
The Role of Deep Learning and Gait Analysis in Parkinson’s Disease: A Systematic Review

 , ,
, ,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
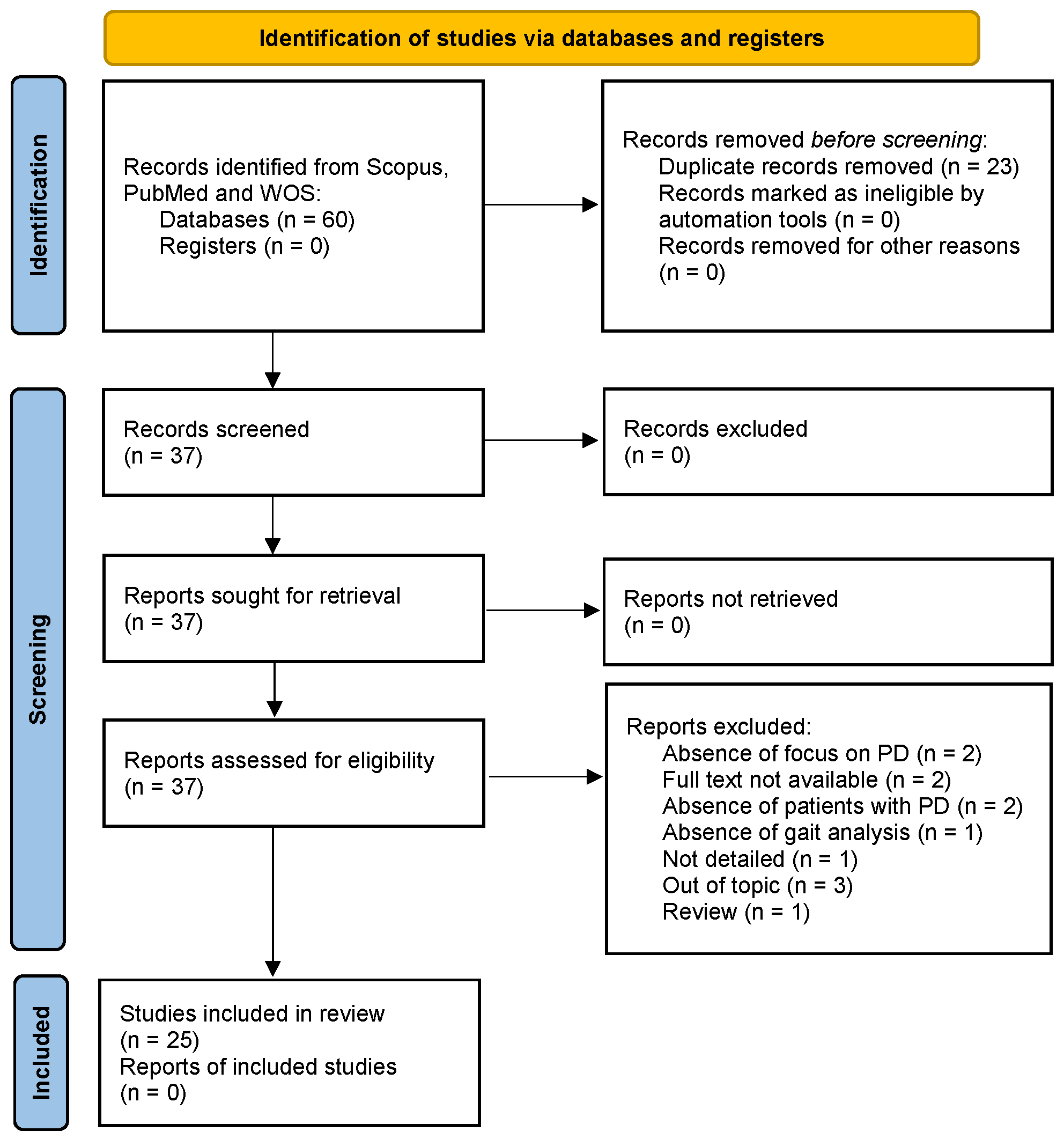
2. Materials and Methods
- Focus on PD with no known cause (idiopathic PD);
- Gait analysis with a clear description of the experimental protocol to study PD;
- Discussion on the details of the neural network used and the performance indices utilized.
- Non-English articles, book chapters, and reviews;
- Articles with unavailable full text;
- Articles related to a healthy control (HC);
- Articles unrelated to DL;
- Articles with an absence of focus on PD and an absence of gait analysis.
3. Results and Discussions
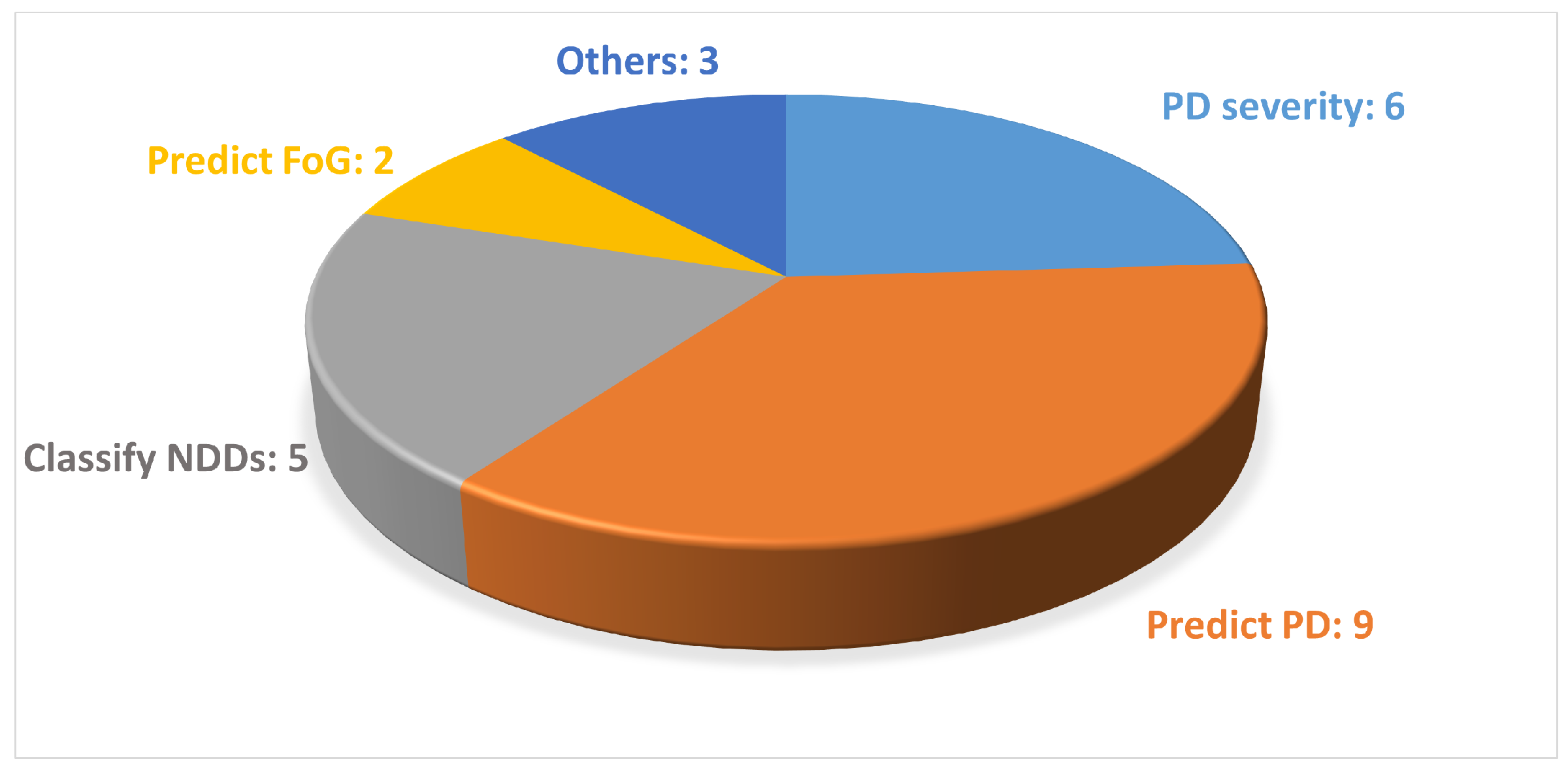
3.1. Characteristics of the Included Studies
3.2. Characteristics of the Datasets
3.3. Experimental Approaches Adopted
3.3.1. Wearable Sensors
3.3.2. Vision-Based Motion Capture System
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALS | amyotrophic lateral sclerosis |
| ARR | Anova with Recursive Reduction |
| ASA | arm swing asymmetry |
| AUC | Area Under the Curve |
| CNN | Convolutional Neural Network |
| CPM | Convolutional Pose Machine |
| DL | Deep Learning |
| DNN | Deep Neural Network |
| FoG | Freezing of Gait |
| FRL | frequency representation learning |
| GAD | graph adaptive network block |
| GCNN | graph convolutional neural network |
| GRU | Gated Recurrent Unit |
| HC | healthy control |
| HD | Huntington’s Disease |
| HPE | Human Pose Estimation |
| LSTM | long short-term memory |
| MDS-UPDRS | Movement Disorder Society-Unified Parkinson’s Disease Rating Scale |
| ML | Machine Learning |
| MS | Multiple Sclerosis |
| NDD | neurodegenerative disease |
| PD | Parkinson’s Disease |
| P-P | peak-to-peak |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RFdGAD | robust frequency-domain-based graph adaptive network |
| RNN | Recurrent Neural Network |
| TDPT-GT | Three-Dimensional Pose Tracker for Gait Test |
| vGRF | Vertical Ground Reaction Force |
| WM-STGCN | Weighted adjacency matrix with virtual connection and Multi-scale temporal convolution in a Spatiotemporal Graph Convolution Networkgraph convolutional neural network |
References
- de Lau, L.M.; Breteler, M.M. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Twelves, D.; Perkins, K.S.M.; Counsell, C. Systematic review of incidence studies of Parkinson’s disease. Mov. Disord. 2002, 18, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Balestrino, R.; Schapira, A. Parkinson disease. Eur. J. Neurol. 2020, 27, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Berg, D.; Stern, M.B.; Poewe, W.; Olanow, C.W.; Oertel, W.H.; Obeso, J.A.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Ba, F.; Obaid, M.; Wieler, M.; Camicioli, R.; Martin, W.W. Parkinson disease: The relationship between non-motor symptoms and motor phenotype. Can. J. Neurol. Sci. 2016, 43, 261–267. [Google Scholar] [CrossRef]
- Dadar, M.; Gee, M.; Shuaib, A.; Duchesne, S.; Camicioli, R. Cognitive and motor correlates of grey and white matter pathology in Parkinson’s disease. NeuroImage Clin. 2020, 27, 102353. [Google Scholar] [CrossRef]
- Gelb, D.J.; Oliver, E.; Gilman, S. Diagnostic criteria for Parkinson disease. Arch. Neurol. 1999, 56, 33–39. [Google Scholar] [CrossRef]
- Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. The unified Parkinson’s disease rating scale (UPDRS): Status and recommendations. Mov. Disord. 2003, 18, 738–750. [Google Scholar] [CrossRef]
- Baker, R. Gait analysis methods in rehabilitation. J. Neuroeng. Rehabil. 2006, 3, 1–10. [Google Scholar] [CrossRef]
- Wren, T.A.; Gorton, G.E., III; Ounpuu, S.; Tucker, C.A. Efficacy of clinical gait analysis: A systematic review. Gait Posture 2011, 34, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Kulig, K.; Burnfield, J.M. The role of biomechanics in orthopedic and neurological rehabilitation. Acta Bioeng. Biomech. 2008, 10, 3–14. [Google Scholar] [PubMed]
- Oung, Q.W.; Muthusamy, H.; Basah, S.N.; Lee, H.; Vijean, V. Empirical Wavelet transform based features for classification of Parkinson’s disease severity. J. Med. Syst. 2017, 42, 29. [Google Scholar] [CrossRef] [PubMed]
- Sofuwa, O.; Nieuwboer, A.; Desloovere, K.; Willems, A.M.; Chavret, F.; Jonkers, I. Quantitative gait analysis in Parkinson’s disease: Comparison with a healthy control group. Arch. Phys. Med. Rehabil. 2005, 86, 1007–1013. [Google Scholar] [CrossRef]
- Pistacchi, M.; Gioulis, M.; Sanson, F.; De Giovannini, E.; Filippi, G.; Rossetto, F.; Marsala, S.Z. Gait analysis and clinical correlations in early Parkinson’s disease. Funct. Neurol. 2017, 32, 28. [Google Scholar] [CrossRef]
- Amboni, M.; Ricciardi, C.; Picillo, M.; De Santis, C.; Ricciardelli, G.; Abate, F.; Tepedino, M.F.; D’Addio, G.; Cesarelli, G.; Volpe, G.; et al. Gait analysis may distinguish progressive supranuclear palsy and Parkinson disease since the earliest stages. Sci. Rep. 2021, 11, 9297. [Google Scholar] [CrossRef]
- Russo, M.; Amboni, M.; Barone, P.; Pellecchia, M.T.; Romano, M.; Ricciardi, C.; Amato, F. Identification of a Gait Pattern for Detecting Mild Cognitive Impairment in Parkinson’s Disease. Sensors 2023, 23, 1985. [Google Scholar] [CrossRef]
- Russo, M.; Ricciardi, C.; Amboni, M.; Volzone, A.; Barone, P.; Romano, M.; Francesco, A. A Cluster Analysis for Parkinson’s Disease Phenotyping with Gait Parameters. In Proceedings of the 2023 IEEE International Conference on Metrology for eXtended Reality, Artificial Intelligence and Neural Engineering (MetroXRAINE), Milano, Italy, 25–27 October 2023; IEEE: Piscataway, NJ, USA, 2023; pp. 882–887. [Google Scholar]
- Morris, M.; Iansek, R.; Matyas, T.; Summers, J. Abnormalities in the stride length-cadence relation in parkinsonian gait. Mov. Disord. Off. J. Mov. Disord. Soc. 1998, 13, 61–69. [Google Scholar] [CrossRef]
- Amboni, M.; Iuppariello, L.; Iavarone, A.; Fasano, A.; Palladino, R.; Rucco, R.; Picillo, M.; Lista, I.; Varriale, P.; Vitale, C.; et al. Step length predicts executive dysfunction in Parkinson’s disease: A 3-year prospective study. J. Neurol. 2018, 265, 2211–2220. [Google Scholar] [CrossRef]
- Ferreira, F.; Gago, M.F.; Bicho, E.; Carvalho, C.; Mollaei, N.; Rodrigues, L.; Sousa, N.; Rodrigues, P.P.; Ferreira, C.; Gama, J. Gait stride-to-stride variability and foot clearance pattern analysis in Idiopathic Parkinson’s Disease and Vascular Parkinsonism. J. Biomech. 2019, 92, 98–104. [Google Scholar] [CrossRef]
- Connie, T.; Aderinola, T.B.; Ong, T.S.; Goh, M.K.O.; Erfianto, B.; Purnama, B. Pose-Based Gait Analysis for Diagnosis of Parkinson’s Disease. Algorithms 2022, 15, 474. [Google Scholar] [CrossRef]
- Cimolin, V.; Galli, M. Summary measures for clinical gait analysis: A literature review. Gait Posture 2014, 39, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Dicharry, J. Kinematics and kinetics of gait: From lab to clinic. Clin. Sport. Med. 2010, 29, 347–364. [Google Scholar] [CrossRef] [PubMed]
- Abate, F.; Russo, M.; Ricciardi, C.; Tepedino, M.F.; Romano, M.; Erro, R.; Pellecchia, M.T.; Amboni, M.; Barone, P.; Picillo, M. Wearable sensors for assessing disease severity and progression in Progressive Supranuclear Palsy. Park. Relat. Disord. 2023, 109, 105345. [Google Scholar] [CrossRef]
- Pisani, N.; Ricciardi, C.; Picillo, M.; Abate, F.; Avallone, A.R.; Amato, F.; Cesarelli, M. Using Wearable Sensors and Motion Parameters for Recognizing Progressive Supranuclear Palsy Phenotypes. In Proceedings of the 2023 IEEE International Conference on Metrology for eXtended Reality, Artificial Intelligence and Neural Engineering (MetroXRAINE), Milano, Italy, 25–27 October 2023; pp. 864–869. [Google Scholar]
- Ricciardi, C.; Pisani, N.; Donisi, L.; Abate, F.; Amboni, M.; Barone, P.; Picillo, M.; Cesarelli, M.; Amato, F. Agreement between Optoelectronic System and Wearable Sensors for the Evaluation of Gait Spatiotemporal Parameters in Progressive Supranuclear Palsy. Sensors 2023, 23, 9859. [Google Scholar] [CrossRef]
- Prisco, G.; Romano, M.; Esposito, F.; Cesarelli, M.; Santone, A.; Donisi, L.; Amato, F. Capability of Machine Learning Algorithms to Classify Safe and Unsafe Postures during Weight Lifting Tasks Using Inertial Sensors. Diagnostics 2024, 14, 576. [Google Scholar] [CrossRef]
- Muro-De-La-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef]
- Gunduz, H. Deep learning-based Parkinson’s disease classification using vocal feature sets. IEEE Access 2019, 7, 115540–115551. [Google Scholar] [CrossRef]
- Wang, W.; Lee, J.; Harrou, F.; Sun, Y. Early detection of Parkinson’s disease using deep learning and machine learning. IEEE Access 2020, 8, 147635–147646. [Google Scholar] [CrossRef]
- Caliskan, A.; Badem, H.; Basturk, A.; Yuksel, M. Diagnosis of the parkinson disease by using deep neural network classifier. IU-J. Electr. Electron. Eng. 2017, 17, 3311–3318. [Google Scholar]
- Landolfi, A.; Ricciardi, C.; Donisi, L.; Cesarelli, G.; Troisi, J.; Vitale, C.; Barone, P.; Amboni, M. Machine Learning Approaches in Parkinson’s Disease. Curr. Med. Chem. 2021, 28, 6548–6568. [Google Scholar] [CrossRef] [PubMed]
- Ricciardi, C.; Amboni, M.; De Santis, C.; Ricciardelli, G.; Improta, G.; Cesarelli, G.; D’Addio, G.; Barone, P. Classifying patients affected by Parkinson’s disease into freezers or non-freezers through machine learning. In Proceedings of the 2020 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Bari, Italy, 1 June–1 July 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Sivaranjini, S.; Sujatha, C. Deep learning based diagnosis of Parkinson’s disease using convolutional neural network. Multimed. Tools Appl. 2020, 79, 15467–15479. [Google Scholar] [CrossRef]
- Alharthi, A.S.; Yunas, S.U.; Ozanyan, K.B. Deep learning for monitoring of human gait: A review. IEEE Sensors J. 2019, 19, 9575–9591. [Google Scholar] [CrossRef]
- Horst, F.; Lapuschkin, S.; Samek, W.; Müller, K.R.; Schöllhorn, W.I. Explaining the unique nature of individual gait patterns with deep learning. Sci. Rep. 2019, 9, 2391. [Google Scholar] [CrossRef]
- Albuquerque, P.; Machado, J.P.; Verlekar, T.T.; Correia, P.L.; Soares, L.D. Remote GAIT type classification system using markerless 2D video. Diagnostics 2021, 11, 1824. [Google Scholar] [CrossRef]
- Kondragunta, J.; Wiede, C.; Hirtz, G. Gait analysis for early Parkinson’s disease detection based on deep learning. Curr. Dir. Biomed. Eng. 2019, 5, 9–12. [Google Scholar] [CrossRef]
- Sibley, K.G.; Girges, C.; Hoque, E.; Foltynie, T. Video-based analyses of Parkinson’s disease severity: A brief review. J. Park. Dis. 2021, 11, S83–S93. [Google Scholar] [CrossRef]
- Park, S.H.; Seo, N.Y.; Hwang, S.M.; Park, H.Y.; Jung, Y.J. Quantifying Finger-tapping-test Scores using a Three-dimensional Motion Analysis Program: A Preliminary Study. J. Magn. 2022, 27, 411–420. [Google Scholar] [CrossRef]
- Shin, J.H.; Yu, R.; Ong, J.N.; Lee, C.Y.; Jeon, S.H.; Park, H.; Kim, H.J.; Lee, J.; Jeon, B. Quantitative gait analysis using a pose-estimation algorithm with a single 2D-video of Parkinson’s disease patients. J. Park. Dis. 2021, 11, 1271–1283. [Google Scholar] [CrossRef]
- Stenum, J.; Rossi, C.; Roemmich, R.T. Two-dimensional video-based analysis of human gait using pose estimation. PLoS Comput. Biol. 2021, 17, e1008935. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.; Akl, E.A.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Abujrida, H.; Agu, E.; Pahlavan, K. DeepaMed: Deep learning-based medication adherence of Parkinson’s disease using smartphone gait analysis. Smart Health 2023, 30, 100430. [Google Scholar] [CrossRef]
- Chen, F.; Chen, S.; Si, A.; Luo, Y.; Hu, W.; Zhang, Y.; Ma, J. The long-term trend of Parkinson’s disease incidence and mortality in China and a Bayesian projection from 2020 to 2030. Front. Aging Neurosci. 2022, 14, 973310. [Google Scholar] [CrossRef]
- Picillo, M.; Nicoletti, A.; Fetoni, V.; Garavaglia, B.; Barone, P.; Pellecchia, M.T. The relevance of gender in Parkinson’s disease: A review. J. Neurol. 2017, 264, 1583–1607. [Google Scholar] [CrossRef]
- Peraza, L.R.; Kinnunen, K.M.; McNaney, R.; Craddock, I.J.; Whone, A.; Morgan, C.; Joules, R.; Wolz, R. An Automatic Gait Analysis Pipeline for Wearable Sensors: A Pilot Study in Parkinson’s Disease. Sensors 2021, 21, 8286. [Google Scholar] [CrossRef]
- Erdaş, Ç.B.; Sümer, E.; Kibaroğlu, S. Neurodegenerative diseases detection and grading using gait dynamics. Multimed. Tools Appl. 2023, 82, 22925–22942. [Google Scholar] [CrossRef]
- Lin, C.; Wen, T.C.; Setiawan, F. Evaluation of vertical ground reaction forces pattern visualization in neurodegenerative diseases identification using deep learning and recurrence plot image feature extraction. Sensors 2020, 20, 3857. [Google Scholar] [CrossRef]
- Setiawan, F.; Lin, C.W. Identification of neurodegenerative diseases based on vertical ground reaction force classification using Time–Frequency Spectrogram and deep learning neural network features. Brain Sci. 2021, 11, 902. [Google Scholar] [CrossRef]
- Vásquez-Correa, J.C.; Arias-Vergara, T.; Orozco-Arroyave, J.R.; Eskofier, B.; Klucken, J.; Nöth, E. Multimodal Assessment of Parkinson’s Disease: A Deep Learning Approach. IEEE J. Biomed. Health Inform. 2019, 23, 1618–1630. [Google Scholar] [CrossRef]
- Carvajal-Castaño, H.A.; Pérez-Toro, P.A.; Orozco-Arroyave, J.R. Classification of Parkinson’s Disease Patients—A Deep Learning Strategy. Electronics 2022, 11, 2684. [Google Scholar] [CrossRef]
- Ma, Y.W.; Chen, J.L.; Chen, Y.J.; Lai, Y.H. Explainable deep learning architecture for early diagnosis of Parkinson’s disease. Soft Comput. 2021, 27, 2729–2738. [Google Scholar] [CrossRef]
- Zhong, C.; Ng, W.W.Y. A Robust Frequency-Domain-Based Graph Adaptive Network for Parkinson’s Disease Detection from Gait Data. IEEE Trans. Multimed. 2023, 25, 7076–7088. [Google Scholar] [CrossRef]
- Aşuroğlu, T.; Oğul, H. A deep learning approach for parkinson’s disease severity assessment. Health Technol. 2022, 12, 943–953. [Google Scholar] [CrossRef]
- Setiawan, F.; Lin, C.W. Implementation of a deep learning algorithm based on vertical ground reaction Force Time–Frequency features for the detection and severity classification of Parkinson’s disease. Sensors 2021, 21, 5207. [Google Scholar] [CrossRef]
- Xia, Y.; Yao, Z.; Ye, Q.; Cheng, N. A Dual-Modal Attention-Enhanced Deep Learning Network for Quantification of Parkinson’s Disease Characteristics. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 42–51. [Google Scholar] [CrossRef]
- Maâchi, I.E.; Bilodeau, G.A.; Bouachir, W. Deep 1D-Convnet for accurate Parkinson disease detection and severity prediction from gait. Expert Syst. Appl. 2020, 143, 113075. [Google Scholar] [CrossRef]
- Eguchi, K.; Takigawa, I.; Shirai, S.; Takahashi-Iwata, I.; Matsushima, M.; Kano, T.; Yaguchi, H.; Yabe, I. Gait video-based prediction of unified Parkinson’s disease rating scale score: A retrospective study. BMC Neurol. 2023, 23, 358. [Google Scholar] [CrossRef]
- Rupprechter, S.; Morinan, G.; Peng, Y.; Foltynie, T.; Sibley, K.; Weil, R.S.; Leyland, L.A.; Baig, F.; Morgante, F.; Gilron, R.; et al. A clinically interpretable computer-vision based method for quantifying gait in parkinson’s disease. Sensors 2021, 21, 5437. [Google Scholar] [CrossRef]
- Zanela, A.; Schirinzi, T.; Mercuri, N.B.; Stefani, A.; Romagnoli, C.; Annino, G.; Bonaiuto, V.; Cerroni, R. Using a video device and a deep learning-based pose estimator to assess gait impairment in neurodegenerative related disorders: A pilot study. Appl. Sci. 2022, 12, 4642. [Google Scholar] [CrossRef]
- Abe, K.; Tabei, K.I.; Matsuura, K.; Kobayashi, K.; Ohkubo, T. Relationship Between the Results of Arm Swing Data From the OpenPose-Based Gait Analysis System and MDS-UPDRS Scores. IEEE Access 2022, 10, 118992–119000. [Google Scholar] [CrossRef]
- Guayacán, L.C.; Manzanera, A.; Martínez, F. Quantification of parkinsonian kinematic patterns in body-segment regions during locomotion. J. Med Biol. Eng. 2022, 42, 204–215. [Google Scholar] [CrossRef]
- Zhang, J.; Lim, J.; Kim, M.H.; Hur, S.; Chung, T.M. WM–STGCN: A novel spatiotemporal modeling method for Parkinsonian gait recognition. Sensors 2023, 23, 4980. [Google Scholar] [CrossRef] [PubMed]
- Li, M.H.; Mestre, T.A.; Fox, S.H.; Taati, B. Vision-based assessment of parkinsonism and levodopa-induced dyskinesia with pose estimation. J. Neuroeng. Rehabil. 2018, 15, 97. [Google Scholar] [CrossRef]
- Sato, K.; Nagashima, Y.; Mano, T.; Iwata, A.; Toda, T. Quantifying normal and parkinsonian gait features from home movies: Practical application of a deep learning–based 2D pose estimator. PLoS ONE 2019, 14, e0223549. [Google Scholar] [CrossRef]
- Hu, K.; Wang, Z.; Mei, S.; Martens, K.A.E.; Yao, T.; Lewis, S.J.; Feng, D.D. Vision-based freezing of gait detection with anatomic directed graph representation. IEEE J. Biomed. Health Inform. 2019, 24, 1215–1225. [Google Scholar] [CrossRef]
- Kaur, R.; Motl, R.W.; Sowers, R.; Hernandez, M.E. A Vision-Based Framework for Predicting Multiple Sclerosis and Parkinson’s Disease Gait Dysfunctions—A Deep Learning Approach. IEEE J. Biomed. Health Inform. 2022, 27, 190–201. [Google Scholar] [CrossRef]
- Gül, S.; Soylu, E.; Terzi, M.; Türkoğlu, M.; Koca, K.A. Making the Discrimination in the Walking Parameters of Individuals with Multiple Sclerosis and Parkinson’s Disease with Machine Learning. Turk. J. Neurol. Noroloji Derg. 2023, 29. [Google Scholar] [CrossRef]
- Iseki, C.; Hayasaka, T.; Yanagawa, H.; Komoriya, Y.; Kondo, T.; Hoshi, M.; Fukami, T.; Kobayashi, Y.; Ueda, S.; Kawamae, K.; et al. Artificial Intelligence Distinguishes Pathological Gait: The Analysis of Markerless Motion Capture Gait Data Acquired by an iOS Application (TDPT-GT). Sensors 2023, 23, 6217. [Google Scholar] [CrossRef]
- Mei, J.; Desrosiers, C.; Frasnelli, J. Machine learning for the diagnosis of Parkinson’s disease: A review of literature. Front. Aging Neurosci. 2021, 13, 633752. [Google Scholar] [CrossRef]
- Kubota, K.J.; Chen, J.A.; Little, M.A. Machine learning for large-scale wearable sensor data in Parkinson’s disease: Concepts, promises, pitfalls, and futures. Mov. Disord. 2016, 31, 1314–1326. [Google Scholar] [CrossRef]
- Shetty, S.; Rao, Y. SVM based machine learning approach to identify Parkinson’s disease using gait analysis. In Proceedings of the 2016 International conference on inventive computation technologies (ICICT), Coimbatore, India, 26–27 August 2016; IEEE: Piscataway, NJ, USA, 2016; Volume 2, pp. 1–5. [Google Scholar]
- Trabassi, D.; Serrao, M.; Varrecchia, T.; Ranavolo, A.; Coppola, G.; De Icco, R.; Tassorelli, C.; Castiglia, S.F. Machine learning approach to support the detection of Parkinson’s disease in IMU-based gait analysis. Sensors 2022, 22, 3700. [Google Scholar] [CrossRef] [PubMed]
- Abdulhay, E.; Arunkumar, N.; Narasimhan, K.; Vellaiappan, E.; Venkatraman, V. Gait and tremor investigation using machine learning techniques for the diagnosis of Parkinson disease. Future Gener. Comput. Syst. 2018, 83, 366–373. [Google Scholar] [CrossRef]
- Loh, H.W.; Hong, W.; Ooi, C.P.; Chakraborty, S.; Barua, P.D.; Deo, R.C.; Soar, J.; Palmer, E.E.; Acharya, U.R. Application of deep learning models for automated identification of Parkinson’s disease: A review (2011–2021). Sensors 2021, 21, 7034. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.D.; Mehdizadeh, S.; Iaboni, A.; Mansfield, A.; Flint, A.; Taati, B. Measuring GAIT variables using computer vision to assess mobility and fall risk in older adults with dementia. IEEE J. Transl. Eng. Health Med. 2020, 8, 2100609. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.C.; Li, Y.C.; Kuo, T.Y.; Chen, S.F.; Lin, C.H. Real-Time Detection of Gait Events by Recurrent Neural Networks. IEEE Access 2021, 9, 134849–134857. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Aim of the Study | Type of Dataset | Number of Subjects (Female\Male) | Mean Age of the Subjects | Acquisition Device | Features | Analytical Methods | Main Results |
|---|---|---|---|---|---|---|---|---|
| Abujrida et al., 2023, [46] | Remotely identify the adherence of PD patients to prescribed therapy through DeepaMed, which is a smartphone-based DL approach that distinguishes patients’ gait before and after therapy. | Private | 154\302 | PD: 63.57 ± 8.09, HC: 40.14 ± 15.45 | Smarphone accelerometer and gyroscope sensors | Time, frequency, statistical, and wavelet domain features | DeepaMed CNN | Accuracy: 98.2%; precision: 97.7%; recall: 97.7%; F1: 98.0% |
| Peraza et al., 2021, [49] | Automatic gait analysis using wearable sensors that leverage triaxial accelerometry and extract gait parameters from four sensors. The detection of gait events is based on DL algorithms (U-Net). | Private | 12 | 64.2 | Two AX3 and two GENEActiv sensors | Spatio-temporal gait features | CNN (U-Net), two-layer DNN | Pearson correlations coefficients > 0.75 for the space parameters. The stance time and stride time were significantly different for the normal gait task |
| Erdaş et al., 2023, [50] | Detect and assess the severity of PD, HD, and ALS using gait data and dynamics through various ML methods, including pure ML and the one-dimensional CNN method, along with ensemble techniques, like voting and stacking to enhance overall performance. | Public (The Gait Dynamics in Neuro-Degenerative Disease Database of PhysioNet) | 36\28 | HC 47, PD 61.5, HD 54, ALS 53 | One ground force sensor on each foot | Kinematic measures | Multi-layer perceptron, random forest, extra trees, and k-nearest neighbor as classification; voting and stacking, and 1-dimensional CNN as regression | Random forest: accuracy 58.61%; precision 58.42%; recall 58.49%; F1 58.45% 1D-CNN: Accuracy 68.11%; Precision 69.05%; Recall 68.16%; F1 67.77% |
| Lin et al., 2020, [51] | Develop aDL-based algorithm (CNN) for detecting NDD disorders (PD, HD, ALS) using a recurrence plot derived from vertical ground reaction force signals. | Public (The Gait Dynamics in Neuro-Degenerative Disease Database of PhysioNet) | 36\28 | HC 47, PD 61.5, HD 54, ALS 53 | One ground force sensor on each foot | Time–frequency spectrograms | AlexNet CNN | Accuracy > 95%; sensitivity > 90%; specificity > 90%; AUC > 90% |
| Setiawan et al., 2021, [52] | Develop an artificial intelligence-based algorithm (CNN) for detecting NDD (PD, HD, ALS) using a time–frequency spectrograms derived from vertical ground reaction force signals. | Public (The Gait Dynamics in Neuro-Degenerative Disease Database of PhysioNet) | 36\28 | HC 47, PD 61.5, HD 54, ALS 53 | One ground force sensor on each foot | Time–frequency spectrograms | AlexNet CNN | Accuracy > 90%; Sensitivity > 80%; Specificity > 90%; AUC > 60% |
| Vásquez-Correa et al., 2019, [53] | Multimodal analysis of motor abilities in patients with PD through the use of DL architectures based on TFR and CNN by integrating information from vocal, writing, and gait signals. The proposed method aimed to model the difficulty patients face in initiating and stopping movements of the upper and lower limbs, as well as in language. | Private | 47\36 | 54.5 | eGaIT system | Time–frequency spectrograms and Spatio-temporal features | Individual CNNs are trained for each modality | Accuracy: 97.6%; AUC: 98.8% (with the fusion of the three bio-signals) |
| Carvajal et al., 2022, [54] | Classify subjects with PD compared with HCs using three different DL architectures: CNN, GRU, and a combination of CNN and GRU, which are considered state-of-the-art in gait analysis. Two subgroups of HC were included: elderly (EHC) and young (YHC). | Private | 68\66 | 52 | eGaIT system | Spatio-temporal gait features (segment of 3 s of raw time series) | CNN, GRU, and CNN + GRU | Accuracy: CNN 82.7% (YHC group), 82.4% (EHC group); 82.7% (classification of PD vs. EHC), 92.1% (classification of PD vs. YHC); CNN and GRU 83.7%; 92.7% (classification of PD vs. EHC/YHC) Sensitivity > 70%; specificity > 72%; AUC > 80% |
| Ma et al., 2023, [55] | Develop of an explainable learning architecture (XGBoost and CNN) that integrates mechanisms of DL and ML, including data selection, feature evaluation, and data balancing, for gait detection in patients with PD. | Public (Ga, Ju, and Si datasets) | 68\98 | 63.3 | 8 ground force sensor on each foot | The force domain, the peak domain (mean, standard deviation, max and min value of peak data) and the abnormality domain | XGBoost and CNN | XGBoost: 97.32%; CNN: 98.4% |
| Zhong et al., 2023, [56] | Develop of a robust and innovative graphical adaptive network based on the frequency domain (RFdGAD) to identify PD through gait information, specifically vertical ground reaction force signals recorded by foot sensors. | Public (Ga, Ju, and Si datasets) | 68\98 | 117 < 70 yo, 49 > 70 yo | 8 ground force sensor on each foot | Time and frequency domain features | RFdGAD | Accuracy > 75%, F1 > 70% |
| Aşuroğlu et al., 2022, [57] | Develop a hybrid DL model to predict the severity of PD. In this combined DL approach, the temporal and frequency features of ground reaction force sensors are converted and used as input for the CNN + LWRF architecture. | Public (Physionet Gait in Parkinson’s Disease) | 68\98 | 63.3 | 8 ground force sensor on each foot | Time and frequency domain features | CNN and LWRF | Accuracy: 99.5%; Sensitivity: 98.7%; Specificity: 99.1% |
| Setiawan et al., 2021, [58] | Develop an innovative algorithm for detecting and classifying the severity of PD using DL approaches and relying on signals of vertical ground reaction force. Various types of CNNs were employed as classifiers. | Public (Ga, Ju, and Si datasets) | 68\98 | 63.3 | 8 ground force sensor on each foot | Time–frequency spectrograms | CNN, AlexNet, ResNet-50, ResNet-101, and GoogLeNet | Multi-class classification: accuracy 98.16%, 98.24%, 98.27% (Ga, Ju, Si datasets); sensitivity 98.15%, 98.06%, 97.73% (Ga, Ju, Si datasets), specificity 98.16%, 98.38%, 98.76% (Ga, Ju, Si datasets), AUC 98% (Ga, Ju, Si datasets); Two-class classification: accuracy 99.11%, 99.01%, 98.56% (Ga, Ju, Si datasets); sensitivity 99.77%, 98.94%, 98.85% (Ga, Ju, Si datasets), specificity 98.80%, 99.04%, 98.41% (Ga, Ju, Si datasets), AUC 99% (Ga, Ju, Si datasets) |
| Xia et al., 2020, [59] | Implement of a gait assessment method to provide a binary classification between PD-associated and normal walks, as well as the severity level of the disease. The proposed system adopts a dual-modal model based on DL, where both left and right walks are separately modeled using a CNN, followed by a LSTM network. | Public (Ga, Ju, and Si datasets) | 68\98 | 63.3 | 8 ground force sensor on each foot | Force vs. time curve | CNN-LSTM | Predict PD gaits (Ga dataset): accuracy 99.31, sensitivity 99.35%; specificity 99.23%; Classify PD patients with different H&Y scores (Si dataset): accuracy 99.01% |
| El Maachi et al., 2020, [60] | Develop an advanced PD detection system based on DL techniques to analyze gait information. The approach of 1D-CNN was adopted to build a classifier. The model processes 18 1D vertical ground reaction force signals from foot sensors. | Public (Physionet Gait in Parkinson’s Disease) | 68\98 | 63.3 | 8 ground force sensor on each foot | Spatio-temporal gait features | 1D-ConvNet | Predict PD: accuracy 98.7%; sensitivity 98.1%; specificity 100%; Predict Parkinson’s severity: accuracy 85.3%; precision 87.3% |
| Reference | Aim of the Study | Type of Dataset | Number of Subjects (Female\Male) | Mean Age of the Subjects | Acquisition Device | Features | Analytical Methods | Main Results |
|---|---|---|---|---|---|---|---|---|
| Eguchi et al., 2023, [61] | Propose a CNN to estimate UPDRS severity scores and subscores of axial symptoms, bradykinesia, rigidity, and tremor. | Private | 44\30 | 63.4 ± 8.2 | Video camera | Spatio-temporal gait features | ECO-Lite CNN | The goodness of the model the coefficient of determination was evaluated. In particular, axial symptoms, bradykinesia, rigidity, and tremor: 0.59, 0.77, 0.56, and 0.46, respectively |
| Rupprechter et al., 2021, [62] | Investigate a markerless motion capture system using videos as a component of routine gait assessments to evaluate the motor performances of PD patients. | Private | Not specified | Not specified | Video camera | Spatio-temporal gait features and arm swing | OpenPose | Correlation coefficient 0.80 |
| Zanela et al., 2022, [63] | Evaluate gait impairments and assessing the disease burden by employing human estimation pose system OpenPose and a stereoscopic device. | Private | 4\6 | 62.7 ± 13.2 | Video camera | Spatial coordinates | OpenPose | The authors demonstrated good effectiveness of the proposed system in extracting the main features concerning the PD patients’ gaits |
| Abe et al., 2022, [64] | Investigate the peak-to-peak data regarding the left and right arm swing in PD patients using OpenPose-based gait analysis and video acquired by a smartphone camera. | Private | 28 (6\13 PD) | not specified | Smartphone or consumer video camera | P-P (peak-to-peak) Left, P-P right, ASA (arm swing asymmetry) | OpenPose | P-P = 72.7% and ASA = 82.4% of accuracy, respectively |
| Guayacán et al., 2022, [65] | Proposing a markerless strategy, DensePose CNN, for the analysis of body segment kinematics to obtain PD characterisation during walking, captured in sagittal video sequences using a single camera. | Private | 10\12 | 72.3 ± 7.4 | Videocamera | Kinematic measures | DensePose | Accuracy: 99.6% for lower-limbs |
| Zhang et al., 2023, [66] | Propose a method for recognising the gait of PD patients. First, skeletal features were extracted from the videos using OpenPose. Then, they used a weighted adjacency matrix with virtual connection and multi-scale temporal convolution in a spatiotemporal graph convolution network graph convolutional neural network (WM-STGCN), which provides an efficient mechanism for direct learning of joint trajectories. | Private | 50 | Not specified | Smartphone accelerometer and gyroscope sensors (Samsung) | Spatio-temporal gait features | OpenPose + WM–STGCN | Accuracy: 87.1%, sensitivity: 86.7%, specificity: 87.5%, precision: 86.7% |
| Michael H. Li et al., 2018, [67] | Propose a DL-based pose estimation algorithm for a CPM for extracting 15 gait kinematic features in order to train an ML model for detecting and estimating the severity of levodopa-induced dyskinesia and parkinsonisms. | Private | 9 (4\5) | 64 | A single camera | Kinematic measures | CPM and random forest classifier | Unified Dyskinesia Rating Scale (UDysRS) and Unified Parkinson’s Disease Rating Scale (UPDRS) scores were predicted with r = 0.741 and 0.530, respectively |
| Sato et al., 2019, [68] | Propose a method for quantifying gait features and detecting FOG events by extracting the cadence from normal and parkinsonian gait movies recorded with a home video camera. | Public (CASIA Dataset-B) | 119 | HC 20, PD 65 | Video camera | Spatio-temporal gait features | OpenPose | Comparison between the cadence laterally viewed movie and the frontally viewed movie of the same gait. Good consistency between them: R = 0.754, RMSE = 7.24, and MAE = 6.05 |
| Hu et al., 2019, [69] | Propose a promised novel graph convolutional neural network (GCNN) using the FoG detection method. | Private | 45 | Not specified | Video camera | Spatial-temporal gait features | GCNN | Accuracy > 87%, sensitivity > 80%, specificity > 79%, AUC > 0.80 |
| Kaur et al., 2022, [70] | Investigate the effectiveness of a vision-based model for classifying gait strides in persons with different neurological disorders. By segmenting the gait steps and identifying heel strikes, several DL algorithms, such as CNN and RNN, were trained. | Private | 14\19 | 66 ± 5 MS, 68 ± 9 PD, 63 ± 9 HC | Video camera | Segmentation of the gait steps and heel strike | 4 convolutional architectures (CNN, ResNet, MSResNet, TCN), 3 recurrent architectures (RNN, LSTM, GRU) | In single task, the RNN resulted in the highest accuracy and AUC of 78.1% and 0.87, and the CNN had highest accuracy of 75% in dual trials. |
| Gül et al., 2023, [71] | Propose a hybrid system based on CNN and use videos of 28 patients taken from front, back, and both sides during walking in order to distinguish different neurological disorders. | Private | 28 | Not specified | Video camera | Joint coordinates | CNN | Accuracy, sensitivity, specificity > 80% |
| Iseki et al., 2023, [72] | Propose a markerless motion capture system (Three-Dimensional Pose Tracker for Gait Test (TDPT-GT)) based on ML combined with an iPhone camera to distinguish a pathological gait from a control gait. | Private | 131\143 | PD: 74.5 ± 7.8, HC: 72.9 ± 11.1 | TDPT-GT (iPhone camera) | Spatio-temporal gait features | Light GBM | Accuracy > 70%; sensitvity > 63%, specificity > 72%, AUC > 0.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franco, A.; Russo, M.; Amboni, M.; Ponsiglione, A.M.; Di Filippo, F.; Romano, M.; Amato, F.; Ricciardi, C. The Role of Deep Learning and Gait Analysis in Parkinson’s Disease: A Systematic Review. Sensors 2024, 24, 5957. https://doi.org/10.3390/s24185957
Franco A, Russo M, Amboni M, Ponsiglione AM, Di Filippo F, Romano M, Amato F, Ricciardi C. The Role of Deep Learning and Gait Analysis in Parkinson’s Disease: A Systematic Review. Sensors. 2024; 24(18):5957. https://doi.org/10.3390/s24185957
Chicago/Turabian StyleFranco, Alessandra, Michela Russo, Marianna Amboni, Alfonso Maria Ponsiglione, Federico Di Filippo, Maria Romano, Francesco Amato, and Carlo Ricciardi. 2024. "The Role of Deep Learning and Gait Analysis in Parkinson’s Disease: A Systematic Review" Sensors 24, no. 18: 5957. https://doi.org/10.3390/s24185957