
Effect of Enamel Matrix Derivatives on Osteoclast Formation from PBMC of Periodontitis Patients and Healthy Individuals after Interaction with Activated Endothelial Cells


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. HUVECs Culture and PBMCs Isolation
2.3. Isolation of Adherent and Non-Adherent Fractions
2.4. Trans-Endothelial Migration of PBMCs
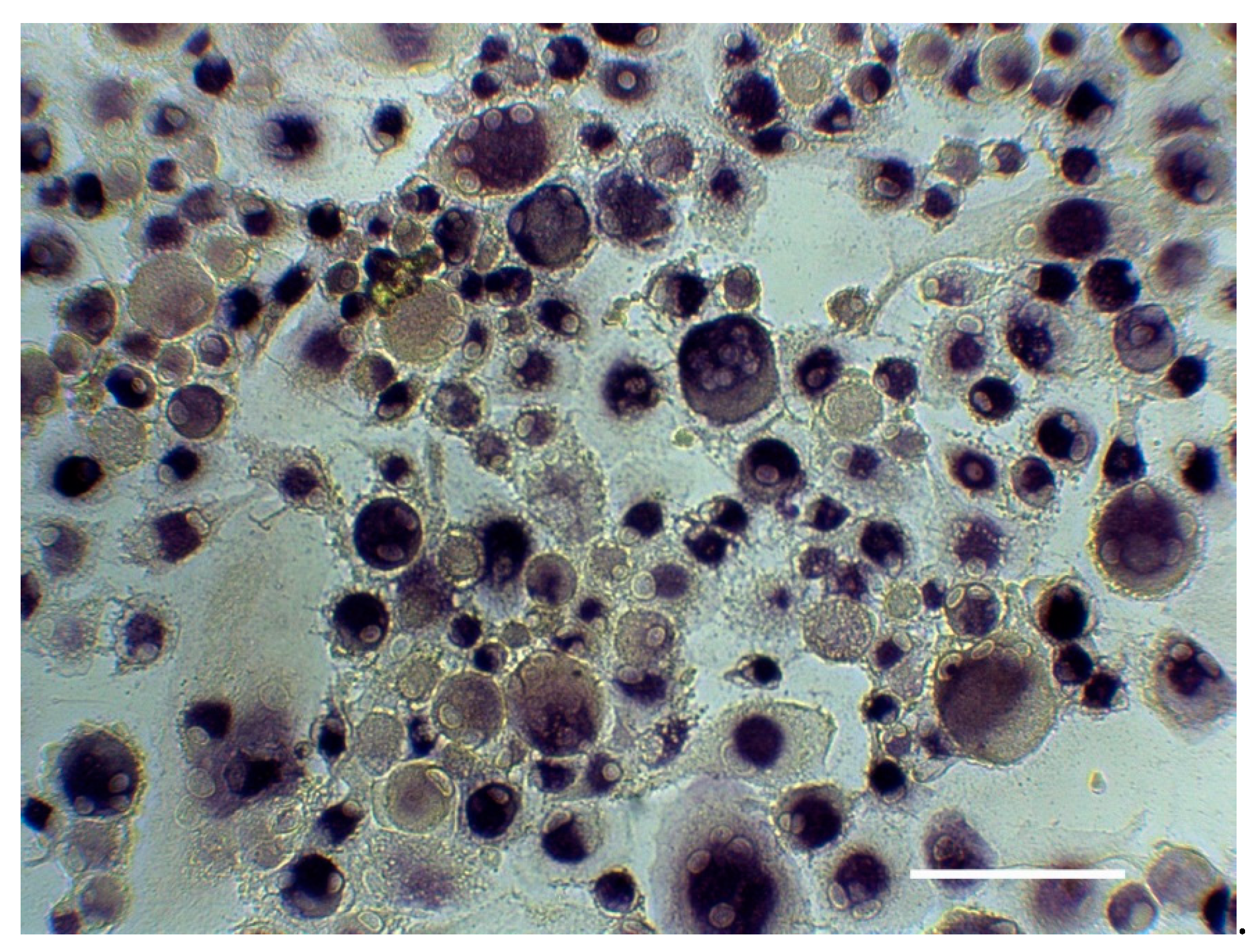
2.5. Generation of Osteoclast-Like Cells from Different PBMCs Fraction
2.6. Statistical Analysis
3. Results
3.1. Study Participants’ Demographical Characteristics and Clinical Parameters
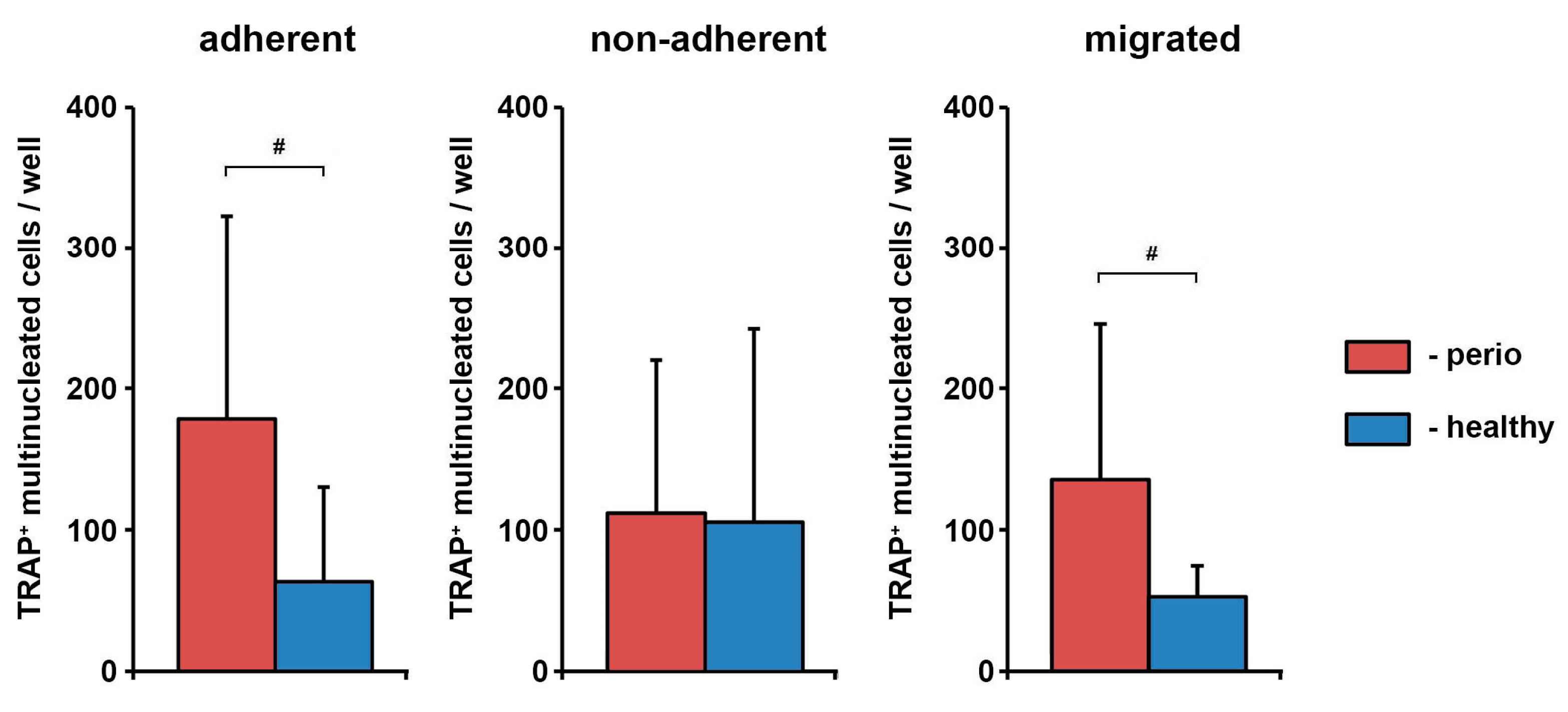
3.2. Osteoclasts-Like Cells in Different PBMCs Fraction Isolated from Healthy Individuals and Periodontitis Patients
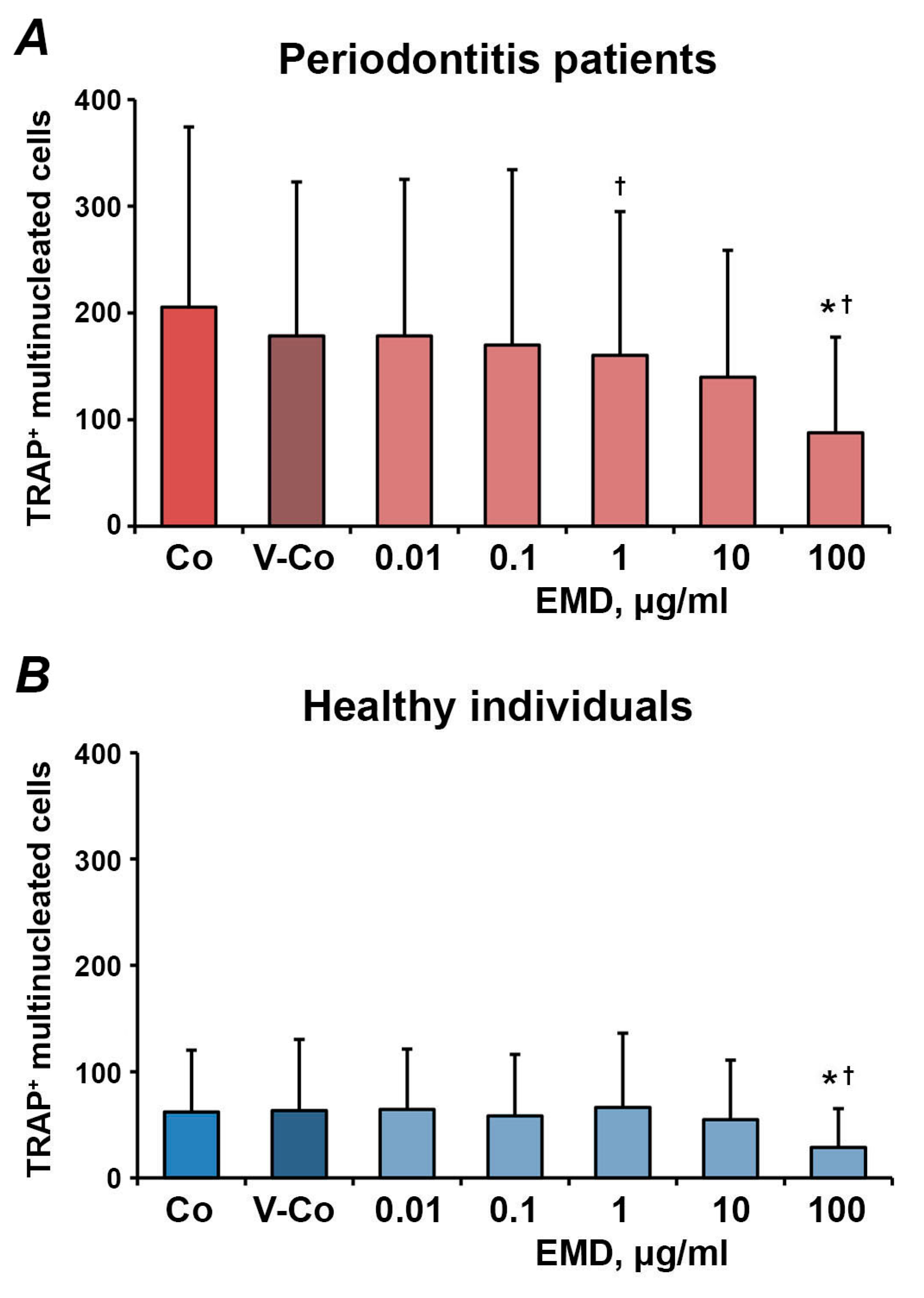
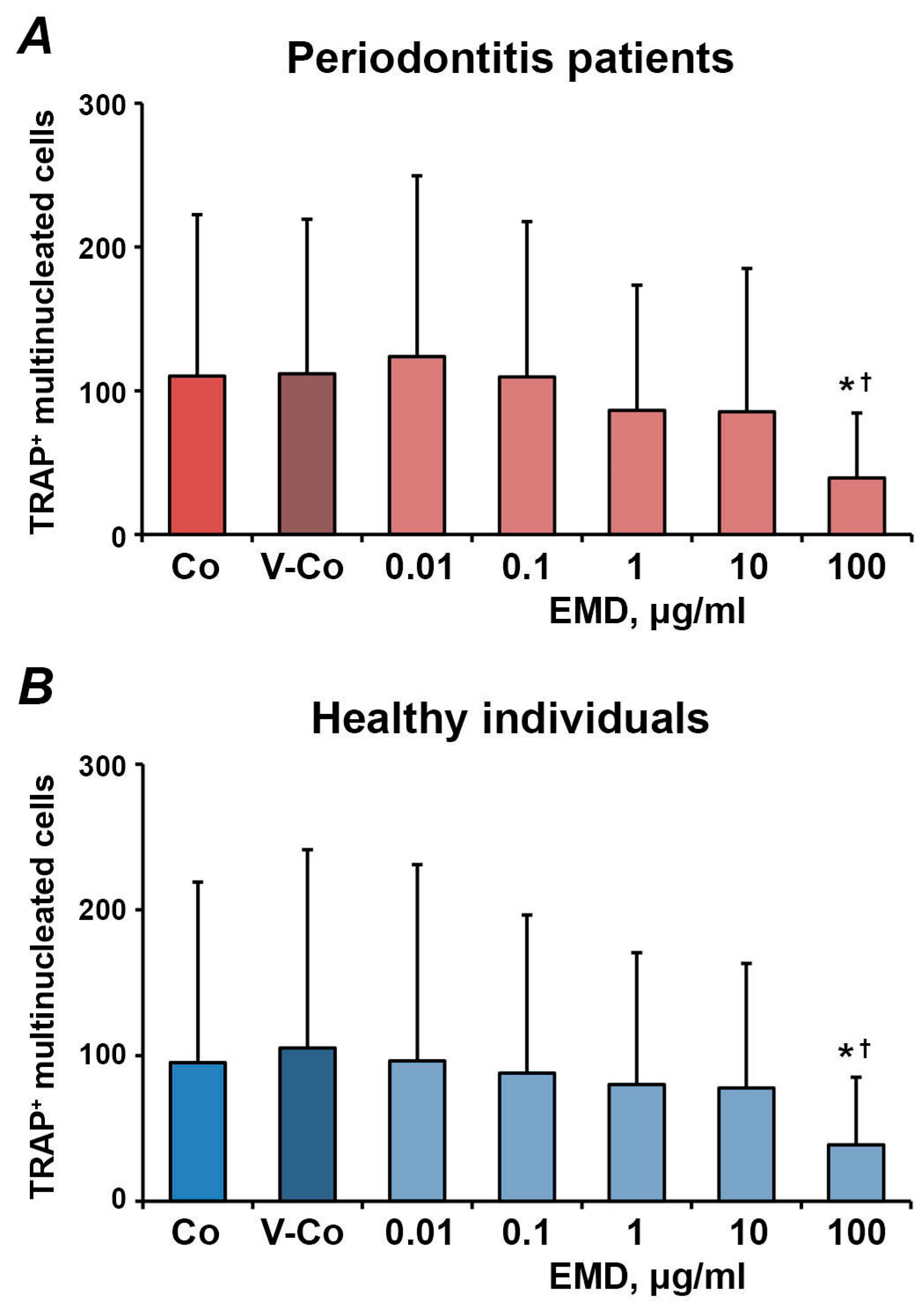
3.3. Effect of EMD on the Number of Osteoclast-Like Cells in Different PBMCs’ Fractions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roodman, G.D. Advances in bone biology: The osteoclast. Endocr. Rev. 1996, 17, 308–332. [Google Scholar] [CrossRef]
- Shalhoub, V.; Faust, J.; Boyle, W.J.; Dunstan, C.R.; Kelley, M.; Kaufman, S.; Scully, S.; Van, G.; Lacey, D.L. Osteoprotegerin and osteoprotegerin ligand effects on osteoclast formation from human peripheral blood mononuclear cell precursors. J. Cell. Biochem. 1999, 72, 251–261. [Google Scholar] [CrossRef]
- Teitelbaum, S.L.; Ross, F.P. Genetic regulation of osteoclast development and function. Nat. Rev. Genet. 2003, 4, 638–649. [Google Scholar] [CrossRef]
- Kayal, R.A. The role of osteoimmunology in periodontal disease. Biomed Res. Int. 2013, 2013, 639368. [Google Scholar] [CrossRef]
- Roodman, G.D. Cell biology of the osteoclast. Exp. Hematol. 1999, 27, 1229–1241. [Google Scholar] [CrossRef]
- Brunetti, G.; Colucci, S.; Pignataro, P.; Coricciati, M.; Mori, G.; Cirulli, N.; Zallone, A.; Grassi, F.R.; Grano, M. T cells support osteoclastogenesis in an in vitro model derived from human periodontitis patients. J. Periodontol. 2005, 76, 1675–1680. [Google Scholar] [CrossRef]
- Tjoa, S.T.; de Vries, T.J.; Schoenmaker, T.; Kelder, A.; Loos, B.G.; Everts, V. Formation of osteoclast-like cells from peripheral blood of periodontitis patients occurs without supplementation of macrophage colony-stimulating factor. J. Clin. Periodontol. 2008, 35, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Herrera, B.S.; Bastos, A.S.; Coimbra, L.S.; Teixeira, S.A.; Rossa, C., Jr.; Van Dyke, T.E.; Muscara, M.N.; Spolidorio, L.C. Peripheral blood mononuclear phagocytes from patients with chronic periodontitis are primed for osteoclast formation. J. Periodontol. 2014, 85, e72–e81. [Google Scholar] [CrossRef] [PubMed]
- McGowan, N.W.; Walker, E.J.; Macpherson, H.; Ralston, S.H.; Helfrich, M.H. Cytokine-activated endothelium recruits osteoclast precursors. Endocrinology 2001, 142, 1678–1681. [Google Scholar] [CrossRef] [PubMed]
- Kindle, L.; Rothe, L.; Kriss, M.; Osdoby, P.; Collin-Osdoby, P. Human microvascular endothelial cell activation by IL-1 and TNF-alpha stimulates the adhesion and transendothelial migration of circulating human CD14+ monocytes that develop with RANKL into functional osteoclasts. J. Bone Min. Res. 2006, 21, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Venezia, E.; Goldstein, M.; Boyan, B.D.; Schwartz, Z. The use of enamel matrix derivative in the treatment of periodontal defects: A literature review and meta-analysis. Crit. Rev. Oral Biol. Med. 2004, 15, 382–402. [Google Scholar] [CrossRef] [Green Version]
- Esposito, M.; Grusovin, M.G.; Papanikolaou, N.; Coulthard, P.; Worthington, H.V. Enamel matrix derivative (Emdogain) for periodontal tissue regeneration in intrabony defects. A Cochrane systematic review. Eur. J. Oral Implant. 2009, 2, 247–266. [Google Scholar]
- Andrukhov, O.; Gemperli, A.C.; Tang, Y.; Howald, N.; Dard, M.; Falkensammer, F.; Moritz, A.; Rausch-Fan, X. Effect of different enamel matrix derivative proteins on behavior and differentiation of endothelial cells. Dent. Mater. 2015, 31, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Grandin, H.M.; Gemperli, A.C.; Dard, M. Enamel matrix derivative: A review of cellular effects in vitro and a model of molecular arrangement and functioning. Tissue Eng. Part B Rev. 2012, 18, 181–202. [Google Scholar] [CrossRef]
- Bosshardt, D.D. Biological mediators and periodontal regeneration: A review of enamel matrix proteins at the cellular and molecular levels. J. Clin. Periodontol. 2008, 35, 87–105. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, T.; Kasai, H.; Yamaguchi, K.; Nishihara, T. Enamel matrix derivative promotes osteoclast cell formation by RANKL production in mouse marrow cultures. J. Dent. 2005, 33, 749–755. [Google Scholar] [CrossRef]
- Itoh, N.; Kasai, H.; Ariyoshi, W.; Harada, E.; Yokota, M.; Nishihara, T. Mechanisms involved in the enhancement of osteoclast formation by enamel matrix derivative. J. Periodontal Res. 2006, 41, 273–279. [Google Scholar] [CrossRef]
- Gruber, R.; Roos, G.; Caballe-Serrano, J.; Miron, R.; Bosshardt, D.D.; Sculean, A. TGF-betaRI kinase activity mediates Emdogain-stimulated in vitro osteoclastogenesis. Clin. Oral Investig. 2014, 18, 1639–1646. [Google Scholar] [CrossRef]
- Nishiguchi, M.; Yuasa, K.; Saito, K.; Fukumoto, E.; Yamada, A.; Hasegawa, T.; Yoshizaki, K.; Kamasaki, Y.; Nonaka, K.; Fujiwara, T.; et al. amelogenin is a negative regulator of osteoclastogenesis via downregulation of RANKL, M-CSF and fibronectin expression in osteoblasts. Arch. Oral Biol. 2007, 52, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Kawana, F.; Sawae, Y.; Sahara, T.; Tanaka, S.; Debari, K.; Shimizu, M.; Sasaki, T. Porcine enamel matrix derivative enhances trabecular bone regeneration during wound healing of injured rat femur. Anat. Rec. 2001, 264, 438–446. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S68–S77. [Google Scholar] [CrossRef]
- Salamanna, F.; Maglio, M.; Borsari, V.; Giavaresi, G.; Aldini, N.N.; Fini, M. Peripheral Blood Mononuclear Cells Spontaneous Osteoclastogenesis: Mechanisms Driving the Process and Clinical Relevance in Skeletal Disease. J. Cell. Physiol. 2016, 231, 521–530. [Google Scholar] [CrossRef] [PubMed]
- de Vries, T.J.; El Bakkali, I.; Kamradt, T.; Schett, G.; Jansen, I.D.C.; D’Amelio, P. What Are the Peripheral Blood Determinants for Increased Osteoclast Formation in the Various Inflammatory Diseases Associated With Bone Loss? Front. Immunol. 2019, 10, 505. [Google Scholar] [CrossRef] [PubMed]
- Xing, L.; Schwarz, E.M.; Boyce, B.F. Osteoclast precursors, RANKL/RANK, and immunology. Immunol. Rev. 2005, 208, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Haraldsen, G.; Kvale, D.; Lien, B.; Farstad, I.N.; Brandtzaeg, P. Cytokine-regulated expression of E-selectin, intercellular adhesion molecule-1 (ICAM-1), and vascular cell adhesion molecule-1 (VCAM-1) in human microvascular endothelial cells. J. Immunol. 1996, 156, 2558–2565. [Google Scholar] [PubMed]
- Ikuta, S.; Kirby, J.A.; Shenton, B.K.; Givan, A.L.; Lennard, T.W. Human endothelial cells: Effect of TNF-alpha on peripheral blood mononuclear cell adhesion. Immunology 1991, 73, 71–76. [Google Scholar] [PubMed]
- Collison, J.L.; Carlin, L.M.; Eichmann, M.; Geissmann, F.; Peakman, M. Heterogeneity in the Locomotory Behavior of Human Monocyte Subsets over Human Vascular Endothelium In Vitro. J. Immunol. 2015, 195, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- Steffen, U.; Andes, F.T.; Schett, G. Generation and Analysis of Human and Murine Osteoclasts. Curr. Protoc. Immunol. 2019, 125, e74. [Google Scholar] [CrossRef] [PubMed]
- Lyngstadaas, S.P.; Wohlfahrt, J.C.; Brookes, S.J.; Paine, M.L.; Snead, M.L.; Reseland, J.E. Enamel matrix proteins; old molecules for new applications. Orthod. Craniofac. Res. 2009, 12, 243–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stahli, A.; Miron, R.J.; Bosshardt, D.D.; Sculean, A.; Gruber, R. Collagen Membranes Adsorb the Transforming Growth Factor-beta Receptor I Kinase-Dependent Activity of Enamel Matrix Derivative. J. Periodontol. 2016, 87, 583–590. [Google Scholar] [CrossRef]
- Suzuki, S.; Nagano, T.; Yamakoshi, Y.; Gomi, K.; Arai, T.; Fukae, M.; Katagiri, T.; Oida, S. Enamel matrix derivative gel stimulates signal transduction of BMP and TGF-{beta}. J. Dent. Res. 2005, 84, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Yagi, Y.; Suda, N.; Yamakoshi, Y.; Baba, O.; Moriyama, K. In vivo application of amelogenin suppresses root resorption. J. Dent. Res. 2009, 88, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Yasui, T.; Kadono, Y.; Nakamura, M.; Oshima, Y.; Matsumoto, T.; Masuda, H.; Hirose, J.; Omata, Y.; Yasuda, H.; Imamura, T.; et al. Regulation of RANKL-induced osteoclastogenesis by TGF-beta through molecular interaction between Smad3 and Traf6. J. Bone Min. Res. 2011, 26, 1447–1456. [Google Scholar] [CrossRef]
- Tokunaga, T.; Mokuda, S.; Kohno, H.; Yukawa, K.; Kuranobu, T.; Oi, K.; Yoshida, Y.; Hirata, S.; Sugiyama, E. TGFbeta1 Regulates Human RANKL-Induced Osteoclastogenesis via Suppression of NFATc1 Expression. Int. J. Mol. Sci. 2020, 21, 800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G.; Nemcovsky, C.; Donos, N.; Lyngstadaas, S.P.; Deschner, J.; Dard, M.; et al. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef]
- He, J.; Jiang, J.; Safavi, K.E.; Spangberg, L.S.; Zhu, Q. Emdogain promotes osteoblast proliferation and differentiation and stimulates osteoprotegerin expression. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 97, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Petretto, E.; Gordon, S.; Bassett, J.H.D.; Williams, G.R.; Behmoaras, J. Common signalling pathways in macrophage and osteoclast multinucleation. J. Cell Sci. 2018, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miron, R.J.; Zohdi, H.; Fujioka-Kobayashi, M.; Bosshardt, D.D. Giant cells around bone biomaterials: Osteoclasts or multinucleated giant cells? Acta Biomater. 2016, 46, 15–28. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adhesion Experiments | TEM Experiments | |||
|---|---|---|---|---|
| Healthy, n = 8 | Periodontitis, n = 9 | Healthy, n = 8 | Periodontitis, n = 7 | |
| Age, years | 37.5 ± 10.5 | 43.8 ± 7.0 | 45.1 ± 9.7 | 48.7 ± 6.0 |
| Gender, m/f | 5/3 | 7/2 | 5/3 | 4/3 |
| PPD, mean, mm | 3.66 ± 0.49 | 3.60 ± 1.10 | ||
| PPD, range, mm | 0–3 | 0–10 | 0–3 | 0–12 |
| BoP, % | 35.8 ± 27.2 | 45.0 ± 32.9 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durstberger, G.; Nguyen, P.Q.; Hohensinner, V.; Pietschmann, P.; Rausch-Fan, X.; Andrukhov, O. Effect of Enamel Matrix Derivatives on Osteoclast Formation from PBMC of Periodontitis Patients and Healthy Individuals after Interaction with Activated Endothelial Cells. Medicina 2021, 57, 269. https://doi.org/10.3390/medicina57030269
Durstberger G, Nguyen PQ, Hohensinner V, Pietschmann P, Rausch-Fan X, Andrukhov O. Effect of Enamel Matrix Derivatives on Osteoclast Formation from PBMC of Periodontitis Patients and Healthy Individuals after Interaction with Activated Endothelial Cells. Medicina. 2021; 57(3):269. https://doi.org/10.3390/medicina57030269
Chicago/Turabian StyleDurstberger, Gerlinde, Phuong Quynh Nguyen, Verena Hohensinner, Peter Pietschmann, Xiaohui Rausch-Fan, and Oleh Andrukhov. 2021. "Effect of Enamel Matrix Derivatives on Osteoclast Formation from PBMC of Periodontitis Patients and Healthy Individuals after Interaction with Activated Endothelial Cells" Medicina 57, no. 3: 269. https://doi.org/10.3390/medicina57030269