
Treatment Modalities of Recurrent Oral Mucosal Melanoma In Situ

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
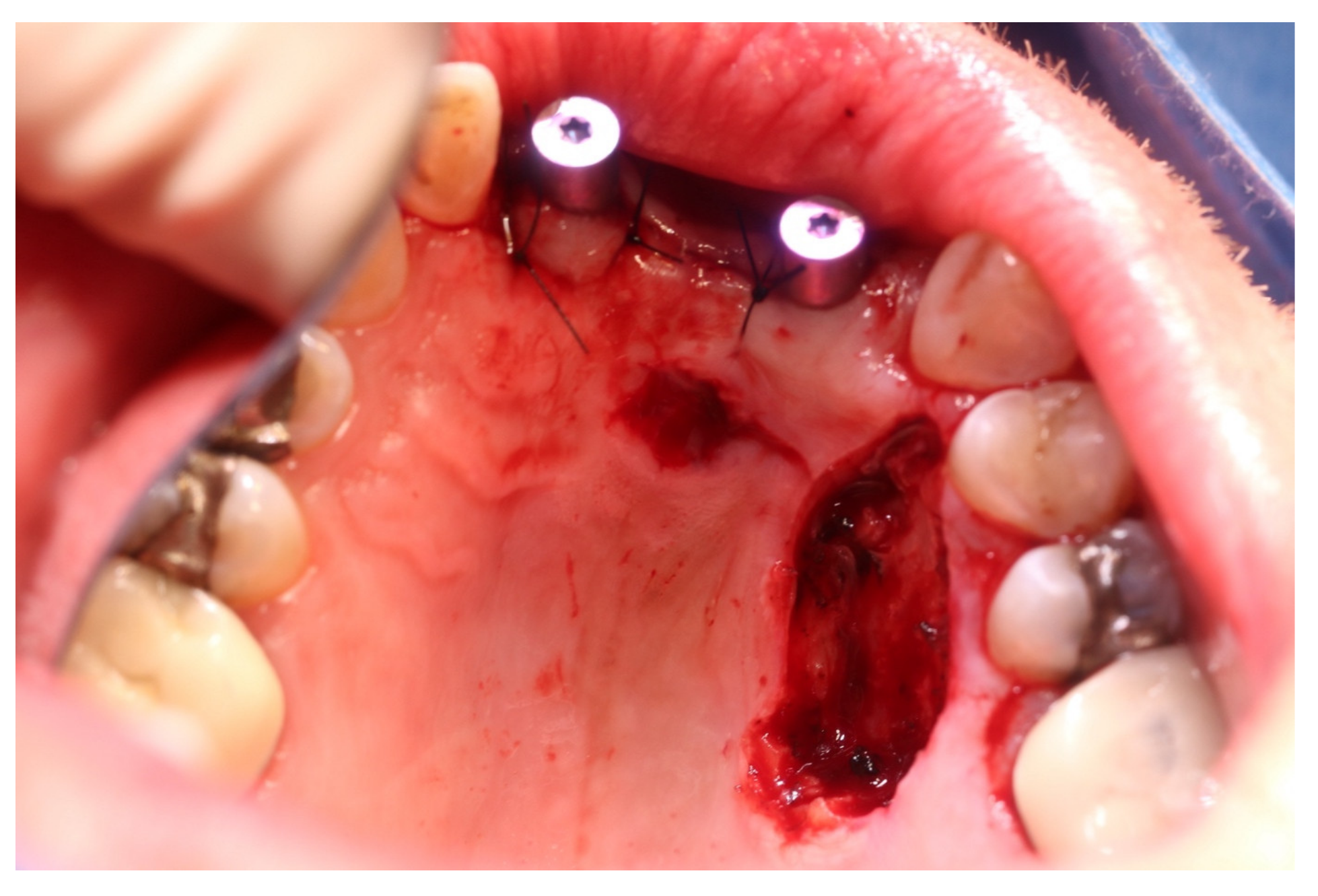
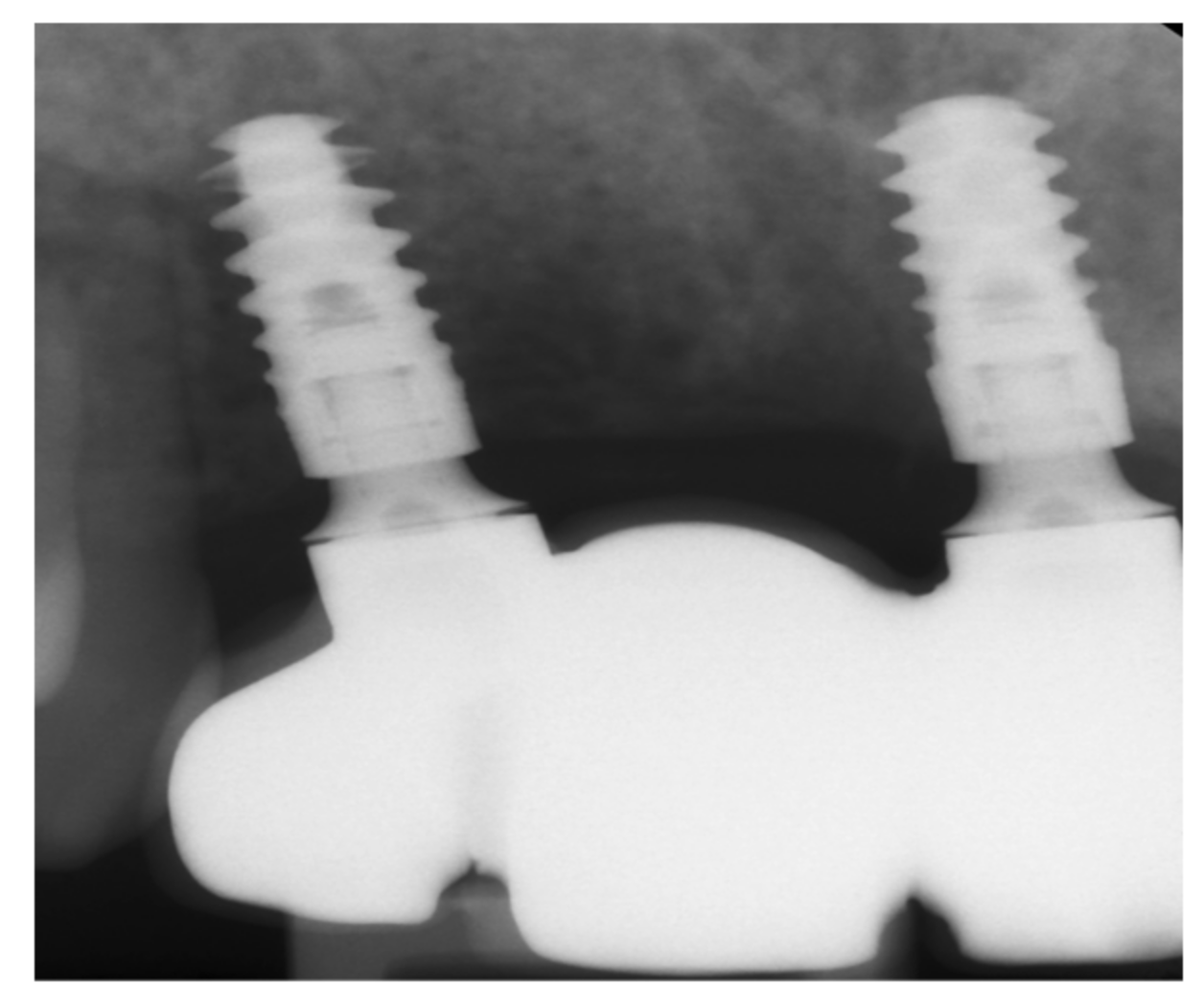
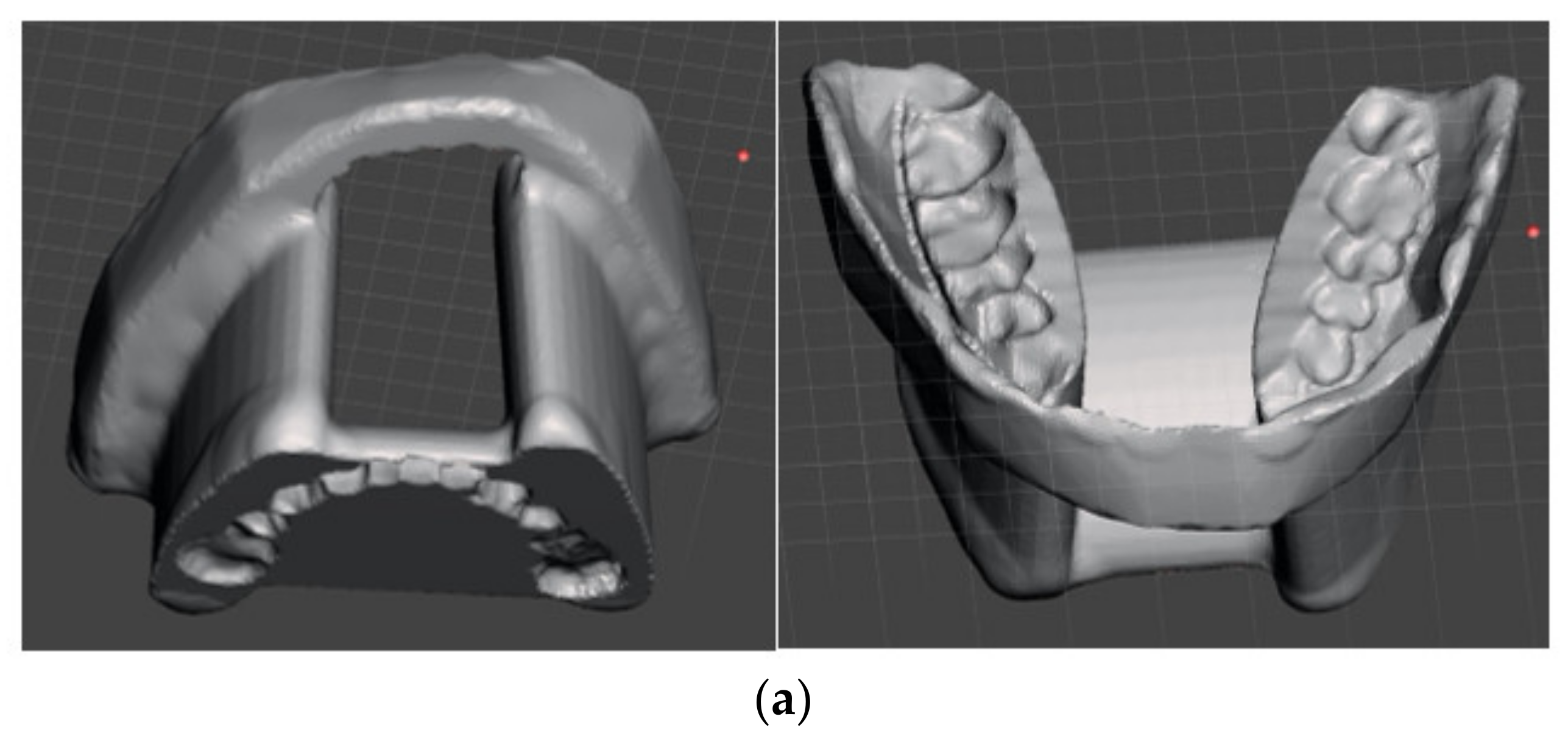
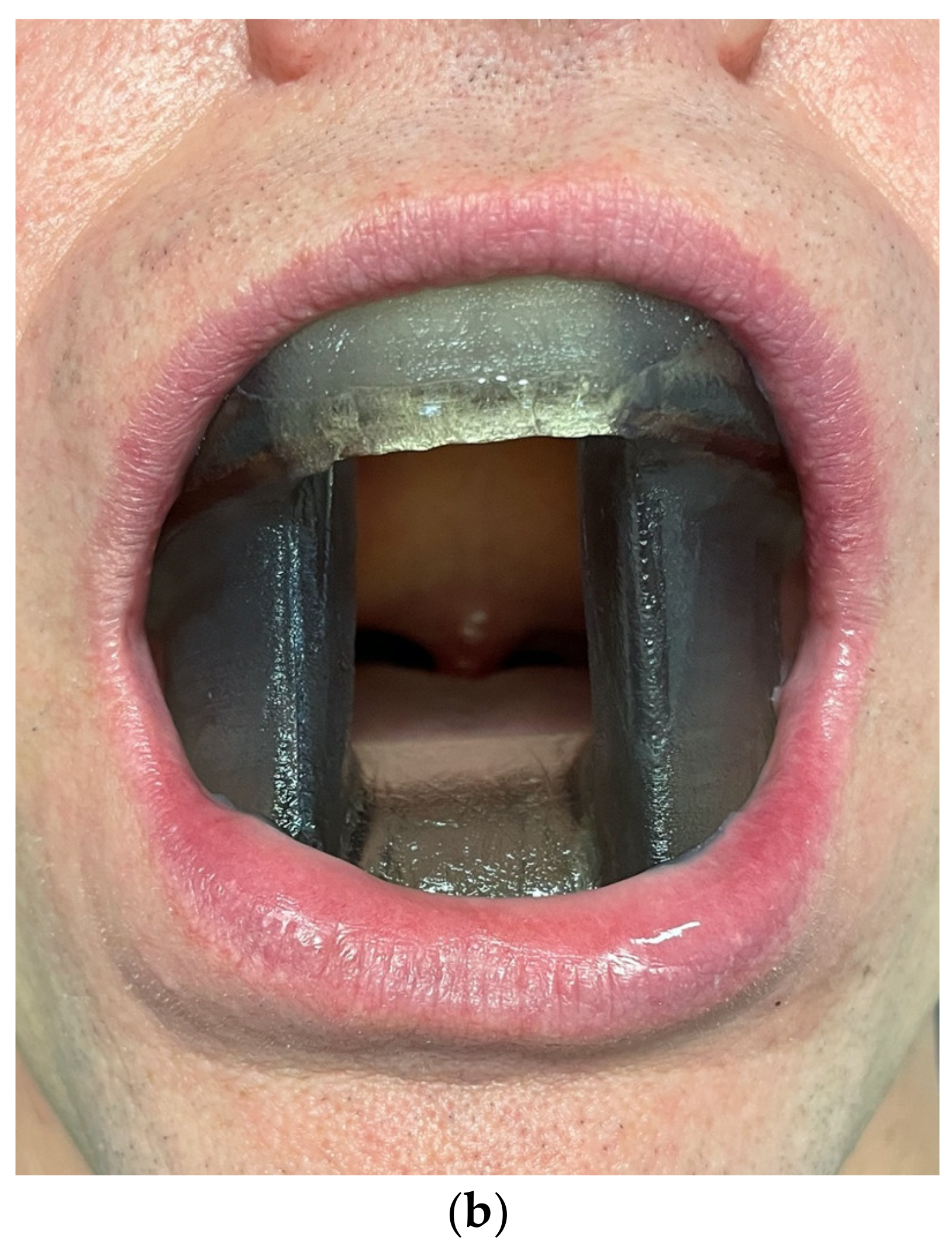
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ashok, S.; Damera, S.; Ganesh, S.; Karri, R. Oral Malignant Melanoma. J. Oral Maxillofac. Pathol. 2020, 24, S82–S85. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, A.J. The Antimicrobial Properties of Melanocytes, Melanosomes and Melanin and the Evolution of Black Skin. J. Theor. Biol. 2001, 211, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Plonka, M.P.; Passeron, T.; Brenner, M.; Tobin, D.J.; Shibahara, S.; Thomas, A.; Slominski, A.; Kadekaro, A.L.; Hershkovitz, D.; Peters, E.; et al. What Are Melanocytes Really Doing All Day Long…? Exp. Dermatol. 2009, 18, 799–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardo, N.; Della Corte, M.; Pelaia, C.; Piazzetta, G.; Lobello, N.; Del Duca, E.; Bennardo, L.; Nisticò, S. Primary Mucosal Melanoma Presenting with a Unilateral Nasal Obstruction of the Left Inferior Turbinate. Medicina 2021, 57, 359. [Google Scholar] [CrossRef] [PubMed]
- Tchernev, G.; Lotti, T.; Wollina, U. Palatal Melanoma: “The Silent Killer”. Open Access Maced. J. Med. Sci. 2018, 6, 364–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandan, S.N.; Shetty, S.K.; Deepa, B.V. Primary malignant melanoma of oral mucosa–Report of two cases. Contemp. Clin. Dent. 2020, 11, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Eigentler, T.; Hoge, J.; Garbe, C.; Schadendorf, D. S3-Leitlinie Zur Diagnostik, Therapie Und Nachsorge Des Melanoms; Leitlinienprogramm Onkologie der Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V. (AWMF); Deutschen Krebsgesellschaft e.V. (DKG); Deutschen Krebshilfe (DKH): Berlin, Germany, 2020. [Google Scholar]
- Patrick, J.R.; Fenske, N.A.; Messina, J.L. Primary Mucosal Melanoma. J. Am. Acad. Dermatol. 2007, 56, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, R.D.; Spencer, S.A.; Lydiatt, W. Mucosal Melanoma: A Clinically and Biologically Unique Disease Entity. J. Natl. Compr. Cancer Netw. 2012, 10, 345–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, D.; Pandey, P.; Singh, M.K.; Kudva, S. Prevalence of malignant melanoma in anatomical sites of the oral cavity: A meta-analysis. J. Oral Maxillofac. Pathol. 2019, 23, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Casiraghi, O.; Lefèvre, M. Undifferentiated Malignant Round Cell Tumors of the Sinonasal Tract and Nasopharynx. Ann. Pathol. 2009, 29, 296–312. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Mallet, Y.; Mirabel, X.; Van, J.T.; Lefebvre, J.-L. Primary Mucosal Melanoma of Head and Neck: Prognostic Value of Clear Margins. Laryngoscope 2006, 116, 993–995. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.; Jamdar, S.F.; Jangra, J.; Beaiji, S.M.A.A.A. Oral malignant melanoma: An aggressive clinical entity-Report of a rare case with review of literature. J. Int. Soc. Prev. Community Dent. 2016, 6, 176–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López, F.; Rodrigo, J.P.; Cardesa, A.; Triantafyllou, A.; Devaney, K.O.; Mendenhall, W.M.; Haigentz, M.; Strojan, P.; Do, P.K.P.; Bradford, C.R.; et al. Update on primary head and neck mucosal melanoma. Head Neck 2014, 38, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, S.-K.; Jeong, J.H.; Ahn, K.-M.; Yoo, C.W.; Park, J.Y.; Choi, S.W. Desmoplastic melanoma of the oral cavity: Diagnostic pitfalls and clinical characteristics. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Castro, M.S.; Reis, B.S.D.A.; Nogueira, D.A.; De Carli, M.L.; Hanemann, J.A.C.; Pereira, A.A.C.; De Almeida, O.P.; Sperandio, F.F. Primary oral melanoma: A clinicopathologic review and case presentation. Quintessence Int. 2017, 48, 815–827. [Google Scholar] [PubMed]
- Shastri, M.; Paterson, T.; Bisase, B.S.; Barrett, A.W. Malignant Melanoma in Situ of the Palate: Radical Treatment or “Watch and Wait”? Oral Oncol. 2020, 110, 104805. [Google Scholar] [CrossRef] [PubMed]
- Medina, J.E.; Ferlito, A.; Pellitteri, P.K.; Shaha, A.R.; Khafif, A.; Devaney, K.O.; Fisher, S.R.; O’Brien, C.J.; Byers, R.M.; Robbins, K.T.; et al. Current management of mucosal melanoma of the head and neck. J. Surg. Oncol. 2003, 83, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.C.; Chen, Y.F.; Jiang, Y.E.; Hu, Z.D.; Yang, A.K.; Song, M. Treatment and Prognosis of Oral Mucosal Melanoma. Oral Oncol. 2012, 48, 647–652. [Google Scholar] [CrossRef] [PubMed]











Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker, P.; Pabst, A.; Bjelopavlovic, M.; Müller, D.; Kämmerer, P.W. Treatment Modalities of Recurrent Oral Mucosal Melanoma In Situ. Medicina 2021, 57, 965. https://doi.org/10.3390/medicina57090965
Becker P, Pabst A, Bjelopavlovic M, Müller D, Kämmerer PW. Treatment Modalities of Recurrent Oral Mucosal Melanoma In Situ. Medicina. 2021; 57(9):965. https://doi.org/10.3390/medicina57090965
Chicago/Turabian StyleBecker, Philipp, Andreas Pabst, Monika Bjelopavlovic, Daniel Müller, and Peer W. Kämmerer. 2021. "Treatment Modalities of Recurrent Oral Mucosal Melanoma In Situ" Medicina 57, no. 9: 965. https://doi.org/10.3390/medicina57090965