How to Manage Impacted Third Molars: Germectomy or Delayed Removal? A Systematic Literature Review





Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Question
2.2. Selection Criteria
2.2.1. Participants
2.2.2. Interventions
2.2.3. Outcomes
2.2.4. Study Design
- Publications in languages other than English, French, German, Spanish, or Italian.
- Case reports, case series, review articles, abstracts, and discussions.
- Studies that evaluated less than five patients.
2.3. Information Sources and Search
- #1
- (Molar, Third/) OR ((“third molar *” OR “wisdom tooth” OR “wisdom teeth” OR “3rd molar *” OR third-molar).mp.)
- #2
- (((Tooth, impacted/) OR ((tooth impact *) OR (teeth impact *).mp.)) OR Tooth, unerupted/)
- #3
- third molar * germ OR wisdom tooth germ OR wisdom teeth germ OR 3rd molar* germ OR third.molar germ.mp.
- #4
- #1 AND (#2 OR #3)
- #5
- (((Tooth extraction/indications) OR ((extract * OR remov *)/indications)) OR Tooth extraction/early) OR Tooth extraction/early
- #6
- #4 AND #5
- #7
- third molar * germectomy OR wisdom tooth germectomy OR wisdom teeth germectomy OR 3rd molar * germectomy OR third-molar germectomy
- #8
- #6 OR #7.
2.4. Study Selection
2.5. Data Collection Process
2.6. Data Items
2.7. Outcomes
2.8. Risk of Bias in Individual Studies and Quality of Evidence
3. Results
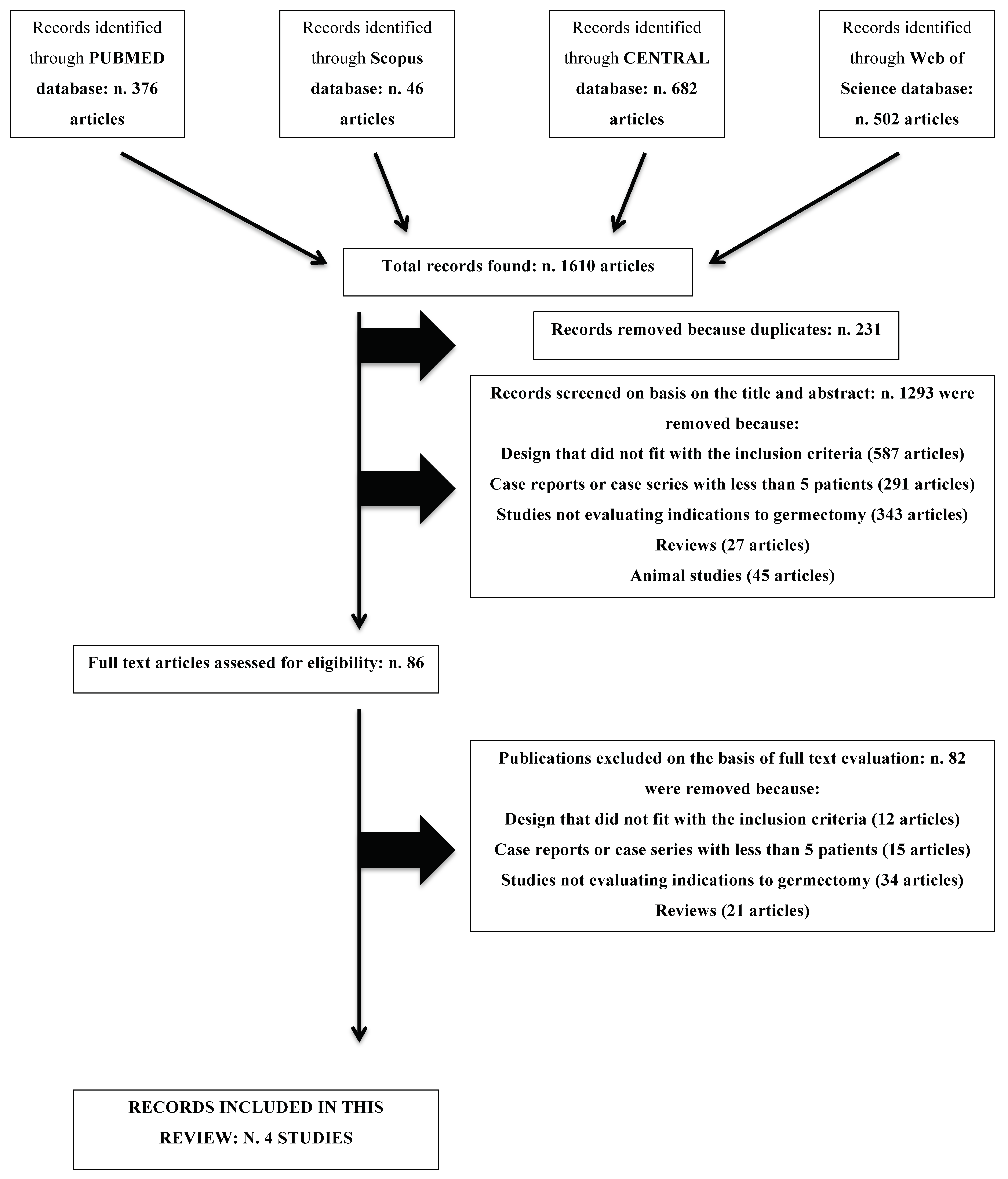
3.1. Exclusion of Studies
3.2. Included Studies
3.3. Characteristics of Participants
3.4. Characteristics of Interventions
3.5. Characteristics of Outcome Measures
3.6. Risk of Bias in Included Studies and Strength of Evidence
3.7. Effects of Interventions
3.7.1. Surgical Complications
3.7.2. Clinical Recommendations
3.7.3. Correction of Second Molar Inclination
4. Discussion
- morphostructural alterations or ectopic impactions;
- eruption not allowed by dysplastic alterations of the tooth germ or pathologic processes of the bone;
- necessity of distalization of first or second molar; or
- excessive anteroposterior growth or severe dentoalveolar discrepancy.
4.1. Clinical Recommendations for Syndrome/Incompliant Patients
4.2. Risk of Nonintervention
4.3. Risk of Intervention
4.4. Benefit of Nonintervention
4.5. Benefit of Intervention
4.6. Indications for Third Molar Extraction in Syndrome Patients—Early Removal
4.7. Indications for Third Molar Extraction in Syndrome Patients—Late Removal
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kaplan, R.G. Some factors related to mandibular third molar impaction. Angle Orthod. 1975, 45, 153–158. [Google Scholar] [PubMed]
- Cassetta, M.; Altieri, F. The influence of mandibular third molar germectomy on the treatment time of impacted mandibular second molars using brass wire: a prospective clinical pilot study. Int. J. Oral Maxillofac. Surg. 2017, 46, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.K.; Whang, C.Z.; Bister, D. Orthodontic uprighting of severely impacted mandibular second molars. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 116–124. [Google Scholar] [CrossRef]
- McAboy, C.P.; Grumet, J.T.; Siegel, E.B.; Iacopino, A.M. Surgical uprighting and repositioning of severely impacted mandibular second molars. J. Am. Dent. Assoc. 2003, 134, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Pogrel, M.A. The surgical uprighting of mandibular second molars. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 180–183. [Google Scholar] [CrossRef]
- Chiapasco, M.; Crescentini, M.; Romanoni, G. Germectomy or delayed removal of mandibular impacted third molars: the relationship between age and incidence of complications. J. Oral Maxillofac. Surg. 1995, 53, 418–422. [Google Scholar] [CrossRef]
- Knutsson, K.; Brehmer, B.; Lysell, L.; Rohlin, M. General dental practitioners’ evaluation of the need for extraction of asymptomatic mandibular third molars. Commun. Dent. Oral Epidemiol. 1992, 20, 347–350. [Google Scholar] [CrossRef]
- Knutsson, K.; Brehmer, B.; Lysell, L.; Rohlin, M. Asymptomatic mandibular third molars: Oral surgeons’ judgement of the need for extraction. J. Oral Maxillofac. Surg. 1992, 50, 329–333. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.J.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Chaparro-Avendaño, A.; Pérez-García, S.; Valmaseda-Castellón, E.; Berini-Aytés, L.; Gay-Escoda, C. Morbidity of third molar extraction in patients between 12 and 18 years of age. Med. Oral Patol. Oral Cir. Bucal 2005, 10, 422–431. [Google Scholar]
- Cunha-Cruz, J.; Rothen, M.; Spiekerman, C.; Drangsholt, M.; McClellan, M.; Huang, G.J.; Northwest Practice-Based Research Collaborative in Evidence-Based Dentistry. Recommendations for third molar removal: A practice-based cohort study. Am. J. Public Health 2014, 104, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Jasinevicius, T.R.; Pyle, M.A.; Kohrs, K.J.; Majors, J.D.; Wanosky, L.A. Early third molar extractions: US dental school departments’ recommendations from 1998/99 to 2004/05. Quintessence Int. 2008, 39, 165–176. [Google Scholar] [PubMed]
- Kupietzky, A. Correction of eruption of permanent molars utilizing the brass wire technique. Pediatr. Dent. 2000, 22, 408–412. [Google Scholar]
- Chiapasco, M.; De Cicco, L.; Marrone, G. Side effects and complications associated with third molar surgery. Oral Surg. Oral Med. Oral Pathol. 1993, 76, 412–420. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Fisher, S.E. Routine review of patients after extraction of third molars: is it justified. Br. J. Oral Maxillofac. Surg. 1997, 35, 393–395. [Google Scholar] [CrossRef]
- Guralnick, W.C.; Laskin, D.M. NIH Consensus Conference for removal of third molars. J. Oral Surg. 1980, 38, 235–236. [Google Scholar]
- Lysell, L.; Rohlin, M. A study of indications used for removal of the mandibular third molar. Int. J. Oral Maxillofac. Surg. 1988, 17, 161–164. [Google Scholar] [CrossRef]
- Bruce, R.A.; Frederickson, G.C.; Small, G.S. Age of patients and morbidity associated with mandibular third molar surgery. J. Am. Dent. Assoc. 1980, 101, 240–245. [Google Scholar]
- Leonard, M.S. Removing third molars: A review for the general practitioner. J. Am. Dent. Assoc. 1992, 123, 77–78. [Google Scholar] [CrossRef]
- Fisher, S.E.; Frame, J.W.; Rout, P.G. Factors affecting the onset and severity of pain following the surgical removal of unilateral impacted mandibular third molar teeth. Br. Dent. J. 1998, 164, 351–354. [Google Scholar] [CrossRef]
- Larsen, P.E. Alveolar osteitis after surgical removal of impacted mandibular third molars. Identification of the patient at risk. Oral Surg. Oral Med. Oral Pathol. 1992, 73, 393–397. [Google Scholar] [CrossRef]
- Ali, A.S.; Benton, J.A.; Yates, J.M. Risk of inferior alveolar nerve injury with coronectomy vs surgical extraction of mandibular third molars-A comparison of two techniques and review of the literature. J. Oral Rehabil. 2018, 45, 250–257. [Google Scholar] [CrossRef] [PubMed]
- La Monaca, G.; Vozza, I.; Giardino, R.; Annibali, S.; Pranno, N.; Cristalli, M.P. Prevention of neurological injuries during mandibular third molar surgery: Technical notes. Ann. Stomatol. (Roma) 2017, 8, 45–52. [Google Scholar] [CrossRef]
- Cervera-Espert, J.; Pérez-Martínez, S.; Cevera-Ballester, J.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Coronectomy of impacted mandibular third molars: A meta-analysis and systematic review of the literature. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e505–e513. [Google Scholar] [CrossRef] [PubMed]
- Lysell, L.; Brehmer, B.; Knuttson, K.; Rohlin, M. Judgement on removal of asymptomatic mandibular third molars: influence of the perceived likelihood of pathology. Dentomaxillofac. Radiol. 1993, 22, 173–177. [Google Scholar] [CrossRef]
- Knuttson, K.; Lysell, L.; Rohlin, M. Dentists’ decisions on early removal of mandibular third molars: A 10-year follow-up study. Community Dent. Oral Epidemiol. 2001, 29, 308–314. [Google Scholar] [CrossRef]
- Knuttson, K.; Lysell, L.; Rohlin, M. Dentists’ judgment strategies on early removal of mandibular third molars. J. Dent. Res. 2000, 79, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Kostopoulou, O.; Brickley, M.R.; Shepherd, J.P.; Newcombe, R.G.; Knuttson, K.; Rohlin, M. Intra-observer reliability regarding removal of asymptomatic third molars. Br. Dent. J. 1998, 184, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, J.F.; Antczak-Bouckoms, A.A. Decision analysis in the evaluation of clinical strategies for the management of mandibular third molars. J. Dent. Educ. 1987, 51, 652–660. [Google Scholar]
- Mercler, P.; Precious, D. Risks and benefits of removal of impacted third molars. A critical review of the literature. Int. J. Oral Maxillofac. Surg. 1992, 21, 17–27. [Google Scholar]
- Kruger, E.; Thomson, W.M.; Konthasinghe, P. Third molar outcomes from age 18 to 26: Findings from a population-based New Zealand longitudinal study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 92, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.J.; Brickley, M.R.; Goodey, R.D.; Shepherd, J.P. The cost, effectiveness and cost effectiveness of removal and retention of asymptomatic, disease free third molars. Br. Dent. J. 1999, 187, 380–384. [Google Scholar] [CrossRef]
- Song, F.; O’Meara, S.; Wilson, P.; Golder, S.; Kleijnen, J. The effectiveness and cost-effectiveness of early removal of wisdom teeth. Health Technol. Assess. 2000, 4, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Károlyházy, K.; Kovács, E.; Kivovics, P.; Fejérdy, P.; Arányi, Z. Dental status andoral health of patients with epilepsy: an epidemiologic study. Epilepsia 2003, 44, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Shapira, J.; Birenboim, R.; Shoshani, M.; Abdel-Kader, A.; Behar, O.; Moskovitz, M.; Ben-Attar, Y.; Chaushu, S.; Becker, C.K. Overcoming the oral aspects of self-mutilation: Description of a method. Spec. Care Dent. 2016, 36, 282–287. [Google Scholar] [CrossRef]
- Patini, R.; Staderini, E.; Gallenzi, P. Multidisciplinary surgical management of Cowden syndrome: Report of a case. J. Clin. Exp. Dent. 2016, 18, 472–474. [Google Scholar] [CrossRef]
- Facciolo, M.T.; Riva, F.; Gallenzi, P.; Patini, R.; Gaglioti, D. A rare case of oral multisystem Langerhans cell histiocytosis. J. Clin. Exp. Dent. 2017, 9, e820–e824. [Google Scholar] [CrossRef] [PubMed]
- Patini, R.; Staderini, E.; Lajolo, C.; Lopetuso, L.; Mohammed, H.; Rimondini, L.; Rocchetti, V.; Franceschi, F.; Cordaro, M.; Gallenzi, P. Relationship between oral microbiota and periodontal disease: A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 5775–5788. [Google Scholar] [PubMed]
- Pippi, R.; Pietrantoni, A.; Patini, R.; Santoro, M. Is telephone follow-up really effective in early diagnosis of inflammatory complications after tooth extraction? Med. Oral Patol. Oral Cir. Bucal 2018, 23, e707–e715. [Google Scholar] [CrossRef]
- Singh Gill, A.; Morrissey, H.; Rahman, A. A systematic review and meta-analysis evaluating antibiotic prophylaxis in dental implants and extraction procedures. Medicina (Kaunas) 2018, 54, 95. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author (Year) | Study Type | Sample Size | Population Details | Male/Female% (Age ± SD) | Complications | Follow-Up (Months ± SD) |
|---|---|---|---|---|---|---|
| Chaparro-Avendaño et al. (2005) | Retrospective | 173 | Patients subjected to third molar surgical extraction in a Master University Course | 33.1/66.9 | Pain and swelling, infection, trismus, ecchymosis, and IAN and LN paresthesia | NR |
| Group A (12–14 yr) | ||||||
| Group B (15–16 yr) | ||||||
| Group C (17–18 yr) | ||||||
| Jasinevicius et al. (2008) | Recommendations | 146 | Questionnaires mailed to department chairpersons regarding recommendations about prophylactic third molar extraction | NR | NR | Not Applicable |
| Adolescent (<21 yr) | ||||||
| Young Adult (21–35 yr) | ||||||
| Adult (>35 yr) | ||||||
| Cunha-Cruz et al. (2014) | Prospective | 797 | Cohort of patients enrolled by dentists as part of the network named PRECEDENT (Northwest Practice-based REsearch Collaborative in Evidence-based DENTistry) | 50.9/49.1 | NR | 19.7 ± 5.3 |
| >16 yr | ||||||
| Cassetta et al. (2017) | Prospective | 14 | Patients subjected to third molar surgical extraction in a University Dental Clinic | 50/50 (12.9 ± 0.5) | None | 0.23 ± NR |
| Item | Chaparro-Avendaño et al. | Jasinevicius et al. | Cunha-Cruz et al. | Cassetta et al. |
|---|---|---|---|---|
| Clear stated aim | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 1 | 0 | 1 | 1 |
| Unbiased assessment of the study endpoint | 2 | 2 | 2 | 2 |
| Appropriate follow-up | 0 | 0 | 2 | 1 |
| Loss to follow-up less than 5% | 2 | 1 | 1 | 2 |
| Appropriate calculation of the study size | 0 | 0 | 0 | 0 |
| Adequate statistical analyses | 2 | 2 | 2 | 2 |
| TOTAL | 9 | 7 | 10 | 10 |
| Overall risk of bias | Medium | High | Medium | Medium |
| Early Removal | Late Removal | |
|---|---|---|
| Indications | Morphologic abnormalities | Orthodontic considerations (dentoalveolar discrepancy, distalization of upper molars) |
| Ekman–Westborg–Julin syndrome | ||
| Self-mutilating behavior or recurrent epilepsy | Patients with increased risk of tooth loss |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staderini, E.; Patini, R.; Guglielmi, F.; Camodeca, A.; Gallenzi, P. How to Manage Impacted Third Molars: Germectomy or Delayed Removal? A Systematic Literature Review. Medicina 2019, 55, 79. https://doi.org/10.3390/medicina55030079
Staderini E, Patini R, Guglielmi F, Camodeca A, Gallenzi P. How to Manage Impacted Third Molars: Germectomy or Delayed Removal? A Systematic Literature Review. Medicina. 2019; 55(3):79. https://doi.org/10.3390/medicina55030079
Chicago/Turabian StyleStaderini, Edoardo, Romeo Patini, Federica Guglielmi, Andrea Camodeca, and Patrizia Gallenzi. 2019. "How to Manage Impacted Third Molars: Germectomy or Delayed Removal? A Systematic Literature Review" Medicina 55, no. 3: 79. https://doi.org/10.3390/medicina55030079
APA StyleStaderini, E., Patini, R., Guglielmi, F., Camodeca, A., & Gallenzi, P. (2019). How to Manage Impacted Third Molars: Germectomy or Delayed Removal? A Systematic Literature Review. Medicina, 55(3), 79. https://doi.org/10.3390/medicina55030079