Abstract
(1) Background: To evaluate the clinical effects of leukocyte-rich platelet-rich plasma (LR-PRP) and hyaluronic acid (HA) injections in treating patients suffering from knee osteoarthritis (OA); (2) Methods: Randomized controlled trials (RCTs) were searched from PubMed, Web of Science, and Cochrane Library. Keywords were: platelet-rich plasma, LR-PRP, leukocyte-rich, hyaluronic acid, and knee osteoarthritis. The included RCTs were published between the 1st of November 2011 and the 3rd of February 2021. Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores, visual analog scale (VAS) scores, International Knee Documentation Committee (IKDC) scores, and adverse events were used as outcomes for evaluation; (3) Results: A total of 14 RCTs were enrolled. At 6 months, revealed that the LR-PRP group was better than the HA group in WOMAC total, pain, and physical function scores. At 12 months, the LR-PRP group was better than the HA group in WOMAC stiffness and physical function scores. There was no significant difference in adverse events; (4) Conclusion: LR-PRP injection showed no significant pain relief effect as compared with HA injection. However, LR-PRP demonstrated better overall outcomes as compared to HA in knee OA patients at the follow-up periods of 3, 6, and 12 months. LR-PRP injection may be recommended as a feasible option in treating patients with knee OA.
1. Introduction
Knee osteoarthritis (OA) is a common degenerative musculoskeletal disorder in the elderly population. Although total knee arthroplasty is proved as an effective solution for severe knee OA, the risks of operation complications have been mentioned. Thus, various non-surgical interventions have been described to treat symptomatic knee OA, including knee joint intra-articular (IA) injections, oral nonsteroidal anti-inflammatory drugs (NSAIDs), and physical therapy. The selection of IA injection treatments includes autologous platelet-rich plasma (PRP), corticosteroids, hyaluronic acid (HA), dextrose, and micronized dehydrated human amnion/chorion membrane [1]. IA application of low intensity radiation with specific wavelengths using Low Level Laser Therapy (LLLT) may be another non-surgical method that can be used in treating knee OA [2]. PRP is an autologous blood product containing growth factors, which include epidermal growth factor, fibroblast growth factor, platelet-derived growth factor, and vascular endothelial growth factor. These growth factors can improve angiogenesis, modulate inflammation, and recruit stem cells and fibroblasts to the area of injuries [3]. HA is a natural glycosaminoglycan in synovial fluid. HA can increase viscoelastic properties of the synovial fluid and increase overall joint lubrication in the injured region. It has been proven to facilitate functional improvements in knee, hip, and ankle OA [4]. In recent years, the efficacy of IA PRP and HA injections in knee OA patients has been compared in numerous studies. Dai et al. found that IA PRP injection is more effective than HA injection in pain relief and functional improvement at 12 months after the injection [5]. A meta-analysis conducted by Tang et al. indicated that IA PRP injection seems to be more effective than HA injection in long-term pain control of knee OA patients [6]. The efficacy of leukocyte-rich platelet-rich plasma (LR-PRP) and leukocyte-poor platelet-rich plasma (LP-PRP) has been controversial and without obvious consensus. Some preclinical studies have found that leukocytes may impair the overall effects of PRP [7]. Thus, further clinical trials are vital to compare the physiological effects of leukocytes in different PRP preparations. Belk et al. conducted a meta-analysis that showed that LP-PRP may be superior to LR-PRP in treating knee OA in terms of IKDC scores, but without significant differences in WOMAC and VAS scores [8]. Although multiple randomized controlled trials (RCTs) revealed that LR-PRP has better functional outcomes and pain relief than HA [9,10,11], no meta-analysis has solely discussed the efficacy of knee IA LR-PRP injection as compared with HA. This study aimed to perform a meta-analysis in investigating the effectiveness and safety of IA LR-PRP injection in the treatment of knee OA as compared with HA.
2. Results
2.1. Literature Search
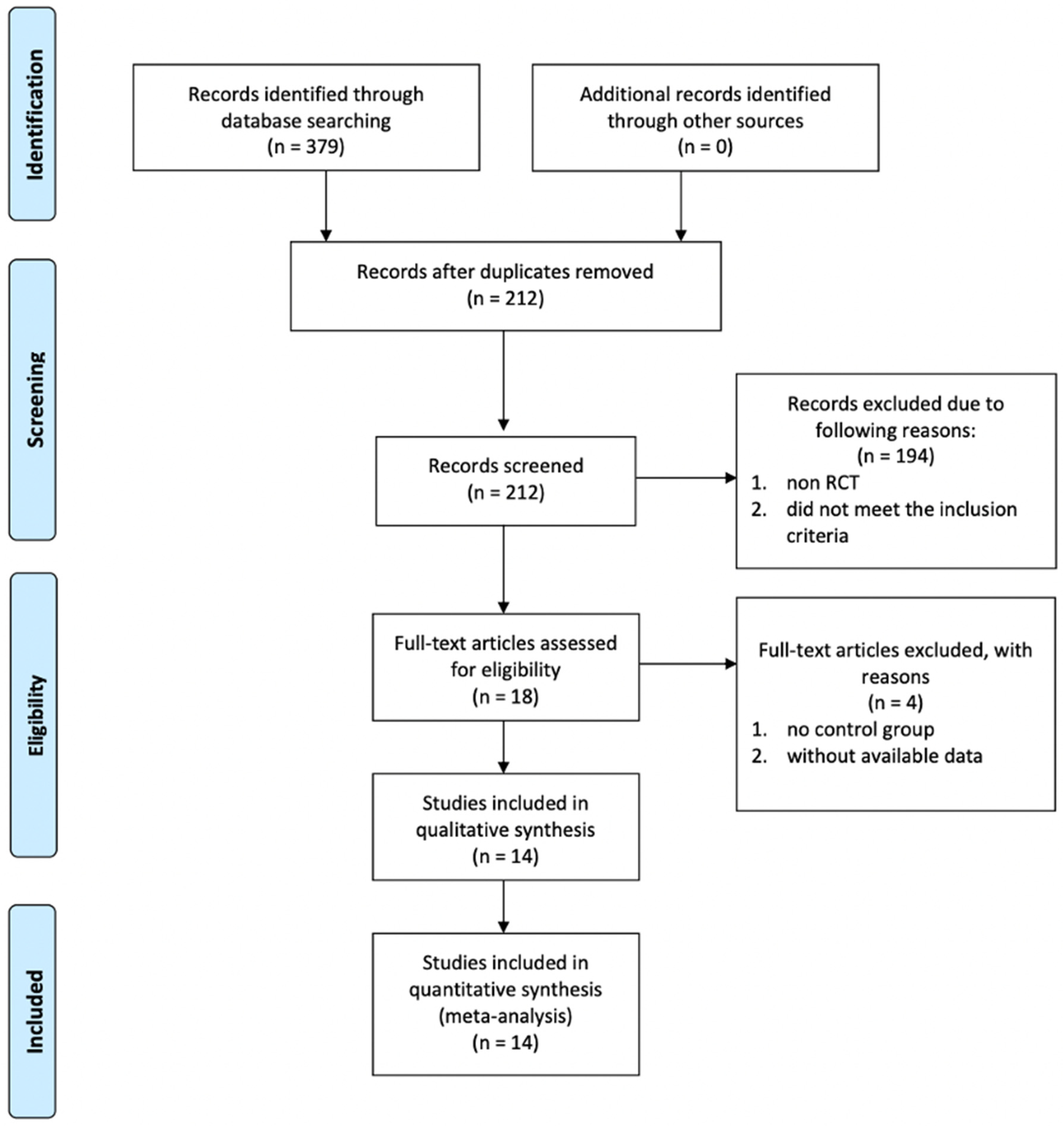
Figure 1 demonstrates the literature selection process that was conducted in this study. During our initial literature search, 379 potentially eligible studies from PubMed, Web of Science, and Cochrane Library were found. A total of 167 duplicated studies were removed. The remaining 212 studies were meticulously screened according to the abstracts, and 194 of them were removed according to the following criteria: non RCTs, and those RCTs, which did not meet our inclusion criteria. Eighteen studies that had the potential for inclusion and their full texts were reviewed. Four studies were subsequently removed as they did not have control groups and data were not available. Finally, 14 RCTs were included in this systematic review and meta-analysis manuscript.
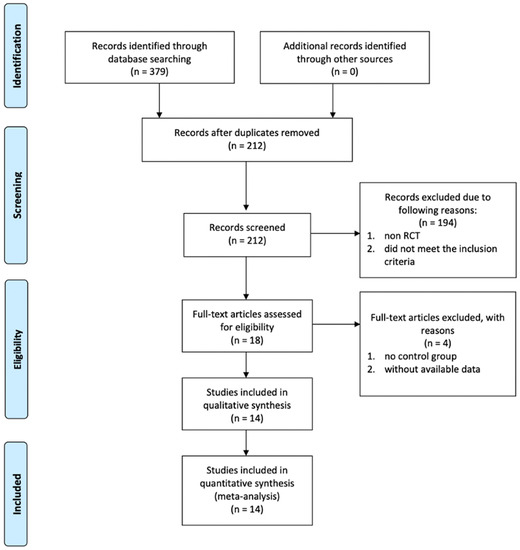
Figure 1.
PRISMA flow chart showing literature search and selection process.
2.2. Main Characteristics of Included Studies
The main characteristics of included studies are listed in Table 1. In total, 14 RCTs were included in our study, with 1485 patients. A total of 815 patients underwent LR-PRP injections, and 670 patients underwent HA injections. These studies were published from 2011 to 2021. Five studies were conducted in Italy; two studies were conducted in Turkey and China, respectively. One study was conducted in Slovakia, Egypt, South Korea, Australia, and Iran, respectively. Further detailed characteristics and results of the involved patients are provided in Table 1. The dosage and the timing of LR-PRP and HA injections are shown in Table 2.

Table 1.
General characteristics of the included studies.
Table 2.
The treatment protocols of IA LR-PRP and IA HA injections.
2.3. Quality of the Studies
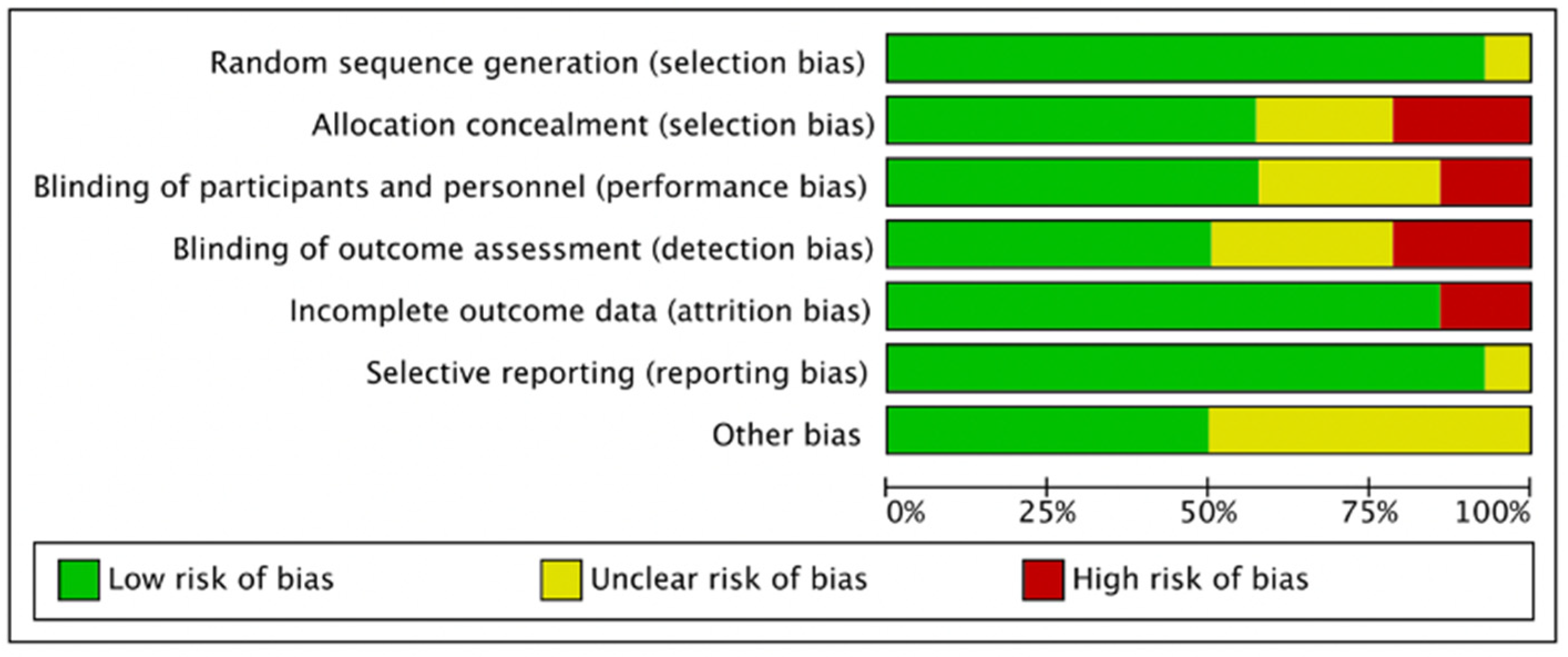
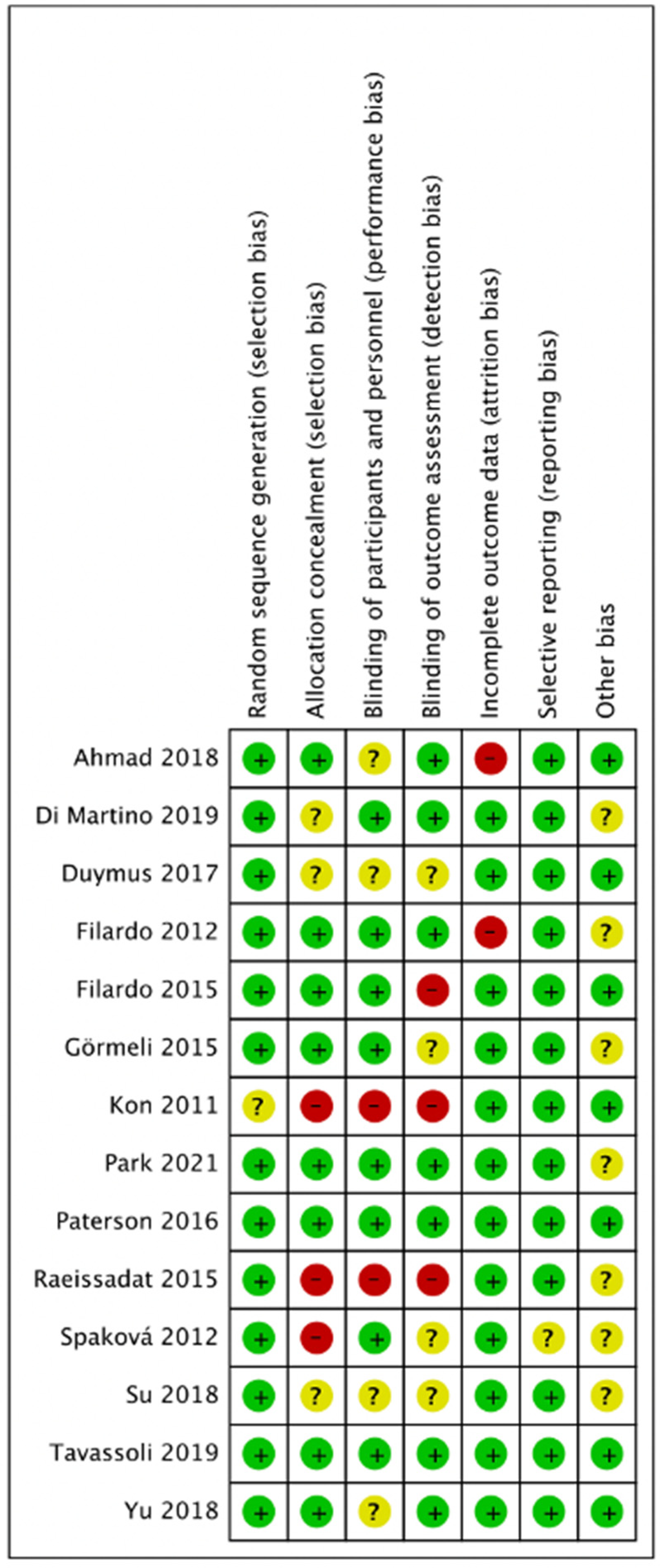
Figure 2 and Figure 3 presented the risk of bias. One study did not report methods of random sequence generation [11]. Eight studies reported allocation concealment [9,13,14,16,18,20,21,22]. Eight studies reported blinding of participants and personnel [9,10,12,13,14,16,20,21,22], and seven studies reported blinding of outcome assessors [9,10,16,18,20,21,22]. In total, five studies were double-blinded [9,10,16,21,22].
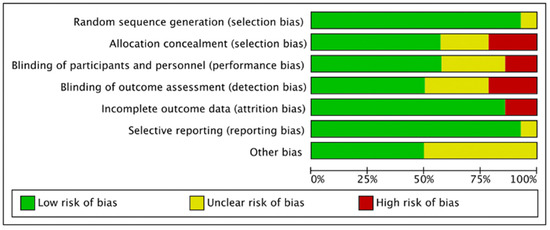
Figure 2.
Graph on the risk of bias.
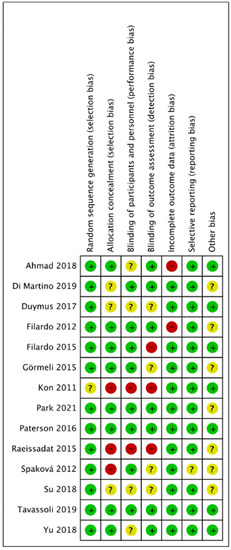
Figure 3.
Summary of risk bias.
2.4. Outcomes of the Meta-Analysis
2.4.1. WOMAC Total Scores (LR-PRP)
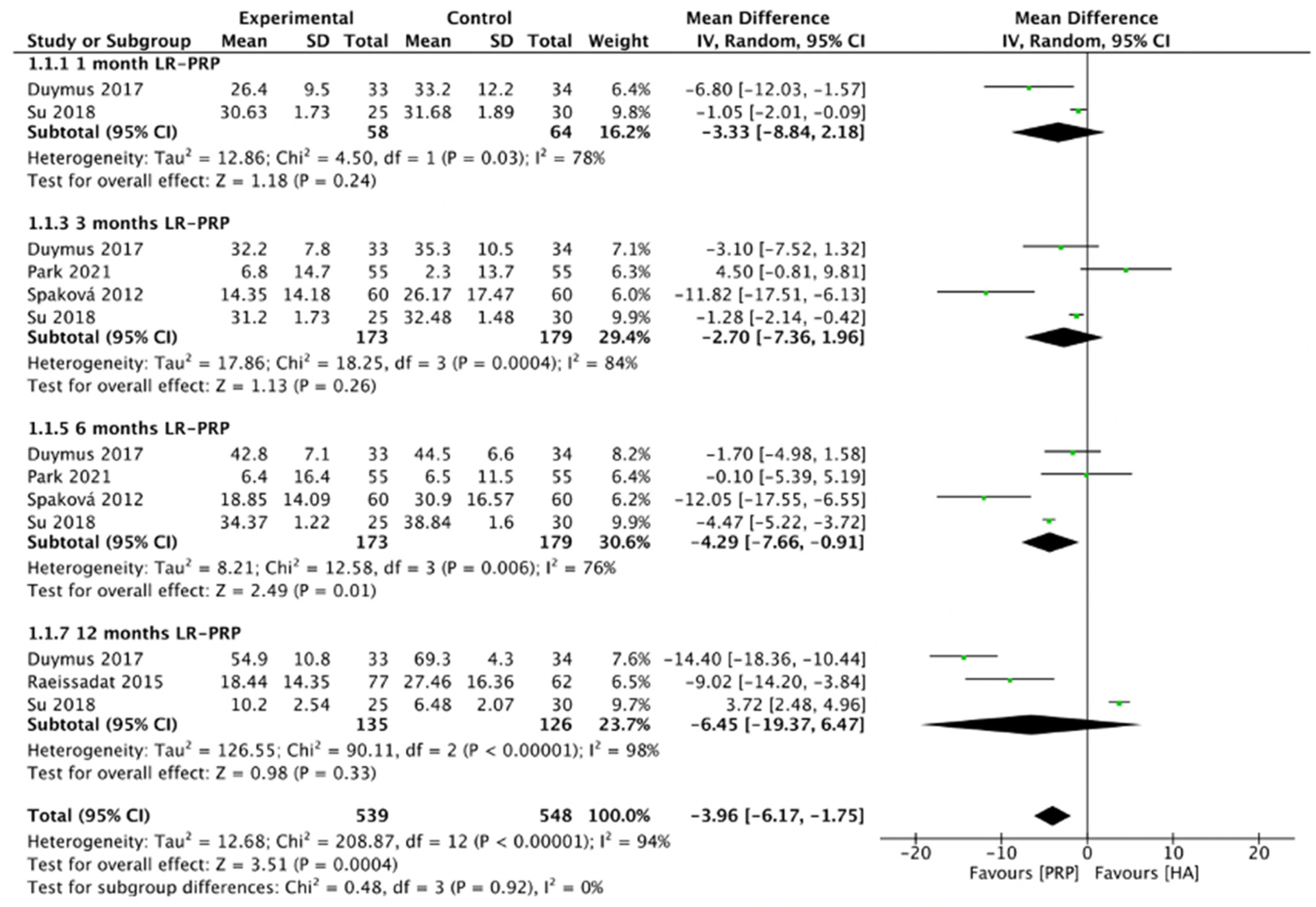
The comparison of LR-PRP and HA injections to the knee joints according to WOMAC total scores is shown in Figure 4. Due to the heterogeneity between trials being significant (I2 = 96%, p < 0.00001), the random-effect model was used. The combined analysis indicated that the LR-PRP injection was related to a decrease in WOMAC total scores as compared to the HA injection (MD = −3.96, 95% CI −6.17 to −1.75, p = 0.0004). A total of two RCTs compared WOMAC total scores at 1 month after injection (I2 = 78%, MD = −3.33, 95% CI: −8.84 to 2.18, p = 0.24) [17,19]; four studies reported WOMAC total scores at 3 months after treatment (I2 = 84%, MD = −2.7, 95% CI: −7.36 to 1.96, p = 0.26) [12,17,19,22]; four studies reported WOMAC total scores at 6 months after treatment (I2 = 95%, MD = −4.29, 95% CI: −7.66 to −0.91, p = 0.01) [12,17,19,22]; 3 studies reported WOMAC total scores at 12 months after treatment (I2 = 98%, MD = −6.45, 95% CI: −19.37 to 6.47, p = 0.33) [15,17,19]. We also performed the subgroup analysis and demonstrated that WOMAC total scores of the LR-PRP group were significantly different at 6 months after injection, compared to the HA group.
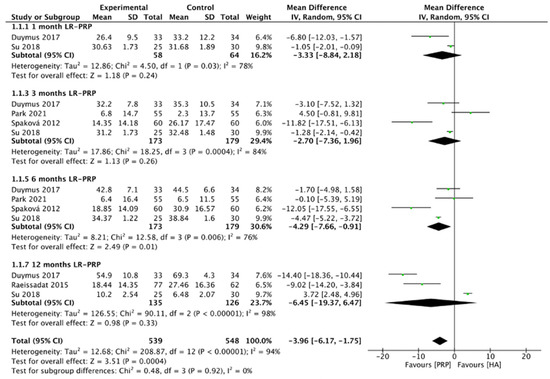
Figure 4.
Trials of LR-PRP versus HA. Forest plot of WOMAC total scores. (IV, inverse variance; CI, confidence interval; SD, standard deviation).
2.4.2. WOMAC Pain Scores (LR-PRP)
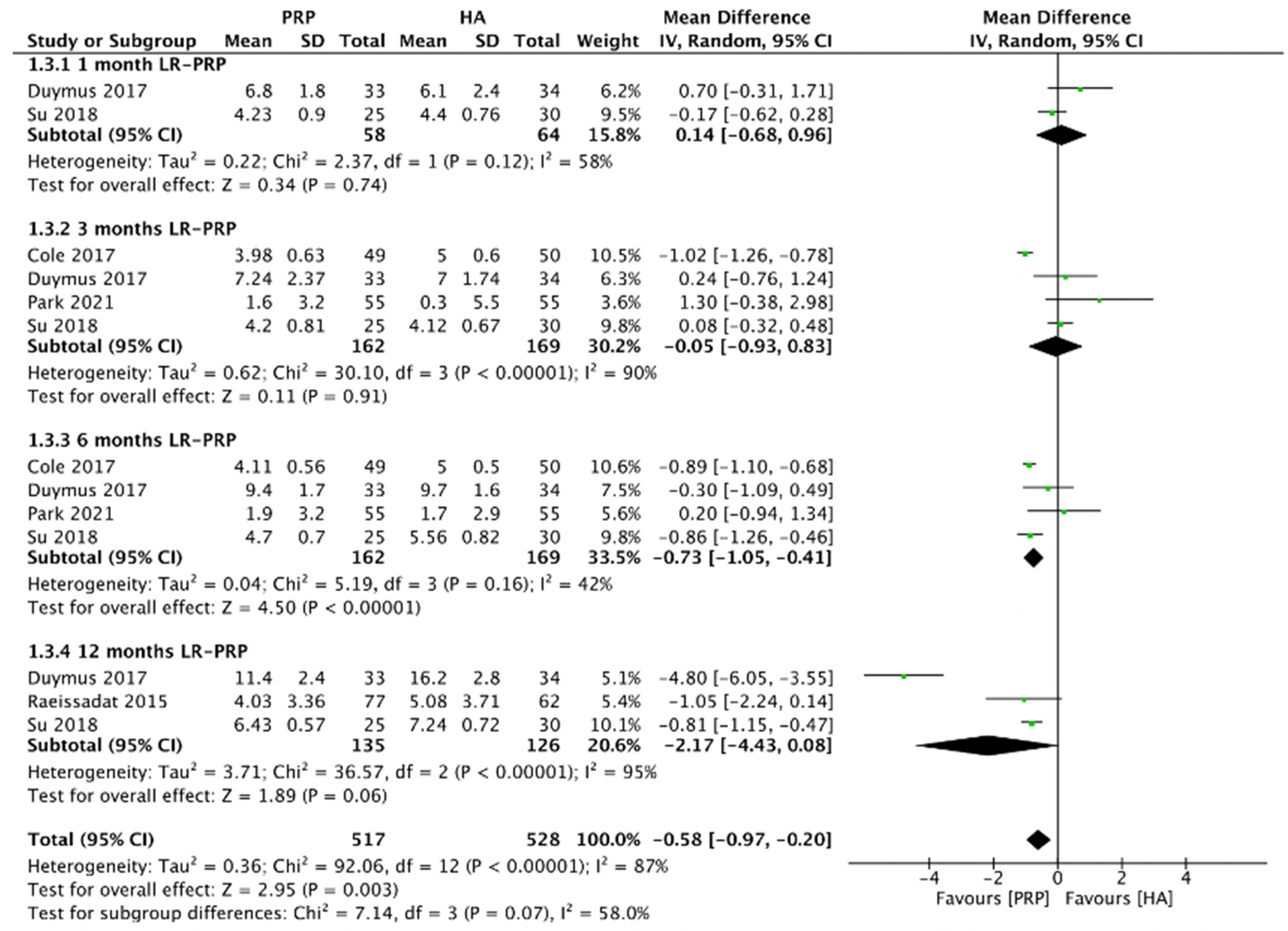
Figure 5 demonstrated the comparison of LR-PRP and HA injections to the knee joints according to WOMAC pain scores. Due to the heterogeneity between trials being significant (I2 = 87%, p < 0.00001), the random-effect model was used. The combined analysis showed that the LR-PRP injection was related to a decrease in WOMAC pain scores as compared to the HA injection (MD = −0.58, 95% CI −0.97 to −0.2, p = 0.003). A total of two RCTs compared WOMAC pain scores at 1 month after injection (I2 = 58%, MD = 0.14, 95% CI: −0.68 to 0.96, p = 0.74) [17,19]; 4 studies reported WOMAC pain scores at 3 months after treatment (I2 = 90%, MD = −0.05, 95% CI: −0.93 to 0.83, p = 0.91) [17,19,22,23]; four studies reported WOMAC pain scores at 6 months after treatment (I2 = 42%, MD = −0.73, 95% CI: −1.05 to −0.41, p < 0.00001) [17,19,22,23]; 3 studies reported WOMAC pain scores at 12 months after treatment (I2 = 95%, MD = −2.17, 95% CI: −4.43 to 0.08, p = 0.06) [15,17,19]. We also performed the subgroup analysis and demonstrated that WOMAC pain scores of the LR-PRP group were significantly different at 6 months after injection, compared to the HA group.
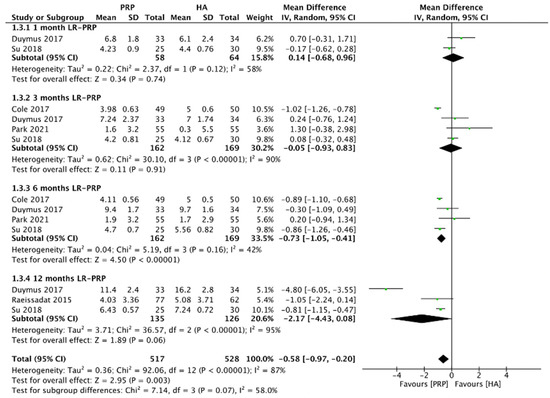
Figure 5.
Trials of LR-PRP versus HA. Forest plot of WOMAC pain scores. (IV, inverse variance; CI, confidence interval; SD, standard deviation).
2.4.3. WOMAC Stiffness Scores (LR-PRP)
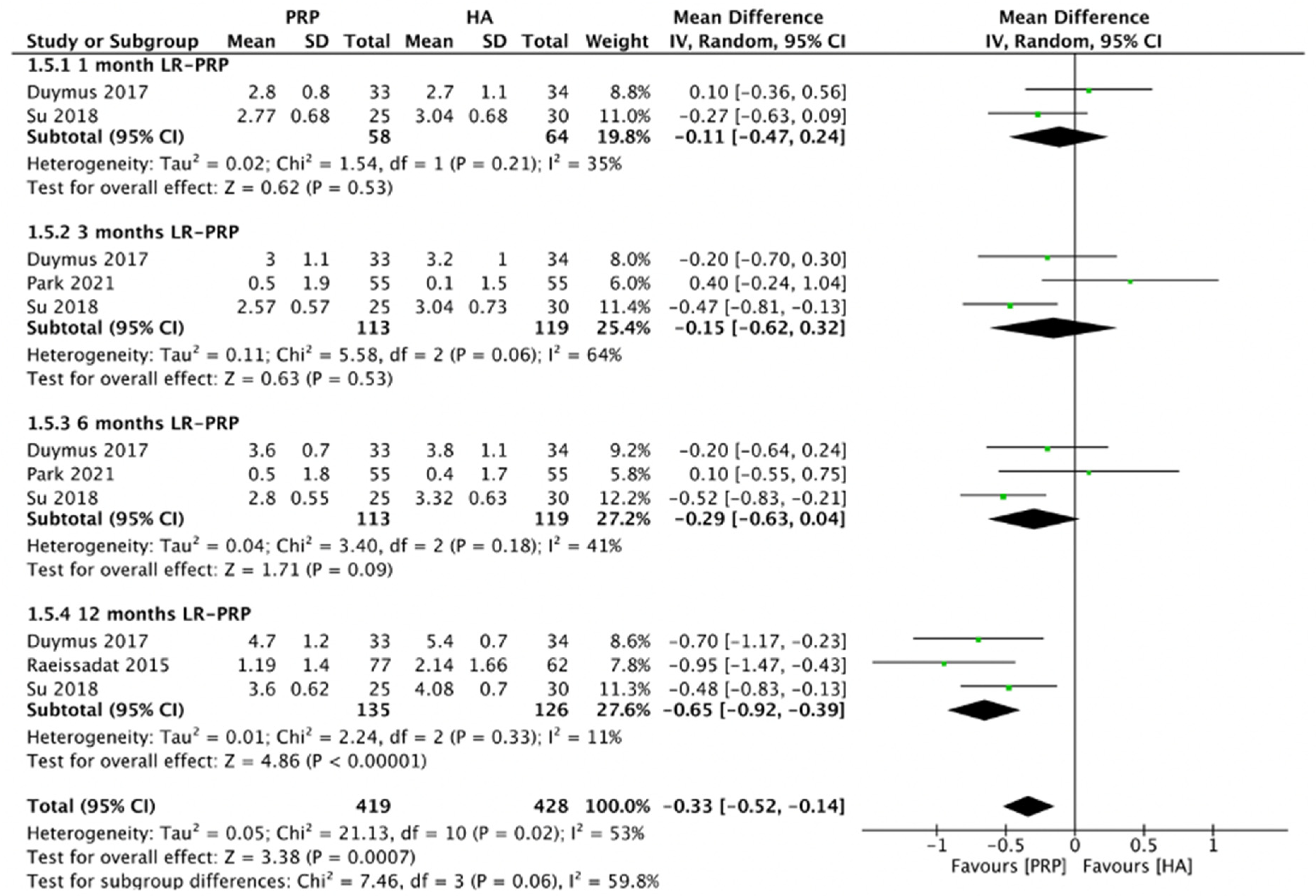
Figure 6 demonstrated the comparison of LR-PRP and HA injection to the knee joints according to WOMAC stiffness scores. Random-effect model was used as the heterogeneity between included RCTs was significant (I2 = 53%, p = 0.02). The combined analysis showed that the LR-PRP injection was related to a decrease in WOMAC stiffness scores as compared to the HA injection (MD = −0.33, 95% CI −0.52 to −0.14, p = 0.0007). A total of two RCTs reported WOMAC stiffness scores at 1 month after injection (I2 = 35%, MD = −0.11, 95% CI: −0.47 to 0.24, p = 0.53) [17,19]; three studies reported WOMAC stiffness scores at 3 months after treatment (I2 = 64%, MD = −0.15, 95% CI: −0.62 to 0.32, p = 0.53) [17,19,22]; 3 studies reported WOMAC stiffness scores at 6 months after treatment (I2 = 41%, MD = −0.29, 95% CI: −0.63 to 0.04, p = 0.09) [17,19,22]; three studies reported WOMAC stiffness scores at 12 months after treatment (I2 = 11%, MD = −0.65, 95% CI: −0.92 to −0.39, p < 0.00001) [15,17,19]. We also performed the subgroup analysis and demonstrated that WOMAC stiffness scores of the LR-PRP group were significantly different at 12 months after injection, compared to the HA group.
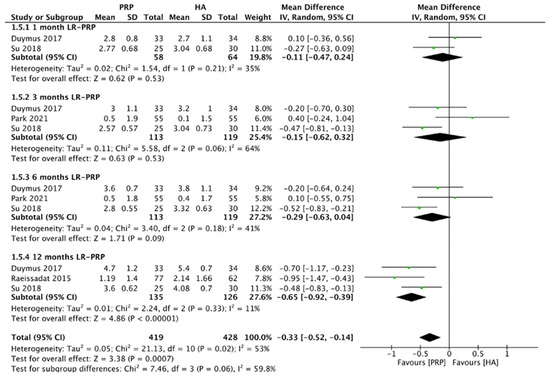
Figure 6.
Trials of LR-PRP versus HA. Forest plot of WOMAC stiffness scores. (IV, inverse variance; CI, confidence interval; SD, standard deviation).
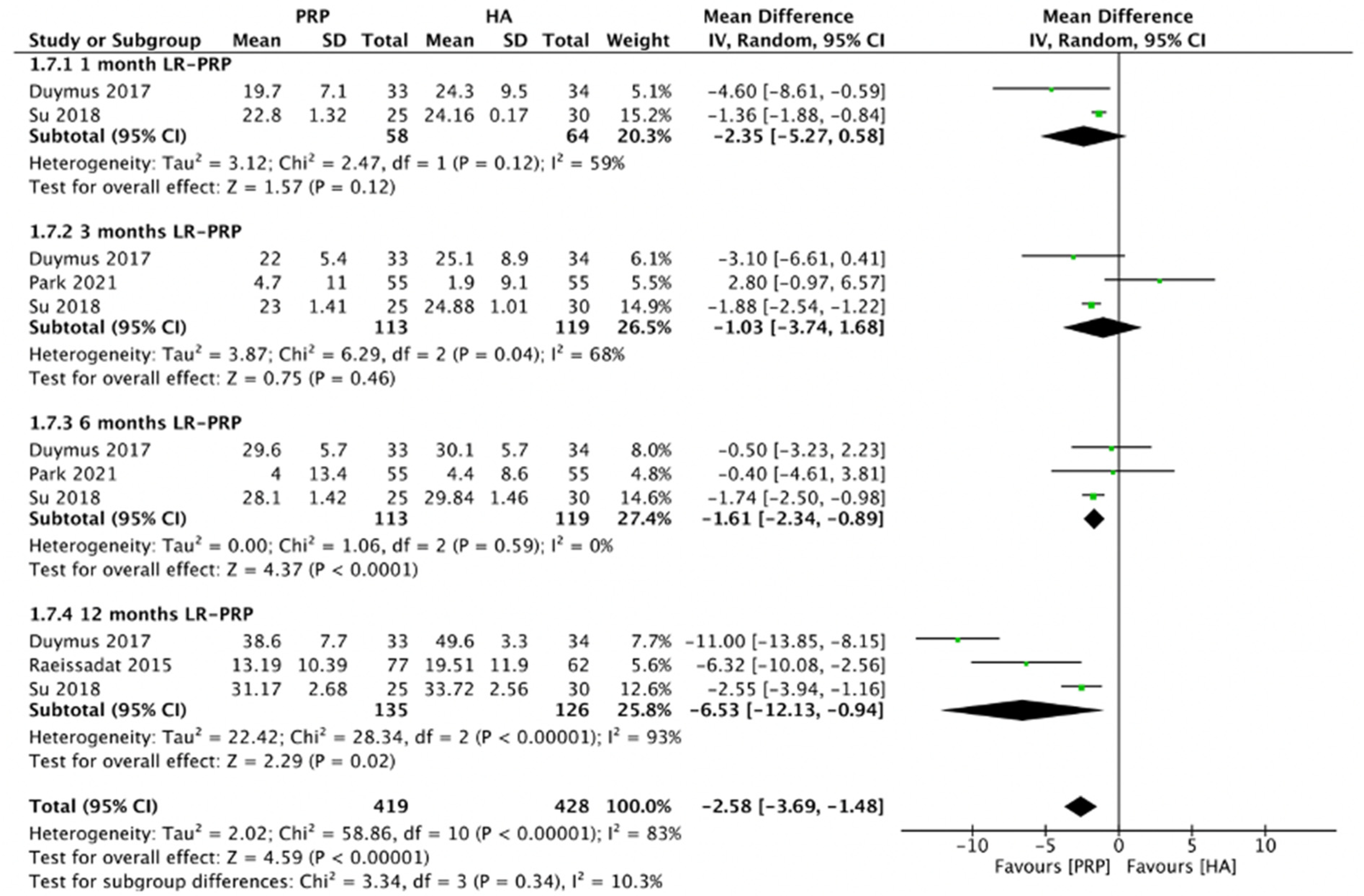
2.4.4. WOMAC Physical Function Scores (LR-PRP)
Figure 7 demonstrated the comparison of LR-PRP and HA injections to the knee joints according to WOMAC physical function scores. Due to the heterogeneity between trials being significant (I2 = 83%, p < 0.00001), the random-effect model was used. The combined analysis showed that the LR-PRP injection was related to a decrease in WOMAC physical function scores as compared to the HA injection (MD = −2.58, 95% CI −3.69 to −1.48, p < 0.00001). A total of two RCTs reported WOMAC physical function scores at 1 month after injection (I2 = 59%, MD = −2.35, 95% CI: −5.27 to 0.58, p = 0.12) [17,19]; 3 studies reported WOMAC physical function scores at 3 months after treatment (I2 = 68%, MD = −1.03, 95% CI: −3.74 to 1.68, p = 0.46) [17,19,22]; three studies reported WOMAC physical function scores at 6 months after treatment (I2 = 0%, MD = −1.61, 95% CI: −2.34 to −0.89, p < 0.0001) [17,19,22]; 3 studies reported WOMAC physical function scores at 12 months after treatment (I2 = 93%, MD = −6.53, 95% CI: −12.13 to −0.94, p= 0.02) [15,17,19]. We also performed the subgroup analysis and demonstrated that WOMAC physical function scores of the LR-PRP group were significantly different at 6 and 12 months after injection, compared to the HA group.
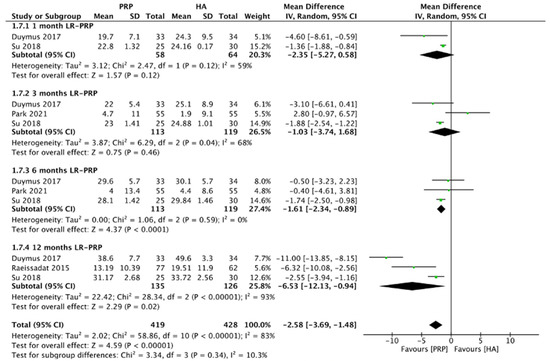
Figure 7.
Trials of LR-PRP versus HA. Forest plot of WOMAC physical functional scores. (IV, inverse variance; CI, confidence interval; SD, standard deviation).
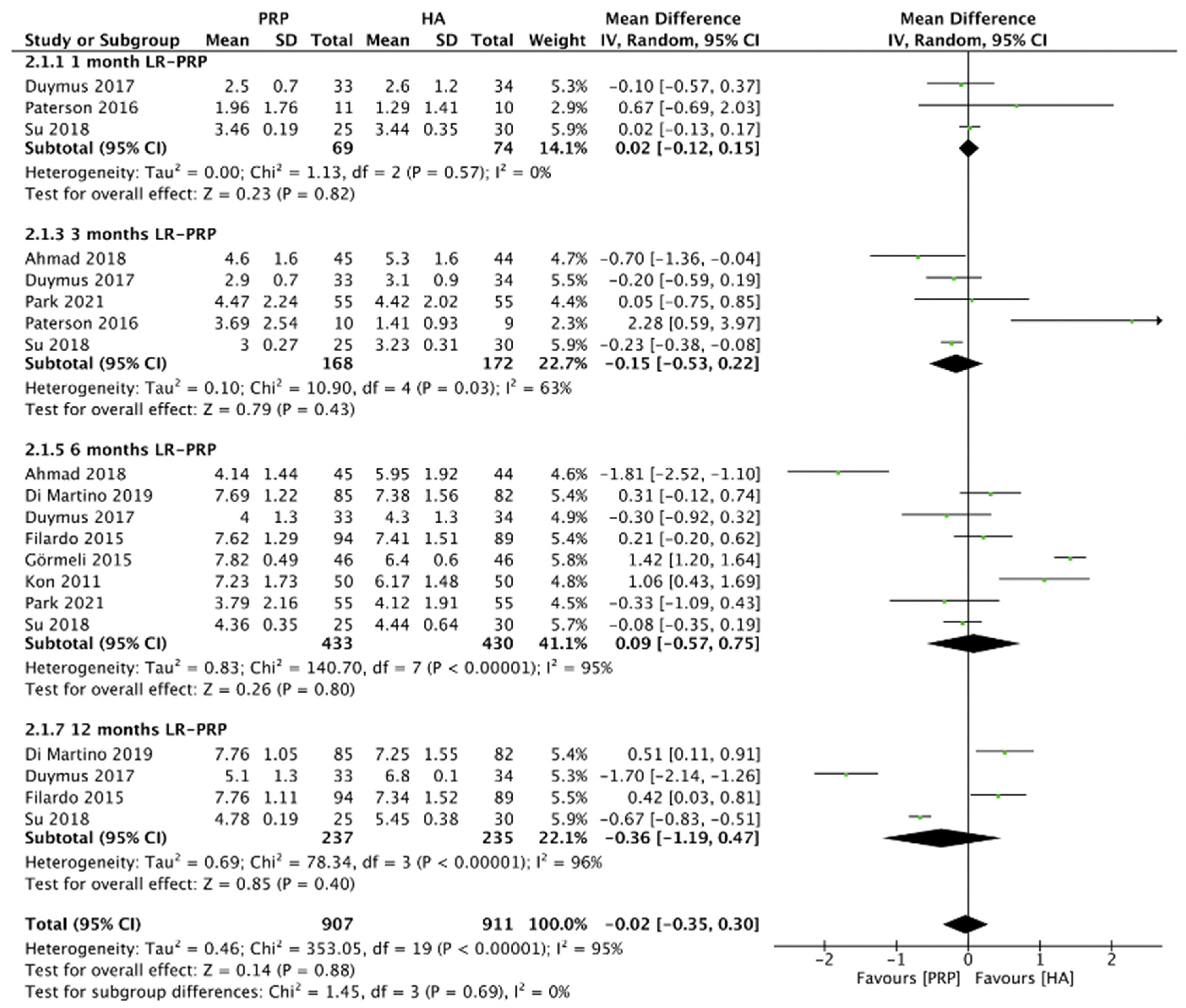
2.4.5. VAS Score (LR-PRP)
Figure 8 showed the comparison of LR-PRP and HA injection to the knee joints according to the VAS score. Due to the heterogeneity between trials being significant (I2 = 95%, p < 0.00001), the random-effect model was used. No significance of VAS score between LR-PRP injection compared to HA injection (MD = −0.02, 95% CI −0.35 to 0.30, p = 0.88) was found. A total of three RCTs reported VAS score at 1 month after injection (I2 = 0%, MD = 0.02, 95% CI: −0.12 to 0.15, p = 0.82) [16,17,19]; five studies reported VAS score at 3 months after treatment (I2 = 63%, MD = −0.15, 95% CI: −0.53 to 0.22, p = 0.43) [16,17,18,19,22]; 8 studies reported VAS score at 6 months after treatment (I2 = 95%, MD = 0.09, 95% CI: −0.57 to 0.75, p = 0.8); [10,11,13,14,17,18,19,22]; 4 studies reported VAS score at 12 months after treatment (I2 = 96%, MD = −0.36, 95% CI: −1.19 to 0.47, p = 0.4 [10,13,17,19]. We also performed the subgroup analysis and demonstrated that the VAS scores of the LR-PRP group showed no significance at 1, 3, 6, and 12 months after injection, compared to the HA group.
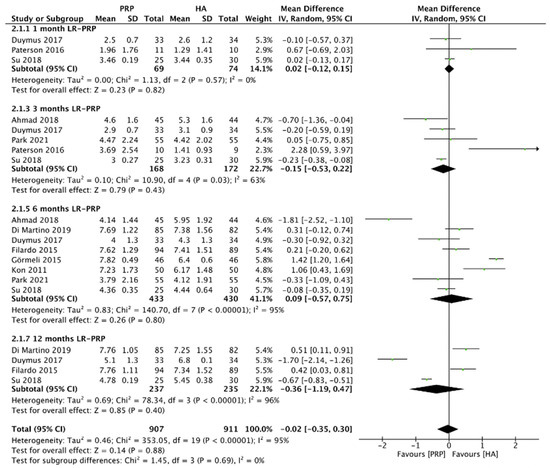
Figure 8.
Trials of LR-PRP versus HA. Forest plot of VAS scores. (IV, inverse variance; CI, confidence interval; SD, standard deviation).
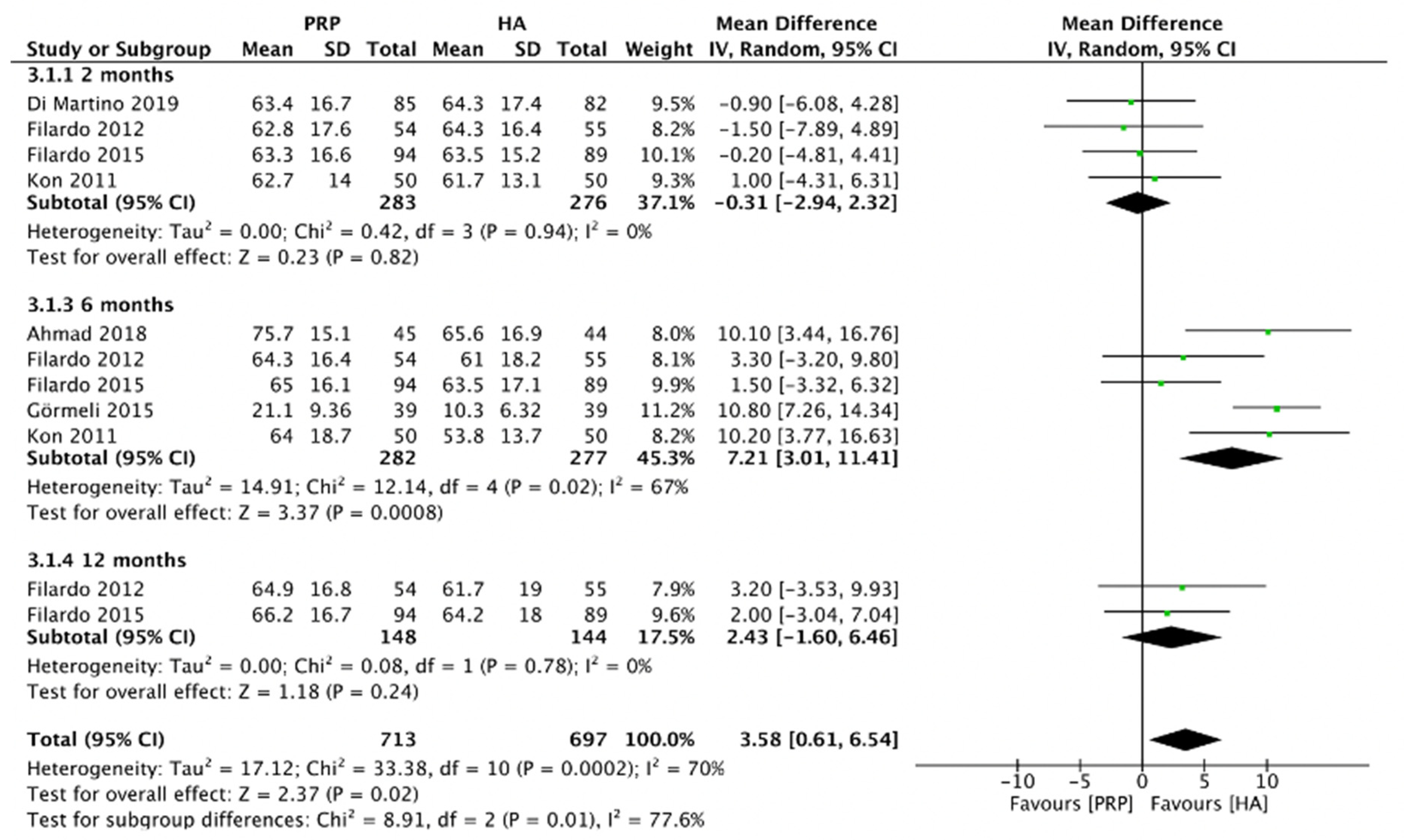
2.4.6. IKDC Score (LR-PRP)
Figure 9 showed the comparison of LR-PRP and HA injection to the knee joints according to the IKDC score. Due to the heterogeneity between trials being significant (I2 =70%, p = 0.0002), the random-effect model was used. The results showed that the HA injection was associated with a decrease in the IKDC score as compared to LR-PRP injection (MD = 3.58, 95% CI 0.61 to 6.54, p = 0.02). A total of three RCTs reported IKDC score at 2 months after injection (I2 = 0%, MD = −0.31, 95% CI: −2.94 to 2.32, p = 0.82) [9,10,13]; 5 studies reported IKDC score at 6 months after treatment (I2 = 67%, MD = 7.21, 95% CI: 3.01 to 11.41, p = 0.0008) [9,11,13,14,18]; 2 studies reported IKDC score at 12 months after treatment (I2 = 0%, MD = 2.43, 95% CI: −1.6 to 6.46, p = 0.24) [9,13]. We also performed the subgroup analysis and demonstrated that the IKDC score of the LR-PRP group was significantly different at 6 months after injection, compared to the HA group.
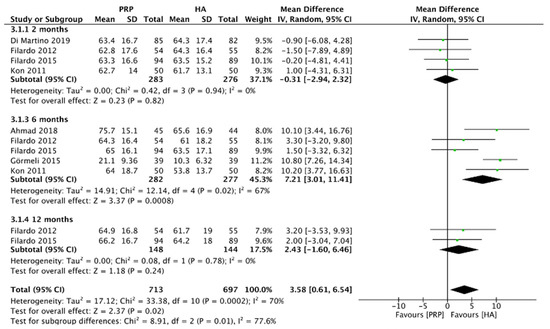
Figure 9.
Trials of LR-PRP versus HA. Forest plot of IKDC scores. (IV, inverse variance; CI, confidence interval; SD, standard deviation).
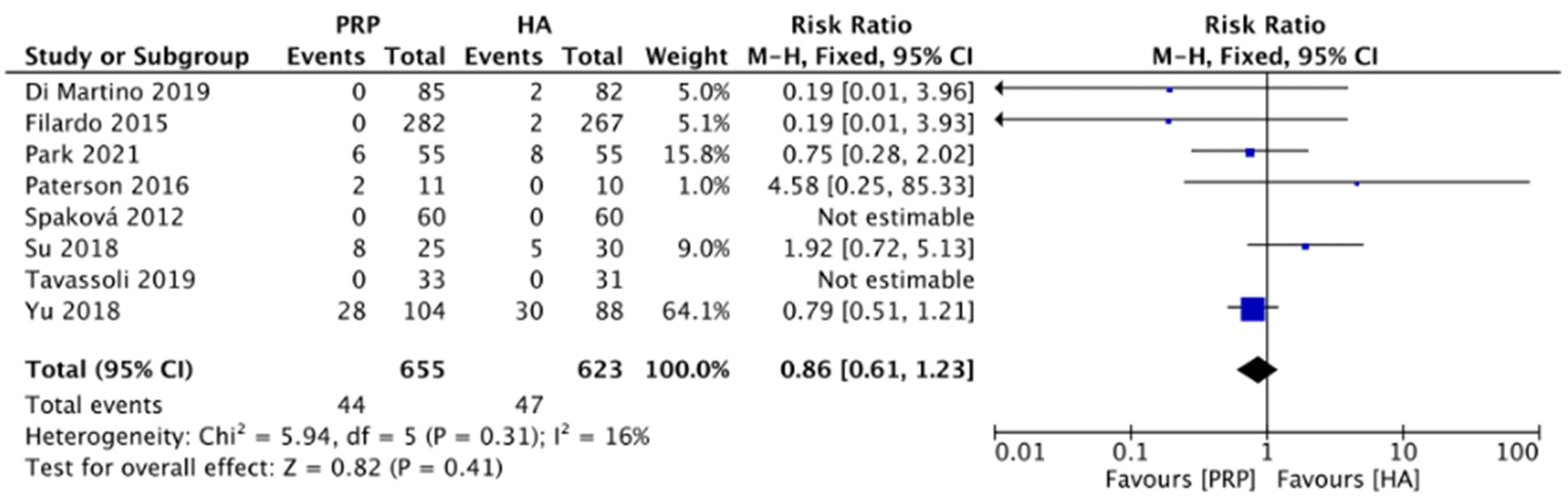
2.4.7. Adverse Events (LR-PRP)
Figure 10 compared the adverse effects between the LR-PRP and HA groups on knee OA in 8 RCTs [10,12,13,16,19,20,21,22]. The most common adverse events were worsening knee pain and swelling, vomiting, and fatigue. No major adverse events were reported in both groups. The heterogeneity test showed mild heterogeneity (I2 = 16%), thus the fixed-effects model was chosen. The results found no significance between LR-PRP and HA groups (RR: 0.86, 95% CI: 0.61 to 1.23, p = 0.41). The result indicated that LR-PRP and HA had similar safety profiles.
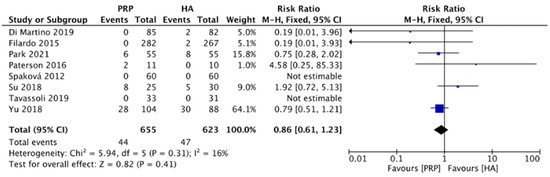
Figure 10.
Trials of LR-PRP versus HA. Forest plot of adverse effects. (M-H: Mantel Haenszel; CI, confidence interval).
3. Discussion
Due to long life expectancy, the prevalence of OA in the elderly population has increased significantly. IA LR-PRP and HA injections have been widely used as the non-surgical treatment of knee OA [24]. This study collected 14 RCTs to investigate the efficacy of IA LR-PRP and HA injections in knee OA treatment. The results showed that LR-PRP significantly improved WOMAC total scores, WOMAC pain scores, WOMAC physical function scores, and IKDC scores at 6 months as compared to the HA group. At 12 months after IA injection, WOMAC stiffness scores and WOMAC physical function scores in the LR-PRP group were significantly better than in the HA group. No significant difference in adverse events was found between LR-PRP and HA groups.
There are various pharmacologic and interventional treatments to manage knee pain caused by knee OA and to prevent the need for knee joint arthroplasty. The non-operative treatment options included oral non-steroidal anti-inflammatory drugs (NSAIDs), activity modification, massage therapy, prolotherapy, IA corticosteroids injection, IA HA injection, IA PRP injection, and IA micronized dehydrated human amnion/chorion membrane injection [1,25]. Although previous evidence showed that IA PRP injection may improve the clinical conditions of pain and functional outcomes, several controversial issues remain, such as which is the best PRP preparation method, the interval between injections, the number of needed total injections, and the validity between LR-PRP and leukocyte-poor PRP (LP-PRP) [24].
Previously, many systematic reviews and meta-analyses have investigated the effects of PRP and HA in knee OA treatment [5,8,25,26]. Dong et al. compared the efficacy of PRP with other IA injections [26]. They found that IA PRP provided better outcomes (in pain relief and functional improvement) in knee OA patients, compared with other injection treatments, such as HA, saline, and prolotherapy. Dai et al. included 10 RCTs with 1069 patients and showed that IA PRP injection may have more benefits in WOMAC total, WOMAC pain, and WOMAC physical functions scores only at 1 year after injection as compared with HA and saline in treating knee OA patients [5]. However, our analyses showed that WOMAC total scores, WOMAC pain scores, and WOMAC physical function scores of the LR-PRP group were superior to the HA group at 3, 6, and 12 months after injection. Gong et al. demonstrated that PRP had significant advantages over HA in WOMAC total scores at 1, 6, and 12 months of follow-up. Our results also showed that WOMAC total scores were better in the LR-PRP group than in the HA group at 6 and 12 months after injection [25]. Tang et al. included 20 RCTs and found that PRP injection may relieve pain more efficiently than HA injection at 6 months and 12 months after treatment [6]. The PRP group also had better WOMAC total scores, WOMAC pain scores, and WOMAC physical function scores, as compared to the HA group at 6 and 12 months after treatment. Evaluated the IKDC scores at 3 and 6 months also showed that PRP injection was significantly more effective. Our results showed that IKDC scores, WOMAC total, WOMAC pain scores, and WOMAC physical function scores of the LR-PRP group were superior to the HA group at 6 and 12 months of follow-up. However, LR-PRP injection showed no significant difference in VAS scores at 6 and 12 months of follow-ups, as compared to HA injection. Belk et al. investigated 18 RCTs including 811 patients and found that IA PRP injection can be expected to improve clinical outcomes compared with HA in treating knee OA patients [8]. The analysis of the studies which compared the LR-PRP and the LP-PRP found no significant differences in the efficacy of WOMAC scores or VAS scores. However, the analysis indicated that LP-PRP may be superior to LR-PRP in IKDC scores.
Autologous platelet-rich plasma (PRP) can be divided into leukocyte-rich PRP (LR-PRP) and leukocyte-poor PRP (LP-PRP). By definition, LR-PRP is regarded as having a neutrophil concentration above baseline. LP-PRP is regarded as having a neutrophil concentration below baseline [27]. Present understanding is that LR-PRP may be associated with pro-inflammatory effects. Catabolic cytokines, such as interleukin-1β (IL-1β), tumor necrosis factor-α, and metalloproteinases, are increased in LR-PRP, which may have deleterious effects on chondrocytes [28]. LP-PRP on the other hand increases anti-inflammatory mediators of IL-4 and IL-10, which can further suppress the release of the inflammatory mediators of TNF-α, IL-6, IL-1β. Inflammation can be further blocked by neutralizing the nuclear factor-kB activity [29]. It seems that LP-PRP may be more suitable in treating knee OA due to its anti-inflammatory effect. However, there are also reports suggesting that the application LR-PRP may be a better choice in the treatment of knee OA. LR-PRP has a high percentage of mononuclear cell (MNC) recovery. Monocytes and macrophages are believed to play a critical role in the development and progression of knee OA. These innate immune cells guide vascular remodeling and recruit local stem cells, further stimulating the regenerative function of myeloid cells [30].
When it comes to the frequency of PRP treatment, most of the included trials received three consecutive LR-PRP injections [9,10,11,12,13,14,16,18]. In a further literature search, we have discovered four studies that received two LR-PRP injection treatments [15,17,19,21]. One study received four consecutive LR-PRP injections [20]. One study has mentioned the treatment effectiveness after receiving only one LR-PRP injection [22]. Due to insufficient trials, it is difficult to perform subgroup analysis to further arrive at the conclusion as to which frequency can offer the best treatment outcome.
The ideal composition, injection intervals, and injection times of PRP for knee OA injection treatment remain controversial. Previous studies did not find improved clinical outcomes when using LP-PRP to treat knee OA [10,17,23]. However, some studies have demonstrated that LP-PRP may be superior to LR-PRP in treating knee OA [9]. LR-PRP contains higher concentrations of growth factors and leukocytes and may be more painful when injected intraarticularly. LP-PRP may have a more anti-inflammatory effect as compared with LR-PRP as fewer proteases are released from white blood cells [9]. Further studies are needed to examine the influence of leukocyte concentrations in the PRP injectant on pain relief and functional outcomes in knee OA patients.
4. Materials and Methods
The meta-analysis of this study was performed based on the recommendations of the Cochrane Handbook for Systematic Reviews of Intervention [31] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA) [32]. IRB approval is unnecessary as this study is a systematic review of previously published RCTs that does not involve further processing of the patient data. The approved PROSPERO protocol number was CRD42022347244.
4.1. Systematic Search for Trials
RCTs were searched from PubMed, Web of Science, and Cochrane Library. MeSH terms and keywords were: leukocyte-rich, platelet-rich plasma, LR-PRP, hyaluronic acid, HA, knee osteoarthritis, and arthritis, which were used in various combinations. Reference lists and bibliographies of relevant systemic reviewers were also searched manually for every publication that may provide further information on PRP and HA studies. The included RCTs in our review were published between the 1st of November 2011 and the 3rd of February 2021. Initially, the two authors (Yu-Ning Peng and Jean-Lon Chen) independently extracted data by the same standard. The authors examined the full studies separately to determine whether they met our inclusion criteria. Discrepancies were resolved through discussion between authors.
4.2. Inclusion Criteria
We limited our search to RCTs related to humans. These RCTs were published in the language of English only. The RCTs were selected based on the following inclusion criteria: RCTs that compared IA LR-PRP injections with HA injections for the management of symptomatic knee OA; and adult patients with the diagnosis of knee OA.
4.3. Exclusion Criteria
Exclusion criteria were: adolescents or children (under 18 years of age); studies that were considered as cohort, case-controlled, cross-sectional, review article, and conference abstracts; RCTs without a control group; and cadaveric or animal studies.
4.4. Risk of Bias Assessment and Data Extraction
Two authors (Yu-Ning Peng and Jean-Lon Chen) independently evaluated each RCT according to the Cochrane risk of bias assessment scale [1]. Seven categories of bias were evaluated as the followings: blinding of participants and outcome assessment, random selection, reporting bias, allocation concealment, outcome data, and other study bias. Three levels were summarized in each category (high risk, low risk, and unclear risk). Two authors (Yu-Ning Peng and Jean-Lon Chen) independently extracted the following information from each included trial: first author’s name, publication year, country of origin, study type, number of patients, age, gender, and outcome measurements, and follow-up periods. We also collected injection time intervals and dosage of LR-PRP and HA injections. All the data were extracted from the RCTs from tables and texts.
4.5. Data Analysis
The systematic review and meta-analysis were conducted by Review Manager 5.3 (Nordic Cochrane Center, Cochrane Collaboration, Copenhagen, Sweden). We used mean differences (MD) and standard deviation (SD) to compare continuous variables. All data were reported with 95% confidence intervals (CI). We set the level of significance as p < 0.05. Higgins I2 statistic was used to evaluate the heterogeneity of individual studies. The fixed-effects model was utilized if no obvious heterogeneity existed (if I2 < 50%). Otherwise, a random-effects model was utilized (if p < 0.1 and I2 > 50%).
5. Limitations and Conclusions
There are some limitations to this study. First, all the included trials in this study were published in English, which may lead to the possibility of selection bias. Second, most of the analyses showed high heterogeneity. Although we tried to minimize the heterogeneity by performing subgroup analyses, high heterogeneity can still be observed in some results. This may be caused by the heterogeneity among patients, including gender, age, and the severity of knee OA. Other influential factors include the difference in PRP injection technique between studies, such as the frequency of PRP injections, injection volume, and injection intervals. Finally, some RCTs’ relatively small patient sample sizes limited the study power.
In conclusion, this is the first meta-analysis that demonstrated that IA LR-PRP injection showed better overall outcomes as compared to IA HA injection in patients with knee OA at 3-, 6-, and 12-month follow-up periods, in terms of WOMAC pain scores, WOMAC physical function scores, WOMAC total scores, and IKDC scores. LR-PRP injection offers a better overall treatment outcome as compared with HA in knee OA patients. As a result, IA LR-PRP injections offer better outcomes in treating knee OA patients, as compared with HA during both short-term and long-term follow-up periods.
Author Contributions
Conceptualization, Y.-N.P., C.P.C.C. and A.S.; Formal analysis, Y.-N.P. and J.-L.C.; Methodology, all authors; Investigation, Y.-N.P., J.-L.C. and C.P.C.C.; Writing—Original Draft Preparation Y.-N.P., J.-L.C. and C.-C.H.; Writing—Review and Editing, Y.-N.P., C.P.C.C. and A.S.; Supervision, C.P.C.C. and A.S.; Project Administration, C.P.C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval and review were waived due to this is a systematic review and meta-analysis, and the included RCTs had all received the IRB.
Informed Consent Statement
Patient consent was waived, due to all the included RCTs receiving the informed consent statement.
Data Availability Statement
Data sharing not applicable.
Acknowledgments
This meta-analysis study was conducted as one part of the series of our research on regenerative medicine. The topics covered in our research include the application of knee intra-articular low level laser therapy (LLLT), and the injection of autologous platelet-rich plasma (PRP), dextrose solution, and micronized dehydrated human amnion/chorion membrane in treating knee osteoarthritis. Grants issued by the Chang Gung Memorial Hospital at Linkou Research Project Grants to conduct these studies were CMRPG5M0071 (IRB: 202200443) and CMRPG5L0061 (IRB:202100425A3). These grants were issued to Carl P.C. Chen.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Alden, K.J.; Harris, S.; Hubbs, B.; Kot, K.; Istwan, N.B.; Mason, D. Micronized Dehydrated Human Amnion Chorion Membrane Injection in the Treatment of Knee Osteoarthritis—A Large Retrospective Case Series. J. Knee Surg. 2021, 34, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Prodromos, C.C.; Finkle, S.; Dawes, A.; Dizon, A. Intra-Articular Laser Treatment Plus Platelet Rich Plasma (PRP) Significantly Reduces Pain in Many Patients Who Had Failed Prior PRP Treatment. Medicines 2019, 6, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spreafico, A.; Chellini, F.; Frediani, B.; Bernardini, G.; Niccolini, S.; Serchi, T.; Collodel, G.; Paffetti, A.; Fossombroni, V.; Galeazzi, M.; et al. Biochemical investigation of the effects of human platelet releasates on human articular chondrocytes. J. Cell. Biochem. 2009, 108, 1153–1165. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.; Awad, M.E.; Hamrick, M.W.; Hunter, M.; Fulzele, S. Recent advances in hyaluronic acid based therapy for osteoarthritis. Clin. Transl. Med. 2018, 7, 6. [Google Scholar] [CrossRef] [Green Version]
- Dai, W.L.; Zhou, A.G.; Zhang, H.; Zhang, J. Efficacy of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-analysis of Randomized Controlled Trials. Arthroscopy 2017, 33, 659–670.e651. [Google Scholar] [CrossRef]
- Tang, J.Z.; Nie, M.J.; Zhao, J.Z.; Zhang, G.C.; Zhang, Q.; Wang, B. Platelet-rich plasma versus hyaluronic acid in the treatment of knee osteoarthritis: A meta-analysis. J. Orthop. Surg. Res. 2020, 15, 403. [Google Scholar] [CrossRef]
- Braun, H.J.; Kim, H.J.; Chu, C.R.; Dragoo, J.L. The effect of platelet-rich plasma formulations and blood products on human synoviocytes: Implications for intra-articular injury and therapy. Am. J. Sports Med. 2014, 42, 1204–1210. [Google Scholar] [CrossRef] [Green Version]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2021, 49, 249–260. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Di Martino, A.; Di Matteo, B.; Merli, M.L.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Platelet-rich plasma vs hyaluronic acid to treat knee degenerative pathology: Study design and preliminary results of a randomized controlled trial. BMC Musculoskelet. Disord. 2012, 13, 229. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, A.; Di Matteo, B.; Papio, T.; Tentoni, F.; Selleri, F.; Cenacchi, A.; Kon, E.; Filardo, G. Platelet-Rich Plasma Versus Hyaluronic Acid Injections for the Treatment of Knee Osteoarthritis: Results at 5 Years of a Double-Blind, Randomized Controlled Trial. Am. J. Sports Med. 2019, 47, 347–354. [Google Scholar] [CrossRef]
- Kon, E.; Mandelbaum, B.; Buda, R.; Filardo, G.; Delcogliano, M.; Timoncini, A.; Fornasari, P.M.; Giannini, S.; Marcacci, M. Platelet-rich plasma intra-articular injection versus hyaluronic acid viscosupplementation as treatments for cartilage pathology: From early degeneration to osteoarthritis. Arthroscopy 2011, 27, 1490–1501. [Google Scholar] [CrossRef] [PubMed]
- Spakova, T.; Rosocha, J.; Lacko, M.; Harvanova, D.; Gharaibeh, A. Treatment of knee joint osteoarthritis with autologous platelet-rich plasma in comparison with hyaluronic acid. Am. J. Phys. Med. Rehabil. 2012, 91, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Filardo, G.; Di Matteo, B.; Di Martino, A.; Merli, M.L.; Cenacchi, A.; Fornasari, P.; Marcacci, M.; Kon, E. Platelet-Rich Plasma Intra-articular Knee Injections Show No Superiority Versus Viscosupplementation: A Randomized Controlled Trial. Am. J. Sports Med. 2015, 43, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- Gormeli, G.; Gormeli, C.A.; Ataoglu, B.; Colak, C.; Aslanturk, O.; Ertem, K. Multiple PRP injections are more effective than single injections and hyaluronic acid in knees with early osteoarthritis: A randomized, double-blind, placebo-controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 958–965. [Google Scholar] [CrossRef]
- Raeissadat, S.A.; Rayegani, S.M.; Hassanabadi, H.; Fathi, M.; Ghorbani, E.; Babaee, M.; Azma, K. Knee Osteoarthritis Injection Choices: Platelet- Rich Plasma (PRP) Versus Hyaluronic Acid (A one-year randomized clinical trial). Clin. Med. Insights Arthritis Musculoskelet. Disord. 2015, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Paterson, K.L.; Nicholls, M.; Bennell, K.L.; Bates, D. Intra-articular injection of photo-activated platelet-rich plasma in patients with knee osteoarthritis: A double-blind, randomized controlled pilot study. BMC Musculoskelet. Disord. 2016, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Duymus, T.M.; Mutlu, S.; Dernek, B.; Komur, B.; Aydogmus, S.; Kesiktas, F.N. Choice of intra-articular injection in treatment of knee osteoarthritis: Platelet-rich plasma, hyaluronic acid or ozone options. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 485–492. [Google Scholar] [CrossRef]
- Ahmad, H.S.; Farrag, S.E.; Okasha, A.E.; Kadry, A.O.; Ata, T.B.; Monir, A.A.; Shady, I. Clinical outcomes are associated with changes in ultrasonographic structural appearance after platelet-rich plasma treatment for knee osteoarthritis. Int. J. Rheum. Dis. 2018, 21, 960–966. [Google Scholar] [CrossRef]
- Su, K.; Bai, Y.; Wang, J.; Zhang, H.; Liu, H.; Ma, S. Comparison of hyaluronic acid and PRP intra-articular injection with combined intra-articular and intraosseous PRP injections to treat patients with knee osteoarthritis. Clin. Rheumatol. 2018, 37, 1341–1350. [Google Scholar] [CrossRef]
- Yu, W.; Xu, P.; Huang, G.; Liu, L. Clinical therapy of hyaluronic acid combined with platelet-rich plasma for the treatment of knee osteoarthritis. Exp. Ther. Med. 2018, 16, 2119–2125. [Google Scholar] [CrossRef] [Green Version]
- Tavassoli, M.; Janmohammadi, N.; Hosseini, A.; Khafri, S.; Esmaeilnejad-Ganji, S.M. Single- and double-dose of platelet-rich plasma versus hyaluronic acid for treatment of knee osteoarthritis: A randomized controlled trial. World J. Orthop. 2019, 10, 310–326. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.B.; Kim, J.H.; Ha, C.W.; Lee, D.H. Clinical Efficacy of Platelet-Rich Plasma Injection and Its Association With Growth Factors in the Treatment of Mild to Moderate Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial As Compared With Hyaluronic Acid. Am. J. Sports Med. 2021, 49, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.J.; Karas, V.; Hussey, K.; Pilz, K.; Fortier, L.A. Hyaluronic Acid Versus Platelet-Rich Plasma: A Prospective, Double-Blind Randomized Controlled Trial Comparing Clinical Outcomes and Effects on Intra-articular Biology for the Treatment of Knee Osteoarthritis. Am. J. Sports Med. 2017, 45, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.P.C.; Hsu, C.C.; Huang, S.C.; Lin, M.Y.; Chen, J.L.; Lin, S.Y. The application of thermal oscillation method to augment the effectiveness of autologous platelet rich plasma in treating elderly patients with knee osteoarthritis. Exp. Gerontol. 2020, 142, 111120. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Li, K.; Xie, R.; Du, G.; Li, L.; Wang, S.; Yin, J.; Gu, J.; Wang, P.; Chen, M.; et al. Clinical therapy of platelet-rich plasma vs hyaluronic acid injections in patients with knee osteoarthritis: A systematic review and meta-analysis of randomized double-blind controlled trials. Medicine 2021, 100, e25168. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Zhang, B.; Yang, Q.; Zhu, J.; Sun, X. The effects of platelet-rich plasma injection in knee and hip osteoarthritis: A meta-analysis of randomized controlled trials. Clin. Rheumatol. 2021, 40, 263–277. [Google Scholar] [CrossRef]
- Le, A.D.K.; Enweze, L.; DeBaun, M.R.; Dragoo, J.L. Current Clinical Recommendations for Use of Platelet-Rich Plasma. Curr. Rev. Musculoskelet. Med. 2018, 11, 624–634. [Google Scholar] [CrossRef]
- Sundman, E.A.; Cole, B.J.; Fortier, L.A. Growth Factor and Catabolic Cytokine Concentrations Are Influenced by the Cellular Composition of Platelet-Rich Plasma. Am. J. Sport Med. 2011, 39, 2135–2140. [Google Scholar] [CrossRef]
- Simental-Mendia, M.; Vilchez-Cavazos, J.; Pena-Martinez, V.M.; Said-Fernandez, S.; Lara-Arias, J.; Martinez-Rodriguez, H.G. Leukocyte-poor platelet-rich plasma is more effective than the conventional therapy with acetaminophen for the treatment of early knee osteoarthritis. Arch. Orthop. Trauma Surg. 2016, 136, 1723–1732. [Google Scholar] [CrossRef]
- Uchiyama, R.; Toyoda, E.; Maehara, M.; Wasai, S.; Omura, H.; Watanabe, M.; Sato, M. Effect of Platelet-Rich Plasma on M1/M2 Macrophage Polarization. Int. J. Mol. Sci. 2021, 22, 2336. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Chichester, UK; Hoboken, NJ, USA, 2008. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).