
Inequalities in Life Expectancy by Education and Its Changes in Lithuania during 2001–2014



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Population
2.3. Statistical Analysis
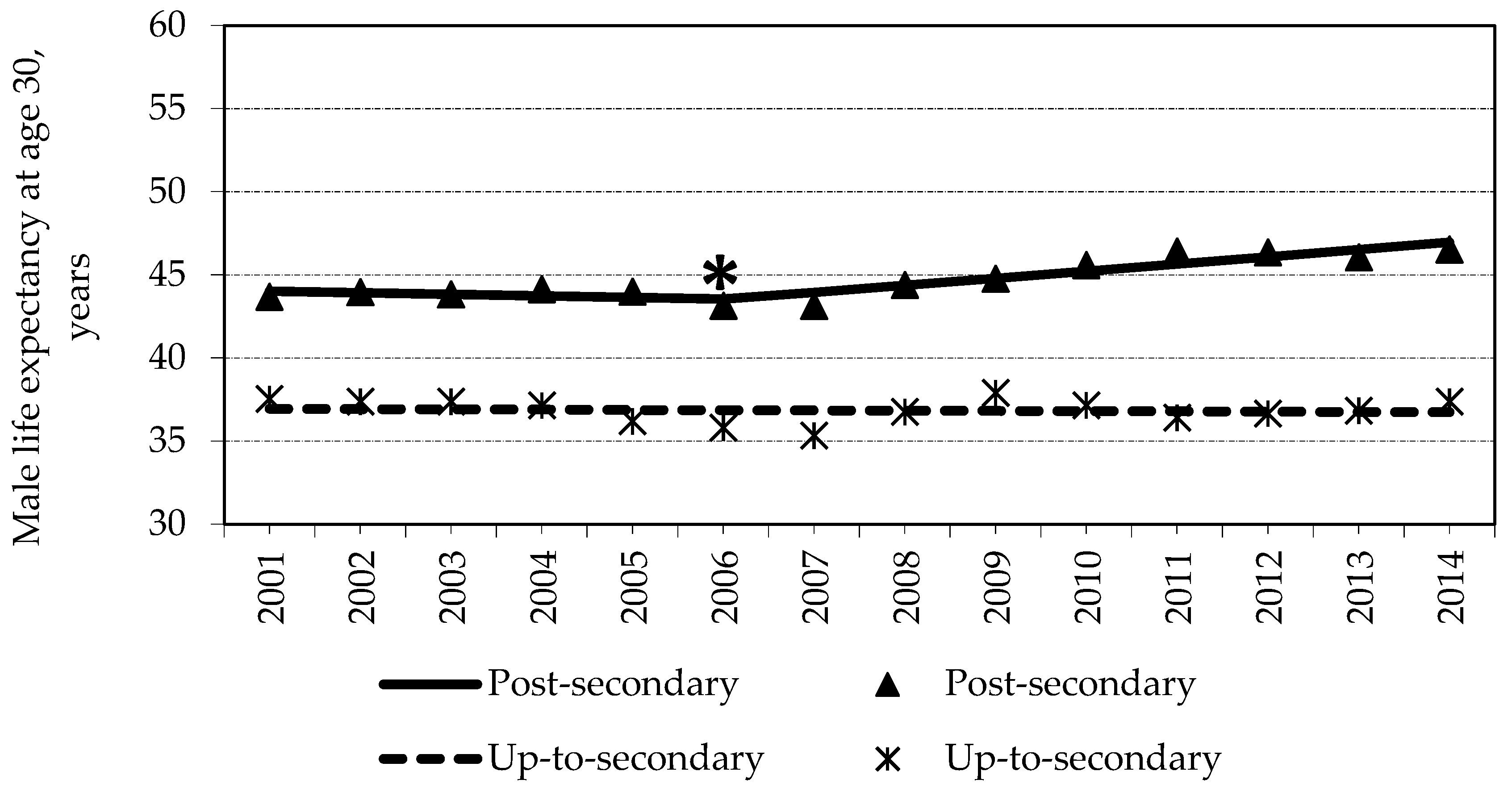
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ministry of Health of the Republic of Lithuania. Lithuanian Health Strategy 2014–2025, Order No. XII-964, 26 June 2014 (in Lithuanian). Available online: https://e-seimas.lrs.lt/portal/legalAct/lt/TAD/35834810004f11e4b0ef967b19d90c08?jfwid=-fxdp770g (accessed on 20 June 2020).
- Eurohealth. Reducing inequalities in Health and Health Care. In Proceedings of the 7th European Public Health Conference, Scotland, UK, 19–22 November 2015; Volume 21. Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/272660/EuroHealth_V21n1_WEB_060315.pdf (accessed on 3 June 2020).
- Crombie, I.K.; Irvine, L.; Elliot, L.; Wallace, H. Closing the Health Inequalities Gap: An International Perspective; WHO Regional Office for Europe: Copenhagen, Denmark, 2005. [Google Scholar]
- Ministry of Health of the Republic of Lithuania. Action Plan for Reducing Health Inequalities in Lithuania 2014–2023, Order No. V-815, 16 July 2014 (in Lithuanian). Available online: https://e-seimas.lrs.lt/portal/legalAct/lt/TAD/40be0b700df611e48595a3375cdcc8a3?jfwid=-9dzqntxh8 (accessed on 20 June 2020).
- Ministry of Health of the Republic of Poland. Poland’s Narodowy Program Drowia 2016–2020. Available online: http://www.archiwum.mz.gov.pl/zdrowie-i-profilaktyka/narodowy-program-zdrowia/npz-2016-2020 (accessed on 4 June 2020).
- World Health Organiation. Health 2020: A European Policy Framework and Strategy for the 21st Century. Regional Office for Europe. 2013. Available online: https://www.euro.who.int/data/assets/pdf_file/0011/199532/Health2020-Long.pdf (accessed on 18 June 2020).
- Valentienė, J.; Nedzinskienė, L.; Liuima, V.; Mekšriūnaitė, S.; Sauliūnė, S.; Kaselienė, S.; Meščeriakova-Veliulienė, O. Monitoring and Evaluation of Health Inequalities; Institute of Hygiene: Vilnius, Lithuania, 2016. [Google Scholar]
- Eurostat. Eurostat Database. Available online: https://ec.europa.eu/eurostat/documents/3433488/5565012/KS-SF-10-024-EN.PDF/f2caf9d2-38104088-bdbe-2f636e6ecc48 (accessed on 20 June 2020).
- Luy, M.; Wegner-Siegmundt, C.; Wiedemann, A.; Spijker, J. Life expectancy by education, income and occupation in Germany: Estimations using the longitudinal survival method. CPoS 2015, 40, 339–436. [Google Scholar] [CrossRef]
- Kinge, J.M.; Modalsli, J.H.; Øverland, S.; Gjessing, H.K.; Tollånes, M.C.; Knudsen, A.K.; Vollset, S.E. Association of Household Income with Life Expectancy and Cause-Specific Mortality in Norway, 2005–2015. JAMA 2019, 321, 1916–1925. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Valverde, J.R.; Bopp, M.; Brønnum-Hansen, H.; Deboosere, P.; Kalediene, R.; Nusselder, W.J. Determinants of inequalities in life expectancy: An international comparative study of eight risk factors. Lancet Public Health 2019, 4, e529–e537. [Google Scholar] [CrossRef] [Green Version]
- OECD/EU. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France; Available online: https://doi.org/10.1787/health_glance_eur-2018-en (accessed on 18 June 2020).
- Eurostat. Eurostat Database. Available online: https://ec.europa.eu/eurostat/data/database (accessed on 18 June 2020).
- Van Baal, P.; Peters, F.; Mackenbach, J.; Nusselder, W. Forecasting differences in life expectancy by education. Popul. Stud. 2016, 70, 201–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics Lithuania. Official Statistics Portal. Available online: https://osp.stat.gov.lt/statistiniu-rodikliu-analize (accessed on 14 February 2021).
- European Commission. Health Inequalities in the EU—Final Report of a Consortium 2013. Available online: http://ec.europa.eu/health/social_determinants/docs/healthinequalitiesineu_2013_en.pdf (accessed on 15 February 2021).
- OECD/European Observatory on Health Systems and Policies, Lithuania: Country Health Profile 2019. Available online: https://doi.org/10.1787/35913deb-en (accessed on 15 February 2021).
- Constitution of Lithuania. Available online: https://www.lrs.lt/home/Konstitucija/Konstitucija.htm/ (accessed on 15 February 2021).
- Statistics Lithuania. Official Statistics Portal. Censuses, Population and Housing Census. Available online: https://osp.stat.gov.lt/documents/10180/217110/Gyv+pagal+i%C5%A1silavinima_ir_kalbu_mokejima.pdf/b75c5e7a-e733-48fa-95e4-83d485c6726a (accessed on 15 February 2021).
- See Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation Tests for Joinpoint Regression with Applications to Cancer Rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Kalėdienė, R.; Starkuvienė, S.; Petrauskienė, J. Inequalities in life expectancy by education and socio-economic transition in Lithuania. Medicina 2008, 44, 713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalediene, R.; Petrauskiene, J. Inequalities in life expectancy in Lithuania by level of education. Scand. J. Public Health. 2000, 28, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Kalediene, R.; Petrauskiene, J. Inequalities in mortality by education and socio-economic transition in Lithuania: Equal opportunities? Public Health 2005, 119, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Jasilionis, D.; Stankūnienė, V.; Shkolnikov, V.M. Socio-Demographic Mortality Differentials in Lithuania, 2001–2004. Outcomes from the first census-linked study Vilnius: Statistics Lithuania; Institute for Social Research: Vilnius, Lithuania, 2016. [Google Scholar]
- Jasilionis, D.; Stankūnienė, V.; Ambrozaitienė, D.; Trofimova, O. Linkages between population census and demographic statistics data: Methodological approaches and research opportunities. Lith. J. Stat. 2014, 53, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Kunst, A.E.; Bos, V.; Andersen, O.; Cardano, M.; Costa, G.; Harding, S.; Hemström, Ö.; Layte, R.; Regidor, E.; Reid, A.; et al. Monitoring of trends in socioeconomic inequalities in mortality: Experiences from a European project. Demogr. Res. 2004, 2, 229–254. [Google Scholar] [CrossRef]
- Ministry of Health of the Republic of Lithuania, Lithuanian Health Program 1998–2010, Order No. VIII-833, 2 July 1998 (in Lithuanian). Available online: https://e-seimas.lrs.lt/portal/legalAct/lt/TAD/TAIS.60036?jfwid=rivwzvpvg (accessed on 20 June 2020).
- Institute of Hygiene. Official Statistics Portal. Available online: http://www.hi.lt/en/the-health-indicators-of-lithuania.html (accessed on 16 February 2021).
- Kalediene, R.; Prochorskas, R.; Sauliune, S. Socio-economic mortality inequalities in Lithuania during 2001–2009: The record linkage study. Public Health 2015, 129, 1645–1651. [Google Scholar] [CrossRef] [PubMed]
- Sauliune, S.; Petrauskiene, J.; Kalediene, R. Alcohol-related injuries and alcohol control policy in Lithuania: Effect of the year of Sobriety, 2008. Alcohol Alcohol. 2012, 47, 458–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denney, J.T.; Rogers, R.G.; Hummer, R.A.; Pampel, F.C. Education inequality in mortality: The age and gender specific mediating effects of cigarette smoking. Soc. Sci. Res. 2010, 39, 662–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laaksonen, M.; Talala, K.; Martelin, T.; Rahkonen, O.; Roos, E.; Helakorpi, S.; Laatikainen, T.; Prättälä, R. Health behaviours as explanations for educational level differences in cardiovascular and all-cause mortality: A follow-up of 60,000 men and women over 23 years. Eur. J. Public Health 2010, 18, 38–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesceriakova-Veliuliene, O.; Kalediene, R.; Sauliune, S. Changes in inequalities of mortality by education level in Lithuania between 2001 and 2014. Public Health 2020, 182, 88–94. [Google Scholar] [CrossRef] [PubMed]
- OECD, Reviews of Health Systems: Lithuania. 2018. Available online: https://www.oecd.org/health/health-systems/OECD-Reviews-of-Health-Systems-Lithuania-2018-Assessment-and-Recommendations.pdf (accessed on 1 June 2020).
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019; Available online: https://doi.org/10.1787/4dd50c09-en (accessed on 1 June 2020).
- World Health Organization. Health21: The health for All Policy Framework for the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Causes of Death | Sex | 2001 | 2014 | ||||
|---|---|---|---|---|---|---|---|
| Up-to- Secondary | Post- Secondary | Difference * | Up-to- Secondary | Post- Secondary | Difference * | ||
| Cardiovascular diseases | Males | 7.39 | 6.93 | 0.46 | 6.91 | 6.50 | 0.41 |
| Females | 7.85 | 6.13 | 1.72 | 9.78 | 5.56 | 4.22 | |
| Cancer | Males | 2.95 | 3.31 | −0.36 | 3.07 | 3.58 | −0.51 |
| Females | 2.56 | 3.36 | 0.80 | 2.83 | 4.08 | −1.25 | |
| External causes | Males | 3.67 | 2.68 | 0.99 | 3.13 | 1.35 | 1.78 |
| Females | 1.21 | 0.74 | 0.47 | 0.97 | 0.62 | 0.35 | |
| Diseases of the digestive system | Males | 0.66 | 0.45 | 0.21 | 1.09 | 0.68 | 0.41 |
| Females | 0.60 | 0.36 | 0.24 | 1.03 | 0.70 | 0.33 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesceriakova-Veliuliene, O.; Kalediene, R.; Sauliune, S.; Urbonas, G. Inequalities in Life Expectancy by Education and Its Changes in Lithuania during 2001–2014. Medicina 2021, 57, 245. https://doi.org/10.3390/medicina57030245
Mesceriakova-Veliuliene O, Kalediene R, Sauliune S, Urbonas G. Inequalities in Life Expectancy by Education and Its Changes in Lithuania during 2001–2014. Medicina. 2021; 57(3):245. https://doi.org/10.3390/medicina57030245
Chicago/Turabian StyleMesceriakova-Veliuliene, Olga, Ramune Kalediene, Skirmante Sauliune, and Gvidas Urbonas. 2021. "Inequalities in Life Expectancy by Education and Its Changes in Lithuania during 2001–2014" Medicina 57, no. 3: 245. https://doi.org/10.3390/medicina57030245