Development of an Adapted Model for Decision-Making to Improve Reasoning and Risk Assessment in an Emergency Team: A Prospective Simulation Study

 ,
,
Abstract
:1. Introduction
Description of the Problem
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Intervention
2.4. Study of the Intervention(s)
2.5. Statistical Methods
2.6. Ethical Considerations
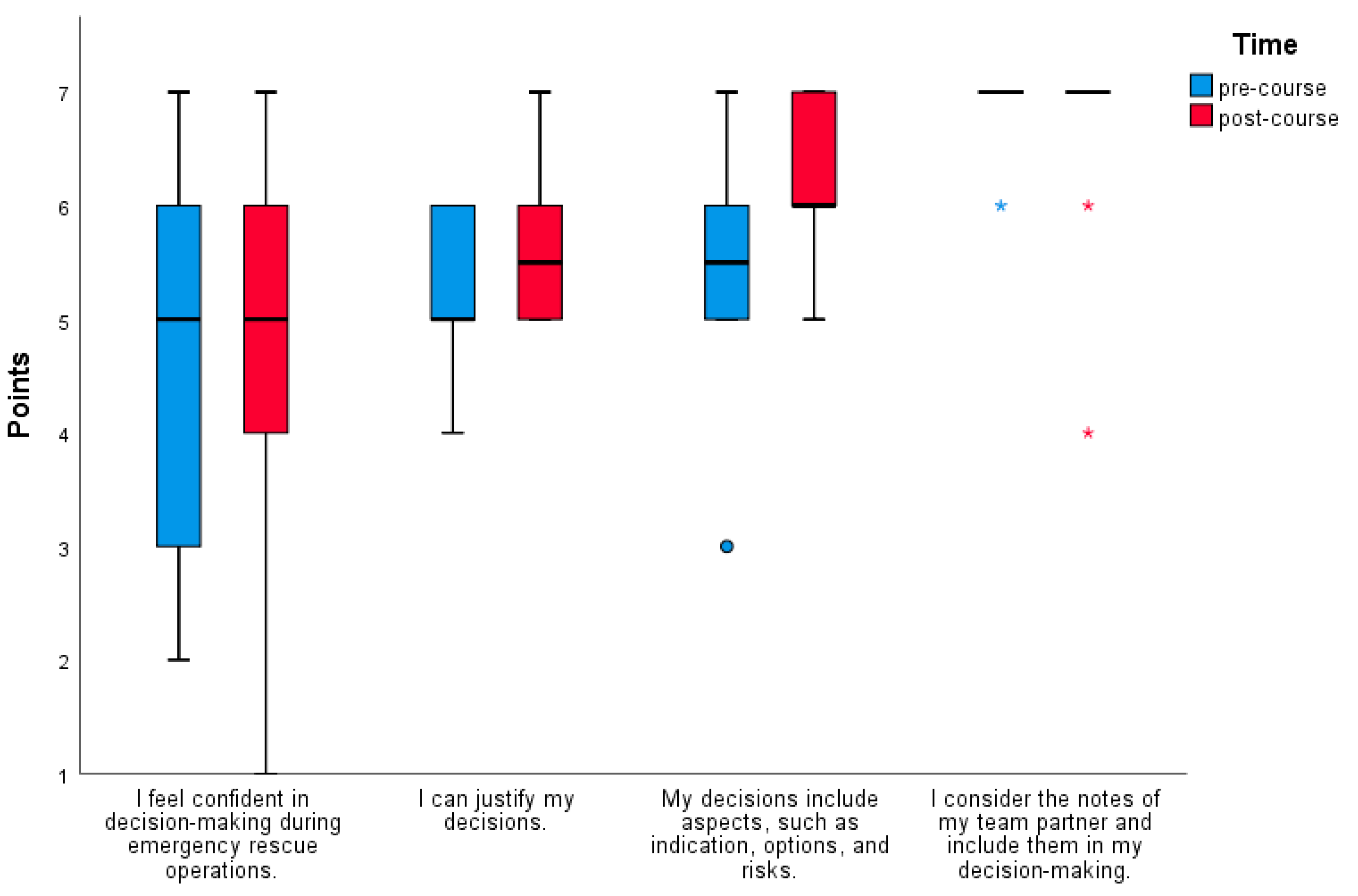
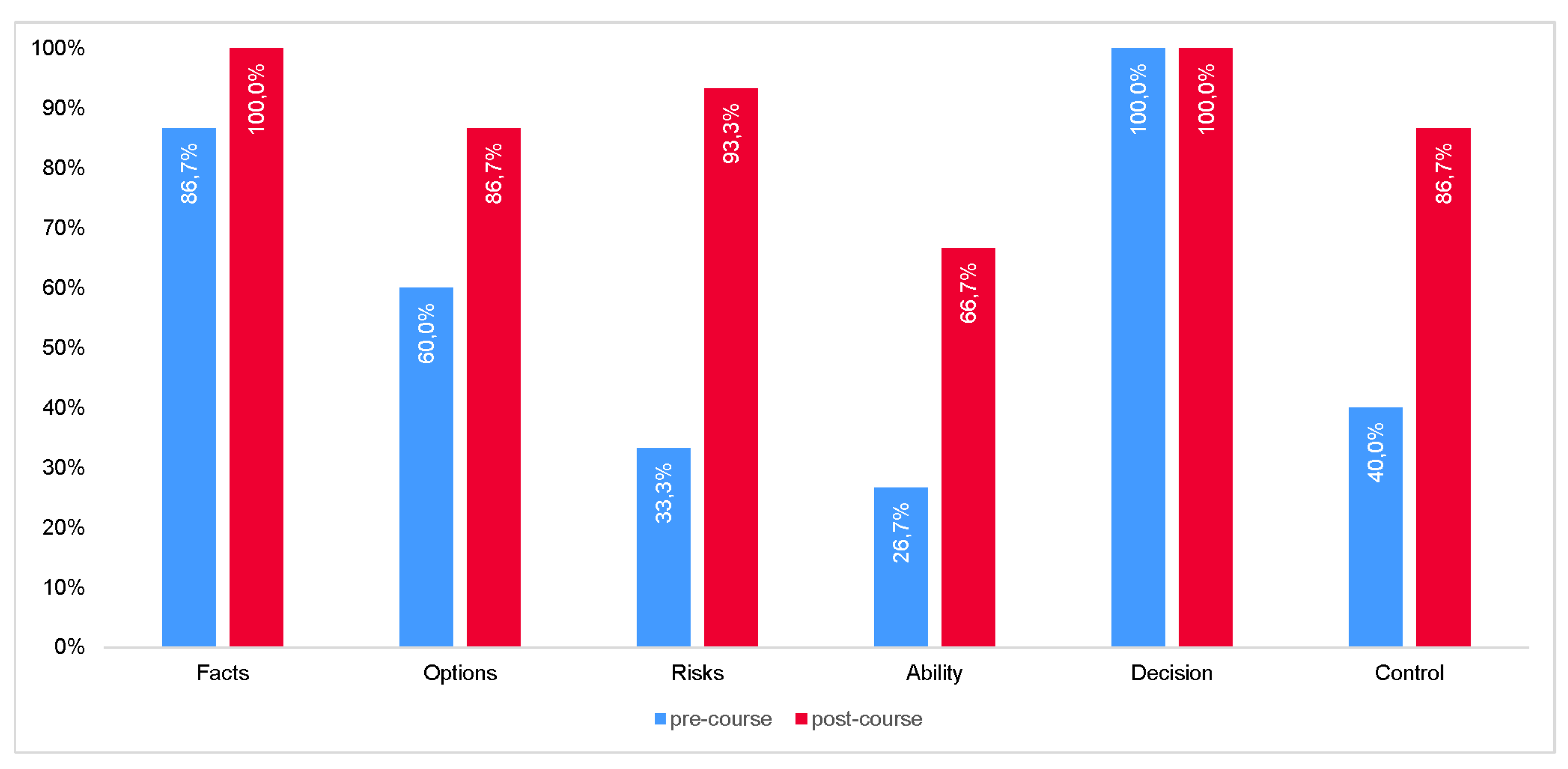
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Croskerry, P. Achieving Quality in Clinical Decision Making: Cognitive Strategies and Detection of Bias. Acad. Emerg. Med. 2002, 9, 1184–1204. [Google Scholar] [CrossRef]
- Meindl-Fridez, C.; Breckwoldt, J.; Battegay, E. Medizinische (Notfall-)Entscheidungen und wie man Fehler vermeidet. Notfall Rettungsmed. 2018, 21, 186–191. (In German) [Google Scholar] [CrossRef]
- Vetter, B.; Gasch, B.; Padosch, S.A. Medizinisches Handeln in komplexen Notfallsituationen: Kompetent und erfolgreich entscheiden, kommunizieren und führen. Anaesthesist 2015, 64, 298–303. (In German) [Google Scholar] [CrossRef] [PubMed]
- Bubb, H. Human reliability: A key to improved quality in manufacturing. Hum. Factors Man. 2005, 15, 353–368. [Google Scholar] [CrossRef]
- Rall, M.; Lackner, C.K. Crisis Resource Management (CRM). Notfall Rettungsmed. 2010, 13, 349–356. [Google Scholar] [CrossRef]
- Soll, H.; Proske, S.; Hofinger, G.; Steinhardt, G. Decision-Making Tools for Aeronautical Teams: FOR-DEC and Beyond. Aviat. Psychol. Appl. Hum. Factors 2016, 6, 101–112. [Google Scholar] [CrossRef]
- Arriaga, A.F.; Bader, A.M.; Wong, J.M.; Lipsitz, S.R.; Berry, W.R.; Ziewacz, J.E.; Hepner, D.L.; Boorman, D.J.; Pozner, C.N.; Smink, D.S.; et al. Simulation-based trial of surgical-crisis checklists. N. Engl. J. Med. 2013, 368, 246–253. [Google Scholar] [CrossRef] [PubMed]
- O’Hare, D. Aeronautical Decision Making: Metaphors, Models, and Methods. In Principles and Practice of Aviation Psychology; Tsang, P.S., Ed.; CRC Press: Boca Raton, FL, USA, 2003. [Google Scholar]
- Hörmann, H.J. FOR-DEC—A Prescriptive Model for Aeronautical Decision Making. Presented at the 21. WEAAP-Conference, Dublin, Ireland, 28–31 March 1994. [Google Scholar]
- Burger, K.H. Basic Competence for Optimum Performance. Competence Criteria for Lufthansa Flight Crew Members; Deutsche Lufthansa AG: Frankfurt, Germany, 2007. [Google Scholar]
- Rall, M.; Glavin, R.J.; Flin, R. The ‘10-seconds-for-10-min principle’. Bull. R. Coll. Anaesthetists 2008, 51, 2614–2616. [Google Scholar]
- Reay, G.; Rankin, J.A.; Smith-MacDonald, L.; Lazarenko, G.C. Creative adapting in a fluid environment: An explanatory model of paramedic decision making in the pre-hospital setting. BMC Emerg. Med. 2018, 18, 42. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Category | Skills |
|---|---|
| Airway management | Bag-valve-mask ventilation, i-gel (supraglottic airway device), non-invasive ventilation, oxygen therapy |
| Pharmacotherapy (Mostly used if an emergency physician was requested—or is en route—to the emergency site) | Crystalloid infusion, acetylsalicylic acid, epinephrine, amiodarone, atropine, butylscopolamine, dimethindene maleate, flumazenil, furosemide, glucose, ipratropium bromide, heparin, ketamine, morphine, naloxone, midazolam, nitroglycerin, prednisolone, salbutamol, tranexamic acid, urapidil |
| Electrotherapy (Mostly used if an emergency physician was requested—or is en route—to the emergency site) | Defibrillation, cardioversion, transcutaneous pacing |
| Trauma | Pelvic sling, tourniquet, hemostatic gauze, needle decompression, spinal immobilization, bandages |
| Routes of administration | Intravenous, intramuscular, intraosseous, inhalation |
| Subjects of the Training |
|---|
| ● Memory and cognitive performance: While under normal circumstances about 7 ± 2 units of information (“chunks”) are simultaneously and callable noticeable, under stress, the brain’s short-term memory capacity decreases substantially. ● Decision-making under stress: The non-reflective, intuitive process is activated, with no conscious decision-making process beforehand. This corresponds to the archaic fight or to the escape reaction. ● Fixation errors and consequences: Since intuitive decision-making under stress is often based on experience, there is a risk of fixation errors. The decision-maker sticks to an impression, loses the overall view and professional objectivity, so that alternatives or risks are misjudged (example: chest pain can only be an acute coronary syndrome). ● Influences on cognitive performance: Being short of sleep, fatigue, dynamic progress of the emergency, action pressure, etc. ● Influence of personal competence: Concerns the point “Ability/Authorization/Competence”. Reflection of one’s own professional capacity and competence. Cross-check with the team partner, 4 eyes principle, know your own weaknesses, own training state of medical skills, knowledge of medical facts and guidelines, etc. ● Examples of decisions from other disciplines: Aircraft ditching in the Hudson River, the sinking of the Costa Concordia, etc. ● Legal aspects of decisions: Those who act beyond their approvals must justify their measures. If an emergency exists, the ‘offender’ may take an action that is necessary, proportionate, and appropriate to avert the danger. In this respect, the paramedic must consider the urgency of the measures, as well as the distance to the nearest appropriate hospital, or the arrival time of the next emergency physician. ● Explanation of existing decision-making aids: For example DESIDE (Detect, Estimate, Set safety objectives, Identify, Do, Evaluate), FOR-DEC (Facts, Options, Risks & Benefits, Decision, Execution, Check), PASS (Problem identification, Acquire information, Survey strategy, Select strategy), SOAR (Situation, Options, Act, Repeat), etc. |
| FOR-DEC | FAR-BEK | Commentary |
|---|---|---|
| Facts | Fakten (facts) | Situation, facts, actual analysis (e.g., what is the correct indication for treatment?) |
| Options | Alternativen (alternatives, options) | Which options are available? Are less invasive measures possible? Have basic measures been completely carried out? |
| Risks | Risikoabwägung (risks) | Consideration of risks and benefits. Which risks and benefits are associated with the respective options for action? |
| Decision | Befugnis/Kompetenz (ability, authorization, competence) | Have I mastered the measure? Do I have approval for it? Do I need more resources, such as physicians, fire department, or a team for extracorporeal life support (ECLS)? |
| Execution | Entscheidung (decision) | Determine a method with the greatest chance of success and lowest associated risks. Perform the procedures (e.g., application according to the four-eye principle). |
| Control | Kontrolle (control) | Review of the implemented measure, monitoring, etc. |
| Example 1: Focus Alternatives and Risks |
| Unconscious patient (GCS 6) with suspected stroke or intracranial hemorrhage at compromised ventilation in a third-floor apartment. Due to the unconsciousness and need for emergency anesthesia with endotracheal intubation for transport, an emergency physician is requested to the site. However, this takes 20 min to the scene. Due to the circumstances of the scene, the only way out remains through the narrow stairwell. Decision making: Staying in the apartment with the advantage to carry out an adequate assisted ventilation under suction, but thereby to extend the rescue time. Or to carry out rapid transport through the stairwell with the advantage of initiating the transport and to approach the emergency physician in order to reach the target clinic more quickly. The risk of unmanageable vomiting and limited ventilation options is accepted. |
| Example 2. Focus Competence and Approval |
| Pregnant patient (36th week of pregnancy) with a painful radius fracture and necessary analgesia. Decision making: Physical measures (cooling, splinting) bring only limited relief so that pharmacological therapy seems inevitable. The paramedics have approval for ketamine for analgesia, which, however, is not recommended for analgesia in monotrauma in pregnant women. Or, as opiates might be indicated as potent analgesics, but for which the paramedics have no approval, to request the emergency physician to the scene. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Häske, D.; Dorau, W.; Heinemann, N.; Stock, J.-P.; Schempf, B. Development of an Adapted Model for Decision-Making to Improve Reasoning and Risk Assessment in an Emergency Team: A Prospective Simulation Study. Medicina 2019, 55, 339. https://doi.org/10.3390/medicina55070339
Häske D, Dorau W, Heinemann N, Stock J-P, Schempf B. Development of an Adapted Model for Decision-Making to Improve Reasoning and Risk Assessment in an Emergency Team: A Prospective Simulation Study. Medicina. 2019; 55(7):339. https://doi.org/10.3390/medicina55070339
Chicago/Turabian StyleHäske, David, Wolfgang Dorau, Niklas Heinemann, Jan-Philipp Stock, and Benjamin Schempf. 2019. "Development of an Adapted Model for Decision-Making to Improve Reasoning and Risk Assessment in an Emergency Team: A Prospective Simulation Study" Medicina 55, no. 7: 339. https://doi.org/10.3390/medicina55070339