1. Introduction
Options in osteoarthritis (OA) treatment have been expanded using the ability of tissue self-renewal properties. The results of platelet rich plasma, growth factors and autologous chondrocyte implantation have been well documented [
1,
2,
3]. Despite of this, new strategies using mesenchymal stem cells (MSCs) have been actively explored in the last decade. The ability of the MSCs to differentiate into chondrocytes and synoviocytes could be utilized in the cartilage repair and the OA treatment [
4,
5]. This biological solution could offer a potential treatment option for the younger patient group and all other patients affected by the OA, where joint replacement would not be considered as the best treatment option. For cartilage repair, the MSCs are mainly acquired from the bone marrow (BM). However, other sources such as the adipose tissue (ASC), the synovial membrane and the umbilical cord have been described. All of these MSCs are expressing the same markers as embryonic stem cells and show also similar pluripotent properties [
6,
7].
In clinical practice both the ASC and the BMSCs have been used for cell based cartilage restoration. However, both of them have their own advantages. Certain studies show the advantage of the BMSC is in ability to produce the collagen type II and sulphated glycosaminoglycans [
8,
9].
In regenerative medicine, the BMSCs used can be divided into the following subgroups: the bone marrow aspirate concentrate, mononuclear cells, the isolated MSCs without in vitro expansion and the cultured MSCs. The bone marrow sample can be separated into plasma, red blood cells, platelets, and mononuclear cells by applying density gradient centrifugation. A mononuclear cell fraction contains a variety of progenitors including the MSCs population. Most of these mononuclear cells are CD34+ hematopoietic lineage progenitors, while very few are actually the MSCs capable to differentiate into bone, cartilage and synovial tissue [
10]. Estimated frequency of the MSC in the BM nucleated cell population differs in range from 0.0017 to 0.034% [
11]. Easy access to the mononuclear cells makes them advantageous in orthopedic practice. In literature we found a variety of clinical studies and case reports about the use of the BMSC in the treatment of isolated cartilage lesions and the OA patients [
12,
13]. These clinical studies describe the use of the MSC from both autologous and allogenic cell sources such as the bone marrow, the adipose tissue and the peripheral blood. Different MSC concentration methods and cell expansion ex vivo, additional augmentation with growth factors, hyaluronic acid and cell introducing methods have been used. A uniform BMSC based therapy analysis of clinical benefits on larger patient groups in orthopedic practice is still missing.
The primary aim of this study was to find out clinical effectiveness, analyze pain and changes in the OA symptoms, after a single intra-articular injection of the BM-MNC on KL stage II–III affected joints over a period of 12 months and to compare it to the clinical effectiveness of the patient group treated with sodium hyaluronate injections. The secondary aim was to observe any presence of adverse events associated with applied therapy.
2. Materials and methods
2.1. The patient randomization and the study design
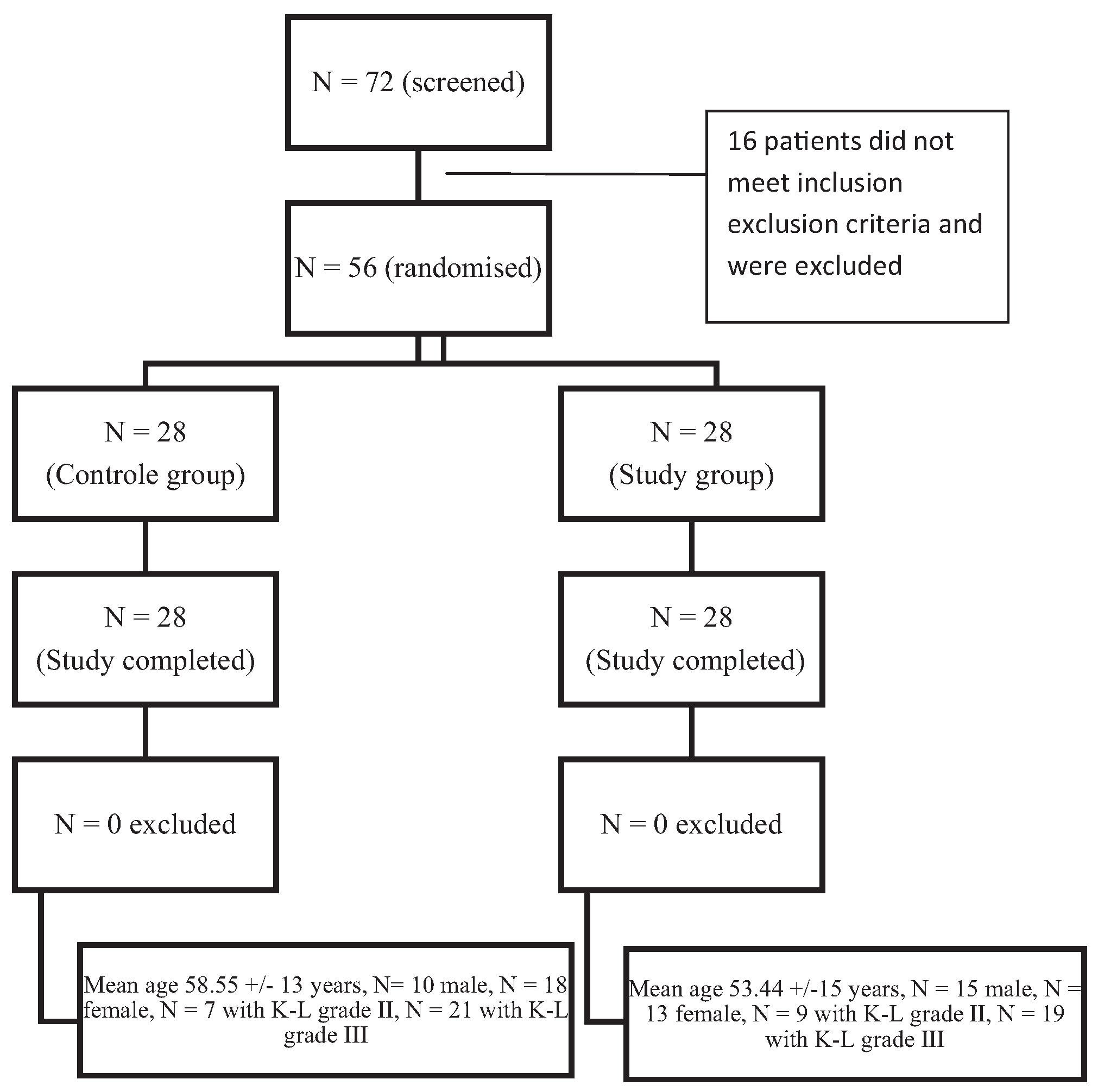
The level of evidence: level II, randomized controlled trail (RCT). Between 2012 and 2015, 72 patients with the KL stage II–III OA in knee were screened, 56 were included in the study according inclusion exclusion criteria outlined in
Table 1.
The patients were randomly divided into two groups: the bone marrow-derived mononuclear cells (BM-MNC) group and the sodium hyaluronate (HA) as a control group. The patient randomization process is represented in
Fig. 1.
The State Central Medical Ethics Committee approved this clinical study. All patients provided an informed consent for the study according to the Helsinki Declaration and all patients voluntarily agreed to participate and signed the informed consent forms. The enrolled patients were randomized into study and control groups 1:1. The mean age in the study group was 53.44 ± 15 years, and there were 15 males (53%) and 13 females (47%). The control group included 10 males (34%) and 21 females (66%) with mean age 58.55 ± 13 years. The OA progression stage according Kellgren–Lawrence classification was 7 (25%) OA stage II and 21 (75%) OA stage III in the control group. The study group contained 9 (32%) OA stage II and 19 (68%) OA stage III patients. Patients in the therapy group underwent a single intra-articular injection of BM-MNC. Patients in the control group received total three Na hyaluronate (HA) intra-articular injections with an interval of one week, starting at the week 1 and finishing at the week 3.
The GO-ON 25 mg/2.5 mL pre-filled syringe containing Na hyaluronate 1% gel, average molecular weight 800–1500 kDa was used.
2.2. The bone marrow harvesting and cell preparation
Cells used in this study were extracted from the patient’s own red bone marrow. The Iliac crest puncture was performed under local anesthesia. A total up to 45 ml of bone marrow was aspirated into heparin-treated syringes. The bone marrow aspirate was shipped at room temperature to the central cell-processing laboratory and diluted with sterile 0.9% NaCl (1:5), filtrated through 70 µm cell strainer (BD Biosciences), and bone marrow mononuclear cells (BM-MNCs) were isolated and enriched by density gradient with the use of Ficoll–Paque Premium (GE Healthcare Ltd.) according to the manufacturer’s instruction, with minor protocol modifications. The MNCs were washed 3 times with 45 ml 0.9% NaCl containing 10 U/mL heparin and re-suspended in saline with 10,000 U/L heparin. The cell count in all samples was made using the flow cytometry analysis. During gradient centrifugation, plasma factors, red blood cells and platelets where removed. The final cell suspension used for injection contains only the mononu-clear cell fraction resuspended in 0.9% NaCl solution in 5-mL syringes. No other additional biological substances were added. Each patient received all of his own cell material extracted from the 45 ml of red bone marrow aspirate.
2.3. The flow cytometry
Samples from the BM and the final product (BM-MNCs) were counted and used for the flow cytometric analysis (FACS) within 2 h after preparation. The cell viability was obtained using the 7AAD method that is included in the ISHAGE protocol. The stem kit from the Beckman Coulter was used for cell labeling with CD45-FITC, CD34-PE, 7-AAD and Stem-Count fluorospheres. Cells were analyzed using the FC-500 (Beckman Coulter). The analysis protocol was developed manually. The Stem CXP program was used for MNC, CD34+ cell count and cell viability detection. Gating was performed according to the ISHAGE protocol according to the manufacturer’s suggestion. Each measurement contained at least 50,000 events. The maximum number of events was 100,000. The obtained numbers of cells/mL were calculated for total number of the MNC and the CD34+ cells within transplantation material. The measurements with less than 50,000 events were excluded from the study.
2.4. The intra-articular injection procedure and the follow-up period
The knee joint puncture without using local anesthesia was performed. To reassure the correct needle placement in the joint cavity, 5–10 mL saline was injected. In case of free drainage of the saline by the aspiration, the correct placement in the knee join cavity was considered. The injection of mononuclear cell suspension into the knee joint was performed without changing the needle position. After 1 h of bed rest the patients were released home. Regarding the physical activity at the enrolment, the patients were given recommendations to avoid excessive physical activity and sport exercises exceeding their normal everyday activities and habits. On the visits at the time points 1, 3, 6 and 12 months it was controlled. The short-term use of pain reliever drugs during the evaluation period of 12 months was accepted. The use of the glucosamine, the chondroitin sulfate, the avocado and the soybean oil OTC drugs was not specially recommended or restricted. The patients maintained previous habit of the SYSODOA drug use.
2.5. The clinical assessment
The pain and changes in the OA symptoms were assessed by using the following questionnaires.
2.5.1. Knee Society Score (KSS)
This scoring system is the version of the knee score as modified by Dr. John Insall in 1993. The scoring system combines a relatively objective knee score that is based on the clinical parameters and the Functional Score based on how the patient perceives the knee functions during specific activities. The maximum Knee Score is 100 points and the maximum Functional Score is 100 points [
14].
2.5.2. Knee Osteoarthritis Outcome Score (KOOS)
The KOOS system consists of 5 subscales: pain, other symptoms, activities of daily living (ADL), sport and recreation function (Sport/Rec), and knee-related quality of life (QOL). A KOOS score of 100 indicates no symptoms and 0 indicates extreme symptoms [
15].
The patient scoring was done on the day of procedure and follow up periods, 1, 3, 6 and 12 months after the BMSCs injection.
2.5.3. Radiological assessment
For radiological assessment digital calibrated X-rays were used before the cell injection procedure and 12 months after.
2.6. Statistical analysis
All data were analyzed using the BM SPSS 22.0. Firstly, data were analyzed for normality using skewness and kurtosis as well as a histogram and a Q–Q plot. If the data were normally distributed, then a paired or independent Student t test was performed. Analyzed in this manner with paired t test were the KSS, OKS, and KOOS subscales between the baseline and follow-up points within each group. A P value of <0.05 was considered as statistically significant. Levene’s test was used to evaluate homogeneity between the two study groups. An independent Student t test was used for comparing the BMSC and the HA groups. If data were not normally distributed, then the Mann–Whitney U test was used.
3. Results
No adverse effects after the BM-MNC injection were observed. The patients reported the procedure of iliac crest puncture as painless and no complications in the donor sites were observed. The knee joint pain or swelling caused by puncture reduced during an hour and no additional treatment was needed. The OA pain decreased in all patients except one patient case. A positive response to the BM-MNC injection was observed in 96% of cases. Pain relive occurred at the first weeks after the BM-MNC injection. In the majority of cases the reduction of pain and other OA signs lasted for more than 12 months. The results vary significantly from patient to patient, starting from complete absence of symptoms to a mild decline of pain and symptoms. In
Fig. 2 the average improvement in all KOOS score subscales during the follow-up period can be seen.
The KSS score results improved during the entire follow-up period (
Fig. 3).
Table 2 demonstrates that at the endpoint at month 12 the KOOS score improved significantly (
P < 0.05) on the pain subscale (+25.44), activity and daily living subscale (+21.36), quality of life subscale (+28.83), and total KOOS (+18.25). However, the KOOS symptoms and sport subscales showed improvement but it was not statistically significant.
The KSS score also demonstrated a significant improvement on the knee score subscale (+25.42) and function subscale (+38.32) (
Table 3).
Results of both the KSS and the KOOS were compared between the BM-MNC and the HA group. The BM-MNC group showed statistically significant (
P < 0.05) superiority in the pain subscale over the HA group at the time points 6 and 12 months after injection (
Fig. 4). In all other score subscales the results were superior in the BM MNC group but the difference was not statistically significant.
To find out how the patient related factors influenced differences in the clinical results of the therapy group patients, the correlations between cell dose, age and OA stages were explored. Before the injection of the flow cytometry (FACS) results were obtained from each extracted mononuclear cell sample.
Fig. 5 shows individual patient cell yields. The average final yield of the mononuclear cell extraction was 38.64 ± 33.7 × 10
6 cells. The cell counts differ significantly (8.3 × 10
6 to 158.79 × 10
6) between processed bone marrow samples. Considering the large difference between the highest and the lowest injected mononuclear cell quantity, the association between the cell count and the clinical effects was analyzed (
Fig. 6). The patients from the therapy group were divided into two groups based on the injected mononuclear cell count: below the mean and above the mean cell count. The group with higher than mean BMSC count had a better improvement than lower than mean BM-MNC group, however statistically significant (
P < 0.05) changes were observed on 12 months follow up time point only.
Improvement between the Kellgren–Lawrence II and the III OA grade groups was compared. Statistically significant differences in the clinical improvement were not found. When comparing the clinical improvement levels between the K–L II and the III OA grade groups, statistically significant differences in both groups were not found. Correlation between age and clinical effects was not evident either.
At the enrolment of patients, X-rays were used for the grading according to the Kellgren–Lawrence classification of both groups. The radiologic assessment of the calibrated X-rays was performed by several radiologists from the department not involved in the study. The X-ray was performed to detect possible side effects in the BM-MNC patient group at 12-month follow up. The X-rays showed no signs of further developing of OA and no radiological changes in bone structure or any periosteal reaction were found either. Because of the limited sensitivity of the X-ray, it was not used to compare the patient groups, therefore the HA group patients were not radiologically evaluated after 12 months.
4. Discussion
Our results clearly demonstrate pain relief in the majority of cases. The stiffness and other OA symptoms had not changed significantly, however the clinical improvement differed among enrolled patients. The results from other clinical studies using the BMAC or the MSCs in knee joint OA treatment have been reported in various publications [
16,
17,
18]. Only some of them were designed as a randomized controlled trial. Different patient material, cell types and cell delivery methods have been analyzed. One of the largest cohort studies by Nejadnik et al. in 2010 compared clinical results of two patient groups treated with autologous BM-MSCs (
n = 36) vs. chondrocytes (
n = 36). An important clinical improvement in both groups was observed [
19]. The results from the RCT by Saw et al. in 2012 demonstrated a score improvement using peripheral blood MSC and superiority against the HA as the control group [
20]. Certain studies have demonstrated both knee pain and functions improvement using the bone marrow aspirate concentrate (BMAC) injection pure and augmented with PRP and adipose tissue in the knee OA treatment [
16,
17,
21]. The improvement range reported was close to our study findings. However, the most adverse effects after bone marrow aspirate concentrate augmented with fat tissue have been reported. The bone marrow aspirate used in our study, was processed in order to isolate mononuclear cells by gradient centrifugation method to reduce red blood cell and erythrocyte lysate contamination. We assume that purification of cell solution is the reason why the adverse effects like swelling and pain after cell injection were not observed.
Cell yields and correlation to clinical effects are an active topic for discussion in all fields using the BMSCs as a therapeutic agent. However, there is no clear answer so far, especially in the field of orthopedics, due to the lack of data. We observed a wide spread of cell yields, that can vary depending on patients’ individual condition, bone marrow acquisition and cell processing quality. In a previous study of the BM-MNC processing efficacy a similar variety of mononu-clear cell quantity was found, but despite to this, the study showed clear correlation between patient age and cell yields. Slightly higher cell yields were obtained in younger patient groups [
22]. In literature there are data that support our findings of no correlation between the patient age and the cell yield. For example, some studies reported that sufficient cell yield could be obtained from a patient of any age and that all patients aged below 55 years are equally good donors [
20,
23].
Some of the lowest cell yields were caused probably by a minor technical failure during the bone marrow acquisition and the cell extraction process. Clot formations were observed in some cases during the red bone marrow aspiration. That could be a reason way the MNC yields in some cases could be lower than average.
The results of the study by Jo et al. demonstrated the influence of the cell count on clinical improvement [
13]. We have also observed that the cell quantity injected in the joint seems to have a positive influence on clinical improvement. However, patients receiving the highest MNC doses, compared to the lowest ones (cell counts range from 5 to 150 million), have demonstrated only slightly higher improvement levels. There was no linear correlation between a cell dose and the clinical effect observed. The cell dosage and the clinical signs improvement correlation patterns should be the next investigation object.
The HA therapy effects on the OA treatment are well known and documented [
24,
25]. There are recent meta-analyses performed about the clinical effectiveness of hyaluronic acid injections used for mild to moderate knee OA treatment. In them it was reported that a therapeutic effect was modest with a peak around 6–8 weeks persisting until 6 months without any serious side effects [
26,
27]. Our scoring results in the control group demonstrated an improvement of about 20 points at 1–3 months with a following decrease to 10 points over the starting point in a 6-month period and persisting until 12 months. Those findings are consistent with various studies regarding the HA clinical effectiveness, but demonstrates even longer duration of clinical effect as reported in meta-analyses. This lets us to assume that with extending the study groups the difference would increase in the clinical effect at the time point of 6–12 months between BM-MNC group and hyaluronic acid group.
The mononuclear cell application provides a good and safe pain-relieving effect. For everyday practice it could be recommended especially in cases if other more traditional OA treatment options fail or are contraindicated. The results of our study clearly demonstrate the great potential of cell-based treatments.
This study has some limitations. First, the placebo effect might play a role in the patients’ subjective self-scoring process, because the study design was not blinded. Some of the differences measured with scores were not statistically significant because of a high variability of results. Of course, the larger sample size and longer follow up period could be helpful to collect data about the factors that influence the outcome. The result evaluation of this study was based on highly subjective tools like clinical scores. In further studies, in the evaluation of the patient condition and objective changes after the BM-MNCs injection more objective methods must be used. MRI could be advantageous to observe changes in the joint structure.
5. Conclusions
The intra-articular injection of the BM MNC seems to be a safe manipulation with no side effects during the 12-month period.
The treatment of stage 2 and 3 OA patients with the BM MNC injection in knee joint leads to statistically significant clinical improvement between the starting point and 3, 6, and 12 months after.
In comparison to the control group patients treated with 3 hyaluronic acid injections, a statistically significant superiority in pain relief of the BM MNC single injection was observed at the 6- and 12-month follow-up period.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}