
Elevated Biomarkers of Inflammation and Vascular Dysfunction Are Associated with Distal Sensory Polyneuropathy in People with HIV
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Participants
2.2. Factor Analysis
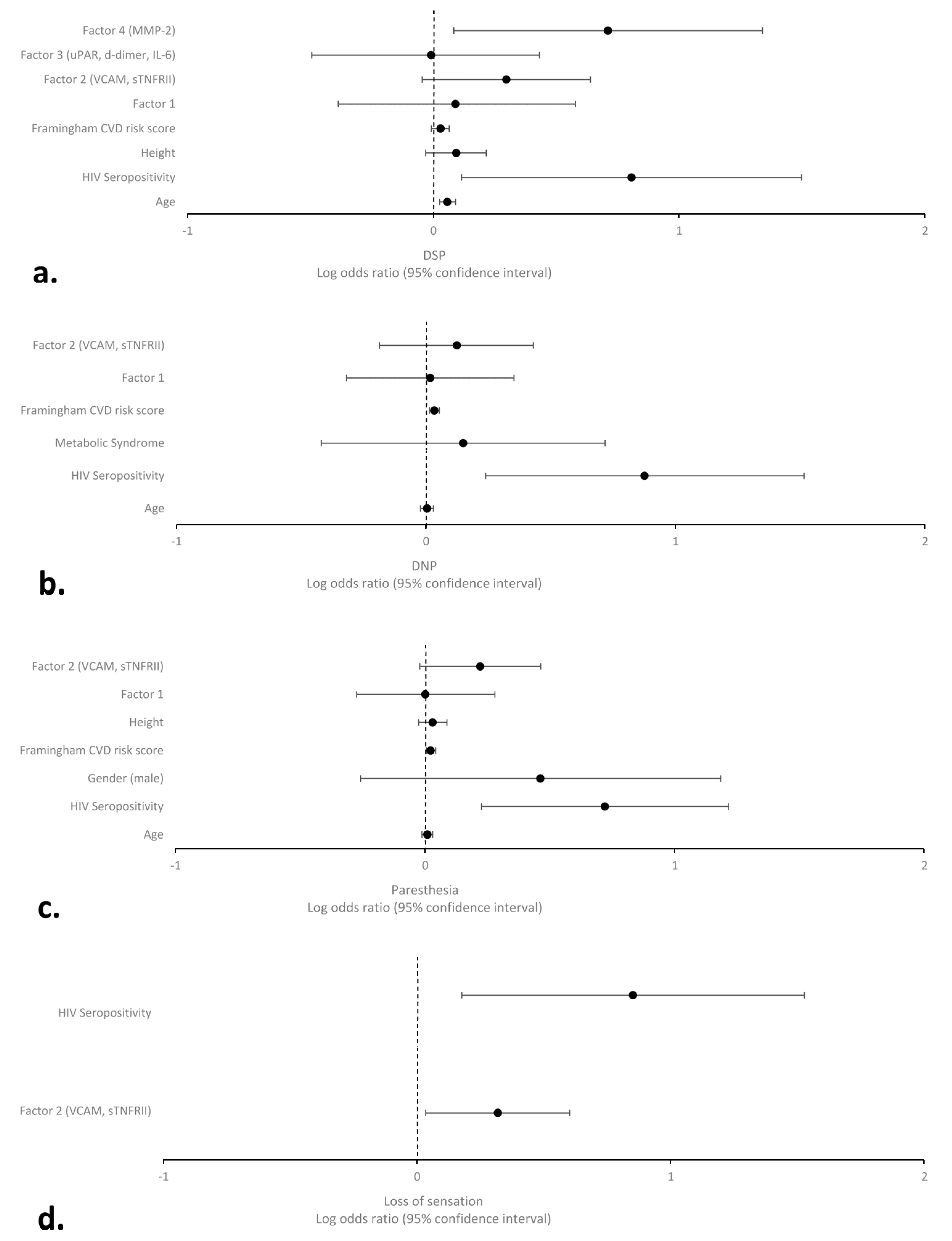
2.3. Association of Plasma Biomarkers of Inflammation and Vascular Integrity with DSP Signs and Symptoms
2.4. Causal Mediation Analyses of Factor 2 (sTNFRII and VCAM) on the Relationships between HIV Serostatus and DSP Signs and Symptoms
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Clinical Evaluations
Distal Sensory Polyneuropathy (DSP) Evaluations
4.3. Laboratory Evaluations
4.4. HIV-Related Assessments and Potential Confounders
4.5. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aziz-Donnelly, A.; Harrison, T.B. Update of HIV-Associated Sensory Neuropathies. Curr. Treat. Options Neurol. 2017, 19, 36. [Google Scholar] [CrossRef]
- Ellis, R.J.; Rosario, D.; Clifford, D.B.; McArthur, J.C.; Simpson, D.; Alexander, T.; Gelman, B.B.; Vaida, F.; Collier, A.; Marra, C.M.; et al. Continued High Prevalence and Adverse Clinical Impact of Human Immunodeficiency Virus–Associated Sensory Neuropathy in the Era of Combination Antiretroviral Therapy: The CHARTER Study. Arch. Neurol. 2010, 67, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Sakabumi, D.Z.; Moore, R.C.; Tang, B.; Delaney, P.A.; Keltner, J.R.; Ellis, R.J. Chronic Distal Sensory Polyneuropathy Is a Major Contributor to Balance Disturbances in Persons Living With HIV. J. Acquir. Immune Defic. Syndr. 2019, 80, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Mugisha, J.; Richards, J.; De Hert, M.; Probst, M.; Stubbs, B. Physical activity correlates in people living with HIV/AIDS: A systematic review of 45 studies. Disabil. Rehabil. 2018, 40, 1618–1629. [Google Scholar] [CrossRef] [PubMed]
- Rusch, M.; Nixon, S.; Schilder, A.; Braitstein, P.; Chan, K.; Hogg, R.S. Impairments, activity limitations and participation restrictions: Prevalence and associations among persons living with HIV/AIDS in British Columbia. Health Qual. Life Outcomes 2004, 2, 46. [Google Scholar] [CrossRef]
- Bernard, C.; Font, H.; Diallo, Z.; Ahonon, R.; Tine, J.M.; Abouo, F.; Tanon, A.; Messou, E.; Seydi, M.; Dabis, F.; et al. Prevalence and factors associated with physical function limitation in older West African people living with HIV. PLoS ONE 2020, 15, e0240906. [Google Scholar] [CrossRef] [PubMed]
- Jazebi, N.; Evans, C.; Kadaru, H.S.; Kompella, D.; Raji, M.; Fang, F.; Pappolla, M.; Tang, S.J.; Chung, J.M.; Hammock, B.; et al. HIV-related Neuropathy: Pathophysiology, Treatment and Challenges. J. Neurol. Exp. Neurosci. 2021, 7, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Van der Watt, J.J.; Wilkinson, K.A.; Wilkinson, R.J.; Heckmann, J.M. Plasma cytokine profiles in HIV-1 infected patients developing neuropathic symptoms shortly after commencing antiretroviral therapy: A case-control study. BMC Infect. Dis. 2014, 14, 71. [Google Scholar] [CrossRef] [PubMed]
- Hahn, K.; Robinson, B.; Anderson, C.; Li, W.; Pardo, C.A.; Morgello, S.; Simpson, D.; Nath, A. Differential effects of HIV infected macrophages on dorsal root ganglia neurons and axons. Exp. Neurol. 2008, 210, 30–40. [Google Scholar] [CrossRef] [PubMed]
- de la Monte, S.M.; Gabuzda, D.H.; Ho, D.D.; Brown, R.H., Jr.; Hedley-Whyte, E.T.; Schooley, R.T.; Hirsch, M.S.; Bhan, A.K. Peripheral neuropathy in the acquired immunodeficiency syndrome. Ann. Neurol. 1988, 23, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Jones, G.; Tsutsui, S.; Opii, W.; Liu, S.; Silva, C.; Butterfield, D.A.; Power, C. Lentivirus infection causes neuroinflammation and neuronal injury in dorsal root ganglia: Pathogenic effects of STAT-1 and inducible nitric oxide synthase. J. Immunol. 2005, 175, 1118–1126. [Google Scholar] [CrossRef]
- Kennedy, J.M.; Hoke, A.; Zhu, Y.; Johnston, J.B.; van Marle, G.; Silva, C.; Zochodne, D.W.; Power, C. Peripheral neuropathy in lentivirus infection: Evidence of inflammation and axonal injury. Aids 2004, 18, 1241–1250. [Google Scholar] [CrossRef]
- Vincent, A.M.; Hayes, J.M.; McLean, L.L.; Vivekanandan-Giri, A.; Pennathur, S.; Feldman, E.L. Dyslipidemia-induced neuropathy in mice: The role of oxLDL/LOX-1. Diabetes 2009, 58, 2376–2385. [Google Scholar] [CrossRef] [PubMed]
- Pek, S.L.T.; Lim, S.C.; Ang, K.; Kwan, P.Y.; Tang, W.E.; Sum, C.F.; Tavintharan, S. Endothelin-1 predicts incident diabetic peripheral neuropathy in Type 2 Diabetes: A cohort study. Eur. J. Endocrinol. 2020, 182, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou-Marketou, N.; Whiss, P.A.; Eriksson, A.C.; Hyllienmark, L.; Papassotiriou, I.; Wahlberg, J. Plasma levels of tissue inhibitor of metalloproteinase-1 in patients with type 1 diabetes mellitus associate with early diabetic neuropathy and nephropathy. Diab Vasc. Dis. Res. 2021, 18, 14791641211002470. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Ma, P.; Wu, M.; Liao, H.; Song, X.J. Role of Matrix Metalloproteinases in Myelin Abnormalities and Mechanical Allodynia in Rodents with Diabetic Neuropathy. Aging Dis. 2021, 12, 1808–1820. [Google Scholar] [CrossRef]
- Marcianò, G.; Vocca, C.; Rania, V.; Citraro, R.; De Sarro, G.; Gallelli, L. Metalloproteases in Pain Generation and Persistence: A Possible Target? Biomolecules 2023, 13, 268. [Google Scholar] [CrossRef]
- Fields, J.; Gardner-Mercer, J.; Borgmann, K.; Clark, I.; Ghorpade, A. CCAAT/enhancer binding protein β expression is increased in the brain during HIV-1-infection and contributes to regulation of astrocyte tissue inhibitor of metalloproteinase-1. J. Neurochem. 2011, 118, 93–104. [Google Scholar] [CrossRef]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int. J. Mol. Sci. 2020, 21, 9739. [Google Scholar] [CrossRef] [PubMed]
- Tavasoli, A.; Gelman, B.B.; Marra, C.M.; Clifford, D.B.; Iudicello, J.E.; Rubin, L.H.; Letendre, S.L.; Tang, B.; Ellis, R.J. Increasing Neuroinflammation Relates to Increasing Neurodegeneration in People with HIV. Viruses 2023, 15, 1835. [Google Scholar] [CrossRef]
- Solanky, D.; Fields, J.A.; Iudicello, J.E.; Ellis, R.J.; Franklin, D.; Clifford, D.B.; Gelman, B.B.; Marra, C.M.; Morgello, S.; Rubin, L.H.; et al. Higher buccal mitochondrial DNA and mitochondrial common deletion number are associated with markers of neurodegeneration and inflammation in cerebrospinal fluid. J. Neurovirol 2022, 28, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Denny, H.; Smith, C.; Granados, J.; Renden, R. Presynaptic loss of dynamin-related protein 1 impairs synaptic vesicle release and recycling at the mouse calyx of Held. J. Physiol. 2018, 596, 6263–6287. [Google Scholar] [CrossRef] [PubMed]
- Fields, J.A.; Serger, E.; Campos, S.; Divakaruni, A.S.; Kim, C.; Smith, K.; Trejo, M.; Adame, A.; Spencer, B.; Rockenstein, E.; et al. HIV alters neuronal mitochondrial fission/fusion in the brain during HIV-associated neurocognitive disorders. Neurobiol. Dis. 2016, 86, 154–169. [Google Scholar] [CrossRef]
- Ferrari, L.F.; Chum, A.; Bogen, O.; Reichling, D.B.; Levine, J.D. Role of Drp1, a Key Mitochondrial Fission Protein, in Neuropathic Pain. J. Neurosci. 2011, 31, 11404–11410. [Google Scholar] [CrossRef]
- Haileselassie, B.; Joshi, A.U.; Minhas, P.S.; Mukherjee, R.; Andreasson, K.I.; Mochly-Rosen, D. Mitochondrial dysfunction mediated through dynamin-related protein 1 (Drp1) propagates impairment in blood brain barrier in septic encephalopathy. J. Neuroinflammation 2020, 17, 36. [Google Scholar] [CrossRef]
- DosSantos, M.F.; Holanda-Afonso, R.C.; Lima, R.L.; DaSilva, A.F.; Moura-Neto, V. The role of the blood-brain barrier in the development and treatment of migraine and other pain disorders. Front. Cell Neurosci. 2014, 8, 302. [Google Scholar] [CrossRef] [PubMed]
- Uçeyler, N.; Rogausch, J.P.; Toyka, K.V.; Sommer, C. Differential expression of cytokines in painful and painless neuropathies. Neurology 2007, 69, 42–49. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, C.; Lan, X.; Li, H.; Chao, Z.; Ning, Y. Plasma inflammatory cytokines and treatment-resistant depression with comorbid pain: Improvement by ketamine. J. Neuroinflammation 2021, 18, 200. [Google Scholar] [CrossRef]
- Ellis, R.J.; Chenna, A.; Lie, Y.; Curanovic, D.; Winslow, J.; Tang, B.; Marra, C.M.; Rubin, L.H.; Clifford, D.B.; McCutchan, J.A.; et al. Higher Levels of Cerebrospinal Fluid and Plasma Neurofilament Light in Human Immunodeficiency Virus-Associated Distal Sensory Polyneuropathy. Clin. Infect. Dis. 2022, 76, 1103–1109. [Google Scholar] [CrossRef]
- Diaz, M.M.; Caylor, J.; Strigo, I.; Lerman, I.; Henry, B.; Lopez, E.; Wallace, M.S.; Ellis, R.J.; Simmons, A.N.; Keltner, J.R. Toward Composite Pain Biomarkers of Neuropathic Pain—Focus on Peripheral Neuropathic Pain. Front. Pain Res. 2022, 3, 869215. [Google Scholar] [CrossRef]
- Njoku, U.C.; Amadi, P.U.; Agomuo, E.N.; Bhebhe, M. The Relationship between Pain and Vascular Function Biomarkers in Dysmenorrheal University Students. Chonnam Med. J. 2020, 56, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Luchting, B.; Hinske, L.C.G.; Rachinger-Adam, B.; Celi, L.A.; Kreth, S.; Azad, S.C. Soluble intercellular adhesion molecule-1: A potential biomarker for pain intensity in chronic pain patients. Biomark. Med. 2017, 11, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Doupis, J.; Lyons, T.E.; Wu, S.; Gnardellis, C.; Dinh, T.; Veves, A. Microvascular reactivity and inflammatory cytokines in painful and painless peripheral diabetic neuropathy. J. Clin. Endocrinol. Metab. 2009, 94, 2157–2163. [Google Scholar] [CrossRef] [PubMed]
- Mu, Z.-P.; Wang, Y.-G.; Li, C.-Q.; Lv, W.-S.; Wang, B.; Jing, Z.-H.; Song, X.-J.; Lun, Y.; Qiu, M.-Y.; Ma, X.-L. Association between tumor necrosis factor-α and diabetic peripheral neuropathy in patients with type 2 diabetes: A meta-analysis. Mol. Neurobiol. 2017, 54, 983–996. [Google Scholar] [CrossRef]
- Nadeau, S.; Filali, M.; Zhang, J.; Kerr, B.J.; Rivest, S.; Soulet, D.; Iwakura, Y.; de Rivero Vaccari, J.P.; Keane, R.W.; Lacroix, S. Functional recovery after peripheral nerve injury is dependent on the pro-inflammatory cytokines IL-1β and TNF: Implications for neuropathic pain. J. Neurosci. 2011, 31, 12533–12542. [Google Scholar] [CrossRef]
- Ellis, R.J.; Diaz, M.; Sacktor, N.; Marra, C.; Collier, A.C.; Clifford, D.B.; Calcutt, N.; Fields, J.A.; Heaton, R.K.; Letendre, S.L. Predictors of worsening neuropathy and neuropathic pain after 12 years in people with HIV. Ann. Clin. Transl. Neurol. 2020, 7, 1166–1173. [Google Scholar] [CrossRef] [PubMed]
- Gabbai, A.A.; Castelo, A.; Oliveira, A.S.B. Chapter 29-HIV peripheral neuropathy. In Handbook of Clinical Neurology; Said, G., Krarup, C., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 115, pp. 515–529. [Google Scholar]
- Ances, B.M.; Vaida, F.; Rosario, D.; Marquie-Beck, J.; Ellis, R.J.; Simpson, D.M.; Clifford, D.B.; McArthur, J.C.; Grant, I.; McCutchan, J.A. Role of metabolic syndrome components in HIV-associated sensory neuropathy. Aids 2009, 23, 2317–2322. [Google Scholar] [CrossRef] [PubMed]
- Robinson-Papp, J.; Morgello, S.; Vaida, F.; Fitzsimons, C.; Simpson, D.M.; Elliott, K.J.; Al-Lozi, M.; Gelman, B.B.; Clifford, D.; Marra, C.M.; et al. Association of self-reported painful symptoms with clinical and neurophysiologic signs in HIV-associated sensory neuropathy. PAIN 2010, 151, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, B.C.; Price, R.S.; Feldman, E.L. Distal Symmetric Polyneuropathy: A Review. Jama 2015, 314, 2172–2181. [Google Scholar] [CrossRef]
- Diaz, M.M.; Keltner, J.R.; Simmons, A.N.; Franklin, D.; Moore, R.C.; Clifford, D.; Collier, A.C.; Gelman, B.B.; Christina Marra, P.D.; McCutchan, J.A.; et al. Paresthesia Predicts Increased Risk of Distal Neuropathic Pain in Older People with HIV-Associated Sensory Polyneuropathy. Pain Med. 2021, 22, 1850–1856. [Google Scholar] [CrossRef]
- Galantino, M.L.; Kietrys, D.M.; Parrott, J.S.; Stevens, M.E.; Stevens, A.M.; Condoluci, D.V. Quality of life and self-reported lower extremity function in adults with HIV-related distal sensory polyneuropathy. Phys. Ther. 2014, 94, 1455–1466. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.J.; Sacktor, N.; Clifford, D.B.; Marra, C.M.; Collier, A.C.; Gelman, B.; Robinson-Papp, J.; Letendre, S.L.; Heaton, R.K.; CNS Antiretroviral Therapy Effects Research (CHARTER) Study Group. Neuropathic pain correlates with worsening cognition in people with human immunodeficiency virus. Brain 2022, 145, 2206–2213. [Google Scholar] [CrossRef]
- Evans, S.R.; Ellis, R.J.; Chen, H.; Yeh, T.M.; Lee, A.J.; Schifitto, G.; Wu, K.; Bosch, R.J.; McArthur, J.C.; Simpson, D.M.; et al. Peripheral neuropathy in HIV: Prevalence and risk factors. Aids 2011, 25, 919–928. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef]
- Tu, W.; Johnson, E.; Fujiwara, E.; Gill, M.J.; Kong, L.; Power, C. Predictive variables for peripheral neuropathy in treated HIV type 1 infection revealed by machine learning. AIDS 2021, 35, 1785–1793. [Google Scholar] [CrossRef]
- Chen, H.; Clifford, D.B.; Deng, L.; Wu, K.; Lee, A.J.; Bosch, R.J.; Riddler, S.A.; Ellis, R.J.; Evans, S.R. Peripheral neuropathy in ART-experienced patients: Prevalence and risk factors. J. NeuroVirology 2013, 19, 557–564. [Google Scholar] [CrossRef]
- Kessler, R.C.; Üstün, T.B. The world mental health (WMH) survey initiative version of the world health organization (WHO) composite international diagnostic interview (CIDI). Int. J. Methods Psychiatr. Res. 2004, 13, 93–121. [Google Scholar] [CrossRef]
- Wittchen, H.-U. Reliability and validity studies of the WHO-Composite International Diagnostic Interview (CIDI): A critical review. J. Psychiatr. Res. 1994, 28, 57–84. [Google Scholar] [CrossRef]
- VanderWeele, T.J. Policy-relevant proportions for direct effects. Epidemiology 2013, 24, 175–176. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PWH n = 69 | PWoH n = 74 | All n = 143 | p-Value | |
|---|---|---|---|---|
| Age (year) | 43.9 ± 15.3 | 44.7 ± 12.6 | 44.3 ± 12.9 | 0.74 |
| Sex (male) | 63 (91.3%) | 33 (44.6%) | 96 (67.1%) | <0.001 |
| Ethnicity | ||||
| Non-Hispanic White | 34 (50.0%) | 36 (48.6%) | 70 (49.3%) | 0.32 |
| Black | 7 (10.3%) | 15 (20.3%) | 22 (15.5%) | |
| Hispanic | 23 (33.8%) | 18 (24.3%) | 41 (28.9%) | |
| Other | 4 (5.9%) | 5 (6.8%) | 9 (6.3%) | |
| Nadir CD4 * median (IQR) | 300 (178–448) | |||
| Current CD4 * median (IQR) | 643 (502–839) | |||
| Duration of infection (year) median (IQR) | 8.7 (2.5–16.6) | |||
| On ART | 60 (87.0%) | |||
| Duration of ART (month) median (IQR) | 55.6 (20.6–142.9) | |||
| Plasma HIV RNA ≤ 50 copies/mL | 54 (80.6%) | |||
| CSF HIV RNA ≤ 50 copies/mL | 41 (97.6%) | |||
| DSP variables | ||||
| Reduced vibration | 13 (20.3%) | 7 (10.3%) | 20 (15.2%) | 0.10 |
| Reduced sharp sensation | 5 (7.8%) | 2 (3.0%) | 7 (5.3%) | 0.21 |
| Reduced or absent ankle reflexes | 19 (29.7%) | 12 (17.6%) | 31 (23.5%) | 0.10 |
| Pain | 13 (20.3%) | 3 (4.4%) | 16 (12.1%) | 0.005 |
| Tingling | 21 (32.8%) | 5 (7.4%) | 26 (19.7%) | <0.001 |
| Loss of sensation | 15 (23.4%) | 2 (2.9%) | 17 (12.9%) | <0.001 |
| 0–1 DSP signs ^ | 53 (82.8%) | 64 (94.1%) | 117 (88.6%) | 0.041 |
| ≥2 DSP signs ^ | 11 (17.2%) | 4 (5.9%) | 15 (11.4%) | |
| Presence of any DSP symptoms | 25 (39.1%) | 8 (11.8%) | 33 (25.0%) | <0.001 |
| Concurrent medical conditions | ||||
| History of diabetes | 3 (4.5%) | 6 (8.5%) | 9 (6.5%) | 0.34 |
| Metabolic syndrome | 24 (34.8%) | 27 (36.5%) | 51 (35.7%) | 0.83 |
| Framingham CVD risk score | ||||
| Low risk | 36 (58.1%) | 44 (65.7%) | 80 (62.0%) | 0.37 |
| Mid-high risk | 26 (41.9%) | 23 (34.3%) | 49 (38.0%) | |
| Substance use disorders | ||||
| Lifetime alcohol use disorder | 38 (60.3%) | 28 (43.1%) | 66 (51.6%) | 0.051 |
| Lifetime methamphethamine use disorder | 40 (63.5%) | 22 (33.8%) | 62 (48.4%) | <0.001 |
| Lifetime opioid use disorder | 2 (3.2%) | 3 (4.6%) | 5 (3.9%) | 0.67 |
| Outcomes | Total Effect (95% CI) | Direct Effect (95% CI) | Mediation Effect (95%CI) | Proportion Mediated |
|---|---|---|---|---|
| DSP * | 3.44 (0.62–22.26) | 2.39 (0.68–8.40) | 1.43 (0.91–2.67) | 29.3 |
| Presence of any Symptoms | 5.07 (1.49–21.75) | 3.66 (1.44–9.29) | 1.38 (1.03–2.35) | 20.0 |
| DNP | 5.64 (0.94–39.25) | 4.40 (1.14–16.94) | 1.28 (0.82–2.32) | 14.4 |
| Paresthesia (Tingling) | 6.56 (1.56–34.12) | 4.61 (1.55–13.65) | 1.42 (1.01–2.51) | 18.8 |
| Loss of sensation | 11.13 (1.53–114.4) | 7.09 (1.50–33.44) | 1.59 (1.03–3.42) | 19.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andalibi, M.S.; Fields, J.A.; Iudicello, J.E.; Diaz, M.M.; Tang, B.; Letendre, S.L.; Ellis, R.J. Elevated Biomarkers of Inflammation and Vascular Dysfunction Are Associated with Distal Sensory Polyneuropathy in People with HIV. Int. J. Mol. Sci. 2024, 25, 4245. https://doi.org/10.3390/ijms25084245
Andalibi MS, Fields JA, Iudicello JE, Diaz MM, Tang B, Letendre SL, Ellis RJ. Elevated Biomarkers of Inflammation and Vascular Dysfunction Are Associated with Distal Sensory Polyneuropathy in People with HIV. International Journal of Molecular Sciences. 2024; 25(8):4245. https://doi.org/10.3390/ijms25084245
Chicago/Turabian StyleAndalibi, Mohammadsobhan Sheikh, Jerel Adam Fields, Jennifer E. Iudicello, Monica M. Diaz, Bin Tang, Scott L. Letendre, and Ronald J. Ellis. 2024. "Elevated Biomarkers of Inflammation and Vascular Dysfunction Are Associated with Distal Sensory Polyneuropathy in People with HIV" International Journal of Molecular Sciences 25, no. 8: 4245. https://doi.org/10.3390/ijms25084245