Point of Care Diagnostics for HIV in Resource Limited Settings: An Overview

Abstract
:1. Introduction
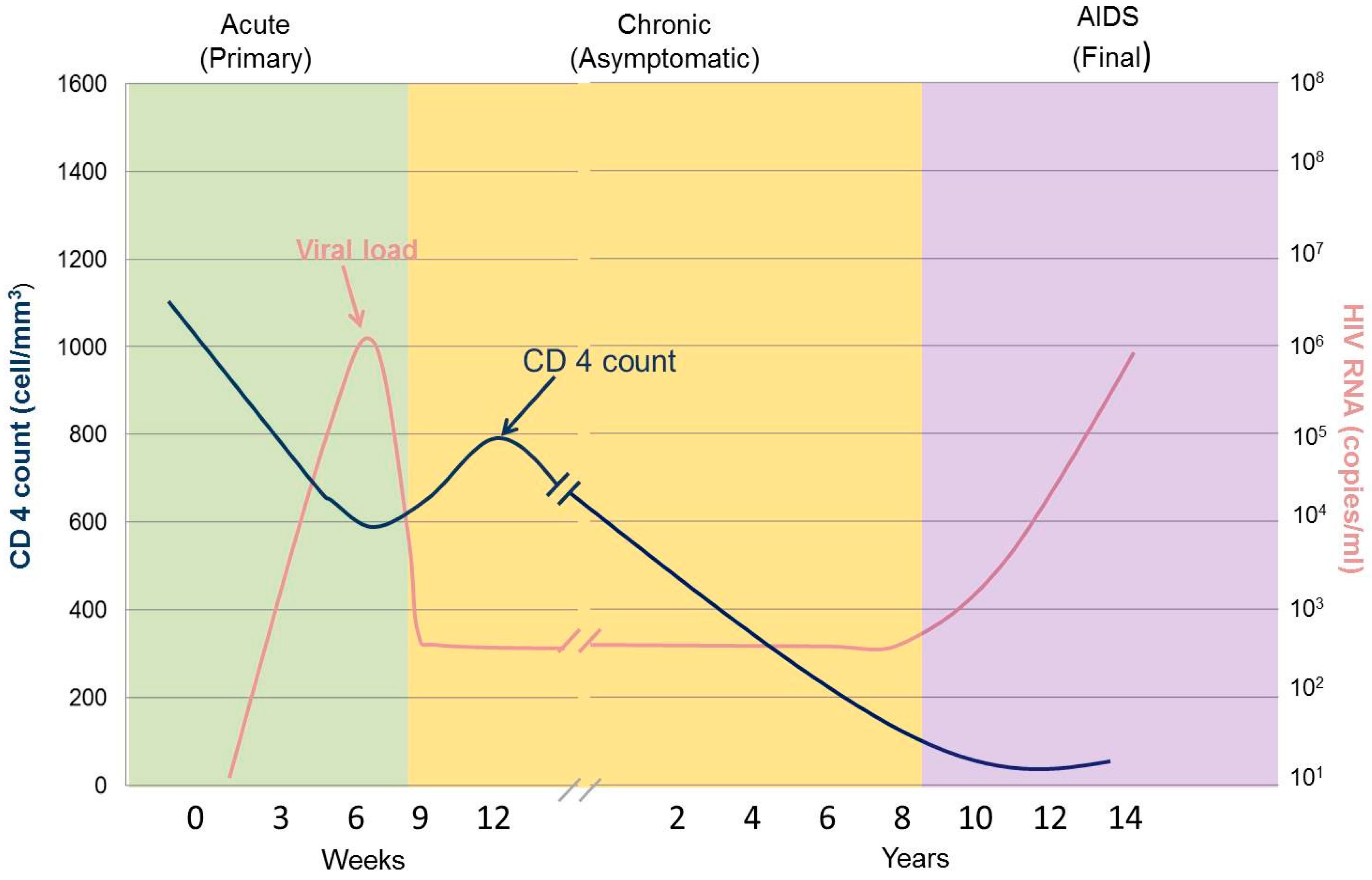
2. Stages of HIV Infection
3. HIV Diagnostic Tests
3.1. HIV Rapid Tests
3.2. HIV Viral Load Measurement
3.2.1. Simple Amplification Based Assay (SAMBA)
3.2.2. EOSCAPE HIV
3.2.3. Liat™ Analyser
3.2.4. Alere™ q Analyser
3.2.5. GeneXpert® System
3.3. Early Infant Diagnosis of HIV
3.4. CD4 Tests
3.4.1. PointCare NOW™
3.4.2. CyFlow® miniPOC
3.4.3. Daktari™ CD4 Counter
3.4.4. MBio™Diagnostics CD4 System
3.4.5. Visitect CD4
3.4.6. BD FACSPresto
3.4.7. Zyomyx CD4 Test
3.4.8. Pima™ Analyser
4. Technical and Commercialization Challenges in POC Diagnostics for HIV
5. Future Prospects
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Barre-Sinoussi, F.; Cherman, J.C.; Rey, F.; Nugeyre, M.T.; Chamaret, S.; Gruest, J.; Dauguet, C.; Axler-Blin, C.; Vézinet-Brun, F.; Rouzioux, C.; et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science 1983, 220, 868–871. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS: Fact Sheet 2015. UNITAID. HIV/AIDS Diagnostics Technology Landscape; Semi-Annual Update. 2015. Available online: http://www.unaids.org/sites/default/files/media_asset/20150901_FactSheet_2015_en.pdf (accessed on 2 February 2017).
- Stevens, W.; Gous, N.; Ford, N.; Scot, L.E. Feasibility of HIV point of care tests for resource limited settings: Challenges and solutions. MBC Med. 2014, 12, 173. [Google Scholar] [CrossRef] [PubMed]
- Setty, M.K.H.G.; Hewlett, I.K. Point of care technologies for HIV. AIDS Res. Treat. 2014, 2014, 497046. [Google Scholar]
- World Health Organization. Interim WHO Clinical Staging of HIV/AIDS and HIV/AIDS Case Definitions for Surveillance, Africa Region. 2005. Available online: http://www.who.int/hiv/pub/guidelines/clinicalstaging.pdf?ua=1 (accessed on 17 January 2017).
- Kranzer, K.; Lawn, S.D.; Johnson, L.F.; Bekker, L.; Wood, R. Community viral load and CD4 count distribution among people living with HIV in a South African township: Implications for treatment as prevention. J. Acquir. Immune Defic. Syndr. 2013, 63, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Holmes, K.K.; Mabey, D.; Ronald, A. Rapid tests for sexually transmitted infections (STIs): The way forward. Sex. Transm. Infect. 2006, 82, v1–v6. [Google Scholar] [CrossRef] [PubMed]
- Gubula, V.; Harris, L.F.; Ricco, A.J.; Tan, M.X.; Williams, D.E. Point of care diagnostics: Status and future. Anal. Chem. 2012, 84, 487–515. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: Antiretroviral Therapy for Infection in Adults and Adolescents: Recommendations for a Public Health Approach. 2010. Available online: http://apps.who.int/iris/bitstream/10665/44379/1/9789241599764_eng.pdf (accessed on 16 November 2016).
- World Health Organization: Guideline on When to Start Antiretroviral Therapy and on Pre-Exposure Prophylaxis for HIV. 2015. Available online: http://apps.who.int/iris/bitstream/10665/186275/1/9789241509565_eng.pdf (accessed on 16 November 2016).
- Gale, H.B.; Gitterman, S.R.; Hoffman, H.J.; Gordin, F.M.; Benator, D.A.; Labriola, A.M.; Kan, V.L. Is frequent CD4+ T-lymphocyte count monitoring necessary for persons with ≥300 cells/μL and HIV-1 suppression? Clin. Infect. Dis. 2013, 56, 1340–1343. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, G.W.; Angelmyer, A.; Eastbrook, P.J.; Horvath, T.; Vitoria, N.; Penazzato, M.; Doherty, M.C. Predicting treatment failure in adults and children on antiretroviral therapy: A systemic review of the performance characteristics of the 2010 WHO immunologic and clinical criteria for virologic failure. AIDS 2014, 28, S161–S169. [Google Scholar] [CrossRef] [PubMed]
- Enger, C.; Graham, N.; Peng, Y.; Chmiel, J.S.; Kingsley, L.A.; Detels, R.; Muñoz, A. Survival from early, intermediate, and late stages of HIV infection. JAMA 1996, 275, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Celum, C.L.; Buchbinder, S.P.; Donnell, D.; Douglas, J.M.; Mayer, K.; Koblin, B.; Marmor, M.; Bozeman, S.; Grant, R.M.; Sheppard, J.F.H.W. Early human immunodeficiency virus (HIV) infection in the HIV Network for Prevention trials vaccine preparedness cohort: Risk behaviours, symptoms, and early plasma and genital tract virus load. J. Infect. Dis. 2001, 183, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Jacquez, J.A.; Simon, C.P.; Koopman, J.S.; Sattenspiel, L.; Perry, T. Modeling and analyzing HIV transmission: The effect of contact patterns. Math. Biosci. 1988, 92, 119–199. [Google Scholar] [CrossRef]
- Schacker, T.; Collier, A.C.; Hughes, J.; Shea, T.; Corey, L. Clinical and epidemiologic features of primary HIV infection. Ann. Intern. Med. 1996, 125, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Roederer, M.; Dubs, J.G.; Anderson, M.T.; Raju, P.A.; Herzenberg, L.A.; Herzenberg, L.A. CD8 naive T cell counts decrease progressively in HIV-infected adults. J. Clin. Investig. 1995, 95, 2061–2066. [Google Scholar] [CrossRef] [PubMed]
- Margolick, J.B.; Donnenberg, A.D.; Chu, C.; O’Gorman, M.R.; Giorgi, J.V.; Munoz, A. Decline in total T cell count is associated with onset of AIDS, independent of CD4(+) lymphocyte count: Implications for AIDS pathogenesis. Clin. Immunol. Immunopathol. 1998, 88, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Gurtler, L. Difficulties and strategies of HIV diagnosis. Lancet 1996, 348, 176–179. [Google Scholar] [CrossRef]
- Zhang, M.; Versalovic, J. HIV update: Diagnostic tests and markers of disease progression and response to therapy. Am. J. Clin. Pathol. 2002, 118, S26–S32. [Google Scholar] [PubMed]
- Arora, D.R.; Maheshwari, M.; Arora, B. Rapid point of care testing for detection of HIV and clinical monitoring. ISRN AIDS 2013, 2013, 287269. [Google Scholar] [CrossRef] [PubMed]
- Aleku, G.A.; Adoga, M.P.; Agwale, S.M. HIV point of care diagnostics: Meeting the special needs of sub-Saharan Africa. J. Infect. Dev. Ctries. 2014, 8, 1231–1243. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Zaman, M.H. Low-cost tools for diagnosing and monitoring HIV infection in low-resource settings. Bull. WHO 2012, 90, 914–920. [Google Scholar] [CrossRef] [PubMed]
- WHO. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection. 2013. Available online: http://www.who.int/hiv/pub/guidelines/arv2013/en/ (accessed on 9 June 2016).
- Luft, L.M.; Gill, M.J.; Church, D.L. HIV-1 viral diversity and its implications for viral load testing: Review of current platforms. Int. J. Infect. Dis. 2011, 15, e661–e670. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, A.V.; Ushiro-Lumb, I.; Edemaga, D.; Joshi, H.A.; De Ruiter, A.; Szumilin, E.; Jendrulek, I.; McGuire, M.; Goel, N.; Sharma, P.I.; et al. SAMBA HIV semiquantitative test, a new point of care viral load monitoring assay for resource limited setting. J. Clin. Microbiol. 2014, 52, 3377–3383. [Google Scholar] [CrossRef] [PubMed]
- Innovations in Molecular Diagnostisc. Available online: http://www.wave80.com/products/ (accessed on 9 June 2016).
- Murtagh, M. UNITAIDS Technical Report: HIV/AIDS Diagnostic Landscape, 2nd ed.; World Health Organization: Geneva, Switzerland, 2012; Available online: http://scms.pfscm.org/portal/pls/portal/!PORTAL.wwpob_page.show?_docname=2808292.PDF (accessed on 15 February 2017).
- Tanriverdi, S.; Chen, L.; Chen, S. A rapid and automated sample to result HIV load test for near patient application. J. Infect. Dis. 2010, 201, S52–S58. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.; Gous, N.; Carmona, S.; Stevens, W. Laboratory Evaluation of the Liat HIV Quant (IQuum) Whole-Blood and Plasma HIV-1 Viral Load Assays for Point-of-Care Testing in South Africa. J. Clin. Microbiol. 2015, 53, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: WHO Prequalification of In Vitro Diagnostics, PUBLIC REPORT. 2016. Available online: http://www.who.int/diagnostics_laboratory/evaluations/pq-list/hiv-vrl/160613PQPublicReport_0226-032-00AlereHIVDetect_v2.pdf?ua=1 (accessed on 15 February 2017).
- Jani, I.V.; Meggi, B.; Vubil, A.; Sitoe, N.E.; Bhatt, N.; Tobaiwa, O.; Quevedo, J.I.; Loquiha, O.; Lehe, J.D.; Vojnov, L.; et al. Evaluation of the Whole Blood Alere Q NAT Point-of-Care RNA Assay for HIV-1 Viral Load Monitoring in a Primary Health Care Setting in Mozambique. J. Clin. Microbiol. 2016, 54, 2104–2108. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, N.; Dunning, L.; Kroon, M.; Myer, L. Laboratory Evaluation of the Alere q Point-of-Care System for Early Infant HIV Diagnosis. PLoS ONE 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization: WHO Prequalification of In Vitro Diagnostics, PUBLIC REPORT. 2016. Available online: http://www.who.int/diagnostics_laboratory/evaluations/pq-list/hiv-vrl/160613PQPublicReport_0259-0700-00_XpertQualHIV_v2.pdf?ua=1 (accessed on 15 February 2017).
- Michaeli, M.; Wax, M.; Gozlan, Y.; Rakovsky, A.; Mendelson, E.; Mor, O. Evaluation of Xpert HIV-1 Qual assay for resolution of HIV-1 infection in samples with negative or indeterminate Geenius HIV-1/2 results. J. Clin. Virol. 2015, 76, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Wittawatmongkol, O.; Vanprapar, N.; Chearskul, P.; Phongsamart, W.; Prasitsuebsai, W.; Sutthent, R.; Chokephaibulkit, K. Boosted p24 antigen assay for early diagnosis of perinatal HIV infection. J. Med. Assoc. Thail. 2010, 93, 187–190. [Google Scholar]
- Boyle, D.S.; Lehman, D.A.; Lillis, L.; Peterson, D.; Singhal, M.; Armes, N.; Parker, M.; Piepenburg, O.; Overbaugh, J. Rapid detection of HIV-1 proviral DNA for early infant diagnosis using recombinase polymerase amplification. MBio 2013, 4, e00135–e00213. [Google Scholar] [CrossRef] [PubMed]
- Fearon, M. The laboratory diagnosis of HIV infections. Can. J. Infect. Dis. Med. Microbiol. 2005, 16, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Moorehouse, M.; Conradie, F.; Venter, F. What is the role of CD4 count in a large public health antiretroviral programme? S. Afr. J. HIV Med. 2016, 17, 1–3. [Google Scholar]
- Masur, H.; Ognibene, F.P.; Yarchoan, R.; Shelhamer, J.H.; Baird, B.F.; Travis, W.; Suffrendini, A.F.; Deyton, L.; Kovacs, J.A.; Falloon, J. HIV targets CD4+ T cells, which are the most crucial cells of the immune system as the immune system uses these cells to fight infection. J. Ann. Intern. Med. 1989, 111, 223–231. [Google Scholar] [CrossRef]
- Boyle, D.S.; Hawkins, K.R.; Steele, M.S.; Singhal, M.; Cheng, X. Emerging technologies for point of care CD4 T-lymphocyte counting. Trends Biotechnol. 2012, 30, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Glynn, M.T.; Kinahan, D.J.; Ducree, J. CD4 counting technologies for HIV therapy monitoring in resource poor settings-state of the art and emerging microtechnologies. Lab Chip 2013, 13, 2731–2748. [Google Scholar] [CrossRef] [PubMed]
- Pointcare 2010. 8 Minutes to Better HIV/AIDS Patient Care. Available online: http://www.pointcare.net/docs/pointcare_now_brochure_eng.pdf (accessed on 3 March 2017).
- Bergeron, M.; Daneau, G.; Ding, T.; Sitoe, N.E.; Westerman, L.E.; Stokx, J.; Jani, I.V.; Coetzee, L.M.; Scott, L.; De Weggheleire, A.; et al. Performance of the PointCare Now system for CD4 counting in HIV patients based on five independent evaluations. PLoS ONE 2012, 7, e41166. [Google Scholar] [CrossRef]
- Shott, J.P.; Galiwango, R.M.; Reynolds, S.J. A Quality Management Approach to Implementing Point-of-Care Technologies for HIV Diagnosis and Monitoring in Sub-Saharan Africa. J. Trop. Med. 2012, 2012, 651927. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.; Diaw, P.A.; Daneau, G.; Diallo, A.A.; Mboup, S.; Dieye, T.N.; Kestens, L. Laboratory and field evaluation of the Partec CyFlow MiniPOC for absolute and relative CD4 T-cell enumeration. PLoS ONE 2015, 10, e0116663. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Liffson, M.A.; Inci, F.; Liang, L.; Sheng, Y.; Demirci, U. Advance in addressing technical challenges of point of care diagnostics in resource limited settings. Expert Rev. Mol. Diagn. 2016, 16, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Liu, Y.S.; Irimia, D.; Demirci, L.J.; Yang, L.; Zamir, W.; Rodrguez, R.; Toner, M.; Bashir, R. Cell detection and counting through cell lysate impedance spectroscopy in microfluidic devices. Lab Chip 2007, 7, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Logan, C.; Givens, M.; Ives, J.T.; Delaney, M.; Lochhead, M.J.; Schooley, R.T.; Benson, C.A. Performance evaluation of the MBio diagnostics point of care CD4 counter. J. Immunl. Methods 2013, 387, 107–113. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Who Prequalification of Diagnostic Programme: Public Report; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Bwana, P.; Vojnov, L.; Adhiambo, M.; Akinyi, C.; Mwende, J.; Prescott, M.; Mwau, M. The BD FACSPresto point of care CD4 test accurately enumerates CD4+ T cell sounts. PLoS ONE 2016, 11, e0167667. [Google Scholar] [CrossRef] [PubMed]
- Chin, C.D.; Linder, V.; Sia, S.K. Commercialization of microfluidic point of care diagnostic devices. Lab Chip 2012, 12, 2118–2134. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Prequalification of Diagnostics Programme: Public Report, Pima CD4 Test. 2011. Available online: http://www.who.int/diagnostics_laboratory/evaluations/111208_0099_032_00_public_report_v2.pdf (accessed on 25 August 2016).
- Kasama, S.; Nattawat, O.; Charin, T.; Korakot, P.; Boonrat, T.; Kovit, P. Performance evaluation of the Alere PIMA CD4 test for monitoring HIV-infected individuals in resource constrained setting. J. Acquir. Immune Defic. Syndr. 2011, 58, 141–147. [Google Scholar]
- Jung, W.; Han, J.; Choi, J.; Ahn, C. Point of care testing (POCT) diagnostic systems using microfluidic lab on a chip technologies. Microelectron. Eng. 2015, 132, 46–57. [Google Scholar] [CrossRef]
- Vashist, S.K.; Luppa, P.B.; Yeo, L.Y.; Ozcan, A.; Luong, J.H.T. Emerging technologies for next-generation point of care testing. Trends Biotechnol. 2015, 33, 692–705. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.K.; Rousseau, C. Point of care diagnostics: Extending the laboraoty network to reach the last lime. Curr. Opin. HIV AIDS 2017, 12, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.; Blumenfeld, N.R.; Laksanasopin, T.; Sia, S.K. Point of care diagnostics: Recent developments in a connected age. Anal. Chem. 2017, 89, 102–123. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Viral Load Tool | POC | Analyte | Detection Method | Time to Result | Sample Type and Volume | Additional Information |
|---|---|---|---|---|---|---|
| SAMBA | Yes | RNA | Isothermic amplification and Hapten-based signal detection | 90 min (SI 4 sample throughput, 24–48 tests/day), (SII 4 tests a day) | Plasma: 200 μL | Semi-quantitative; Detection: 1000 copies/mL Regulatory status: CE marked |
| EOSCAPE HIV | Yes | RNA | Amplification/Detection | 50 min | Whole blood: 100, plasma: 100 μL | Qualitative and quantitative Detection threshold: 1000 copies/mL Regulatory status: NA |
| Liat analyser | Yes | RNA | Multiplex Real-Time PCR Amplification/Detection | 30–35 min | Whole blood: 75 μL, plasma: 150 μL | Quantitative Detection threshold: 1000 copies/mL Regulatory status: In development |
| Alere q analyser | Yes | RNA | Real time PCR/microprobe array | 52 min (8 h throughput, 8 tests) | Whole blood: 25 μL; plasma: 25 μL or 500 μL | Quantitative Detection threshold: 1000 copies/mL Regulatory status: CE marked |
| GeneXpert | Near POC | RNA | Multiplex Real-Time PCR NA Amplification/Detection | 90 min | Plasma: 1 mL | Quantitative Detection range: 40–10,000,000 copies/mL Regulatory status: CE marked |
| CD4 Tool | Analyte | Detection Method | Technology | Time to Result or Tests | Additional Information |
|---|---|---|---|---|---|
| PointCare NOW™ | CD4, CD4%, 12 blood parameters, haemoglobin | CD4 monoclonal antibody labelled with colloidal gold | Flow cytometry | 8 min | Measures blood, fully automated, portable, table top Regulatory status: FDA approved CE marked |
| CyFlow® miniPOC | CD4, T cell, CD4% | Antibodies | Flow cytometry including laser modules, Optics, fluidics and electronics | 250 tests per day | Blood samples can be run one at a time or in batches, portable, compact Regulatory status: CE marked |
| Daktari™ CD4 Counter | CD4 | Antibody, label free, functions without optics, lenses or cameras | Microfluidic cell chromatography and lysate impedance spectroscopy | 14 min | Portable, robust Regulatory status: NA |
| MBio™Diagnostics CD4 System | CD4 and CD3 | Labelled antibodies | Imaging cytometry, immunostaining | +/−20 min per sample | Robust, uses low cost lasers Regulatory status: NA |
| Visitect CD4 | CD4 on T cells | Antibodies, colloidal gold | Lateral flow | 40 min | Semi-quantitative CD4 > 350, CD4 > 500 Regulatory status: CE marked |
| BD FACSPresto | CD4, %CD4 and haemoglobin | Fluorochrome conjugated antibody | Image based counting technology | 60 tests in 8 h | Cartridge contains dried reagents Regulatory status: CE marked WHO prequalification |
| Zyomyx CD4 Test | CD4 | Antibodies | Mechanical mixer/spinner, capillary tube | 6 min | Instrument free Regulatory status: CE marked |
| Pima™ Analyser | CD4, CD3 | Antibodies | Image based immune haematology test, fluorescence | 20 min | Good technical support, no routine maintenance Regulatory status: WHO prequalification |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manoto, S.L.; Lugongolo, M.; Govender, U.; Mthunzi-Kufa, P. Point of Care Diagnostics for HIV in Resource Limited Settings: An Overview. Medicina 2018, 54, 3. https://doi.org/10.3390/medicina54010003
Manoto SL, Lugongolo M, Govender U, Mthunzi-Kufa P. Point of Care Diagnostics for HIV in Resource Limited Settings: An Overview. Medicina. 2018; 54(1):3. https://doi.org/10.3390/medicina54010003
Chicago/Turabian StyleManoto, Sello Lebohang, Masixole Lugongolo, Ureshnie Govender, and Patience Mthunzi-Kufa. 2018. "Point of Care Diagnostics for HIV in Resource Limited Settings: An Overview" Medicina 54, no. 1: 3. https://doi.org/10.3390/medicina54010003
APA StyleManoto, S. L., Lugongolo, M., Govender, U., & Mthunzi-Kufa, P. (2018). Point of Care Diagnostics for HIV in Resource Limited Settings: An Overview. Medicina, 54(1), 3. https://doi.org/10.3390/medicina54010003