Abstract
Opioids are the strongest analgesics available and are crucial in the treatment of acute and chronic pain. The line between these critical medications and how they are used beyond standard therapeutics in cases such as abuse, misuse, and medication errors needs to be understood, as it affects their safety, efficacy, and manner of use. The aim of this systematic review was to identify what is known about the adverse events resulting from the abuse, misuse, and medication errors associated with opioid use. A systematic search was conducted in the PubMed®, Scopus® and, EBSCO® databases to retrieve studies from the inception to December 2023 reporting abuse, misuse, and medication errors associated with medicinal opioid use. Two authors independently screened titles and abstracts and full text according to eligibility using Covidence® software. Full articles were examined by two independent reviewers, and disagreements were resolved by a third reviewer. The risk of bias was assessed by the JBI’s critical appraisal tools. A total of 934 articles were screened by their title and abstract. Then, 151 articles were selected for full text screening. Of these, 34 studies were eligible for inclusion in this review. The included studies varied significantly in their population sizes, ranging from 9 individuals to 298,433 patients, and encompassed a diverse demographic, including all ages and both sexes. The studies consistently reported a range of adverse events associated with opioid use. Fentanyl, morphine, oxycodone, tramadol, and hydrocodone were frequently implicated. The data heterogeneity in this field resulted in challenges in drawing conclusions. The review highlights that some opioids, particularly fentanyl, morphine, and oxycodone, are frequently associated with preventable adverse drug reactions, abuse, and medication errors, underscoring the need for robust preventative measures and ongoing research to mitigate opioid-related harm.
1. Introduction
Every day, millions of people make use of medicines, some only occasionally, others on a daily basis. While medicines are fundamentally designed to benefit health, their use also involves risks [1,2,3]. Despite rigorous assessments of their quality, safety, and efficacy by regulatory bodies, to ensure a favorable benefit-risk balance at the time of authorization, adverse drug reactions (ADRs) remain a significant concern [1]. ADRs can range from mild to severe, potentially resulting in hospitalization or, tragically, death [4]. A comprehensive review in Europe highlighted that approximately 3.6% of all hospital admissions are due to adverse reactions and about 10% of patients experience an ADR during their hospital stay [5], both children and adults [6,7].
Different definitions of ADR can be found in the literature [8,9]. The WHO defines an adverse drug reaction as “a response to a drug that is noxious and unintended and occurs at doses normally used in man for the prophylaxis, diagnosis or therapy of disease, or for modification of physiological function” [8,10]. Although, in Europe, the definition is actually broader [11], with the European Medicines Agency (EMA) defining an adverse drug reaction as “a noxious and unintended response to a medicine”. This definition was applied in European Union after the change in Pharmacovigilance legislation in 2012 due to the implementation of the Directive 2010/84/EU [11]. The term adverse reaction started to not only include effects from authorized use of the medicinal product and recommended doses but also reactions occurring in different patterns of use (e.g., overdose, abuse, misuse, off-label use, medication errors, or use of falsified products) [11,12]. Abuse of a medicinal product can be defined as a “persistent or sporadic, intentional excessive use of medicinal products which is accompanied by harmful physical or psychological effects”, misuse of a medicinal product is defined as “situations where a medicinal product is intentionally and inappropriately used not in accordance with the terms of the marketing authorization”, while medication error can be defined as “an unintended failure in the drug treatment process that leads to, or has the potential to lead to, harm to the patient” [13]. The relationship between these definitions are represented in a Venn diagram in Figure 1.
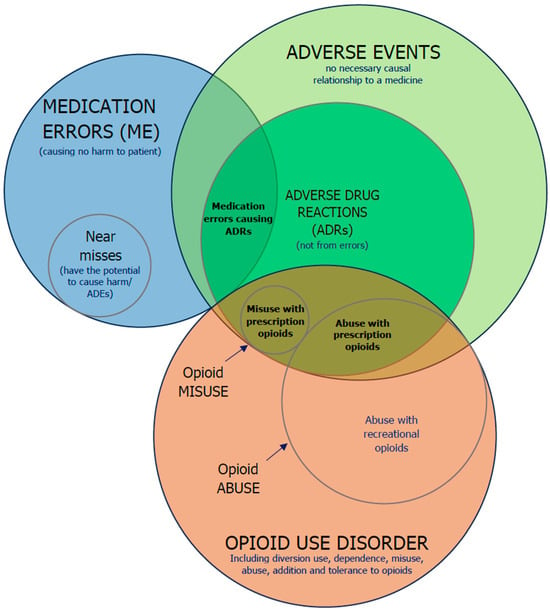
Figure 1.
A Venn diagram showing the relation among adverse events, ADRs, medication errors and opioid use disorder; the sizes of the plots do not reflect the relative frequencies of the events illustrated. Illustration supported on the research of previous authors [14,15,16,17,18].
Opioids
Opioids are agents which binds to the opioid receptors in the human body [19]. They are classified as the strongest painkillers and play an important role in managing short- and medium-term pain, but their use for long-term pain is debatable [20]. Opioid receptors are G protein-coupled receptors that mediate the effects of opioids, both endogenous (like endorphins) and exogenous (such as morphine and fentanyl) [21]. The main types of opioid receptors are mu (μ), delta (δ), kappa (κ), nociceptin/orphanin (N/OFQ), and zeta (ZOR). Mu receptors primarily provide pain relief and euphoria; delta receptors are involved in pain relief and mood regulation; kappa receptors produce pain relief but can also cause dysphoria; nociceptin receptors modulate pain and influence anxiety and memory [21,22]. The response can be agonistic, partial agonistic, or antagonistic, but the majority of opioids used in clinical settings elicit an agonistic response, resulting in analgesia [19].
ADRs associated with opioids include respiratory depression, constipation, nausea, vomiting, abdominal pain, bloating, cramping, sedation, confusion, hallucinations, hyperalgesia, central sensitization, pruritus, analgesic tolerance, and addiction liability [19,23,24,25,26], which can affect patients’ quality of life leading to discontinue opioid treatment and, therefore, inadequate pain control [27]. The administration route also determines the pattern of ADRs associated with each opioid. Different administration methods, such as oral, intravenous, transdermal, and intrathecal, can significantly influence the onset, intensity, and type of ADRs experienced by patients [28]. Intravenous administration is more susceptible to the development of ADRs, unlike intramuscular and subcutaneous routes [29]. However, the long-term effectiveness of opioids in managing pain is a topic of debate, with concerns raised about their efficacy over extended periods [20,30].
Long-term use of opioids has been found to cause tolerance that reduces the effectiveness of such drugs, leading to shorter opioid duration of action with repeat administrations [31,32,33]. This tolerance, which is characterized by a decrease in the potency of the drug with repeated administration, is a significant concern with long-term opioid therapy [31], contributing to challenges in the management of chronic pain. Furthermore, prolonged use of opioid therapy has shown a connection with increased possibility of later opioid dependence and overdose without improving functional status [34].
In the past two decades, nearly 600,000 people in the USA and Canada died from opioid overdose events [35]. The opioid crisis in the U.S. has been one of the biggest public health threats in recent decades, with more than 500,000 deaths since 2005 [36], significant reductions in life expectancy, and the development of secondary health conditions including infection, sleep, and affective disorders [37,38]. This crisis developed over the years from the overprescribing of pain relievers and progressed through different stages, from heroin to highly potent synthetic opioid use, such as fentanyl [39]. These substances have exacerbated the epidemic, highlighting the crisis’s dynamic nature and the necessity of addressing polysubstance use [40]. As substances like fentanyl become more common, the risk of overdoses grows, highlighting the urgent need to improve prevention and treatment efforts that address both opioid use and its overlap with other drug use [40].
The ongoing crisis increases mortality but also inflicts broad medical, social, and economic hardships. It was estimated that 1.2 million people might die from opioid overdose by 2029 [35,41]. Recent studies from USA shows that 4.4% of the patients that were prescribed opioids misused them [42], and that in 2020, approximately 9.5 million people misused opioids. Similarly, the European continent has also experienced a rise in opioid use, with misuse and abuse leading to a significant increase in admissions to substance abuse treatment programs and deaths from overdose [43]. Additionally, research has emphasized the importance of estimating the healthcare burden of prescription opioid abuse in European countries in order to develop effective strategies for managing opioid-related issues [44].
In this sense, the aim of this systematic review was to identify what is known about the adverse events resulting from the abuse, misuse, and medication errors associated with opioid use.
2. Methods
The protocol of this systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO registration number CRD42022358490). The review was structured followed the Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) guidelines [45]. The complete PRISMA checklist is available in Table S1.
2.1. Search Strategy
A literature search was conducted from inception to December 2023 in the following databases: PubMed®, Scopus®, and EBSCO®. The search strategy is presented in Supplementary Materials Tables S2–S4. All studies were extracted and exported to Covidence ® software (Covidence Systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org) for screening, review, and data extraction. To reduce the risk of overlooking relevant articles, the reference lists of identified relevant articles were reviewed, and an additional search was conducted using similar search terms.
2.2. Eligibility Criteria
Studies about opioids that involved AEs and either abuse, misuse, or medication errors were included. There was no restriction on age, sex, or geographic location. Systematic reviews, preclinical studies, and studies without information of abuse, misuse, or medication errors related to opioids were excluded. Studies not authored in English or that were not possible to translate with clarity were also excluded.
2.3. Strategy for Data Synthesis
The Covidence® software (https://www.covidence.org/) was used to screen, select, and extract data from the articles. Covidence® was chosen because it improves evidence synthesis by enhancing the efficiency of the systematic review. The software mirrors the multiphase review process, including data extraction, directly in its design [46]. Imported duplicates were automatically removed by the software. A title and abstract screening were performed by two independent reviewers (MG and VS), and disagreements were resolved between the two parties or by discussion with a third reviewer (CV). The included articles from the abstract and title screening were subjected to a full text review. Articles were excluded based on criteria such as incorrect outcome, incorrect study design, incorrect setting, or because full-text was not possible to obtain. The data extraction was performed according to the data extraction table (see Supplementary Materials Table S5) by two authors (MG and VS) and reviewed by a third author (CV). Figure 2 represents the preferred reporting items for systematic reviews and meta-analysis flow diagram.
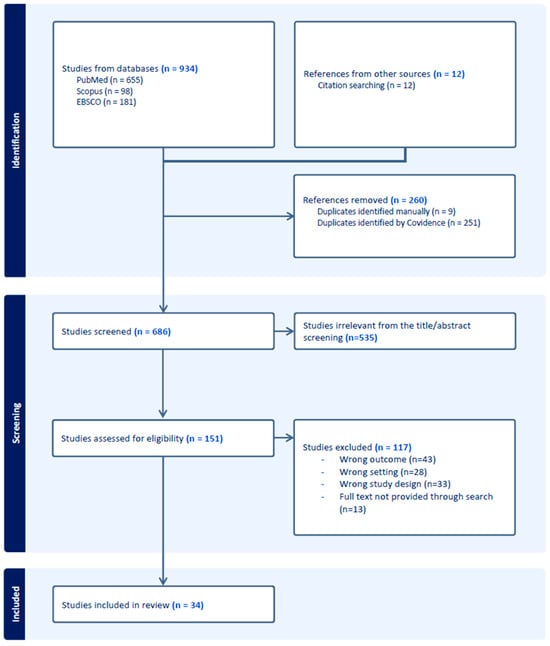
Figure 2.
Preferred reporting items for systematic reviews and meta-analysis flow diagram.
2.4. Quality Assessment
The quality of the 34 included studies were assessed by using the JBI’s critical appraisal tools. JBI is an international research organization which develops and delivers evidence-based information, software, education, and training designed to improve healthcare practice and health outcomes, including the critical appraisal tools to assess the methodological quality of a study and to determine the extent to which a study has addressed the possibility of bias in its design, conduct and analysis. The JBI tool for case series was applied to the 25 case series studies. The JBI tool for cohort studies was applied to the nine cohort studies. The result of the quality assessment is presented in the Supplementary Materials—see Tabled S6 and S7. Based on the risk of bias score, no paper was rejected.
3. Results
In the 34 included studies, the research population ranged from 9 [47] to 298,433 patients [48]. The studies included different age ranges, including pediatric population [49,50,51,52], elderly [53,54], or all ages [28,35,48,55,56,57,58,59,60,61,62]. Other references used that did not specify the age of their patients [63,64,65,66]. In one publication, abuse was the only exposure investigated [60]. In the remaining studies, medication errors were either the only topic of investigation [49,50,52,53,55,58,62,63,64,66,67,68,69,70,71,72,73,74,75,76] or were combined with abuse [28,56,57,60,65,77,78,79,80,81,82,83,84] or unintentional misuse [48]. Additional issues such as addiction, AEs [28,54,65,78,83,84,85], and overdose were also addressed in different studies [35,64,65,79] (Table 1).

Table 1.
Summary of the data included in this study.
3.1. Prevalence of Opioid Abuse
The prevalence of opioid abuse varies significantly across different regions and healthcare settings, reflecting the complexity and scope of this subject globally [83,84]. Studies included in the review cover different regions such as the USA [35,48,52,57,59,60,62,64,66,68,69,75,77,79,80,82,84], Europe [28,49,50,55,56,57,58,63,65,67,78], Australia [54,73,74], and Canada [51,83], while countries from Asia, Africa, and South America were not included. A study reported a prevalence of opioid prescription in primary care settings from 0.6% to 0.8% [86], as well as a lower rate of abuse compared to other settings, possibly due to more controlled prescription practices and closer patient monitoring in primary care [86]. Lower abuse rates in primary care settings were inferred from general patterns of prescription and abuse [65] when compared with specialized clinics due to opioid-related AEs in emergency departments [75,76]. In contrast, in clinical settings, the prevalence of opioid abuse is reported as significantly higher, ranging from 8% to 16% [86], with patients often prescribed opioids for chronic pain management, potentially leading to higher risks of dependency and misuse [86].
The abuse of opioids goes far beyond their prescription use: the use of opioids without a prescription significantly increases the rate of abuse in the population, as the lack of adequate medical monitoring can lead to misuse and dependence [77]. Different authors highlight adverse events arising from abuse and diversion [28], including overdose deaths [48,75,87]. This abuse uses opioids in potentially harmful ways but without the intention of achieving a euphoric effect (misuse), and those who use opioids intentionally to achieve such effects (abuse) [28].
The most commonly abused opioids have changed over time and vary depending on the country [56,77,83]. Tilidine was initially the most commonly abused opioid in Germany, but over time, tramadol became more predominant [56]. Tilidine has faced concerns about its potential for abuse from early on [88] and is no longer available in the market in some EU countries [89]. In different European countries, the potential of abuse was highlighted [89,90], with Belgium withdrawing it due to issues related to its abuse [90]. In Canada, fentanyl emerged as the principal opioid of abuse, particularly when combined with benzodiazepines, leading to an increase in fentanyl-related deaths since 2012 [83]. In the United States, regulatory changes in 2014 resulted in a reduction in supratherapeutic ingestions of hydrocodone/acetaminophen and an increase in codeine/acetaminophen ingestions from 2015 onward [77]. In this review, the most frequently mentioned opioid in the list was morphine (16 mentions), followed by fentanyl (15 mentions) and oxycodone (12 mentions). Other opioids included hydrocodone, tramadol, and codeine (eight times each), buprenorphine and hydromorphone (seven times), methadone (five times), and tapentadol (two times).
The heterogeneous effects that different opioids evoke could be one of several contributing factors leading to intentional abuse [91], but it seems that drug availability has the biggest influence [92]. A survey from the United States revealed that 94% of respondents claimed they chose heroin over prescription painkillers because it was less expensive and simpler to obtain [93]. Those results are consistent with the previous research, namely that abuse behavior is influenced by availability of the substance [92].
3.2. AE Following Medication Errors
Medication errors involving opioids are a significant concern due to their high potential for causing AEs and harm to patients. They were described in 27 studies [28,35,48,49,50,51,52,53,55,58,59,62,63,64,66,67,68,69,74,75,78,80,81,82,83] and different errors were found: (a) errors during prescription, including inappropriate or ineffective prescribing practices and both underprescribing and overprescribing [51,66,80]. Those errors involve issues such as illegibility or unclear electronic entries [50,51,66]; (b) dispensing errors, with the wrong drug or formulation, as well as labeling mistakes [49,53,59,73,74]; (c) administration errors which involve incorrect dosage, route, or timing [55,67,68]; and lastly, (d) monitoring errors with insufficient treatment monitoring and failure in therapy adjustment based on patient response or side effects [67], especially in treatments needing close supervision for efficacy and safety [67]. Medication errors can be caused by both healthcare professionals and patients. Healthcare professional errors include prescribing errors due to illegible handwriting or unclear electronic inputs and administration errors such as incorrect dosage, route, or timing [50,51,55,66,67,68]. Healthcare professionals may also be responsible for monitoring errors when there is insufficient monitoring or failure to adjust therapy based on patient response [67,74]. However, patients themselves can contribute to medication errors by misunderstanding prescription instructions, taking incorrect doses, or failing to adhere to the prescribed use [49,53,58].
The incidence of these errors varies between studies: in a study focused on pediatric anesthesia, opioids were identified as the drug class most responsible for medication errors, with 10 (0.7%) cases of errors identified involving opioids [49]. Andreaggi et al. found that out of 300,985 ADRs analyzed, 3.4% were due to medication errors involving opioids [80]. Cobaugh et al. reported 543 (1.71%) cases of therapeutic errors using opioids among older adults, of which 305 were from morphine and 238 from other opioids, highlighting the hazard resulting from these medications [53]. In the general population, Ni et al. reported 30.3% (n = 51,715) of drug overdose reports as involving opioids out of the total number of drug overdose reports in the FAERS database, indicating a high incidence of medication errors [35].
Medication errors involving opioids can lead to severe adverse effects on various organ systems, primarily impacting the respiratory and gastrointestinal systems [49,52,63,65]. Common adverse events with opioids include respiratory depression, with occurrence dependent on the dosage [28,49,74] and identified for different opioids such as alfentanil [49], remifentanil [49], sufentanil [49] tramadol, and morphine [49,65]. Other AEs include gastrointestinal disorders, constipation, nausea, and vomiting, which were reported by Cobaugh et al. among older adults due to therapeutic errors [53] or by Lovegrove et al. among children under the age of six, who found that opioids were the most implicated medication class in emergency department visits involving prescription solid exposures, often leading to gastrointestinal symptoms such as nausea and vomiting [69].
Despite the fact that the opioid crisis is still more evident in the USA, opioid-related problems are perceptible in different countries: the most common substances to cause fatal medication errors in Ireland are cocaine, antidepressants, and benzodiazepines [94]; in England and Wales, anticoagulants and opioids were reported as responsible for almost half of the medication-related deaths (22%) [78].
3.3. AEs Following Abuse and Misuse
AEs following opioid intentional abuse or unintentional misuse were described in seven studies [56,57,65,77,80,81,83]. The rates of misuse and abuse depends on the opioid substance observed as well as the setting. Andreaggi et al. reported a total of 22,167 (7.4%) cases of drug abuse [80]. Harris et al. found that abuse and misuse resulting in overdose were found in 25% of cases (n = 186) in an emergency department for paracetamol/opioid-containing products [77]. Lorenzini et al. found that 64 patients visited the emergency department due to opioid-related ADRs, with 16 overdoses and 19 (29.7%) cases of abuse or misuse identified [65]. Common opioids involved included tramadol, morphine, and buprenorphine [65]. The use of opioids combined with another medication increases the risk of AE through abuse and misuse [83], e.g., the coadministration of tapentadol with other medications, including opioids, benzodiazepines, antidepressants, and antihistamines, significantly increased the risk of AE [81]. This misuse resulted in significantly higher tapentadol concentrations in postmortem cases than therapeutic levels, indicating potential abuse [81]. Chatterton et al. reviewed 2812 fentanyl-positive cases, with approximately 45% of these cases also involving benzodiazepines [83]. The median concentration of fentanyl in cases involving benzodiazepines was significantly higher than in cases without benzodiazepines, indicating that higher or more potent doses of fentanyl were being abused [83].
The abuse of hydrocodone and oxycodone are frequently highlighted due to their potent effects and widespread availability, leading to significant misuse and associated medication [56,77]. Similarly, methadone and morphine are also related to misuse and abuse [56,57]. Their dual role in therapeutic contexts and high potential for abuse make them a focal point in discussions about opioid misuse [57].
Dependence, withdrawal symptoms, and cognitive impairment are common neurological consequences of long-term opioid misuse [56]. Jobski et al. reported on the neurological effects of opioid dependence and withdrawal, highlighting the significant impact on patients’ central nervous systems [56]. Additionally, Chiappini et al. analyzed AE from major pharmacovigilance databases to detect issues related to abuse, misuse, dependence, and withdrawal of opioids, providing insights into the long-term neurological effects of misuse [57].
3.4. Medication Related Deaths
Several studies have documented the occurrence and impact of drug overdoses, focusing on opioids [35,64,65,73,79]. Looking at drug overdose events reported to the U.S. Food and Drug Administration (FDA), opioid analgesics were found to be the most frequently implicated drug class. They accounted for approximately 30.3% of all drug overdose reports from 2017 to 2021, making them the top drug class associated with overdose incidents [35,95]. Heneka et al. documented that opioid toxicity was in 39% (n = 7) of these overdose patients [74]. Lorenzini et al. provided detailed numbers of opioid overdoses in their review of emergency division (ED) visits [65]. In a total of 12,470 emergency room visits, overdose cases were identified in 16 opioid users (1.5% of opioid users; 0.1% of total ED visits), accidental (n = 8) and deliberated overdoses (n = 8) [65]. Seth et al. documented a 21.5% increase in overdose deaths from 2015 to 2016, with synthetic opioids contributing significantly to the rise [79]. In USA, ten states experienced increases of ≥100% in the number of overdoses, with Columbia (392.3%), Illinois (227.3%), and Maryland (206.9%), being the states with the greatest increases [79].
Fentanyl has been extensively documented as particularly contributing to the high number of overdose deaths occurring in non-pharmacological use [68,79]. In 2016, synthetic opioids, including fentanyl, accounted for 30.5% of all drug overdose deaths in the United States, with a 100% increase in the rate of these deaths from the previous year, primarily driven by illicitly manufactured fentanyl [79]. Lorenzini et al. and Gariel et al. have documented respiratory depression due to overdose [49,65].
Some of the remaining articles investigated whether or not the ADRs had major consequences or caused death [80,84], as well as whether or not the ADRs could have been avoided without going into detail about what those serious effects were [78].
Medication-related deaths following AEs were described by different authors [53,68,78,79,81]. Bailey et al. reported 8 deaths out of 51 cases with major serious events in a large number of young children exposed to opioids (n = 9179). The study highlighted that nearly all exposures occurred through ingestion (99%) and in the home (92%) and were unintentional, involving medications prescribed for adults in the household, primarily the child’s parents [68]. Opioids accounted for approximately 20% of all medication-related deaths reported in the USA [96].
Chatterton et al. analyzed postmortem blood concentrations of fentanyl and benzodiazepines, linking high concentration levels directly to toxicity and deaths [83].
3.5. Preventability of Adverse Events and Medication Errors
According to Culleré et al., 9.3% of all preventable AEs were triggered by use of opiates [67]. Based on three studies focused on opioid-related ADRs, 39% [58] to 64% [64] of them could have been prevented [58,64,73]. Heneka et al. concluded that many errors could be avoided with adequate training and clinical decision support systems [73].
Different studies have explored strategies and interventions aimed at reducing medication errors associated with opioids, particularly focusing on high-risk medications like fentanyl [63,72,97]. Adequate storage and child-resistant packaging measures were highlighted as significant in preventing AE and medication errors [68]. One study highlighted the importance of pictorial prescription in reducing fentanyl drug administration errors, using visual aids in prescribing practices to minimize medication errors related to opioid administration [97]. Another study explored Technology-Based Interventions that introduce smart pump systems to prevent medication administration errors, especially with opioid infusions [65]. The importance of continuous quality improvement and error reporting systems has been highlighted to identify and address medication errors involving opioids [63].
3.6. Pediatric Population
Pediatric populations were highlighted in different studies [49,50,51,52,68]. A study addressing medication errors in pediatric anesthesia revealed that opioid analgesics, such as morphine and fentanyl, are frequently implicated in incidents, and are the drug class involved in the most errors; however, they were also the type of medication that was most frequently used [49]. In pediatric care, errors commonly occur through dosing errors, including uncertainty between weight-based calculations and doses actually administered [50,52]. Incidents involving incorrect opioid dosages have led to serious adverse events, including respiratory depression and overdose, which can result in prolonged hospitalization, serious outcomes, or eventually death [49,52]. In Bailey et al.’s study, 9179 children were identified as having been exposed to prescribed opioids [68]. Of these, there were 8 deaths and 43 cases classified as major effects. Most exposures occurred accidentally at home, with nearly all resulting from ingestion of medications prescribed to adults within the household [68].
Hicks et al. indicated that pediatric opioid use must be handled with extreme caution to avoid dosing errors that can lead to overdose or inadequate pain control [52]. To improve safety, the use of standardized protocols for opioid administration, double-checking systems, and advanced training for their professionals in pediatric dosing and opioid management have been recommended [52].
3.7. Genetic Polymorphisms Associated with Adverse Events
Based on the studies analyzed, genetic polymorphisms, particularly involving the CYP2D6 enzyme, significantly influence the pharmacokinetics and pharmacodynamics of certain opioids. Lorenzini et al. (2022) highlighted that genetic variations in CYP2D6 can lead to poor metabolizers producing fewer active metabolites, reducing the analgesic effects of opioids like tramadol, codeine, and oxycodone [65]. Moulis et al. (2018) also noted the impact of CYP2D6 polymorphisms, mentioning that ultrarapid metabolizers can significantly alter drug metabolism [50]. Similarly, Day et al. (2016) discussed how codeine, a prodrug requiring conversion to morphine via CYP2D6, exhibits considerable metabolic variability due to these genetic differences, affecting its efficacy as an analgesic [48].
3.8. Quality Assessment
The risk of bias of the articles was evaluated using the JBI bias tool for systematic reviews, see Supplementary Materials Tables S6 and S7.
4. Discussion
Opioids are considered the strongest analgesics and have an important role in managing short- and medium-term pain, while their role in managing long-term pain is under discussion [28]. Their use is not without risks, as there is a growing concern about the misuse and abuse of opioid analgesics, leading to serious consequences [98].
The pharmacological characteristics of opioids, including their potential to induce euphoria, can lead to recreational use, misuse, and eventually abuse [35]. Chronic use of opioids leads to tolerance, whereby larger doses are needed to produce the same level of effect, and dependence or withdrawal symptoms, which refer to the occurrence of certain effects when the drug is not administered [65,83].
Also, chronic and severe pain patients often cannot receive sufficient pain management treatments and have to depend on opioids: inadequate availability of alternative pain treatments forces patients to depend on opioids, increasing the risk of misuse and dependence [66].
Medication-related problems, such as medication errors, misuse, and abuse involving opioids, are common across different settings, including hospitals and palliative care, as well between different population groups, such as elderly people and children. ADRs associated with opioids include serious outcomes resulting in hospitalizations and deaths, with morphine, fentanyl, oxycodone, tramadol, and hydromorphone frequently implicated [28,65,83,84].
Economic factors contribute to these opioid-related problems, since the high cost of prescribed opioids may push individuals to seek cheaper, illicit alternatives like heroin, further complicating the problem [79]. However, prescribed opioids are readily available and prescribed in large quantities, making them easily accessible for non-medical use [52]. Studies have highlighted that the excessive prescription of opioids could increase the potential for abuse [52,56]. Additionally, the recreational use of prescribed opioids for unauthorized use is a significant issue, leading to widespread community abuse and increasing the risk of dependence and overdose [68,73].
Inadequate prescription practices lead to errors such as incorrect dosages and insufficient monitoring of patients can result in medication errors [49,50,56,76], and ultimately bring patients to misuse or abuse situations. Patients often lack proper guidance on the safe use of opioids, which contributes to inappropriate use of the drugs [77,80]. Furthermore, sociocultural and psychological factors, such as self-medication for emotional or psychological pain and social influence, exacerbate the issue. Individuals may resort to using opioids not only for physical pain relief but also to manage emotional distress, while peer pressure and cultural norms around substance use can drive opioid abuse [49,57].
Dependence and withdrawal problems related to opioids are often described in cases of abuse or chronic use, with authors studies utilizing post-marketing surveillance databases highlighting dependence [28,56,57]. Data from the European Medicines Agency (EMA) EudraVigilance database provide descriptive statistics on opioid dependence and abuse, highlighting variations in reporting completeness and characteristics by different healthcare professionals and consumers [56]. The overall incidence rate of AEs in hospitalized patients was 10.3%, with 51.6% of these AEs being preventable [67]. Opioid dependence can develop quickly, particularly with potent opioids such as fentanyl or oxycodone [56,65]. This dependence is enhanced by the pharmacological characteristics of opioids [35]. Withdrawal symptoms such discomfort, pain, nausea, vomiting, and diarrhea present a challenge for individuals dependent on opioids [56,65]. This underscores the necessity for appropriate medical intervention and support to manage withdrawal and help individuals cease opioid use effectively.
Regarding opioid overdoses, most of the evidence comes from North America, especially the USA and Canada, where the opioid crisis is most pronounced, with studies focusing on both adults and children and analyzing a wide range of opioids [51,68,75,79,83,84], fentanyl being a common cause of overdose [75,84]. Studies from Germany, France, the Netherlands, and Australia also underscore significant opioid-related problems, recurrently noting dependence, abuse, and medication errors [28,49,50,54,56,73,74,81,84]. Studies use surveillance databases like the FAERS [35] and EudraVigilance [57], analyzed patterns of abuse, ADRs, and medication errors, while case reports offer detailed insights into specific opioid-related issues. Raising awareness and educating healthcare professionals, along with rigorous patient monitoring, are essential to reduce the risks associated with opioid use [73,74].
The application of different strategies, such as integrating smart pump information and data quality evaluation to detect and prevent medication administration errors, particularly in the context of opioid infusions [72], would help healthcare providers to further strengthen their medication safety practices and minimize the number of these potent opioid-related medication errors. Effective approaches include thorough education for patients and healthcare providers, stringent monitoring of opioid prescriptions, and improving access to alternative pain management options [67,74]. Implementing these strategies can help mitigate the risks associated with opioid use and improve patient outcomes [48,74].
The types of drugs most included in medication errors were also studied in the articles in this systematic review. However, the results are diverse, with results ranging from concluding that opioids are the drug type that causes the most errors [52] to presenting opioids as the 9th most error-causing drug type [55]. Deaths following the use of opioids were reported in four articles without comparisons to other drug classes [47,55,57,65]. This variation may be due to several factors, including differences in study design, populations examined, and specific healthcare settings. For example, in general medical settings where a greater variety of medications are used, opioids may not be the predominant medication type involved in errors. Understanding the diverse results and contexts presented in studies is important for developing strategies to minimize opioid-related medication errors and improve patient safety in different healthcare settings.
Different strategies could be used to prevent adverse events such as misuse, abuse, and medication errors associated with opioids. For healthcare professionals, education and training on safe opioid prescription practices [99], on the management of opioid-related ADRs, and on the use and implementation of clinical decision support systems can aid in reducing errors and improving prescription and pharmacotherapy for patients using such drugs. Education on the topic should be addressed in their medical curricula and through continuous education campaigns [99,100]. Stricter opioid prescription practices and prescription-monitoring programs have been implemented in order to lower the population exposure to these drugs [100,101]. Other strategies identified in the literature include risk assessment plans and interventions to improve the use of opioid analgesics, education on pain management to reduce opioid prescription, and the implementation of evidence-based primary prevention programs to reduce the demand for opioids [100,101]. Patients with prescribed opioids should be continuously monitored, including regular follow-ups that can help identify and mitigate potential misuse or abuse earlier or disclose an accidental error. The use of pictorial aids for better patient understanding, smart pump systems for controlled opioid administration, and double-checking protocols for dosing (e.g., in pediatrics) can significantly reduce the medication errors associated with opioids. On the other hand, there is major underreporting for medication errors due to several reasons, including fear of legal action, blaming individuals instead of the system, ineffective reporting systems, lack of feedback, and insufficient support for those who commit errors, as well as the absence of a reporting system and lack of awareness about how to report medication errors [102]. Awareness of reporting systems can help to improve the information about medication errors. Finally, raising awareness about the risks of opioid misuse and abuse through public health campaigns can help reduce stigma.
In the USA, the heavy economic burden of opioid abuse, dependency, and overdoses has led to the emergence of this issue as a major priority. Studies have highlighted the substantial costs associated with opioid-related issues, including healthcare expenses and criminal justice costs [103,104].
Regulatory agencies have a responsibility to ensure that drugs on the market have a positive risk–benefit balance. In the US, authors have voiced concerns [105,106,107] that the U.S. FDA was not strict enough in the past in enforcing marketing regulations for opioid drugs, especially since there has been an incredibly steep increase in the use of opioids in the U.S. [108,109]. In combatting issues with opioid addiction, regulatory agencies, such as the FDA, have the authority to approve new and safer formulations of immediate- and long-acting opioid medications, restrict indications, issue Dear Healthcare Professional Communications (DHPCs) and risk minimalization materials, regulate industry promotion, and suspend the marketing approval for products with a negative risk–benefit balance [110]. These are all potential regulatory actions that can be used to make opioid use safer, and the FDA has issued a timeline of the actions they have taken to address substance abuse and overdose prevention [95]. However, in order to let these regulatory actions be impactful, changes in behavior and in the clinical practice of other stakeholders, such as clinicians, patients, and marketing authorization holders, are also needed [95,111,112].
The quality of the studies was assessed using the JBI bias tools for systematic reviews, chosen due to the included articles’ study designs. Five cohort studies received lower scores (<50%), and all of these studies did not adequately identify or address confounding factors, which are essential to validating the reliability of study results. Furthermore, these studies failed to report completeness of follow-up, nor did they employ strategies to mitigate the impact of incomplete follow-up data. There were inconsistencies in how exposures were measured between groups, and it was unclear whether study participants were free of the outcome at the start of the studies. These methodological deficiencies significantly compromised the overall reliability and validity of their results, explaining the lower scores, but none of the studies were excluded due to the large number of not-applicable answers [58,59,64,66,73]. The case series did not report clinical information of the patients in detail, which might make it difficult to draw conclusions about the correlation between the opioid and ADRs. Most of the articles provided clear demographic information, including age range and sex. Ethnicity was reported in some studies, and it has been reported that this can affect drug metabolism, such as the risk of being an ultra-rapid metabolizer for codeine through the CYP2D6 enzyme, which can result in medication errors for this subgroup. However, extensive variability within subpopulations has also been reported, and relying on reported ethnicity alone without pharmacogenomics is unadvisable [113]. Socioeconomic status may influence the number of medication errors, abuse, and misuse, since some studies reported that higher socioeconomic status correlates with better health [70,114].
Strength and Limitations
The risk of bias of the included studies were generally low (see Supplementary Materials Tables S6 and S7), demonstrating the good quality of the studies included. The heterogeneity of the data is one of the limitations of this study. It makes it difficult to compare results. Additionally, the country information often refers to the database origin, but databases such as FAERS and EMA receive reports from countries other than those represented, which can lead to inconsistencies and duplicated data. Furthermore, different studies often report data from the same databases, resulting in also potential conflicts and duplication of data [115]. These factors can make complex interpretation and reliability of the findings.
The aspects that are investigated in the studies are also limited and some relevant information is not presented or investigated. Medication errors, abuse, and misuse are costly [104], but none of the articles investigated the economic burden impact of those problems. Cost-analysis studies could highlight the importance of prevention and the potential to significantly reduce the economic burden of the opioid pandemic.
Unintentional misuse was investigated in different studies [56,57,65,77,80,81,83]. However, the definition of misuse lacks clarity, being “situations where a medicinal product is intentionally and inappropriately used not in accordance with the terms of the marketing authorization” [13]. An unintentional misuse would therefore more likely be a also a medication error as long as it is an error caused by a prescribed drug. If a described misuse is an “excessive use of medicinal products which” or “is accompanied by harmful physical or psychological effects”, it should be also classified as abuse; however, the definition of abuse is restricted to intentional use, which is controversial [13]. Given the overlaps and ambiguities in the current definitions of misuse, abuse, and medication errors, further clarification is needed to ensure accurate classification and avoid data loss or overlap.
All the studies that made up this systematic review gathered their data from patients who had interacted with healthcare providers. As a result, there is a significant risk of underreporting, both from healthcare professionals [116,117] and from patients [118]. Due to the stigma associated with opioid use, there is also a risk that fewer ADRs will be reported [119]. Patients may also avoid reporting due to concerns about legal repercussions, damage to their reputation, or fear of losing access to future prescriptions [35,65]. Some articles categorized the ADRs that followed opioid use as serious or not without naming the specific ADRs [51,80]. Further to this, there was no other data only concerned with the ADRs brought on by the misuse of opioids. Differences in study designs and countries included help to illustrate the geographic variations in opioid-related problems. Larger study populations and more studies investigating the preventability of such problems would have been required to narrow the spread in this study [57].
This systematic review only focused on published papers regarding opioids in combination with medication errors and/or abuse and/or misuse. Currently, it was not possible to determine which opioid causes the greatest incidence of opioid misuse, abuse, or medication errors.
5. Conclusions
In different regions, studies show that opioids are frequently associated with abuse, misuse, and medication errors, indicating a widespread issue. Certain opioids, such as fentanyl, morphine, oxycodone, tramadol, and hydrocodone, are recurrently involved in ADRs, abuse, and medication errors. Fentanyl, in particular, is highlighted for its high risk of abuse and overdose. Many of the reported ADRs, including serious outcomes like respiratory depression, constipation, nausea, sedation, and overdose deaths, appear to be preventable. Overdose deaths are particularly prevalent with opioids like fentanyl, morphine, and oxycodone. Several studies indicate that a significant portion of opioid-related ADRs and medication errors are preventable, which underscores the importance of implementing robust preventative measures and safety protocols. Continued research is essential to better understand the safety profiles of different opioids and develop effective strategies for preventing opioid-related harm, including continuous education, stricter prescribing practices, effective monitoring, and public health campaigns to mitigate the risks of opioid misuse, abuse, and medication errors.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ph17081009/s1, Table S1: PRISMA 2020 Checklist; Table S2: Search strategy for PubMed database; Table S3: Search strategy for Scopus database; Table S4: Search strategy for EBSCO database; Table S5: Data extraction template; Table S6: Risk of bias evaluation of the cohort studies included in this study; Table S7: Risk of bias evaluation of the case studies included in this study.
Author Contributions
Conceptualization, C.M. and F.v.H.; methodology, C.M. and F.v.H.; Screening and full-text review M.G., V.S. and C.V.; writing—original draft preparation, M.G and V.S.; writing—review and editing, C.M., J.J. and F.v.H.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
No approval or consent was needed for this study.
Data Availability Statement
Requests to access the datasets should be directed to the corresponding author and will be granted upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ferner, R.E.; McGettigan, P. Adverse drug reactions. BMJ 2018, 363, k4051. [Google Scholar] [CrossRef] [PubMed]
- Callahan, D. Managed care and the goals of medicine. J. Am. Geriatr. Soc. 1998, 46, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.J.; Pontefract, S.K. Adverse drug reactions. Clin. Med. 2016, 16, 481. [Google Scholar] [CrossRef] [PubMed]
- Jay, G.W.; Heit, H.A.; Gourlay, D.L. When the best of intentions leads to bad outcomes. Pain Ther. 2019, 8, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Bouvy, J.C.; De Bruin, M.L.; Koopmanschap, M.A. Epidemiology of adverse drug reactions in Europe: A review of recent observational studies. Drug Saf. 2015, 38, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Rashed, A.N.; Wong, I.C.; Cranswick, N.; Hefele, B.; Tomlin, S.; Jackman, J.; Lee, K.; Hon, K.L.; Ong, J.; Ghaleb, M.; et al. Adverse Drug Reactions in Children—International Surveillance and Evaluation (ADVISE) A Multicentre Cohort Study. Drug Saf. 2012, 35, 481–494. [Google Scholar] [CrossRef]
- van Hunsel, F.; Ekhart, C. Unexpected beneficial effects of drugs: An analysis of cases in the Dutch spontaneous reporting system. Eur. J. Clin. Pharmacol. 2021, 77, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: Definitions, diagnosis, and management. Lancet 2000, 356, 1255–1259. [Google Scholar] [CrossRef]
- Laurence, D.R.; Carpenter, J. A Dictionary of Pharmacology and Allied Topics; Elsevier: Amsterdam, The Netherlands, 1998. [Google Scholar]
- World Health Organization. International drug monitoring: The role of national centres. In Proceedings of the Report of a WHO Meeting, Geneva, Switzerland, 20–25 September 1971; World Health Organization: Geneva, Switzerland, 1972. [Google Scholar]
- Parliament, E.; The Council of the European Union. Directive 2010/84/EU of the European Parliament and of the Council of 15 December 2010 amending, as regards pharmacovigilance, Directive 2001/83/EC on the Community code relating to medicinal products for human use. OJ 2010, 348, 74–99. [Google Scholar]
- Agency, E.M. Guideline on Good Pharmacovigilance Practices (GVP), Module VI—Management and Reporting of Adverse Reactions to Medicinal Products, 1st Revised; European Medicines Agency and Heads of Medicines Agencies: London, UK, 2014. [Google Scholar]
- Baldo, P.; Francescon, S.; Fornasier, G. Pharmacovigilance workflow in Europe and Italy and pharmacovigilance terminology. Int. J. Clin. Pharm. 2018, 40, 748–753. [Google Scholar] [CrossRef]
- Morimoto, T.; Gandhi, T.K.; Seger, A.C.; Hsieh, T.C.; Bates, D.W. Adverse drug events and medication errors: Detection and classification methods. Qual. Saf. Health Care 2004, 13, 306–314. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aronson, J.K. Medication errors: What they are, how they happen, and how to avoid them. QJM 2009, 102, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Ferner, R.E.; Aronson, J.K. Clarification of terminology in medication errors: Definitions and classification. Drug Saf. 2006, 29, 1011–1022. [Google Scholar] [CrossRef]
- Gandhi, T.K.; Seger, D.L.; Bates, D.W. Identifying drug safety issues: From research to practice. Int. J. Qual. Health Care 2000, 12, 69–76. [Google Scholar] [CrossRef]
- Ackroyd-Stolarz, S.; Hartnell, N.; Mackinnon, N.J. Demystifying medication safety: Making sense of the terminology. Res. Soc. Adm. Pharm. 2006, 2, 280–289. [Google Scholar] [CrossRef]
- Pathan, H.; Williams, J. Basic opioid pharmacology: An update. Br. J. Pain 2012, 6, 11–16. [Google Scholar] [CrossRef]
- Fields, H.L. The doctor’s dilemma: Opiate analgesics and chronic pain. Neuron 2011, 69, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Stein, C. Opioid receptors. Annu. Rev. Med. 2016, 67, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Waldhoer, M.; Bartlett, S.E.; Whistler, J.L. Opioid receptors. Annu. Rev. Biochem. 2004, 73, 953–990. [Google Scholar] [CrossRef]
- Branford, R.; Droney, J.; Ross, J. Opioid genetics: The key to personalized pain control? Clin. Genet. 2012, 82, 301–310. [Google Scholar] [CrossRef]
- Smith, M.; Kong, D.; Kuo, A.; Imam, M.; Williams, C. Analgesic opioid ligand discovery based on nonmorphinan scaffolds derived from natural sources. J. Med. Chem. 2022, 65, 1612–1661. [Google Scholar] [CrossRef] [PubMed]
- Vijayvargiya, P.; Camilleri, M.; Vijayvargiya, P.; Erwin, P.; Murad, M. Systematic review with meta-analysis: Efficacy and safety of treatments for opioid-induced constipation. Aliment. Pharmacol. Ther. 2020, 52, 37–53. [Google Scholar] [CrossRef]
- Polati, E.; Nizzero, M.; Rama, J.; Martini, A.; Gottin, L.; Donadello, K.; Del Balzo, G.; Varrassi, G.; Marinangeli, F.; Vittori, A.; et al. Oxycodone-naloxone combination hinders opioid consumption in osteoarthritic chronic low back pain: A retrospective study with two years of follow-up. Int. J. Environ. Res. Public Health 2022, 19, 13354. [Google Scholar] [CrossRef]
- Ahlbeck, K. Opioids: A two-faced janus. Curr. Med. Res. Opin. 2011, 27, 439–448. [Google Scholar] [CrossRef]
- Gustafsson, M.; Matos, C.; Joaquim, J.; Scholl, J.; van Hunsel, F. Adverse drug reactions to opioids: A study in a national pharmacovigilance database. Drug Saf. 2023, 46, 1133–1148. [Google Scholar] [CrossRef] [PubMed]
- Daoust, R.; Paquet, J.; Lavigne, G.; Piette, É.; Chauny, J. Impact of age, sex and route of administration on adverse events after opioid treatment in the emergency department: A retrospective study. Pain Res. Manag. 2015, 20, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.; Koroshetz, W. Lack of evidence for benefit from long-term use of opioid analgesics for patients with neuropathy. JAMA Neurol. 2017, 74, 761. [Google Scholar] [CrossRef]
- Macey, T.; Bobeck, E.; Hegarty, D.; Aicher, S.; Ingram, S.; Morgan, M. Extracellular signal-regulated kinase 1/2 activation counteracts morphine tolerance in the periaqueductal gray of the rat. J. Pharmacol. Exp. Ther. 2009, 331, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Bialas, P.; Maier, C.; Klose, P.; Häuser, W. Efficacy and harms of long-term opioid therapy in chronic non-cancer pain: Systematic review and meta-analysis of open-label extension trials with a study duration ≥ 26 weeks. Eur. J. Pain 2020, 24, 265–278. [Google Scholar] [CrossRef]
- Maier, C.; Schaub, C.; Willweber-Strumpf, A.; Zenz, M. Long-term efficiency of opioid medication in patients with chronic non-cancer-associated pain: Results of a survey 5 years after onset of medical treatment. Der. Schmerz. 2005, 19, 410–417. [Google Scholar] [CrossRef]
- Hoffman, E.; Watson, J.; Sauver, J.; Staff, N.; Klein, C. Association of long-term opioid therapy with functional status, adverse outcomes, and mortality among patients with polyneuropathy. JAMA Neurol. 2017, 74, 773. [Google Scholar] [CrossRef]
- Ni, J.; Tang, X.; Chen, L. Medication overdose data analysis: A review of medication error reports in the FDA adverse event reporting system (FAERS). BMC Pharmacol. Toxicol. 2023, 24, 41. [Google Scholar] [CrossRef] [PubMed]
- Hedegaard, H.; Miniño, A.M.; Warner, M. Drug Overdose Deaths in the United States, 1999–2018; NCHS Data Brief No. 356; National Center for Health Statistics: Hyattsville, MD, USA, 2020.
- Compton, W.M.; Jones, C.M. Epidemiology of the U.S. opioid crisis: The importance of the vector. Ann. N. Y. Acad. Sci. 2019, 1451, 130–143. [Google Scholar] [CrossRef]
- Cranston, K.; Alpren, C.; John, B.; Dawson, E.; Roosevelt, K.; Burrage, A.; Bryant, J.; Switzer, W.M.; Breen, C.; Peters, P.J.; et al. Notes from the field: HIV diagnoses among persons who inject drugs—Northeastern Massachusetts, 2015–2018. Morb. Mortal. Wkly. Rep. 2019, 68, 253–254. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.; Einstein, E.; Compton, W. Changes in synthetic opioid involvement in drug overdose deaths in the united states, 2010–2016. JAMA 2018, 319, 1819. [Google Scholar] [CrossRef]
- Compton, W.; Valentino, R.; DuPont, R. Polysubstance use in the U.S. opioid crisis. Mol. Psychiatry 2020, 26, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Health, T.L. Opioid overdose crisis: Time for a radical rethink. Lancet Public Health 2022, 7, e195. [Google Scholar] [CrossRef]
- Mojtabai, R.; Amin-Esmaeili, M.; Nejat, E.; Olfson, M. Misuse of prescribed opioids in the United States. Pharmacoepidemiol. Drug Saf. 2019, 28, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Kalkman, G.A.; van den Brink, W.; Pierce, M.; Atsma, F.; Vissers, K.C.P.; Schers, H.J.; van Dongen, R.T.M.; Kramers, C.; Schellekens, A.F.A. Monitoring opioids in Europe: The need for shared definitions and measuring drivers of opioid use and related harms. Eur. Addict. Res. 2022, 28, 231–240. [Google Scholar] [CrossRef]
- Shei, A.; Hirst, M.; Kirson, N.; Enloe, C.; Birnbaum, H.; Dunlop, W. Estimating the health care burden of prescription opioid abuse in five European countries. Clin. Outcomes Res. 2015, 7, 477–488. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Kellermeyer, L.; Harnke, B.; Knight, S. Covidence and rayyan. J. Med. Libr. Assoc. 2018, 106, 580. [Google Scholar] [CrossRef]
- Marraffa, J.M.; Stork, C.M.; Hoffman, R.S.; Su, M.K. Poison control center experience with tianeptine: An unregulated pharmaceutical product with potential for abuse. Clin. Toxicol. 2018, 56, 1155–1158. [Google Scholar] [CrossRef] [PubMed]
- Day, L.; Kleinschmidt, K.; Forrester, M.B.; Feng, S.-Y. Comparison of unintentional exposures to codeine and hydrocodone reported to Texas poison centers. J. Emerg. Med. 2016, 50, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Gariel, C.; Cogniat, B.; Desgranges, F.P.; Chassard, D.; Bouvet, L. Incidence, characteristics, and predictive factors for medication errors in paediatric anaesthesia: A prospective incident monitoring study. Br. J. Anaesth. 2018, 120, 563–570. [Google Scholar] [CrossRef]
- Moulis, F.; Durrieu, G.; Masmoudi, K.; Boyer, M.G.; Rocher, F.; Montastruc, F.; Montastruc, J.-L. Medication errors with tramadol drops in children. Eur. J. Clin. Pharmacol. 2018, 74, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Mc Donnell, C. Opioid medication errors in pediatric practice: Four years’ experience of voluntary safety reporting. Pain Res. Manag. 2011, 16, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Hicks, R.W.; Becker, S.C.; Cousins, D.D. Harmful medication errors in children: A 5-year analysis of data from the USP’s MEDMARX®program. J. Pediatr. Nurs. 2006, 21, 290–298. [Google Scholar] [CrossRef]
- Cobaugh, D.J.; Krenzelok, E.P. Adverse drug reactions and therapeutic errors in older adults: A hazard factor analysis of poison center data. Am. J. Health Pharm. 2006, 63, 2228–2234. [Google Scholar] [CrossRef]
- Mullan, J.; Burns, P.; Mohanan, L.; Lago, L.; Jordan, M.; Potter, J. Hospitalisation for medication misadventures among older adults with and without dementia: A 5-year retrospective study. Australas. J. Ageing 2019, 38, e135–e141. [Google Scholar]
- Cassidy, N.; Duggan, E.; Williams, D.J.P.; Tracey, J.A. The epidemiology and type of medication errors reported to the National Poisons Information Centre of Ireland. Clin. Toxicol. 2011, 49, 485–491. [Google Scholar] [CrossRef]
- Jobski, K.; Bantel, C.; Hoffmann, F. Characteristics and completeness of spontaneous reports by reporter’s role in Germany: An analysis of the EudraVigilance database using the example of opioid-associated abuse, dependence, or withdrawal. Pharmacol. Res. Perspect. 2023, 11, e01077. [Google Scholar] [CrossRef]
- Chiappini, S.; Vickers-Smith, R.; Guirguis, A.; Corkery, J.M.; Martinotti, G.; Harris, D.R.; Schifano, F. Pharmacovigilance signals of the opioid epidemic over 10 years: Data mining methods in the analysis of pharmacovigilance datasets collecting adverse drug reactions (ADRs) Reported to EudraVigilance (EV) and the FDA Adverse Event Reporting System (FAERS). Pharmaceuticals 2022, 15, 675. [Google Scholar] [CrossRef]
- Schutijser, B.C.F.M.; Jongerden, I.; Klopotowska, J.E.; Moesker, M.; Langelaan, M.; Wagner, C.; de Bruijne, M. Nature of adverse events with opioids in hospitalised patients: A post-hoc analysis of three patient record review studies. BMJ Open 2020, 10, e038037. [Google Scholar] [CrossRef]
- Eluri, M.; A Spiller, H.; Casavant, M.J.; Chounthirath, T.; A Conner, K.; A Smith, G. Analgesic-related medication errors reported to US poison control centers. Pain Med. 2018, 19, 2357–2370. [Google Scholar] [CrossRef]
- Min, J.; Osborne, V.; Kowalski, A.; Prosperi, M. Reported adverse events with painkillers: Data mining of the US Food and Drug Administration adverse events reporting system. Drug Saf. 2018, 41, 313–320. [Google Scholar] [CrossRef]
- Madeiro, A.C.; Dayana, P.; Carrilho, L.; Bonfim, M.; Braqueais, A.R.; Elisângela, F.; Lima, T. Adesão de portadores de insuficiência renal crônica ao tratamento de hemodiálise. Acta Paul. Enferm. 2010, 23, 546–551. [Google Scholar] [CrossRef][Green Version]
- Brophy, T.J.; Spiller, H.A.; Casavant, M.J.; Chounthirath, T.; Smith, M.D.; Xiang, H. Medication errors reported to US poison control centers, 2000–2012. Clin. Toxicol. 2014, 52, 880–888. [Google Scholar] [CrossRef]
- Lövborg, H.; Holmlund, M.; Hägg, S. Medication errors related to transdermal opioid patches: Lessons from a regional incident reporting system. BMC Pharmacol. Toxicol. 2014, 15, 1–6. [Google Scholar] [CrossRef]
- Whipple, J.K.; Ausman, R.K.; Quebbeman, E.J. Narcotic Use in the Hospital: Reasonably Safe? SAGE Publications: Los Angeles, CA, USA, 1992. [Google Scholar]
- Ing Lorenzini, K.; Wainstein, L.; Spechbach, H.; Sarasin, F.; Ramlawi, M.; Desmeules, J.; Piguet, V. Opioid-related adverse drug reactions in patients visiting the emergency division of a tertiary hospital. Pharmacol. Res. Perspect. 2022, 10, e01033. [Google Scholar] [CrossRef]
- Boockvar, K.S.; Liu, S.; Goldstein, N.; Nebeker, J.; Siu, A.; Fried, T. Prescribing discrepancies likely to cause adverse drug events after patient transfer. BMJ Qual. Saf. 2009, 18, 32–36. [Google Scholar] [CrossRef]
- Culleré, C.B.; Torner, M.G.; Ruiz, J.A.; Creus, M.T.; Martín, M.B.; Sunyer, M.C.; Gubert, M.T.; Cortinas, M.C.; Sabaté, E.B.; Solà, J.F.; et al. Detecting adverse drug events during the hospital stay. Farm. Hosp. 2009, 33, 312–323. [Google Scholar] [CrossRef]
- Bailey, J.E.; Campagna, E.; Dart, R.C. The underrecognized toll of prescription opioid abuse on young children. Ann. Emerg. Med. 2009, 53, 419–424. [Google Scholar] [CrossRef]
- Lovegrove, M.C.; Weidle, N.J.; Budnitz, D.S. Trends in emergency department visits for unsupervised pediatric medication exposures, 2004–2013. Pediatrics 2015, 136, e821–e829. [Google Scholar] [CrossRef]
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic status and access to healthcare: Interrelated drivers for healthy aging. Front. Public Health 2020, 8, 512143. [Google Scholar] [CrossRef]
- Jones, T.A.; Como, J.A. Assessment of medication errors that involved drug allergies at a university hospital. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2003, 23, 855–860. [Google Scholar] [CrossRef]
- Ni, Y.; Lingren, T.; Huth, H.; Timmons, K.; Melton, K.; Kirkendall, E.S. Integrating and evaluating the data quality and utility of smart pump information in detecting medication administration errors: Evaluation study. JMIR Med. Inform. 2020, 8, e19774. [Google Scholar] [CrossRef]
- Heneka, N.; Shaw, T.; Rowett, D.; Lapkin, S.; Phillips, J.L. Opioid errors in inpatient palliative care services: A retrospective review. BMJ Support. Palliat. Care 2018, 8, 175–179. [Google Scholar] [CrossRef]
- Heneka, N.; Shaw, T.; Rowett, D.; Lapkin, S.; Phillips, J.L. Exploring factors contributing to medication errors with opioids in Australian specialist palliative care inpatient services: A multi-incident analysis. J. Palliat. Med. 2018, 21, 82. [Google Scholar] [CrossRef]
- Beaudoin, F.L.; Merchant, R.C.; Janicki, A.; McKaig, D.M.; Babu, K.M. Preventing iatrogenic overdose: A review of in–emergency department opioid-related adverse drug events and medication errors. Ann. Emerg. Med. 2015, 65, 423–431. [Google Scholar] [CrossRef]
- McDonald, H.P.; Garg, A.H.R. Interventions to enhance patient adherence to medication prescriptions: Scientific review. J. Am. Med. Assoc. 2002, 2002, 288. [Google Scholar] [CrossRef]
- Harris, E.; Harms, M.; Cao, D.; Prestwood, C.; DeBinya, L.; Kleinschmidt, K.; Young, A.; Saha, S.; Rule, J.; Alvarez, K.; et al. Declining rates of opioid/acetaminophen combination product overdose: 2011–2020. Hepatol. Commun. 2023, 7, e0067. [Google Scholar] [CrossRef] [PubMed]
- France, H.S.; Aronson, J.K.; Heneghan, C.; Ferner, R.E.; Cox, A.R.; Richards, G.C. Preventable deaths involving medicines: A systematic case series of coroners’ reports 2013–2022. Drug Saf. 2023, 46, 335–342. [Google Scholar] [CrossRef]
- Seth, P. Overdose deaths involving opioids, cocaine, and psychostimulants—United States, 2015–2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 349–358. [Google Scholar] [CrossRef]
- Andreaggi, C.A.; Novak, E.A.; Mirabile, M.E.; Sampathkumar, S.; Gray, M.P.; He, M.; Kane-Gill, S.L. Safety concerns reported by consumers, manufacturers and healthcare professionals: A detailed evaluation of opioid-related adverse drug reactions in the FDA database over 15 years. Pharmacoepidemiol. Drug Saf. 2020, 29, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, L.; van den Heuvel, C.; Humphries, M.; Scott, T.; Byard, R.W. Increased incidence of mixed drug toxicity deaths involving tapentadol–A forensic study. Med. Sci. Law 2024, 64, 113–120. [Google Scholar] [CrossRef]
- Tardelli, V.; Xu, K.Y.; Bisaga, A.; Levin, F.R.; Fidalgo, T.M.; Grucza, R.A. Prescription amphetamines in people with opioid use disorder and co-occurring psychostimulant use disorder initiating buprenorphine: An analysis of treatment retention and overdose risk. BMJ Ment. Health 2023, 26, e300728. [Google Scholar] [CrossRef]
- Chatterton, C.N.; Handy, R.P. Fentanyl concentrations in ligated femoral blood in the presence and absence of NPS benzodiazepine drugs. A review of over 1250 benzo-dope/fentanyl toxicity cases in Alberta Canada. Forensic Sci. Int. 2023, 350, 111777. [Google Scholar] [CrossRef]
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. Assessing the 2004–2018 fentanyl misusing issues reported to an international range of adverse reporting systems. Front. Pharmacol. 2019, 10, 428774. [Google Scholar] [CrossRef]
- Dunbar-Jacob, J.; Mortimer-Stephens, M.K. Treatment adherence in chronic disease. J. Clin. Epidemiol. 2001, 54, S57–S60. [Google Scholar] [CrossRef]
- Chou, R.; Turner, J.A.; Devine, E.B.; Hansen, R.N.; Sullivan, S.D.; Blazina, I.; Dana, T.; Bougatsos, C.; Deyo, R.A. The effectiveness and risks of long-term opioid therapy for chronic pain: A systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 2015, 162, 276–286. [Google Scholar] [CrossRef]
- Kyung, E.J.; Ryu, J.H.; Kim, E.Y. Evaluation of adverse reactions to contrast media in the hospital. Br. J. Radiol. 2013, 86, 20130418. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-84888617835&doi=10.1259%2Fbjr.20130418&partnerID=40&md5=b8fd8bf7066e4b204d926ee33ba84372NS (accessed on 20 June 2024). [CrossRef]
- Trojan, A.; Beil, H.W. Tilidine abuse and dependence. Drug Alcohol. Depend. 1978, 3, 383–391. [Google Scholar] [CrossRef]
- Radbruch, L.; Glaeske, G.; Grond, S.; Münchberg, F.; Scherbaum, N.; Storz, E.; Tholen, K.; Zagermann-Muncke, P.; Zieglgänsberger, W.; Hoffmann-Menzel, H.; et al. Topical review on the abuse and misuse potential of tramadol and tilidine in Germany. Subst. Abus. 2013, 34, 313–320. [Google Scholar] [CrossRef]
- Vlaams Expertisecentrum Alcohol en Andere Drugs. Dossier Opioïde Pijnstillers. 2018. Available online: https://www.vad.be/catalogus/detail/dossier-opioide-pijnstillers (accessed on 20 June 2024).
- Drewes, A.M.; Jensen, R.D.; Nielsen, L.M.; Droney, J.; Christrup, L.L.; Arendt-Nielsen, L.; Riley, J.; Dahan, A. Differences between opioids: Pharmacological, experimental, clinical and economical perspectives. Br. J. Clin. Pharmacol. 2013, 75, 60–78. [Google Scholar] [CrossRef]
- Wightman, R.; Perrone, J.; Portelli, I.; Nelson, L. Likeability and abuse liability of commonly prescribed opioids. J. Med. Toxicol. 2012, 8, 335–340. [Google Scholar] [CrossRef]
- Cicero, T.J.; Ellis, M.S.; Surratt, H.L.; Kurtz, S.P. The changing face of heroin use in the United States: A retrospective analysis of the past 50 years. JAMA Psychiatry 2014, 71, 821–826. [Google Scholar] [CrossRef]
- Lynn, E.; Cousins, G.; Lyons, S.; Bennett, K.E. Trends in drug poisoning deaths, by sex, in Ireland: A repeated cross-sectional study from 2004 to 2017. BMJ Open 2021, 11, e048000. [Google Scholar] [CrossRef]
- Food and Drug Administration. Timeline of Selected FDA Activities and Significant Events Addressing Substance Use and Overdose Prevention. 2024. Available online: https://www.fda.gov/drugs/food-and-drug-administration-overdose-prevention-framework/timeline-selected-fda-activities-and-significant-events-addressing-substance-use-and-overdose (accessed on 25 July 2024).
- Ferner, R.E.; Easton, C.; Cox, A.R. Deaths from medicines: A systematic analysis of coroners’ reports to prevent future deaths. Drug Saf. 2018, 41, 103–110. [Google Scholar] [CrossRef]
- Booth, S.; Gloag, M.; Kinna, S.; Bell, A.; Wheble, J.; Wheeler, D. Pictorial prescribing reduces fentanyl drug administration errors: A simulated controlled study. BMJ Support. Palliat. Care 2015, 7, 173–178. [Google Scholar] [CrossRef]
- Vadivelu, N.; Schermer, E.; Kodumudi, G.; Berger, J. The clinical applications of extended-release abuse-deterrent opioids. CNS Drugs 2016, 30, 637–646. [Google Scholar] [CrossRef]
- Ratycz, M.C.; Papadimos, T.J.; Vanderbilt, A.A. Addressing the growing opioid and heroin abuse epidemic: A call for medical school curricula. Med. Educ. Online 2018, 23, 1466574. [Google Scholar] [CrossRef] [PubMed]
- Ostling, P.S.; Davidson, K.S.; Anyama, B.O.; Helander, E.M.; Wyche, M.Q.; Kaye, A.D. America’s opioid epidemic: A comprehensive review and look into the rising crisis. Curr. Pain Headache Rep. 2018, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Sanapati, J.; Benyamin, R.M.; Atluri, S.; Kaye, A.D.; Hirsch, J.A. Reframing the prevention strategies of the opioid crisis: Focusing on prescription opioids, fentanyl, and heroin epidemic. Pain Physician 2018, 21, 309. [Google Scholar] [CrossRef] [PubMed]
- Sabblah, G.T.; Seaneke, S.K.; Kushitor, M.; van Hunsel, F.; Taxis, K.; Duwiejua, M.; van Puijenbroek, E. Evaluation of pharmacovigilance systems for reporting medication errors in Africa and the role of patients using a mixed-methods approach. PLoS ONE 2022, 17, e0264699. [Google Scholar] [CrossRef]
- Reinhart, M.; Scarpati, L.; Kirson, N.; Patton, C.; Shak, N.; Erensen, J. The economic burden of abuse of prescription opioids: A systematic literature review from 2012 to 2017. Appl. Health Econ. Health Policy 2018, 16, 609–632. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.S.; Zhou, C.; Luo, F.; Xu, L. The economic burden of prescription opioid overdose, abuse, and dependence in the United States, 2013. Med. Care 2016, 54, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Kolodny, A. How FDA failures contributed to the opioid crisis. AMA J. Ethics 2020, 22, 743–750. [Google Scholar]
- Yakubi, H.; Gac, B.; Apollonio, D.E. Industry strategies to market opioids to children and women in the USA: A content analysis of internal industry documents from 1999 to 2017 released in State of Oklahoma v. Purdue Pharma, LP et al. BMJ Open 2022, 12, e052636. [Google Scholar] [CrossRef]
- Feldscher, K. What Led to the Opioid Crisis—And How to Fix It. Harvard Sch. Public Health. 2022. Available online: https://www.hsph.harvard.edu/news/features/what-led-to-the-opioid-crisis-and-how-to-fix-it/ (accessed on 20 June 2024).
- Jantarada, C.; Silva, C.; Guimarães-Pereira, L. Prevalence of Problematic Use of Opioids in Patients with Chronic Noncancer Pain: A Systematic Review with Meta-analysis. Pain Pract. 2021, 21, 715–729. [Google Scholar] [CrossRef]
- Vowles, K.E.; McEntee, M.L.; Julnes, P.S.; Frohe, T.; Ney, J.P.; Van Der Goes, D.N. Rates of opioid misuse, abuse, and addiction in chronic pain: A systematic review and data synthesis. Pain 2015, 156, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.K.; Ford, M.A.; Bonnie, R.J. National Academies of Sciences Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Committee on Pain Management and Regulatory Strategies to Address Prescription Opioid Abuse. Pain Management and the Opioid Epidemic: Balancing Societal and Individual Benefits and Risks of Prescription Opioid Use; National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Matos, C.; Rodrigues, L.; Joaquim, J. Attitudes and opinions of Portuguese community pharmacy professionals towards patient reporting of adverse drug reactions and the pharmacovigilance system. Drugs Ther. Perspect. 2017, 33, 188–194. [Google Scholar] [CrossRef]
- van Hoof, M.; Chinchilla, K.; Härmark, L.; Matos, C.; Inácio, P.; van Hunsel, F. Factors Contributing to Best Practices for Patient Involvement in Pharmacovigilance in Europe: A Stakeholder Analysis. Drug Saf. 2022, 45, 1083–1098. [Google Scholar] [CrossRef] [PubMed]
- Virbalas, J.; Morrow, B.E.; Reynolds, D.; Bent, J.P.; Ow, T.J. The prevalence of Ultrarapid metabolizers of Codeine in a diverse urban population. Otolaryngol. Neck Surg. 2019, 160, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Adler, N.E.; Boyce, T.; Chesney, M.A.; Cohen, S.; Folkman, S.; Kahn, R.L.; Syme, S.L. Socioeconomic status and health: The challenge of the gradient. Am. Psychol. 1994, 49, 15. [Google Scholar] [CrossRef] [PubMed]
- van Stekelenborg, J.; Kara, V.; Haack, R.; Vogel, U.; Garg, A.; Krupp, M.; Gofman, K.; Dreyfus, B.; Hauben, M.; Bate, A. Individual case safety report replication: An analysis of case reporting transmission networks. Drug Saf. 2023, 46, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Gonzalez, E.; Herdeiro, M.T.; Figueiras, A. Determinants of under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2009, 32, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Varallo, F.R.; Guimarães, S.D.O.P.; Abjaude, S.A.R.; Mastroianni, P.D.C. Causes for the underreporting of adverse drug events by health professionals: A systematic review. Rev. Esc. Enferm. USP 2014, 48, 739–747. [Google Scholar] [CrossRef]
- Härmark, L.; Van Hunsel, F.; Grundmark, B. ADR reporting by the general public: Lessons learnt from the Dutch and Swedish systems. Drug Saf. 2015, 38, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.D.; Ali, S.; Burnich-Line, D.; Gonzales, W.; Stanton, M.V. Stigma Opioids, and Public Health Messaging: The Need to Disentangle Behavior From Identity. Am. J. Public Health 2020, 110, 807–810. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).