Z.; Kiessling, F.; Buhl, E.M.; Hölzle, F.; Modabber, A. A Biodegradable Tissue Adhesive for Post-Extraction Alveolar Bone Regeneration under Ongoing Anticoagulation—A Microstructural Volumetric Analysis in a Rodent Model. Int. J. Mol. Sci. 2024, 25, 4210. https://doi.org/10.3390/ijms25084210
Heitzer M, Winnand P, Ooms M, Magnuska Z, Kiessling F, Buhl EM, Hölzle F, Modabber A. A Biodegradable Tissue Adhesive for Post-Extraction Alveolar Bone Regeneration under Ongoing Anticoagulation—A Microstructural Volumetric Analysis in a Rodent Model. International Journal of Molecular Sciences. 2024; 25(8):4210. https://doi.org/10.3390/ijms25084210
Chicago/Turabian StyleHeitzer, Marius, Philipp Winnand, Mark Ooms, Zuzanna Magnuska, Fabian Kiessling, Eva Miriam Buhl, Frank Hölzle, and Ali Modabber. 2024. "A Biodegradable Tissue Adhesive for Post-Extraction Alveolar Bone Regeneration under Ongoing Anticoagulation—A Microstructural Volumetric Analysis in a Rodent Model" International Journal of Molecular Sciences 25, no. 8: 4210. https://doi.org/10.3390/ijms25084210
APA StyleHeitzer, M., Winnand, P., Ooms, M., Magnuska, Z., Kiessling, F., Buhl, E. M., Hölzle, F., & Modabber, A. (2024). A Biodegradable Tissue Adhesive for Post-Extraction Alveolar Bone Regeneration under Ongoing Anticoagulation—A Microstructural Volumetric Analysis in a Rodent Model. International Journal of Molecular Sciences, 25(8), 4210. https://doi.org/10.3390/ijms25084210